See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/46037656 Social cognition in schizophrenia: Cognitive and affective factors Article in Cognitive Neuropsychiatry · January 2011 DOI: 10.1080/13546805.2010.492693 · Source: PubMed CITATIONS 39 READS 31 3 authors, including: Ido Ziv College for Academic Studies 5 PUBLICATIONS 44 CITATIONS SEE PROFILE David Leiser Ben-Gurion University of the Negev 92 PUBLICATIONS 931 CITATIONS SEE PROFILE All content following this page was uploaded by David Leiser on 25 November 2016. The user has requested enhancement of the downloaded file. All in-text references underlined in blue are linked to publications on ResearchGate, letting you access and read them immediately.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Seediscussions,stats,andauthorprofilesforthispublicationat:https://www.researchgate.net/publication/46037656
Socialcognitioninschizophrenia:Cognitiveandaffectivefactors
ArticleinCognitiveNeuropsychiatry·January2011
DOI:10.1080/13546805.2010.492693·Source:PubMed
CITATIONS
39
READS
31
3authors,including:
IdoZiv
CollegeforAcademicStudies
5PUBLICATIONS44CITATIONS
SEEPROFILE
DavidLeiser
Ben-GurionUniversityoftheNegev
92PUBLICATIONS931CITATIONS
SEEPROFILE
AllcontentfollowingthispagewasuploadedbyDavidLeiseron25November2016.
Theuserhasrequestedenhancementofthedownloadedfile.Allin-textreferencesunderlinedinbluearelinkedtopublicationsonResearchGate,lettingyouaccessandreadthemimmediately.
Ziv, Leiser and Levine 1
Running head: Social cognition in Schizophrenia
Submitted: Cognitive Neuropsychiatry
Social cognition in schizophrenia: cognitive and affective factors
Ido Ziva*, David Leiserb, Joseph Levinec
a School of Behavioral Sciences, Academic College of Tel Aviv-Yafo, Israel b Dept. of Psychology, Ben-Gurion University, Israel
c Medical school, Ben-Gurion University, Israel; Mental Health Centre, Beer-Sheva, Israel
Keywords: Social cognition, Theory of mind, Irony, Emotion understanding
Ziv, Leiser and Levine 2
Abstract
Introduction. Social cognition refers to how people conceive, perceive and draw
inferences about mental and emotional states of others in the social world. Previous
studies suggest that the concept of social cognition involves several abilities,
including those related to affect and cognition.
The present study analyses the deficits of individuals with schizophrenia in two areas
of social cognition: Theory of Mind and emotion recognition and processing.
Examining the impairment of these abilities in patients with schizophrenia has the
potential to elucidate the neurophysiological regions involved in social cognition and
may also have the potential to aid rehabilitation
Methods. Two experiments were conducted. Both included the same five tasks: first-
and second-level false-belief Theory of Mind tasks, emotion inferencing,
understanding of irony, and matrix reasoning (a WAIS-R subtest). The matrix
reasoning task was administered to evaluate and control for the association of the
other tasks with analytic reasoning skills. Experiment 1 involved factor analysis of the
task performance of 75 healthy participants. Experiment 2 compared 30 patients with
schizophrenia to an equal number of matched controls.
Results. (1) The five tasks were clearly divided into two factors corresponding to the
two areas of social cognition, Theory of Mind and emotion recognition and
processing. (2) Schizophrenics’ performance was impaired on all tasks, particularly
on those loading heavily on the analytic component (matrix reasoning and second-
order ToM). (3) Matrix reasoning, second-level Theory of Mind, and irony were
found to distinguish patients from controls, even when all other tasks that revealed
significant impairment in the patients' performance were taken into account.
Conclusions. The two areas of social cognition examined are related to distinct factors.
The mechanism for answering ToM questions (especially ToM2) depends on analytic
reasoning capabilities, but the difficulties they present to individuals with
schizophrenia is due to other components as well. The impairment in social cognition
in schizophrenia stems from deficiencies in several mechanisms, including the
abilities to think analytically and to process emotion information and cues.
Ziv, Leiser and Levine 3
Acknowledgements
This research was done with the help of the outpatient department of the Mental
Health Hospital in Beer Sheva, Israel. The authors wish to thank the following
research members for their assistance with data collection: Merav Saweri, Eyal Akiva,
and Revital Maroz from Ben-Gurion University; and Nurit ben-Arie-Ayulker and Noa
Berrzin-Cohen from the outpatient department. We are extremely grateful to Philip
Tyson and an anonymous reviewer for their helpful comments.
Ziv, Leiser and Levine 4
The present work addresses the issue of social cognition in schizophrenia.
Social cognition is related to the process of drawing inferences about other people's
beliefs and intentions in the social world (Green et al., 2008; Penn, Sanna, & Robert,
2008). In an extensive analysis of research findings, Green et al. (2008) propose that
the term "social cognition" covers five areas: Theory of Mind (ToM), social
perception, social knowledge, attribution bias, and emotion processing (Green, Olivier,
Crawley, Penn, & Silverstein, 2005; Penn, Addington, & Pinkham, 2006). They
maintain that there is convincing evidence suggesting that social cognition is not a
unitary concept. Understanding the factor structure of social-cognitive task measures
may thus be important to better understand these distinct domains of social cognition,
which will, in turn, inform studies of the distinct underlying neurophysiological
circuits and the development of specific, targeted social-cognitive treatments.
The realisation of the importance of measuring more than one aspect of social
cognition has begun to influence studies on schizophrenia (e.g.,Pinkham & Penn,
2006b; Sergi et al., 2007). However, this phase is in its initial stages and none of the
previous studies have measured the social cognition factor structure. The present work
strengthens this approach while focusing on two areas of social cognition: Theory of
Mind (ToM) and recognition and processing of emotion cues and information
(henceforth: RPE: recognition and processing of emotions).
The body of knowledge that has been gathered on social cognition and
mentalising in schizophrenia does not yet permit a satisfactory understanding of the
underlying mechanisms and components involved (Harrington, Siegert, & McClure,
2005; Sprong, Schothorst, Vos, Hox, & England, 2007). This study will specifically
examine the role of executive dysfunction in social cognition impairment. We will
follow the terminology used by Picket (2008) and others, and refer broadly to the
range of cognitive functions as we discuss Executive Functions (EF). If an executive
deficit is involved in impaired ToM in schizophrenia, it is likely that one of two
specific primary EFs are concerned: (1) the ability to disengage from and inhibit
salient information, such as the current reality of a situation, so that less salient
information (e.g., another person’s beliefs) can be considered; and (2) the ability to
manipulate representations of hypothetical situations in order to reason
consequentially (e.g., inferring another person’s beliefs about the current state of
Ziv, Leiser and Levine 5
affairs). The first EF is typically tested by using the Weigl Test (Weigl, 1941), the
Wisconsin Card Sorting Test (Heaton, 1981; Stroop, 1935), or the Stroop Colour-
Word Test (Stroop, 1935). The second EF is tested by evaluating strategic planning
tasks such as the Tower of London (Shallice, 1982), Key Search, or the Zoo Map
(Wilson, Alderman, Burgess, Emslie, & Evans, 1996). We will concentrate on the
second, that is expected to entertain contrasting relations with ToM and RPE, the
facets of social cognition we will be focusing on.
Schizophrenia, ToM, and EF
ToM is defined as the ability to attribute mental states (including beliefs,
intentions, desires, and goals) to the self and others. It also involves the ability to
understand that behaviour is the result of these mental states (Premack & Woodruff,
1978). Effective ToM abilities are important for normal social functioning because
they facilitate the understanding of people’s behaviour (Baron-Cohen, 1995).
There is converging evidence from many sources suggesting that EF plays a
significant role in ToM tasks performance. The development of ToM and success in
false belief inferences was shown to be based in part on that of EF, allowing for the
contribution of planning, response inhibition and cognitive flexibility to ToM function
(Carlson, Moses, & Breton, 2002; Carlson, Moses, & Claxton, 2004; Hughes, 2002;
Sabbagh, Xu, Carlson, Moses, & Lee, 2006; Wellman, Cross, & Watson, 2001).
Further, results from elderly participants indicate that their decreased ability to
understand others' beliefs and desires is related to a decline in executive skills,
especially inhibition, rather than to an inferior ability to mentalise (German &
Hehman, 2006). The extent of performance impairment in belief and desire reasoning
among both the elderly and younger adults has been related to the degree of
processing demand (McKinnon & Moscovitch, 2007). Similar conclusions were
reached with a student population, using a dual-task paradigm that manipulated EF
(inhibition, updating and switching) to assess their implication in ToM tasks (Bull,
Phillips, & Conway, 2008). For a further and more extensive discussion regarding
ToM and EF, see Ziv and Leiser (submitted).
ToM impairment is observed in schizophrenia. Five studies summarising the
schizophrenia research conducted in the last three decades were recently published.
Ziv, Leiser and Levine 6
Three of the studies provided an overview of social cognition: Brüne (2005b),
Harrington et al. (2005), and Penn et al. (2008). The remaining two were broad meta-
analyses of ToM and schizophrenia conducted by Pickup (2008) and Sprong et al.
(2007). Each of these studies explored the extent of mentalising impairment in
patients with schizophrenia, and all found a robust and serious impairment of ToM
abilities. Sprong et al. (2007) found that, on average, the ToM performance of
participants with schizophrenia was more than one standard deviation below that of
healthy controls. Applying Cohen’s (1988) statistical power analysis typology, they
found that the magnitude of the effect size of patients corresponded to a "large" effect,
and the effect size of mentalising impairments in patients in remission demonstrated a
"medium to large" effect. This finding was not the result of a verbalisation deficiency
(which is also a characteristic of patients suffering from schizophrenia) because tasks
relying on cartoon strips and pointing revealed the same impairment (Leiser &
Bonshtein, 2003; Sarfati, Hardy-Bayle, Brunet, & Widloecher, 1999; Sarfati, Hardy-
Bayle, Besche, & Wildlocher, 1997; Sarfati, Passerieux, & Hardy-Bayle, 2000).
Further, the deficiency in schizophrenia is more severe in individuals with other
psychiatric disorders, such as depressive disorder, unless psychotic features are
present (Bonshtein, Leiser, & Levine, 2006; Penn et al., 2008).
Results relating to specific schizophrenia symptoms have been ambiguous
thus far. Some studies have found connections between ToM impairment and positive
symptoms (Harrington, Langdon, Siegert, & Mc-Clure, 2005; Langdon, Coltheart,
Ward, & Catts, 2002), while others have found associations with negative symptoms
(Bora, Eryavuz, Kayahan, Sungu, & Veznedaroglu, 2006; Langdon, Coltheart, &
Ward, 2006). Several have produced no evidence of any relationship (Brüne, 2005;
Janssen, Krabbendam, Jolles, & Os, 2003). These findings imply that the mentalising
impairment is not just a manifestation of the acute phase of the disorder, but may
instead be a permanent trait. This belief stems from the finding that patients in
remission continue to show impaired abilities (Herold, Tenyi, Lenard, & Trixler, 2002;
Inoue et al., 2006), though the difference between patients in remission and healthy
participants was reduced (Bonshtein et al., 2006). Other studies claim that
performance returns to normal during periods of remission (Concoran, Cahill, & Frith,
1997; Drury, Robinson, & Birchwood, 1998; Pinkham & Penn, 2006a).
Ziv, Leiser and Levine 7
The findings we summarized on the pairwise relations between ToM, EF, and
schizophrenia raise the question of the involvement of EF in the ToM impairment
observed in schizophrenia. In a recent review, Pickup (2008) examined studies either
directly or indirectly addressing the relationship between ToM and EF in
schizophrenia. Overall, Pickup (2008) reported that, relative to controls, patients with
schizophrenia were significantly impaired both on ToM and EF tasks. Further, of the
17 studies reviewed, 14 reported significant correlations between ToM tasks and EF
tasks.
However, having examined the studies closely, Pickup (2008) made some
observations that do not support the summary presented above. First, no correlation
was found when the relationship between EF and ToM abilities was tested with
healthy control participants (as was done in only three studies: Brüne (2005a),
Langdon, Coltheart, Ward, & Catts (2001), and Pinkham & Penn (2006a)). Pickup
therefore suggested that the correlation that was found with the patient population
may be attributable to some other common cause, rather than to an inherent
relationship between EF and ToM. Second, Pickup further pointed out that eight
superior studies (Brüne , 2005a; Harrington, Langdon, Siegert, & Mc-Clure, 2005;
Janssen, Krabbendam, Jolles, & Os, 2003; Langdon, Coltheart, & Ward, 2006;
Langdon et al., 2001; Langdon, Coltheart, Ward, & Catts, 2002; Langdon, Corner,
McLaren, Ward, & Coltheart, 2006; Langdon, Davies, & Coltheart, 2002) that relied
on multivariate statistics revealed that even when EF was controlled for, ToM ability
continued to predict whether an individual had schizophrenia or was a healthy control.
It remains therefore unclear whether impairment in EF is involved in the
deficiency in ToM observed in schizophrenia. There is evidence that impairment to
the inhibitory control component of EF does not adequately account for social-
cognitive deficits in schizophrenia, while less is known of the relations between social
cognition and fluid, analytic reasoning. It also seems reasonable to expect that fluid
reasoning is more involved in tasks such as the False Belief tasks, especially those
relating to second-order false beliefs, than in the more affective component of social
cognition, RPE, to which we now turn our attention.
Ziv, Leiser and Levine 8
Emotion recognition and emotion understanding in schizophrenia
Emotion processing is primarily related to the ability to recognise and use
emotions (Feldman-Barrett & Salovey, 2002; Slater & Lewis, 2002). It includes four
abilities: identifying emotions, facilitating emotions, understanding emotions, and
managing emotions (Mayer, Salovey, Caruso, & Sitarenios, 2001; Salovey & Sluyter,
1997). Of these characteristics, two have been extensively studied in schizophrenia
research: (1) identifying emotions via facial expressions and affective prosody; and
(2) understanding emotions with ironic expressions.
A decade ago, Mandal, Pandey, and Prasad (1998) conducted a general review
of previous studies and found evidence that schizophrenia patients are strongly
impaired in the ability to recognise other people’s emotions based on their facial
expressions, gestures, or voices. This result was repeatedly found in later studies
(Brüne, 2005a; Hooker & Park, 2003). The duration of schizophrenia is closely
related to this impaired ability, and chronic patients suffering from marked negative
symptoms are more impaired than less chronic patients (Brüne, 2005a; Mueser et al.,
1996; Penn, Spaulding, Reed, & Sullivan, 1996).
Inferring the emotions involved in a social situation (like that a boy who was
tripped by his classmate will feel angry) is a more complicated process than merely
identifying facial expressions (Shamay-Tsoory, Tomer, & peretz, 2005), because it
requires a reasoning process.
The same holds for irony. The ironic meaning of a sentence is derived from
the difference between the literal meaning of the sentence and the speaker’s meaning
(Winner, 1988), that must be inferred. For example, someone who was embarrassed
by his friend may state: “you have acted like a gentleman”. The listener must
understand the difference between the literal meaning, "acted like a gentleman", and
the implicit intention, "you have acted badly". As Dennis, Purvis, Barnes, Wilkinson,
and Winner (2001) stress, the speaker intends for the listener to identify and
understand the deliberate falseness of his expression. Irony is typically used in
situations that include negative affect, such as contempt, scorn, or disapproval, and is
often used to convey criticism (Sperber & Wilson, 1986). While understanding of
irony involves an additional process relative to identifying emotions from facial
Ziv, Leiser and Levine 9
expressions, Shamay-Tsoory et al. (2005) found that both abilities are mediated by the
right prefrontal lobe.
The impaired understanding of irony in schizophrenia is well-established
(Langdon & Coltheart, 2004; Langdon, Coltheart et al., 2002; Langdon, Davies, &
Coltheart, 2002; Shamay-Tsoory & Aharon-Peretz, 2007; Shamay-Tsoory, Aharon-
Peretz, & Levkovitz, 2006; Shamay-Tsoory et al., 2007; Shuliang, Yanjie, Chan, &
Jianxin, 2008). The relationship between ToM understanding and irony understanding
has also been studied, though the findings are conflicting. Mo, Su, Chan, and Liu
(2008) found no support for the claim that insensitivity to irony in patients with
schizophrenia was associated with a deficient ToM, whereas Langdon and Coltheart
(2004) claimed that an intact ToM is a prerequisite for the interpretation of irony.
Studies of patients with localised lesions revealed dissociable prefrontal
networks for ToM and irony (Shamay-Tsoory & Aharon-Peretz, 2007; Shamay-
Tsoory, Tibi-Elhanany, & Aharon-Peretz, 2006). Based on these dissociable networks,
Shamay-Tsoory, Aharon-Peretz, and Levkovitz (2006) distinguish between cognitive
ToM, that primarily relates to traditional ToM tasks, and affective ToM, that relates to
RPE. This distinction corresponds to two of the social cognition areas identified by
Green et al. (2008): ToM and emotion processing. Shamay-Tsoory et al. (2005) argue
in favour of the relationship between ToM and irony, claiming that the understanding
of irony requires an integration of both components, (cognitive) ToM and emotion
processing.
The present study
We aimed to address two main objectives. First, we explored the factor
structure of two of the social cognition areas, ToM understanding and emotion
processing, as well as their associations with fluid, analytic reasoning. This analysis is
useful in elucidating the distinction and commonalities between these areas, and their
respective relations with the ability to reason analytically. Second, we studied the
independent contribution of each of the social cognition areas in order to discriminate
between schizophrenia patients and controls. This was intended to shed light on the
on-going debate regarding whether schizophrenia is domain-specific (Brune, 2005b;
Bryson, Bell, & Lysaker, 1997; Harrington, Siegert et al., 2005; Langdon et al., 1997)
Ziv, Leiser and Levine 10
or whether the impairment is fundamentally domain-general (e.g., as in the lack of
‘cognitive coordination’ proposed by Phillips and Silverstein (2003)). The two social
cognitive areas behaving as a single factor would suggest that the impairment in
schizophrenia is domain-general. The domain-specific hypothesis would be supported
by evidence that they function as two distinct factors.
Correspondingly, two experiments were constructed. In the first experiment,
we factor-analysed healthy participants performing a range of cognitive and affective
social cognition tests, and an analytic reasoning task. In keeping with the distinction
between the cognitive and emotional facets of social cognition posited in the literature
("ToM" and "emotion processing" in the list by Green et al. (2008), "cognitive ToM"
and "affective ToM", in the terms of Shamay-Tsoory, Aharon-Peretz, and Levkovitz
(2006)), we expected to find that the tasks would be divided into two factors. In the
second experiment, we compared the performance of schizophrenia patients and a
matching control group on the same cognitive and affective social cognition tests,
while controlling for analytic reasoning. We expected the performance of
schizophrenic patients to be impaired on both the cognitive and the affective social
cognition tasks. We also used logistic regression analyses to determine whether the
impairments in the cognitive and the affective aspects of social cognition dissociated
in the patients. Understanding the factor structure of social-cognitive task measures
may be important to better understand these distinct domains of social
cognition, which may, in turn, inform studies of the distinct underlying
neurophysiological circuits and the development of specific, targeted social-cognitive
treatments.
Experiment 1
Method
Seventy-five healthy participants (40 males, 35 females) with no history of
psychiatric disorders were recruited from the community. Their mean age was 29.86
(SD=10.69), with mean years of education 13.5 (SD=2.12). All of the participants
completed all of the tasks. The order of the tasks was counterbalanced across
participants.
Ziv, Leiser and Levine 11
Task Assessment
ToM Assessment (False Belief Stories)
This task was based on six ToM false belief stories (Frith & Corcoran, 1996)
that test the ability of participants to identify trickery and deal with first- and second-
order false beliefs. In first-order stories, the character has a mistaken belief about
reality. In second-order stories, there is a mistaken belief about the beliefs of another
character. The stories are simple and short. At the end of each story, two questions are
presented to the participants. The first can only be answered if the mental state of the
character is inferred. More specifically, to realize that a given belief is mistaken, the
participants must know the correct belief. The second question serves as a control and
to answer it, only the situation must be understood, while the use of ToM is
unnecessary. The second question ensures that the participant is cooperating,
understands the situation, and remembers the plot. For example, in one of the first-
order stories the subject is told about "Betty that put her chocolate in the drawer and
left the room. In her absence, her brother moved the chocolate to his closet". The
following two questions are: "A. Where will Betty search for her chocolate?" and "B.
Where did her brother put the chocolate?"
The second-order stories include an episode about "Dan who plans to visit
with Ruth an exhibition that should take place in Tel Aviv. While purchasing a
newspaper for their train journey Dan sees an advertisement, announcing that the
exhibition was moved to Haifa. On the way to the tickets office, Ruth sees the same
advertisement." The following two questions are: "A. To which city does Dan think
Ruth buy the tickets." and "B. What is the new location of the exhibition?" An
experimenter read all the questions to each participant and marked the participant’s
answer on the questionnaire sheet. The participant's score was the proportion of
correct answers.
Emotion Inference Questionnaire (EIQ)
For this novel task, participants were asked to infer an emotion related to a
relatively simple social situation presented in a short sentence. The following are
examples of the scenarios presented to participants: “In the course of giving a talk, Gil
Ziv, Leiser and Levine 12
began to stutter and his voice trembled. Did he feel embarrassed?”; “ Your mom’s
garden is blooming like her close friend’s garden. Will your mom be jealous of her
friend?” and “The neighbour's son did not get any presents for his birthday. Will he
be sad?” (see Appendix). In order to successfully complete this task, participants had
to grasp the situation and identify the emotion congruent with the situation. The
questions were forced-choice (yes/no). The questionnaire included 24 sentences
related to seven emotions: three basic emotions (happiness, sadness, and anger), and
four advanced emotions (insult, jealousy, embarrassment, and guilt). Each emotion
was represented by four sentences, two of which required a “yes” answer and two a
“no” answer. The scale yield cronbach's alpha =0.92.
Irony Understanding
This task was devised by Ackerman (1981) and translated into Hebrew by
Lapidot, Most, Pik, and Schneider (1998). The task consists of two versions (ironic
and neutral) of eight short stories. The sixteen stories were presented in randomised
order. The stories all involve some interaction between two characters. At the end of
each interaction, one of the characters makes a comment directed at the other. The
verbal comment was the same in both versions, but the intonation was manipulated. In
the ironic version, the comment was uttered with an ironic intonation, whereas the
neutral utterances were spoken with a neutral intonation. Consequently, the literal
meaning of the speaker’s comment in the ironic version was positive, though the
speaker’s true meaning was negative. In the neutral version, on the other hand, both
the literal meaning and the speaker’s intended meaning were positive. To illustrate, an
ironic version item described Joe, who came to work but sat down to rest instead of
beginning to work. His boss noticed his behaviour and said, “Joe, don’t work too
hard!” The neutral version was the same but the intonation was sincere and serious.
Each story was followed by two questions. The first question assessed the
participant’s understanding of the content by asking, “Did Joe work hard?” The
second question examined whether the participant appreciated the true meaning of the
speaker by asking, “Did the manager believe Joe was working hard?” The participant
received a score for the irony question only when both answers were correct. To
control for memory load, we discarded the question if the participant failed to answer
the content question correctly. Two scores were given to participants for this task: one
Ziv, Leiser and Levine 13
for the proportion of correct answers on understanding the irony, and one for the
proportion of correct answers on the control questions. Participants who made more
than two errors on the neutral version items were excluded and replaced. There was
therefore almost no variance in the scores on the neutral versions, and only those on
the irony versions of the stories will be used.
Matrix Reasoning
The matrix reasoning test, a WAIS-R subtest, is a standard measure of
nonverbal abstract problem solving, inductive reasoning, and spatial reasoning
abilities. The materials consist of 25 cards. On each card, a combination of figures is
presented. The participants’ task is to analyse the relationship between the figures
based on several variables (e.g., colour and spatial orientation), and to select a figure
that best fits the sequence from a set of options given at the bottom of the card. The
cards displayed are increasingly difficult, as answering them requires consideration of
an increasing number of variables, such as colour × size or colour × size × spatial
orientation.
Procedure
Participants were tested individually. An experimenter read the questions out
loud and marked the participant’s answer on a questionnaire sheet for each of the
tasks. Filler questions were interspersed as a control. The participant's score was
based on the proportion of correct answers on each task.
Results
A principal components factor analysis was conducted including all task
expect of the irony control task that yielded a ceiling effect. The number of factors
was not restricted. Two factors were extracted using principal-axes factoring and the
criteria of eigenvalue >1.0; they were optimised using varimax with Kaiser
normalisation rotation. The two factors account for 75.7% of the variance in the data.
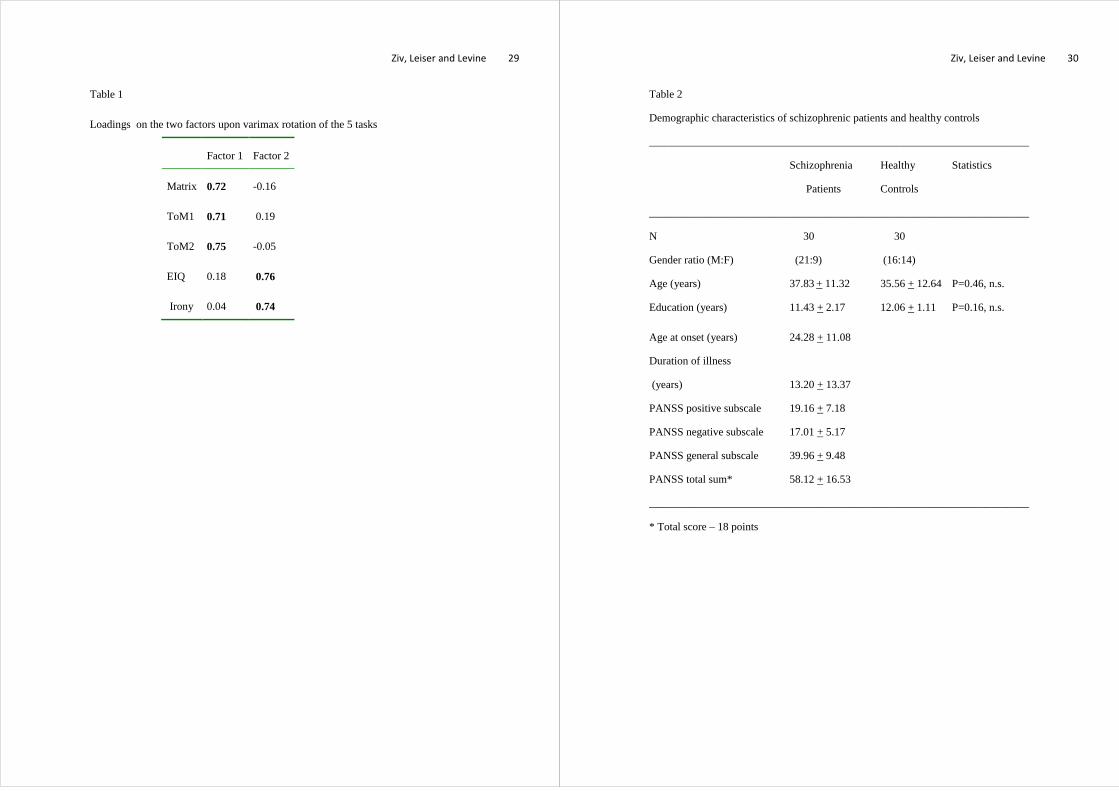
Table 1 presents the loading upon rotation of the five tasks on the two factors. The
variables that loaded on the first factor were matrix reasoning, ToM1, and ToM2.
Those that loaded on the second factor were EIQ and understanding of irony. No
Ziv, Leiser and Levine 14
cross-loadings had weights above 0.20, and the two factors are not correlated (r=-
0.07).
Insert Table 1
Discussion
The results of Experiment 1 reveal a two-factor structure. The first factor
included ToM1, ToM2, and matrix reasoning; the second factor included EIQ and
understanding of irony. Delving into the first factor, we see that both ToM tasks (first-
and second-order) and matrix reasoning share the same underlying features. Matrix
reasoning is a WAIS-R subtest used to measure nonverbal abstract problem solving,
inductive reasoning, and spatial reasoning abilities. Matrix reasoning is strongly
related to advanced analytic abilities. The common pattern of loading of ToM1 and
ToM2 and Matrix reasoning suggests that both ToM tasks are related to a cognitive-
based factor and require analytic skills to successfully tackle the questions. EIQ and
irony understanding load on a second factor. Green et al.’s (2008) typology proposes
that social cognition covers five areas, including ToM and emotion processing. The
current findings suggest that these two areas are related to distinct factors.
These results are in line with the growing body of recent evidence that distinguishes
between cognitive and affective aspects of interpersonal skills, such as the
differentiation between cognitive ToM and affective ToM (Shamay-Tsoory, Aharon-
Peretz et al., 2006; Shamay-Tsoory et al., 2007). Recent neurophysiological findings
also support this distinction. Shamay-Tsoory, Aharon-Peretz, & Perry (2009) found
that subjects with ventromedial prefrontal damage showed impaired cognitive
empathy and ToM2 abilities while still exhibiting intact emotion recognition. Patients
with inferior frontal gyrus lesions, on the other hand, presented deficits in emotion
recognition while maintaining cognitive empathy and ToM2 abilities.
We nex turn to Experiment 2 in order to identify which factors and tasks were
significantly more difficult for schizophrenia patients than for healthy controls.
Ziv, Leiser and Levine 15
Experiment 2
Experiment 2 was designed to provide an analysis of the impairment of
schizophrenia patients regarding the two-factor structure. An additional goal of
Experiment 2 was to create a map of the significant inter-correlations of performance
on the tasks for both patients and controls.
Method
Participants and Design
Thirty patients with schizophrenia (21 males, 9 females), diagnosed according
to the DSM-IV (American Psychiatric Association, 1994), participated in this study.
Participants were treated in a day-care clinic at the Mental Health Centre in Beer
Sheva, Israel. They provided informed consent before participating. Patients’
psychopathology was measured using the Positive and Negative Syndrome Scale
(PANSS; Kay et al., 1989). The researchers rating psychopathology were blind to the
patients’ performance on the tasks used in the study. All of the patients were being
treated with antipsychotic medication. The patients’ mean age at onset of the disorder
was 23.5 years (range: 13–60 years; SD=11 years), with a mean duration of illness of
13.2 years (range: 1–35 years; SD=10.3 years). A similar number of healthy controls
(16 males, 14 females) with no history of psychiatric disorders were recruited from
the community. All participants performed the tasks presented in Experiment 1: ToM
false belief stories (first- and second-order), EIQ, irony understanding, and matrix
reasoning. Materials and procedure were identical to those of Experiment 1. Patients
and controls were matched according to age and education. Demographic
characteristics of the participants, including their psychopathology ratings, are shown
in Table 2.
Insert Table 2
Results
A mixed-design ANOVA Group × Task was used to analyse the data. The
score for each task was treated as a within-participant variable, and the group
(schizophrenia patient versus control) was a between-participants variable. There is
Ziv, Leiser and Levine 16
little purpose in comparing the means across tasks, as the questions were
heterogeneous and not matched for difficulty. Our interest lies in the differential
effect of schizophrenia on the tasks.
Overall, we found the expected significant main effect for schizophrenia,
F(1,57)=25.50; p<0.0001, as participants in the control group performed significantly
better than those in the schizophrenia group. We also observed a significant
interaction effect, F(5,285)=9.835; p<0.0001.
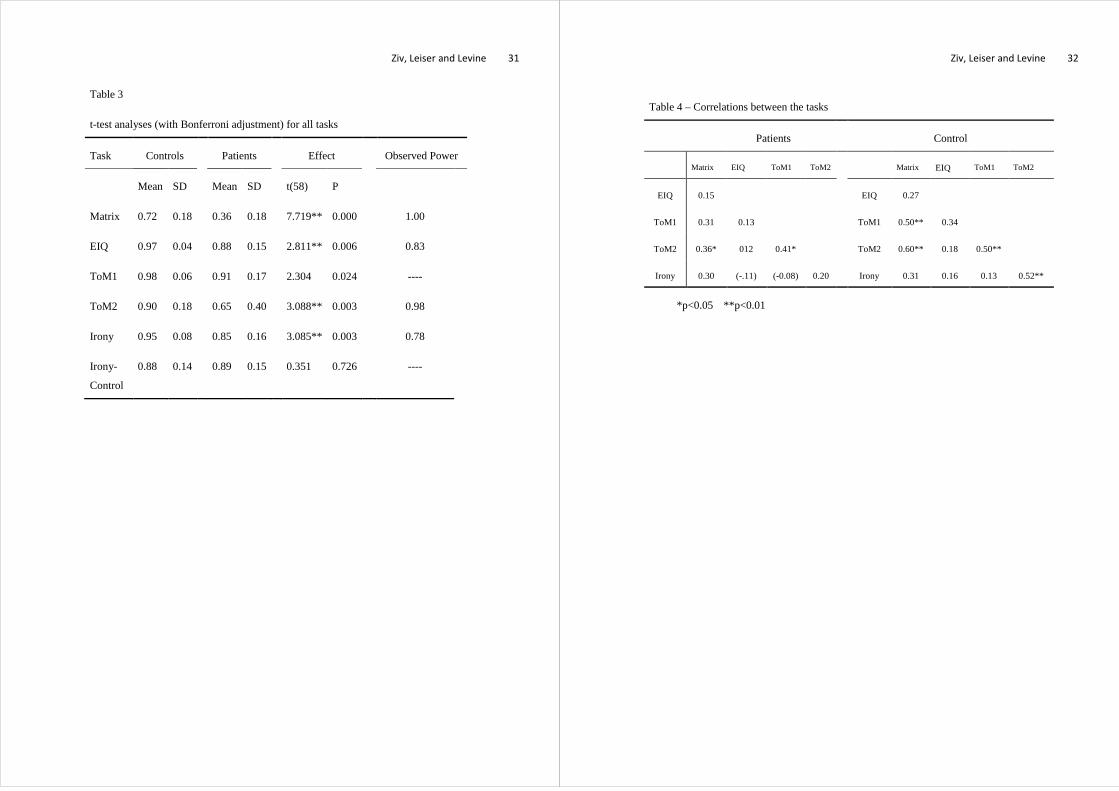
Table 3 presents follow-up t-test analyses (with Bonferroni adjustment of the
alpha to 0.05/6=0.00625) contrasting the performance of schizophrenic patients and
control group for each task. Both groups performed at similar levels on the irony-
control questions, indicating that patients and controls alike could handle a simple
conversation that did not include emotionally complicated phrases or analytic
understanding. The difference in performance between the groups was larger for the
matrix and ToM2 tasks, and slightly less pronounced for the Emotional Inference,
ToM1, and Irony Understanding tasks as reflected by the power analysis values. All
the differences were significant, except for two -- ToM1, and irony-control.
Insert Table 3
We computed the correlations between the main tasks (see Table 4).
Examining the correlation matrix for the patients group, we observe a significant
correlation between ToM1 and ToM2, as well as between matrix reasoning and ToM2.
The first correlation reflects the shared processes common to ToM1 and ToM2; the
second correlation indicates the need for analytic abilities when confronting ToM2
questions. The correlation between matrix reasoning and ToM1 trends in the same
direction (p=0.09), though it does not reach significance.
Insert Table 4
Proceeding to the right side and the data for the control group, the correlations
between the matrix task and ToM2 and between ToM1 and ToM2 are more marked.
In addition, the correlation between the matrix task and ToM1 is now significant.
Lastly, a correlation between ToM2 and the irony understanding task emerges. The
control group reflects the cognitive mechanisms required for the tasks, and a
Ziv, Leiser and Levine 17
comparison of the two tables may provide information regarding the deteriorated
mechanism in the patient group. Table 5 presents the correlations between the PANSS
evaluation dimensions and the tasks. Significant relationships were only found when
the negative psychological symptoms assessed by the PANSS were correlated with
the matrix, ToM2, and irony tasks (all these correlations are negative).
Insert Table 5
We used logistic regression to identify the task performances that discriminate
between patients and controls. The predictor variables were the five tasks (matrix
reasoning, ToM1, ToM2, EIQ and irony). Three of them – matrix, ToM2, and irony --
were found to distinguish patients from controls, even when all other tasks that
showed significant impairment in the patients' performance were taken into account.
The log L-R (likelihood-reduction) χ2 statistic -- that tests the significance of the
decrease in predictive power if a variable is removed from the full model-- is
significant for all three tasks (matrix: χ2 =43.8, p=0.003; ToM2: χ2 =10.646, p=0.01;
irony: χ2 =20.486, p=0.008).
General Discussion
Analysing the performance of healthy subjects on five tasks, Experiment 1
revealed that the tasks (first- and second-order ToM, EIQ and irony understanding,
and matrix reasoning) divide into two distinct factors that correspond to the two areas
of the social cognition ability, Theory of Mind (ToM), and EIQ. This pattern of
factors is also in accord with the findings of Shamay-Tsoory et al. (2007) and
Shamay-Tsoory & Tibi-Elhanany et al. (2006) regarding the distinction between
cognitive ToM and affective ToM, that are supported by recent neurophysiological
brain studies (Shamay-Tsoory et al., 2009).
Experiment 2 compared schizophrenia patients and healthy controls. The
patients and the control groups answered the irony-control questions with equal
accuracy. This shows that individuals with schizophrenia have adequate abilities
when it comes to comprehending a simple conversation that rarely demands advanced
cognitive or affective abilities. Experiment 2 confirmed the serious performance
impairment of patients with schizophrenia on all five tasks: ToM1, ToM2, EIQ, irony,
Ziv, Leiser and Levine 18
and matrix (and not on the irony-control task). These results are congruent with those
of Pickup (2008) and in line with previous studies showing that patients with
schizophrenia demonstrate impaired performance on all tasks involving EF and RPE
(emotion recognition, and the ability to appreciate the mental states of others) (Brüne,
2005b; Evans, Chua, McKenna, & Wilson, 1997; Langdon & Coltheart, 2004;
Langdon, Coltheart et al., 2002; Langdon, Davies et al., 2002; Pickup & Frith, 2001;
Poole, Tobias, & Vinogradov, 2000; Shamay-Tsoory & Aharon-Peretz, 2007;
Shamay-Tsoory, Aharon-Peretz et al., 2006; Shamay-Tsoory et al., 2007; Shuliang et
al., 2008). However, while Brüne (2005a), Langdon, Coltheart, Ward, and Catts
(2001), and Pinkham and Penn (2006a) failed to find significant correlations between
the ability to reason analytically and their ToM measures, we did find a significant
and positive correlation between matrix reasoning scores and performance on ToM2.
Our findings regarding the marked negative correlation between the negative
psychological symptoms assessed by the PANSS and performance on the tasks are in
line with the findings of Shamay-Tsoory et al. (2007), who also found significant
negative correlations between ToM measures and negative symptom ratings, but
differ from those Brüne (2005a), who failed to find significant correlations of this
type.
Negative symptoms signify a lack of certain abilities in schizophrenia patients
when compared to healthy individuals. The significant correlations between negative
symptoms and ToM2, irony understanding and matrix reasoning indicate a deficiency
in the mechanisms underlying these abilities.
What ability is involved? The extent of the difference between the patients
group and the control group was the largest for the matrix and ToM2 tasks.
Performance on these two tasks is correlated, in both the patients and control groups.
This fits well with the finding in Experiment 1 that ToM1 and ToM2 relate to the
same factor as matrix reasoning, while irony and emotion inference relate to another.
A natural interpretation is that the false-belief tasks require significant analytical
competence, and that ToM ability is related to the quality of fluid mental abilities.
The ToM2 and irony tasks were found to be correlated within the control
group. Mo et al. (2008) did not find this correlation, though they did produce related
findings, namely, that metaphor understanding was correlated with ToM2. For their
Ziv, Leiser and Levine 19
part, Langdon and collaborators (Langdon, Coltheart et al. (2002), Langdon, Davies et
al. (2002), and Langdon and Coltheart (2004)) found a significant correlation between
metaphor comprehension and ToM1. Mo et al. (2008) proposed that the relationship
between metaphor and ToM may be explained using the Relevance Theory of Sperber
and Wilson (1986, 1998). This theory holds that non-literal speech comprehension is
related to the understanding of mental states, such as those assessed by the false-belief
tasks. The significant correlation we found between ToM2 and irony supports this
notion to some extent, as irony is also a form of non-literal speech understanding.
The results of Experiment 2 provide important complements to the two-factor
structure found in Experiment 1 with healthy participants. The logistic regression
showed that matrix reasoning, ToM2, and irony all made significant independent
contributions to discrimination between patients and controls, even when all other
tasks that reveal significant impairment in the patients' performance are taken into
account. This suggests that: (1) the understanding of irony (as assessed in this study)
and ToM dissociate in schizophrenic patients; and (2) poor analytic reasoning
(indexed by matrix reasoning) does not completely explain the patients' difficulty with
second-order ToM and the understanding of irony.
Taken together, these results suggest several conclusions for social cognition
with respect to schizophrenia. First, the two areas of social cognition ability, Theory
of Mind and RPE, are related to distinct factors. This finding corresponds to Green et
al.’s (2008) typology. Second, while the mechanism needed for answering ToM
questions (especially of second-order) is significantly related to fluid intelligence, the
ability to reason analytically does not entirely account for the difficulties manifested
by schizophrenic patients on this task. The impaired social cognition skills of
individuals with schizophrenia appear to be due to the combination of several
deteriorated mechanisms, including both the ability to think analytically and the
ability to process emotional cues and information. Individuals with schizophrenia
suffer from several specific cognitive impairments that not only relate to the semantic
network or the inhibitory control ability, as proposed by Brüne (2005a), but also to the
interaction of these abilities with the cognitive impairment of analytical reasoning and
emotion processing. Accordingly, when discussing social cognition in relation to
schizophrenia, it is critical to stress both the emotional components and the
Ziv, Leiser and Levine 20
cognitive/analytic components. This is extremely important, because it implies that
patients could benefit from the development of specific clinical rehabilitation
programs that would address these varied and distinct impairments. Moreover, the
current results also support the study of separate neurophysiological circuits, as has
been done extensively by Shamay-Tsoory and colleagues (2007; 2006; 2009; 2006).
In closing, we wish to stress the importance and the necessity of future studies
that will validate and extend the results presented in this paper. We hypothesised that
the social cognition areas of ToM understanding and emotion processing were divided
into a two-factor structure. The results clearly support this claim. However, this
conclusion should be taken with caution, as an experimenter read all the tasks to the
participants and may have provided them with prosodic cues. This might account for
the irony task and the emotion inference tasks loading on the same factor. Future
studies should clarify the role of prosodic cues by using both written and oral stories
in modified irony tasks. More importantly, there is a need for broader studies that will
clarify whether all the areas of social cognition identified by Green et al (2005)
correspond to distinct factors when indexed by a range of suitable tasks, and how this
factor structure is modulated by schizophrenia.
Ziv, Leiser and Levine 21
References
Ackerman, B. (1981). Young children’s understanding of a false utterance. Developmental Psychology, 31, 472-480.
Baron-Cohen, S. (1995). Mindblindness: An Essay on Autism and Theory of Mind. Cambridge: MA: MIT Press.
Bonshtein, U., Leiser, D., & Levine, J. (2006). Naive Theory Impairment in Schizophrenia: Is It Domain-Specific? . Journal of Nervous & Mental Disease, 194(10), 753-759.
Bora, E., Eryavuz, A., Kayahan, B., Sungu, G., & Veznedaroglu, B. (2006). Social functioning, theory of mind and neurocognition in outpatients with schizophrenia; mental state decoding may be a better predictor of social functioning than mental state reasoning. Psychiatry Research (145), 95-103
Brüne, M. (2005a). Emotion recognition, 'theory of mind,' and social behavior in schizophrenia. Psychiatry Research, 133(2-3), 135 - 147.
Brüne, M. (2005b). 'Theory of Mind' in Schizophrenia: A Review of the Literature. Schizophrenia Bulletin, 31(1), 21-42.
Bryson, G., Bell, M., & Lysaker, P. (1997). Affect recognition in schizophrenia: a function of global impairment or a specific cognitive deficit. Psychiatry Research 71, 105-113.
Bull, R., Phillips, L., & Conway, C. (2008). The role of control functions in mentalizing: Dual-task studies of Theory of Mind and executive function. Cognition, 107(2), 663-672.
Carlson, S. M., Moses, L. J., & Breton, C. (2002). How specific is the relation between executive function and theory of mind ? Contributions of inhibitory control and working memory. Infant and Child Development, 11(2), 73-92.
Carlson, S. M., Moses, L. J., & Claxton, L. J. (2004). Individual differences in executive functioning and theory of mind: An investigation of inhibitory control and planning ability. Journal of Experimental Child Psychology, 87(4), 299-319.
Cohen, J. (1988). Statistical Power Analysis for the Behavioral Sciences (2 ed.). Hillsdale, New Jersy: Lawrence Erlbaum Association.
Concoran, R., Cahill, C., & Frith, C. D. (1997). The appriciation of visual jokes in people with schizophrenia: A study of "mentalizing" ability. Schizophrenia Research, 24, 319-327.
Dennis, M., Purvis, K., Barnes, M. A., Wilkinson, M., & Winner, E. (2001). Understanding of literal truth, ironic criticism, and deceptive praise following childhood head injury. Brain and Language, 78(1-16).
Ziv, Leiser and Levine 22
Drury, V. M., Robinson, E. J., & Birchwood, M. (1998). Theory of mind skills during an acute episode of psychosis and following recovery. Psychological Medicine, 28, 1101-1112.
Evans, J. J., Chua, S. E., McKenna, P. J., & Wilson, B. A. (1997). Assessment of the dysexecutive syndrome in schizophrenia. Psychological Medicine, 27, 635-646.
Feldman-Barrett, L., & Salovey, P. (2002). The Wisdom in Feeling: Psychological Processes in Emotional Intelligence. New York: NY: Guilford Press.
German, T., & Hehman, J. (2006). Representational and executive selection resources in ‘theory of mind’: Evidence from compromised belief-desire reasoning in old age. Cognition 101(1), 129-152.
Green, M. F., Olivier, B., Crawley, J. N., Penn, D. L., & Silverstein, S. (2005). Social cognition in schizophrenia: recommendations from the MATRICS New Approaches Conference. Schizophrenia Bulletin, 31, 882-887.
Green, M. F., Penn, D. L., Bentall, R., Carpenter, W. T., Gaebel, W., Gur, R. C., et al. (2008). Social Cognition in Schizophrenia: An NIMH Workshop on Definitions, Assessment, and Research Opportunities. Schizophrenia Bulletin, 34(6), 1211-1220.
Harrington, L., Langdon, R., Siegert, R. J., & Mc-Clure, J. (2005). Schizophrenia, theory of mind and persecutory delusions. Cognitive Neuropsychiatry, 2005(10), 87-104.
Harrington, L., Siegert, R. J., & McClure, J. (2005). Theory of mind in schizophrenia: a critical review. Cognitive Neuropsychiatry, 10, 249-286.
Heaton, R. K. (1981). A Manual for the Wisconsin Card Sorting Test. Odessa: Psychological Assessment Resources.
Herold, R., Tenyi, T., Lenard, K., & Trixler, M. (2002). Theory of mind deficit in people with schizophrenia during remission. Psychological Medicine, 32, 1125-1129.
Hooker, C., & Park, S. (2003). Emotion processing and its relationship to social functioning in schizophrenia patients. Psychiatry Research, 112, 41-50.
Hughes, C. (2002). Executive functions and development: Emerging themes. Child Developemt, 11, 201-209.
Inoue, Y., Yamada, K., Hirano, M., Shinohara, M., Tamaoki, T., Iguchi, H., et al. (2006). Impairment of theory of mind in patients in remission following first episode of schizophrenia. Journal of European Archives of Psychiatry and Clinical Neuroscience, 256, 326-328.
Ziv, Leiser and Levine 23
Janssen, I., Krabbendam, L., Jolles, J., & Os, J. v. (2003). Alterations in theory of mind in patients with schizophrenia and non-psychotic relatives. Acta Psychiatrica Scandinavica, 108, 110-117.
Langdon, R., & Coltheart, M. (2004). Recognition of metaphor and irony in young adults: the impact of schizotypal personality traits. Psychiatry Research, 125, 9-20.
Langdon, R., Coltheart, M., & Ward, P. B. (2006). Empathetic perspective-taking is impaired in schizophrenia: evidence from a study of emotion attribution and theory of Mind. Cognitive Neuropsychiatry, 11, 133-155.
Langdon, R., Coltheart, M., Ward, P. B., & Catts, S. V. (2001). Mentalising, executive planning and disengagement in schizophrenia. Cognitive Neuropsychiatry, 6(2), 81-108.
Langdon, R., Coltheart, M., Ward, P. B., & Catts, S. V. (2002). Disturbed communication in schizophrenia: the role of poor pragmatics and poor mind-reading. Psychological Medicine, 32(1), 1273-1284.
Langdon, R., Davies, M., & Coltheart, M. (2002). Understanding minds and understanding communicated meanings in schizophrenia. Mind and Language, 17, 68-104.
Langdon, R., Michie, P. T., Ward, P. B., McConaghy, N., Catts, S., & Coltheart, M. (1997). Defective self and/or other mentalising in schizophrenia: a cognitive neuropsychological approach. Cognitive Neuropsychiatry 2, 167-193.
Lapidot, M., Most, T., Pik, E., & Schneider, R. (1998, August). Effects of prosodic information and context on perception of irony by children and adults. Paper presented at the 24th World Congress of the International Association of Logopedics and Phoniatrics, Amsterdam, the Netherlands.
Leiser, D., & Bonshtein, U. (2003). Theory of Mind in Schizophrenia: Damaged Module or Deficit in Cognitive Coordination? A Commentary on: Phillips and Silverstein: Convergence of biological and psychological perspectives on cognitive coordination in schizophrenia. Behavioral and Brain Science, 26(1), 95-96.
Mandal, M. K., Pandey, R., & Prasad, A. B. (1998). Facial expressions of emotions and schizophrenia: a review. Schizophrenia Bulletin, 24, 399-412.
Mayer, J. D., Salovey, P., Caruso, D. R., & Sitarenios, G. (2001). Emotional intelligence as a standard intelligence. Emotion(1), 232-242.
McKinnon, M. C., & Moscovitch, M. (2007). Domain-general contributions to social reasoning: Theory of mind and deontic reasoning re-explored. Cognition 102(2), 179-218.
Ziv, Leiser and Levine 24
Mo, S., Su, Y., Chan, R. C. K., & Liu, J. (2008). Comprehension of metaphor and irony in schizophrenia duringremission: The role of theory of mind and IQ. Psychiatry Research 157, 21-29.
Mueser, K. T., Doonan, R., Penn, D. L., Blanchard, J. J., Bellack, A. S., Nishith, P., et al. (1996). Emotion recognition and social competence in chronic schizophrenia. Journal of Abnormal Psychology, 105, 271- 275.
Penn, D. L., Addington, J., & Pinkham, A. (2006). Social cognitive impairments. In S. T. Lieberman JA, Perkins DO, eds. (Ed.), American Psychiatric Association Textbook of Schizophrenia (pp. 261-274).
Penn, D. L., Sanna, L. J., & Robert, D. L. (2008). Social Cognition in Schizophrenia: An Overview. Schizophrenia Bulletin, 34(3), 408-411.
Penn, D. L., Spaulding, W., Reed, D., & Sullivan, M. (1996). relationship of social cognition to ward behavior in chronic schizophrenia. Schizophrenia Research 20, 114-132.
Phillips, W. A., & Silverstein, S. M. (2003). Convergence of biological and psychological perspectives on cognitive coordination in schizophrenia. behavioral and Brain Sciences, 26, 63-135.
Pickup, G. J. (2008). Relationship between Theory of Mind and Executive Function in Schizophrenia:A Systematic Review. Psychopathology, 41, 206-213.
Pickup, G. J., & Frith, C. D. (2001). Schizotypy, theory of mind and weak central coherence. Schizophrenia Research, 49( ), 118.
Pinkham, A. E., & Penn, D. L. (2006a). Neurocognitive and social cognitive predictors of interpersonal skill in schizophrenia. Psychiatry Research 143, 167-178.
Pinkham, A. E., & Penn, D. L. (2006b). Neurocognitive and social cognitive
predictors of interpersonal skill in schizophrenia. Psychiatry Research, 143, 167-178.
Poole, J. H., Tobias, F. C., & Vinogradov, S. (2000). The functional relevance of affect recognition errors in schizophrenia. Journal of the International Neuropsychological Society 6, 649- 658.
Premack, D., & Woodruff, G. (1978). Does the chimpanzee have a theory of mind? Behavioral and Brain Sciences, 4, 515-526.
Sabbagh, M. A., Xu, F., Carlson, S. M., Moses, L. J., & Lee, K. (2006). The Development of Executive Functioning and Theory of Mind. A Comparison of Chinese and U.S. Preschoolers. Psychological Science, 17, 74-81.
Salovey, P., & Sluyter, D. J. (1997). Emotional Development and Emotional Intelligence. New York: NY: Basic Books.
Ziv, Leiser and Levine 25
Sarfati, Y., Hardy-Bayle, M., Brunet, E., & Widloecher, D. (1999). Investigating theory of mind in schizophrenia: Influence of verbalization in disorganized and non-disorganized patients. Schizophrenia Research, 37(2), 183-190.
Sarfati, Y., Hardy-Bayle, M. C., Besche, C., & Wildlocher, D. (1997). Attribution of intentions to others in people with schizophrenia: A non verbal exploration with comic-strips. Schizophrenia Research, 25, 199-209.
Sarfati, Y., Passerieux, C., & Hardy-Bayle, M. (2000). Can verbalization remedy the theory of mind deficit in schizophrenia? . Psychopathology, 33, 246-251.
Sergi, M., Rassovsky, Y., Widmark, C., Reist, C., Erhart, S., Braff, D., et al. (2007). Social cognition in schizophrenia: relationships with neurocognition and negative symptoms. Schizophrenia Research, 90(1-3), 316-324.
Shallice, T. (1982). Specific impairments of planning. Philosophical transactions of the Royal Society of London, 198, 199-209.
Shamay-Tsoory, S. G., & Aharon-Peretz, J. (2007). Dissociable prefrontal networks for cognitive and affective theory of mind: A lesion study. Neuropsychologia, 45(13), 3054-3067.
Shamay-Tsoory, S. G., Aharon-Peretz, J., & Levkovitz, Y. (2006). The Neuroanatomial Basis of Affective Mentalizing in Schizophrenia: Comparison of Patients with Schizophrenia and Patients with Localized Prefrontal Lesions. Schizophrenia Research, 90(1-3), 274-283.
Shamay-Tsoory, S. G., Aharon-Peretz, J., & Perry, D. (2009). Two systems for empathy: a double dissociation between emotional and cognitive empathy in inferior frontal gyrus versus ventromedial prefrontal lesions. Brain, 132, 617-627
Shamay-Tsoory, S. G., Shur, S., Barcai-Goodman, L., Medlovich, S., Harari, H., & Levkovitz, Y. (2007). Dissociation of cognitive from affective components of theory of mind in schizophrenia. Psychiatry Research 149(1-3), 11-23.
Shamay-Tsoory, S. G., Tibi-Elhanany, Y., & Aharon-Peretz, J. (2006). The ventromedial prefrontal cortex is involved in understanding affective but not cognitive theory of mind stories. Journal of Social Neuroscience, 1(3-4), 149-166.
Shamay-Tsoory, S. G., Tomer, R., & peretz, J. A. (2005). The Neuroanatomical basis of understanding sarcasm and it's relationship to social cognition. Neuropsychology, 19(3), 288-300.
Shuliang, M., Yanjie, S., Chan, C. K. R., & Jianxin, L. D. (2008). Comprehension of metaphor and irony in schizophrenia during remission: The role of theory of mind and IQ. Psychiatry Research 157, 21-29.
Slater, A., & Lewis, M. (2002). Introduction to Infant Development. Oxford: Oxford University Press.
Ziv, Leiser and Levine 26
Sperber, D., & Wilson, D. (1986). Relevance: Communication and cognition. Oxford, England: Basil Blackwell.
Sperber, D., & Wilson, D. (1998). The mapping between the mental and the public lexicon. In P. Carruthers & J. Boucher (Eds.), Language and Thought: Interdisciplinary Themes (pp. 184-200). Cambridge: Cambridge University Press.
Sprong, M., Schothorst, P., Vos, E., Hox, J., & England, H. V. (2007). Theory of Mind in Schizophrenia Meta-Analysis British Journal of Psychiatry 191, 5-13.
Stroop, J. R. (1935). Studies of interference in serial verbal reactions. Journal of Experimental Psychology 18, 643-662.
Weigl, E. (1941). On the psychology of so-called processes of abstraction. The Journal of Abnormal and Social Psychology 36(1), 3-33.
Wellman, H. M., Cross, D., & Watson, J. (2001). Meta-Analysis of theory of mind development: The truth about false belief. Child Development, 72(2), 655-624.
Wilson, B. A., Alderman, N., Burgess, P., Emslie, H., & Evans, J. J. (1996). Behavioural Assessment of the Dysexecutive Syndrome (BADS). Edmunds: Thames Valley Test Company.
Winner, E. (1988). The point of words: Children’s understandin of metaphor and irony. Cambridge, MA: Harvard University Press.
Ziv, I., & Leiser, D. (submitted). The use of domain-general resources in naive biology, psychology, and economics inference.
Ziv, Leiser and Levine 27
Appendix – Emotion Inferencing Questionnaire
During the break ToM ran in the garden. One of his classmates tripped him and he fell.
Will he be angry with the other boy?
Tomorrow Lisa will have a long day at school. Her mother will prepare her a
sandwich for lunch. Will Lisa be angry with her mother?
Dan asked his friend to help him study for a test. Instead, the friend went to sleep.
Will Dan be angry with his friend?
On the way to the local grocery, Rina does some shopping for her neighbours as well.
Will they be angry with her?
Your friend wrote a love letter for a girl and was rejected by her. Will he feel hurt?
The neighbour's son cleaned the garden and received from his mother his favourite
chocolate. Will he feel hurt?
Nir bought a birthday present for his friend with the money he saved. However, the
friend tossed it to the garbage in front of his eyes. Will Nir be hurt?
One of your classmates read his homework answer. Your teacher is enthusiastic about
the answer and praises your friend. Will the friend feel insulted?
The neighbour's son did not get any present for his birthday. Will he be sad?
Rinat won the first prize in the lottery. Will she be sad?
Mica was the only boy that was not invited to the birthday party. Will Mica be sad?
Ben achieved the best grade in the math test in his class. Will he be sad?
Your friend was chosen as "student of the month" and won a prize. Will he be happy?
The bicycle of the neighbour's daughter was stolen yesterday. Will she be happy?
You friend returned home hungry after a long and intensive basketball training. His
older brother made him supper. Will he be happy?
Ziv, Leiser and Levine 28
Ruth broke the flower vase in the living room. Her mother shouted at her. Will she be
happy?
Your friend studied for the test with her twin sister and received a lower grade than
her. Will she be jealous of her sister?
Solomon bought a brand-new car like his cousin. Will he be jealous of him?
Your younger brother asked your parents to buy him a toy he saw at his friend’s house.
However, your parents refused. Will your younger brother be jealous of his friend?
Your mom’s garden is blooming like her close friend’s garden. Will your mom be
jealous of her friend?
While ToM gave a talk, he started to stutter and his voice trembled. Will he feel
embarrassed?
Sera went with her parents to have dinner in a restaurant. When they entered the
restaurant, they found out that their table was not prepared even though they made
reservations in advance. The parents got angry and shouted at the manager and a fuss
broke out. Will Sera be embarrassed?
Miriam was angry with her friend. When she met her, she yelled at her and offended
her more than she previously intended. Will she feel guilty?
During a basketball game, the players from the rival team pushed Danni the entire
time. After the break, Danny decided to push them back. Will he feel guilty?
Ziv, Leiser and Levine 29
Table 1
Loadings on the two factors upon varimax rotation of the 5 tasks
Factor 1 Factor 2
Matrix 0.72 -0.16
ToM1 0.71 0.19
ToM2 0.75 -0.05
EIQ 0.18 0.76
Irony 0.04 0.74
Ziv, Leiser and Levine 30
Table 2
Demographic characteristics of schizophrenic patients and healthy controls
_____________________________________________________________________
Schizophrenia Healthy Statistics
Patients Controls
_____________________________________________________________________
N 30 30
Gender ratio (M:F) (21:9) (16:14)
Age (years) 37.83 + 11.32 35.56 + 12.64 P=0.46, n.s.
Education (years) 11.43 + 2.17 12.06 + 1.11 P=0.16, n.s.
Age at onset (years) 24.28 + 11.08
Duration of illness
(years) 13.20 + 13.37
PANSS positive subscale 19.16 + 7.18
PANSS negative subscale 17.01 + 5.17
PANSS general subscale 39.96 + 9.48
PANSS total sum* 58.12 + 16.53
_____________________________________________________________________
* Total score – 18 points
Ziv, Leiser and Levine 31
Table 3
t-test analyses (with Bonferroni adjustment) for all tasks
Task Controls Patients Effect Observed Power
Mean SD Mean SD t(58) P
Matrix 0.72 0.18 0.36 0.18 7.719** 0.000 1.00
EIQ 0.97 0.04 0.88 0.15 2.811** 0.006 0.83
ToM1 0.98 0.06 0.91 0.17 2.304 0.024 ----
ToM2 0.90 0.18 0.65 0.40 3.088** 0.003 0.98
Irony 0.95 0.08 0.85 0.16 3.085** 0.003 0.78
Irony-
Control
0.88 0.14 0.89 0.15 0.351 0.726 ----
Ziv, Leiser and Levine 32
Table 4 – Correlations between the tasks
Patients Control
Matrix EIQ ToM1 ToM2 Matrix EIQ ToM1 ToM2
EIQ 0.15 EIQ 0.27
ToM1 0.31 0.13 ToM1 0.50** 0.34
ToM2 0.36* 012 0.41* ToM2 0.60** 0.18 0.50**
Irony 0.30 (-.11) (-0.08) 0.20 Irony 0.31 0.16 0.13 0.52**
*p<0.05 **p<0.01
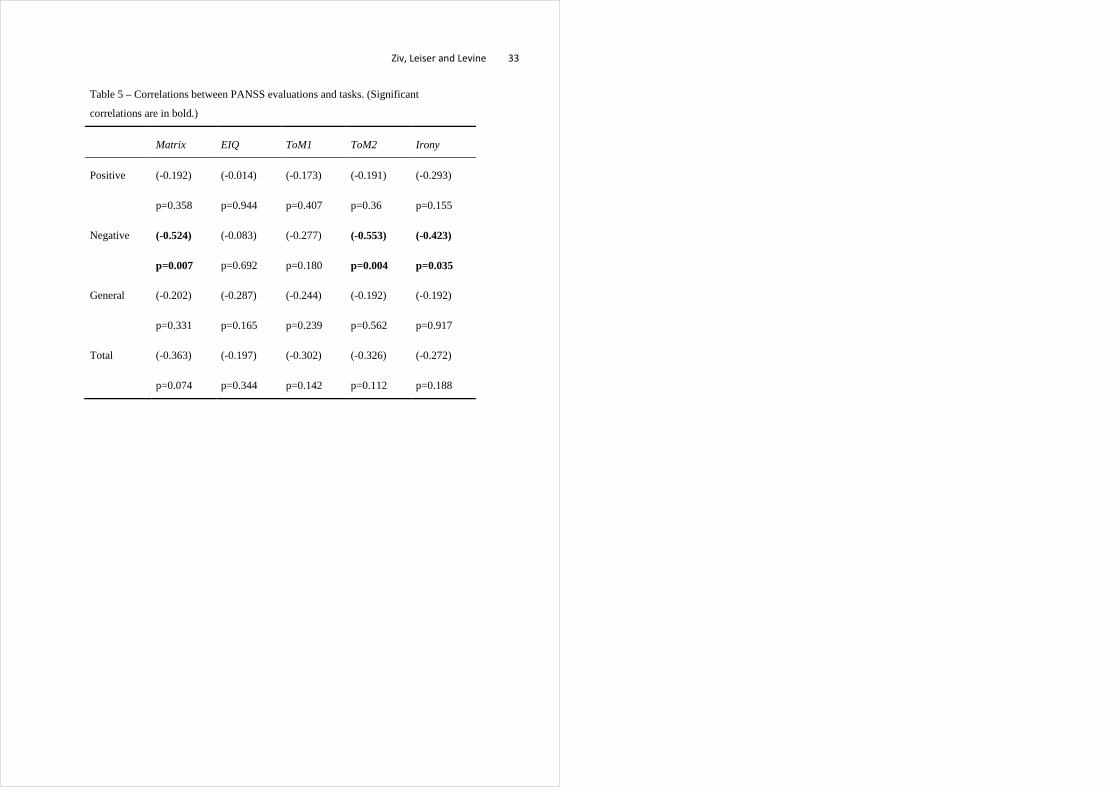
Ziv, Leiser and Levine 33
Table 5 – Correlations between PANSS evaluations and tasks. (Significant
correlations are in bold.)
Matrix EIQ ToM1 ToM2 Irony
Positive (-0.192)
p=0.358
(-0.014)
p=0.944
(-0.173)
p=0.407
(-0.191)
p=0.36
(-0.293)
p=0.155
Negative (-0.524)
p=0.007
(-0.083)
p=0.692
(-0.277)
p=0.180
(-0.553)
p=0.004
(-0.423)
p=0.035
General (-0.202)
p=0.331
(-0.287)
p=0.165
(-0.244)
p=0.239
(-0.192)
p=0.562
(-0.192)
p=0.917
Total (-0.363)
p=0.074
(-0.197)
p=0.344
(-0.302)
p=0.142
(-0.326)
p=0.112
(-0.272)
p=0.188
Related Documents