Non-carious cervical lesions: influence of morphology and load type on biomechanical behaviour of maxillary incisors PV Soares,* PCF Santos-Filho,† CJ Soares,† VLG Faria,* MF Naves,* JA Michael,‡ JA Kaidonis,‡ S Ranjitkar,‡ GC Townsend‡ *Nucleus of Extension, Research and Teaching of NCCL, Operative Dentistry and Dental Materials Department, School of Dentistry, Federal University of Uberlandia, Brazil. †Operative Dentistry and Dental Materials Department, School of Dentistry, Federal University of Uberlandia, Brazil. ‡School of Dentistry, The University of Adelaide, South Australia. ABSTRACT Background: The aim of this study was to measure the effect of simulating two different loads on maxillary incisors dis- playing eight morphological types of non-carious cervical lesions, unrestored and restored with an adhesive restoration, by quantifying the stress distributions generated using finite element analysis. Methods: Virtual models of maxillary incisors were generated using the CAD software (RhinoCeros). After composing virtual dental and supporting structures with and without non-carious cervical lesions, each model was meshed using a control mesh device (ANSYS Finite Element Analysis Software). All of the virtual models were subjected to two load types, oblique load and vertical load, to simulate occlusal forces of 100 N each. Comparisons were made between simu- lated teeth with non-carious cervical lesions, with and without composite resin restorations, and a simulated sound tooth. Data summarizing the stress distributions were obtained in MPa using von Mises criteria. Results: Oblique loading on simulated non-carious cervical lesions resulted in greater stress concentration compared with vertical loading, and non-carious cervical lesions with acute angles displayed higher stress concentrations at the depth of the lesion. Restoring the lesions with an adhesive restoration, such as composite resin, appeared to overcome this stress concentration. Conclusions: Restoring NCCLs with adhesive restorative materials, such as a nanohybrid composite resin, appears to recover the biomechanical behaviour similar to sound teeth. Keywords: Biomechanical behaviour, composite resin, finite element analysis, non-carious cervical lesion, teeth. Abbreviations and acronyms: FEA = finite element analysis; GIC = glass ionomer cement; NCCLs = non-carious cervical lesions. (Accepted for publication 7 November 2012.) INTRODUCTION Non-carious cervical lesions (NCCLs) are formed by loss of tooth structure in the cervical third of the crown and root surface that is unrelated to dental car- ies. 1,2 It is generally accepted that the lesions are not generated by a single factor but result from a combi- nation of factors. 1,3,4 Among the factors proposed to be related to the formation and progression of NCCLs are: biocorrosion (chemical, biochemical and electro- chemical degradation) caused by intrinsic and extrin- sic acids; friction (wear) caused by traumatic brushing; and possibly stresses (abfraction) caused by parafunction, traumatic occlusion and load applica- tion. 4 It is most probable that not all of these factors are involved in any particular case, but more likely only a small number. So far, erosion and toothbrush abrasion have been implicated definitely. 5 In addition, reports of NCCLs developing on teeth that did not have an opposing tooth for many decades add to the controversy surrounding the aetiology of these lesions. 6 NCCLs are usually diagnosed based on a detailed history, visual inspection and tactile examina- tion. 1 It has been proposed that a major factor con- tributing to the progression of NCCLs is a high level of loading associated with occlusal forces. 7,8 Two types of loading on maxillary incisors have been described, 8 one being an oblique type (due to oblique or inclined contact with the lingual surface) and the second a vertical load (along the long axis of the tooth, applied via the incisal edge). Several studies have examined the characteristics of NCCLs, such as which teeth show greater involve- ment and the extent of damage, through subjective 306 © 2013 Australian Dental Association Australian Dental Journal 2013; 58: 306–314 doi: 10.1111/adj.12084 Australian Dental Journal The official journal of the Australian Dental Association

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Non-carious cervical lesions: influence of morphology andload type on biomechanical behaviour of maxillary incisors
PV Soares,* PCF Santos-Filho,† CJ Soares,† VLG Faria,* MF Naves,* JA Michael,‡JA Kaidonis,‡ S Ranjitkar,‡ GC Townsend‡
*Nucleus of Extension, Research and Teaching of NCCL, Operative Dentistry and Dental Materials Department, School of Dentistry, FederalUniversity of Uberlandia, Brazil.†Operative Dentistry and Dental Materials Department, School of Dentistry, Federal University of Uberlandia, Brazil.‡School of Dentistry, The University of Adelaide, South Australia.
ABSTRACT
Background: The aim of this study was to measure the effect of simulating two different loads on maxillary incisors dis-playing eight morphological types of non-carious cervical lesions, unrestored and restored with an adhesive restoration,by quantifying the stress distributions generated using finite element analysis.Methods: Virtual models of maxillary incisors were generated using the CAD software (RhinoCeros). After composingvirtual dental and supporting structures with and without non-carious cervical lesions, each model was meshed using acontrol mesh device (ANSYS Finite Element Analysis Software). All of the virtual models were subjected to two loadtypes, oblique load and vertical load, to simulate occlusal forces of 100 N each. Comparisons were made between simu-lated teeth with non-carious cervical lesions, with and without composite resin restorations, and a simulated soundtooth. Data summarizing the stress distributions were obtained in MPa using von Mises criteria.Results: Oblique loading on simulated non-carious cervical lesions resulted in greater stress concentration compared withvertical loading, and non-carious cervical lesions with acute angles displayed higher stress concentrations at the depth ofthe lesion. Restoring the lesions with an adhesive restoration, such as composite resin, appeared to overcome this stressconcentration.Conclusions: Restoring NCCLs with adhesive restorative materials, such as a nanohybrid composite resin, appears torecover the biomechanical behaviour similar to sound teeth.
Keywords: Biomechanical behaviour, composite resin, finite element analysis, non-carious cervical lesion, teeth.
Abbreviations and acronyms: FEA = finite element analysis; GIC = glass ionomer cement; NCCLs = non-carious cervical lesions.
(Accepted for publication 7 November 2012.)
INTRODUCTION
Non-carious cervical lesions (NCCLs) are formed byloss of tooth structure in the cervical third of thecrown and root surface that is unrelated to dental car-ies.1,2 It is generally accepted that the lesions are notgenerated by a single factor but result from a combi-nation of factors.1,3,4 Among the factors proposed tobe related to the formation and progression of NCCLsare: biocorrosion (chemical, biochemical and electro-chemical degradation) caused by intrinsic and extrin-sic acids; friction (wear) caused by traumaticbrushing; and possibly stresses (abfraction) caused byparafunction, traumatic occlusion and load applica-tion.4 It is most probable that not all of these factorsare involved in any particular case, but more likelyonly a small number. So far, erosion and toothbrush
abrasion have been implicated definitely.5 In addition,reports of NCCLs developing on teeth that did nothave an opposing tooth for many decades add to thecontroversy surrounding the aetiology of theselesions.6 NCCLs are usually diagnosed based on adetailed history, visual inspection and tactile examina-tion.1 It has been proposed that a major factor con-tributing to the progression of NCCLs is a high levelof loading associated with occlusal forces.7,8 Twotypes of loading on maxillary incisors have beendescribed,8 one being an oblique type (due to obliqueor inclined contact with the lingual surface) and thesecond a vertical load (along the long axis of thetooth, applied via the incisal edge).Several studies have examined the characteristics of
NCCLs, such as which teeth show greater involve-ment and the extent of damage, through subjective
306 © 2013 Australian Dental Association
Australian Dental Journal 2013; 58: 306–314
doi: 10.1111/adj.12084
Australian Dental JournalThe official journal of the Australian Dental Association

observations and also using scanning electron micros-copy.5,9,10 Michael et al.11 proposed a classificationfor NCCLs based on their morphological appearance,following an analysis of more than 15 000 extractedanterior teeth. These researchers catalogued anddefined eight different morphological types of NCCLsin anterior teeth.The selection of appropriate direct restorative mate-
rials for NCCLs involves consideration of aesthetics,presence of dentinal hypersensitivity and the amountand state of remaining tooth structure. Restorativematerials, such as glass ionomer cement, resin-modi-fied glass ionomer, flowable composites, and microand nanohybrid composite resins, may be used torestore NCCLs.1,12 Finite element analysis (FEA) hasbeen shown to be a useful method for measuringstress distributions in teeth and restorations inresponse to various loads, and it is possible to modelthe responses of different dental tissues to load appli-cation, taking account of their biological proper-ties.3,8,13,14
We hypothesize that the biomechanical behaviourof maxillary central incisors will differ depending onthe morphology of the NCCL present on the tooth,the presence of a composite resin restoration, and thetype of load applied. Therefore, our objective was tosimulate the influence of an adhesive restoration, suchas a nanohybrid composite resin, and two types ofload application (oblique and vertical) on maxillaryincisors with eight different NCCL morphologies, byanalysing the stress distribution patterns using thefinite element method.
MATERIALS AND METHODS
Two-dimensional elastic linear analysis was per-formed using anatomically based geometric represen-tations for the dentine, pulp, enamel, periodontalligament, cortical bone and trabecular bone.15 Wesimulated eight NCCL morphologies: concave (CO),three types of irregular form (IR1, IR2 and IR3),notched (NO), two types of shallow form (SH1 andSH2), wedged-shape (WS) and also a sound model(SO), according to the classification system ofMichael et al.11 (Fig. 1).
The external and internal contours of enamel, den-tine, pulp, periodontal ligament space, cortical andtrabecular bone were generated by CAD Software(RhinoCeros 3D, McNeel, USA) based on the anatom-ical geometry of the maxillary central incisor. Thesecontours were made by point and line associationusing a polyline module of CAD software. The areascorresponding to each structure were created usingthe biomechanical analysis software ANSYS 12.0(ANSYS Inc., Houston, USA). With this software, thefollowing steps were performed: the pre-process step(area definition, mechanical properties insertion,boundary conditions and mesh creation of each struc-ture), process step (data calculation) and post-processstep (results analysis by stress distribution criteria).The data obtained were exported to ANSYS 12.0using the IGES format. Areas corresponding to eachstructure were meshed with controlled and connectedelements. The meshing process involved division ofthe system to be studied into a set of small discreteelements defined by nodes. The number of elementsgenerated varied depending on the different geome-tries that were meshed, so that the final model accu-rately represented the original geometry. Theisoparametric elements of eight nodes with threedegrees of freedom per node (plane 183) were usedaccording to the mechanical properties of each struc-ture (Fig. 2). The values for mechanical propertieswere obtained by means of a literature review and arelisted in Table 1. For this initial analysis, all of thedental structures and the restorative material in themodels were considered to be homogeneous and iso-tropic, displaying linear elastic properties.The nanohybrid composite resin restorations were
simulated in all models16 (Fig. 3). The restorationswere bonded by mesh connection with dentine andenamel, simulating an adhesive hybrid layer (Fig. 3).The step of establishing boundary conditions consistedof developing a displacement/restriction model withload application. Model displacement of all nodes onthe lateral surface and base of the cortical bone wereconstrained (Fig. 2). Two load types were applied onthe nodes: vertical load (VL) and oblique load (OL),simulating occlusal forces on the palatal surface of anincisor during clenching (in maximum intercuspation)
Fig. 1 2D-finite element models representing NCCL morphologies: SO = sound, CO = concave, IR1 = irregular (with acute internal angles), IR2 = irregular(with rounded internal angles), IR3 = irregular (with acute and rounded internal angles), NO = notched, SH1 and SH2 = shallow and WS = wedge-shaped.
© 2013 Australian Dental Association 307
Biomechanical behaviour of NCCLs
and on the incisal edge during an incising movement.8
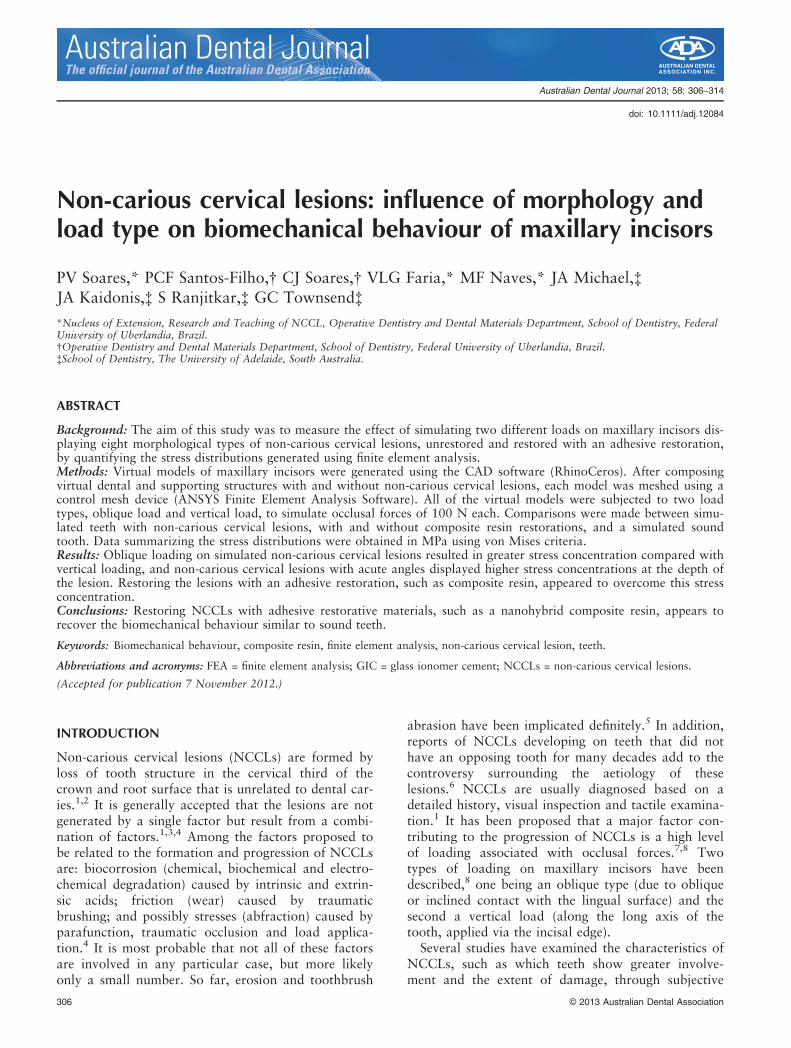
The value of each load was 100 N. The VL wasapplied down through the incisal edge, parallel to thelongitudinal axis of the tooth; the OL was applied tothe palatal cingulum at 130 degrees to the longitudi-nal axis (Fig. 2). The stress distribution analyses wererecorded using the criteria of von Mises, measured inMPa. Five points were chosen for each NCCL,according to morphology type, for analysis of specificregions (Fig. 4).
RESULTS
Rounded angle lesions (CO, NO, SH1, SH2, IR2)showed less stress concentration than acute anglelesions (IR1, IR3, WS). The OL increased the stressconcentration in the cervical area, in the deep dentineand next to pulp, while the VL promoted lower levelsof stress in the supporting structures, with more stressconcentration in the incisal enamel (Fig. 5).For OL, points that represented the deep areas of
the lesion showed the highest indices of stress concen-tration (Fig. 6). NCCLs with deep and acute angleshad the highest stress concentration (IR1, WS, IR3).
In the dual centre morphologies (IR1, IR2, IR3 andSH2), there was more stress concentration in the cer-vical centre of the NCCL. The lesions IR1 and WShad stress levels above 100.0 MPa. Lesions CO, IR2,IR3 showed high stress levels above 40.0 MPa. Thelesion SH2 presented a stress level of 25.8 MPa(Fig. 7).The VL model was associated with lower levels of
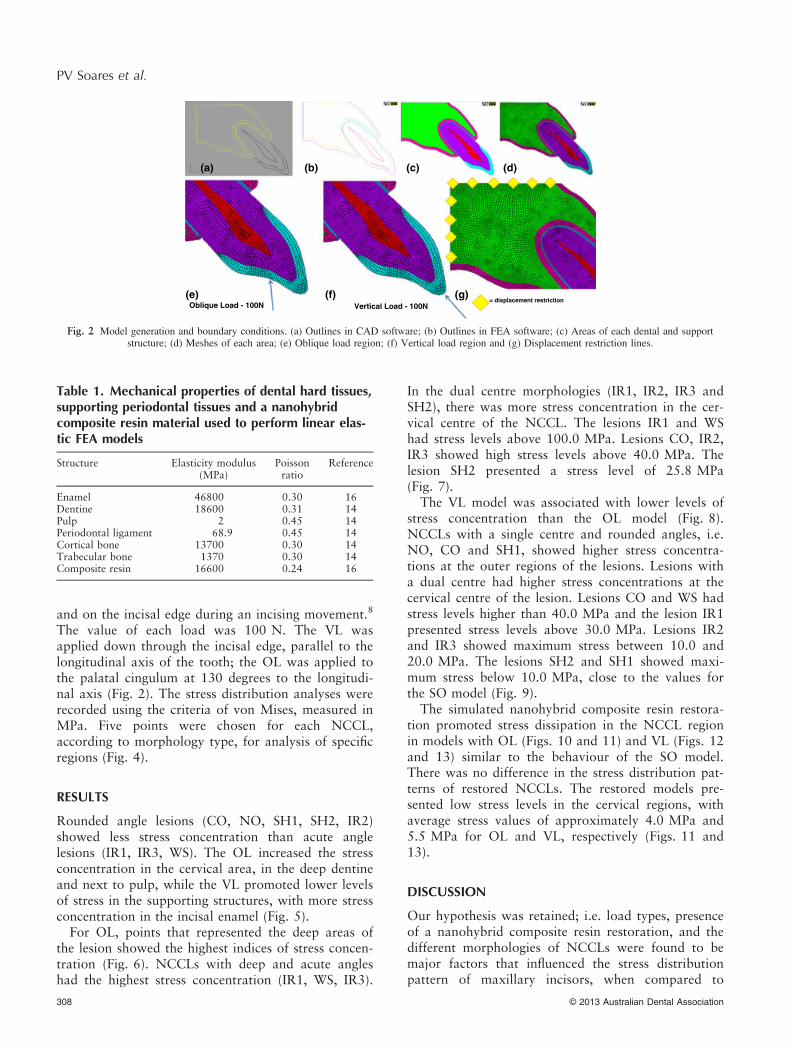
stress concentration than the OL model (Fig. 8).NCCLs with a single centre and rounded angles, i.e.NO, CO and SH1, showed higher stress concentra-tions at the outer regions of the lesions. Lesions witha dual centre had higher stress concentrations at thecervical centre of the lesion. Lesions CO and WS hadstress levels higher than 40.0 MPa and the lesion IR1presented stress levels above 30.0 MPa. Lesions IR2and IR3 showed maximum stress between 10.0 and20.0 MPa. The lesions SH2 and SH1 showed maxi-mum stress below 10.0 MPa, close to the values forthe SO model (Fig. 9).The simulated nanohybrid composite resin restora-
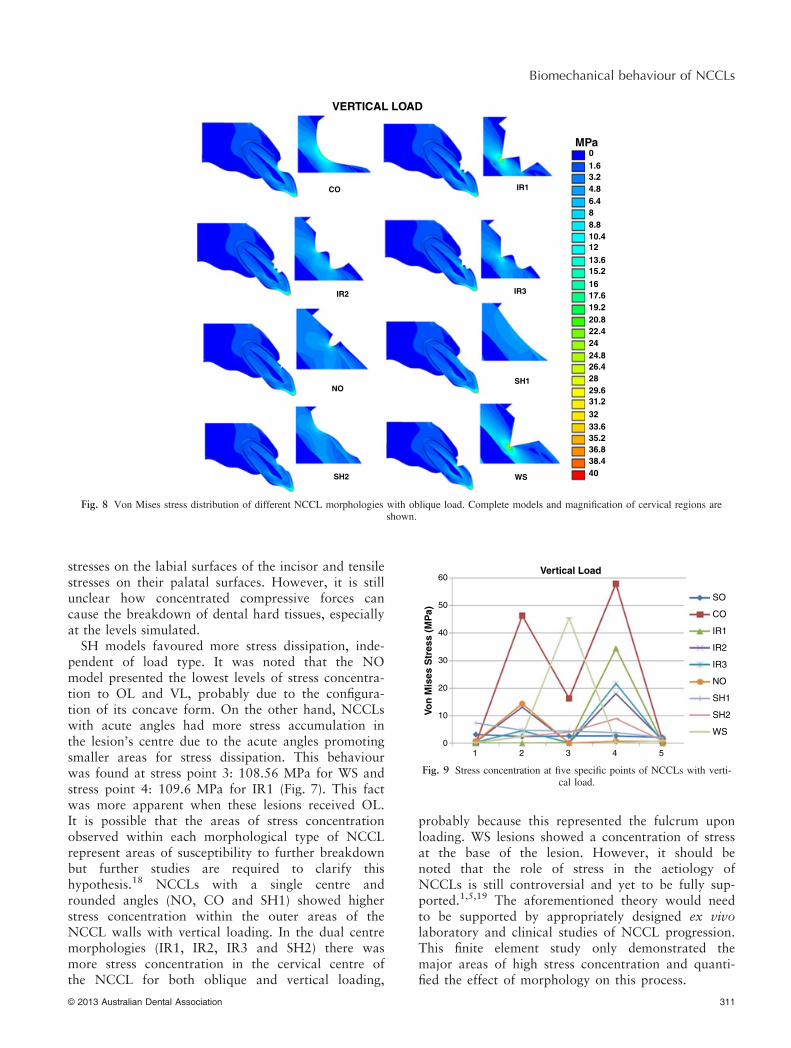
tion promoted stress dissipation in the NCCL regionin models with OL (Figs. 10 and 11) and VL (Figs. 12and 13) similar to the behaviour of the SO model.There was no difference in the stress distribution pat-terns of restored NCCLs. The restored models pre-sented low stress levels in the cervical regions, withaverage stress values of approximately 4.0 MPa and5.5 MPa for OL and VL, respectively (Figs. 11 and13).
DISCUSSION
Our hypothesis was retained; i.e. load types, presenceof a nanohybrid composite resin restoration, and thedifferent morphologies of NCCLs were found to bemajor factors that influenced the stress distributionpattern of maxillary incisors, when compared to
Table 1. Mechanical properties of dental hard tissues,supporting periodontal tissues and a nanohybridcomposite resin material used to perform linear elas-tic FEA models
Structure Elasticity modulus(MPa)
Poissonratio
Reference
Enamel 46800 0.30 16Dentine 18600 0.31 14Pulp 2 0.45 14Periodontal ligament 68.9 0.45 14Cortical bone 13700 0.30 14Trabecular bone 1370 0.30 14Composite resin 16600 0.24 16
(a)
(e)Oblique Load - 100N Vertical Load - 100N
= displacement restriction(f) (g)
(b) (c) (d)
Fig. 2 Model generation and boundary conditions. (a) Outlines in CAD software; (b) Outlines in FEA software; (c) Areas of each dental and supportstructure; (d) Meshes of each area; (e) Oblique load region; (f) Vertical load region and (g) Displacement restriction lines.
308 © 2013 Australian Dental Association
PV Soares et al.

COR IR1R IR2R IR3R
NOR SH1R SH2R WSR
(a) (b) (c)
Fig. 3 Composite restorations in an NCCL. (a) Composite resin area; (b) Mesh of restoration and (c) Interface composite/enamel/dentine.
(a)
5
55
4 43
32
12
1
43
21
(b) (c)
Fig. 4 Specific points chosen for quantitative analysis of different NCCL morphologies. (a) SO model analysis; (b) IR1, IR2, IR3 and SH2 analysis; (c)CO, NO, SH1 and WS analysis.
SO/OL
MPa01.63.24.86.488.8
1210.4
13.615.21617.619.220.822.42424.826.42829.631.23233.635.236.838.440
SO/VL
Fig. 5 Stress distribution by von Mises criteria (MPa) of sound (SO) model with two load types (OL and VL). Complete models and magnification ofcervical regions are shown.
© 2013 Australian Dental Association 309
Biomechanical behaviour of NCCLs

sound teeth. The applied loads were chosen becausethey simulated two types of occlusal forces, one onthe palatal cingulum that simulated a clenching activ-ity in intercuspal occlusion and the other on the inci-sal edge that simulated a biting action.8
The ultimate tensile strength value of cervicalenamel in a perpendicular direction, measured experi-mentally by microtensile tests, is approximately11.5 MPa; the corresponding value for superficialdentine is 61.6 MPa and the value for middle dentine
is 48.7 MPa.17 These values are much higher than thestress values modelled in this study and, therefore, ourmodelled values are unlikely to be sufficient to causecatastrophic damage to dental tissues.The VL induced high levels of stress concentration
in the incisal enamel and the apical aspect of the root.In this case, the stress concentration occurs in the inci-sal region because of the greater enamel thickness.The high elasticity modulus (Table 1) of enamelfavours high stress concentration into its structure.These models enabled estimates of stress concentra-tion deep in the NCCLs; however, they did not allowaetiological factors to be assessed.When NCCLs were present, those models simulat-
ing an OL showed higher stress concentration com-pared with VL. This behaviour is due to the directionof the force that promotes bending of the tooth crownbecause the load is inclined at 130 degrees to the longaxis of the tooth. The VL was applied to the incisaledge, and this favoured a lower dissipation of thestresses within the tooth structure because the enamelis thicker in this region and the resultant force is sub-stantially parallel to the tooth long axis with the pointof load application being remote from the lesion. It isimportant to note that the simulated oblique forcesapplied in this study tended to produce compressive
CO IR1
OBLIQUE LOAD
IR3IR2
NO SH1
SH2 WS
MPa01.63.24.86.4
88.8
1210.4
13.615.216
17.619.220.822.424
24.826.42829.631.23233.635.236.838.440
Fig. 6 Von Mises stress distribution of different NCCL morphologies with oblique load. Complete models and magnification of cervical regions areshown.
110
SO
CO
IR1
IR2
IR3
NO
SH1
SH2
WS
Oblique Load
100
90
80
70
60
50
40
30
20
10
Von
Mis
es S
tres
s (M
Pa)
01 2 3 4 5
Fig. 7 Stress concentration at five specific points of NCCLs with obli-que load.
310 © 2013 Australian Dental Association
PV Soares et al.
stresses on the labial surfaces of the incisor and tensilestresses on their palatal surfaces. However, it is stillunclear how concentrated compressive forces cancause the breakdown of dental hard tissues, especiallyat the levels simulated.SH models favoured more stress dissipation, inde-
pendent of load type. It was noted that the NOmodel presented the lowest levels of stress concentra-tion to OL and VL, probably due to the configura-tion of its concave form. On the other hand, NCCLswith acute angles had more stress accumulation inthe lesion’s centre due to the acute angles promotingsmaller areas for stress dissipation. This behaviourwas found at stress point 3: 108.56 MPa for WS andstress point 4: 109.6 MPa for IR1 (Fig. 7). This factwas more apparent when these lesions received OL.It is possible that the areas of stress concentrationobserved within each morphological type of NCCLrepresent areas of susceptibility to further breakdownbut further studies are required to clarify thishypothesis.18 NCCLs with a single centre androunded angles (NO, CO and SH1) showed higherstress concentration within the outer areas of theNCCL walls with vertical loading. In the dual centremorphologies (IR1, IR2, IR3 and SH2) there wasmore stress concentration in the cervical centre ofthe NCCL for both oblique and vertical loading,
probably because this represented the fulcrum uponloading. WS lesions showed a concentration of stressat the base of the lesion. However, it should benoted that the role of stress in the aetiology ofNCCLs is still controversial and yet to be fully sup-ported.1,5,19 The aforementioned theory would needto be supported by appropriately designed ex vivolaboratory and clinical studies of NCCL progression.This finite element study only demonstrated themajor areas of high stress concentration and quanti-fied the effect of morphology on this process.
MPa01.63.24.86.488.8
1210.4
13.615.2
1617.619.220.822.42424.826.42829.631.2
3233.635.236.838.440
CO IR1
VERTICAL LOAD
IR3IR2
NOSH1
SH2 WS
Fig. 8 Von Mises stress distribution of different NCCL morphologies with oblique load. Complete models and magnification of cervical regions areshown.
60
50
40
30
20
10
0
SO
CO
IR1
IR2
IR3
NO
SH1
SH2
WS
Vertical Load
Von
Mis
es S
tres
s (M
Pa)
1 2 3 4 5
Fig. 9 Stress concentration at five specific points of NCCLs with verti-cal load.
© 2013 Australian Dental Association 311
Biomechanical behaviour of NCCLs

Our finding of reduction in stress concentration inNCCLs after placement of a simulated adhesive dentalmaterial, i.e. a nanohybrid composite resin, providessome support for its use in restoring these lesions.Composite resin has been shown to provide good clin-ical outcomes for longevity, aesthetics, adhesion andbiomechanical properties for various types ofcavities.12,20–22 Glass ionomer cement (GIC) and
resin-modified GIC are also commonly used to restoreNCCLs,23 but clinical studies show shorter longevityfor these materials compared with composite resin.22
GIC has also been considered to possess inadequatematerial and bond strengths in NCCLs when thelesions are subjected to high tensile stresses.24 Futurestudies investigating stress concentration in NCCLsusing different types of adhesive materials could assistclinicians in choosing the appropriate restorativematerial. However, other issues, including ease ofaccess to the cavity (for light-curing purposes), mois-ture control problems and need for fluoride release,will need to be considered in making that decision.Although, based on our findings, some clinicians
may consider rounding of the internal angles ofNCCLs with diamond burs rather than restoringthem. We believe that removal of sound tooth struc-ture in the deeper parts of NCCLs would increase thechances of pulpal irritation or mechanical pulp expo-sure, outweighing the benefits associated with thistype of management. This approach is also contraryto the philosophy of minimally invasive dentistry. In
COR IR1R
OBLIQUE LOAD
IR3RIR2R
SH1R
SH2R
NOR
WSR
MPa0
1.6
3.2
4.8
6.4
8
8.8
12
10.4
13.6
15.2
16
17.6
19.2
20.8
22.4
24
24.8
26.4
28
29.6
31.2
32
33.6
35.2
36.8
38.4
40
Fig. 10 Von Mises stress distribution of different NCCL morphologies restored with composite resin with oblique load. Complete models and magnifica-tion of cervical regions are shown.
2
3
4
5
6
7
1
0
COR
IR1R
IR2R
IR3R
NOR
SH1R
SH2R
WSR
Oblique Load
Von
Mis
es S
tres
s (M
Pa)
1 2 3 4 5
Fig. 11 Stress concentration at five specific points of restored NCCLswith oblique load.
312 © 2013 Australian Dental Association
PV Soares et al.
our opinion, the use of an adhesive restorative mate-rial, when indicated, is a more practical and non-inva-sive treatment of choice, since the results of this paperprove that biomechanically the tooth affected byNCCL when restored behaves as sound teeth.Some important limitations of this research should
be acknowledged. This study analysed only the influ-ence of morphology types and direction of loads onstress concentration within existing NCCLs, not therole of stress as an aetiological factor in the initiation
of NCCLs. Also, we have performed a linear analysis,assuming that the dental tissues display isotropicproperties, which is a simplification of the real situa-tion. Further studies are being performed associatingorthotropic properties, shrinkage stresses and 3Dgeometry on stress concentrations in NCCLs. FutureFEA analyses and experimental studies incorporatingstrain gauge analysis, microscopic analyses, experi-mental fracture tests for different restorative materialsand longitudinal clinical studies, will further serve toelucidate the behaviour of NCCLs and add to thefindings of the present study.
CONCLUSIONS
Within the limits of this study, we can conclude thatin maxillary incisors oblique loading results in greaterstress concentration compared with vertical loadingwithin existing NCCLs, and those NCCLs with acuteangles display the highest stress concentrations at thedepth of the lesion. Restoring NCCLs with adhesiverestorative materials, such as a nanohybrid compositeresin, appears to overcome this stress concentration
MPa0
1.6
3.2
4.8
6.4
8
8.8
12
10.4
13.6
15.2
16
17.6
19.2
20.8
22.4
24
24.8
26.4
28
29.6
31.2
32
33.6
35.2
36.8
38.4
40
COR IR1R
VERTICAL LOAD
IR3RIR2R
NOR SH1R
SH2R WSR
Fig. 12 Von Mises stress distribution of different NCCL morphologies restored with composite resin with vertical load. Complete models and magnifica-tion of cervical regions are shown.
2
3
4
5
6
7
1
0
COR
IR1R
IR2R
IR3R
NOR
SH1R
SH2R
WSR
Vertical Load
Von
Mis
es S
tres
s (M
Pa)
1 2 3 4 5
Fig. 13 Stress concentration at five specific points in restored NCCLswith vertical load.
© 2013 Australian Dental Association 313
Biomechanical behaviour of NCCLs

whether the internal angles of the lesions are roundedor not.
ACKNOWLEDGEMENTS
This study was supported by a grant (SAU022/12 –FAPEMIG-Brazil) from the Minas Gerais ResearchFoundation.
REFERENCES
1. Michael JA, Townsend GC, Greenwood LF, Kaidonis JA.Abfraction: separating fact from fiction. Aust Dent J 2009;54:2–8.
2. Pecie R, Krejci I, Garcia-Godoy F, Bortolotto T. Noncariouscervical lesions – a clinical concept based on the literaturereview. Part 1: prevention. Am J Dent 2011;24:49–56.
3. Rees JS, Hammadeh M, Jagger DC. Abfraction lesion formationin maxillary incisors, canines and premolars: a finite elementstudy. Eur J Oral Sci 2003;111:149–154.
4. Grippo JO, Simring M, Coleman TA. Abfraction, abrasion, bio-corrosion, and the enigma of noncarious cervical lesions: a20-year perspective. J Esthet Restor Dent 2012;24:10–23.
5. Nguyen C, Ranjitkar S, Kaidonis JA, Townsend GC. A qualita-tive assessment of non-carious cervical lesions in extractedhuman teeth. Aust Dent J 2008;53:46–51.
6. Kaidonis JA, Richards LC, Townsend GC. Non-carious changesto tooth crowns. In: Mount GJ, Hume WR, eds. Preservationand restoration of tooth structure. Brighton: Knowledge Booksand Software, 2005:47–60.
7. Rees JS. A review of the biomechanics of abfraction. Eur J Pros-thodont Restor Dent 2000;8:139–144.
8. Dejak B, Młotkowski A. Finite element analysis of strength andadhesion of cast posts compared to glass fiber-reinforced com-posite resin posts in anterior teeth. J Prosthet Dent 2011;105:115–126.
9. Bartlett DW, Shah PA. Critical review of non-carious cervical(wear) lesions and the role of abfraction, erosion, and abrasion.J Dent Res 2006;85:306–312.
10. Daley TJ, Harbrow DJ, Kahler B, Young WG. The cervicalwedge-shaped lesion in teeth: a light and electron microscopicstudy. Aust Dent J 2009;54:212–219.
11. Michael JA, Kaidonis JA, Townsend GC. Non-carious cervicallesions on permanent anterior teeth: a new morphological clas-sification. Aust Dent J 2010;55:134–137.
12. Ferracane JL. Resin composite – state of the art. Dent Mater2011;27:29–38.
13. Soares CJ, Soares PV, Santos-Filho PC, et al. The influence ofcavity design and glass fiber posts on biomechanical behavior ofendodontically treated premolars. J Endod 2008;34:1015–1019.
14. Silva NR, Castro CG, Santos-Filho PC, et al. Influence of differ-ent post design and composition on stress distribution in maxil-lary central incisor: finite element analysis. Indian J Dent Res2009;20:153–158.
15. Soares PV, Santos-Filho PC, Martins LR, Soares CJ. Influenceof restorative technique on the biomechanical behavior of end-odontically treated maxillary premolars. Part I: fracture resis-tance and fracture mode. J Prosthet Dent 2008;99:30–37.
16. Soares PV, Santos-Filho PC, Gomide HA, et al. Influence ofrestorative technique on the biomechanical behavior of end-odontically treated maxillary premolars. Part II: strain measure-ment and stress distribution. J Prosthet Dent 2008;99:114–122.
17. Giannini M, Soares CJ, de Carvalho RM. Ultimate tensilestrength of tooth structures. Dent Mater 2004;20:322–329.
18. Romeed SA, Malik R, Dunne SM. Stress analysis of occlusalforces in canine teeth and their role in the development of non-carious cervical lesions: abfraction. Int J Dent 2012; Article ID234845.
19. Kaidonis JA. Tooth wear: the view of the anthropologist. ClinOral Investig 2008;12(Suppl 1):S21–S26.
20. Soares PV, Santos-Filho PC, Queiroz EC, et al. Fracture resis-tance and stress distribution in endodontically treated maxillarypremolars restored with composite resin. J Prosthodont 2008;17:114–119.
21. Stewardson D, Thornley P, Bigg T, et al. The survival of ClassV restorations in general dental practice: part 1, baseline data.Br Dent J 2010;208:E17.
22. Stewardson D, Creanor S, Thornley P, et al. The survival ofClass V restorations in general dental practice: part 3, five-yearsurvival. Br Dent J 2012;212:E14.
23. Vandewalle KS, Vigil G. Guidelines for the restoration of ClassV lesions. Gen Dent 1997;45:254–260.
24. Ichim I, Schmidlin PR, Kieser JA, Swain MV. Mechanical eval-uation of cervical glass-ionomer restorations: 3D finite elementstudy. J Dent 2007;35:28–35.
Address for correspondence:Paulo Vin�ıcius Soares, DDS, MS, PhD
Av Par�a 1720 Campus UmuaramaUberlandia 38400-000
Federal University of UberlandiaMinas Gerais
BrazilEmail: [email protected]
314 © 2013 Australian Dental Association
PV Soares et al.
Related Documents











