http://aph.sagepub.com/ Public Health Asia-Pacific Journal of http://aph.sagepub.com/content/20/1/16 The online version of this article can be found at: DOI: 10.1177/1010539507308504 2008 20: 16 Asia Pac J Public Health Nguyen Van Huy, Dao Thi Minh An and Dao Ngoc Phong Smoking Among Vietnamese Medical Students: Prevalence, Costs, and Predictors Published by: http://www.sagepublications.com On behalf of: Asia-Pacific Academic Consortium for Public Health can be found at: Asia-Pacific Journal of Public Health Additional services and information for http://aph.sagepub.com/cgi/alerts Email Alerts: http://aph.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: http://aph.sagepub.com/content/20/1/16.refs.html Citations: at Queensland University of Tech on March 10, 2011 aph.sagepub.com Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

http://aph.sagepub.com/Public Health
Asia-Pacific Journal of
http://aph.sagepub.com/content/20/1/16The online version of this article can be found at:
DOI: 10.1177/1010539507308504
2008 20: 16Asia Pac J Public HealthNguyen Van Huy, Dao Thi Minh An and Dao Ngoc Phong
Smoking Among Vietnamese Medical Students: Prevalence, Costs, and Predictors
Published by:
http://www.sagepublications.com
On behalf of:
Asia-Pacific Academic Consortium for Public Health
can be found at:Asia-Pacific Journal of Public HealthAdditional services and information for
http://aph.sagepub.com/cgi/alertsEmail Alerts:
http://aph.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://aph.sagepub.com/content/20/1/16.refs.htmlCitations:
at Queensland University of Tech on March 10, 2011aph.sagepub.comDownloaded from
16
Asia-Pacific Journal OfPublic Health
Volume 20 Number 1January 2008 16-24
© 2008 APACPH10.1177/1010539507308504
http://aph.sagepub.com hosted at
http://online.sagepub.com
Smoking Among Vietnamese Medical Students: Prevalence, Costs, and Predictors
Nguyen Van Huy, MHID, Dao Thi Minh An, PhD, and Dao Ngoc Phong, PhD, MPH
This cross-sectional study investigated smoking patterns and predictors among Vietnamese medicalstudents. In total, 4720 medical students from 3 universities, each located in South, Central,and North Vietnam, were interviewed using an adapted Global Youth Tobacco Survey Questionnaire.Ideas on smoking behavior and tobacco control derived from group discussions with studentsand from unstructured interviews with student managers and university directors. Overall, thecurrent smoking rate was 25.0% and dominant in men at 43.7%. Most started smoking when justentering university (18 ± 3.3 years). Male students from the central region had the highest smokingrate (35.1%), whereas their northern counterparts had the greatest smoking magnitude: age ofsmoking initiation (18.6 ± 3.5), number of cigarettes per day (4.4 ± 4.5), number of smokingdays per month (16.5 ± 11.6), and proportion of smoking cost among total expenses per month(10.9% ± 11.9%). Smoking tended to increase across academic years, being highest in years 5 to6 (35.0%). In contrast, the practice of ever quitting and the intention of quitting tendedto decline from years 1-2 to years 5-6 (from 82.2% to 71.5%, P < .05, and from 70.8% to 51.5%,P < .001, respectively). Positive attitudes toward smoking (odds ratio = 1.4, P < .05), negativebeliefs on hazards of smoking (odds ratio = 1.7), and daily exposure to family smokers (odds ratio= 2.0, P < .05) and to social smokers (odds ratio = 4.5, P < .05) were main predictors of smoking.Qualitative results suggest that nonsmoking university regulations played a critical role in tobaccocontrol among medical students. Nonsmoking regulations and penalties for students who smokeneed to be formulated at medical universities. The message that medical students must make anonsmoking role model for community should be systematically promoted.
Keywords: Vietnam; medical students; smoking; knowledge; belief; attitude; predictors
Although medical students and health professionals are expected to play a key role incontrolling tobacco use,1-3 many of them smoke cigarettes. Although vast data haveshowed very common smoking rates among the general population,4 numerous studies
have also pinpointed that smoking among medical students is of great concern because oftheir prevalence and influence. In Albania, 55% of male and 34% of female fifth-year medicalstudents were smokers.5 In addition, 74.3% of Chinese medical students and health workersstarted smoking before age 20 years.6 Nearly 50% of medical science students in Ahwaz,
From the Public Health Faculty, Hanoi Medical University, Hanoi, Vietnam.
Address correspondence to: Nguyen Van Huy, Faculty of Public Health, Hanoi Medical University, 01 Ton That Tung Str,Dong Da Dist, Hanoi, Vietnam; e-mail: [email protected].
at Queensland University of Tech on March 10, 2011aph.sagepub.comDownloaded from

Smoking Among Vietnamese Medical Students / Huy et al 17
Iran, smoked.7 Tuscany, Italy, saw 30% of its medical students smoke.8 More than 30% ofItalian medical students smoked, of whom 40% and 25% were men and women, respectively.8
A worldwide survey revealed that among 9000 students from 51 medical universities in42 countries, smoking prevalence varied remarkably from 0% to 48% among male medicalstudents and from 0% to 22% among female students.9 Smoking among health providers,including medical students, is not only harmful to their own health but also to the public,due to their exemplary behavioral role.8 Their smoking behavior affects not only their healthand their families’ health but also the health care services they provide to their futurepatients.10,11 However, these studies have not investigated predictors of smoking amongmedical students, which may play a crucial part in informing tobacco control initiatives.
In Vietnam, extensive data on smoking patterns among general university students areavailable, but information on smoking among medical students is limited. A survey showedthat 20.6% of university students, not including medical students, were smokers.12 Somestudies indicated that the smoking rate was 70.5% to 76.1% among male students versus2.8% to 5.3% among female students, not including medical students.13 Although the healthsector has been actively attempting to provide messages about smoking prevention to thegeneral population, specific regulations against tobacco at medical universities are still limitedand not well recognized.
This study thus aims to investigate the prevalence of and the costs for smoking, and itidentifies predictors of smoking among Vietnamese medical students.
Setting, Sample, and Procedure
The study was conducted at the 3 largest medical universities from 3 major regions ofVietnam: Hanoi Medical University in North Vietnam, Hue Medical University in CentralVietnam, and Can Tho University in South Vietnam. All students from the first to the sixthacademic years were eligible for study. A total of 4720 male and female medical studentswere surveyed, using the anonymous self-administered questionnaires. The questionnaireswere distributed after class and were voluntarily filled out on-site by students and thenreturned immediately to the research team. Of the 4720 students who provided informedconsent, 4701 from all 6 academic years—first year (1060), second year (859), third year(662), fourth year (647), fifth year (871), and sixth year (602)—returned their completelyfilled questionnaires, reaching a 99.5% response rate.
Some further qualitative research was also undertaken in which at each university, 1in-depth interview with 1 student manager, another in-depth interview with 1 vice director,and 2 group discussions with student volunteers were conducted.
Instrument
The Global Youth Tobacco Survey Questionnaire14 was adopted for quantitative survey. Thequestionnaire was adapted and double translated (English into Vietnamese and vice versa)to ensure the original meanings of the questions. The questionnaire was in 6 key parts: personalinformation, knowledge and attitudes, tobacco use behavior, exposure to smokers, accessto tobacco information, and access to antitobacco health education at medical universities.A pretest survey of 1 class in each university was done before actual surveys to checkthe appropriateness of the questionnaire. The necessary amendments of wording for somequestions were made so the questions were better understood according to languages anddialects of each region, but these revisions did not change the originality of the main ideasof the questions.
at Queensland University of Tech on March 10, 2011aph.sagepub.comDownloaded from

18 Asia-Pacific Journal of Public Health / Vol. 20, No. 1, January 2008
The qualitative approaches used 2 developed guidelines: one for in-depth interviews andthe other for group discussions with technical advice of some experts from the Institute forGlobal Tobacco Control and Johns Hopkins University.
Data Collection and Analysis
Both quantitative and qualitative data were collected by well-trained surveyors. Supervisionswere made during surveys; if any questions were raised by students, researchers would providenecessary on-site guidance. A smoker is defined as one who has ever smoked in the past or isnow smoking (current smoker), whereas a nonsmoker is defined as one who has never smoked.
Quantitative data were input by using EPI-INFO (Version 6.04), then transferred intoSTATA (Version 7.0). The analytical process included cleaning data and generating frequenciesand percentages for intended variables. The chi-square test was used for comparing 2 percent-ages, analysis of variance (ANOVA) was used to compare mean values between groups, theodds ratio (OR) measured the causal combination, multivariate analysis controlledconfounders, and the trend test examined the trends of the data. Statistical significance wasdefined as P < .05, and nonsignificant difference was marked as NS (ie, P ≥ .05).
Qualitative data were converted from a tape recorder into word text using a tape trans-lation method and coding for variables of interest by researchers. Quotations were done tosupport quantitative findings.
Results
A brief pattern of smoking among medical students is presented in Table 1. The overallcurrent smoking prevalence was 25.0% and significantly varied by regions, ranging from
Table 1. Major Demographic Patterns of Smoking Status
Variables North n (%) Central n (%) South n (%) Total n (%) P Valuea
Total number of subjects 2539 1092 1070 4701Smoking status
Ex smoker 6 (0.2) 1 (0.1) 19 (1.8) 26 (0.6) .000Current smoker 596 (23.5) 383 (35.1) 194 (18.1) 1173 (25.0) .000Nonsmoker 1937 (76.3) 708 (64.8) 857 (80.1) 3502 (74.4) .000
Total Subjects in Each Category
Nb n (%) Nb n (%) Nb n (%) Nb n (%) P Valuea
Current smoking status by sex and academic years according to regions Sex
Male 1348 580 (43.0) 626 366 (58.5) 619 188 (30.4) 2593 1134 (43.7) .000Female 1191 16 (1.3) 466 17 (3.7) 451 6 (1.3) 2108 39 (1.9) .010
Class yearYears 1-2 992 161 (16.2) 466 116 (24.9) 456 53 (11.6) 1914 330 (17.2) .000Years 3-4 791 190 (24.1) 208 69 (33.2) 315 68 (21.6) 1314 327 (24.9) .000Years 5-6 756 245 (32.4) 418 198 (47.4) 299 73 (24.4) 1473 516 (35.0) .000
Trend testc .000
a. Compares smoking rates by categories among regions.b. N = Total subjects in each category.c. Examines the trends in smoking rate across academic years.
at Queensland University of Tech on March 10, 2011aph.sagepub.comDownloaded from

Smoking Among Vietnamese Medical Students / Huy et al 19
18.3%, 23.5%, and 35.1% in the south, north, and central regions, respectively (P = .000).Notably, smoking was dominant in men, with the highest rate in Central Vietnam (58.5%).The smoking rate tended to increase across academic years (P = .000); it was lowest in years1 to 2 (17.2%) and greatest in years 5 to 6 (35.0%). This upward trend from the first to sixthyear is clear in all 3 regions (P = .000).
Smoking habits among male students are shown in Table 2. Although gender distributionwas similar in all 3 regions, with more male (55.09%) than female students, the rate ofsmoking was much lower in female students. Due to this reason, we only analyze data relatedto male students in the tables that follow. Although current smoking rate (58.5%) and thecost of buying a package of cigarettes (0.6 ± 0.2 USD) were highest among male studentsin Central Vietnam, male students in North Vietnam displayed the greatest smoking magnitude.Among students in North Vietnam, the age of starting smoking was lowest (18.6 ± 3.5), butthe number of smoking days per month (16.5 ± 11.6) and the number of cigarettes smokedper day (4.4 ± 4.5) were the highest. These figures were lowest in South Vietnam (P < .05).In particular, the students from North Vietnam had the highest proportion of costs for smoking(10.9% ± 11.9%) compared with students from Central and South Vietnam (P = .010) andthe lowest rate of intentions of quitting in the 12 next months (53.1%) (P = .001).
In parallel with an increased trend of smoking across academic years (Table 1), smokingextent also increased across academic years, as seen in Table 2. The age when studentsstarted smoking tended to decrease from years 5-6 to years 1-2 (19.2 ± 3.6 to 17.8 ± 3.0,P = .000). The number of smoking days per month (14.3 ± 10.4 to 16.6 ± 11.1), the numberof cigarettes smoked per day (3.4 ± 3.8 to 4.6 ± 4.6), morning smoking habits (35.9% to 44.6%),and the proportion of costs for smoking over total costs (8.4% ± 10.9% to 11.0% ± 11.5%)
Table 2. Smoking Habits and Costs of Male Students Across Regions and Academic Years
North, Central, South, 1-2 Years, 3-4 Years, 5-6 Years, Variables Mean ± SD Mean ± SD Mean ± SD P Value Mean ± SD Mean ± SD Mean ± SD P Value
Average age started 18.6 ± 3.5 18.9 ± 3.2 19.4 ± 3.1 .015 17.8 ± 3.0 19.1 ± 3.0 19.2 ± 3.6 .000smoking
Average number of 16.5 ± 11.6 15.9 ± 9.8 13.7 ± 11.2 .010 14.3 ± 10.4 16.3 ± 11.3 16.6 ± 11.1 .008smoking days in a month
Average number of 4.4 ± 4.5 4.0 ± 4.1 3.5 ± 3.4 .031 3.4 ± 3.8 4.2 ± 3.8 4.6 ± 4.6 .000cigarettes smoked a day
Average percentage 10.9 ± 11.9 9.4 ± 11.4 8.3 ± 8.3 .010 8.4 ± 10.9 10.0 ± 11.3 11.0 ± 11.5 .004of costs for smoking out of total spending per montha
n (%) n (%) n (%) P Value n (%) n (%) n (%) P Value
Smoking habits 215 (37.1) 178 (48.6) 67 (35.6) .000 113 (35.9) 121 (38.8) 226 (44.6) .030every morning
Ever tried to quit 437 (75.6) 281 (76.8) 132 (70.2) NS 259 (82.2) 230 (73.7) 361 (71.5) .001smoking
Intention to quit 308 (53.1) 251 (68.6) 116 (61.7) .000 223 (70.8) 191 (61.2) 261 (51.5) .000in next 12 months
NS, not significant.a. Calculated as means of expenses for tobacco per month over total general expenses per month, then multipliedby 100.
at Queensland University of Tech on March 10, 2011aph.sagepub.comDownloaded from
20 Asia-Pacific Journal of Public Health / Vol. 20, No. 1, January 2008
all also tended to rise from years 1-2 to years 5-6 (P < .05). In contrast, the practice of everquitting and the intention of quitting tended to decline from years 1-2 to years 5-6 (82.2%to 71.5% and 70.8% to 51.5%, with P = .001 and P = .000, respectively). Two main possiblereasons for smoking are as follows: (1) smoking is considered a way of communicating andsocializing with friends and community (33.3%). One participant said, “Without smoking,I feel it is difficult to join my friends” (focus group discussion with second-year male studentin North Vietnam). (2) Smoking also helps them deal with sadness, tension, or nervousness(32.4%). Another participant said, “One cigarette made me reduce my sorrow and get some-thing fresh to learn” (focus group discussion with fifth-year male student in Central Vietnam).One of the factors contributing to more smoking among students from North and CentralVietnam than among students from South Vietnam related to a lack of cigarette restrictionregulations at the northern and central universities, as shown from discussions with leadersof 3 medical universities. “At our university, we made the no-smoking regulations in the hall;if one commits, he or she will get a penalty,” a student manager of Can Tho University said.For the Hanoi and Hue medical universities in North and Central Vietnam, the studentmanagers say, “We know that there needs to be a regulation of no smoking, but it is still notavailable in lecture halls and hospitals.”
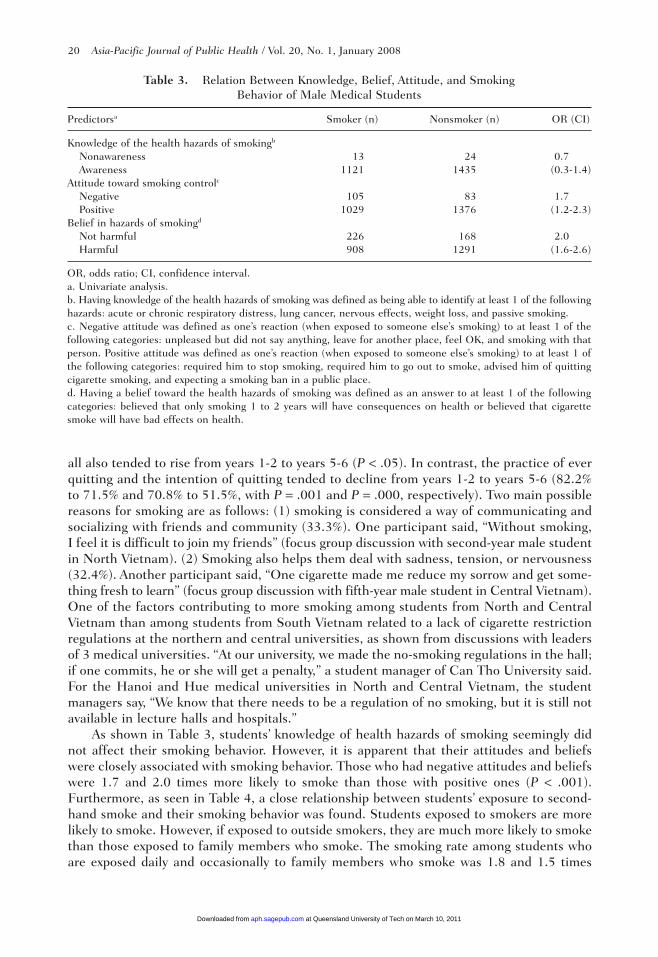
As shown in Table 3, students’ knowledge of health hazards of smoking seemingly didnot affect their smoking behavior. However, it is apparent that their attitudes and beliefswere closely associated with smoking behavior. Those who had negative attitudes and beliefswere 1.7 and 2.0 times more likely to smoke than those with positive ones (P < .001).Furthermore, as seen in Table 4, a close relationship between students’ exposure to second-hand smoke and their smoking behavior was found. Students exposed to smokers are morelikely to smoke. However, if exposed to outside smokers, they are much more likely to smokethan those exposed to family members who smoke. The smoking rate among students whoare exposed daily and occasionally to family members who smoke was 1.8 and 1.5 times
Table 3. Relation Between Knowledge, Belief, Attitude, and Smoking Behavior of Male Medical Students
Predictorsa Smoker (n) Nonsmoker (n) OR (CI)
Knowledge of the health hazards of smokingb
Nonawareness 13 24 0.7Awareness 1121 1435 (0.3-1.4)
Attitude toward smoking controlc
Negative 105 83 1.7Positive 1029 1376 (1.2-2.3)
Belief in hazards of smokingd
Not harmful 226 168 2.0Harmful 908 1291 (1.6-2.6)
OR, odds ratio; CI, confidence interval.a. Univariate analysis.b. Having knowledge of the health hazards of smoking was defined as being able to identify at least 1 of the followinghazards: acute or chronic respiratory distress, lung cancer, nervous effects, weight loss, and passive smoking.c. Negative attitude was defined as one’s reaction (when exposed to someone else’s smoking) to at least 1 of thefollowing categories: unpleased but did not say anything, leave for another place, feel OK, and smoking with thatperson. Positive attitude was defined as one’s reaction (when exposed to someone else’s smoking) to at least 1 ofthe following categories: required him to stop smoking, required him to go out to smoke, advised him of quittingcigarette smoking, and expecting a smoking ban in a public place.d. Having a belief toward the health hazards of smoking was defined as an answer to at least 1 of the followingcategories: believed that only smoking 1 to 2 years will have consequences on health or believed that cigarettesmoke will have bad effects on health.
at Queensland University of Tech on March 10, 2011aph.sagepub.comDownloaded from

Smoking Among Vietnamese Medical Students / Huy et al 21
higher than that among students not exposed, whereas students who are exposed daily andoccasionally to outside smokers had a 6.0- and 2.4-fold rate of smoking as compared withthose students who are not exposed (P < .05, CI ≠ 1 and OR > 1).
Table 5 shows that, after adjusting for regions, academic years, exposure to family members,exposure to social members, and knowledge, attitudes, and beliefs (KAB), the odds ratioswere similar to those of univariate analysis (ie, before making necessary adjustments).These results suggest that if the factors of region, academic year, knowledge, and attitude aresimilar between smoker and nonsmoker groups, then exposure to smoker surroundings, espe-cially in external settings, would be a significant determinant of smoking habits of students.Reversely, if such factors as family, region, academic year, and exposure were similarbetween smoker and nonsmoker groups, then attitude toward cigarette control and beliefabout hazards of smoking are factors influencing smoking behavior among students. In mostinstances, the prediction is statistically significant (OR > 1, CI ≠ 1).
Discussion
The above figures show a relatively common current smoking phenomenon amongVietnamese medical students (25%), especially in men (44.7%; Table 1). Compared withsome developed and developing countries, such as Bosnia and Herzegovina,2 the UnitedStates,15 Iran,7 China,6 Italy,8 Albania,5 and France,16 Vietnamese medical students demon-strate a lower smoking rate.
However, a striking feature to note is that the smoking rate among Vietnamese medicalstudents tends to increase across academic years (Table 1). Also, there is an increasing trendin the magnitude of smoking over academic years. The result also shows that students startedsmoking when just entering the university (Table 2). These data suggest that to reducesmoking among medical students, more attention should be given to early smoking prevention,when students are in their first years at the university.
However, what is more important is to determine the factors influencing smokingbehaviors and what kinds of intervention need to be taken into account. Responding to theseconcerns, results from univariate and multivariate analyses in Tables 3 and 5 show thatknowledge is not a decisive factor in smoking. Smoking is not significantly greater in thosepersons without knowledge of the hazards of smoking (OR < 1). Other studies on knowledge,attitudes, beliefs, and practices (KABP) related to smoking also show a similar pattern.Razak et al17 also found that medical students still decided to smoke, even though they had
Table 4. Relation Between Exposure to Secondhand Smoke and Smoking Behavior of Male Medical Students
Predictorsa Smoker (n) Nonsmoker (n) OR (CI)
Exposure to social smokers Seldom 28 120 1Occasional 515 916 2.4 (1.6-3.8)Daily 586 421 6.0 (3.8-9.5)
Exposure to family smokersNever 226 408 1Seldom 225 292 1.4 (1.1-1.8)Occasionally 438 511 1.5 (1.3-1.9)Daily 243 245 1.8 (1.4-2.3)
OR, odds ratio; CI, confidence interval.a. Univariate analysis.
at Queensland University of Tech on March 10, 2011aph.sagepub.comDownloaded from

22 Asia-Pacific Journal of Public Health / Vol. 20, No. 1, January 2008
fairly good knowledge of the harmful effects of smoking. According to Detels,18 the impactof knowledge is not strong enough to change behavior. By contrast, attitudes and beliefs areclosely associated with smoking. Medical students who have negative attitudes toward smokingcontrol and who do not believe in the hazards of smoking are more likely to smoke (OR =1.4 and 1.7, respectively; Table 5). As such, to prevent smoking among medical students, it isnot enough to provide them only with antitobacco information. Attention should also be givento their beliefs and attitudes toward smoking. The process of the behavioral transformation ofmedical students could thus be possible by involving more students in research related to theconsequences of tobacco smoking, which could affect all 3 major channels: from knowledgeto beliefs and attitudes toward cigarette use among medical students at universities.
The study also indicates that exposure to secondhand smoking from family or socialmembers is another smoking predictor of medical students (Tables 4, 5), and other studiesalso have shown the remarkable impact of this exposure.17,19,20,21 This suggests an importantrole of focusing intervention impacts on students’ surrounding environments, where theirfamily members and friends are smokers, by promoting messages via information, educationand communication channels about the hazards of smoking. Furthermore, qualitative datasuggest that the lack of strict regulations on smoking restrictions or a ban is also a criticaldeterminant of smoking, which is also consistent with quantitative data showing a greatersmoking rate among students from North and Central Vietnam than among studentsfrom South Vietnam. The lowest prevalence of smoking in South Vietnam (Table 1) can beattributed to stricter no-smoking regulations than in other regions. The significant effects of
Table 5. Predictors of Smoking
% Smokers by Predictorsa Categories OR 95% CI
RegionSouth 51.1 1.0 2.7-4.4North 32.3 3.4 1.5-2.4Central 16.6 1.9
Academic year1-2 years 27.8 1.0 1.3-1.93-4 years 27.5 1.6 2.1-3.15-6 years 44.7 2.5
Exposure to family membersNever 19.7 1.0 1.2-2.0Seldom 19.9 1.5 1.3-2.1Occasionally 38.7 1.6 1.5-2.6Daily 21.5 2.0
Exposure to social membersSeldom 2.5 1.0 1.3-3.0Occasionally 45.6 2.0 2.9-7.1Daily 51.9 4.5
Having knowledge of health hazards of smokingNo 98.9 0.7 0.3-1.3Yes 1.1 1.0
Positive attitude toward not smokingNo 90.9 1.4 1.0-2.0Yes 9.1 1.0
Belief in the hazards of smokingNo 79.7 1.7 1.3-2.2Yes 20.3 1.0
OR, odds ratio; CI, confidence interval.a. Multivariate analysis.
at Queensland University of Tech on March 10, 2011aph.sagepub.comDownloaded from

Smoking Among Vietnamese Medical Students / Huy et al 23
smoking restrictions, one of the components of a comprehensive tobacco control program, onsmoking behaviors of the community have also been well documented.22,23 Hence, tobaccocontrol policies should include official and strict regulations on smoking restrictions at med-ical universities.
In sum, tobacco control policies, such as regulations of no smoking and penalties forsmoking, need to be made available at medical universities. Moreover, the message that“medical students must be a nonsmoking role model for people around” should be promoted,and the study of the health hazards of smoking should get students involved when they enteruniversity.
The study should be interpreted in light of some potential limitations. Because of thenature of self-administrated questionnaires, some missing data are inevitable. Some informa-tion requires students to recall from their history; thereby, recall bias may occur. Also, dueto their self-esteem, some students may have over- or underreported their smoking status.However, because the study had well-informed consent with confidentiality ensured beforethe surveys, this could have kept the above bias to a minimum. In addition, the questionnairesused are adapted from the Global Youth Tobacco Survey Sample Questionnaire,14 which hasbeen believed to be well designed, thereby perhaps helping reduce some certain errors.
Acknowledgments
The authors wish to thank Professor Jonathan M. Samet, Ms Mai Hoang Anh, and Ms ErikaTang, all from the Institute for Global Tobacco Control at Johns Hopkins University for theirgreat support and help to the manuscript. We acknowledge Associate Professor Do Van Dung,Faculty of Public Health, Ho Chi Minh Medical and Pharmacology University, Vietnam, andMs Kylie Lange, statistical consultant, Flinders University, Australia, for their useful consul-tancy on statistical approaches of this study. The authors also thank Ms Menchi G. Velascofrom the Thai Health Promotion Foundation for her vital initial guidance. Mr Byron Crapefrom the Institute of Global Tobacco Control is appreciated for his provision of some valuablematerials for our study. Last, the implementation of this study was made possible with financialsupport from the Rockefeller Foundation and Thai Health Promotion Foundation.
References
1. Schoberberger R. Smoking cessation and different roles of health professionals. In: Book ofAbstracts: The Third World Assembly on Tobacco Counters Health (WATCH 2004); March 7-11,2004:26.
2. Omanic A, Niksic D, Mujicic AK, Dzubur A. Smoking habit among health workers in FBIH. In:Book of Abstracts: The Third World Assembly on Tobacco Counters Health (WATCH 2004); March7-11, 2004:192.
3. Faseru B, Barengo N, Sandstrom PH, Omokhodion F. Medical students support FCTC in Nigeria.In: Book of Abstracts: The Third World Assembly on Tobacco Counters Health (WATCH 2004);March 7-11, 2004:194.
4. Centers for Disease Control and Prevention (CDC). Tobacco Information and Prevention Source:Overview. Available at: http://www.cdc.gov/tobacco/issue.htm. Accessed June 10, 2005.
5. Vakeflliu Y, Argjiri D, Peposhi I, Argon S, Melani AS. Tobacco smoking habits, beliefs and attitudesamong medical students in Tirana, Albania. Prev Med. 2002;34:370-373.
6. Li HZ, Fish D, Zhou X. Increase in cigarette smoking and decline of anti-smoking counseling amongChinese physicians 1987-1996. Health Promot Int. 1999;2:123-131.
7. Ahmadizadeh M, Haghighizadeh MH. Affecting factors in tendency toward tobacco smoke amongmedical science students in Ahwaz. In: Book of Abstracts: The Third World Assembly on TobaccoCounters Health (WATCH 2004); March 7-11, 2004:149.
at Queensland University of Tech on March 10, 2011aph.sagepub.comDownloaded from

8. Melani AS, Verponziani W, Boccoli E, et al. Tobacco smoking habits, attitudes and beliefs amongnurse and medical students in Tuscany. Eur J Epidemiol. 2000;16:607-611.
9. Crofton J, Tesseir JF. A worldwide survey of knowledge and attitudes of tobacco among medicalstudents. In: Richmond R, ed. Educating Medical Students About Tobacco Planning andImplementation, Tobacco Prevention Section. Paris: International Union Against Tuberculosis andLung Disease (IUATLD); 1996:271-280.
10. Spencer JK. Nurses’ cigarette smoking in England and Wales. Int J Nurs Stud. 1984;21:69-79.11. Tish Knobf MK, Morra M. Smokers, former smokers and non-smokers: a correlational study of
nurses in Connecticut. Oncol Nurs Forum. 1983;10:40-45.12. Vietnamese and Swedish Health Cooperation Program. Reports on Results of Anti-Tobacco Project
for the 1999-2000 Period. Hanoi: Vietnam Ministry of Health; 2002.13. Vietnam National Centre for Social Sciences and Humanities, Ho Chi Minh Centre for Information
and Health Education & California University. Vietnam: A Tobacco Epidemic in the Making. Hanoi:Vietnam National Centre for Social Sciences and Humanities; 1995.
14. Centers for Disease Control and Prevention. Global Youth Tobacco Survey Sample Questionnaire.http://www.cdc.gov/tobacco/global.htm. Accessed June 10, 2005.
15. Torabi MR, Yang J, Li J. Comparison of tobacco use knowledge, attitude and practice among collegestudents in China and the United States. Health Promot Int. 2002;17:247-253.
16. Josseran L, Raffin J, Dautzenberg B, Brucker G. Knowledge, opinions and tobacco consumptionin a French faculty of medicine. Presse Med. 2003;32:1883-1886.
17. Razak HL, Rahmat A, Harris AWA, Yusoff HM, Lim BK. Knowledge and attitude of adolescentsin a tobacco cessation training programme. In: Book of Abstracts, The Third World Assembly onTobacco Counters Health (WATCH 2004); March 7-11, 2004:77.
18. Detels R. Principles of community intervention. Workshop on community intervention in QuangNinh Province; August 18-20, 2005.
19. Singh MCVV, Singh CZ, Banerjee A, Basannar S. Determinants of smoking habit among medicalstudents. Med J Armed Forces India. 2003;59:209-211.
20. Mohtashami J, Noghani F. Familial factors influencing addition. In: Book of Abstracts: The ThirdWorld Assembly on Tobacco Counters Health (WATCH 2004); March 7-11, 2004:44.
21. Rafiee A, Haghighizadeh MH. Prevalence rate and individual, familial and social characteristicsassociated with cigarette smoking among high school students of Behbahan city, Iran. In: Book ofAbstracts: The Third World Assembly on Tobacco Counters Health (WATCH 2004); March 7-11,2004:140.
22. Collishaw NE. Global tobacco control: current status. In: Richmond R, ed. Educating MedicalStudents About Tobacco Planning and Implementation, Tobacco Prevention Section. Paris, France:International Union Against Tuberculosis and Lung Disease (IUATLD); 1996:197-214.
23. World Health Organization. Guidelines for Controlling and Monitoring the Tobacco Epidemic.Geneva, Switzerland: World Health Organization; 1998.
24 Asia-Pacific Journal of Public Health / Vol. 20, No. 1, January 2008
at Queensland University of Tech on March 10, 2011aph.sagepub.comDownloaded from
Related Documents











