Smartphones and Information Management for Rural Health Care Clinics in Africa Melissa Ho ([email protected]) PhD Student, School of Information “Global Development in Action” Student Symposium Thursday, October 4, 2007 Blum Center for Developing Economies, UC Berkeley

Smartphones and Information Management for Rural Health Care Clinics in Africa Melissa Ho ([email protected]) PhD Student, School of Information.
Dec 18, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Smartphones and Information Management for Rural Health Care Clinics in
Africa
Melissa Ho ([email protected])
PhD Student, School of Information
“Global Development in Action” Student Symposium
Thursday, October 4, 2007
Blum Center for Developing Economies, UC Berkeley

Moving right along…
A quick overview of the context Communications Infrastructure Healthcare Information Practices What is a smartphone?
Research Framework Findings on the Ground
Framing the Context Learning from Experience Proposing Solutions

CIA World Factbook
Population: 30,262,610 Infant Mortality Rate:
total: 67.22 deaths/1,000 live births
HIV/AIDS prevalence: 4.1%
Landlines: 108,100 (2006)
Mobiles: 2.009 million (2006)
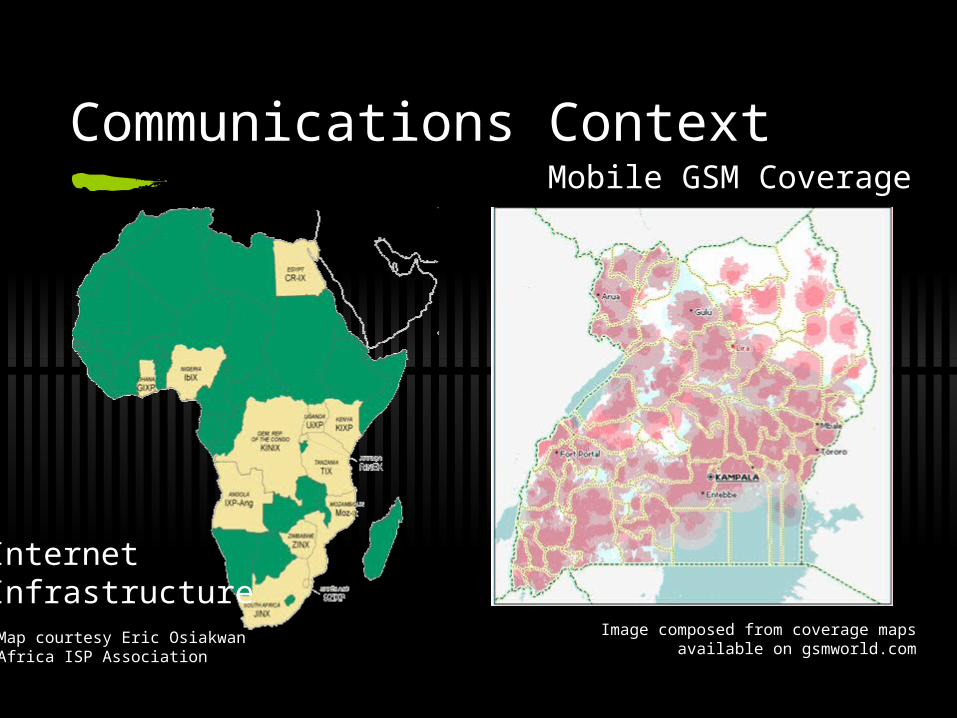
Communications Context
Image composed from coverage mapsavailable on gsmworld.com
InternetInfrastructure
Mobile GSM Coverage
Map courtesy Eric Osiakwan Africa ISP Association
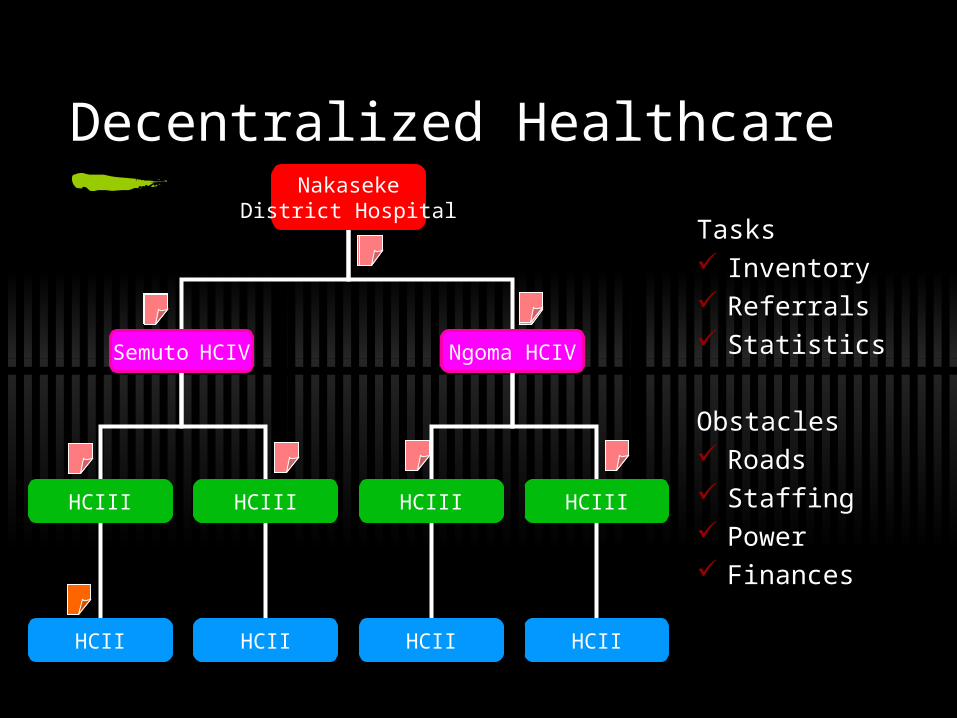
NakasekeDistrict Hospital
Semuto HCIV
HCIII HCIII
HCII HCII
Ngoma HCIV
HCIII
HCII
HCIII
HCII
Decentralized Healthcare
Tasks Inventory Referrals Statistics
Obstacles Roads Staffing Power Finances

Output-based Aid (OBA) Voucher Program Subsidized voucher for treatment of sexually
transmitted infections (STIs) with modified syndromic and lab diagnostics
brand price per voucher
barcode sticker partner
or client

Marie Stopes International Uganda (MSI-U) & Microcare Insurance Ltd.
Community distributors(44 at start)
Clients(+350 per month)
Clinics(16 at start)
Submit claims
Pay service provider
Sell vouchers
Submit voucher to provider
Send vouchers
Record voucher
sales data
Provide STI diagnosis and
treatment Paycash
avg 30 days
max 60 days
avg 15 days
max 45 days
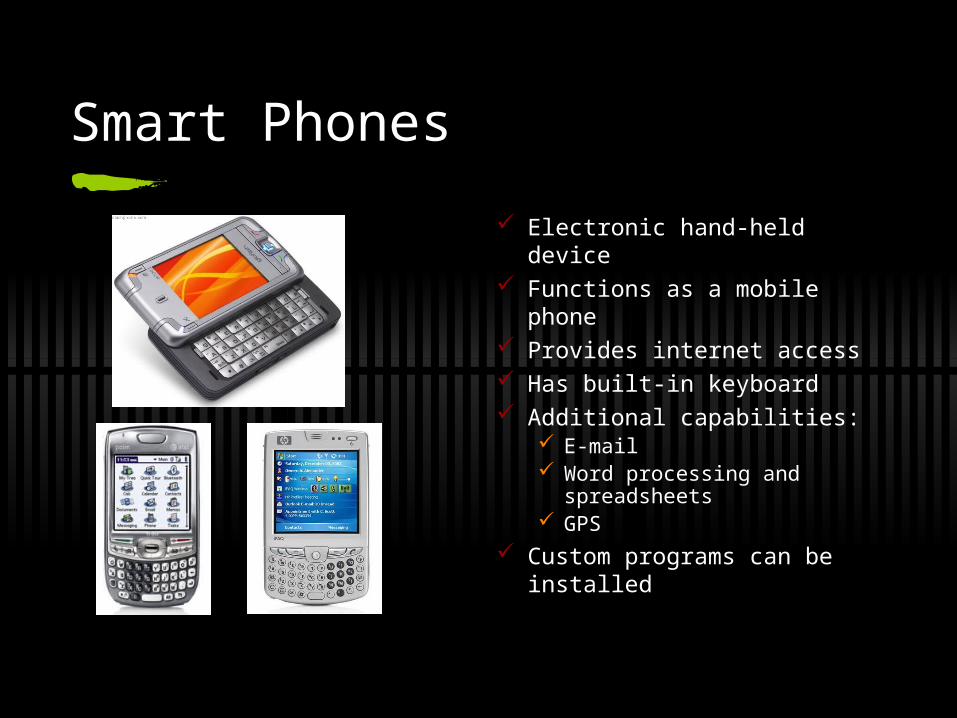
Smart Phones
Electronic hand-held device Functions as a mobile phone Provides internet access Has built-in keyboard Additional capabilities:
E-mail Word processing and
spreadsheets GPS
Custom programs can be installed

Why Phones in Rural Areas ?
Already widely prevalent in developing regions Usage familiar to rural users Powerful enough to be used for computing resources,
rather than just communication – so possible PC replacement for vertical tasks
Suitable for rural areas: low power, robust, cheaper, lower operating cost, use existing networks
Integrated features: camera, GPS, audio Appropriate for use across multiple households

Rural Data Collection Problems
Data frequently missing or incorrect or contradictory. E.g. sex is male but pregnant is yes on health form – very hard to validate after the fact
Forms are very long and frequently incompletely filled – questions are not prioritized if partially filled
Data collected not rich enough – no audio, pictures, GPS without specialized hardware (and also not integrated)

What Can Smartphones Offer ? (1)
Immediate Validation Correct data upon entry, and also crosscheck with other fields if
dependencies exist
Dynamic Forms Reduce burden on health worker by asking only relevant
question based on previous answers, thus reducing chances of errors
Also makes partially filled forms more useful
Richer Data collection Photos, audio input, GPS (entire medical record possible)

What Can Smartphones Offer ? (2)
Auditability Audio samples can be used to double-check responses
Transparency Generating reports of and viewing system-wide statistics and data
Operation in disconnected areas Use only for computation, communication not necessary for collecting
data on the field
Synchronization of data When connectivity is available, upload to central server over the
cellphone network either through multiple SMSes, or data packets over GPRS, eVDO, etc.
Expected Results
Increased data accuracy Improved data timeliness Reduction of burden on healthworkers Reduction of the number of times surveyors
have to be re-sent back into the field to redo surveys because of errors
Better organization of data

Framing the questions
Be reflexive - question what you think you know and ask open-ended questions
Observe - find out about their current practices
Identifying Pain Points
What are the current processes? What do health workers do on a day to day basis? What are the data collection and information management practices?
Who are the key players? Is there a local “champion” and local collaborators? Who is using health information?
What infrastructure is available? Do the health workers have fixed line or mobile phones? How do they communicate with their superiors and subordinates? How is information relayed using current infrastructure? What communications infrastructure is available but not being leveraged?
Metrics What metrics are important to the community? How do they currently evaluate their own successes?

MOHUHIN
(Kampala)
UHIN Deployment(Rakai District)
OBA Uganda(Mbarara District)
Health Centers(Nakaseke District)
Health Clinic Visits

Framing the Context: Nakaseke
Infrastructure
Health Centers
Data Reporting
Mobile Phone Usage

Poor road infrastructure makes it difficult (and expensive) to travel between the health clinics and the hospital

Hospitals and upper-level health centers often have co-located water pumps for the community

Public health campaigns are carried out through radio and posters like these

HCIV

HCIII

HCII

The Ministry of Health mandates monthly and weekly reporting of outpatient statistics

This district hospital keeps all of the HMIS forms from each of the health centers in its district here

Creating the reports…
Data is collated from hand-written patient ledgers (sometimes exercise books)
Forms are completed in triplicate
Submitted within 3 days of the end of the month
Hand delivered to the District hospital
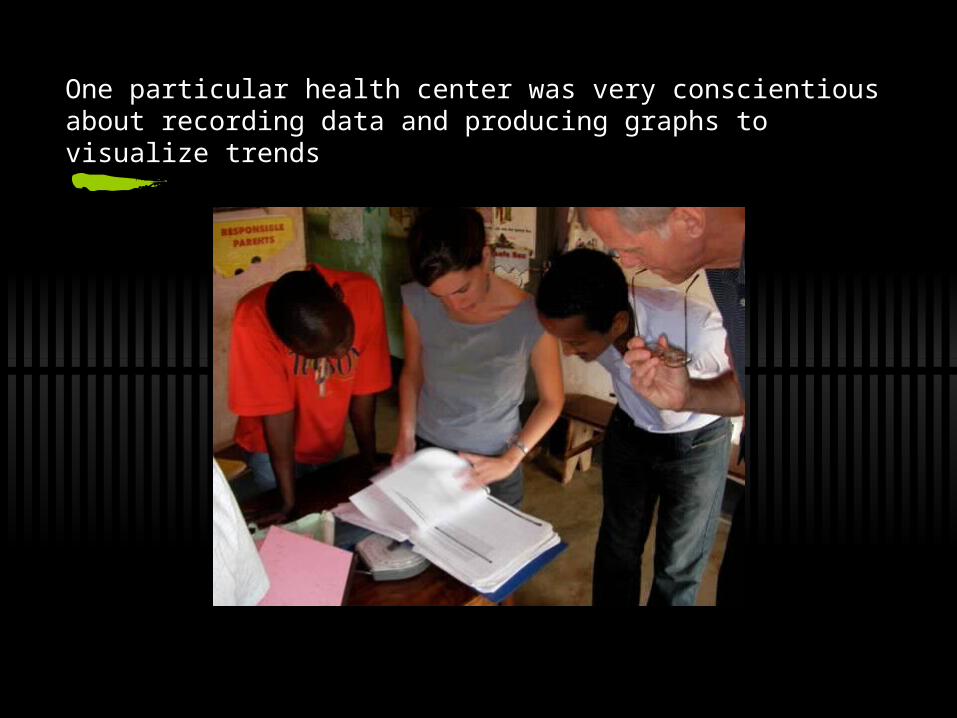
One particular health center was very conscientious about recording data and producing graphs to visualize trends

Aggregating Data

Mobile phone use in HCs
Every health center has at least one
personal mobile phone
Innovative charging solutions
Current Uses
Emergency reporting
Submitting weekly HMIS forms
Checking salary and drug order status
Requesting transportation
Clinical consultations
securityairtime
network coverage

Choosing a smartphone…
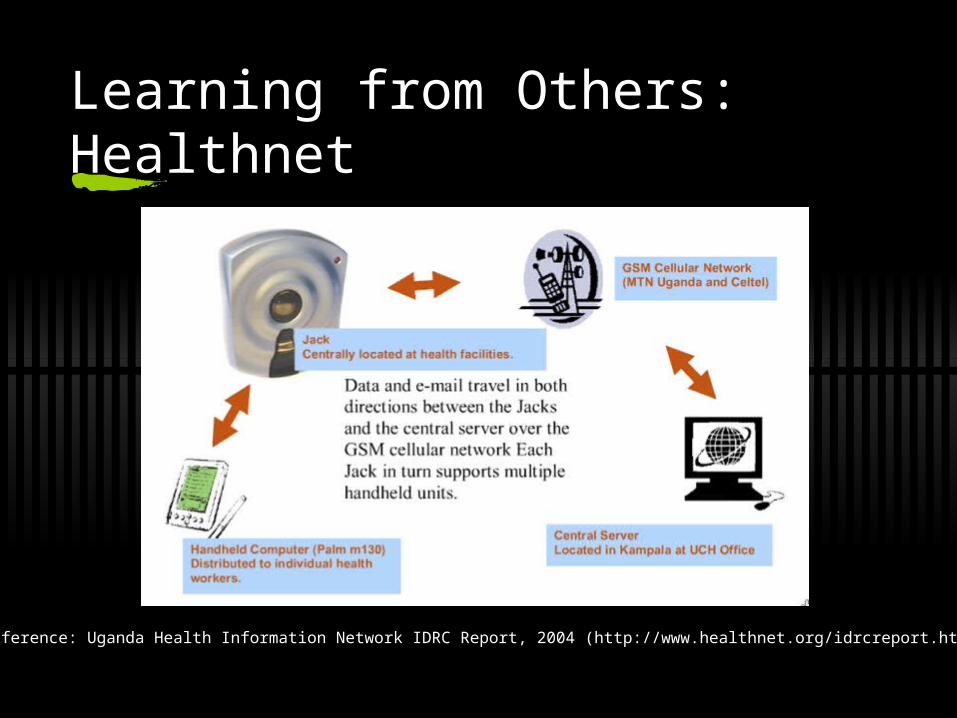
Learning from Others: Healthnet
Reference: Uganda Health Information Network IDRC Report, 2004 (http://www.healthnet.org/idrcreport.html)

A project champion

Report Generation

Paper and Digital Data

“Sometimes I use it as a torch”

Power Issues
Power shortage
Accessibility of relay points
Ownership
Existing Hierarchies
Duplicate Tasking

Appropriatable Technology

NakasekeDistrict Hospital
Semuto HCIV
HCIII HCIII
HCII HCII
Ngoma HCIV
HCIII
HCII
HCIII
HCII
smartphone
smartphone + pdas
MoH
computers + broadband
computer + smartphone
or paper
Lessons Learned

Marie Stopes International Uganda (MSI-U) & Microcare Insurance Ltd.
Community distributors(44 at start)
Clients(+350 per month)
Clinics(16 at start)
Submit claims
Pay service provider
Sell vouchers
Submit voucher to provider
Send vouchers
Record voucher
sales data
Provide STI diagnosis and
treatment Paycash
avg 30 days
max 60 days
avg 15 days
max 45 days

Structured Facility Survey
Conducted by Richard Lowe as part of a separate evaluation project
Providers vary greatly:Facility+Infrastructure DifferencesNumber of ClientsDistance from Mbarara

Part of the process
11/12 Complete claims forms during patient consultation
Timely processing7 days: 2/1214-15 days: 7/1230 days: 2/12
4/12 have computer training
12/12 own a mobile phone

Struggling to Participate
Providers travel up to 3.5 hours to submit claim forms
Fewer clients --> Infrequent Submission
6/12 providers claim that delays in payment interferes with ability to serve patients
4/12 don’t know how many claims have been rejected. 3 have not gotten feedback

Paper vs Digital
Paper is a powerless backup
Authentication using physical artifacts
Flexibility
client
fingerprint
voucherbarcode
clinicstamp
signatures

Open Questions
Pushing verification to the client Eliminate simple errors Biometrics (e.g. fingerprint, photo) ?
Paper and Digital Is there a low cost printing solution? Can we make the digital process advantageous for all parties?
Training and Usability Power Privacy and Information Security Sustainability, Scalability

Execution
Co-design and Co-deploy Local collaboration is key to the sustainability and appropriate
design of the system Collaborating with Mbarara University to integrate solar power into
health centers Development
Leverage computer scientists at Mbarara and Makarere Develop SmartForms in collaboration with people who will be using
them: records officers, nursing assistants, in-charges Training
Develop training plan and information practices with local stakeholders
Specialized training for key Handoff of Maintenance integrated early in the project

Acknowledgements
Thanks to all of the Blum East Africa Fellows, especially Katrina, Mallory, Simon, and Admas for letting me observe and participate in their project
Thanks to Professors Kristi Raube, Sandra Dratler, and Eric Brewer for faciliating this research
Thanks to Ben Bellows, Richard Lowe, Francis Somerwell, and all others at MSIU and Microcare
Thanks to the Blum Center for Developing Regions for inviting me to speak and financing this research
Related Documents
![MHO TESTING TECHNIQUES AND MATH [Read-Only] GUIDE Why have a MHO unit testing techniques and math lecture? Simplified explanation of a MHO unit Ohms law & phase to phase (ph-ph) MHO](https://static.cupdf.com/doc/110x72/5ac257cd7f8b9ad73f8df4fe/mho-testing-techniques-and-math-read-only-guide-why-have-a-mho-unit-testing-techniques.jpg)










