PII S0360-3016(99)00101-7 CLINICAL INVESTIGATION Head and Neck SMART (SIMULTANEOUS MODULATED ACCELERATED RADIATION THERAPY) BOOST: A NEW ACCELERATED FRACTIONATION SCHEDULE FOR THE TREATMENT OF HEAD AND NECK CANCER WITH INTENSITY MODULATED RADIOTHERAPY E. BRIAN BUTLER, M.D.,* BIN S. TEH, M.D.,* WALTER H. GRANT, III, PH.D.,* BARRY M. UHL, M.D.,* RONALD B. KUPPERSMITH, M.D., ² J. KAM CHIU, M.D.,* DONALD T. DONOVAN, M.D., ² AND SHIAO Y. WOO, M.D.* *Department of Radiation Oncology, Baylor College of Medicine, Houston, TX, , USA and ² The Methodist Hospital and The Bobby R. Alford Department of Otorhinolaryngology and Communicative Sciences, Houston, TX Purpose: To report the initial experience in the definitive treatment of head and neck carcinomas using SMART (Simultaneous Modulated Accelerated Radiation Therapy) boost technique. Radiation was delivered via IMRT (Intensity Modulated Radiotherapy). The following parameters were evaluated: acute toxicity, initial tumor response, clinical feasibility, dosimetry and cost. Methods and Materials: Between January 1996 and December 1997, 20 patients with primary head and neck carcinomas were treated with SMART boost technique. The treatment fields encompassed two simultaneous targets. The primary target included palpable and visible disease sites. The secondary target included regions at risk for microscopic disease. Daily fractions of 2.4 Gy and 2 Gy were prescribed and delivered to the primary and secondary targets to a total dose of 60 Gy and 50 Gy, respectively. Lower neck nodes were treated with a single conventional anterior portal. This fractionation schedule was completed in 5 weeks with 5 daily fractions weekly. Toxicity was evaluated by RTOG acute toxicity grading criteria, evidence of infection at immobilization screw sites, subjective salivary function, weight loss, and the need for treatment split. Mean follow-up was 15.2 months. Initial tumor response was assessed by clinical and radiographical examinations. Clinical feasibility was evalu- ated by the criteria: time to treat patient, immobilization, and treatment planning and QA time. In dosimetry, we evaluated the mean doses of both targets and normal tissues and percent targets’ volume below goal. To evaluate cost, Medicare allowable charge for SMART boost was compared to those of conventional fractionated and accelerated radiotherapy. Results: Acute toxicity: None of the patients had a screw site infection and all patients healed well after completion of radiotherapy. Sixteen of 20 patients (80%) completed the treatment within 40 days without any split. Sixteen patients (80%) had RTOG Grade 3 mucositis while 10 patients (50%) had Grade 3 pharyngitis. Three of 20 patients (15%) had weight loss greater than 10% of their pretreatment weight. Ten patients (50%) required intravenous fluids, tube feeding or both. Nine patients (45%) reported moderate xerostomia with significant relief reported within 6 months. Initial tumor response: 19 patients (95%) had complete response (CR) while one had partial response (PR). The patient with PR had stable disease on imaging at 12 months follow-up. Two patients were found to have lung metastases at 2 months and 5 months follow-up. To date, there have been two local recurrences in the complete responders. Both patients had nasopharyngeal primary; one was retreated with radioactive Cesium-137 implant and the other died from the disease. Clinical feasibility: The average treatment time for a three-arc treatment was 17.5 minutes and 2.5 minutes for each additional arc. Eleven patients (55%) had four-arc treatment while six patients (30%) had five-arc treatment and three patients (15%) had three-arc treatment. Immobilization was reproducible within less than 2 mm. The treatment planning, QA and documentation prior to treatment averaged 2 days. Dosimetry: The mean doses to the primary and secondary targets were 64.4 Gy and 54.4 Gy, respectively; 8.9% of the primary target volume and 11.6% of the secondary target volume were below prescribed dose goal. The mean dose delivered to the mandible was 30 Gy, spinal cord 17 Gy, ipsilateral parotid 23 Gy, and contralateral parotid 21 Gy. Cost: Total Medicare allowable charge for SMART boost was $7000 compared to $8600 (conventional ) and $9400 (accelerated fractionation). Conclusions: SMART boost technique is an accelerated radiotherapy scheme that can be delivered with acceptable toxicity. It allows parotid sparing as evidenced both clinically and by dosimetry. Initial tumor response has been encouraging. It is clinically feasible and cost saving. A larger population of patients and a long-term follow-up are warranted to evaluate ultimate tumor control and late toxicity. © 1999 Elsevier Science Inc. SMART boost, Intensity modulated radiotherapy, Head and neck carcinoma. Int. J. Radiation Oncology Biol. Phys., Vol. 45, No. 1, pp. 21–32, 1999 Copyright © 1999 Elsevier Science Inc. Printed in the USA. All rights reserved 0360-3016/99/$–see front matter 21

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PII S0360-3016(99)00101-7
CLINICAL INVESTIGATION Head and Neck
SMART (SIMULTANEOUS MODULATED ACCELERATED RADIATIONTHERAPY) BOOST: A NEW ACCELERATED FRACTIONATION SCHEDULEFOR THE TREATMENT OF HEAD AND NECK CANCER WITH INTENSITY
MODULATED RADIOTHERAPY
E. BRIAN BUTLER, M.D.,* BIN S. TEH, M.D.,* WALTER H. GRANT, III, PH.D.,*BARRY M. UHL, M.D.,* RONALD B. KUPPERSMITH, M.D.,† J. KAM CHIU, M.D.,*
DONALD T. DONOVAN, M.D.,† AND SHIAO Y. WOO, M.D.*
*Department of Radiation Oncology, Baylor College of Medicine, Houston, TX, , USA and†The Methodist Hospital and The BobbyR. Alford Department of Otorhinolaryngology and Communicative Sciences, Houston, TX
Purpose: To report the initial experience in the definitive treatment of head and neck carcinomas using SMART(Simultaneous Modulated Accelerated Radiation Therapy) boost technique. Radiation was delivered via IMRT(Intensity Modulated Radiotherapy). The following parameters were evaluated: acute toxicity, initial tumorresponse, clinical feasibility, dosimetry and cost.Methods and Materials: Between January 1996 and December 1997, 20 patients with primary head and neckcarcinomas were treated with SMART boost technique. The treatment fields encompassed two simultaneoustargets. The primary target included palpable and visible disease sites. The secondary target included regions atrisk for microscopic disease. Daily fractions of 2.4 Gy and 2 Gy were prescribed and delivered to the primary andsecondary targets to a total dose of 60 Gy and 50 Gy, respectively. Lower neck nodes were treated with a singleconventional anterior portal. This fractionation schedule was completed in 5 weeks with 5 daily fractions weekly.Toxicity was evaluated by RTOG acute toxicity grading criteria, evidence of infection at immobilization screwsites, subjective salivary function, weight loss, and the need for treatment split. Mean follow-up was 15.2 months.Initial tumor response was assessed by clinical and radiographical examinations. Clinical feasibility was evalu-ated by the criteria: time to treat patient, immobilization, and treatment planning and QA time. In dosimetry,we evaluated the mean doses of both targets and normal tissues and percent targets’ volume below goal. Toevaluate cost, Medicare allowable charge for SMART boost was compared to those of conventional fractionatedand accelerated radiotherapy.Results: Acute toxicity: None of the patients had a screw site infection and all patients healed well aftercompletion of radiotherapy. Sixteen of 20 patients (80%) completed the treatment within 40 days without anysplit. Sixteen patients (80%) had RTOG Grade 3 mucositis while 10 patients (50%) had Grade 3 pharyngitis.Three of 20 patients (15%) had weight loss greater than 10% of their pretreatment weight. Ten patients (50%)required intravenous fluids, tube feeding or both. Nine patients (45%) reported moderate xerostomia withsignificant relief reported within 6 months. Initial tumor response: 19 patients (95%) had complete response (CR)while one had partial response (PR). The patient with PR had stable disease on imaging at 12 months follow-up.Two patients were found to have lung metastases at 2 months and 5 months follow-up. To date, there have beentwo local recurrences in the complete responders. Both patients had nasopharyngeal primary; one was retreatedwith radioactive Cesium-137 implant and the other died from the disease. Clinical feasibility: The averagetreatment time for a three-arc treatment was 17.5 minutes and 2.5 minutes for each additional arc. Elevenpatients (55%) had four-arc treatment while six patients (30%) had five-arc treatment and three patients (15%)had three-arc treatment. Immobilization was reproducible within less than 2 mm. The treatment planning, QAand documentation prior to treatment averaged 2 days. Dosimetry: The mean doses to the primary andsecondary targets were 64.4 Gy and 54.4 Gy, respectively; 8.9% of the primary target volume and 11.6% of thesecondary target volume were below prescribed dose goal. The mean dose delivered to the mandible was 30 Gy,spinal cord 17 Gy, ipsilateral parotid 23 Gy, and contralateral parotid 21 Gy. Cost: Total Medicare allowablecharge for SMART boost was $7000 compared to $8600 (conventional ) and $9400 (accelerated fractionation).Conclusions: SMART boost technique is an accelerated radiotherapy scheme that can be delivered withacceptable toxicity. It allows parotid sparing as evidenced both clinically and by dosimetry. Initial tumorresponse has been encouraging. It is clinically feasible and cost saving. A larger population of patients and along-term follow-up are warranted to evaluate ultimate tumor control and late toxicity. © 1999 Elsevier ScienceInc.
SMART boost, Intensity modulated radiotherapy, Head and neck carcinoma.
Int. J. Radiation Oncology Biol. Phys., Vol. 45, No. 1, pp. 21–32, 1999Copyright © 1999 Elsevier Science Inc.Printed in the USA. All rights reserved
0360-3016/99/$–see front matter
21

INTRODUCTION
Accelerated repopulation of tumor clonogens during con-ventional fractionated radiotherapy has been recognized asan important cause of treatment failure in head and neckcancers, especially if the overall treatment time is pro-longed. Both laboratory and clinical data (1–3) supportedthis hypothesis. The reduction of overall treatment time hasthe potential for improving tumor control by minimizingtumor clonogen regeneration. Various purely acceleratedtreatment schedules have been used,e.g., Polish Trial(CAIR) (4), Danish Trial (DAHANCA) (5), VancouverTrial (6), and Concomitant Boost (7). These trials haveshown improved tumor control but also increased treatment-related toxicity.
Simultaneous Modulated Accelerated Radiation Therapy(SMART) boost technique is a new fractionation schemeinitiated at the Baylor College of Medicine in March 1994.Compared to other accelerated fractionation schemes,which involve more than five fractions a week, the SMARTboost technique allows one treatment per day, five fractionsper week for a total of 5 weeks. It delivers a larger fraction(2.4 Gy) to the primary target (palpable and visible disease)while delivering a conventional fraction (2 Gy) to the sec-ondary target (regions at risk for microscopic disease). It isan accelerated form of radiotherapy as the treatment iscompleted in 5 weeks. We report our initial experience inthe definitive treatment of head and neck cancers with theSMART boost technique. This article will focus on acutetoxicity, initial tumor response, clinical feasibility, dosime-try, and cost.
METHODS AND MATERIALS
Patient selectionBetween January 1996 and December 1997, 20 patients
with primary head and neck carcinoma were treated with theSMART boost technique at The Methodist Hospital, Hous-ton, Texas. Patient eligibility criteria included:
1. Histologically confirmed squamous cell carcinoma, lym-phoepithelioma, anaplastic carcinoma, and adenoid cys-tic carcinoma in the head and neck regions.
2. No clinical evidence of distant metastasis.3. Karnofsky performance status more than 60.4. No primary surgery for the tumor under study except
biopsy for tissue diagnosis. Patients with a prior malig-nancy (other than non-melanoma skin cancer) were in-eligible, unless the cancer was treated 5 years or moreprior to the current tumor and the patient has remainedfree of disease.
5. No prior radiotherapy of the head and neck.6. Written informed consent.
There were 7 females and 13 males. Median age was 65(range 46–77). There were 17 Caucasians, 1 African-Amer-ican, and 2 Latin-Americans. Follow-up of the patientsranged from 2 months to 36 months with a mean of 15.2months.
The pretreatment staging evaluation included medicalhistory and physical examination by a combined modalitytreatment team. All the patients underwent triple endoscopicexamination under anesthesia. Computerized tomography(CT) of soft tissue neck was done on all patients to assessthe extent of primary tumor and the draining lymphatics.Chest x-rays, complete blood counts and liver function testwere also obtained. The AJCC (American Joint Committeeon Cancer, 4th ed.) TNM tumor classification system (tumorextension [T], nodal involvement [N] and metastatic spread[M]) was used for staging purposes. All patients also un-derwent pretreatment dental evaluation with appropriatecare such as the use of fluoride trays.
Table 1 shows the histology types, the sites of disease andthe TNM stage of the patients. All patients had biopsyproven malignancy with 18 squamous cell carcinomas andtwo adenoid cystic carcinomas (ACC). Twelve patients(60%) had oropharyngeal primary. Three patients (15%)had nasopharyngeal primary and the other three (15%) hadlaryngeal primary. There was one patient with oral cavityprimary and one patient with sphenoid sinus primary. Tenpatients (50%) had Stage IV disease, six patients (30%) hadStage III, and three patients (15%) had Stage II. One patient
Reprint requests to: E. Brian Butler, M.D., Department of Ra-diation Oncology, Baylor College of Medicine, One Baylor Plaza,165B, Houston, TX 77030-3498. Tel: (713) 790-2091 or (713)790-2637; Fax: (713) 793-1300 or (713) 793-1063; E-mail:
[email protected]—The authors wish to thank Shirley Clark for herassistance in the preparation of this manuscript.
Accepted for publication 15 March 1999.
Table 1. Tumor histology, site, and stage
Patient Histology Site Stage
1 SCCA Supraglottic larynx T2N02 SCCA Base of tongue T1N13 SCCA Base of tongue T2N2c4 SCCA Base of tongue T1N35 SCCA Base of tongue T1N2a6 SCCA Nasopharynx T4N07 SCCA Base of tongue T1N38 SCCA Tonsil T2N19 SCCA Tonsil T1N2b
10 SCCA Sphenoid sinus N/A11 SCCA Base of tongue T1N112 SCCA Base of tongue T2N2b13 ACC Soft palate T4N014 SCCA Nasopharynx T3N015 ACC Hard palate T2N016 SCCA Supraglottic larynx T3N2b17 SCCA Glottic larynx T3N018 SCCA Soft palate T3N019 SCCA Soft palate T3N020 SCCA Nasopharynx T3N2a
SCCA 5 squamous cell carcinoma; ACC5 adenoid cysticcarcinoma.
22 I. J. Radiation Oncology● Biology ● Physics Volume 45, Number 1, 1999

had a sphenoid sinus primary for which there was no TNMstaging.
Performing treatment using Peacock systemUtilization of the NOMOS Peacock™ system (NOMOS
Corporation, Sewickley, PA) in the treatment of head andneck malignancies involved a series of steps as previouslyreported (8,9). Briefly, the steps were:
1. Patient had a customized intraoral stent to immobilizethe tongue when necessary.
2. For immobilization purpose, the “Talon” fixation devicewas secured to the skull in the operating room by aneurosurgeon. Under local anesthesia, two twist drillholes were placed through the inner table of the skull.Self-taping screw sockets were threaded into the holesand the Talon secured to the sockets (Fig. 1a).
3. For imaging, a CT scan was performed at 3-mm slices onthe same day the screws were placed. The diagnosticimages were transferred to the Peacock computer forplanning.
4. During treatment planning, targets and avoidance struc-
tures were delineated after review with the ENT sur-geons and neuroradiologists. The primary target wasdetermined from both physical examination and imagingstudies. The secondary target was determined with theunderstanding of the anatomical compartments in thehead and neck regions and the location of lymph nodeswithin those compartments (10). Doses to targets anddose limitations to avoidance normal structures are thenassigned.
5. After the plan was generated, it was reviewed. Afterapproval of the plan, a film verification cassette (a phan-tom) was set up on the treatment couch and secured to analignment bracket in the same fashion as the patient. Theplan-specific delivery floppy was loaded onto theMIMiC (Multivane Intensity Modulating Collimator)(Fig.1b) control computer and the plan was delivered tothe verification cassette. Quantitative and qualitative as-sessments were made regarding the shape and position ofthe dose distribution in the phantom. The ratio of themeasured dose of the QA plan to that predicted by thetreatment plan should be within 5%. If this is more than5%, the monitor unit setting for the patient treatment isadjusted to deliver the prescribed dose to within 5%.
6. On the day of the first treatment, alignment checks wereperformed on the MIMiC and the room lasers werecalibrated. The alignment box was secured to the bracketand leveled with respect to the room lasers and/orMIMiC. The “crane” couch-indexing device was securedto the treatment couch and correctly aligned.
7. The prescription was entered on the accelerator consoleand treatment initiated. After the first rotation was com-pleted, the therapists entered the treatment room to indexthe couch for the next rotation. Rotations were deliveredin sequence until the fraction was completed.
8. The Talon was removed from the skull screws and stand-offs.
9. The patient was taught how to take care of the screwsites. He/she was also prescribed with prophylactic an-tibiotic during the full course of radiotherapy. On com-pletion of radiotherapy, the screws and standoffs wereremoved from the skull, the scalp wounds covered withsterile gauze and the patient sent home with frequentfollow-up until the scalp wounds were fully closed. Theclosure usually took approximately 5 to 10 days.
SMART boost radiotherapy and dosimetric evaluationRadiation was delivered with a megavoltage linear accel-
erator using 10 MV photons. No electron beam was re-quired. Peacock system delivered IMRT using arc therapy.The beam was intensity modulated by a special collimatorcalled the MIMiC. The MIMiC consists of 40 vanes, each ofwhich was an 8 cm thick tungsten block which projects to a1 3 1 cm2 or 2 3 1 cm2 field at isocenter. There were tworows of 20 vanes each, so an arc can be treated to a 2 cm or4 cm length. (Figs. 2a and 2b). Peacock IMRT systemallowed different doses to be delivered to different targetssimultaneously. The primary target included palpable as
Fig. 1. (a) “Talon” secured to the socket in a patient with head andneck cancer. (b) MIMiC—Multivane Intensity Modulating Colli-mator.
23SMART boost● E. B. BUTLER et al.

well as visible (either on clinical examination or on imag-ing) disease. The secondary target included regions at riskfor microscopic disease such as draining lymphatics orperineural spread via cranial nerves. The dose prescribedand delivered to the primary target was 2.4 Gy, while 2 Gywas delivered to the secondary target simultaneously eachday. Lower neck nodes were treated with a single anteriorbeam split portal using 6 MV photons to Dmax. A typicalIMRT field had 2 mm divergence into the lower neck field.A junctional block was used with this field. This field wasmatched to the inferior border of the lowest arc treated withIMRT. All fields must be treated on each treatment day. Allpatients were treated 5 days per week to a total of 25fractions over 5 weeks. Primary target was prescribed to 60Gy while both secondary target and lower neck nodes wereprescribed 50 Gy.
Detailed evaluation of dosimetry was performed prior tocommencement of treatment. Each axial image was evalu-ated for dosimetric coverage of the tumor and the anatom-ical compartments as well as any over-dosage of normaltissues. Mean doses to the targets and the normal tissueswere reviewed. Adequate coverage of the targets withoutoverdosage of normal tissues was used as a criteria foracceptability of the treatment plan. Homogeneity was notused as a criterion for acceptability.
Computer-controlled conformal avoidance is a conceptthat attempts to limit the deposition of radiation to theparticular normal structure. With IMRT, we were able toapply this concept to all the critical surrounding structureswith the prescribed threshold limit. Generally, the limitingdoses for the critical structures at our institution were shownin Table 2. Serial organs,e.g., spinal cord, were usuallyweighted more importantly than parallel organs,e.g., pa-
rotid glands. Sometimes, some serial structures wereweighted even more than targets (e.g., in the case of opticchiasm if a patient could not accept decreased visual acuityas treatment toxicity). The limiting doses to the parotidsdepended on the location of the tumors. Twenty-five Gy waslimited to each parotid for midline primary tumor. Forunilateral tumor ipsilateral and contralateral parotids wereweighted differently.
All patients received SMART boost radiotherapy. Gen-erally three to five arcs were used depending on the size andsite of primary, the draining lymphatics to be covered in thetreatment portal and the primary location of the tumor. Allpatients had Peacock Talon placed for immobilization pur-poses.
Toxicities evaluationAll patients were seen weekly during treatment for as-
sessment and management of treatment related toxicity.
Fig. 2. (a) MIMiC consisting of 40 vanes, which projects to a 13 1 cm2 at isocenter. The arc treated is 2 cm length.(b) MIMiC consisting of 40 vanes, which projects to a 23 1 cm2 at isocenter. The arc treated is 4 cm length.
Table 2. Radiotherapy dose limits to various normal structures
Normal structuresDose limits
(Gy)
Spinal cord 40Mandible 58Lens 12Lacrimal glands 30Optic nerves 45Brain stem 50Optic chiasm 45Retina 45Parotid (Ipsilateral) 35Parotid (Contralateral) 25
24 I. J. Radiation Oncology● Biology ● Physics Volume 45, Number 1, 1999
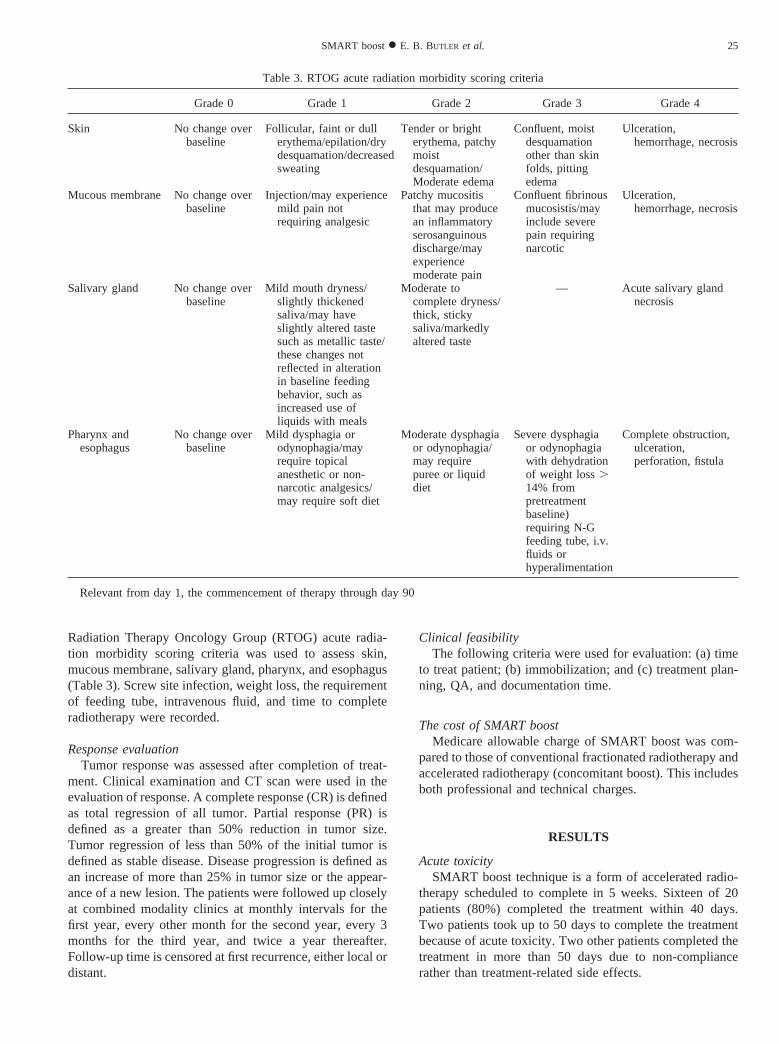
Radiation Therapy Oncology Group (RTOG) acute radia-tion morbidity scoring criteria was used to assess skin,mucous membrane, salivary gland, pharynx, and esophagus(Table 3). Screw site infection, weight loss, the requirementof feeding tube, intravenous fluid, and time to completeradiotherapy were recorded.
Response evaluationTumor response was assessed after completion of treat-
ment. Clinical examination and CT scan were used in theevaluation of response. A complete response (CR) is definedas total regression of all tumor. Partial response (PR) isdefined as a greater than 50% reduction in tumor size.Tumor regression of less than 50% of the initial tumor isdefined as stable disease. Disease progression is defined asan increase of more than 25% in tumor size or the appear-ance of a new lesion. The patients were followed up closelyat combined modality clinics at monthly intervals for thefirst year, every other month for the second year, every 3months for the third year, and twice a year thereafter.Follow-up time is censored at first recurrence, either local ordistant.
Clinical feasibilityThe following criteria were used for evaluation: (a) time
to treat patient; (b) immobilization; and (c) treatment plan-ning, QA, and documentation time.
The cost of SMART boostMedicare allowable charge of SMART boost was com-
pared to those of conventional fractionated radiotherapy andaccelerated radiotherapy (concomitant boost). This includesboth professional and technical charges.
RESULTS
Acute toxicitySMART boost technique is a form of accelerated radio-
therapy scheduled to complete in 5 weeks. Sixteen of 20patients (80%) completed the treatment within 40 days.Two patients took up to 50 days to complete the treatmentbecause of acute toxicity. Two other patients completed thetreatment in more than 50 days due to non-compliancerather than treatment-related side effects.
Table 3. RTOG acute radiation morbidity scoring criteria
Grade 0 Grade 1 Grade 2 Grade 3 Grade 4
Skin No change overbaseline
Follicular, faint or dullerythema/epilation/drydesquamation/decreasedsweating
Tender or brighterythema, patchymoistdesquamation/Moderate edema
Confluent, moistdesquamationother than skinfolds, pittingedema
Ulceration,hemorrhage, necrosis
Mucous membrane No change overbaseline
Injection/may experiencemild pain notrequiring analgesic
Patchy mucositisthat may producean inflammatoryserosanguinousdischarge/mayexperiencemoderate pain
Confluent fibrinousmucosistis/mayinclude severepain requiringnarcotic
Ulceration,hemorrhage, necrosis
Salivary gland No change overbaseline
Mild mouth dryness/slightly thickenedsaliva/may haveslightly altered tastesuch as metallic taste/these changes notreflected in alterationin baseline feedingbehavior, such asincreased use ofliquids with meals
Moderate tocomplete dryness/thick, stickysaliva/markedlyaltered taste
— Acute salivary glandnecrosis
Pharynx andesophagus
No change overbaseline
Mild dysphagia orodynophagia/mayrequire topicalanesthetic or non-narcotic analgesics/may require soft diet
Moderate dysphagiaor odynophagia/may requirepuree or liquiddiet
Severe dysphagiaor odynophagiawith dehydrationof weight loss.14% frompretreatmentbaseline)requiring N-Gfeeding tube, i.v.fluids orhyperalimentation
Complete obstruction,ulceration,perforation, fistula
Relevant from day 1, the commencement of therapy through day 90
25SMART boost● E. B. BUTLER et al.
Peacock screw sites were evaluated during treatment andat follow-ups. All patients were on prophylactic antibiotics.None of the patients had a screw site infection. All patientsfound the care of the screw sites to be manageable and easy.They found the placement of the head screws and the Talonduring radiotherapy to be tolerable and without discomfort.All patients had no problem with healing of the screw sitesafter completion of treatment.
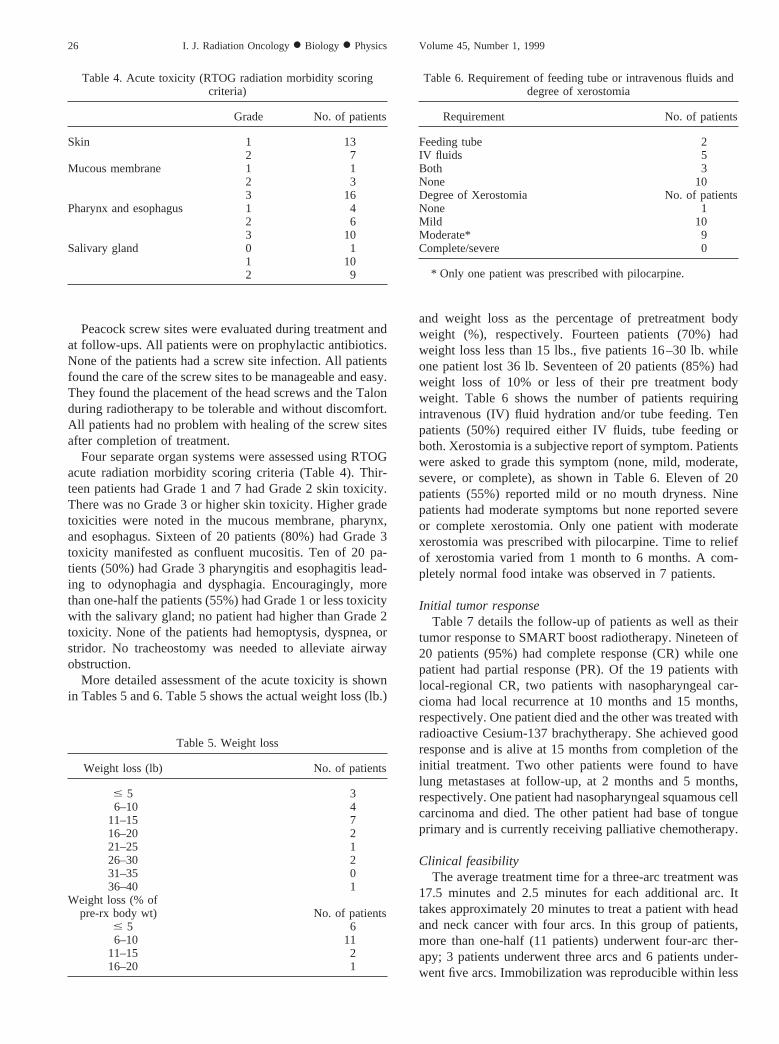
Four separate organ systems were assessed using RTOGacute radiation morbidity scoring criteria (Table 4). Thir-teen patients had Grade 1 and 7 had Grade 2 skin toxicity.There was no Grade 3 or higher skin toxicity. Higher gradetoxicities were noted in the mucous membrane, pharynx,and esophagus. Sixteen of 20 patients (80%) had Grade 3toxicity manifested as confluent mucositis. Ten of 20 pa-tients (50%) had Grade 3 pharyngitis and esophagitis lead-ing to odynophagia and dysphagia. Encouragingly, morethan one-half the patients (55%) had Grade 1 or less toxicitywith the salivary gland; no patient had higher than Grade 2toxicity. None of the patients had hemoptysis, dyspnea, orstridor. No tracheostomy was needed to alleviate airwayobstruction.
More detailed assessment of the acute toxicity is shownin Tables 5 and 6. Table 5 shows the actual weight loss (lb.)
and weight loss as the percentage of pretreatment bodyweight (%), respectively. Fourteen patients (70%) hadweight loss less than 15 lbs., five patients 16–30 lb. whileone patient lost 36 lb. Seventeen of 20 patients (85%) hadweight loss of 10% or less of their pre treatment bodyweight. Table 6 shows the number of patients requiringintravenous (IV) fluid hydration and/or tube feeding. Tenpatients (50%) required either IV fluids, tube feeding orboth. Xerostomia is a subjective report of symptom. Patientswere asked to grade this symptom (none, mild, moderate,severe, or complete), as shown in Table 6. Eleven of 20patients (55%) reported mild or no mouth dryness. Ninepatients had moderate symptoms but none reported severeor complete xerostomia. Only one patient with moderatexerostomia was prescribed with pilocarpine. Time to reliefof xerostomia varied from 1 month to 6 months. A com-pletely normal food intake was observed in 7 patients.
Initial tumor responseTable 7 details the follow-up of patients as well as their
tumor response to SMART boost radiotherapy. Nineteen of20 patients (95%) had complete response (CR) while onepatient had partial response (PR). Of the 19 patients withlocal-regional CR, two patients with nasopharyngeal car-cioma had local recurrence at 10 months and 15 months,respectively. One patient died and the other was treated withradioactive Cesium-137 brachytherapy. She achieved goodresponse and is alive at 15 months from completion of theinitial treatment. Two other patients were found to havelung metastases at follow-up, at 2 months and 5 months,respectively. One patient had nasopharyngeal squamous cellcarcinoma and died. The other patient had base of tongueprimary and is currently receiving palliative chemotherapy.
Clinical feasibilityThe average treatment time for a three-arc treatment was
17.5 minutes and 2.5 minutes for each additional arc. Ittakes approximately 20 minutes to treat a patient with headand neck cancer with four arcs. In this group of patients,more than one-half (11 patients) underwent four-arc ther-apy; 3 patients underwent three arcs and 6 patients under-went five arcs. Immobilization was reproducible within less
Table 4. Acute toxicity (RTOG radiation morbidity scoringcriteria)
Grade No. of patients
Skin 1 132 7
Mucous membrane 1 12 33 16
Pharynx and esophagus 1 42 63 10
Salivary gland 0 11 102 9
Table 5. Weight loss
Weight loss (lb) No. of patients
# 5 36–10 4
11–15 716–20 221–25 126–30 231–35 036–40 1
Weight loss (% ofpre-rx body wt) No. of patients
# 5 66–10 11
11–15 216–20 1
Table 6. Requirement of feeding tube or intravenous fluids anddegree of xerostomia
Requirement No. of patients
Feeding tube 2IV fluids 5Both 3None 10Degree of Xerostomia No. of patientsNone 1Mild 10Moderate* 9Complete/severe 0
* Only one patient was prescribed with pilocarpine.
26 I. J. Radiation Oncology● Biology ● Physics Volume 45, Number 1, 1999

than 2 mm. Treatment planning, QA, and documentationprior to treatment averaged 2 days.
Dosimetric evaluationAll axial images were reviewed for coverage and avoid-
ance. Figure 3a shows an example of axial image of a baseof tongue treatment plan. The primary target or tumorvolume (red) is treated at 2.4 Gy/fraction. The secondarytarget or microscopic disease (purple) is treated at 2 Gy/
fraction concurrently. In addition to the differential targetdoses, there is also conformal avoidance of the parotidglands and the spinal cord as shown on both the treatmentplan (Fig. 3a) and the quality control (QC) film (Fig. 3b).When treating patients with nasopharyngeal SCCA there isconformal avoidance of the orbits, retina, optic chiasm,optic nerves, lens, and spinal cord. Table 8 shows the dosesprescribed and delivered to primary and secondary targets.The primary target was prescribed to a total dose of 60 Gy
Fig. 3. (a) Axial treatment plan of a patient with base of tongue primary. Note the two separate targets: (i) primary (red)and (ii) secondary (purple). Also note the conformal avoidance of spinal cord (turquoise), mandible (light green), andparotid glands, ipsilateral (green), and contralateral (dark green). Also note isodose line: dark blue—60 Gy; yellow—50Gy; red—45 Gy; green—30 Gy. (b) Quality control film showing the sparing of parotid glands and spinal cord.■—Primary target;Œ—Secondary target;r—Spinal cord;F—Ipsilateral parotid gland;✚—Contralateral parotidgland. Note: The degree of optical density is proportional to the amount of radiation dose received in that particular area.
Table 7. Follow-up1 tumor response
Patient Follow-up Tumor response Patient Follow-up Tumor response
1 13 months CR 11 16 months CR2 12 months CR 12 5 months Local CR; lung metastases3 18 months CR 13 16 months CR4 12 months CR 14 10 months Local recurrence5 25 months CR 15 36 months CR6 2 months Local CR; lung metastases 16 17 months CR7 12 months CR 17 16 months CR8 12 months CR 18 28 months CR9 14 months CR 19 13 months CR
10 12 months PR 20 15 months Local recurrence
Range5 2 to 36 months; mean5 15.2 months; median5 13.5 months.
27SMART boost● E. B. BUTLER et al.
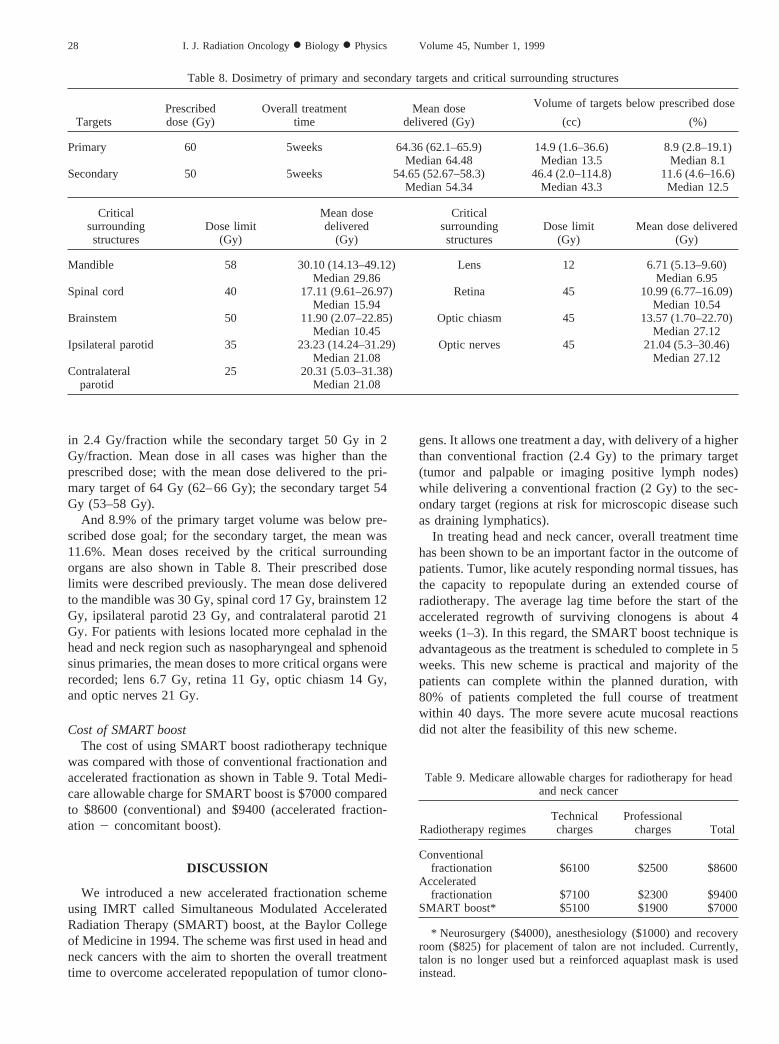
in 2.4 Gy/fraction while the secondary target 50 Gy in 2Gy/fraction. Mean dose in all cases was higher than theprescribed dose; with the mean dose delivered to the pri-mary target of 64 Gy (62–66 Gy); the secondary target 54Gy (53–58 Gy).
And 8.9% of the primary target volume was below pre-scribed dose goal; for the secondary target, the mean was11.6%. Mean doses received by the critical surroundingorgans are also shown in Table 8. Their prescribed doselimits were described previously. The mean dose deliveredto the mandible was 30 Gy, spinal cord 17 Gy, brainstem 12Gy, ipsilateral parotid 23 Gy, and contralateral parotid 21Gy. For patients with lesions located more cephalad in thehead and neck region such as nasopharyngeal and sphenoidsinus primaries, the mean doses to more critical organs wererecorded; lens 6.7 Gy, retina 11 Gy, optic chiasm 14 Gy,and optic nerves 21 Gy.
Cost of SMART boostThe cost of using SMART boost radiotherapy technique
was compared with those of conventional fractionation andaccelerated fractionation as shown in Table 9. Total Medi-care allowable charge for SMART boost is $7000 comparedto $8600 (conventional) and $9400 (accelerated fraction-ation 2 concomitant boost).
DISCUSSION
We introduced a new accelerated fractionation schemeusing IMRT called Simultaneous Modulated AcceleratedRadiation Therapy (SMART) boost, at the Baylor Collegeof Medicine in 1994. The scheme was first used in head andneck cancers with the aim to shorten the overall treatmenttime to overcome accelerated repopulation of tumor clono-
gens. It allows one treatment a day, with delivery of a higherthan conventional fraction (2.4 Gy) to the primary target(tumor and palpable or imaging positive lymph nodes)while delivering a conventional fraction (2 Gy) to the sec-ondary target (regions at risk for microscopic disease suchas draining lymphatics).
In treating head and neck cancer, overall treatment timehas been shown to be an important factor in the outcome ofpatients. Tumor, like acutely responding normal tissues, hasthe capacity to repopulate during an extended course ofradiotherapy. The average lag time before the start of theaccelerated regrowth of surviving clonogens is about 4weeks (1–3). In this regard, the SMART boost technique isadvantageous as the treatment is scheduled to complete in 5weeks. This new scheme is practical and majority of thepatients can complete within the planned duration, with80% of patients completed the full course of treatmentwithin 40 days. The more severe acute mucosal reactionsdid not alter the feasibility of this new scheme.
Table 8. Dosimetry of primary and secondary targets and critical surrounding structures
TargetsPrescribeddose (Gy)
Overall treatmenttime
Mean dosedelivered (Gy)
Volume of targets below prescribed dose
(cc) (%)
Primary 60 5weeks 64.36 (62.1–65.9) 14.9 (1.6–36.6) 8.9 (2.8–19.1)Median 64.48 Median 13.5 Median 8.1
Secondary 50 5weeks 54.65 (52.67–58.3) 46.4 (2.0–114.8) 11.6 (4.6–16.6)Median 54.34 Median 43.3 Median 12.5
Criticalsurroundingstructures
Dose limit(Gy)
Mean dosedelivered
(Gy)
Criticalsurroundingstructures
Dose limit(Gy)
Mean dose delivered(Gy)
Mandible 58 30.10 (14.13–49.12) Lens 12 6.71 (5.13–9.60)Median 29.86 Median 6.95
Spinal cord 40 17.11 (9.61–26.97) Retina 45 10.99 (6.77–16.09)Median 15.94 Median 10.54
Brainstem 50 11.90 (2.07–22.85) Optic chiasm 45 13.57 (1.70–22.70)Median 10.45 Median 27.12
Ipsilateral parotid 35 23.23 (14.24–31.29) Optic nerves 45 21.04 (5.3–30.46)Median 21.08 Median 27.12
Contralateralparotid
25 20.31 (5.03–31.38)Median 21.08
Table 9. Medicare allowable charges for radiotherapy for headand neck cancer
Radiotherapy regimesTechnicalcharges
Professionalcharges Total
Conventionalfractionation $6100 $2500 $8600
Acceleratedfractionation $7100 $2300 $9400
SMART boost* $5100 $1900 $7000
* Neurosurgery ($4000), anesthesiology ($1000) and recoveryroom ($825) for placement of talon are not included. Currently,talon is no longer used but a reinforced aquaplast mask is usedinstead.
28 I. J. Radiation Oncology● Biology ● Physics Volume 45, Number 1, 1999

SMART boost is a form of accelerated radiotherapy.Although there are many different schemes of acceleratedfractionation, SMART boost is the only scheme that offersone fraction per day and only 5 days per week. In compar-ison, other accelerated fractionation schemes make use ofeither: (a) more than once a day treatment, either throughoutthe full course,e.g., in Vancouver trials, two fractions of 2Gy/day to a total dose of 66 Gy in 3 weeks or as part of thetreatment regime in MD Anderson concomitant boost, 30fractions of 1.8 Gy over 6 weeks, to which a second (boost)dose of 1.5 Gy is given for the last 12 days (to a reducedvolume), for a total dose of 72 Gy in 6 weeks; (b) once a daytreatment but more than 5 days per week,e.g., in Polishtrials (CAIR), 2 Gy was given 7 days per week to 70 Gy in5 weeks (boost fields were treated on Saturdays and Sun-days); or (c) a combination of (a) and (b),e.g., in Danishtrials (DAHANCA 6 & 7), six fractions of 2 Gy per week,initially 6 days/week, but later with 2 fractions on 1 day.With five single daily fraction per week for a total of 5weeks, the SMART boost technique offers patients and theircaregivers convenience, as well as time and money savings.The heavy workload burden on a very busy linear acceler-ator is lessened when compared to other accelerated frac-tionation schemes.
Despite the vital role played by fractionation in the out-come in radiation oncology, there is no true standard or bestfractionation. Commonly used radiotherapy regimes world-wide involve daily fraction sizes ranging from 1.8 Gy to 3.5Gy, total doses of 50 to 72 Gy, and overall treatmentduration of 3 to 8 weeks. Its variability worldwide is mul-tifactorial including tradition, empiric observations, influ-ence of individual clinicians, socioeconomics, resourceavailability, consideration of morbidity following cure aswell as radiobiology. In the United States, conventionalradiotherapy for head and neck malignancies uses a frac-tionation scheme of 1.8–2 Gy per fraction, five daily frac-tions per week to a total dose of 65–70 Gy. At ChristieHospital, Manchester, England, the standard scheme is 3.4Gy per fraction, five daily fractions per week totaling 55 Gyover approximately 3 weeks (11). The standard scheduleused at Princess Margaret Hospital, Toronto, Canada, is 2.6Gy per fraction, five daily fractions per week to the total of51 Gy over 4 weeks (12). However, similar treatment resultswere achieved with different fraction sizes. The real radio-biological considerations are tumor control and treatmentrelated toxicities. The daily fraction size has more effect andimpact on late responding normal tissues than the earlyresponding tissues. Late responding normal tissues such asspinal cord and optic chiasm with low alpha/beta ratio (theratio of 3 is used) are intolerant of large fraction size. Wechose 2.4 Gy daily fraction size that is very close to thePrincess Margaret Hospital 2.6 Gy; but much lower than 3.4Gy used at Christie Hospital, Manchester, England; 2.4 Gyis used as we plan to complete the full course of treatmentin 5 weeks, the duration required to treat the lymphatics andsubclinical sites with 2 Gy daily fraction size. One majordifference is the irradiated volume. In our SMART boost,
the 2.4 Gy is delivered to the tumor volume itself (like areduced boost field) sparing the late responding normaltissue such as spinal cord. Conventional 2 Gy is maintainedand delivered to the draining lymphatics and other sites atrisk for microscopic disease. Two patients in the study hadACC, which is well known for its propensity for perineuralinvasion. We were able to deliver the desired 2 Gy to theparticular cranial nerve at risk for microscopic disease andyet spare the critical surrounding organ,e.g., brain and opticapparatus.
In fact the late responding normal structures,e.g., spinalcord, are receiving a much lower fraction size (, 2 Gy) asdemonstrated in Table 8 when compared to the conventionalradiotherapy. The highest daily dose to the spinal cord wasonly 1.1 Gy. The SMART boost technique is theoreticallyvery safe. Long-term follow-ups are warranted to evaluatethe long-term toxicity especially of the late respondingtissues,e.g., spinal cord.
In addition, the repair of sub-lethal damage (SLD) isslower in most late responding tissues than in acutely re-sponding tissues. Therefore, a 6-hour interval between dosefractions (with b.i.d. or t.i.d. treatment) is desirable. For acritical structure like the spinal cord, which is characterizedby a relatively slow rate of repair of SLD, the recommendedinterval is at least 8 hours, and it should not be irradiatedmore than twice a day and preferably only once a day. Thesignificance of appropriate length of inter-fractional intervalhas been proven clinically in the earlier CHART trial wherethere was an increased incidence of radiation myelitis whenthe inter-fractional interval was less than 6 hours (13). Incontrast, the SMART boost technique obviates the need ofinter-fractional interval (when patients are treated more thanonce a day) and allows better repair of SLD in the lateresponding tissues. This will ultimately increase the thera-peutic ratio because of the possibility of dose escalation tothe tumor without causing any damage to normal tissues.
We also applied biological equivalent dose (BED) con-cept using alpha/beta to the SMART boost. As shown inTable 8, the mean doses to the primary and secondarytargets were 64 Gy and 54 Gy respectively, slightly higherthan the prescribed 60 Gy and 50 Gy. In terms of BED, thetumor and acutely responding tissues such as mucous mem-brane received approximately 84 Gy (conventional fraction-ation) and 81 Gy (SMART boost). Clinically, a significantproportion of patients treated with SMART boost had Grade3 toxicity in mucous membrane (80%) as well as pharynxand esophagus (50%) as shown in Table 4. Objective acutemucosal reactions were more severe than those reportedwith conventional treatment, which was approximately 50%(14).
Three of 20 patients (15%) had weight loss of more than10% of their pretreatment weight (Table 5). A total of 10patients required either IV fluid for hydration, tube feedingor both during treatment. Five patients required hospitaliza-tion for acute mucositis either during the last week oftreatment or after completion of treatment. All of them,however, recovered well after treatment. The acute mucosi-
29SMART boost● E. B. BUTLER et al.

tis resolved in all cases. All patients had tubes removed afterthe acute mucositis resolved. Radiation induced skin reac-tion is very acceptable in patients treated with SMARTboost. Thirteen patients (65%) had Grade 1 toxicity and 7patients had Grade 2. None of the patients had Grade 3 orhigher skin toxicity. This favorable observation is probablydue to the lower skin dose as electron beam supplement isnot required to the posterior neck (the spinal cord toleranceis not reached).
We recognize the disadvantage of SMART boost and theprice of “speeding” (15), the most significant being theincreased acute mucosal reactions. Active and aggressivesupportive care were carried out such as twice weeklyweighing, patients counseling regarding the importance oforal care and maintaining weight, early IV hydration andearly enteral alimentation as well as hospitalization. Thisapproach may appear to be inconvenient, time consumingand expensive, but certainly has contributed to the clinicalfeasibility of this scheme and the ultimate improved patientcare.
Xerostomia as a result of irradiation during the treatmentof head and neck cancer can be permanent and is wellknown to affect quality of life. Pilocarpine has been shownto have some effect (16). However, the cost, side effects,compliance and degree of effectiveness with the use ofpilocarpine are all real issues. However, if we can conformlow radiation dose (below the tolerance) to the parotidglands, the incidence of xerostomia can be decreased.SMART boost, delivered via IMRT, allows parotid sparingbilaterally in midline lesions, and contra lateral parotidsparing if the ipsilateral lesion is close to ipsilateral parotids.None of the patients in this study reported severe or com-plete xerostomia. Fifty-five percent of the patients reportednone or mild xerostomia while the rest had moderate symp-toms. It is also encouraging to note that all patients reporteda significant relief of symptom within 1 to 6 months post-radiotherapy. Seven patients even claimed that they had acompletely normal food intake. It is of note that only onepatient in this study was prescribed pilocarpine. SMARTboost appears to be able to preserve subjective parotidfunction, which will certainly improve the quality of life ofpatients. More detailed both qualitative and quantitativestudies on salivary function are warranted and underway.An analysis of specific tumor-site related parotid preserva-tion will also be important.
In the treatment of head and neck cancer with IMRT, it isnecessary to understand pathways of spread of disease andcompartments within the head and neck area (10). Thelocation of lymph nodes within defined compartments isfundamental to define the target. A defined margin of 1 cmwould be inadequate for head and neck cancer. One mustdefine margin to provide adequate coverage of a compart-ment. There are many compartments within the head andneck that are pathways of spread of disease of each primarysite. There must be adequate dosimetric coverage of thesepathways of spread of disease and not merely a definedquantitative margin of 1.0 cm around radiographic disease.
This is in contrast to well-defined margin that are utilized intreating other disease sites, (e.g., prostate cancer). Therewas 11.6% of the secondary target that was below the goalof 50 Gy but the target was encompassed by the 45 Gyisodose line (which is thought to be tumoricidal for subclin-ical disease) as shown in Fig. 3a.
Various studies (17) have shown that complete response(CR) after completion of radiotherapy suggests better dis-ease control. It is encouraging to note that 19 out of the 20patients achieved CR after SMART boost. Two patientsfrom this group had local recurrence. Two patients who haddistant (lung) metastases 2 months and 5 months aftercompletion of radiotherapy probably had micro-metastasesinitially. Long-term follow-up is needed to confirm whetherinitial CR will translate into better local regional diseasecontrol.
The SMART boost appears to be an effective and clini-cally feasible tool in modern radiation oncology. In additionto its ability to deliver different doses to different targetssimultaneously, IMRT allows “conformal avoidance” of thecritical structures. In treating head and neck cancers, thereare many normal structures (mandible, parotids, spinal cord,lens, optic chiasm, optic nerves, lacrimal glands, retina,brainstem, temporal lobes, and orbits), which may limit thedelivery of higher dose of radiation to tumors because oftheir disastrous sequelae if their radiation tolerance is ex-ceeded. Table 8 demonstrates that all these normal struc-tures can be kept well under their respective tolerance andyet the delivery of high dose to the tumor and the micro-scopic sites are still possible. The differential weightings areused for the serial and parallel organs. Serial organs such asspinal cord and optic chiasm are weighted significantlymore than the parallel organs such as parotid glands. Some-times, the serial organs were weighted more than the targetsif the patients could not accept the treatment-related toxicitysuch as blindness in the case of optic chiasm adjacent to thetumor. The importance of partial organ volume toleranceneeds to be investigated. More work needs to be done at amore basic radiobiology level as well as a long-term fol-low-up to evaluate its clinical significance especially thelate effects, local regional control, and survival.
The other challenge in the use of IMRT to treat head andneck cancers is adequate dosimetric coverage. A criterionfor dosimetric coverage is the percent target below goal.The percent target below goal is defined as the percentage ofplanning target volume that is below prescribed dose. Thisis often difficult to interpret in patients with head and neckcancer as normal structures are often in the middle of thetarget (e.g., optic chiasm for nasopharyngeal carcinoma).For this reason it is necessary to evaluate each axial slice foradequacy of coverage and adequacy of avoidance.
Other concerns raised in IMRT included matchline anddose inhomogeneity. We have addressed the physical as-pects of the issue of matchline previously (18). The hotspots are typically in the center of the target. If the deliveryof radiation is applied correctly,i.e., within 1 mm of thesetup, there is a 2% to 3% dose gradation at the matchline.
30 I. J. Radiation Oncology● Biology ● Physics Volume 45, Number 1, 1999

As we have learned clinically, in conventional radiotherapytechniques when field matching is used, a schedule of 15 to35 fractions tends to “feather” out the overdosage (hot-spots) or underdosage (cold-spots) in any single fraction,unless the junctional error is unidirectional. The PeacockIMRT system is only used for fractionated radiation therapyin our department. Our current clinical experience with nolocal failure, marginal recurrence, or geographical missadditionally supported our previous discussion. It is rou-tinely necessary to prescribe to the 85% isodose of themaximum dose to provide adequate coverage of targets.There were 17 patients in our series that had the 85%prescription. Occasionally we prescribe up to 90% if thethreshold of the critical structure is exceeded,e.g.,3 patientsin our series. There is dose inhomogeneity as we prescribedto 85% of the maximum dose, as compared to the conven-tional prescription of 98% to 100%. Homogeneity is notused as a criterion in accepting a treatment plan. Based onICRU 50 recommendation of conformal radiotherapy, themean (average) dose is used as one of the criteria. However,the most optimum dosimetric assessment is still being eval-uated. Homogeneity is being followed closely in the dataaccrual but it is too early to attempt to correlate it withoutcome.
SMART boost is clinically feasible in view of the treat-ment planning, QA and documentation as well as the actualtreatment time for patients. On average, treatment planning,QA and documentation take 2 days prior to commencementof treatment. The therapists take approximately 20 minutesto treat a patient with a four-arc plan. It is feasible to treatup to 25 patients a day with IMRT in the clinic.
Essentially, SMART boost is more cost saving (Table 9).
The allowable Medicare charges for the SMART boost areabout 20% less than conventional fractionation and about33% less than accelerated fractionation scheme. This is animportant issue in the present era of cost consciousness andmanaged care that has created an increasing interest in theeconomics of malignant disease (19). Currently, Talon is nolonger used for our patients with head and neck cancers. Areinforced aquaplast mask is used instead. Threfore, thecharges for neurosurgery and anesthesiology are not con-sidered.
CONCLUSION
SMART boost appears to be a new effective acceleratedradiotherapy in the treatment of head and neck cancers. It issound and feasible both radio-biological and from our initialclinical experience. It has offered many advantages andappears encouraging to all currently available acceleratedfractionation schemes. Acute toxicities are more severe butacceptable. Long-term follow-up is needed to evaluate latetoxicities. Subjective parotid function is achieved.
Encouraging initial complete response rate suggests theeffectiveness of SMART boost. SMART boost is clinicallyfeasible. Mean doses to targets are higher than prescribeddose, which may be beneficial and normal tissues can bekept will below their tolerance. Dosimetric coverage oftargets and avoidance of normal tissues can be achieved.The fractionation schedule is also cost saving. A random-ized trial is proposed against conventional and other alteredfractionation schemes. Studies of a larger population ofpatients and a long-term follow-up are underway.
REFERENCES
1. Fowler JF. The linear-quadratic formula and program in frac-tionated radiotherapy. Br J Radiol 1989;62:679–694.
2. Peters LJ, Ang KK, Mames HD Jr. Accelerated fractionationin the radiation treatment of head and neck cancer. Acta Oncol1988;27:185–194.
3. Withers HR, Taylor JMG, Macejewski B. The hazard ofaccelerated tumor clonogen repopulation during radiotherapy.Acta Oncol 1988;27:131–146.
4. Sladowski K, Macejewski B, Pileski B, Swiatmicka J, GolenM, Przeorek W. Randomized clinical trial of accelerated 7days per week fractionation in radiotherapy for head and neckcancer. Preliminary report on therapy toxicity. Radiother On-col 1996;40:S40.
5. Overgaard J, Sand Hansen H, Sapru W, Overgaard M, Grau C,Jergensen K, Bastholt L, Hansen O, Specht L, Berthelsen A,Pedersen M. Conventional radiotherapy as the primary treat-ment of squamous cell carcinoma (SCC) of the head and neck.A randomized multicenter study of 5 versus 6 fractions perweek—preliminary report from DAHANCA 6 and 7 trial.Radiother Oncol 1996;40:531.
6. Jackson SM, Weir LM, Hay JH, Tsang VHY, Durham JS. Arandomized trial of accelerated versus conventional radiotherapyin head and neck cancer. Radiother Oncol 1997; 43:39–46.
7. Ang KK, Peters LJ, Weber R. Concomitant boost radiotherapyschedules in the treatment of carcinoma of the oropharynx and
nasopharynx. Int J Radiat Oncol Biol Phys 1990;19:1339–1345.
8. Grant W. Experience in intensity modulated beam delivery.In: Mackie TR, Palta JR, editors. Teletherapy present andfuture. Madison, WI: Advanced Medical Publishing; 1996:793–803.
9. Woo SY, Grant WH, Bellezza D, Grossman R, Gildenberg P,Carpenter LS, Carol M, Butler EB. A comparison of intensitymodulated conformal therapy with a conventional externalbeam stereotactic radiosurgery system for the treatment ofsingle and multiple intracranial lesions. Int J Radiat OncolBiol Phys 1996;35:593–597.
10. Hornsberger HR. Imaging of the suprahyoid and infrahyoidneck. In: Harnsberger HR, editor. Head and neck imaging. St.Louis, MO: Year Book Medical Publishers, 1990:1–224.
11. Slevin NJ, Vasanthan S, Dougal M. Relative clinical influenceof tumor dose versus dose per fraction on the occurance of latenormal tissue morbidity following larynx radiotherapy. Int JRadiat Oncol Biol Phys 1993;25:23–28.
12. Harwood AR. Cancer of the larynx. The Toronto experience.J Laryngol 1982;11:1–21.
13. Saunders MI, Dische S, Grosch EJ, Fermont DC, AshfordRFU, Maher EJ, Makepeace AR. Experience with CHART.Int J Radiat Oncol Biol Phys 1991;21(3):871–878.
14. Horiot JC, Le Fur R, N’Guyen T, Chenal C, Schraub S,
31SMART boost● E. B. BUTLER et al.

Alfonsi S, Gardani G, Van Den Bogaert W, Danczak S, BollaM, Van Glabbeke M, De Pauw M. Hyperfractionation versusconventional fractionation in oropharyngeal carcinoma: Finalanalysis of a randomized trial of the EORTC Cooperativegroup of radiotherapy. Radiother Oncol 1992;25:231–241.
15. Ang KK. Accelerated fractionation: What is the price forspeeding? Radiother Oncol 1997;44:97–99.
16. Johnson JT, Ferretti GA, Nethery WJ, Valdez IH, Fox PC, NgD, Muscoplat CC, Gallagher SC. Oral pilocarpine for post-irradiation xerostomia in patients with head and neck cancer.N Engl J Med 1993;329:390–395.
17. Bataini JP, Bernier J, Jaulerry C, Brunin F, Pontvert D, LaveC. Impact of neck node radioresponsiveness on the regionalcontrol probability in patients with oropharynx and pharyngo-larynx cancers managed by definitive radiotherapy. Int J Ra-diat Oncol Biol Phys 1987; 13:817–824.
18. Carol M, Grant WH, Bleier AR, Kania AA, Targovnik HS,Butler EB, Woo SY. The field-matching problem as it applies tothe peacock three dimensional conformal system for intensitymodulation. Int J Radiat Oncol Biol Phys 1996;34:183–187.
19. Pfister DG, Ruchlin HS, Elkin EB. Economic consideration inthe care of patients with head and neck malignancies. CurrOpin Oncol 1997;9:241–246.
32 I. J. Radiation Oncology● Biology ● Physics Volume 45, Number 1, 1999
Related Documents