Devolution of Health and Social Care to UK Cities: The end of the ‘National’ Health Service? #DevoHealth A Guest Lecture and Panel Discussion Event

Slides - 'Devolution of Health and Social Care to UK Cities' event at Leeds Beckett 25/06/15
Aug 07, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Devolution of Health and Social Care to UK Cities: The end of the ‘National’ Health Service?
#DevoHealth
A Guest Lecture and Panel Discussion Event

Professor Judith Smith Director of the Health Services Management Centre, University of Birmingham
#DevoHealth

Devolution of health and social care to UK cities: the end of the
‘National’ Health Service?
Professor Judith Smith
Leeds 25 June 2015
Agenda
The (inter)national contextDevolution and the four NHSsRegional governance: risks and
opportunitiesAnd what about the research
evidence?

The (inter)national context

The nature of the NHS
The NHS is run as one of the most centralised health systems in the world
Strongly focused on government, national bodies, London, and taxes raised nationally
A culture among managers and boards of looking upwards for guidance and approval
And the political centre tends to default to micro-management
The public and politicians reinforce this – ‘NHS the closest thing we have to a national religion’

How others do it
Many of our neighbours run health through local government, e.g. Denmark, Sweden
They tend to have a very small Ministry of Health Typically draw together health and social care funding and
provision at local level And others have stronger local control and involvement
through devolved social insurance purchasing in states or regions, e.g. France, Germany
Others have directly elected health boards (e.g. NZ) So we are an outlier for health, but not in other areas such
as social care, pre-school education

© Nuffield Trust

Devolution and the four NHS

A disunited kingdom
There is no longer ‘a UK NHS’ Was always run differently across the four
nations Markedly so since political devolution Changed entitlements, e.g. to free prescriptions
and eye tests, and to free personal social care And four very different systems, with their own
policy priorities, & structures

© Nuffield Trust

Compare and contrast
Study of the four nations is contentious and complex (Bevan et al, 2014)
Despite significant policy differences, performance variations not in fact so marked
All 4 countries have improved performance of the NHS, and variations across the 4 have reduced
All are facing austerity and tough decisions Targets (e.g. waiting lists) seem to make some impact Wider policy context seems less influential

Regional governance: risks and opportunities
What is in it for the NHS?
A service still reeling from Lansley’s reforms in the Health and Social Care Act (2012)
The lack of a regional strategic tier results from those reforms
NHS England Five Year Forward View (rightly) wants new models of care and shift of priority to primary and preventative care
Who will decide, arbitrate, persuade – and lead implementation?
And frailty – people living with several long-term conditions – needs a holistic local response

© The Kings Fund

What is in it for local government?
Reclaiming some local commissioning and planning powers that have been eroded over the years?
Bringing health decision making to a more local and democratically engaged level
A formal arrangement that draws the NHS properly alongside, for real budget sharing?
A way of coordinating different levels of place-based decision making for specific services
Especially for frailty, vulnerable families, people living with mental health problems


Risks
Leaping to devolve, without working out what is actually the question to be answered
Assuming a ‘one size fits all’ approach to devolution to regions or cities
Another structural reorganisation that distracts from developing new models of care
The politicians continuing to micro-manage difficult NHS decisions and issues
Failing to work out how best to embrace at a regional level the sociology of the professions
Concentrating on structures and governance, at the expense of local service change

Opportunities
Build on strong local relationships and joint working – solutions often already here
Decisions about NHS services being more properly local (e.g. a local reconfiguration panel)
A chance to establish new ways of engaging local people in the difficult decisions facing public services
Testing out (over the long term) place-based commissioning for the most complex users
Capacity to lever investment that can in turn support improved health and wellbeing

What about the research evidence?

Commissioning
Joint commissioning has a long, mixed and well-researched history
Tendency to concentrate on aspiration, process, structures and relationships (Dickinson, 2008)
Much less on determining clear desired outcomes and enacting and measuring these (Dickinson et al, 2013)
Health commissioning likewise favours the relational and struggles to transact change (Smith et al, 2013)
Is this all connected to the lack of a proper statutory forum in which tough health and care decisions can be made? (Glasby et al, 2006)

Integrated care
Efforts across OECD health and care systems to find the holy grail of ‘integrated care’ (Nolte et al, 2014)
Many now focusing more on coordination of care for those with most complex needs
Evidence points to improved user experience But equivocal about economic benefits Takes significant time to make such change, and has to be
contextually sensitive (Best et al, 2012) Beware the emergency admission reduction target…
(Bardsley et al, 2013)
Structural reorganisation
There is an extensive base of evidence across sectors and nations (Edwards, 2010)
Restructuring and reorganisation rarely achieve the stated objectives (and indeed these are rarely assessed) (Peck et al 2006)
It is arguably harder to merge or restructure in the public sector
The people and ‘soft’ aspects tend to get less attention (Dickinson et al 2006)
Can be a distraction activity from the tough business of making changes to services with and for local people and staff

In conclusion
We do need to create more of an ‘NHS Local’ (Glasby et al, 2006)
Place-based commissioning and planning feel intuitively right And we have do address the London and South-East centric
nature of decision making But the last thing we need is an imposed or rushed structural
reorganisation We need to work out what we are trying to do and why, and
then think about how to do it Is England (and especially the NHS) ready for such localism,
for it would challenge the ‘national’ in NHS?


@DrJudithSmith
@_HSMCentre
http://www.birmingham.ac.uk/HSMC
Professor Judith Smith
References
Bardesley, M., Steventon, A., Smith, J. and Dixon, J. (2013) Evaluating integrated and community-based care: how do we know what works? [online] Available at: http://www.nuffieldtrust.org.uk/publications/evaluating-integrated-and-community-based-care-how-do-we-know-what-works [Accessed 24 June 2015]
Best, A., Greenhalgh, T., Lewis, S. et al. (2012) Large-system transformation in health care: a realist review. Milbank Quarterly, 90(3): 421-456
Bevan, G. and Mays, N. (2014) The four health systems of the UK: How do they compare? [online] Available at: http://www.nuffieldtrust.org.uk/compare-UK-health [Accessed 24 June 2015]
Dickinson, H. (2008) Evaluating outcomes in health and social care. Bristol: Policy Press.
Dickinson, H., Peck, E. and Smith, J. (2006) Leadership in organisational transition – what can we learn from research evidence? Summary report. Birmingham: Health Services Management Centre.
References continuedDickinson, H. et al. (2013) Joint commissioning in health and social care: an exploration of definitions, processes, services and outcomes [online]. Available at: http://www.nets.nihr.ac.uk/__data/assets/pdf_file/0004/85054/FR-08-1806-260.pdf [Accessed 24 June 2015]
Edwards, N. (2010) The triumph of hope over experience [online]. Available at: http://www.nhsconfed.org/resources/2010/06/the-triumph-of-hope-over-experience [Accessed 24 June 2015]
Glasby, J., Smith, J. and Dickinson, H. (2006) Creating 'NHS local': a new relationship between PCTs and local government [online]. Available at: http://www.birmingham.ac.uk/Documents/college-social-sciences/social-policy/HSMC/publications/2006/Creating-NHS-Local.pdf [Accessed 24 June 2015]
Health and Social Care Act (2012) – Health and Social Care Act 2012. (c. 7) [online]. Available at: http://www.legislation.gov.uk/ukpga/2012/7/contents/enacted/data.htm [Accessed 24 June 2015]

References continuedHealth and Social Care Act (2012) – Health and Social Care Act 2012. (c. 7) [online]. Available at: http://www.legislation.gov.uk/ukpga/2012/7/contents/enacted/data.htm [Accessed 24 June 2015]
Nolte, E. and Pitchforth, E. (2014) What is the evidence on the economic impacts of integrated care? [online] Available at: http://www.euro.who.int/en/about-us/partners/observatory/news/news/2014/06/what-is-the-evidence-on-the-economic-impacts-of-integrated-care [Accessed 24 June 2015]
Peck, E., Dickinson, H. and Smith, J. (2006) Transforming or transacting? The role of leaders in organisational transition. British Journal of Leadership in Public Services, 2(3): 4-14
Smith, J. et al. (2013) Commissioning high-quality care for people with long-term conditions [online]. Available at: http://www.nuffieldtrust.org.uk/sites/files/nuffield/publication/130301_commissioning-high-quality-care-for-long-term-conditions_0.pdf [Accessed 24 June 2015]

Warren HeppoletteStrategic Director - Health & Social Care Reform, Greater Manchester
#DevoHealth

Ian WilliamsonChief OfficerGreater Manchester Health and Social Care Devolution
NW Finance Directors
Friday 15 May 2015
NW Finance Directors
Friday 15 May 2015
Ian Williams
Chief Officer
Greater Manchester Health and Social Care Devolution
Chief Officer
Greater Manchester Health and Social Care Devolution
Health & Social Care Devolution - Introduction
25th June 2015
Warren Heppolette

GM Devolution – the background
Greater Manchester Devolution Agreement settled with Government in November 2014, building on GM Strategy development.
Powers over areas such as transport, planning and housing – and a new elected mayor.
Ambition for £22 billion handed to GM.
MOU Health and Social Care devolution signed February 2015: NHS England plus the 10 GM councils, 12 Clinical Commissioning Groups and NHS and Foundation Trusts
MoU covers acute care, primary care, community services, mental health services, social care and public health.
To take control of estimated budget of £6 billion each year from April 2016.

To ensure the greatest and fastest possible improvement to the health and wellbeing of the 2.8 million citizens of Greater Manchester
Vision
Objectives
• Improve the health and wellbeing of all of the residents of Greater Manchester from early age to older people, recognising that this will only be achieved with a focus on the prevention of ill health and the promotion of wellbeing
• Move from having some of the worst health outcomes to having some of the best
• Close the health inequalities gap within GM and between GM and the rest of the UK faster

• Enable us to have a bigger impact, more quickly, on the health, wealth and wellbeing of GM people
• Be more free to respond to what local people want - using their experience and expertise to help change the way we spend the money
• Create more formal collaboration and joint decision making across the region to co-ordinate services to tackle some of the major health, housing, work and other challenges - supporting physical, mental and social wellbeing
Benefits
37
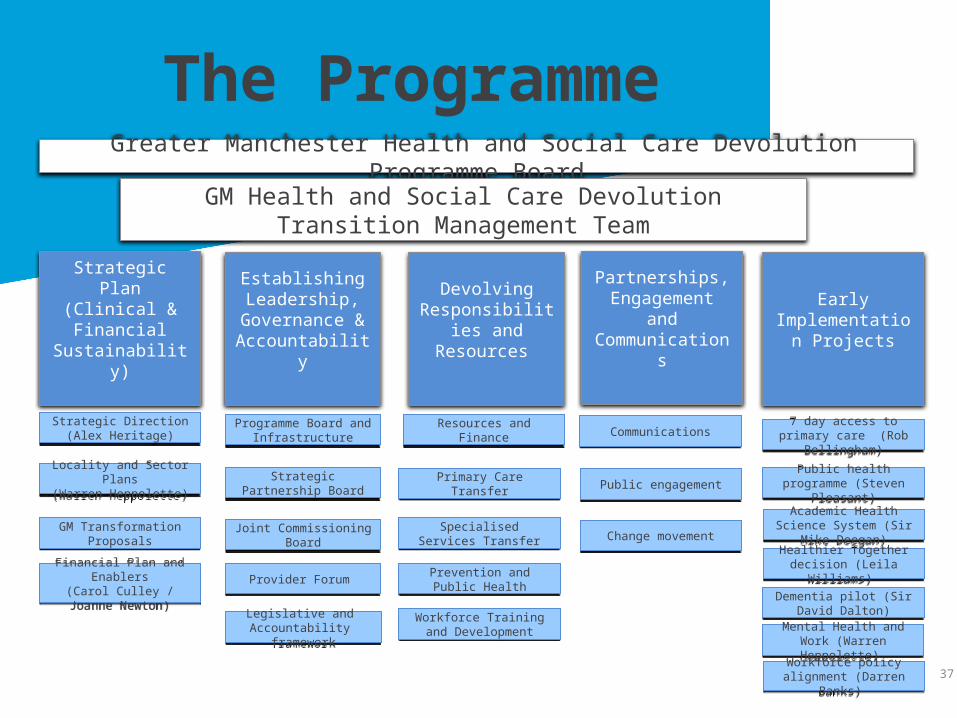
Strategic Plan (Clinical & Financial
Sustainability)
Greater Manchester Health and Social Care Devolution Programme Board
Establishing Leadership,
Governance & Accountability
Devolving Responsibilities and Resources
Partnerships, Engagement and Communications
Early Implementation
Projects
7 day access to primary care (Rob Bellingham)
7 day access to primary care (Rob Bellingham)
Public health programme (Steven Pleasant)
Public health programme (Steven Pleasant)
Academic Health Science System (Sir Mike Deegan)Academic Health Science System (Sir Mike Deegan)
Healthier Together decision (Leila Williams)
Healthier Together decision (Leila Williams)
Dementia pilot (Sir David Dalton)
Dementia pilot (Sir David Dalton)
Mental Health and Work (Warren Heppolette)
Mental Health and Work (Warren Heppolette)
Programme Board and Infrastructure
Programme Board and Infrastructure
Strategic Partnership BoardStrategic Partnership Board
Joint Commissioning BoardJoint Commissioning Board
Provider Forum Provider Forum
Legislative and Accountability framework
Legislative and Accountability framework
Workforce policy alignment (Darren Banks)
Workforce policy alignment (Darren Banks)
Strategic Direction(Alex Heritage)
Strategic Direction(Alex Heritage)
Locality and Sector Plans(Warren Heppolette)
Locality and Sector Plans(Warren Heppolette)
GM Transformation Proposals
GM Transformation Proposals
Financial Plan and Enablers(Carol Culley / Joanne
Newton)
Financial Plan and Enablers(Carol Culley / Joanne
Newton)
Resources and FinanceResources and Finance
Primary Care TransferPrimary Care Transfer
Specialised Services TransferSpecialised Services Transfer
Prevention and Public HealthPrevention and Public Health
Workforce Training and Development
Workforce Training and Development
The Programme
CommunicationsCommunications
Public engagementPublic engagement
Change movementChange movement
GM Health and Social Care Devolution Transition Management Team

Devolution is the mechanism, not the master…What is the problem we are trying to solve…?
….devolution can be the trigger for greater and necessary positive reform
A growing ageing population
Poorer health & growth in chronic conditions
Instability & fragmentation in the health & care system
Consequences • Unplanned,
Haphazard change
• Poorer care and treatment
• Difficulty in meeting future health needs
• Failing the health & care workforce
Consequences • Unplanned,
Haphazard change
• Poorer care and treatment
• Difficulty in meeting future health needs
• Failing the health & care workforce
Increasing pressure on health & social care

Greater Manchester local health profile is significantly worse than England Average
SOURCE: 2014 Local Health Profiles, AHPO Better MixedGenerally worse
General health
Lower than averageHigher than average
Deprivation
Comparison to England average
Local Authority
Trafford
Wigan
Tameside
Stockport
Salford
Oldharn
Manchester
Bury
Bolton
Children living in poverty
Life expectancy gap. most and least deprived areasLife expectancyDeprivation
Year 6 children classed as obese
General health
Rochdale11,900 Lower for men and
women20.7%• 9.7 years lower for men.
• 7.9 years lower for women
6,500 Higher for women 18.4%• 10.1 years lower for men.
• 6.3 years lower for women
12,000 Lower for men and women
18.9 %• 9.4 years lower for men.
• 8.5 years lower for women
10,300 Lower for men and women
18.6%• 10.9 years lower for men.
• 8.2 years lower for women
8,500 Similar for men and women
17.1 %• 10.8 years lower for men.
• 8.4 years lower for women
12,700 Lower for men and women
21.5 %• 11.5 years lower for men.
• 8.2 years lower for women
13,300 Lower for men and women
19.3%• 11.2 years lower for men
• 9.2 years lower for women
34,630 Lower for men and women
24.7%• 9.6 years lower for men.
• 8.2 years lower for women
6,670 Lower for men and women
19.3 %• 11.5 years lower for men.
• 7.6 years lower for women
13,040 Lower for men and women
20.0 %• 12.1 years lower for men.
• 9.2 years lower for women

Rate of avoidable admissions in all Greater Manchester CCGs is higher than national average
Whilst our disease registers show a high level of disease prevalence we've still only found about half of the preventable disease that exists.
In those patients with disease we have only around 40% are treated to evidence based levels leading to our high level of ambulatory care admissions.
We can improve treatment processes resulting in real impacts on the rates of disease progression and reductions in preventable admission costs.
41SOURCE: January 2015 ASC, CCG and Trust information returns
NHS commissioners
NHS Trusts
Adult Social Care
Challenge1
£1,184m
£851m3
£333m
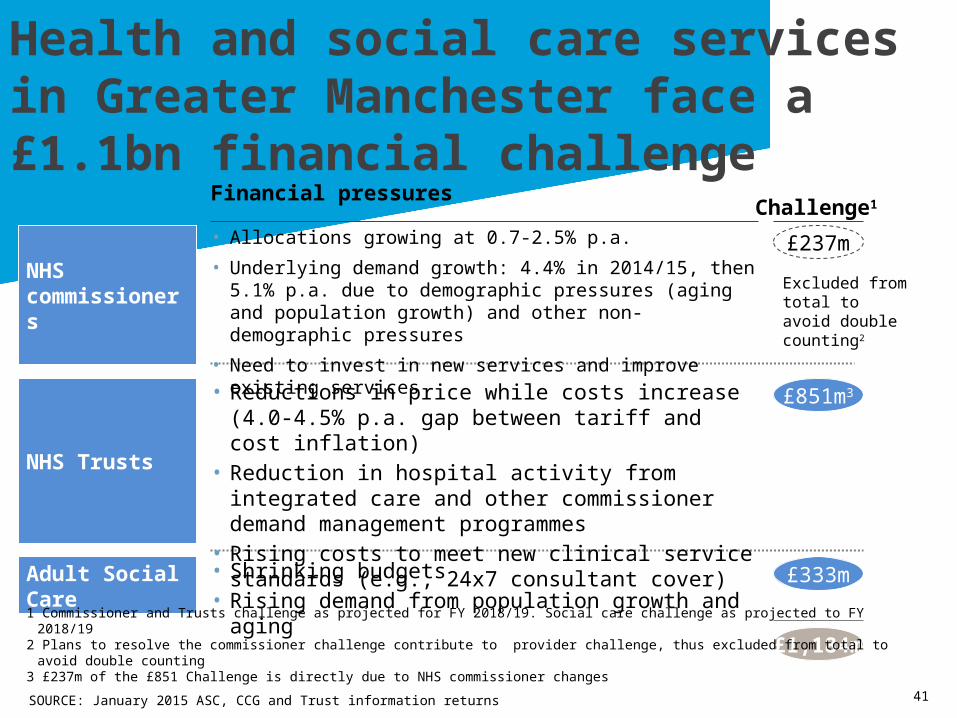
Financial pressures
• Allocations growing at 0.7-2.5% p.a.
• Underlying demand growth: 4.4% in 2014/15, then 5.1% p.a. due to demographic pressures (aging and population growth) and other non-demographic pressures
• Need to invest in new services and improve existing services
• Reductions in price while costs increase (4.0-4.5% p.a. gap between tariff and cost inflation)
• Reduction in hospital activity from integrated care and other commissioner demand management programmes
• Rising costs to meet new clinical service standards (e.g., 24x7 consultant cover)
• Shrinking budgets • Rising demand from population growth and aging
Health and social care services in Greater Manchester face a £1.1bn financial challenge
1 Commissioner and Trusts challenge as projected for FY 2018/19. Social care challenge as projected to FY 2018/192 Plans to resolve the commissioner challenge contribute to provider challenge, thus excluded from total to avoid double counting3 £237m of the £851 Challenge is directly due to NHS commissioner changes
£237m
Excluded from total to avoid double counting2

42
This isn’t just about Health
Worklessness & Low Skills Children & Young People Crime & Offending Health & Social Care Long-term JSA claimants ESA claimants (WRAG) ‘Low pay no pay’ cycles
Working Tax Credit claimants Low skill levels (vocational or
academic) Insecure employment
NEET (Young People) Compounding factors:
Lone parents with children 0-4 Poor literacy and numeracy Poor social skills Low aspirations Living alone
Child in Need Status (CIN) / known to Children’s Social Care Child not school ready Low school attendance & exclusions Young parents Missing from home Compounding factors:
Repeat involvement with social care
LAC with risk of offending Poor parenting skills SEN Frequent school moves Single parents
Repeat offenders Family member in prison Anti-social behaviour Youth Offending Domestic Abuse Organised Crime Compounding factors:
Lost accommodation Dependent on service Vulnerability to sexual
exploitation Missing from home Violent crime
Mental Health (including mild to moderate) Alcohol Misuse Drug Misuse Chronic Ill-health (including long-term illness / disability) Compounding factors:
Unhealthy lifestyle Social isolation Relationship breakdown / loss
or bereavement Obesity Repeat self-harm Living alone Adult learning difficulties
The roots of poor health are found across society and the public service – we need to do more than just respond at the point of crisis. This requires integration of not just health and care, but contributing wider public services
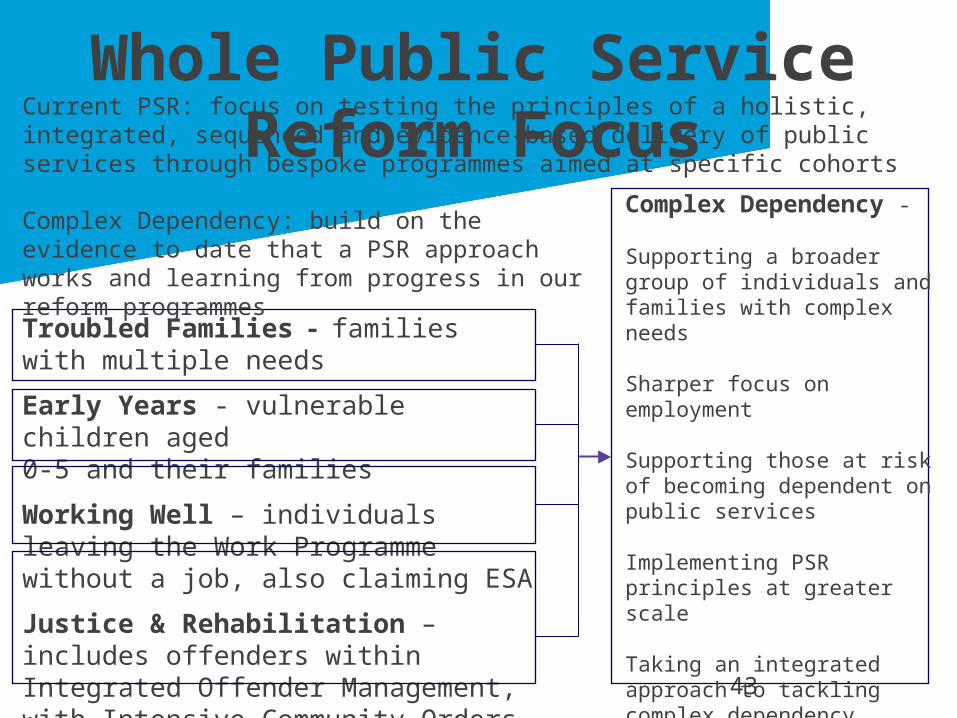
Whole Public Service Reform Focus
43
Troubled Families - families with multiple needs
Early Years - vulnerable children aged 0-5 and their families
Working Well – individuals leaving the Work Programme without a job, also claiming ESA
Justice & Rehabilitation – includes offenders within Integrated Offender Management, with Intensive Community Orders and Women Offenders
Current PSR: focus on testing the principles of a holistic, integrated, sequenced and evidence-based delivery of public services through bespoke programmes aimed at specific cohorts
Complex Dependency -
Supporting a broader group of individuals and families with complex needs
Sharper focus on employment
Supporting those at risk of becoming dependent on public services
Implementing PSR principles at greater scale
Taking an integrated approach to tackling complex dependency through whole system change in a place
Complex Dependency: build on the evidence to date that a PSR approach works and learning from progress in our reform programmes
44
The characteristics of our current modelsThe main causes of Greater Manchester's high cost/poor outcomes are:
• ‘Too late care’ where conditions are either not prevented or detected early enough, nor treated to evidenced based standards, and patients' needs escalate resulting in preventable hospital based emergency and elective care and for longer than is necessary.
• The perverse incentives and associated self-interested organisational behaviours of Greater Manchester's hospitals, and weak and uncoordinated system management
• A population that is "inactivated". That is too many of our population don't know that better health outcomes are significantly driven by appropriate lifestyle choices, self-care, the health benefits of work and the potential of a prevention driven NHS and Social Care service.

What does radical reform look like?
45
• Shifting the balance of investment towards proactive, early help and away from a crisis response
• Health & care defined by an approach based on prevention
• Intelligence led, highly targeted preventative action based on a deep knowledge of our communities and their strengths
• More integrated public services responding to all forms of vulnerability
• Increased healthy life expectancy
Wanless for GM 2022…
“Levels of public engagement in relation to their health are high. Life expectancy increases go beyond current forecasts, health status improves dramatically and people are confident in the health system and demand high quality care. The health service is responsive with high rates of technology uptake, particularly in relation to disease prevention. Use of resources is more efficient.”

What does it take to get there?• Embed a new city wide “offer” to the population, of ensuring the systematic implementation
of primary, secondary and tertiary prevention in all health and social care.
• Use our Public Service Reform opportunities to transform the balance between social and medical support to address properly the social determinants of poor health.
• A new model of general practice, extended in scope and scale to exploit the power of both “big data” using a single electronic record, continuity of care and “people powered health”, to lead a systematic implementation of a prevention service and producing a step change improvement in outcomes.
• Develop a “new contract” with our public detailing their new responsibilities regarding lifestyle choices, self-care and self-management of long term conditions.
• Achieve world class standards of elective and emergency hospital care, with hospital Providers’ collaborating as a system to create a “Centre of Excellence” in Greater Manchester providing “best in world” outcomes, to an “activated” population.
• Effective and objective system management, to ensure that both the new primary care led Provider services and the "Hospital Chain" services deliver continually improving, evidence based standards of care.
• An aligned Academic Health System ensuring we genuinely operate at the margins of science and drive innovation across a ‘Learning Health System’.

Professor Rob WebsterChief Executive, NHS Confederation
Visiting Professor, Leeds Beckett University
#DevoHealth

Tom RiordanChief Executive, Leeds City Council
#DevoHealth

Panel SessionQ&A
#DevoHealth

Related Documents











