
Sleep Medicine for Ortho-Pedo Residents
Jul 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Optimum Development of the Teeth, Jaws and Face: Yet Another Reason to Breastfeed
Kevin Boyd, M.Sc. (Nutrition), D.D.S.
Hypothesis: Ancestral (Paleo) regimens of Infant and Early Childhood Feeding (IECF) were/are protective against skeletal malocclusion pre-Industrial/Westernized cultures


The Problem:
SDB/OSA/Neuro-cognative Impairment:
The Solution:
Early Identification and Collaboration:
- compromised naso-respiratory function
-unhealthy sleep architecture (PSG)
-Sleep Medicine
-Evolutionary Medicine
-Evolutionary Dentistry

1. Sleep is not a luxury, sleep is as necessary to survival and well-being as food and water
Take Away Points:
2. There is a bi-directional association(e.g., perio/T2DM)between certain craniofacial phenotypes(high-vaulted palate, posterior crossbite, retrognathia, hyper-divergent
growth) and clustering with other known risk factorsfor SDB/OSA (snoring, ATH, bedwetting, night terrors, restless legs/active sleep, etc.)
3. preventive strategies include OMT, infant feeding/diet counseling; Tx alternatives to CPAP/surgery include RME, BB-O
4. collaborativeopportunities(responsibility?) exist for orthodontists, pediatric dentists, GP’s and RDH’s to identify/screen at-risk kids for SDB/OSA….refer (ENT’s, OMT’s, Sleep specialists) and Tx p.r.n.
e.g., The AAPMD

In conclusion:-abnormal craniofacial morphology, but not excess body fat, was associated with SDB in children 6–8 years of age.-patients with dental malocclusions, deviant craniofacial features and tonsillar enlargement should always be examined as regards to their sleeping habits, snoring and pauses in breathing during sleep.-children with tonsillar hypertrophy, cross bite and convex facial profile could be candidates for
early intervention and orthodontic treatment to prevent the progression of SDB in coming years.


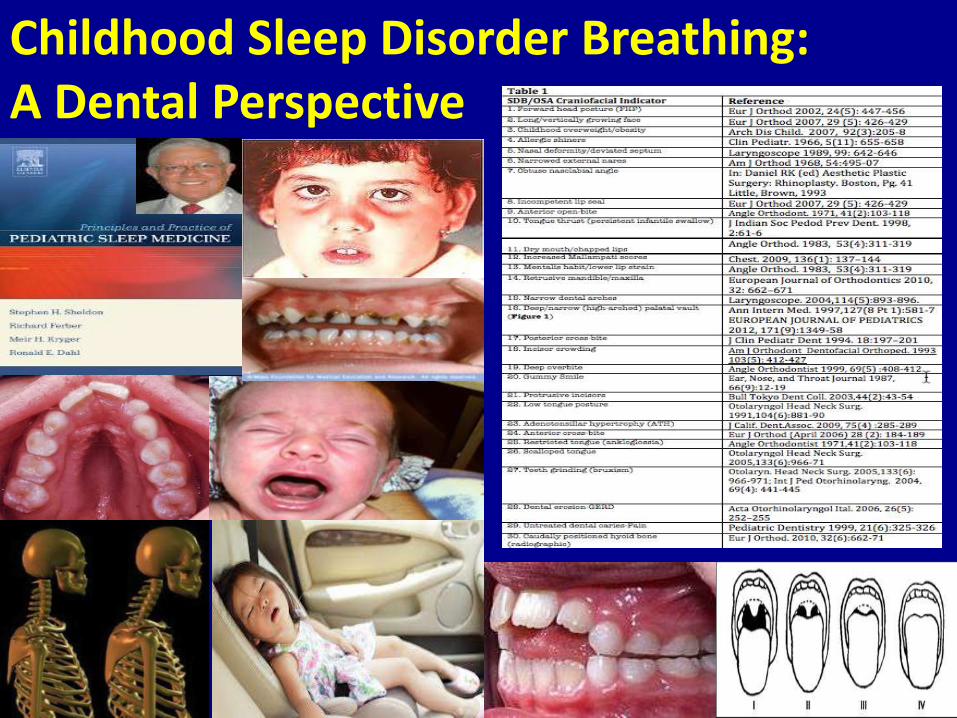
Childhood Sleep Disorder Breathing: A Dental Perspective
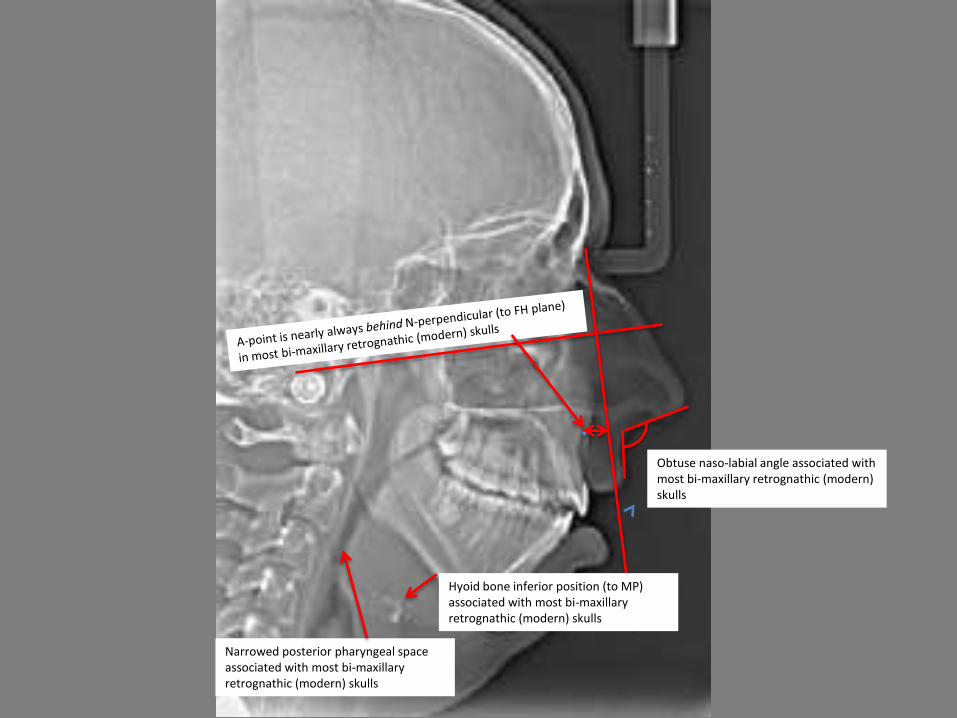
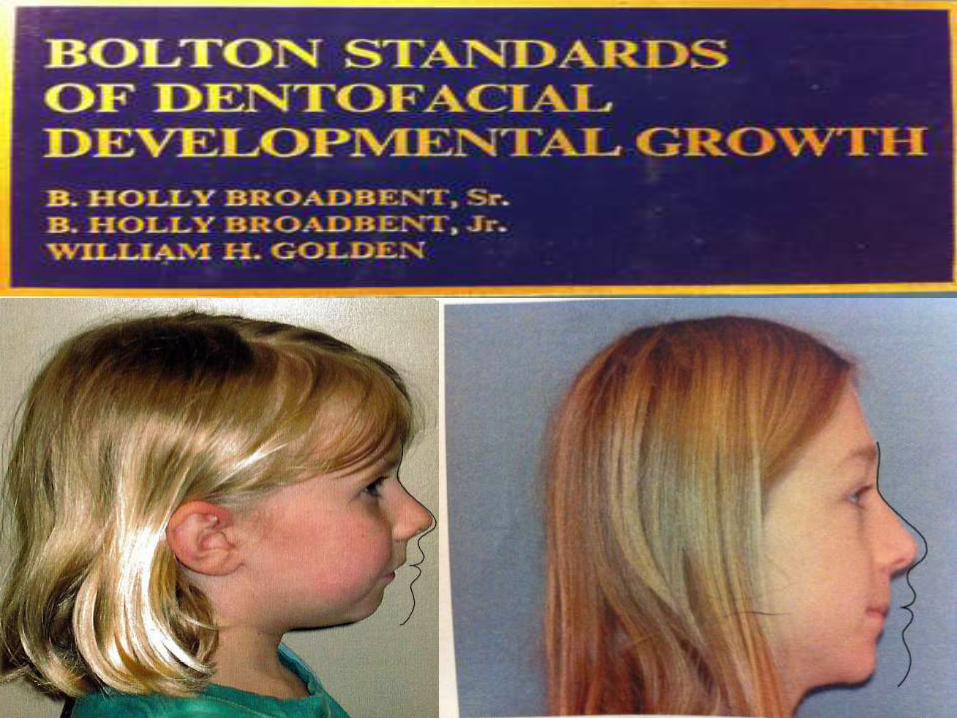
Narrowed posterior pharyngeal space associated with most bi-maxillary retrognathic (modern) skulls
Hyoid bone inferior position (to MP) associated with most bi-maxillary retrognathic (modern) skulls
Obtuse naso-labial angle associated with most bi-maxillary retrognathic (modern) skulls


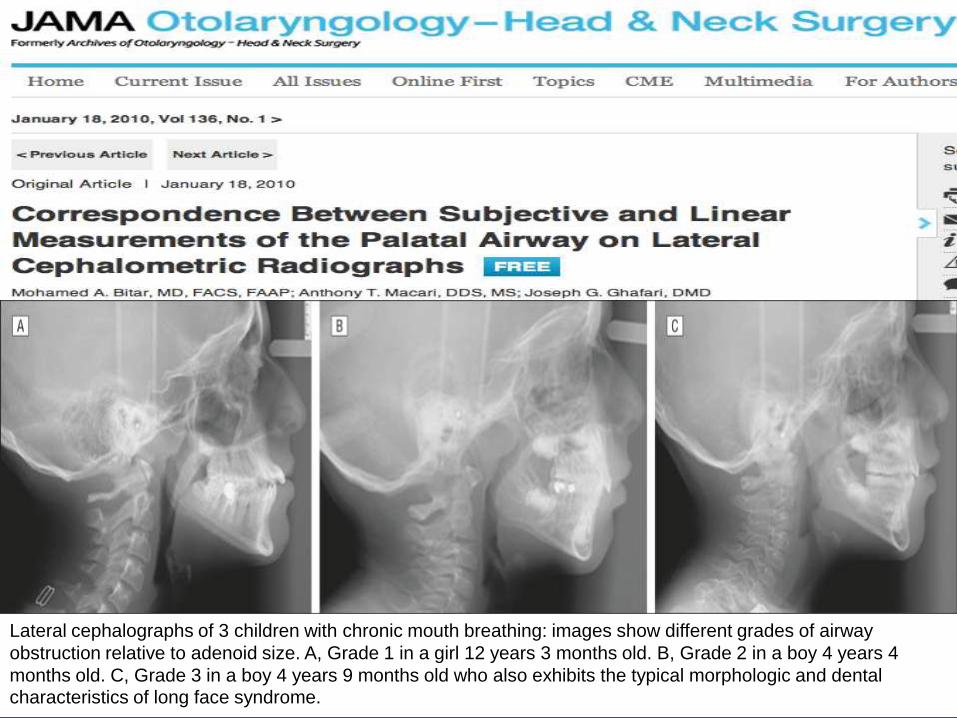
Lateral cephalographs of 3 children with chronic mouth breathing: images show different grades of airway
obstruction relative to adenoid size. A, Grade 1 in a girl 12 years 3 months old. B, Grade 2 in a boy 4 years 4
months old. C, Grade 3 in a boy 4 years 9 months old who also exhibits the typical morphologic and dental characteristics of long face syndrome.
-In the deciduous dentition, a distinctive occlusal and skeletal pattern of Class II maloccluson exists. In addition to concomitant diagnostic dental relationships in the sagittal plane (distal step, Class II deciduous canine relationship, excessive overjet), transverse interarch discrepancy due to a narrower maxillary arch is a constant feature of early Class II malocclusion. Skeletal findings in children with Class II malocclusion typically include significant mandibular retrusion and shorter total
mandibular length.
-the clinical signs of Class II malocclusion are evident in the
deciduous dentition and persist into the mixed dentition.
Am J Orthod Dentofacial Orthop. 1997 May;111(5):502-9.




3. preventive strategies include OMT, infant feeding/diet counseling; Tx alternatives to CPAP/surgery include RME, BB-O
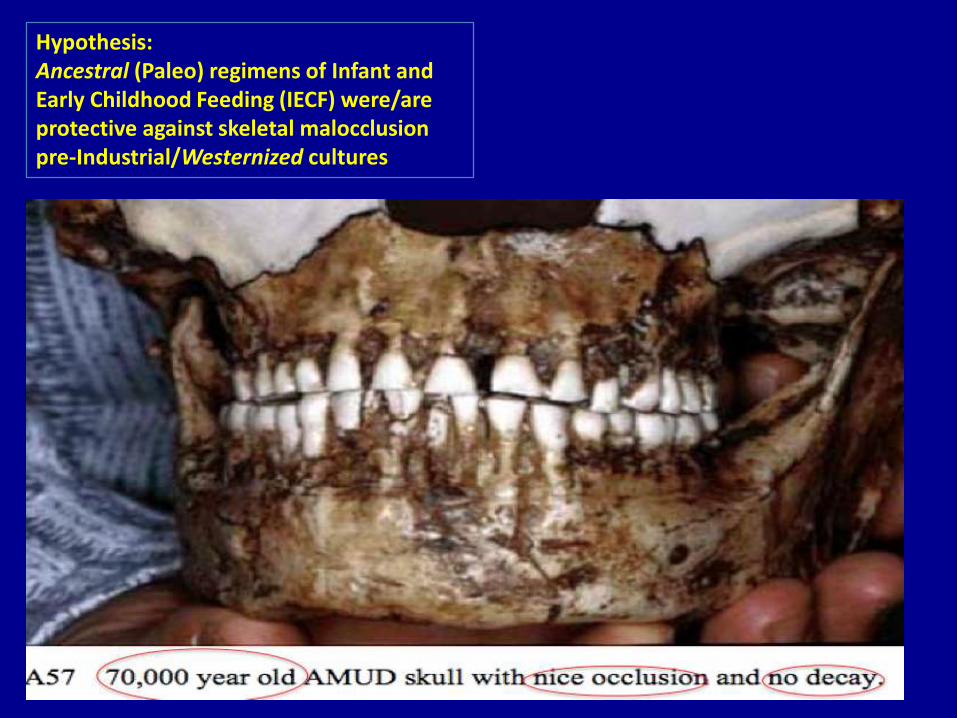
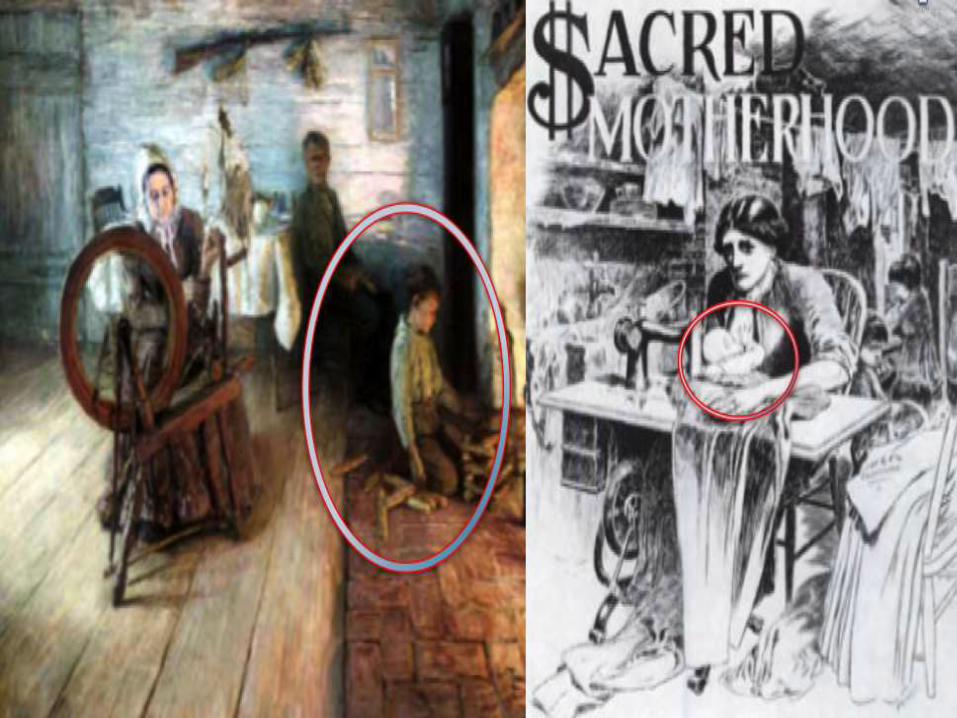
Hypothesis: Ancestral (Paleo) regimens of Infant and Early Childhood Feeding (IECF) were/are protective against skeletal malocclusion pre-Industrial/Westernized cultures

“ …(malocclusion) is a relatively new phenomenon in the human population and we do not find it in skeletons until after the seventeenth century. ” -Peter Gluckman
“… jaw anomalies (malocclusions wherein the teeth cannot fit properly in the jaw) are relatively new to European populations. Well-preserved skeletons from the 15th and 16th centuries show almost no malocclusion in the population….”

“….there is much circumstantial evidence that jaws and faces do not grow to the same size that they used to precisely because of our softer, more processed diets.” Daniel E. Lieberman

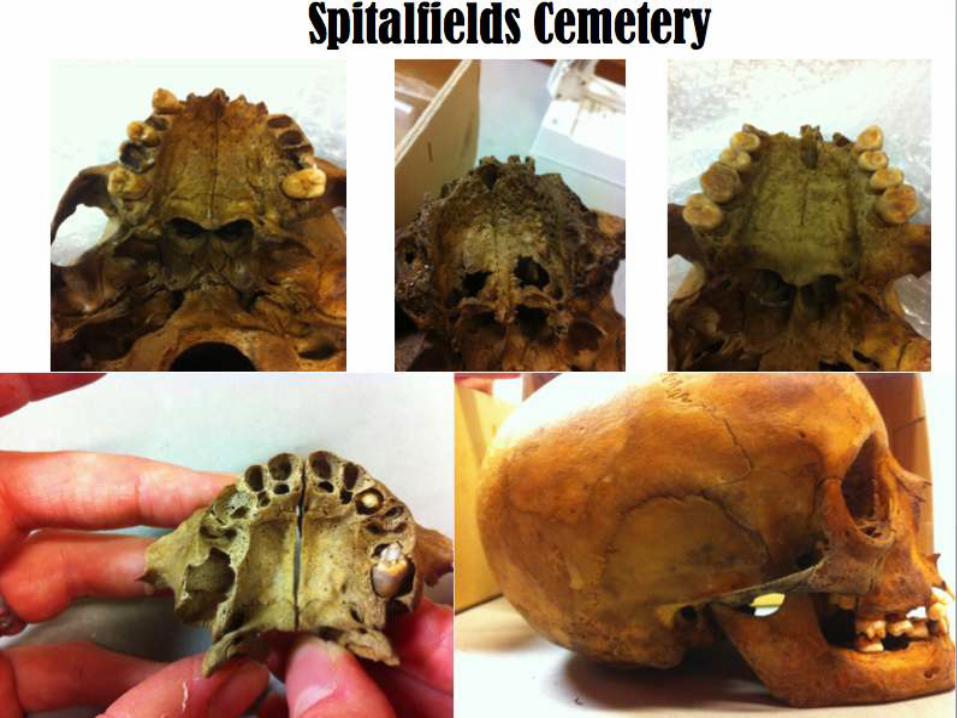
Abingdon Cemetery







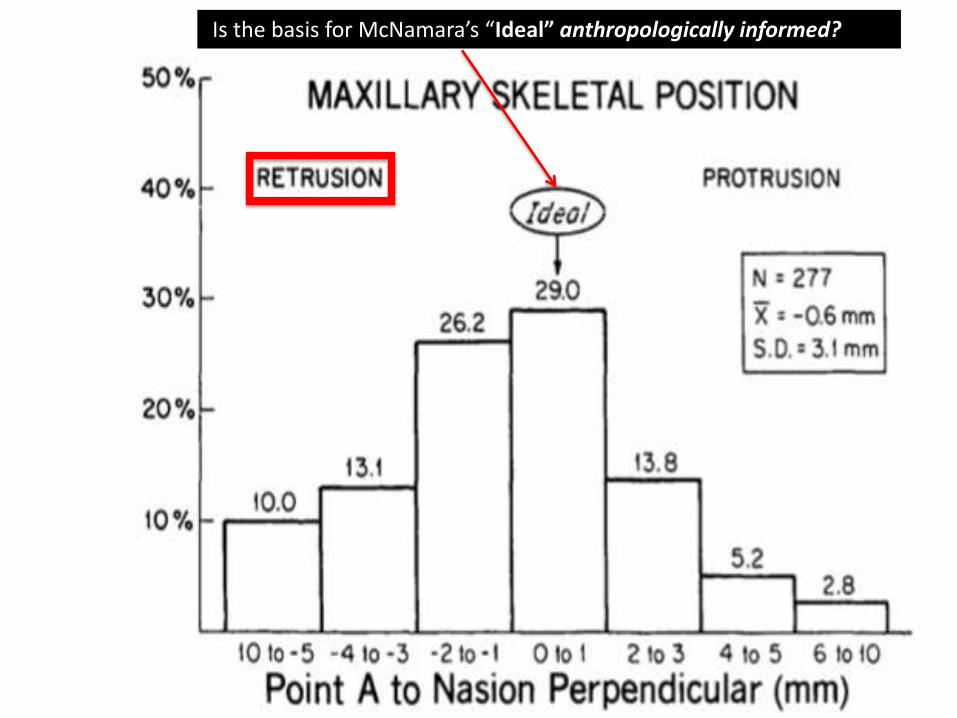
Is the basis for McNamara’s “Ideal” anthropologically informed?

The Angle Orthodontist: 54 (1): 5-17 1984
Angle Orthod. 54(1): 5-17 1984
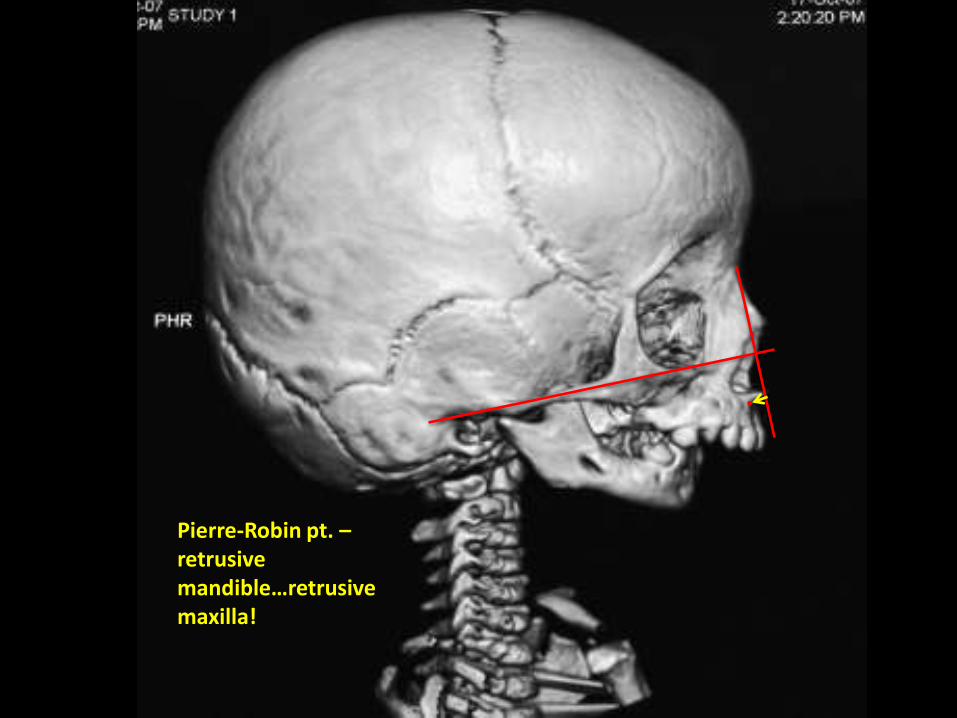
Pierre-Robin pt. –retrusive mandible…retrusive maxilla!
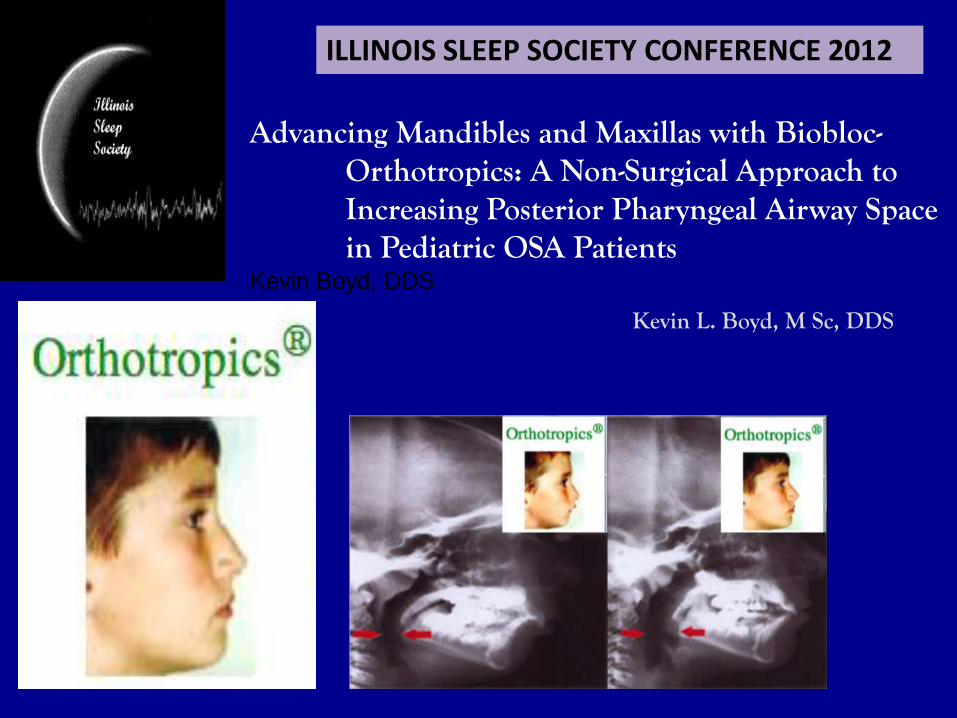
ILLINOIS SLEEP SOCIETY CONFERENCE 2012
Advancing Mandibles and Maxillas with Biobloc-Orthotropics: A Non-Surgical Approach to Increasing Posterior Pharyngeal Airway Space in Pediatric OSA Patients
Kevin Boyd, DDS
Kevin L. Boyd, M Sc, DDS
Courtesy of Brian Hockel, DDS

2/15/2010 BIOBLOC STAGE-1 Tx 2/21/2012 BIOBLOC STAGE- 3 Tx
Example: Assign an arbitrary control value for airway radius of 1.0. A 50% reduction in airway radius would mean that the new airway radius would be 0.5. Now, according to Poiseuille, that gives us...R = 1/(0.5)4R = 1/0.0625 = 16Therefore, resistance to airflow is increased 16-fold with a decrease in airway diameter (and radius) of 50%.

Stephen Sheldon, MD CMHCorrelating PSG data with Biobloc TX response
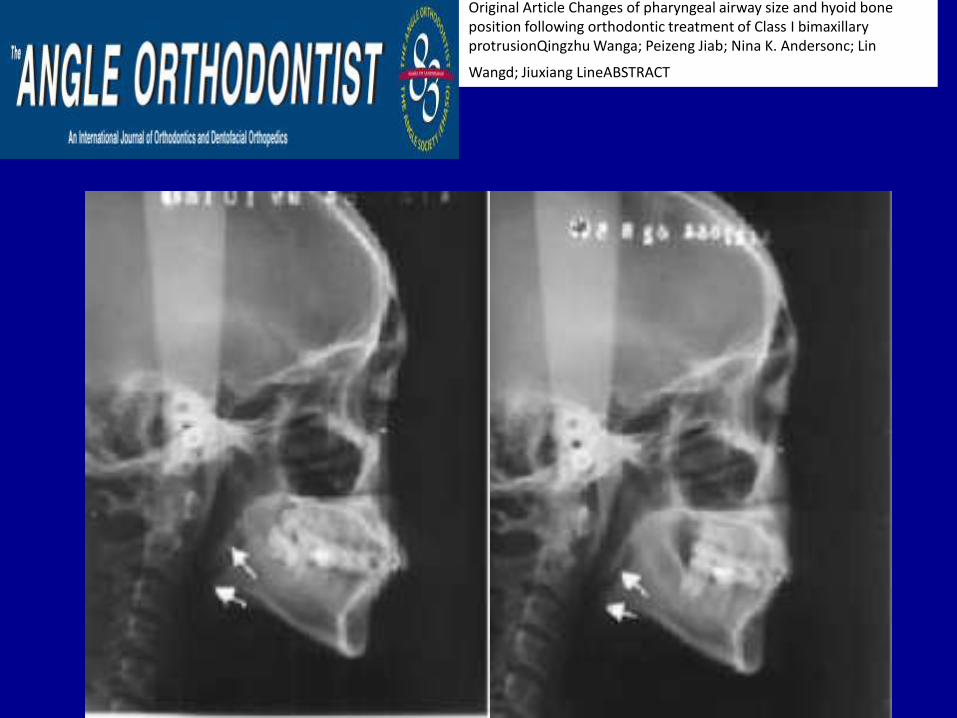
Original Article Changes of pharyngeal airway size and hyoid bone position following orthodontic treatment of Class I bimaxillary protrusionQingzhu Wanga; Peizeng Jiab; Nina K. Andersonc; Lin
Wangd; Jiuxiang LineABSTRACT




Although dentists and orthodontia recognize the importance of evaluating and treating OSA, they have yet to realize howwell-positioned they are for the prevention of sleep-
disordered breathing (SDB).
Another possible explanation for our findings is that oral cavity features such as high palates, narrow dental arches, and retruded chin all are additional risk factors for SDB in children38
38. Kushida CA, Efron B, Guilleminault C. A predictive morphometric model for the obstructive sleep apnea syndrome. Ann Intern Med. 1997;127:581–587
Related Documents











