Original article Sleep disorders in multiple system atrophy: a correlative video-polysomnographic study Roberto Vetrugno a, * , Federica Provini a , Pietro Cortelli b , Giuseppe Plazzi a , Enrico M. Lotti a , Giulia Pierangeli a , Carlotta Canali a , Pasquale Montagna a a Department of Neurological Sciences, University of Bologna, Via Ugo Foscolo 7, Bologna 40123, Italy b Institute of Clinical Neurology, University of Modena and Reggio Emilia, Via Dal Pozzo, Modena 41100, Italy Received 12 February 2003; received in revised form 17 June 2003; accepted 20 July 2003 Abstract Objective: The reciprocal relation between breathing, heart and motor system abnormalities during sleep was studied in multiple system atrophy (MSA) by means of video-polysomnographic recordings (VPSG). Patients and Methods: Nineteen consecutive MSA patients underwent VPSG with scoring for sleep, respiratory abnormalities, heart (HR) and breathing (BR) rates, and abnormal motor activities. A comparative analysis was performed versus 10 patients with obstructive sleep apnoea syndrome (OSAS). Results: All MSA patients displayed snoring, 42% stridor, and 37% OSAS. Mean sleep SaO 2 was 92.7%, and lowest SaO 2 86%. Patients with stridor had a significant increase in BR from Wake to NREM and REM sleep, and higher HR during sleep. Respiratory muscles and tibialis anterior EMG tonic activity was frequently found, more often in patients with stridor. All patients had REM sleep behaviour disorders (RBD) and 88% periodic limb movements during sleep (PLMS). No OSAS patient had RBD or respiratory muscles and tibialis anterior tonic activity. Conclusions: MSA patients, especially those with associated stridor, commonly display impaired breathing and abnormal control of respiratory and limb muscles during sleep. Breathing and motor abnormalities are often concomitant in the same patient, indicating a diffuse impairment of sleep homeostatic integration that should be included within the diagnostic features of MSA. q 2003 Elsevier B.V. All rights reserved. Keywords: Multiple system atrophy; Sleep; Stridor; Snoring; Video-polysomnography 1. Introduction Several sleep-related respiratory and motor disturbances have been reported in multiple system atrophy (MSA). Subjective sleep complaints reported by patients or relatives include insomnia, excessive daytime sleepiness (EDS), snoring or other respiratory noises, and motor restlessness while asleep, sleep talking or overt violent behaviours [1]. Video-polysomnographic recordings (VPSG) demonstrate abnormal sleep architecture, respiratory disturbances such as nocturnal alveolar hypoventilation [2–4], obstructive and central sleep apnoeas [5–8] and nocturnal stridor [9–13] and motor abnormalities including periodic limb move- ments during sleep (PLMS) [14] and REM sleep behaviour disorder (RBD), the latter often forerunning the disease [15–19]. The relation between abnormal motor control and sleep- related breathing abnormalities in MSA, and the occurrence in the same patient of sleep-related breathing and motor abnormalities have not been systematically analysed, except by questionnaire analysis [1], which may be open to criticism when not checked against VPSG recordings. We performed VPSG recordings in 19 consecutive MSA patients, monitoring respiration, heart (HR) and breathing rate (BR) and limb muscular EMG activity, to define the extent and reciprocal relation of sleep-related autonomic and motor disturbances in MSA. 1389-9457/$ - see front matter q 2003 Elsevier B.V. All rights reserved. doi:10.1016/j.sleep.2003.07.002 Sleep Medicine 5 (2004) 21–30 www.elsevier.com/locate/sleep * Corresponding author. Tel.: þ39-051-644-2225; fax: þ39-051-644-2165. E-mail address: [email protected] (R. Vetrugno).

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Original article
Sleep disorders in multiple system atrophy: a correlative
video-polysomnographic study
Roberto Vetrugnoa,*, Federica Provinia, Pietro Cortellib, Giuseppe Plazzia,Enrico M. Lottia, Giulia Pierangelia, Carlotta Canalia, Pasquale Montagnaa
aDepartment of Neurological Sciences, University of Bologna, Via Ugo Foscolo 7, Bologna 40123, ItalybInstitute of Clinical Neurology, University of Modena and Reggio Emilia, Via Dal Pozzo, Modena 41100, Italy
Received 12 February 2003; received in revised form 17 June 2003; accepted 20 July 2003
Abstract
Objective: The reciprocal relation between breathing, heart and motor system abnormalities during sleep was studied in multiple system
atrophy (MSA) by means of video-polysomnographic recordings (VPSG).
Patients and Methods: Nineteen consecutive MSA patients underwent VPSG with scoring for sleep, respiratory abnormalities, heart (HR)
and breathing (BR) rates, and abnormal motor activities. A comparative analysis was performed versus 10 patients with obstructive sleep
apnoea syndrome (OSAS).
Results: All MSA patients displayed snoring, 42% stridor, and 37% OSAS. Mean sleep SaO2 was 92.7%, and lowest SaO2 86%. Patients
with stridor had a significant increase in BR from Wake to NREM and REM sleep, and higher HR during sleep. Respiratory muscles and
tibialis anterior EMG tonic activity was frequently found, more often in patients with stridor. All patients had REM sleep behaviour disorders
(RBD) and 88% periodic limb movements during sleep (PLMS). No OSAS patient had RBD or respiratory muscles and tibialis anterior tonic
activity.
Conclusions: MSA patients, especially those with associated stridor, commonly display impaired breathing and abnormal control of
respiratory and limb muscles during sleep. Breathing and motor abnormalities are often concomitant in the same patient, indicating a diffuse
impairment of sleep homeostatic integration that should be included within the diagnostic features of MSA.
q 2003 Elsevier B.V. All rights reserved.
Keywords: Multiple system atrophy; Sleep; Stridor; Snoring; Video-polysomnography
1. Introduction
Several sleep-related respiratory and motor disturbances
have been reported in multiple system atrophy (MSA).
Subjective sleep complaints reported by patients or relatives
include insomnia, excessive daytime sleepiness (EDS),
snoring or other respiratory noises, and motor restlessness
while asleep, sleep talking or overt violent behaviours [1].
Video-polysomnographic recordings (VPSG) demonstrate
abnormal sleep architecture, respiratory disturbances such
as nocturnal alveolar hypoventilation [2–4], obstructive and
central sleep apnoeas [5–8] and nocturnal stridor [9–13]
and motor abnormalities including periodic limb move-
ments during sleep (PLMS) [14] and REM sleep behaviour
disorder (RBD), the latter often forerunning the disease
[15–19].
The relation between abnormal motor control and sleep-
related breathing abnormalities in MSA, and the occurrence
in the same patient of sleep-related breathing and motor
abnormalities have not been systematically analysed, except
by questionnaire analysis [1], which may be open to
criticism when not checked against VPSG recordings.
We performed VPSG recordings in 19 consecutive MSA
patients, monitoring respiration, heart (HR) and breathing
rate (BR) and limb muscular EMG activity, to define the
extent and reciprocal relation of sleep-related autonomic
and motor disturbances in MSA.
1389-9457/$ - see front matter q 2003 Elsevier B.V. All rights reserved.
doi:10.1016/j.sleep.2003.07.002
Sleep Medicine 5 (2004) 21–30
www.elsevier.com/locate/sleep
* Corresponding author. Tel.:þ39-051-644-2225; fax:þ39-051-644-2165.
E-mail address: [email protected] (R. Vetrugno).
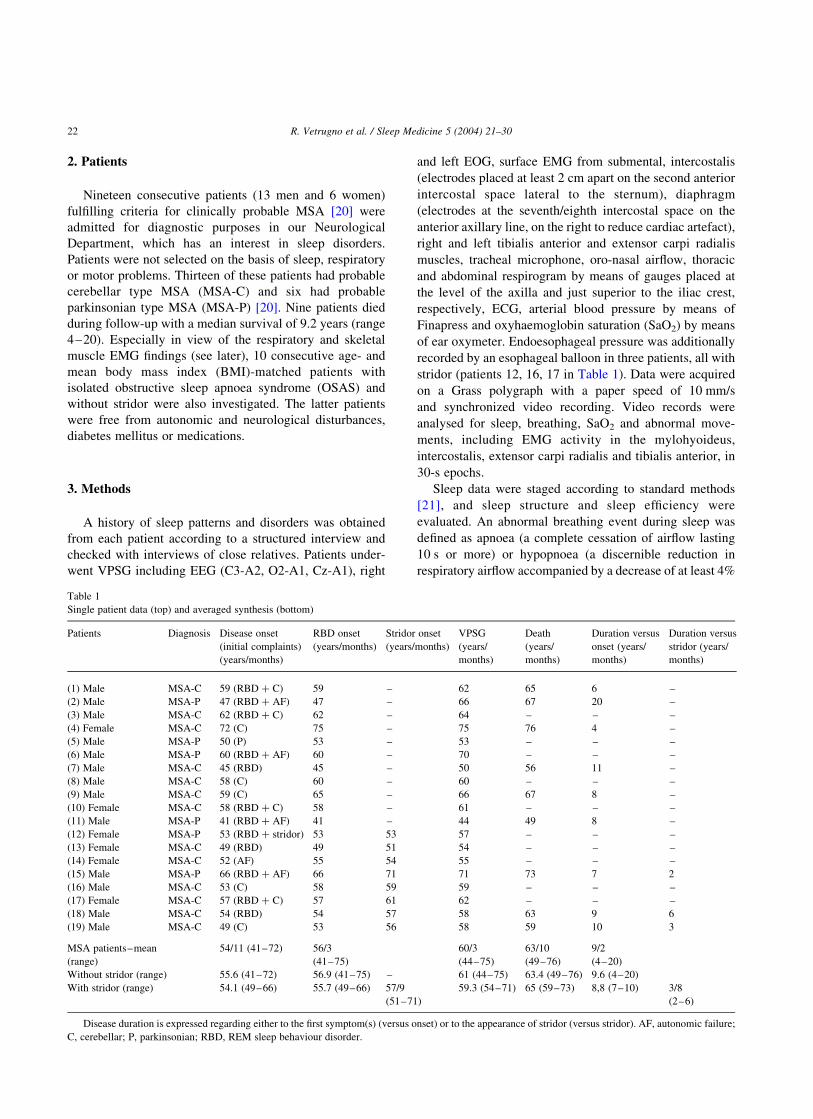
2. Patients
Nineteen consecutive patients (13 men and 6 women)
fulfilling criteria for clinically probable MSA [20] were
admitted for diagnostic purposes in our Neurological
Department, which has an interest in sleep disorders.
Patients were not selected on the basis of sleep, respiratory
or motor problems. Thirteen of these patients had probable
cerebellar type MSA (MSA-C) and six had probable
parkinsonian type MSA (MSA-P) [20]. Nine patients died
during follow-up with a median survival of 9.2 years (range
4–20). Especially in view of the respiratory and skeletal
muscle EMG findings (see later), 10 consecutive age- and
mean body mass index (BMI)-matched patients with
isolated obstructive sleep apnoea syndrome (OSAS) and
without stridor were also investigated. The latter patients
were free from autonomic and neurological disturbances,
diabetes mellitus or medications.
3. Methods
A history of sleep patterns and disorders was obtained
from each patient according to a structured interview and
checked with interviews of close relatives. Patients under-
went VPSG including EEG (C3-A2, O2-A1, Cz-A1), right
and left EOG, surface EMG from submental, intercostalis
(electrodes placed at least 2 cm apart on the second anterior
intercostal space lateral to the sternum), diaphragm
(electrodes at the seventh/eighth intercostal space on the
anterior axillary line, on the right to reduce cardiac artefact),
right and left tibialis anterior and extensor carpi radialis
muscles, tracheal microphone, oro-nasal airflow, thoracic
and abdominal respirogram by means of gauges placed at
the level of the axilla and just superior to the iliac crest,
respectively, ECG, arterial blood pressure by means of
Finapress and oxyhaemoglobin saturation (SaO2) by means
of ear oxymeter. Endoesophageal pressure was additionally
recorded by an esophageal balloon in three patients, all with
stridor (patients 12, 16, 17 in Table 1). Data were acquired
on a Grass polygraph with a paper speed of 10 mm/s
and synchronized video recording. Video records were
analysed for sleep, breathing, SaO2 and abnormal move-
ments, including EMG activity in the mylohyoideus,
intercostalis, extensor carpi radialis and tibialis anterior, in
30-s epochs.
Sleep data were staged according to standard methods
[21], and sleep structure and sleep efficiency were
evaluated. An abnormal breathing event during sleep was
defined as apnoea (a complete cessation of airflow lasting
10 s or more) or hypopnoea (a discernible reduction in
respiratory airflow accompanied by a decrease of at least 4%
Table 1
Single patient data (top) and averaged synthesis (bottom)
Patients Diagnosis Disease onset
(initial complaints)
(years/months)
RBD onset
(years/months)
Stridor onset
(years/months)
VPSG
(years/
months)
Death
(years/
months)
Duration versus
onset (years/
months)
Duration versus
stridor (years/
months)
(1) Male MSA-C 59 (RBD þ C) 59 – 62 65 6 –
(2) Male MSA-P 47 (RBD þ AF) 47 – 66 67 20 –
(3) Male MSA-C 62 (RBD þ C) 62 – 64 – – –
(4) Female MSA-C 72 (C) 75 – 75 76 4 –
(5) Male MSA-P 50 (P) 53 – 53 – – –
(6) Male MSA-P 60 (RBD þ AF) 60 – 70 – – –
(7) Male MSA-C 45 (RBD) 45 – 50 56 11 –
(8) Male MSA-C 58 (C) 60 – 60 – – –
(9) Male MSA-C 59 (C) 65 – 66 67 8 –
(10) Female MSA-C 58 (RBD þ C) 58 – 61 – – –
(11) Male MSA-P 41 (RBD þ AF) 41 – 44 49 8 –
(12) Female MSA-P 53 (RBD þ stridor) 53 53 57 – – –
(13) Female MSA-C 49 (RBD) 49 51 54 – – –
(14) Female MSA-C 52 (AF) 55 54 55 – – –
(15) Male MSA-P 66 (RBD þ AF) 66 71 71 73 7 2
(16) Male MSA-C 53 (C) 58 59 59 – – –
(17) Female MSA-C 57 (RBD þ C) 57 61 62 – – –
(18) Male MSA-C 54 (RBD) 54 57 58 63 9 6
(19) Male MSA-C 49 (C) 53 56 58 59 10 3
MSA patients–mean
(range)
54/11 (41–72) 56/3
(41–75)
60/3
(44–75)
63/10
(49–76)
9/2
(4–20)
Without stridor (range) 55.6 (41–72) 56.9 (41–75) – 61 (44–75) 63.4 (49–76) 9.6 (4–20)
With stridor (range) 54.1 (49–66) 55.7 (49–66) 57/9
(51–71)
59.3 (54–71) 65 (59–73) 8,8 (7–10) 3/8
(2–6)
Disease duration is expressed regarding either to the first symptom(s) (versus onset) or to the appearance of stridor (versus stridor). AF, autonomic failure;
C, cerebellar; P, parkinsonian; RBD, REM sleep behaviour disorder.
R. Vetrugno et al. / Sleep Medicine 5 (2004) 21–3022

in SaO2) [22–24]. The average number of apnoea–
hypopnoea episodes per hour of sleep was the respiratory
disturbance index (RDI). As a criterion for OSAS, we chose
an RDI above 10, which is an accepted international scoring
standard [24–26].
Respiratory noise was inspiratory when synchronous
with down-deflection of oral and thoracic-abdominal
respiratory traces representing inspiration and with inter-
costal EMG burst activity; expiratory if synchronous with
up-deflection of respiratory traces and positive excursion of
endoesophageal pressure. Stridor was defined as a strained,
high-pitched, harsh respiratory sound on audio–video
monitoring. Paradoxical breathing (PB) was identified as a
phase-out of thoracic as opposed to abdominal respiratory
traces [24]. Sleep time with snoring or with stridor was
arbitrarily defined as the number of epochs with at least 50%
of respiratory movements associated with snoring or stridor,
and the percentage of time of snoring (sleep time with
snoring/total sleep time) and percentage of time of stridor
(sleep time with stridor/total sleep time) were then
calculated. Intercostalis EMG activity was evaluated and
limb EMG activity was scored for PLMS according to
Coleman’s criteria [27]: a series of four or more consecutive
movements lasting 0.5–5 s with an intermovement interval
of 4–90 s. The PLMS index (number of PLMS per hour of
sleep) was calculated. EMG activity of tonic type (in the
shape either of continuous muscle recruitment pattern or of
repetitive uninterrupted motor unit potentials at rates greater
than 5–7 impulses per second [28]) on the tibialis anterior,
mylohyoideus, and intercostalis muscles was analysed and
scored whenever it was present in at least two consecutive
epochs. Given its high frequency among MSA patients (see
later) and to ensure reliability, it was arbitrarily scored as
pathological when present in at least one third of total VPSG
epochs. PLMS and other simple or complex motor events
during sleep, in particular REM behavioral disorders
(RBD), the latter defined according to Mahowald and
Schenck [29], were checked against the video recordings.
Mean HR and mean BR were calculated for every 5 min
of noise and/or artefact-free epochs.
Ten OSAS patients were subjected to the same
procedures as the MSA patients. Endoesophageal pressure
was obtained in all of them.
Statistical analysis was done with non-parametric tests of
significance (the Wilcoxon test for continuous variables and
the Mann –Whitney test for nominal variables). We
considered statistically significant P values of less than
0.05 ðP , 0:05Þ:
4. Results
4.1. MSA: subjective complaints and clinical findings
All patients complained of autonomic symptoms and 15
had mild–moderate symptomatic postural hypotension
(dizziness, syncope and visual disturbances). The most
frequent sleep-related subjective complaints were abnormal
violent motor behaviours during sleep and respiratory
noises.
Eight out of the 19 patients (42%), six with MSA-C
(three men) and two with MSA-P (one man) complained of
nocturnal stridor upon admission. Mean BMI was 25.9 (24.1
in patients without stridor). Remarkably, RBD was reported
as the initial (or among the initial) complaints of disease in
12 patients, and in three patients isolated RBD had preceded
other symptoms by 2–15 years. Diurnal and nocturnal
irregular respiration, e.g. gasp, snoring and respiratory
stridor, were a complaint in 10 patients. None of these
symptoms was, however, the cause for referral, evaluation
or admission.
Mean age at disease onset was slightly lower in patients
with stridor (54.1 versus 55.6 years), and disease duration
shorter in patients with stridor (8.8 versus 9.6 years).
Patients with stridor had RBD earlier than patients without
stridor (55.7 versus 56.9 years, Table 1). These differences
between MSA with and without stridor were not significant.
4.2. MSA: VPSG findings
4.2.1. Sleep structure
Sleep structure was characterized by increased NREM
sleep stages 1–2 (63%, n.v. 45–55%), decreased stages 3–4
(12%, n.v. 15–25%) and a normal amount of REM sleep
(25%, n.v. 20–25%) [30]. Sleep efficiency was reduced
(52%; n.v. . 85%). Except for sleep latency, there were no
differences in sleep structure between patients with and
without sleep-related respiratory disturbances.
4.2.2. Respiratory abnormalities
All patients displayed inspiratory noise during sleep:
snoring in 100%, stridor in 42%. The mean sleep RDI was
10.6 in the whole group of MSA patients, with significant
differences between NREM (mean RDI 11.9) and REM
sleep (mean RDI 6.3, P ¼ 0:01, Table 2). Only seven MSA
patients had a sleep RDI higher than 10, thus fulfilling the
criterion adopted in this study for a diagnosis of OSAS
[24–26]. Of these seven patients, four did not display
nocturnal stridor, and could thus be categorized as OSAS-
only MSA patients; three patients with stridor had
concomitant OSAS (Table 2).
The three patients with stridor (patients 12, 16, 17,
Tables 1 and 2) who had endoesophageal pressure
measurements showed mean negative values during sleep
ranging from 24 to 224 cm H2O (mean 214 cm H2O,
n.v. $ 2 4 cm H2O) [31], suggesting increased sleep-
related respiratory effort.
For the whole group of patients, mean SaO2 throughout
sleep remained at 92.7%, with the lowest values at 82%.
SaO2 was not especially reduced during REM sleep. Mean
SaO2 during sleep remained practically the same in patients
with and without stridor and there was no significant mean
R. Vetrugno et al. / Sleep Medicine 5 (2004) 21–30 23

SaO2 difference between MSA with and without OSAS
(Table 2).
PB (Fig. 1) was found in about half of the patients, more
frequent in patients with stridor (Table 2). Expiratory noise
was present in 74% of the patients, accompanied in all with
expiratory intercostalis EMG activation. All patients with
stridor showed expiratory intercostalis EMG activation
associated with concomitant slightly positive endoesopha-
geal pressure (Fig. 2). Stridor persisted also during relaxed
wakefulness in six out of the eight (75%) patients with
nocturnal stridor.
4.2.3. Breathing and heart rates
The mean BR while awake in the whole group of MSA
patients was 19 ^ 4 cycles/min, with increases during
NREM and REM sleep (Table 3). Though slight,
differences between REM, Wake and NREM sleep were
significant ðP , 0:05Þ: The increased rates during sleep
were, however, due to the presence of the stridor subgroup:
patients with stridor had BR comparable to patients
without stridor during Wake but higher rates during both
NREM and REM sleep when compared to patients without
stridor and to Wake values (the latter differences being
statistically significant, P , 0:05), whereas patients with-
out stridor showed significantly lower BR during NREM
versus REM sleep ðP , 0:05Þ but not versus Wake
(Table 3).
Mean HR was 70 ^ 10 beats/min during Wake, decreas-
ing during NREM and REM sleep for the whole group of
patients, differences between Wake and NREM and
between NREM and REM being significant (P , 0:05;
Table 3). There were no significant differences between
patients with and without stridor in mean HR during the
various Wake and sleep stages. However, patients with
stridor showed no significant decrease during NREM and
higher HR during REM sleep compared to Wake, while
patients without stridor had significantly lower HR between
Wake and NREM sleep (P , 0:05; Table 3).
Oscillations of HR and arterial pressure related to the
respiratory events, whether snoring, sleep apneas or stridor,
were notably blunted in MSA patients especially when
compared with the OSAS controls (Fig. 3). No effort,
however, was made to quantify these changes.
4.2.4. Motor activity, PLMS, RBD
Intercostalis EMG tonic activity in the shape of
subcontinuous muscle recruitment patterns and repetitive
motor unit potential discharges (Fig. 4) was scored in most
of MSA patients during Wake, decreasing but still present
during NREM and even during REM sleep (Table 4).
Tibialis anterior tonic EMG activity (continuous EMG
activity and repetitive motor unit potential discharges) was
recorded in 17 out of 19 patients with MSA (6 with stridor
and 11 without stridor) again more prevalent among patients
Table 2
Sleep-related quantitative respiratory and PLMS findings: single patient data and averaged synthesis
Patients Stridor Sleep Eff
(%)
PB Sleep RDI NREM
RDI
REM
RDI
Mean SaO2
(%)
Lowest
SaO2 (%)
Mean NREM
SaO2 (%)
Mean REM
SaO2 (%)
Time
snoring
(%)
Time
stridor
(%)
PLMS
index
(1)a – 38.1 Yes 15a 16.9 0 91a 88 91 90 30.4 – 24.3
(2) – 72.5 Yes 6.9 6.9 7.1 90.7 86 90.6 91.8 70.5 – 60.8
(3) – 17.7 4.0 0 7.1 95.8 94 96 95.8 32 – 48
(4) – 30.9 8.4 6.4 11 90.4 88 91.4 89.6 20.7 – 41.3
(5)a – 76.7 17.8a 18.5 14.1 93.3a 90 93.4 93 39.7 – 76.1
(6) – 73.4 1.5 1.8 0 93.6 93 93.6 92 46 – 26
(7)a – 85.4 21a 26.9 5.6 92.6a 90 92.5 93.9 14.9 – 24.9
(8) – 51.7 Yes 6.7 8.7 0 95.5 94 95.5 95 90 – 19.2
(9)a – 18.7 17.6a 22.2 3 95.2a 92 95.1 96 33 – 14.5
(10) – 67.9 Yes 1.5 2.4 0 92.6 88 92.6 92 46 – 28
(11) – 51.2 3 3.5 0 94.3 88 94.3 94 48 – 16
(12) Stridor 46.5 Yes 4.3 4 8.6 90 86 91 89 22.2 67 26
(13) Stridor 39.3 Yes 8 8.3 6.7 94.7 92 94.7 95 28.7 36.3 33.3
(14) Stridor 78.9 5.2 5.2 5.2 94.7 90 94.7 95 2.9 34.1 43
(15)a Stridor 73.8 Yes 16.1a 16.6 10 89.2a 82 89.3 87.8 23 23 NA
(16)a Stridor 26.5 Yes 15.5a 16.9 10 89.3a 88 89.2 90 56.3 40 NA
(17) Stridor 63.5 Yes 5.2 6.1 4.5 89.2 86 89.1 89.3 5.7 93 38
(18) Stridor 51.7 7 9 1 94.6 92 94.6 95 48.8 47 34
(19)a Stridor 29.0 Yes 36.9a 45.6 25.1 94.5a 92 94.7 94.1 57.7 26.9 20
Mean 52.3 53% 10.6 11.9 6.3 92.7 92.8 92.5 37.7 33.7
Without stridor 53.1 36% 9.4 10.4 4.4 93.2 93.3 93 42.8 34.4
With stridor 51.2 75% 12.3 14 8.9 92 92.1 91.9 30.6 45.9 32.3
Sleep Eff, sleep efficiency; RDI, respiratory disturbance index; SaO2, oxyhaemoglobin saturation; PB, paradoxical breathing; PLMS, periodic limb
movement during sleep. NA, not available.a Marks patient with concomitant OSAS (RDI . 10).
R. Vetrugno et al. / Sleep Medicine 5 (2004) 21–3024

during Wake, but still present during NREM and also REM
sleep. Both intercostalis and tibialis anterior EMG activity
were more frequent in patients with stridor. PLMS were
present in 88% of patients and in all patients with stridor,
with varying but always abnormal PLMS index (n.v. # 5,
Tables 2 and 4).
All MSA patients showed continuous EMG activity
and repetitive motor unit potential discharges in the
submental mylohyoideus muscle while awake and during
sleep, with phasic or tonic increase during REM sleep.
Excessive chin muscle tone persisted throughout sleep
(Table 4). EMG twitching during REM sleep could be
synchronous or asynchronous with complex limb move-
ments. Sometimes bursts of EMG activity on the
mylohyoideus muscle could recur synchronously with
brief central apnoeas during wake and sleep.
RBD in the form of complex motor behaviours such as
limb and body jerks or complex vigorous movements were
recorded in all patients (Table 4).
4.3. Comparative analysis of MSA versus OSAS patients
Ten OSAS patients had a mean of BMI 25.9 (range
25.1–26.8), a mean age of 56.5 years (range 54–61) and
a mean disease duration of 4 years (range 1–10); all
these values were not significantly different from our
MSA patients.
Sleep structure showed prevalent stages 1–2 NREM
sleep (67%, n.v. 50%), and reduced stages 3–4 NREM
(17%, n.v. 25%) and REM sleep (16%, n.v. 25%) with sleep
efficiency of 83% (n.v. . 85%). Mean RDI was 47 (range:
21–58, 38 during NREM and 55 during REM sleep), and
mean SaO2 86%, dropping to 81% during REM sleep. Mean
sleep-apnea related endoesophageal pressure negative value
was 230 cm H2O (range 220 to 260 cm H2O), values
significantly worse than our MSA patients ðP , 0:05Þ:
Typical oscillations of HR and arterial pressure
accompanied each apnoea event (Fig. 3). None of the
OSAS patients showed expiratory intercostalis EMG
activity or tonic intercostalis or tibialis anterior EMG
activity and/or repetitive motor unit potentials discharges
either while awake or during sleep, whereas 60% of them
displayed PLMS. All of the OSAS patients showed
physiological atonia without abnormal motor behaviour
during REM sleep (Table 4).
5. Discussion
5.1. Wake–sleep architecture and parameters
Our patients with MSA had abnormal sleep structure,
with reduced NREM deep sleep and decreased sleep
efficiency. Though these findings probably relate at least
Fig. 1. NREM sleep recording (excerpts) in an MSA-C patient (no. 16) shows inspiratory and expiratory noise. Hypopnoeas and paradoxical breathing, marked
by the asterisk (*) are present with slightly positive endoesophageal pressure and minimal SaO2 variability. EOG, electro-oculogram; mylohyoid.,
mylohyoideus muscle; ECG, electrocardiogram; microph., microphone; Interc., intercostalis muscle; Thor., thoracic; Abd., abdominal; resp., respiration;
intraoesoph. press., endoesophageal pressure; system. art. press., systemic arterial pressure; SaO2, oxyhaemoglobin saturation.
R. Vetrugno et al. / Sleep Medicine 5 (2004) 21–30 25

in part to a first night effect, the decreased sleep efficiency,
striking in MSA compared to the OSAS patients who were
subjected to the same procedures, seems to indicate that lack
of sleep is characteristic of MSA, and cannot be attributed
entirely to the disturbing effects of our investigational
procedures.
Lack of sleep is also a potentially relevant finding when
trying to explain the prevalence of sleep-related respiratory
abnormalities in MSA. Indeed sleep disruption may
promote sleep apnea. Such a possibility cannot be
discounted in our patients, even though a comparison of
the sleep efficiency with RDI did not disclose any obvious
correlation in our MSA patients (Table 2).
5.2. Respiratory abnormalities during sleep
Significant findings in our MSA sample were the high
rates of respiratory disturbances observed during sleep.
Inspiratory noise was universal, while noise upon expiration
was found in nearly 4/5 of patients. More relevantly, stridor
was found in nearly half of our patients, while, based on our
adopted diagnostic criterion for OSAS (RDI above 10), 37%
had OSAS. Remarkably, patients spent more than 1/3 or
nearly 1/2 of their sleep time snoring or with stridor. OSAS
and stridor were not always coincidental, since four patients
had OSAS only in the absence of stridor. Stridor also
persisted also during relaxed wakefulness in 75% of
patients. These sleep-related respiratory disturbances in
MSA remained generally unassociated with marked SaO2
changes, especially when MSA was compared to OSAS.
Mild (93.3%) O2 desaturation, however, occurred during
sleep in MSA even unassociated with OSAS or stridor,
indicating that sleep-related O2 desaturation may be
intrinsic to the disease. SaO2 was only slightly worsened
in MSA associated with OSAS (mean SaO2 at 92.1%) or
Fig. 2. NREM sleep recording (excerpts) in an MSA-C patient (no. 17) with inspiratory stridor (microph.). Abbreviations as per Fig. 1. Note the additional
intercostalis (interc.) expiratory activation with concomitant slightly positive endoesophageal pressure, the normal thoracic and abdominal respiratory traces
and the absence of significant SaO2 changes.
Table 3
Mean breathing and heart rates during Wake, NREM and REM sleep
Wake
(mean ^ SD)
NREM sleep
(mean ^ SD)
REM sleep
(mean ^ SD)
Mean breathing rate
MSA patients (no. 19) 19 ^ 4 20 ^ 6 21 ^ 5
Without stridor (no. 11) 19 ^ 2 18 ^ 3 19 ^ 3
With stridor (no. 8) 19 ^ 5 23 ^ 8 23 ^ 9
Mean heart rate
MSA patients (no. 19) 70 ^ 10 67 ^ 11 69 ^ 11
Without stridor (no. 11) 69 ^ 10 65 ^ 10 66 ^ 10
With stridor (no. 8) 72 ^ 11 71 ^ 13 73 ^ 12
SD, standard deviation.
R. Vetrugno et al. / Sleep Medicine 5 (2004) 21–3026

stridor (mean SaO2 at 92.6%). Noticeably, our MSA
patients did not demonstrate worsened SaO2 during REM
sleep and the mean RDI observed during NREM sleep was
higher than during REM sleep, an unusual finding when
compared to the opposite pattern typical of OSAS and
confirmed also in our cohort of OSAS controls. Except for
further emphasizing that REM sleep is distinctly abnormal
in MSA, these latter findings remain difficult to explain.
Finally, sleep-related respiratory disturbances, in particular
stridor, were more frequent in MSA type C.
Fig. 3. Polygraphic recordings in MSA-C patient (no. 16, panel A) show markedly blunted systemic blood pressure oscillations related to the respiratory events
when compared to OSAS (panel B). Abbreviations as per Fig. 1. Time scale is identical in the two panels.
Fig. 4. NREM sleep recordings (excerpts) in MSA type C patient (patient no. 3) showing subcontinuous motor unit potential discharges in the intercostalis and,
to a lesser extent, tibialis anterior muscles EMG. Abbreviations as per Fig. 1. Delt, deltoid muscle; tib, tibialis anterior.
R. Vetrugno et al. / Sleep Medicine 5 (2004) 21–30 27

5.3. Heart and breathing rates
When considering BR and HR, patients with stridor,
already tachypnoic during Wake, had a significant increase
in BR from Wake to NREM and REM sleep. Moreover,
their HR did not significantly decrease in NREM and
actually increased in REM sleep. These findings, striking in
the face of the characteristic fixed pulse rate in MSA,
indicate impaired sleep state-related heart and respiratory
regulation [32–34] in MSA with stridor. In agreement with
the autonomic denervation typical of MSA, however, the
oscillations in HR and blood pressure associated with the
respiratory events were markedly blunted. Abnormal
circadian variations in HR with decreased correlation
between HR and blood pressure have already been reported
in MSA [35]. Our BR findings are also in good agreement
with Isono et al. who reported increased respiratory
frequency during sleep compensating for a reduction of
tidal volume in MSA with stridor [36].
5.4. Motor abnormalities
Major findings of our study were also the abnormal
motor patterns involving limb and respiratory muscles
during sleep. Sustained EMG activity in the intercostalis
muscle, especially during wake but persisting throughout
sleep, was present in MSA patients, in particular those with
stridor. Together with intercostalis expiratory EMG acti-
vation and PB, these findings indicate a pathological sleep-
related respiratory muscle pattern. EMG tonic activity was
not, however, restricted to muscles related to respiration but
also involved skeletal limb muscles such as the tibialis
anterior, in which both tonic discharges of motor unit EMG
potentials and more complex patterns of PLMS were found.
This respiratory and limb motor overactivity throughout
wake and sleep was always more prevalent in MSA with
stridor. Finally, RBD was found in all of our MSA patients.
We entertained the hypothesis that the increased EMG
activity could be due to increased respiratory effort. None of
the 10 OSAS patients, however, in whom airflow restriction
and respiratory effort as measured by endoesophageal
balloon, were clearly more severe, presented sustained
tonic type intercostalis and tibialis anterior EMG activity
during wake or sleep; none had RBD or abnormal lack of
atonia during REM sleep. This clearly shows that the
abnormal sustained EMG activity of respiratory and limb
muscles in MSA does not simply relate to increased
respiratory effort. We think that it reflects central overactive
and disordered motor output, which could best be defined as
a kind of dystonia. Recent EMG data indeed suggest that
stridor in MSA is not simply due to denervation of laryngeal
muscles but rather to abnormal motor control similar to
dystonia [37]. We also consider that the universal
presence of RBD in MSA fits this interpretation of the
EMG findings, reflecting dysfunction in inhibitory brain-
stem pathways [38,39].
5.5. Final considerations
Our data show that disordered breathing and abnormal
motor control during sleep are common and often associated
features in MSA. The clinical relevance of these findings is
underlined by their high prevalence in our cohort of patients,
who were not expressely selected for respiratory or motor
disturbances during sleep. Respiratory and motor sleep-
related abnormalities should rightly be incorporated within
the useful diagnostic markers of the disease [20]. In MSA
with stridor in particular, abnormal breathing patterns and
motor abnormalities during sleep represent a constant
feature found concomitantly in all of our patients.
Our study allows for some pathophysiological consider-
ations on the relevance of stridor in MSA. Stridor is related
to a poorer prognosis in MSA, but how exactly this happens
remains unclear. Recordings in nine MSA patients with
stridor demonstrated airflow limitation only during inspira-
tion, associated with laryngeal narrowing and phasic
inspiratory thyro-arytenoid (TA) muscle EMG activity
[36]. Since TA is reflexively activated in normal subjects
by external resistive loads, stridor in MSA was considered
to result from hyperactivity of the TA uncontrasted by the
denervated posterior crico-arytenoid muscles, which are
the vocal cord abductors. Indeed CPAP, by abolishing the
resistive load, abolished the abnormal TA activity and
stridor [36]. The posterior crico-arytenoid muscles were not,
however, specifically searched for denervation in this study
[36]. Stridor in MSA is thus associated with laryngeal
narrowing, at variance with OSAS, in which obstruction in
airflow occurs at several levels in the pharynx [40–43].
Table 4
EMG activity in MSA and OSAS patients expressed as percentage of patients having such activity during wake, NREM sleep and REM sleep
Intercostalis EMG
activity (%)
Tibialis anterior EMG
activity (%)
PLMS (%) Mylohyoideus EMG activity RBD (%)
Wake NREM REM Wake NREM REM Wake NREM REM
MSA patients (no. 19) 89 79 37 76 65 24 88 100 100 100 100
Without stridor (no. 11) 91 64 27 73 55 18 82 100 100 100 100
With stridor (no. 8) 87 100 50 83 83 33 100 100 100 100 100
OSAS patients (no. 10) 0 0 60 Atonia in REM sleep 0
TA, tibialis anterior; PLMS, periodic limb movement during sleep; RBD, REM sleep behaviour disorder.
R. Vetrugno et al. / Sleep Medicine 5 (2004) 21–3028

SaO2 and endoesophageal pressure values during sleep
were not, however, particularly severe in MSA with stridor,
and mild when compared to OSAS. In our opinion, stridor
just represents a harbinger of severe changes in autonomic
centres controlling respiration and other vital functions,
accounting for death in MSA. Recently, impaired chemo-
sensitivity to hypoxia was reported as an early marker and a
risk factor for respiratory failure and sudden death in MSA
patients, independently of any mechanical airway obstruc-
tive factors [44]. Our patients had a mild degree of O2
desaturation during sleep even in the absence of stridor or
OSAS. If the impaired chemoceptor response to hypoxia
makes MSA patients unable to compensate for worsening
ventilatory insufficiency, even slight additional O2 desatura-
tion due to the combined effects of sleep and stridor or
OSAS may then prove fatal. These considerations beg the
still unanswered question of the type, timing and extent of
assisted ventilation needed to overcome the sleep-related
respiratory disturbances and the risk for sudden death
in MSA.
Acknowledgements
A. Laffi gave invaluable secretarial help, and A. Collins
corrected the English manuscript. Supported by MURST
ex-60% 2000, MURST ex-40% cofin 2000 prot.
MM06244347_004 and MURST ex-40% cofin 1999 prot.
9906037938 grants.
References
[1] Ghorayeb I, Yekhlef F, Chrysostome V, et al. Sleep disorders and their
determinants in multiple system atrophy. J Neurol Neurosurg
Psychiatry 2002;72:798–800.
[2] Chokroverty S. Sleep, breathing and neurological disorders. In:
Chokroverty S, editor. Sleep disorders medicine. Boston, MA:
Butterworth-Heineman; 1994. p. 295–335.
[3] Williams A, Hanson D, Calne DB. Vocal cord paralysis in the Shy-
Drager syndrome. J Neurol Neurosurg Psychiatry 1979;42:151–3.
[4] Chester CS, Gottfried SB, Cameron DI, Strohl KP. Pathophysiological
findings in a patient with Shy-Drager and alveolar hypoventilation
syndromes. Chest 1988;94:212–4.
[5] Castaigne P, Laplane D, Autret A, et al. Shy-Drager syndrome with
disturbances of the respiratory rhythm and consciousness. A propos of
an anatomo-clinical case. Rev Neurol 1977;133:455–6.
[6] Guilleminault C, Lehrman AT, Forno L, Dement WC. Sleep apnoea
syndrome: states of sleep and autonomic dysfunction. J Neurol
Neurosurg Psychiatry 1977;40:718–25.
[7] McNicholas WT, Rutherford R, Grossman R, et al. Abnormal
respiratory pattern generation during sleep in patients with autonomic
dysfunction. Am Rev Respir Dis 1983;128:429–33.
[8] Chokroverty S, Sachdeo R, Masdeu J. Autonomic dysfunction and
sleep apnea in olivopontocerebellar degeneration. Arch Neurol 1984;
41:926–31.
[9] Teravainen H, Udd B. Vocal cord paralysis in the Shy-Drager
syndrome. Acta Neurol Scand 1982;66:505–7.
[10] Martinovits G, Leventon G, Goldhammer Y, Sadeh M. Vocal cord
paralysis as a presenting sign in the Shy-Drager syndrome. J Laryngol
Otol 1988;102:280–1.
[11] Sadaoka T, Kakitsuba N, Fujiwara Y, et al. Sleep-related breathing
disorders in patients with multiple system atrophy and vocal fold
palsy. Sleep 1996;19:479–84.
[12] Wenning GK, Tison F, Ben-Shlomo Y, et al. Multiple system atrophy:
a review of 203 pathologically proven cases. Mov Disord 1997;12:
133–47.
[13] Kakitsuba N, Sadaoka T, Kanai R, et al. Peculiar snoring in patients
with multiple system atrophy: its sound source, acoustic character-
istics and diagnostic sygnificance. Ann Otol Rhinol Laryngol 1997;
106:380–4.
[14] Wetter TC, Collado-Seidel V, Pollmacher T, et al. Sleep and periodic
leg movement patterns in drug-free patients with Parkinson’s disease
and multiple system atrophy. Sleep 2000;23:361–7.
[15] Tachibana N, Kimura K, Kitajima K, et al. REM sleep without atonia
at early stage of sporadic olivopontocerebellar atrophy. J Neurol Sci
1995;132:28–34.
[16] Tison F, Wenning GK, Quinn NP, Smith SJ. REM sleep behaviour
disorder as the presenting symptom of multiple system atrophy.
J Neurol Neurosurg Psychiatry 1995;58:379–80.
[17] Plazzi G, Corsini R, Provini F, et al. REM sleep behaviour disorders in
multiple system atrophy. Neurology 1997;48:1094–7.
[18] Plazzi G, Cortelli P, Montagna P, et al. REM sleep behaviour
disorders differentiates pure autonomic failure from multiple system
atrophy with autonomic failure. J Neurol Neurosurg Psychiatry 1998;
64:683–5.
[19] Olson EJ, Boeve BF, Silber MH. Rapid eye movement sleep
behaviour disorders: demographic, clinical and laboratory findings
in 93 cases. Brain 2000;123:331–9.
[20] Gilman S, Low PA, Quinn A, et al. Consensus statement on diagnosis
of multiple system atrophy. J Neurol Sci 1999;163:94–8.
[21] Rechtschaffen A, Kales A. A manual of standardized terminology,
techniques and scoring system for sleep stages of human subjects. Los
Angeles: Brain Information Service, Brain Research Institute; 1968.
[22] Guilleminault C, van den Hoed J, Mitler MM. In: Guilleminault C,
Dement C, editors. Sleep apnea syndromes. New York: Alan R. Liss;
1978. p. 1–12.
[23] Block AJ, Boysen PG, Wynne JM, Hunt LA. Sleep apnea, hypopnea
and oxygen desaturation in normal subjects. A strong male
predominance. N Engl J Med 1979;300:513–7.
[24] Kryger MH. Monitoring respiratory and cardiac function. In: Kryger
M, Roth T, Dement W, editors. Principles and practice of sleep
medicine, 3rd ed. Philadelphia, PA: W.B. Saunders; 2000. p.
1217–30.
[25] Polysomnography task force, American Sleep Disorders Association
Standards of Practice Committee, Practice parameters for the
indications for polysomnography and related procedures. Sleep
1997;20:406–22.
[26] American Academy of Sleep Medicine, Sleep related breathing
disorders in adults: recommendations for syndrome definition and
measurement techniques in clinical research. Sleep 1999;22:667–89.
[27] Coleman RM. Periodic movement in sleep (nocturnal myoclonus) and
restless legs syndrome. In: Guilleminault C, editor. Sleeping and
waking disorders: indications and techniques. Menlo Park, CA:
Addison-Wesley; 1982. p. 265–95.
[28] Kimura J. Techniques and normal findings. In: Kimura J, editor.
Electrodiagnosis in diseases of nerve and muscle: principles and
practice, 2nd ed. Philadelphia, PA: F.A. Davis; 1989. p. 227–48.
Chapter 12.
[29] Mahowald MW, Schenck CM. REM sleep parasomnias. In:
Kryger M, Roth T, Dement W, editors. Principles and practice of
sleep medicine, 3rd ed. Philadelphia, PA: W.B. Saunders; 2000.
p. 724–37.
[30] Carskadon MA, Dement WC. Normal human sleep: an overview.
In: Kryger M, Roth T, Dement W, editors. Principles and practice
R. Vetrugno et al. / Sleep Medicine 5 (2004) 21–30 29

of sleep medicine, 3rd ed. Philadelphia, PA: W.B. Saunders; 2000.
p. 15–25.
[31] Petit JM, Milic-Emili G. Measurement of endoesophageal pressure.
J Appl Physiol 1958;3:481–5.
[32] Zemaityte D, Varoneckas G, Sokolov E. Heart rhythm control during
sleep. Psychophysiology 1984;21:279–89.
[33] Hornyak M, Cejnar M, Elam M, et al. Sympathetic muscle nerve
activity during sleep in man. Brain 1991;114:1281–95.
[34] Okada H, Iwase S, Mano T, et al. Changes in muscle sympathetic
nerve activity during sleep in humans. Neurology 1991;41:1961–6.
[35] Kitae S, Murata Y, Tachiki N, et al. Assessment of cardiovascular
autonomic dysfunction in multiple system atrophy. Clin Auton Res
2001;11:39–44.
[36] Isono S, Shiba K, Yamaguchi M, et al. Pathogenesis of laryngeal
narrowing in patients with multiple system atrophy. J Physiol 2001;
536:237–49.
[37] Merlo IM, Occhini A, Pacchetti C, Alfonsi E. Not paralysis, but
dystonia causes stridor in multiple system atrophy. Neurology 2002;
58:649–52.
[38] Benarroch EE. New findings on the neuropathology of multiple
system atrophy. Auton Neurosci 2002;96:59–62.
[39] Benarroch EE, Schmeichel AM. Depletion of cholinergic mesopon-
tine neurons in multiple system atrophy: a substrate for Rem
behaviour disorders? Neurology 2002;58(Suppl. 3):A345. Abstract.
[40] Lugaresi E, Coccagna G, Cirignotta F. Polygraphic and cineradio-
graphic aspects of obstructive apneas occurring during sleep:
physiopathological implications. In: Von Euler C, Lagercrantz H,
editors. Central nervous control mechanisms in breathing. Oxford:
Pergamon Press; 1979. p. 495–501.
[41] Fujita S, Conway W, Zorick F, Roth T. Surgical correction of anatomic
abnormalities in obstructive sleep apnea syndrome: uvulo-palato-
pharyngo-plasty. Otolaryngol Head Neck Surg 1981;89:923–34.
[42] Lugaresi E, Cirignotta F, Montagna P. Pathogenic aspects of snoring
and obstructive apnea syndrome. Schweiz Med Wochenschr 1988;
118:1333–7.
[43] Kuna S, Remmers JE. Anatomy and physiology of upper airway
obstruction. In: Kryger M, Roth T, Dement W, editors. Principles and
practice of sleep medicine. Philadelphia, PA: W.B. Saunders; 2000. p.
840–58.
[44] Tsuda T, Onodera H, Okabe S, Kilichi Y, Itoyama Y. Impaired
chemosensitivity to hypoxia is a marker of multiple system atrophy.
Ann Neurol 2002;52:367–71.
R. Vetrugno et al. / Sleep Medicine 5 (2004) 21–3030
Related Documents











