1 SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016 SLE by DR Magdi Awad Sasi Systemic lupus erythematosus (SLE or lupus) is a chronic autoimmune wide spread inflammatory disease that can be fatal, though with recent medical advances, fatalities are becoming increasingly rare. It involves connective tissues ,blood vessels and serosal surfaces. Lupus is treatable symptomatically, mainly with corticosteroids and immunosuppressants, though there is currently no cure. Survival in patients with SLE in the United States, Canada, Europe, and China is approximately 95% at 5 years, 90% at 10 years, and 78% at 20 years. Age --- Lupus can occur at any age, and is most common in women, particularly of non-European descent. Onset is usually after puberty in the 20 decade and 30. Sex: female : male 9:1 Race : more common in African Americans than in white female 130/100000. Predisposing factors: As with other autoimmune diseases, the immune system attacks the body’s cells and tissue, resulting in inflammation and tissue damage 1. Genetic predisposition: Complex ,involving > 100 genes ,HLA DR & DQ allels Genes that control programmed cell death ((apoptosis)) are important in human lupus. The proteins to which the lupus patient amounts an autoAB response are exposed on nuclear blebs during programmed cell death. Genes involved in immune comlex clearance ((Fc & receptor allels)) may predispose patients to lupus nephritis. 10% of patient have first degree relative with SLE. 2. Environmental factors: UV light exposure ----UV β &α play a role in the onset of SLE and triggering the flares. SLE Patients' are more likely than controls to have drug allergies especially to sulphonamide. Other association –precipitating flares: a. Common cold b. Smoking c. EBV 3. Hormonal factors: SLE more common in female & puberty. Increased late SLE in oral contraceptive and estrogen replacement. Pregnancy is associated with SLE flares in some. Elevation of prolactin may be associated with activity of SLE. ACTIVITY OF SLE: The classic pattern ((flare )) ----relapsing –remitting The continuous active pattern. The long period of disease quiescence ((few))

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
SLE by DR Magdi Awad Sasi
Systemic lupus erythematosus (SLE or lupus) is a chronic autoimmune wide spread inflammatory
disease that can be fatal, though with recent medical advances, fatalities are becoming increasingly
rare. It involves connective tissues ,blood vessels and serosal surfaces. Lupus is treatable
symptomatically, mainly with corticosteroids and immunosuppressants, though there is currently
no cure. Survival in patients with SLE in the United States, Canada, Europe, and China is
approximately 95% at 5 years, 90% at 10 years, and 78% at 20 years.
Age --- Lupus can occur at any age, and is most common in women, particularly of non-European
descent. Onset is usually after puberty in the 20 decade and 30.
Sex: female : male 9:1
Race : more common in African Americans than in white female 130/100000.
Predisposing factors: As with other autoimmune diseases, the immune system attacks the body’s
cells and tissue, resulting in inflammation and tissue damage
1. Genetic predisposition:
Complex ,involving > 100 genes ,HLA DR & DQ allels
Genes that control programmed cell death ((apoptosis)) are important in human lupus.
The proteins to which the lupus patient amounts an autoAB response are exposed on
nuclear blebs during programmed cell death.
Genes involved in immune comlex clearance ((Fc & receptor allels)) may predispose
patients to lupus nephritis.
10% of patient have first degree relative with SLE.
2. Environmental factors:
UV light exposure ----UV β &α play a role in the onset of SLE and triggering the flares.
SLE Patients' are more likely than controls to have drug allergies especially to
sulphonamide.
Other association –precipitating flares:
a. Common cold
b. Smoking
c. EBV
3. Hormonal factors:
SLE more common in female & puberty.
Increased late SLE in oral contraceptive and estrogen replacement.
Pregnancy is associated with SLE flares in some.
Elevation of prolactin may be associated with activity of SLE.
ACTIVITY OF SLE:
The classic pattern ((flare )) ----relapsing –remitting
The continuous active pattern.
The long period of disease quiescence ((few))
2
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
CLASSIFICATION:
1) Acute systemic lupus erythematosus or SLE
2) Subacute cutaneous lupus erythematosus, which causes non-scarring skin lesions on
patches of skin exposed to sunlight.
3) Discoid lupus erythematosus, a skin disorder which causes a red, raised rash on the face,
scalp or rest of the body, which occasionally (1-5%) develops into SLE.
4) Drug-induced lupus erythematosus
5) Lupus nephritis, an inflammation of the kidneys caused by SLE
6) Neonatal lupus, a rare disease affecting babies born to women with SLE, Sjögren's
syndrome or sometimes no autoimmune disorder. It is theorized that maternal antibodies
attack the fetus, causing skin rash, liver problems, low blood counts (which gradually fade)
and heart block leading to bradycardia.
COURSE:
>50% of SLE patients have acquired permenant damage.
This can be related to disease itself or corticosteroids.
Mortality :
Survival of SLE 89% at 10 years after diagnosis.
Mortality had actually increased in young women.
The major cause of death in SLE is accelerated atherosclerosis.
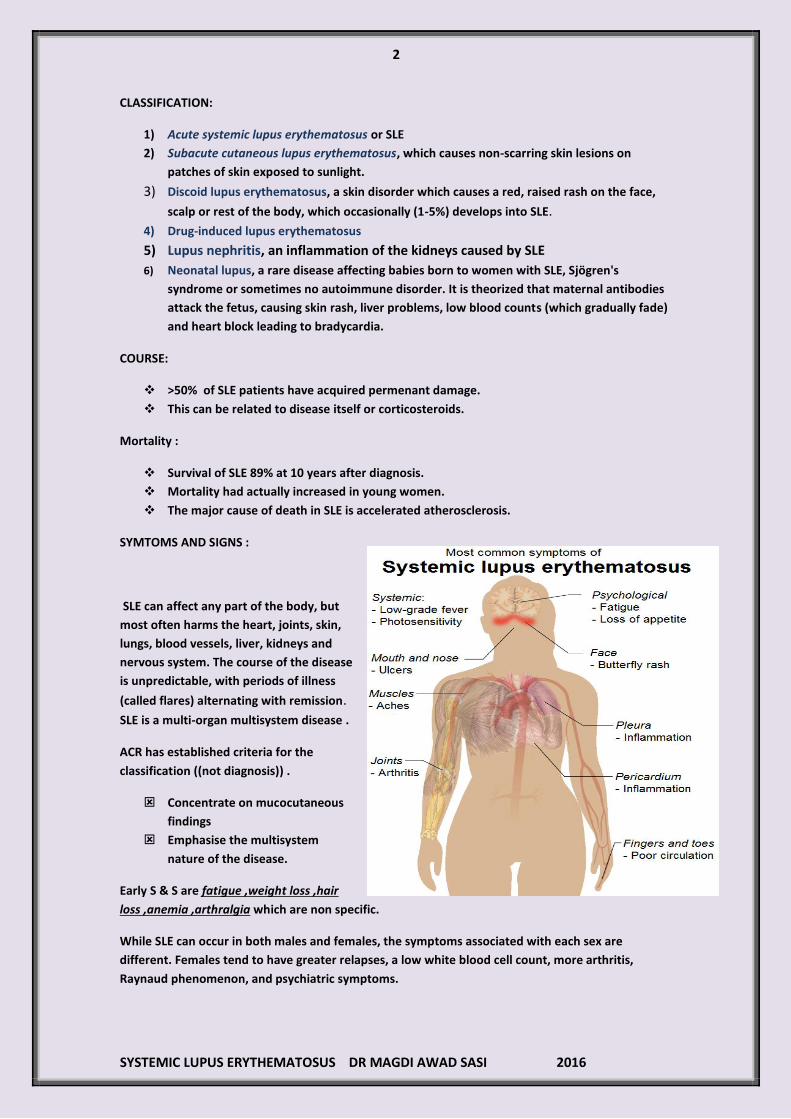
SYMTOMS AND SIGNS :
SLE can affect any part of the body, but
most often harms the heart, joints, skin,
lungs, blood vessels, liver, kidneys and
nervous system. The course of the disease
is unpredictable, with periods of illness
(called flares) alternating with remission.
SLE is a multi-organ multisystem disease .
ACR has established criteria for the
classification ((not diagnosis)) .
Concentrate on mucocutaneous
findings
Emphasise the multisystem
nature of the disease.
Early S & S are fatigue ,weight loss ,hair
loss ,anemia ,arthralgia which are non specific.
While SLE can occur in both males and females, the symptoms associated with each sex are
different. Females tend to have greater relapses, a low white blood cell count, more arthritis,
Raynaud phenomenon, and psychiatric symptoms.

3
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
Males tend to have more seizures, kidney disease, serositis (inflammation of tissues lining the
lungs and heart), skin problems, and peripheral neuropathy.
The classic presentation of a triad of fever, joint pain, and rash in a woman of
childbearing age should prompt investigation into the diagnosis of SLE. In
patients with suggestive clinical findings, a family history of autoimmune
disease should raise further suspicion of SLE.
Fatigue, fever, arthralgia, and weight changes are the most common symptoms in new cases or
recurrent active SLE flares. Fatigue, the most common constitutional symptom associated with SLE,
can be due to active SLE, medications, lifestyle habits, or concomitant fibromyalgia or affective
disorders.
SLE-specific fatigue or fever generally occurs in concert with other clinical markers. Fever may
reflect active SLE, infection, and reactions to medications (ie, drug fever). Always exclude an
infectious etiology; patients with SLE are considered immunocompromised and are therefore at
higher risk for developing infections and complications. Most infections are bacterial in origin, but
clinicians should always consider the possibility of atypical and opportunistic infections, particularly
when these individuals are receiving immune-modulating or immunosuppressive therapy. Note that
an acute infectious process may also trigger SLE and that the two can occur concomitantly.
Weight loss may occur in patients with active SLE. Weight gain may also be due to corticosteroid
treatment or active disease, such as nephrotic syndrome (with
anasarca) or myocarditis.
1. Musculoskeletal
Joint pain is one of the most common reasons for the
initial clinical presentation of patients with SLE.
Arthralgia, myalgia, and frank arthritis may involve
the small joints of the hands, wrists, and knees
(usually symmetrical, polyarticular).
In contrast to rheumatoid arthritis, SLE arthritis or
arthralgia may be asymmetrical, with pain that is
disproportionate to swelling.
SLE arthropathy is rarely erosive or deforming.
Characteristic hand deformities are swan neck
deformities that result from recurrent synovitis and
inflammation of the joint capsule, tendons, and ligaments.
These deformities are usually reducible and nonerosive
(resembling Jaccoud arthropathy, which is a nonerosive
arthritis following acute rheumatic fever).
Another important consideration is the increased
prevalence of avascular necrosis (AVN) in the SLE
population relative to healthy individuals. It may be due to
SLE pathogenesis and/or concomitant heavy steroid use.
Asymptomatic AVN is seen in up to 44% of SLE patients in
the first year of therapy with high-dose corticosteroids.
The most commonly affected site is the femoral head. Independent risk factors for AVN in
patients with SLE include the use of glucocorticosteroid or cytotoxic agents and the
presence of arthritis.
4
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
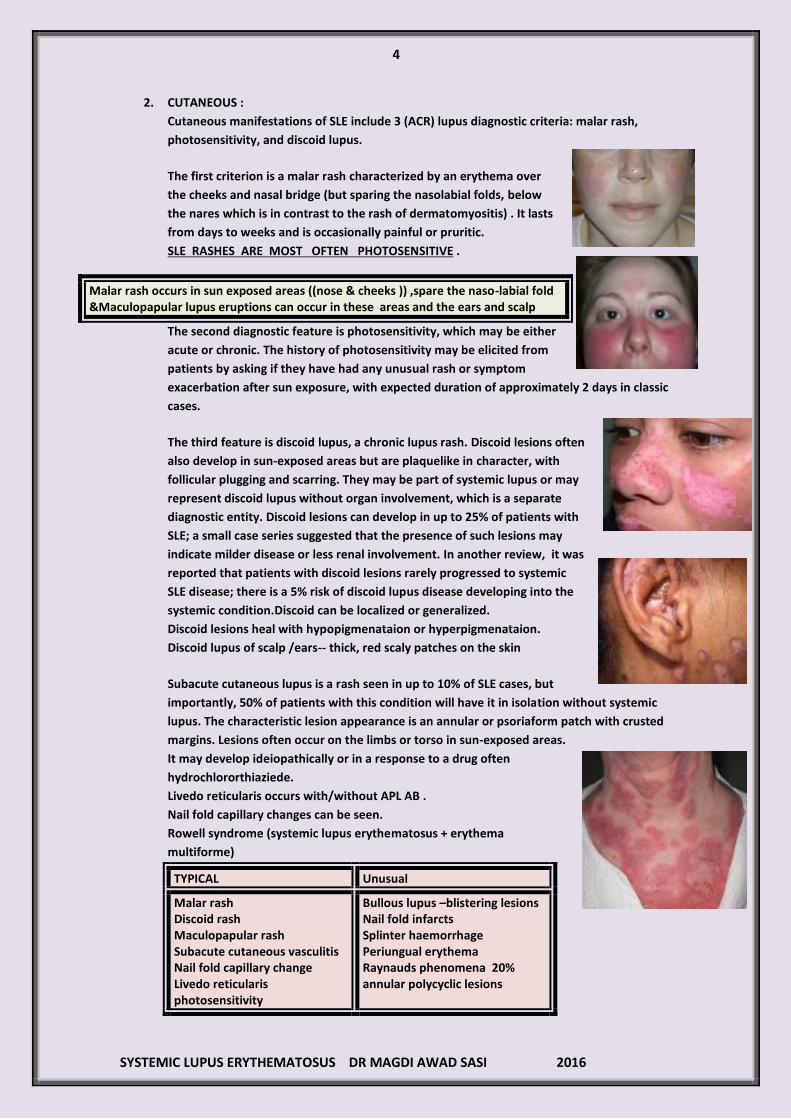
2. CUTANEOUS :
Cutaneous manifestations of SLE include 3 (ACR) lupus diagnostic criteria: malar rash,
photosensitivity, and discoid lupus.
The first criterion is a malar rash characterized by an erythema over
the cheeks and nasal bridge (but sparing the nasolabial folds, below
the nares which is in contrast to the rash of dermatomyositis) . It lasts
from days to weeks and is occasionally painful or pruritic.
SLE RASHES ARE MOST OFTEN PHOTOSENSITIVE .
Malar rash occurs in sun exposed areas ((nose & cheeks )) ,spare the naso-labial fold &Maculopapular lupus eruptions can occur in these areas and the ears and scalp
The second diagnostic feature is photosensitivity, which may be either
acute or chronic. The history of photosensitivity may be elicited from
patients by asking if they have had any unusual rash or symptom
exacerbation after sun exposure, with expected duration of approximately 2 days in classic
cases.
The third feature is discoid lupus, a chronic lupus rash. Discoid lesions often
also develop in sun-exposed areas but are plaquelike in character, with
follicular plugging and scarring. They may be part of systemic lupus or may
represent discoid lupus without organ involvement, which is a separate
diagnostic entity. Discoid lesions can develop in up to 25% of patients with
SLE; a small case series suggested that the presence of such lesions may
indicate milder disease or less renal involvement. In another review, it was
reported that patients with discoid lesions rarely progressed to systemic
SLE disease; there is a 5% risk of discoid lupus disease developing into the
systemic condition.Discoid can be localized or generalized.
Discoid lesions heal with hypopigmenataion or hyperpigmenataion.
Discoid lupus of scalp /ears-- thick, red scaly patches on the skin
Subacute cutaneous lupus is a rash seen in up to 10% of SLE cases, but
importantly, 50% of patients with this condition will have it in isolation without systemic
lupus. The characteristic lesion appearance is an annular or psoriaform patch with crusted
margins. Lesions often occur on the limbs or torso in sun-exposed areas.
It may develop ideiopathically or in a response to a drug often
hydrochlororthiaziede.
Livedo reticularis occurs with/without APL AB .
Nail fold capillary changes can be seen.
Rowell syndrome (systemic lupus erythematosus + erythema
multiforme)
TYPICAL Unusual
Malar rash Discoid rash Maculopapular rash Subacute cutaneous vasculitis Nail fold capillary change Livedo reticularis photosensitivity
Bullous lupus –blistering lesions Nail fold infarcts Splinter haemorrhage Periungual erythema Raynauds phenomena 20% annular polycyclic lesions

5
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
Acute cutaneous lupus
erythematosus:
Malar rash
Subacute cutaneous
lupus---papular
squamous or annular
polycystic rash
Chronic cutaneous lupus
(( discoid lupus ))
Alopechia
Photosensitivity
Uriticaria
Livedo reticularis
Mucosal ulceration
Raynuds phenomena
3. Head ,ears ,eyes ,nose and throat:
Alopechia can occur as diffuse or focal areata . Diffuse thinning or hair fragility with visible
broken hair in the absence of other causes ((androgenic ,anemia )) may be seen.
Alopecia is an often less specific cutaneous feature of SLE. It often affects the temporal
regions or creates a patchy pattern of hair loss.
Discoid lupus can cause scarring alopechia.
2ry sjogrens occurs in some patients with SLE.
Ocular involvement can be scleritis ,episcleritis ,uveitis
,retinitis and optic atrophy.
Both the nose and mouth ((palatal and buccal mucosa )) may
have aphthous ulcers ((painless and painfull)).
Scarring alopechia: 1) Psoriasis 2) Dermatitis 3) SLE 4) Sarcoidosis 5) Trauma 6) burns
In summary ; typical
Alopechia
Oral /nasal ulcers
Discoid lupus of scalp /ears-- thick, red scaly patches on the skin ,scaling ,pigmentary
changes ,skin atrophy ,follicular plugging ,scarring.
Keratoconjunctivitis sicca
Sclertitis
Dry mouth
Uveitis
Unusual---retinitis ,polychondritis ,optic neuritis ,angiedema
Vasculitis should be excluded as such finding may be seen.
6
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
4. CARDIO-VASCULAR SYSTEM :
Typical -- pericarditis /pericardial effusion Unusual --- Myocarditis Libman sacks endocarditis---atypical verrucom)) Coronary arteritis Coronary aneurysm Cardiac arrhythmias CCF---HTN ,MYOCARDITIS
Pericardial disease----
ECHO is one of the most sensitive tests for detection of pericardial disease.
This causes pericarditis ,cardiac temponade and constriction.
Pericardiocenresis – WBC 544 -199000 cells /mm3 PMN , LE cells found in smear ANA +ve
Myocardial disease----
Primary myocarditis --- unexplained tachycardia ,CCF ,ventricular arrhythmia or conduction
defects ,ST –T wave changes or cardiomegally without evidence of valvular or pericardial
disease.
Some of the SLE patients have elements of reversible myocardial dysfunction of perfusion
abnormalities.
2ry myocardial dysfunction: 1. Coronary artery diseas 2. Valvular disease 3. Pulmonary disease 4. Systemic HTN 5. Drug toxicity 6. Amyloidosis
Reversible =Ischemia / Persistent = scarring
Coronary artery disease –premature:
Embolic –Libmann sacks endocardis
Thrombosis ----antiphospholipid antibodies
Vasculitis ----can occur in the absence of extra-cardiac SLE.
D/D Atherosclerosis
It present with symptoms of ischemia and respond to steroids.
Myocardial infarction –common ,48years mean age and causes death.
It is liable to occur in younger.
HTN ,DM ,and hyperlipidemia increase the risk.
APLA has been associated with recurrent A/V thrombosis by:
Platelet activation Vascular endothelial cell proliferation Interfere with prostacyclin production
INV----
ECG ,Echocardiography ,thallium stress teat
Coronary angiography
Note :
If the patient present with ischemic symptoms ,and arteriogram can be instituted ,start
anti-anginal treatment and moderate to high doses of steroid .

7
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
Once stabilized ,tapper the steroids gradually .
If the symptoms recur , coronary arteritis diagnosis is made.
If angiography shows thrombosis without atherosclerosis ,you have to start antiplatelets &
anticoagulants.
Libmann sacks endocardititis:
The most characteristic cardiac manifestation ((60%))
Found on ventricular surface of mitral valve ,chodae tendinae
,papillary muscle.
Doesn’t correlate with the murmurs and rarely produce
valvular dysfunction.
MR,AR ---result from steroid by promoting healing of verrucous lesions—scarring
& retraction.
Outcome – 2ry bacterial endocarditis 7% ,cerebral emboli
Need prophylactic antibiotic in certain surgical process.
5. pulmonary:
Dyspnea on exertion 80%
Dyspnea at rest 40%
Chest pain 35%
Cough 44%
i. Pleurisy /pleural effusion
ii. Interstitial pneumonitis
iii. Pulmonary HTN
iv. Pulmonary haemorrhage
Pulmonary function testing has been the most sensitive indicator of pulmonary involvement.
Pleurisy and pleural effusion :
Pleural disease is the most common thoracic abnormality present in lupus patients
Pleural effusion or pleural thickening occurs in about 70% of cases.
Pleural effusions in SLE are usually bilateral, small and exudative.
Although isolated pleural effusion is a nonspecific radiologic finding, its presence,
particularly when chronic, may suggest the diagnosis of SLE if other clinical features of
autoimmune disease are present.
Thoracocentesis indicated
8
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
Fibrothorax is a rare complication occurring after refractory pleuritis resulting in thickening
of visceral and parietal pleura and usually presents with loculated pleural effusion, pleural
thickening and atelectasis of the adjacent lung parenchyma.
Exudative pericardial effusions and pericarditis may occur in up to 50% of patients.
Pleural effusion –exudative ,PH 7.3 ,glucose normal ,leucocyte <10000cells/mm3 ,LE ,ANA
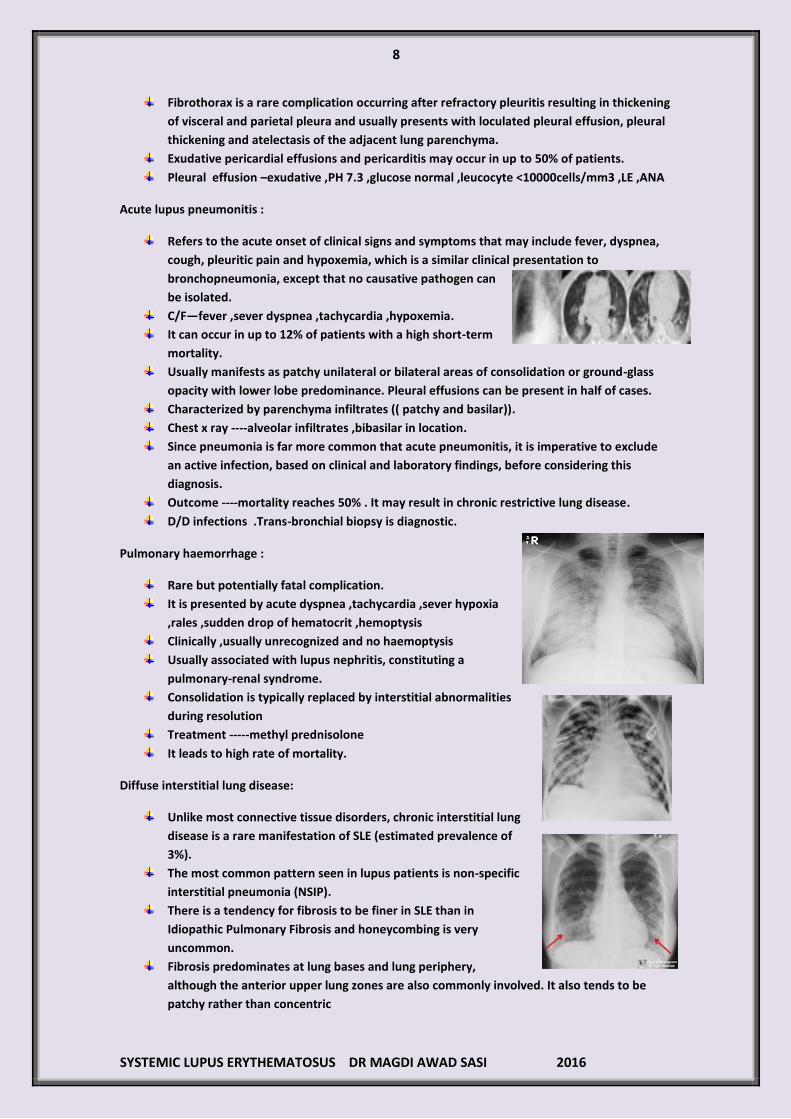
Acute lupus pneumonitis :
Refers to the acute onset of clinical signs and symptoms that may include fever, dyspnea,
cough, pleuritic pain and hypoxemia, which is a similar clinical presentation to
bronchopneumonia, except that no causative pathogen can
be isolated.
C/F—fever ,sever dyspnea ,tachycardia ,hypoxemia.
It can occur in up to 12% of patients with a high short-term
mortality.
Usually manifests as patchy unilateral or bilateral areas of consolidation or ground-glass
opacity with lower lobe predominance. Pleural effusions can be present in half of cases.
Characterized by parenchyma infiltrates (( patchy and basilar)).
Chest x ray ----alveolar infiltrates ,bibasilar in location.
Since pneumonia is far more common that acute pneumonitis, it is imperative to exclude
an active infection, based on clinical and laboratory findings, before considering this
diagnosis.
Outcome ----mortality reaches 50% . It may result in chronic restrictive lung disease.
D/D infections .Trans-bronchial biopsy is diagnostic.
Pulmonary haemorrhage :
Rare but potentially fatal complication.
It is presented by acute dyspnea ,tachycardia ,sever hypoxia
,rales ,sudden drop of hematocrit ,hemoptysis
Clinically ,usually unrecognized and no haemoptysis
Usually associated with lupus nephritis, constituting a
pulmonary-renal syndrome.
Consolidation is typically replaced by interstitial abnormalities
during resolution
Treatment -----methyl prednisolone
It leads to high rate of mortality.
Diffuse interstitial lung disease:
Unlike most connective tissue disorders, chronic interstitial lung
disease is a rare manifestation of SLE (estimated prevalence of
3%).
The most common pattern seen in lupus patients is non-specific
interstitial pneumonia (NSIP).
There is a tendency for fibrosis to be finer in SLE than in
Idiopathic Pulmonary Fibrosis and honeycombing is very
uncommon.
Fibrosis predominates at lung bases and lung periphery,
although the anterior upper lung zones are also commonly involved. It also tends to be
patchy rather than concentric

9
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
C/F---dyspnea on exertion ,productive cough ,pleuritis ,rales
Ig and complement in the interstitium in focal and diffuse pattern.
Steroids beneficial in pre fibrotic stage.
Pulmonary HTN:
Changes are : Intimal thickening and fibrosis Medial hypertrophy Altered lamina Periadvential fibrosis
Primary or secondary pulmonary arterial hypertension (PAH) is not frequent in SLE (up to
6%).
The pathophysiology of PAH in systemic lupus is multifactorial and may encompass
pulmonary vasculopathy, chronic thromboembolic disease (related to antiphospholipid
antibody syndrome), left heart disease, lung disease or the combination of these factors.
Contrast-enhanced CT chest may demonstrate the presence of large central pulmonary
arteries with pruned peripheral arterial trees and myocardial hypertrophy.
Contrast-enhanced CT chest may be warranted when a lupus patient presents with acute
dyspnea, because antiphospholipid antibody syndrome acts as an independent risk factor
for the development of deep venous thrombosis and pulmonary embolism.
There is associated a greater frequency of Raynauds phenomenon.
Presence of antiphospholipid antibodies 6%
Pulmonary embolism (9%) and peripheral vaso-occlusive disease 12%
Diaphragmatic dysfunction (( shrinking lung syndrome)):
This syndrome refers to progressive loss of lung
volumes and is thought to be due to
diaphragmatic dysfunction or pleuritic chest
pain with restriction of respiration.
It is a sluggish diaphragm or shrinking lungs .
Presents with hemidiaphragmatic elevation,
often with radiologic evidence of linear bibasilar
atelectasis and ill-defined juxtadiaphragmatic
areas of increased opacity .
Diaphragmatic dysfunction should be suspected
when dyspnea is out of proportion to the
severity of radiographic abnormalities and when
a restrictive pattern is shown on pulmonary
function tests.
It is presented by dyspnea due to myopathy of diaphragm
PULMONARY INFECTIONS
Pulmonary infections constitute a predictable complication related to medication of SLE.
Constitutes a major cause of morbidity and mortality (57% of all fatal infections).
Pneumonia is the most common cause of pulmonary infiltrates in SLE patients.

11
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
Although community-acquired bacterial pneumonia is the most common cause of pulmonary
infection, they may also be due to atypical microorganisms (Mycobacteria, Pneumocystis jiroveci,
Cytomegalovirus, Aspergillus and Nocardia).
For patients who are undergoing treatment with high-dose corticosteroids or immunosuppressive
drugs, regular screening for pulmonary tuberculosis is mandatory in geographic areas in which this
entity is prevalent.
6. GASTRO-INTESTINAL TRACT :
Mild esophageal dysmotility occurs
Hepatomegally
Splenomegally child form
Rare manifestation---
Ascites
Colitis
Mesenteric vasculitis
Protein losing enteropathy
Primary biliary cirrhosis
Budd chiari syndrome
Ileus
A. Small vessel vasculitis:
Most serious GIT complication
The extent and severity varies
80% die when vasculitis associated with perforation or infarction of the viscous.
The classical abdominal finding obscured as patient on steroids.
It is associated with :
CNS involvement ,Thrombocytopenia , and cutaneous vascilitis.
INVEASTIGATION ---plain films and paracentesis D/D peritonoitis
Mesenteric arteritis ---pseudo-obstruction ,thumb –printing ,mucosal abnormalities.
Endoscopy or colonoscopy may be useful.
B. Lupus peritonitis---ascitis may be present.
C. GIT bleeding
D. Pancreatitis
E. Esophageal disease
F. Pneumatosis intestinalis or intramural air ----benign & infarct
If patient present with peritonitis ,high dose of steroid should be started. If no response (( 12—48%)) ,exploratory laparotomy should be done.
7. Neurologic :
Typical Unusual
Psychosis Seizures Encephalopathy Coma Meningitis Transverse myeilitis Mononeuritis multiplex Peripheral neuropathy Stroke
Cranial neuropthy Chorea Pseudotumor cerebri
11
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
CNS in SLE & autoantibodies----CNS involvement can be diffuse or focal.
3 types :
1. S.antiphospholipid AB with focal CNS SLE-- intravascular occlusion
2. CSF antineuronal AB with diffuse CNS lupus
3. S.anti P AB –Ribososmal P protein with psychosis in SLE
CNS lupus is characterized by :
Diffuse manifestation
Neuropsychiatric manifestation lupus erythematous
Caused by auto –AB directed to neuronal cells.
These autoantibodies are hypothesized to affect neuronal function in generalized manners.
a. Increased level of inflammatory cytokines
b. Induction of NO production
c. Oxidative stress
d. Excitatory A.A. toxicity
Elevated level of IgG and oligoclonla bands are a marker of auto-antibodies production within CNS
and present in patient with diffuse CNS lupus.
S. Anti P antibodies is a helpful diagnosis marker for psychiatric disease.
CNS lupus with focal manifestation ===intravascular occlusion
A. NONFOCAL CEREBRAL DYSFUNCTION (( 35 --- 60%)):
a) Organic brain disease ---
Memory deficits
Impaired cognitive function
Agitation and delirium +functional ---depression ,affective disorder
Delirium represents a spectrum of fluctuating altered consciousness
characteristic of SLE. Delirium may be caused by CNS vasculitis,
encephalopathy, cerebritis, or the manifestations previously called organic
brain syndrome. Aseptic meningitis, myelopathy, optic neuropathy, or other
demyelinating disorders may also require urgent evaluation.
b) Psychosis 25%
c) Affective disorders
d) Neurosis
B. SEIZURES (( 15---35%)):
Can antedate the onset of SLE or develop during the course of disease.
Grand mal , Petit mal , Temporal lobe ,Focal
50% is due to uremia ,infections and metabolic.
C. FOCAL DEFICITS ((10---35%)):
1. Cranial neuropathies—eye
2. Asymmetric peripheral neuropathy ---like GBS
3. Optic neuritis ,Visual deficits ,Ophthalmoplegia ,Nystagmus ,Retinal infarction
4. Ptosis
5. Facial palsy
6. Trigeminal neuralgia
7. Tinnitus ,vertigo
8. Stroke –due to:
12
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
a. Hyper -coagulant state ---lupus A/G , antiphospholipid antibody
b. Libmann sacks endocarditis
c. Arteritis
D. MOVEMENT DISORDERS:
Athetosis
Chorea
Hemiballismus
Cerebellar infarct
E. OTHERS:
Aseptic meningitis
Headache
Multiple sclerosis like
Eaton lambert syndrome
Myasthenia gravis
Infection
Transverse myelitis with spastic paraparesis and sensory loss at a given level is a rare but
severe complication of SLE or antiphospholipid antibody syndrome. Stroke and transient
ischemic attack (TIA) may be related to antiphospholipid antibody syndrome or SLE
vasculitis. Posterior reversible encephalopathy syndrome (PRES) is, as the name implies, a
reversible encephalopathy linked to hypertension that even may be a presenting feature
for young SLE patients.
Cognitive disorders may be variably apparent in many patients with SLE. Formal
neuropsychiatric testing reveals deficits in 21-67% of patients with SLE. Whether this
represents true encephalopathy, neurologic damage, medication effects, depression, or
some other process is unclear.
Migraine headaches may be linked to antiphospholipid syndrome. Headache and mood
disorders may be the most commonly reported neurologic manifestation of SLE, but cause
and effect may be difficult to distinguish.
Acute psychiatric manifestations in CNS lupus should be considered as a diagnosis of
exclusion in an SLE patient.
8. RENAL:
The kidney is the most commonly involved visceral organ in SLE. Although only
approximately 50% of patients with SLE develop clinically evident renal disease, biopsy
studies demonstrate some degree of renal involvement in most patients. Therefore, it is
important to correctly classify the extent of renal involvement in SLE to improve the
correlation between histologic findings and the prognosis of the renal disease .
Glomerular disease usually develops within the first few years of SLE onset and is often
asymptomatic.
The presentation is wide and include:
1) Acute or chronic renal failure may cause symptoms related to uremia and fluid
overload.
2) Acute nephritic disease may manifest as hypertension and hematuria.
3) Nephrotic syndrome may cause edema, weight gain, or hyperlipidemia
Classification ------------
1) Mesengial glomerulonephritis
2) Focal proliferative glomerulonephritis
13
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
3) Diffuse proliferative glomerulonephritis
4) Membranous glomerulonephritis
Sudden deterioration of renal function should prompt careful consideration of :
A. Hypovolemia
B. Renal insufficiency
C. Renal vein thrombosis
D. Drug induced interstitial nephritis
E. Contrast induced acute tubular necrosis
Response to treatment : 1. Decreased Double strand DNA titer 2. Decreased C3 C4 CH 50 3. Increased creatinine clearance 4. Decreased proteinuria
Long term steroids and cyclophosphamide ----diarrhea ,alopecia ,menstrual irregularity
,granulocytopenia ,increased infections
• Acute interstitial nephritis --rising plasma creatinine concentration and a urinalysis that is
relatively normal or shows only a few red cells and/or white cells.
• These changes may be accompanied by signs of tubular dysfunction such as metabolic
acidosis due to type 1 (distal) renal tubular acidosis, hyperkalemia due to impaired distal
potassium secretion, or hypokalemia due to salt-wasting and secondary
hyperaldosteronism .
9. MUSCULOSKELETAL:
Polyarthralgia /arthritis of SLE patients
Non erosive
Small joints of hands and wrists
Myositis /dermatomyssitis
30% of SLE patients have coexsisting fibromyalgia
10. HAEMATOLOGICAL DISEASES:
A. Anemia ---- 57---80%
Most common
Causes:
1) Autoimmune hemolytic anemia:
Warm IgG autoantibodies and complement on RBC ((characteristic))
40% during the course of the illness & 65% positive coombs assay.
Lab ---- increased reticulocyte count &indirect bilirubin with low haptoglobin
It is not indicator of poor prognosis.
75% respond to high doses of corticosteroids
Splenectomy produce permanent remission <50%
It causes Immune –suppression.
Danazol 200mg/3-4times/day
2) Pure red cell aplasia ---BM erythroid hypoplasia
3) Occult GIT blood loss /peptic ulcer

14
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
4) Myelosuppression ---Azathioprine
5) Aplastic anemia & agranulocytosis ---Phenyl butazone
B. Leucopenia WBC < 4500/mm3 60%
C. Lymphopenia <1500/mm3 during disease activity 80%
D. Thrombocytopenia :
Platelet count < 100000/mm3 (( 20—40%))
Sever < 50 000/mm3 ((10%))
In evaluation ,five major causes:
a) Decreased production from megakaryocyte defects /drugs
b) Insffective thrombopoiesis
c) Abnormal platelet function as in congestive splenomegally
d) Dilutional effects
e) Abnormal platelet destruction by:
DIC Hemolytic malignancies
TTP Drug induced infection
HUS Vasculitis
ITP may be the initial presentation of SLE.
SLE associated ITP is characterized by an increased number of megakayocytes.
Treatment ---corticosteroids ,splenectomy ,Danazole ,Immunosuppression
Acute –I.V.Immunoglobulins 0.4gm/kg/day for 5 days
TTP + SLE Five major manifestation---
1. Fever 2. Altered mental status 3. Wosening renal function 4. Hemolytic anemia 5. Thrombocytopenia
Patient with SLE can develop TTP ((D/D SLE flare )) The quickest way ---DO PBF ----schistocytes –microangiopathic hemolytic anemia with negative coombs test Aeitiology : IgG autoantibody against the metalloprotease responsible for cleavage of monomeric subunits of von willbrand factors. Allows for accumulation of unusually large multimers of VWF secreted by endothelial cells Multimers bind to platelet glycoprotein receptors causing platelet adhesion and microthrombi Treatment : NO RULE OF CORTICOSTEROID OR IMMUNE-SUPPRESIVE THERAPY Plasmaphresis to remove autoantibody +multilers Fresh frozen plasma to replace metalloproteases CS and immunosuppression to preven recurrence by decreasing antibody production.
E. LAC—LUPUS ANTICOAGULANT:
Interferes with the activation of prothrombin activator complex Xa ,V ,Ca+ ,PL
This leads to prolonged APTT, normal or prolonged PT
It is Associated with venous and arterial thrombosis.
Anti-cardiolipin AB directed at the phospholipid in the PAC and LAC causes various
signs and symptoms in arteries and veins .

15
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
(1) Acute Cutaneous Lupus OR Subacute Cutaneous Lupus:
Acute cutaneous lupus: lupus malar rash (do not count if malar discoid), bullous lupus, toxicepidermal necrolysis variant
of SLE, maculopapular lupus rash, photosensitive lupus rash (in the absence of dermatomyositis).
Subacute cutaneous lupus: nonindurated psoriaform and/or annular polycyclic lesions that resolve without scarring,
although occasionally with postinflammatory dyspigmentation or telangiectasias).
(2) Chronic Cutaneous Lupus:
Classic discoid rash localized (above the neck) or generalized (above and below the neck), hypertrophic (verrucous) lupus, lupus
panniculitis (profundus), mucosal lupus, lupus erythematosus tumidus, chillblains lupus, discoid lupus/lichen planus overlap
Serositis:
Typical pleurisy for more than 1 day OR pleural effusions OR pleural rub
Typical pericardial pain for more than 1 day OR pericardial effusion OR pericardial rub OR pericarditis by ECG.
In the absence of other causes, such as infection, uremia, and Dressler’s pericarditis
Renal:
Urine protein–to-creatinine ratio (or 24-hour urine protein) representing 500 mg protein/24 hours OR red blood cell casts
Neurologic:
Seizures, psychosis, mononeuritis multiplex(in the absence of other known causes such as primary vasculitis), myelitis,
peripheral or cranial neuropathy (in the absence of other known causes such as primary vasculitis, infection, and diabetes
mellitus), acute confusional state (in the absence of other causes, including toxic/metabolic, uremia, drugs)
Leukopenia (<4000/mm3) OR Lymphopenia (<1000/mm3)
Leucopenia at least once: In the absence of other known causes such as Felty’s syndrome, drugs, and portal hypertension.
Lymphopenia at least once: in the absence of other known causes such as corticosteroids, drugs, and infection
16
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
DIAGNOSIS:
The diagnosis of (SLE) must be based on the proper constellation of clinical findings and
laboratory evidence.
The 1982 American College of Rheumatology (ACR) criteria summarized features necessary
to diagnose SLE. The presence of 4 of the 11 criteria yields a sensitivity of 85% and a
specificity of 95% for SLE . Keep in mind that individual features are variably sensitive and
specific. Patients with SLE may present with any combination of clinical features and
serologic evidence of lupus.
The Systemic Lupus International Collaborating Clinics (SLICC) group revised and validated
the ACR SLE classification criteria in 2012.According to the revision, a patient is classified as
having SLE if the patient has biopsy-proven lupus nephritis with ANA or anti-dsDNA
antibodies or if the patient satisfies 4 of the diagnostic criteria, including at least 1 clinical
and 1 immunologic criterion.
The following are the ACR diagnostic criteria in SLE, presented in the "SOAP BRAIN MD"
mnemonic:
Serositis - Pleurisy, pericarditis clinically or (ECG) or imaging
Oral ulcers - Oral or nasopharyngeal, usually painless; palate is most specific
Arthritis - Nonerosive, 2 or more peripheral joints with tenderness or swelling
Photosensitivity - Unusual skin reaction to light exposure
Blood disorders - Leukopenia (< 4 × 10 3 cells/µL on >1 occasion), lymphopenia (< 1500
cells/µL on >1 occasion), thrombocytopenia (< 100 × 10 3 cells/µL in the absence of
offending medications), hemolytic anemia
Renal involvement – Based on presence of proteinuria (>0.5 g/day or 3+ positive on
dipstick testing) or cellular casts (including red blood cells [RBCs], hemoglobin, granular,
tubular, or mixed) .
Antinuclear antibodies (ANAs) - Higher titers generally more specific (>1:160); must be in
the absence of medications associated with drug-induced lupus
Immunologic phenomena - dsDNA; anti-Smith (Sm) antibodies; antiphospholipid
antibodies (anticardiolipin immunoglobulin G [IgG] or immunoglobulin M [IgM] or lupus
anticoagulant); biologic false-positive serologic test results for syphilis, lupus
erythematosus (LE) cells (omitted in 1997 revised criteria)
Neurologic disorder - Seizures or psychosis in the absence of other causes
Malar rash - Fixed erythema over the cheeks and nasal bridge, flat or raised
Discoid rash - Erythematous raised-rimmed lesions with keratotic scaling and follicular
plugging, often scarring
In patients with high clinical suspicion and/or high ANA titers, additional testing is indicated. This commonly includes evaluation of antibodies to dsDNA, complement, and ANA subtypes such as Sm, SSA, SSB, and ribonucleoprotein (RNP) (often called the ENA panel), as well as screening anticardiolipin antibodies, lupus anticoagulant, and +/- beta-2 glycoprotein antibodies.
The spot protein/spot creatinine ratio may be used to quantify proteinuria. The 2012 ACR
guidelines for lupus nephritis indicate that a spot protein/spot creatinine ratio greater than
0.5 g/day can substitute for the 24-hour protein measurement and that an active urinary
sediment (defined as >5 red blood cells [RBCs] per high-power field ; >5 white blood cells
[WBCs] in the absence of infection; or cellular casts limited to RBC or WBC casts can
substitute for cellular casts.
17
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
Early markers of SLE disease activity:
1) High ESR.
2) Low C4.
3) High Anti-dsDNA titres.
4) Falling Hb, TLC & PLT.
5) Falling albumin.
6) Rising immunoglobulins (e.g. high IgG)
LABORATORY:
Complete blood count (CBC) with differential
RFT—blood urea & Serum creatinine
Urinalysis with microscopy
Erythrocyte sedimentation rate (ESR) or C-reactive protein (CRP)
Complement levels
Liver function tests
Creatine kinase assay
Spot protein/spot creatinine ratio
i. CBC/CBP:
Anemia –very common and multifactorial
Hemolytic anemia with increased reticulocyte –direct coombs ,low haptoglobin
Anemia of chronic illness ---most common
Anemia of iron deficiency ,renal failure
WBC ---leukopenia ---common & mild ,rare < 1000/ml
Lymphopenia is frequent
Neutropenia can occur but rare.
ii. The chemistry :
BUN & creatinine may be elevated
Cholestrol may be elevated due to NS.
Transaminases may be elevated ((mild)).
ALP may indicate primary biliary cirrhosis ,renal osteodystrophy.
CPK may be increased 2ry to myositis.
Homocystine may be elevated , ((30%)) ,especially with renal insufficiency.
iii. URINALYSIS:
Proteinuria ,RBC casts ,WBC casts
iv. IMAGING STUDIES:
MRI brain to evaluate CNS involvement is mandatory.
It may show small white matter lesions ---represent immune deposition
A true vasculitis is almost never seen on cerebral arteriogram.
v. Autoantibodies :
96% SLE patients have positive ANA
Antinuclear antibody & Antibodies which stain nuclear structures.
Occurs in 20 - 25% of normal people
Screening test and is not diagnostic.
Titer (1:80 ?) > 1:160 is significant Qualitative not quantitative test. Following
titers is meaningless
Titres of 1:640 or higher are more indicative of CTD.
18
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
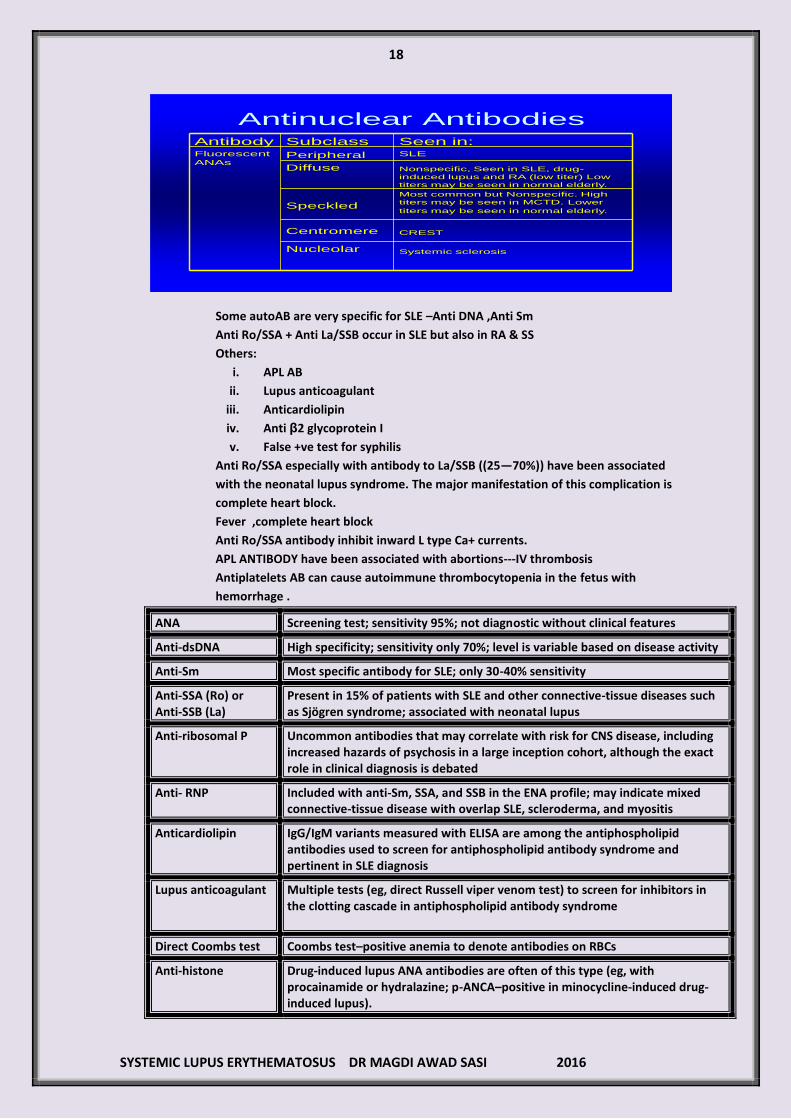
Antinuclear AntibodiesSeen in:SLE
Nonspecific, Seen in SLE, drug-
induced lupus and RA (low titer) Low
titers may be seen in normal elderly.
Most common but Nonspecific. High
titers may be seen in MCTD. Lower
titers may be seen in normal elderly.
CREST
Systemic sclerosis
Subclass
Peripheral
Diffuse
Speckled
Centromere
Nucleolar
AntibodyFluorescent
ANAs
Some autoAB are very specific for SLE –Anti DNA ,Anti Sm
Anti Ro/SSA + Anti La/SSB occur in SLE but also in RA & SS
Others:
i. APL AB
ii. Lupus anticoagulant
iii. Anticardiolipin
iv. Anti β2 glycoprotein I
v. False +ve test for syphilis
Anti Ro/SSA especially with antibody to La/SSB ((25—70%)) have been associated
with the neonatal lupus syndrome. The major manifestation of this complication is
complete heart block.
Fever ,complete heart block
Anti Ro/SSA antibody inhibit inward L type Ca+ currents.
APL ANTIBODY have been associated with abortions---IV thrombosis
Antiplatelets AB can cause autoimmune thrombocytopenia in the fetus with
hemorrhage .
ANA Screening test; sensitivity 95%; not diagnostic without clinical features
Anti-dsDNA High specificity; sensitivity only 70%; level is variable based on disease activity
Anti-Sm Most specific antibody for SLE; only 30-40% sensitivity
Anti-SSA (Ro) or Anti-SSB (La)
Present in 15% of patients with SLE and other connective-tissue diseases such as Sjögren syndrome; associated with neonatal lupus
Anti-ribosomal P Uncommon antibodies that may correlate with risk for CNS disease, including increased hazards of psychosis in a large inception cohort, although the exact role in clinical diagnosis is debated
Anti- RNP Included with anti-Sm, SSA, and SSB in the ENA profile; may indicate mixed connective-tissue disease with overlap SLE, scleroderma, and myositis
Anticardiolipin IgG/IgM variants measured with ELISA are among the antiphospholipid antibodies used to screen for antiphospholipid antibody syndrome and pertinent in SLE diagnosis
Lupus anticoagulant Multiple tests (eg, direct Russell viper venom test) to screen for inhibitors in the clotting cascade in antiphospholipid antibody syndrome
Direct Coombs test Coombs test–positive anemia to denote antibodies on RBCs
Anti-histone Drug-induced lupus ANA antibodies are often of this type (eg, with procainamide or hydralazine; p-ANCA–positive in minocycline-induced drug-induced lupus).

19
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
ANA = antinuclear antibody; CNS = central nervous system; ds-DNA = double-stranded DNA; ELISA = enzyme-linked immunoassay; ENA = extractable nuclear antigen; Ig = immunoglobulin; p-ANCA = perinuclear antineutrophil cytoplasmic antibody; RBCs = red blood cells; RNP = ribonucleic protein; SLE = systemic lupus erythematosus; Sm = Smith; SSA = Sjögren syndrome A; SSB = Sjögren syndrome B.
D/D:
1. Rheumatoid arthritis
2. Dermatomyositis
3. Fibromyalgia
4. Drug induced lupus
5. HIV---thrombocytopenia and direct coombs test
6. HBV ,HCV------renal &CNS ----
CRYOGLOBULINEMIA
7. Multiple myeloma
8. Parovirus -------polyarthritis and positive ANA
The most common bony radiographs in SLE show
periarticular osteopenia and soft-tissue swelling
without erosions.
Chest imaging studies include radiography and
computed tomography (CT) scanning .
These modalities can be used to monitor interstitial lung disease and to assess for
pneumonitis, pulmonary emboli, and alveolar
hemorrhage.
Echocardiography is used to assess for pericardial
effusion, pulmonary hypertension, or verrucous
Libman-Sacks endocarditis
Brain magnetic
resonance imaging (MRI)/magnetic resonance
angiography (MRA) is used to evaluate for central
nervous system (CNS) lupus white-matter changes ,
vasculitis, or stroke, although findings are often
nonspecific and may be absent in as many as 42% of
cases with neuropsychiatric symptoms .
Investigators have suggested that cardiac MRI (CMR)
provides an excellent alternative to clinical assessment,
electrocardiography, and echocardiography for
diagnosing SLE myocarditis. They reported that patients
who were positive for infectious myocarditis on CMR
were more symptomatic than those with active SLE
disease and that more than 50% of patients with CMR-positive myocarditis had a concurrent
positive endomyocardial biopsy.

21
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
Arthrocentesis
Arthrocentesis may be performed in patients with joint effusions, which can be inflammatory or
noninflammatory. The cell count may range from less than 25% (PMNs) in noninflammatory effusions
to more than 50% in inflammatory effusions. Viscosity will be high in noninflammatory effusions and
low in inflammatory effusions. The gross appearance of these fluids will be straw-colored or clear in
noninflammatory cases and either cloudy or yellow in inflammatory ones.
Lumbar puncture
Lumbar puncture may be performed to exclude infection with fever or neurologic symptoms.
Nonspecific elevations in cell count and protein level and decrease in glucose level may be found in
the cerebrospinal fluid of patients with central nervous system lupus.
Renal biopsies
The 2012 American College of Rheumatology (ACR) guidelines for lupus nephritis
recommend renal biopsy for all cases of active, previously untreated lupus nephritis, unless
contraindicated.Renal biopsy is used to confirm the presence of lupus nephritis; to aid in
classification of systemic lupus erythematosus (SLE) nephritis based on the International
Society of Nephrology/Renal Pathology Society (ISN/RPS) classification ,and to guide
therapeutic decisions. Another benefit of renal biopsy is in distinguishing renal lupus from
renal vein thrombosis, which may be a complication of antiphospholipid antibody
syndrome and require anticoagulation rather than immunomodulatory therapy.
Renal biopsy is indicated in the presence of the following features : 1) Increasing serum creatinine in the absence of strong evidence for another etiology (eg, sepsis, hypovolemia, medication)
2) Proteinuria of more than 1.0 g per 24 hours, as confirmed by 24-hour urine specimens or spot protein/spot creatinine ratios
3) Proteinuria of 1.5 g or more per 24 hours, along with either (1) hematuria (≥5 RBCs/hpf) or (2) cellular casts, as confirmed by a minimum of 2 tests within a short period and in the absence of alternative causes
The ISN/RPS published revisions to the World Health Organization (WHO) classification for
lupus nephritis in 2003. The classification is based on light microscopy, electron
microscopy, and immunofluorescence findings from renal biopsy results, as summarized in
the table below
Class Classification
Features
Class I Minimal mesangial Normal light microscopy findings; abnormal electron microscopy findings
Class II Mesangial proliferative Hypercellular on light microscopy
Class III Focal proliferative < 50% of glomeruli involved
Class III lupus nephritis is further Subclassified as follows:
1) Class III (A), focal proliferative: Active lesions
2) Class III (A/C), focal proliferative and
21
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
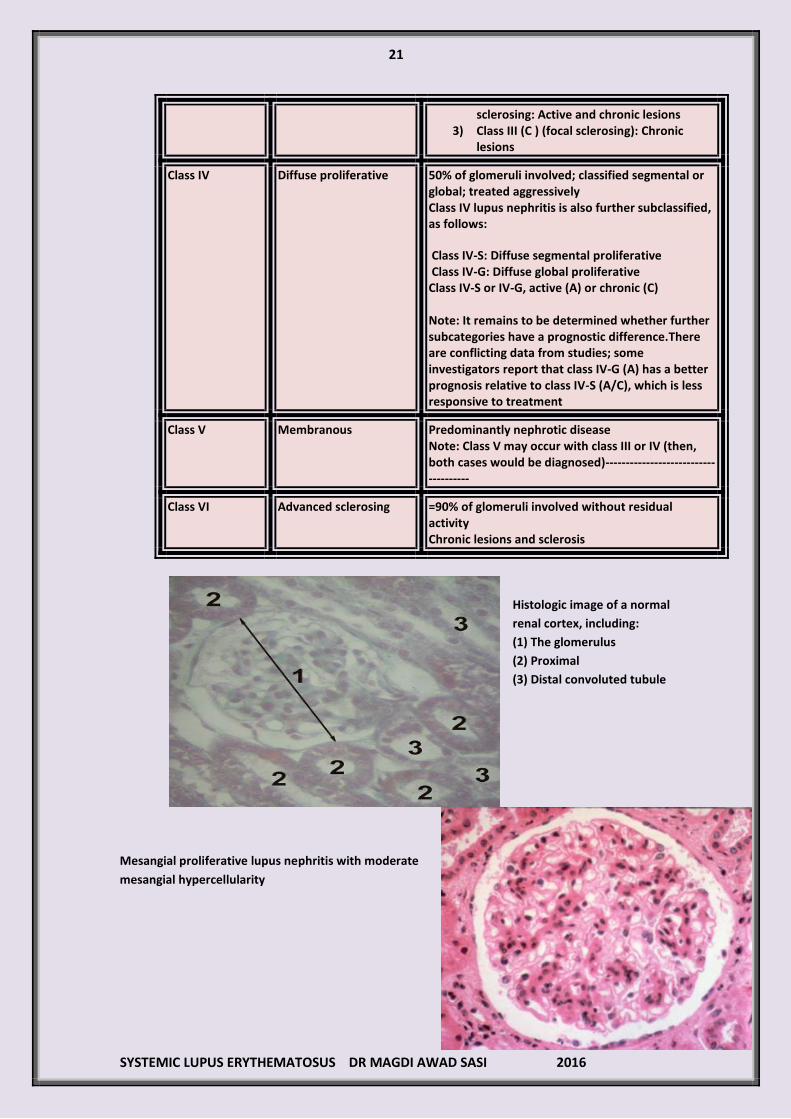
sclerosing: Active and chronic lesions 3) Class III (C ) (focal sclerosing): Chronic
lesions
Class IV Diffuse proliferative 50% of glomeruli involved; classified segmental or global; treated aggressively
Class IV lupus nephritis is also further subclassified, as follows:
Class IV-S: Diffuse segmental proliferative Class IV-G: Diffuse global proliferative Class IV-S or IV-G, active (A) or chronic (C) Note: It remains to be determined whether further subcategories have a prognostic difference.There are conflicting data from studies; some investigators report that class IV-G (A) has a better prognosis relative to class IV-S (A/C), which is less responsive to treatment
Class V Membranous Predominantly nephrotic disease
Note: Class V may occur with class III or IV (then, both cases would be diagnosed)-------------------------------------
Class VI
Advanced sclerosing =90% of glomeruli involved without residual activity
Chronic lesions and sclerosis
Histologic image of a normal
renal cortex, including:
(1) The glomerulus
(2) Proximal
(3) Distal convoluted tubule
Mesangial proliferative lupus nephritis with moderate
mesangial hypercellularity

22
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
Focal lupus nephritis.
Membranous lupus nephritis
showing thickened glomerular
basement membrane
Skin biopsies:
Many different rashes may herald
SLE, making review by a
dermatopathologist important.
Lupus skin rash often demonstrates
inflammatory infiltrates((IgG &C)) at
the dermoepidermal junction and
vacuolar change in the basal columnar
cells. Discoid lesions demonstrate
more-significant skin inflammation,
with hyperkeratosis, follicular
plugging, edema, and mononuclear
cell infiltration at the dermoepidermal
junction. In many SLE rashes,
immunofluorescent stains
demonstrate immunoglobulin and
complement deposits at the
dermoepidermal basement.
SLE and pregnancy Unlike many autoimmune diseases, (SLE) often becomes worse during pregnancy and the puerperium. Risk of maternal autoantibodies crossing placenta Leads to condition termed neonatal lupus erythematous. Neonatal lupus presents as erythematous macular rash on face or trunk, which may be photosensitive. It is a transient self-resolving illness due to passively transmitted maternal antibodies. Neonatal complications include congenital complete heart block (CHB). Strongly associated with anti-Ro (SSA) antibodies. Risk of pre-eclampsia is increased in SLE. It may be difficult to differentiate between pre-eclampsia and renal flare of SLE, and both may coexist. Differentiating features include raised anti-dsDNA antibody, decreased levels (C3 and C4) and response to steroids in the case of renal flare.
SLE >>> antibody associated with congenital heart block of baby is >>> Anti-Ro

23
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
Drug-induced lupus (DIL) :
In drug-induced lupus not all the typical features of SLE are seen, with renal and nervous
system involvement being unusual.
It usually resolves on stopping the drug.
Symptoms are said to appear some 3 weeks to 2 years after onset of therapy.
Patients with the HLA-DR3 antigen appear to be particularly at risk of developing drug-
induced lupus.
Glomerulonephritis is unusual in drug-induced lupus
Features:
Arthralgia
Myalgia
Malaise
Skin (e.g. malar rash) on face and upper chest in 25% of sufferers.
Raynaud’s phenomenon is seen in around 25%.
Pulmonary involvement (e.g. pleurisy) are common
ANA positive in 100%, but dsDNA negative
Anti-histone antibodies are found in 95% .
Anti-Ro, anti-Smith positive in around 5%
Hypergammaglobulinaemia (↑ IgG)
Normal C3 and C4.
A strongly positive ANA is a risk factor for developing drug-induced lupus, but a negative ANA would not exclude the diagnosis.
Classically, drug-induced lupus erythematosus is characterised by
a. Systemic disease with a lower incidence of nephritis
b. Lack of cutaneous involvement and
c. The presence of anti-histone antibodies.
24
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
There are features which distinguish drug-induced lupus from idiopathic SLE: a. Males and females are equally affected in drug-induced lupus, whereas idiopathic SLE
affects females nine times more frequently. b. Caucasians are affected by drug-induced lupus more commonly than AfroCaribbeans,
whereas the inverse is true of idiopathic SLE. c. In addition, the age of onset is typically older in drug-induced lupus at 50-70 years, but this
depends on the age at drug exposure. d. Fever, arthralgia, serositis and ANA occur at least as frequently in drug induced lupus as
idiopathic SLE. e. Haematological, renal and CNS involvement, and ds-DNA Ab are rare.
Most common causes:
Hydralazine , Procainamide
Less common causes:
1. Anti-epileptic--Phenytoin ,Valproate (Depakin) ,Carbamazepine
2. Anti –rheumatoid -- Penicillamine
3. Anti –tuberculous --Isoniazid
4. IBD drugs ---Sulfasalazine
5. Minocycline (ttt of acne)
6. Chlorpromazine
7. Anti hypertensive --Methyldopa ,Beta blocker , ACEI (captopril)
8. HMG –reductase inhibitor -- Statins
9. Anti thyroid -- PTU
10. Interferons
11. Anti- TNF alpha agents (infliximab and etanercept)
Discoid lupus erythematous :
It is a benign disorder generally seen more commonly
in younger African-Caribbean females.
It is a variant of SLE with only skin involvement.
It very rarely progresses to SLE (< 5% of cases).
Usually , there is negative ANA and anti-DNA.
It is characterised by follicular keratin plugs .
Lesions are discrete plaques, often erythematous,
covered by scales that extend into dilated hair
follicles.
These lesions most typically occur on the face, scalp, in the pinnae, behind
the ears and on the neck.
They can exist in areas not exposed to the sun.
The lesions can progress, with active indurated erythema at the periphery.
Central atrophic scarring is characteristic.
Diagnosis is made by lesion biopsy.
Features(( SUMMARY)):
Erythematous, raised rash, sometimes scaly
May be photosensitive
More common on face, neck, ears and scalp
25
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
Lesions heal with atrophy, scarring (may cause scarring alopecia), and
pigmentation
Management:
Topical steroid cream
Oral antimalarials may be used second-line e.g. hydroxychloroquine.
Avoid sun exposure
NB: Skin disease may occur as part of SLE, or be present as cutaneous lupus
erythematosus (frequently without any systemic disease), and with variable chance of
progression to SLE.
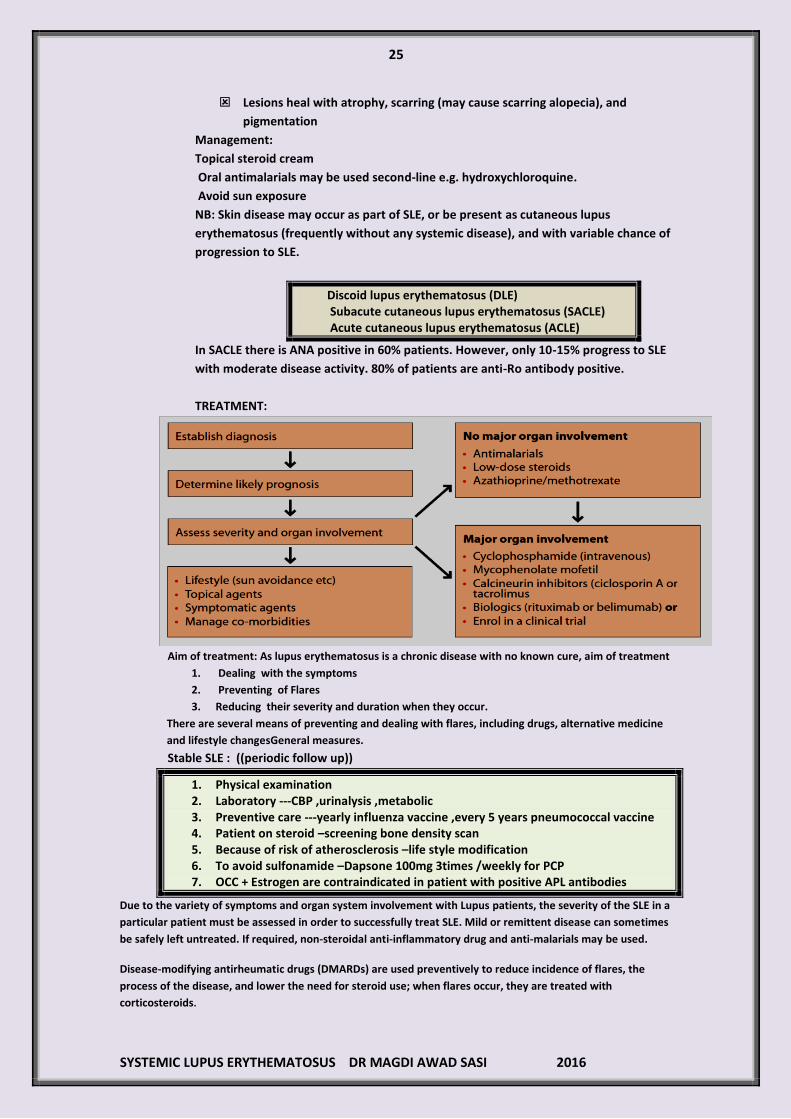
Discoid lupus erythematosus (DLE) Subacute cutaneous lupus erythematosus (SACLE) Acute cutaneous lupus erythematosus (ACLE)
In SACLE there is ANA positive in 60% patients. However, only 10-15% progress to SLE
with moderate disease activity. 80% of patients are anti-Ro antibody positive.
TREATMENT:
Aim of treatment: As lupus erythematosus is a chronic disease with no known cure, aim of treatment
1. Dealing with the symptoms
2. Preventing of Flares
3. Reducing their severity and duration when they occur.
There are several means of preventing and dealing with flares, including drugs, alternative medicine
and lifestyle changesGeneral measures.
Stable SLE : ((periodic follow up))
1. Physical examination 2. Laboratory ---CBP ,urinalysis ,metabolic 3. Preventive care ---yearly influenza vaccine ,every 5 years pneumococcal vaccine 4. Patient on steroid –screening bone density scan 5. Because of risk of atherosclerosis –life style modification 6. To avoid sulfonamide –Dapsone 100mg 3times /weekly for PCP 7. OCC + Estrogen are contraindicated in patient with positive APL antibodies
Due to the variety of symptoms and organ system involvement with Lupus patients, the severity of the SLE in a
particular patient must be assessed in order to successfully treat SLE. Mild or remittent disease can sometimes
be safely left untreated. If required, non-steroidal anti-inflammatory drug and anti-malarials may be used.
Disease-modifying antirheumatic drugs (DMARDs) are used preventively to reduce incidence of flares, the
process of the disease, and lower the need for steroid use; when flares occur, they are treated with
corticosteroids.
26
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
Cutaneous lupus---
Base line :
Avoidance of sun exposure
Use of sun blocks ((block both UV A + UV B))
For photosensitive rashes ---HYDROXYCHLOROQUINE
Onset is slow
Some improvement 1 month
Maximal effect 3 month
Bridging therapy with glucocorticoids may be necessary especially disoid lupus
If there is an incomplete response ,Quinacrine may be added.
Immunosuppressive drugs are used to control disease and steroid spare.
Examples(( Mycophenolate mofetil ,methotrexate))
Cyclophosphamide ----used for sever cutaneous vasculitis ,disfiguring lupus rashes
Thalidomide can be considered in postmenopausal patient or premenopausal with
hysterectomy or tubal ligation.
S/E : thrombosis ,peripheral neuropathy ,ovarian failure
Arthritis :
NSAIDS are the main stay of treatment.
COX 2 have not been studied for safety in SLE.
Hydroxychloroquine is added to NSAIDS for control of arthralgia and arthritis
with bridging therapy with corticosteroids.
To control severe arthritis and for steroid spare, methotrexate or leflunomide
can be added.
Folic acid must be given with methotrexate.
NOTE –the biologics that block TNF are not used for SLE because THEY CAN
INDUCE ANTIPHOSPHOLIPID ANTIBODIES AND ANTI DS DNA.
Serositis---
Mild pleurisy /pericarditis ---NSAIDS + prednislone 10mg/day
More sever ----pulse IV methylprednisolone 1000mg daily for 3 days followed by
40mg /day prednisolone.
Frequent recurrence -----Hydroychloroquine
If there is high glucocorticoid requirement ,Azathioprine or mycophenolate can
be added.
Recurrent pericardial effusion -----pericardial window
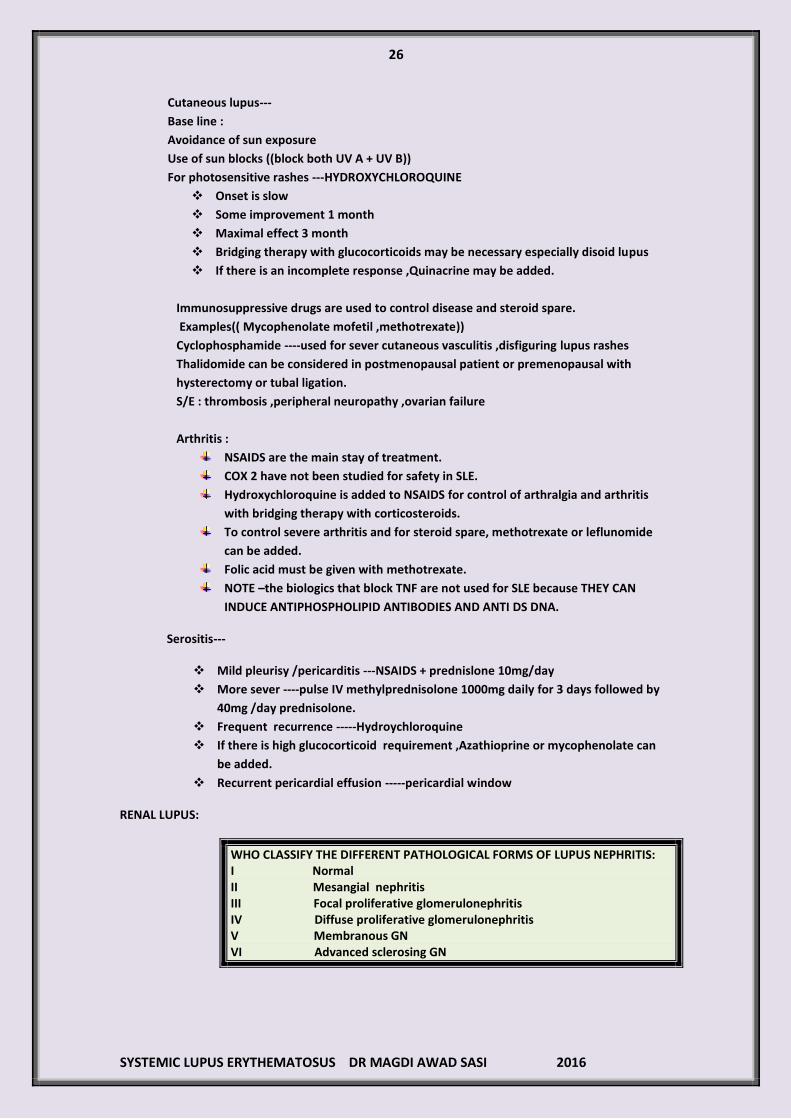
RENAL LUPUS:
WHO CLASSIFY THE DIFFERENT PATHOLOGICAL FORMS OF LUPUS NEPHRITIS: I Normal II Mesangial nephritis III Focal proliferative glomerulonephritis IV Diffuse proliferative glomerulonephritis V Membranous GN VI Advanced sclerosing GN
27
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
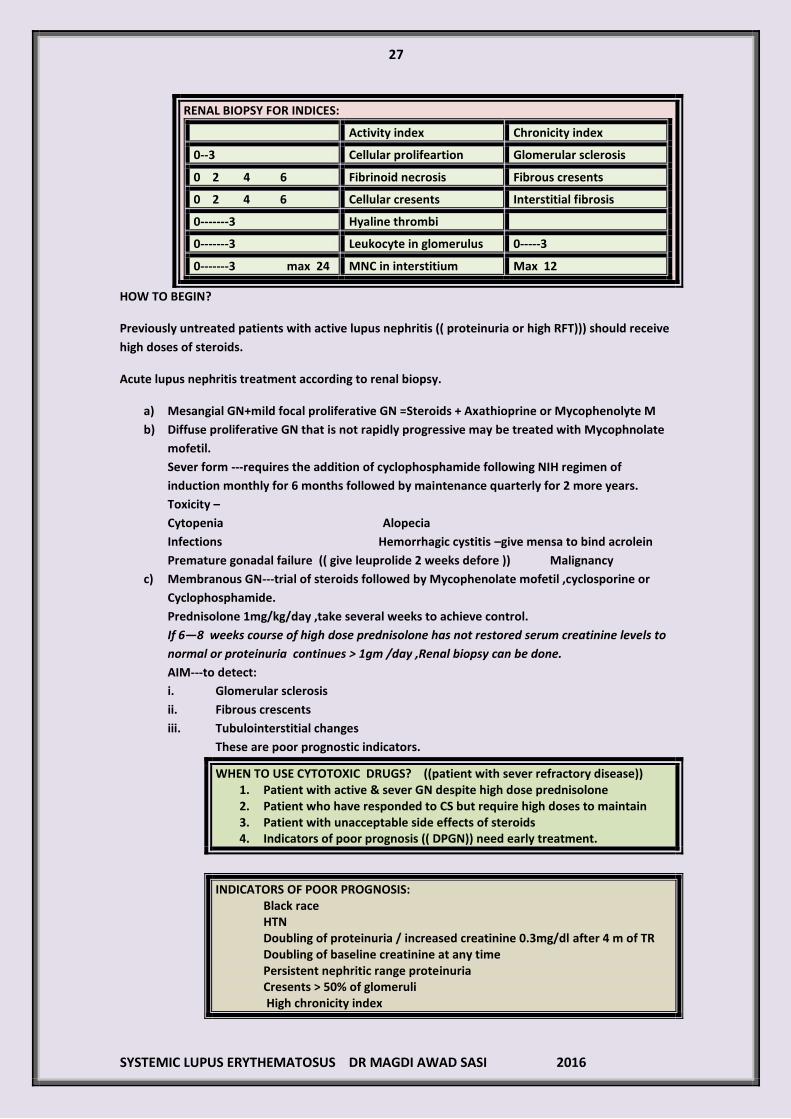
RENAL BIOPSY FOR INDICES:
Activity index Chronicity index
0--3 Cellular prolifeartion Glomerular sclerosis
0 2 4 6 Fibrinoid necrosis Fibrous cresents
0 2 4 6 Cellular cresents Interstitial fibrosis
0-------3 Hyaline thrombi
0-------3 Leukocyte in glomerulus 0-----3
0-------3 max 24 MNC in interstitium Max 12
HOW TO BEGIN?
Previously untreated patients with active lupus nephritis (( proteinuria or high RFT))) should receive
high doses of steroids.
Acute lupus nephritis treatment according to renal biopsy.
a) Mesangial GN+mild focal proliferative GN =Steroids + Axathioprine or Mycophenolyte M
b) Diffuse proliferative GN that is not rapidly progressive may be treated with Mycophnolate
mofetil.
Sever form ---requires the addition of cyclophosphamide following NIH regimen of
induction monthly for 6 months followed by maintenance quarterly for 2 more years.
Toxicity –
Cytopenia Alopecia
Infections Hemorrhagic cystitis –give mensa to bind acrolein
Premature gonadal failure (( give leuprolide 2 weeks defore )) Malignancy
c) Membranous GN---trial of steroids followed by Mycophenolate mofetil ,cyclosporine or
Cyclophosphamide.
Prednisolone 1mg/kg/day ,take several weeks to achieve control.
If 6—8 weeks course of high dose prednisolone has not restored serum creatinine levels to
normal or proteinuria continues > 1gm /day ,Renal biopsy can be done.
AIM---to detect:
i. Glomerular sclerosis
ii. Fibrous crescents
iii. Tubulointerstitial changes
These are poor prognostic indicators.
WHEN TO USE CYTOTOXIC DRUGS? ((patient with sever refractory disease)) 1. Patient with active & sever GN despite high dose prednisolone 2. Patient who have responded to CS but require high doses to maintain 3. Patient with unacceptable side effects of steroids 4. Indicators of poor prognosis (( DPGN)) need early treatment.
INDICATORS OF POOR PROGNOSIS: Black race HTN Doubling of proteinuria / increased creatinine 0.3mg/dl after 4 m of TR Doubling of baseline creatinine at any time Persistent nephritic range proteinuria Cresents > 50% of glomeruli High chronicity index
28
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
NOTE:
Patient who do not have a complete response may require a 2nd
renal biopsy to
determine for active nephritis.
If activity index is low ,effects to reduce the progression of sclerosis should be
instituted. This is by strict control of HTN.
Patient with renal failure :
1. Are candidates for transplantation
2. Recurrence of lupus nephritis in graft is low 10%
3. Patient with haemodialysis decrease disease activity.
4. Wait for 6---12 months on dialysis.
CNS ---
Focal ------Antineuronal
Psychosis ----Antimicrosomal
1. Cognitive dysfunction:
Most common
Usually mild /not rapidly progressive
Need careful follow up
Progressive should lead to a repeat MRI of brain with gadolinium ,LP ,consideration of
cerebral arteriogram.
2. APL AB should be checked & low dose aspirin used if present.
3. Psychosis & seizures are treated accordingly with an evaluation to determine for active
lupus.
If active CNS SLE is present ,treat with C.S. and immunosuppressive is initiated.
Psychosis can be caused by corticosteroids.
Seizures can be due to:
1. Infection
2. HTN encephalopathy
3. Eclampsia
4. Past infarcts –APL ,HTN , Atherosclerosis
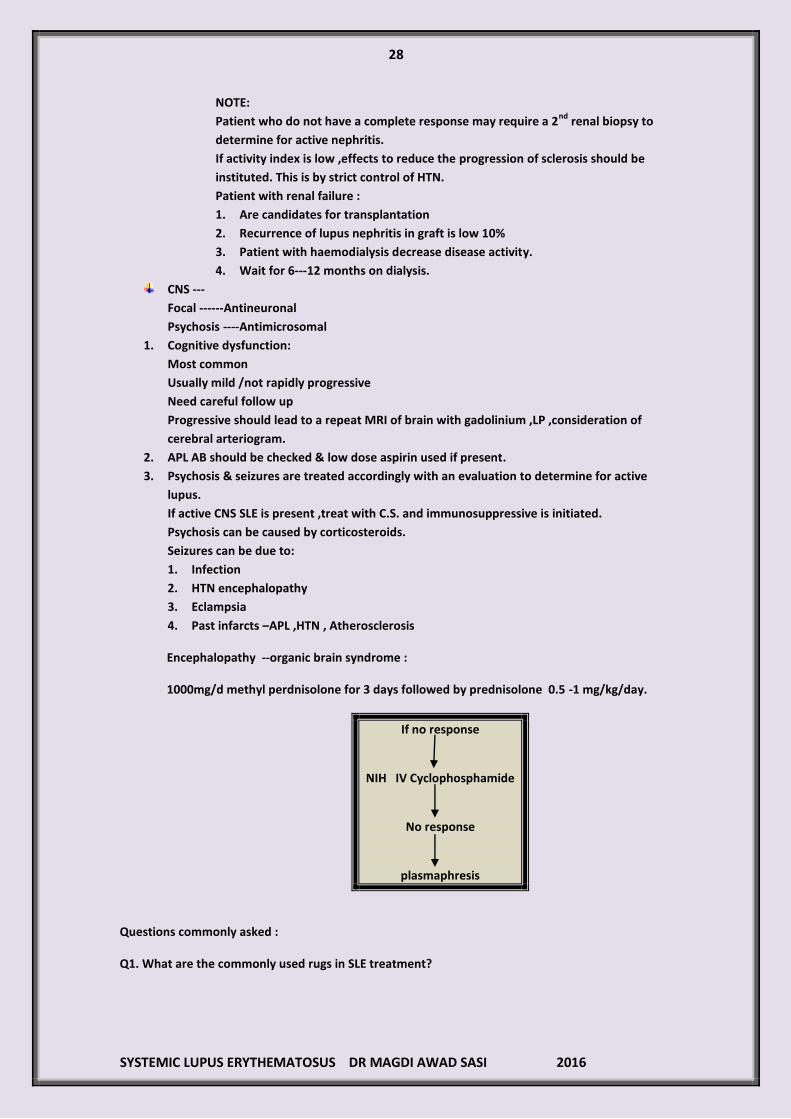
Encephalopathy --organic brain syndrome :
1000mg/d methyl perdnisolone for 3 days followed by prednisolone 0.5 -1 mg/kg/day.
If no response
NIH IV Cyclophosphamide
No response
plasmaphresis
Questions commonly asked :
Q1. What are the commonly used rugs in SLE treatment?
29
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
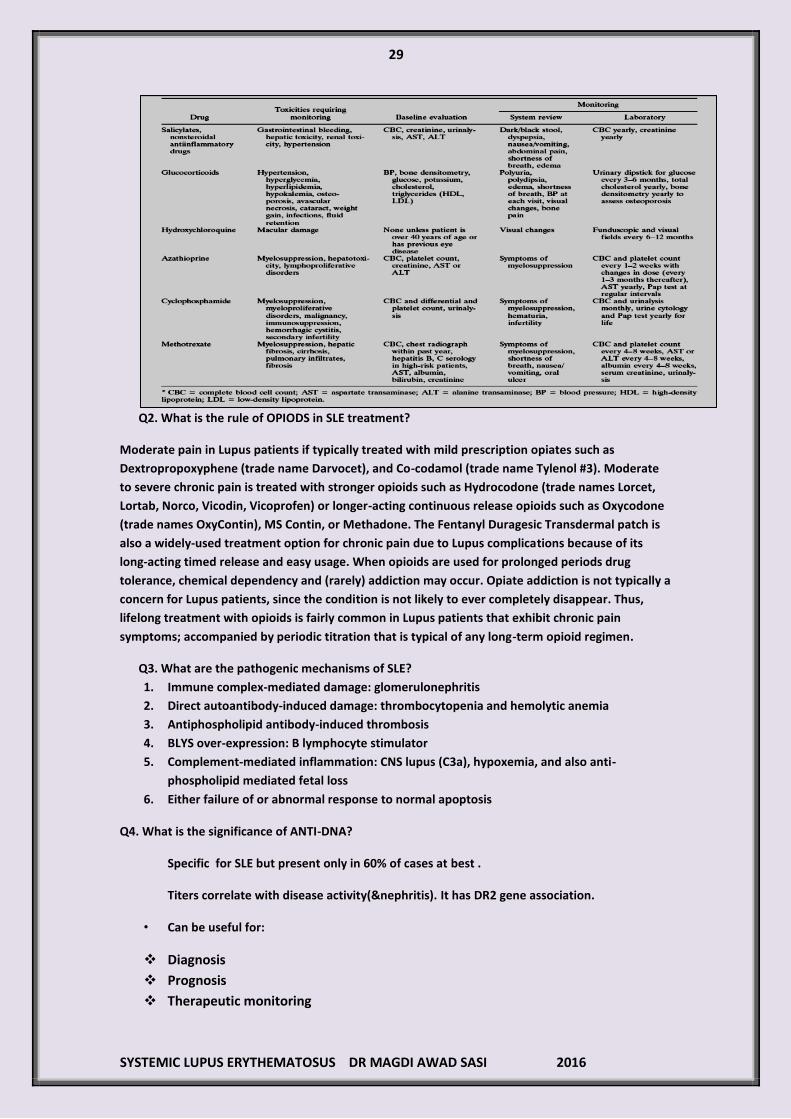
Q2. What is the rule of OPIODS in SLE treatment?
Moderate pain in Lupus patients if typically treated with mild prescription opiates such as
Dextropropoxyphene (trade name Darvocet), and Co-codamol (trade name Tylenol #3). Moderate
to severe chronic pain is treated with stronger opioids such as Hydrocodone (trade names Lorcet,
Lortab, Norco, Vicodin, Vicoprofen) or longer-acting continuous release opioids such as Oxycodone
(trade names OxyContin), MS Contin, or Methadone. The Fentanyl Duragesic Transdermal patch is
also a widely-used treatment option for chronic pain due to Lupus complications because of its
long-acting timed release and easy usage. When opioids are used for prolonged periods drug
tolerance, chemical dependency and (rarely) addiction may occur. Opiate addiction is not typically a
concern for Lupus patients, since the condition is not likely to ever completely disappear. Thus,
lifelong treatment with opioids is fairly common in Lupus patients that exhibit chronic pain
symptoms; accompanied by periodic titration that is typical of any long-term opioid regimen.
Q3. What are the pathogenic mechanisms of SLE?
1. Immune complex-mediated damage: glomerulonephritis
2. Direct autoantibody-induced damage: thrombocytopenia and hemolytic anemia
3. Antiphospholipid antibody-induced thrombosis
4. BLYS over-expression: B lymphocyte stimulator
5. Complement-mediated inflammation: CNS lupus (C3a), hypoxemia, and also anti-
phospholipid mediated fetal loss
6. Either failure of or abnormal response to normal apoptosis
Q4. What is the significance of ANTI-DNA?
Specific for SLE but present only in 60% of cases at best .
Titers correlate with disease activity(&nephritis). It has DR2 gene association.
• Can be useful for:
Diagnosis
Prognosis
Therapeutic monitoring

31
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
Q5. What is the risk of thrombosis in SLE patients?
About 20% of lupus pts have aCL and/or anti-2-glycoprotein 1 antibodies, and yet don’t have
clinical thrombosis, i.e., they are at risk. However, if any of the following factors present, alone or in
combination:
Smoking, long flights, surgery, immobilization
Drug use, e.g., cocaine
Estrogens, e.g., OC or HRT
Perhaps hyperhomocysteinemia, infection, lupus flares, other factors
Clinical Thrombosis----------------- (DVTs, PE, MIs, CVAs, PVDs)
Q6. What is the usual presentation of diffuse proliferative GN?
More common and the most severe form of GN
Hematuria and hypertension are seen in all cases with proteinuria.
Clinically --- oedema, nephrotic / high blood pressure ,hematuria /renal insufficiency .
Investigation --- decrease C3,C4 ,CH50 with antiDNA levels
Histology -----proliferative and necrotizing lesions
EM--Crescent formation in more than 50% of glomeruli on light microscope
Ig and Complement deposition ----glomerlar capillary wall
There will be marked influx of inflammatory cells—cellular cresents ,monocytes ,T cells
2 stages:
1.Active--------------inflammation
2.Chronic------------glomerular scarring ,tubulointerstitial fibrosis ,atrophy
Treatment: Cyclophosphamide and steroids
Cyclophosphamide—2 micro/kg/m2----monthly 6 months every 3 months/2 years
Q7. What is the cause of persistent low complement in patient with SLE?
Patients who are always hypocomplementemic regardless of clinical disease activity may have an
underlying complement deficiency!
Q8. What are renal complications of SLE Other than GN?
1. Renal vein thrombosis
2. Interstitial nephritis
3. Chronic renal failure on presentation
Q9.what is the cause of potassium disturbance in SLE patient ?
The cause is Interstitial nephritis .
• Rising plasma creatinine concentration and a urinalysis that is relatively normal or shows
only a few red cells and/or white cells.
• These changes may be accompanied by signs of tubular dysfunction such as metabolic
acidosis due to type 1 (distal) renal tubular acidosis, hyperkalemia due to impaired distal
potassium secretion, or hypokalemia due to salt-wasting and secondary
hyperaldosteronism .
31
SYSTEMIC LUPUS ERYTHEMATOSUS DR MAGDI AWAD SASI 2016
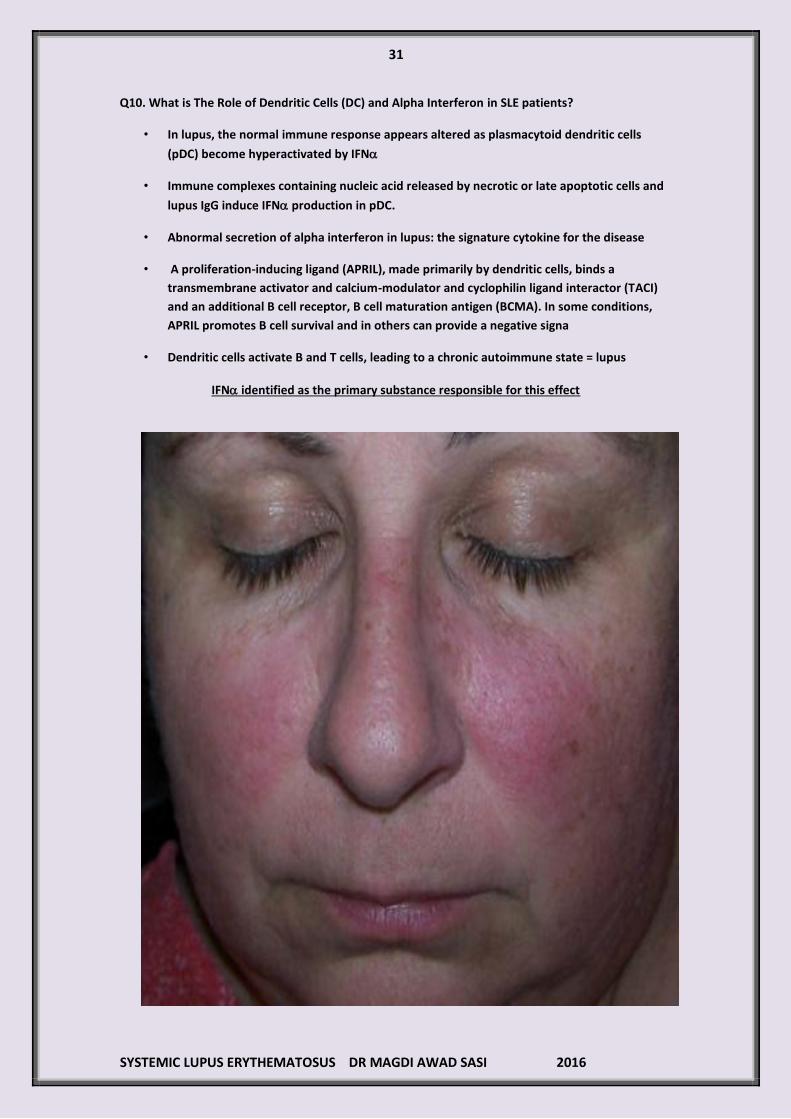
Q10. What is The Role of Dendritic Cells (DC) and Alpha Interferon in SLE patients?
• In lupus, the normal immune response appears altered as plasmacytoid dendritic cells
(pDC) become hyperactivated by IFN
• Immune complexes containing nucleic acid released by necrotic or late apoptotic cells and
lupus IgG induce IFN production in pDC.
• Abnormal secretion of alpha interferon in lupus: the signature cytokine for the disease
• A proliferation-inducing ligand (APRIL), made primarily by dendritic cells, binds a
transmembrane activator and calcium-modulator and cyclophilin ligand interactor (TACI)
and an additional B cell receptor, B cell maturation antigen (BCMA). In some conditions,
APRIL promotes B cell survival and in others can provide a negative signa
• Dendritic cells activate B and T cells, leading to a chronic autoimmune state = lupus
IFN identified as the primary substance responsible for this effect
Related Documents











