JANUARY 2013 VOLUME 109 NUMBER 1 EXPLORING PROFESSIONAL ISSUES SINCE 1905 icebreaker arctic Six weeks on an

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

JANUARY 2013 VOLUME 109 NUMBER 1
EXPLORING PROFESSIONAL ISSUES SINCE 1905
icebreakerarctic
Six weeks on an

Departments
2 FROM THE EDITOR-IN-CHIEF
3 PRESIDENT’S MESSAGE
4 FEEDBACK
“Time to reinstate the basics” | Oral care in LTC | Flu shot debate
6 PERSPECTIVES News | Calculations | The Hospital Series
12 THE RESEARCH FILE: CRITICAL READ Shift work and risk for type 2 diabetes
14 @CNA: YOUR LINK TO THE CANADIAN NURSES ASSOCIATION
20 PROMISING PRACTICES Group insulin pump starts in a pediatric diabetes program
32 REFLECTION Straight talk: Why we need to do better Barb Fry speaks out about the worrisome state of the profession
34 NURSE TO KNOW Creative expression in abundance Lynda McLeod, founder of Art by Nurses, encourages the practice of self-care through art
39 CLASSIFIEDS
40 THE LAST WORD What will U.S. health-care reform mean for Canada? Rodney Loeppky looks at the potential consequences of the implementation of Obamacare
CON
TEN
TS
canadian-nurse.com
A publication of the Canadian Nurses Association
JANUARY 2013 VOLUME 109 NUMBER 1
Feature
24 Making Sense of Indicators We are taking more health measurements than ever before, but too much data without a coordinated plan can lead to a phenomenon known as indicator chaos
Cover story
24
29 ON THE JOB
Six weeks on an Arctic icebreaker As a health officer on the Canadian Coast Guard Ship Sir Wilfrid Laurier, Theresa McGuire provided primary care, counselling, health and safety promotion and emergency treatment for the ship’s crew and passengers
We’re looking for stories of nurse-led innovation in primary care. If you have a story to share, e-mail us! [email protected]
These words held much meaning for Dr. Helen Mussallem. They were the last her father spoke to her before he died in 1963, the year she became CNA’s executive director.
Dr. M., as she was affectionately known, died on Nov. 9. She was one of the most influential nurses of our time, with a list of accomplishments that is truly humbling. At CNA House, we live her legacy every day. During her tenure as executive director, she worked to integrate the staff of Canadian Nurse with the association’s staff, developing a productive and beneficial arrangement that has continued. Our tribute to Dr. M. will appear in the February issue. But as we begin this new year, we are reminded again of the giants of the profession who built what we have today, as we carry on their work.
In this issue, we launch a special series examining different aspects of the hospital environment. In part one, we look at how hospitals manage parking facilities and revenues. Upcoming topics include environmental concerns, security and food.
Our feature article explores health indicators and the phenomenon of indicator chaos, the result of an increase in the collection of indicators and a lack of agreement on what information to collect and how to use it.
If you’re ready for some thought-provoking reflections from a colleague, look no further than Barb Fry’s column. Fry shares good news/bad news about the state of the profession and what she has committed to do to bring about positive change. We’ve invited her to expand on her ideas about scopes of practice, leadership and the art of nursing in upcoming issues.
In Promising Practices, diabetes educators describe a program designed to support groups of young patients with type 1 diabetes who are starting insulin pump therapy. We also bring you the story of occupational health nurse Theresa McGuire, who joined the crew of a coast guard ship travelling through the Northwest Passage.
So, carry on with reading this issue and, please, send us your comments. We want to hear from you.
“Carry on”
FRO
M T
HE
EDIT
OR-
IN-C
HIE
F Lisa Brazeau
EDITOR-IN-CHIEF Lisa Brazeau
MANAGING EDITOR Nahanni McIntosh
SENIOR COPY EDITOR Joan Salton
WRITER Sue Cavanaugh
PRODUCTION AND ADVERTISING Blair LeBlanc
CIRCULATION Jason Katsikaris
LAYOUT AND DESIGN Hector Palermo
@CNA Denise Rideout
CONTRIBUTORS Beverly Ensom, Kate Headley, Brenda Missen,
Jennifer Thomas
© CANADIAN NURSES ASSOCIATION
Published monthly (except July, August and December)
Canadian Nurses Association 50 Driveway Ottawa, ON K2P 1E2 Tel.: 613-237-2133 or 1-800-361-8404 Fax: 613-237-3520 [email protected] [email protected]
Peer-reviewed feature articles appearing in this publication have undergone a double-blind peer review process. The views or opinions expressed in the editorials or articles are those of the authors and do not necessarily represent the policies of CNA. Publication does not constitute CNA endorsement of, or assumption of liability for, any claims made in advertisements. Content may not be reproduced in any manner or redistributed without the prior written consent of the Canadian Nurses Association.
SUBSCRIPTIONS (One year)
Individual: Canada,* $46; U.S., $81; Foreign, $103. Student: Canada,* $25. Single copies: $20. Institutional rates are available at www.canadian-nurse.com. *Canadian subscribers, subject to applicable taxes.
CHANGE OF ADDRESS
Notice should be given at least six weeks in advance. Include previous address, along with subscriber number or registration number. [email protected]
COMMERCIAL ADVERTISING
Michelle Garneau Barbara Lebo McCormick & Associates Lebo Media Services 450-691-9515 905-709-2272 [email protected] [email protected]
CLASSIFIED AND RECRUITMENT ADVERTISING
Blair LeBlanc Ken Marskell Canadian Nurses Association The Marskell Group 613-237-2159, ext. 358 416-620-1940 [email protected] [email protected]
PUBLICATIONS MAIL AGREEMENT # 40062599
ISSN 0008-4581
Printed in Canada
Dollco, a division of the Lowe-Martin Group
2

PRES
IDEN
T’S
MES
SAG
E
On Nov. 28, CNA’s board of directors approved a position statement on influenza immunization for RNs. Recognizing that RNs care for those most vulnerable to the flu and its complications, CNA has stated that all RNs should receive the vaccine annually, to protect themselves, their families and those in their care — except those who have a condition that exempts them. CNA also believes that any immunization policy should be part of a comprehensive workplace and patient-safety strategy developed with the input of front-line RNs.
Our position statement is consistent with CNA’s commitments to advance nursing excellence and positive health outcomes in the public interest and to act in the public interest for Canadian nursing and nurses, providing national and international leadership in nursing and health. Our literature review showed that influenza immunization rates among health-care workers are as low as two per cent; the average is between 40 and 60 per cent. Given that the Public Health Agency of Canada estimates that between 2,000 and 8,000 Canadians die each year because of influenza or related complications, it is in the interest of the public that nurses are immunized and that they use other infection prevention and control precautions, including handwashing, staying home when ill and cough etiquette. It was for those reasons that in August, the B.C. government introduced a policy requiring health-care workers to either get the flu vaccine or wear a mask during flu season. In response to opposition, that policy will be studied further before being enforced. CNA received both negative and positive feedback on our position statement. While some asserted a right to personal choice, others thanked us and applauded our stand.
Florence Nightingale, a pioneer in infection control and epidemiology, was rigorous in identifying and addressing the factors contributing to illness and death in soldiers in the Crimean War, women in childbirth and people in poor house infirmaries. She believed that public policy should be guided by statistical knowledge and documented outcomes. I think she would be proud of the leadership stance CNA has taken in the interest of the public. I know I am.
Florence would be proud
January 2013 | Volume 109 | Number 1
PUBLISHER Canadian Nurses Association
BOARD OF DIRECTORS
PRESIDENT Barbara Mildon
PRESIDENT-ELECT Karima Velji
PUBLIC REPRESENTATIVE Joseph Mapa
PUBLIC REPRESENTATIVE Vincent MacLean
ASSOCIATE MEMBER REPRESENTATIVE Claire Betker
ASSOCIATE MEMBER REPRESENTATIVE Jocelyn Reimer-Kent
CHIEF EXECUTIVE OFFICER Rachel Bard
CANADIAN NURSING
STUDENTS’ ASSOCIATION Maggie Danko
ASSOCIATION OF REGISTERED NURSES
OF BRITISH COLUMBIA Susan Duncan
COLLEGE AND ASSOCIATION OF
REGISTERED NURSES OF ALBERTA Dianne Dyer
SASKATCHEWAN REGISTERED
NURSES’ ASSOCIATION Kandice Hennenfent
COLLEGE OF REGISTERED NURSES
OF MANITOBA Cathy Rippin-Sisler
REGISTERED NURSES’ ASSOCIATION
OF ONTARIO Rhonda Seidman-Carlson
NURSES ASSOCIATION OF NEW BRUNSWICK France Marquis
COLLEGE OF REGISTERED NURSES
OF NOVA SCOTIA Peter MacDougall
ASSOCIATION OF REGISTERED
NURSES OF PRINCE EDWARD ISLAND Cheryl Banks
ASSOCIATION OF REGISTERED NURSES
OF NEWFOUNDLAND AND LABRADOR Cathy Stratton
REGISTERED NURSES ASSOCIATION OF THE
NORTHWEST TERRITORIES AND NUNAVUT Angela Luciani
YUKON REGISTERED NURSES ASSOCIATION Peggy Heynen
ADVISORS FROM CNA PROVINCIAL/TERRITORIAL JURISDICTIONS
COLLEGE AND ASSOCIATION
OF REGISTERED NURSES OF ALBERTA Mary-Anne Robinson
SASKATCHEWAN REGISTERED
NURSES’ ASSOCIATION Karen Eisler
COLLEGE OF REGISTERED NURSES OF
MANITOBA Diane Wilson Maté
REGISTERED NURSES’ ASSOCIATION
OF ONTARIO Doris Grinspun
NURSES ASSOCIATION OF NEW BRUNSWICK Roxanne Tarjan
COLLEGE OF REGISTERED NURSES
OF NOVA SCOTIA Donna Denney
ASSOCIATION OF REGISTERED
NURSES OF PRINCE EDWARD ISLAND Becky Gosbee
ASSOCIATION OF REGISTERED NURSES
OF NEWFOUNDLAND AND LABRADOR Pegi Earle
REGISTERED NURSES ASSOCIATION OF THE
NORTHWEST TERRITORIES AND NUNAVUT Sheila Humphrey
YUKON REGISTERED NURSES ASSOCIATION Joy Peacock
CNA SENIOR MANAGEMENT
CHIEF EXECUTIVE OFFICER Rachel Bard
CHIEF OPERATING OFFICER Anne Sutherland Boal
Directors
PROFESSIONAL PRACTICE Patricia McGarr
POLICY AND LEADERSHIP June Webber
COMMUNICATIONS AND MEMBER OUTREACH Lisa Brazeau
FINANCE AND ADMINISTRATION Brenda Beauchamp
CORPORATE PROJECT MANAGEMENT AND
INFORMATION TECHNOLOGY SERVICES Donna Dewar
As of January 1, 2013
Barb Mildon RN, PhD, CHE, CCHN(C)
3JANUARY 2013 VOLUME 109 NUMBER 1

“TIME TO REINSTATE THE BASICS” I AGREE THAT FOSTERING THE IMAGE OF NURSES AS
“technologically capable and clinically effective” who carry out their duties with kindness and compassion is of critical importance, as Ian Peate writes (Guest Editorial, November). But I disagree that the main cause of poor-quality nursing care is poor-quality nurses. The RNs I work with, or who have cared for me, practise holistic patient/family-centred care and have the technical expertise and the caring bedside manner of educated professionals.
Much of the care patients receive is from nurses’ aides, dietary staff and, in some cases, even ambulance staff, all of whom can be mistaken for nurses because they wear scrubs. The training for workers in those disciplines is strictly task oriented. Some of
these workers actually do provide holistic care, in spite of their training, but it is not what we can expect from them.
Meanwhile, nurses are being replaced on the front lines, in direct management ranks...and throughout the health system. Instead of chastising nurses, Peate could better use his energies by nding ways to ensure that there are more nurses on the units and that the patients know who the nurses are.
– Natasha Burger, RN Faust, Alta.
ORAL CARE IN LTC THANK YOU FOR HIGHLIGHTING THE NEED FOR
better oral hygiene in long-term care (Feature, November). From 1995 to 1998, I worked as a health-care aide while training to become an RN. We received training from oral hygienists more than once on how to brush the teeth of residents, and we were encouraged to oss their teeth as well. However, this was unrealistic to maintain, because of heavy workloads. I was responsible for getting 10 to 14 residents ready for bed and up in the morning. We averaged approximately eight to 10 minutes per resident. Almost all of these residents were incontinent, required total care and were two-person transfers. Many of them had contractures, making it difficult to get them dressed and undressed. I often felt guilty for not brushing their teeth and worried about their oral health, but time constraints made it impossible to provide all the desired care.
I feel that to really accomplish better and sustained oral hygiene, there needs to be more money infused into long-term care to
decrease ratios of residents to caregivers. Otherwise, there are only good intentions and no sustainable change in practice.
– Carmen Jones, RN Toronto, Ont.
THE PHOTOS WERE ENDEARING, BUT IT WAS SAD TO
read an article about long-term care practices with no mention of staffing levels and workload. That LTC centres have terrible staff-to-patient ratios is a matter of common knowledge. By including the stat on the average time spent on carrying out oral care (16.2 seconds), it was almost as if the authors were blaming care aides. It is entirely possible that those care aides had 10 or more people they were responsible for and that was all the time they had available for this task.
We know only too well that management frequently adds additional tasks to our work, without any consideration of where the time to complete these tasks will come from. This article is further proof that managers and academics are disconnected from the day-to-day realities of patients and staff. It is really unfortunate that CN published an article with such a glaring omission. An opportunity was missed to give some attention to the issue of overworked health-care aides and the resulting poor care of the residents.
The authors proclaim the success of this intervention, but if the staf ng challenges are not addressed, it will be challenging to have success in the long term.
Calgary, Alta.
FEED
BA
CK
WE WANT TO HEAR FROM YOU…
Do you have feedback about something you’ve read
in Canadian Nurse?
E-mail us: [email protected]
Canadian Nurse Attn: Feedback
50 Driveway Ottawa, ON K2P 1E2
Please limit your submissions to no more than 250 words. Include a daytime phone number and your mailing address. Letters selected for publication may be edited for
length and clarity.
POLL
Results from the last pollAre you getting
a flu shot this year?
67%
33%
YES
333%NO
NOVEMBER 2012 VOLUME 108 NUMBER 9
EXPLORING PROFESSIONAL ISSUES SINCE 1905
CANADIAN NURSES FOUNDATION AT 50
THE STATE OF NURSING IN THE U.K.
A New Protocol for Oral Care
LOG IN AT CANADIAN-NURSE.COM TO
ANSWER OUR POLL QUESTION.
the january
poll Are you happy
with your weight? (Yes/No)
4 CANADIAN-NURSE.COM

I APPLAUD THE “NEW THINKING” THAT RESULTED IN
standardizing and implementing regular oral hygiene as a means of improving the quality of care at Deer Lodge Centre. However, let’s remember that years ago, nurses were taught to do oral care as a “basic” procedure. What we should be addressing is getting back to the basics of care. It is unfortunate that any change in policy must be justi ed to the nth degree before it is implemented. I am not undermining the hard work of those who went to such great lengths at this centre, but I must ask, Whatever happened to common sense?
– Lisa Kowalski, RN Kapuskasing, Ont.
WHEN IT COMES TO RECEIVING APPROPRIATE ORAL
care, residents in all LTC facilities get shortchanged. Is it so hard for caregivers to put toothpaste on a toothbrush so residents can brush their own teeth, or for a caregiver to do it for them? Caregivers often use the excuse that they don’t have time. There is a lot of room for education in this area. It is good that Deer Lodge Centre recognized this and is making inroads. Let’s see if it can be mandated in all LTCs across Canada.
– Jill L. O’Donnell, RN, DPH, CSSA, BA President, IRIS: Consulting for Seniors, Inc.
Toronto, Ont.
THIS ARTICLE WAS LIKE CHRISTMAS IN NOVEMBER
for me! I am so proud that another group in long-term care has decided to connect the mouth with the rest of the body and to share the results of their efforts. I work in a 60-bed LTC facility. I suggested that we adopt Brushing Up on Mouth Care, an oral health resource for those who care for older adults. This program, out of Dalhousie University, is based on research conducted in Nova Scotia that included nurses and a complete dental team.
After we implemented the oral care policy and created oral care plans for our residents, we started seeing a signi cant improvement in their oral health and in their health in general. Some of the residents had refused to eat, or were confused, lifeless and aggressive because of underlying oral problems. What a sense of accomplishment to see someone starting to live again and enjoying food and social activities!
Our biggest challenge is to keep the momentum going, which is why we have champions on each unit to remind everyone from time to time that oral care is as important
as a bath or a meal. I encourage all nursing staff in LTC to become champions for oral care in their respective facilities.
– Georgette Beaulieu, RN Truro, N.S.
FLU SHOT DEBATE I RECEIVED A FLU SHOT THIS YEAR AND IN EVERY
other year that I have worked in the health-care eld. I feel that it is a responsibility of all health-care providers to do what they can to protect patients and their families. For anyone who cannot receive vaccinations because of allergies, there is an alternative way — wearing a mask — to uphold this professional responsibility. Vaccinating care providers protects vaccinated and unvaccinated patients, reduces sick leave and sets a good example for the public. I personally support this new policy (Perspectives, October) and believe that it will help to protect those who are already vulnerable.
– Carmen Zmaeff Fourth-year BSN student
Campbell River, B.C.
I AM PROUD CN PRINTED THE LETTER FROM SARA
Gough (Feedback, November) regarding the forced vaccination policy underway in British Columbia. Vaccines are medical marvels, but the u vaccine, which is based on weak science, is no such wonder. We live in frightening times when a medical intervention of questionable ef cacy can be forced upon our nurses. Whether we personally support the vaccine or not, we must not allow this erosion of human rights to occur.
– Jeff Campbell, RN, BScN Toronto, Ont.
National Nursing Week May 6-12, 2013
cna-aiic.ca
Excited to see this year’s
NNW poster? Check it out online
and buy yours today!
CHOOSE THE COVER OF
CANADIAN NURSE!
We want you to tell us what you’d like to see on the cover of the
May issue of Canadian Nurse — our National Nursing Week issue.
The theme for National Nursing Week for 2013-2014 is Nursing:
A Leading Force for Change. You can send us your suggestion for a photo shoot or an illustration, or you can
even send us original artwork — whatever you think
E-mail [email protected] (with “NNW cover” in the subject
line) by March 1. The winning entry will receive
a CNA prize pack.
For complete guidelines and rules, visit www.canadian-nurse.com.
5JANUARY 2013 VOLUME 109 NUMBER 1
6 CANADIAN-NURSE.COM
PER
SPE
CTIV
ES
How do you say in Inuktitut?
Is spending under control?
Communicating clearly and accurately with patients is always important, particularly when it comes to sexual health information. But in Inuit communities, problems with translations of health terms into Inuktitut means that patients may not even understand what they are being diagnosed with, never mind what their treatment options are. A new tool aims to change that. Tukisiviit: Do You Understand? is a glossary of sexual health terms translated from English into the five most common dialects of Inuktitut — according to the last census, the mother tongue of more than 33,000 Canadians.
The glossary, available as a booklet or online, has been distributed to schools, clinics and hospitals across the Inuit regions of the North. It covers male and female sexual anatomy, sexually transmitted infections, including chlamydia, syphilis and HIV, f luids that
After a decade that saw yearly increases of seven per cent in total spending on health care in Canada, the latest numbers from the Canadian Institute for Health Information may come as a relief. National Health Expenditure Trends, 1975 to 2012 estimates that total public- and private-sector expenditures in 2012 will be $207.4 billion, an increase of just 3.4 per cent over the figure estimated for 2011. The last time there was such a small increase was the mid-1990s.
Why is the pace of spending
slowing? Some experts argue that increasing use of technology and new models of care are creating efficiencies. Others point to cost-containing efforts in expenditures for hospitals, drugs and physician services, which together represent 59.5 per cent of total spending. Staff compensation — the majority of which goes to nurses — accounts for 60 per cent of hospital costs.
Of all jurisdictions, Nova Scotia dedicates the highest proportion of its budget to health care, estimated at 47.9 per cent for 2011; Quebec’s
can transmit STIs, risk behaviours for contracting STIs, what to expect during examinations, testing and treatments, and prevention strategies.
The glossary was produced by Pauktuutit Inuit Women of Canada, a national non-profit organization that works to address Inuit-specific HIV and sexual health issues as part of a broad range of activities. In 2010, after extensive consultation with stakeholders, Pauktuutit developed a strategic plan to address the gaps in knowledge, programs and services for Inuit sexual health; language terminology was identified as a priority. Funded by the Public Health Agency of Canada, the glossary is the result of a forum attended by members of the Canadian Inuit HIV/AIDS Network, language experts, sexual-health content
proportion is the lowest (at 30.1 per cent). In dollar figures, Newfoundland and Labrador is expected to spend $5,190 per person in 2012 (the highest across the country); the estimate for Quebec is $3,513 (the lowest amount). Not surprisingly, the per-person spending estimates fluctuate dramatically within age groups. Nationally, the average health-care expenditure in 2010 for infants under one was $9,264; for all those age 80 and older, it was $20,113.
experts, community health and social service providers, educators, elders and youth, among others.
Sexually transmitted diseases are a major problem in the North, occurring at rates much higher than the national average. In 2009, the chlamydia rate in Nunavut was 3,772.2 per 100,000 population; the rate for Canada as a whole was 258.5 per 100,000. And during the same year, the rate of gonorrhea infections was almost 50 times higher in Nunavut (1,603.3/100,000) than the national average (33.1/100,000).
6 CANADIAN-NURSE.COM

PER
SPE
CTIV
ES
IN BRIEF
Visit canadian-nurse.com to find links to these studies.
Expanded prescribing authority
The federal government has approved the New Classes of Practitioners Regulations, which gives NPs, midwives and podiatrists the authority to prescribe, administer and provide drugs listed under the Controlled Drugs and Substances Act. Health Canada says the move is intended to enhance the flexibility and timeliness of health-care service delivery. Up to this point, only medical doctors, dentists and veterinarians have been allowed to prescribe controlled substances.
NPs have been granted the widest authority of the three provider groups and are approved to prescribe everything covered under the act, except for heroin, cannabis, opium, coca and anabolic steroids other than testosterone. Decisions made to exclude particular drugs were based on the needs of each profession’s patients as well as the risk of drug diversion or abuse.
Although some jurisdictions already have legislated scopes of practice for NPs that include controlled substance prescribing, federal law prohibited NPs from doing so. But even with this barrier removed, all NPs can’t break out their prescription pads just yet. As provincial and territorial colleges and associations made clear soon after the regulation was approved, much depends on the existing legislation and scope of practice in a jurisdiction. Some regulatory bodies will have to develop educational requirements and prescribing competencies and standards before scopes of practice can be changed...a process that will likely take quite a while.
Ancient Chinese secret The mung bean, a legume native to India and commonly eaten in China, may protect against life-threatening sepsis, by neutralizing one of the
have been used since the 11th century in Chinese Evidence-Based
Complementary and Alternative Medicine, researchers administered mung bean extract to
Low-tech treatment for infections There is growing evidence that fecal transplantation is an effective therapy for recurrent
transplantation is performed by collecting stool from a healthy donor, mixing it with water
Feds say yes to oxycodone manufacturers
her provincial counterparts to delay approval of a generic version
a complete ban on the drug; the province is dealing with widespread oxycodone addictions, particularly in northern aboriginal reserves, where estimates are that more than half of
Obese patients more likely to make it through pneumonia Excess weight appears to have a protective effect when it comes to surviving pneumonia, according to a study published in Clinical Microbiology and Infection
More than meets the eye
been able to communicate for the first time with
patient was instructed to indicate whether he was in
another case, a patient showed awareness of an
had formed new memories afterdoesn’t mean all such patients have consciousness but agree that it does raise ethical issues
ALL
PH
OTO
S:
7JANUARY 2013 VOLUME 109 NUMBER 1
CALCULATIONS
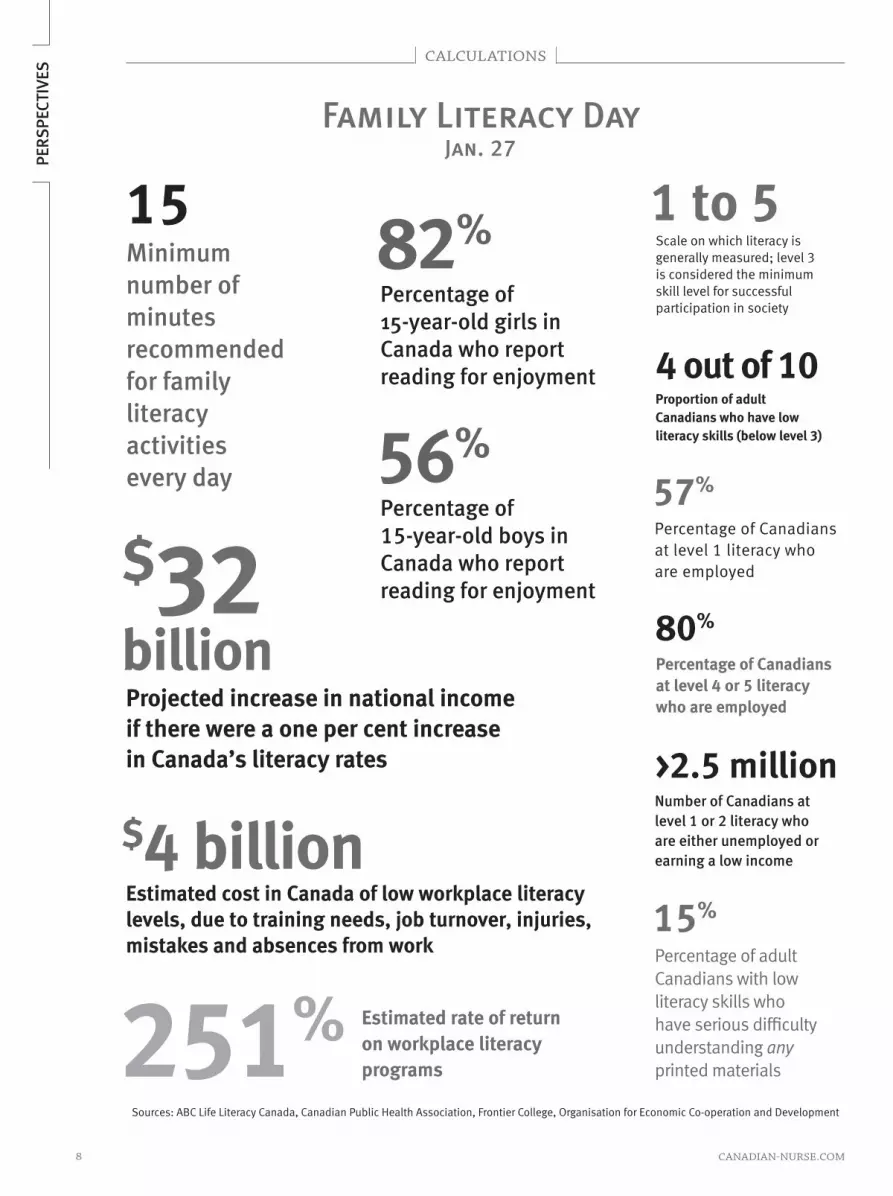
Sources: ABC Life Literacy Canada, Canadian Public Health Association, Frontier College, Organisation for Economic Co-operation and Development
PER
SPE
CTIV
ES
15 Minimum number of minutes recommended for family literacy activities every day
$32billion Projected increase in national income if there were a one per cent increase in Canada’s literacy rates
$4 billion Estimated cost in Canada of low workplace literacy levels, due to training needs, job turnover, injuries, mistakes and absences from work
Scale on which literacy is generally measured; level 3 is considered the minimum skill level for successful participation in society
1 to 5
Proportion of adult Canadians who have low literacy skills (below level 3)
4 out of 10
Percentage of Canadians at level 1 literacy who are employed
57%
Percentage of Canadians at level 4 or 5 literacy who are employed
80%
Number of Canadians at level 1 or 2 literacy who are either unemployed or earning a low income
>2.5 million
Percentage of adult Canadians with low literacy skills who have serious dif culty understanding any printed materials
15%
Estimated rate of return on workplace literacy programs 251%
82% Percentage of 15-year-old girls in Canada who report reading for enjoyment
56%Percentage of 15-year-old boys in Canada who report reading for enjoyment
Family Literacy DayJan. 27
8 CANADIAN-NURSE.COM

9JANUARY 2013 VOLUME 109 NUMBER 1
I heard hernia surgeryis incredibly painful.
NOT ANYMORE. The Covidien ProGrip™ composite mesh for hernia repair is a self-gripping technology that potentially eliminates the need for fixation of any kind. The result? Patients experience less post-operative pain than conventional fixation-based repair, according to a recent clinical trial. It’s just one example of how Covidien is collaborating with healthcare professionals to solve medical issues to help improve patient care and safety.
At Covidien, we’re not just committed to medical innovation — we’re committed to making a difference in patients’ lives. See how at covidien.com
COVIDIEN, COVIDIEN with logo, Covidien logo, and positive results for life are U.S. and internationally registered trademarks of Covidien AG. Other brands are trademarks of a Covidien company. © 2012 Covidien

Hospitals: they can be large or small; historic buildings or sleek, modern facilities that function like mini-cities; patient-centred...or patient-terrifying.
In The Hospital Series, we’re looking at the challenges of providing non-clinical services — parking, environmental responsibilities, patient meals, building
and room design, and security — and how some facilities are innovating
Parking: Who should pay?
n November 2011, an editorial in the Canadian Medical Association Journal called hospital parking fees a barrier to health care, saying the charges amount to “parking-centred health care,” and recommended hospitals stop charging patients for parking. The editorial stirred up a
debate in the media. The Ontario Nurses’ Association, for one, agreed with the recommendation and noted that many of its members could tell stories about patients who had avoided seeking care or had cut appointments because of high parking costs.
Tom Badcock is the executive director of the Physically Disabled Service Centre in St. John’s and a cancer outpatient at the city’s Health Sciences Centre. He is campaigning against the practice of charging patients for parking, claiming that such costs contravene the Canada Health Act because they constitute indirect user fees. After complaining to the hospital administration and the provincial health minister to no avail, Badcock told local media he planned to file a lawsuit against Eastern Health.
Some argue that parking fees should remain in place as a deterrent to our car-happy culture — particularly in urban centres, where public transit is both readily available and encouraged. Considering the all-hours nature of life and work in hospitals, however, not to mention the
harshness of Canadian winters, expecting hospital workers and visitors to use public transportation is probably not going to be met with enthusiasm, particularly in towns that are underserved by transit. And patients who live in rural areas have no choice but to drive into town for care.
One of the main arguments against abolishing parking fees is that hospitals often use these revenues for chaplaincy, foundation programs and other patient services. In Ontario, hospitals receive only 85 per cent of their budget from the health ministry and therefore, some would argue, need the estimated one per cent of revenue that comes from parking fees. Others ask, if parking structures were not revenue generating, who would pay to maintain them? Should hospitals be expected to cover the cost of snow removal, for example, in their already constrained budgets?
Some hospitals have gone so far as to contract out their parking to private, for-profit companies such as Impark, which manages parking facilities for nearly 100 health-care centres across North America. In the case of a new hospital, a public-private partnership may see a parking company take on not only the operation but also the construction and maintenance of the parking garage. Hospitals can reduce costs by contracting out parking, but the people who have to park in privately managed lots are paying the
PER
SPE
CTIV
ESTHE HOSPITAL SERIES
10 CANADIAN-NURSE.COM

price. The Internet is full of complaints about the high fees and predatory ticketing practices that often come with privatization.
There are some signs of greater accommodation. Parking fees for patients, visitors and staff were abolished at hospitals in Scotland and Wales in 2008, except in privately owned lots. Several hospitals in North America have recognized the needs of patients and are trying to make parking less painful. Children’s Hospital Colorado in Denver provides free parking to patients and visitors and even offers a complimentary valet service from 6 a.m. to 6 p.m. The Vancouver Island Health Authority offers free parking for renal dialysis patients at all its hospitals. Here’s hoping these trends toward people-centred parking continue. ■
More than 300 nurses
walked off the job in
Western Australia one day
last fall to attend a rally
to protest increases in
parking rates for staff and
patients. A representative
from the Australian
Nursing Federation noted
that costs at Sir Charles
Gairdner Hospital in Perth
rose from AU$1.50 per
day in 2010 to AU$4.80
per day in 2012 (a 220
per cent increase) and
that in some locations,
costs were projected to
increase sevenfold in the
next three years.
How rates compare
public hospitals in mid-sized cities
of countries with comparable health
$12
Regi
na,
Cana
da
Regina General Hospital
$1298
Pitt
sbur
gh,
U.S
.
Allegheny General Hospital
$1347
Live
rpoo
l, En
glan
dRoyal
Liverpool University Hospital
$1017
Fran
kfur
t,
Ger
man
y
J. W. Goethe University Hospital
$2938
Nag
ano,
Ja
pan
Nagano Red Cross Hospital
$0
Canb
erra
, Au
stra
lia
Canberra Hospital
Think some of the daily maximum rates hospitals charge for
parking are outrageous? In some hospital lots, there is no daily
maximum — the meter never stops running. The emergency lot at
Vancouver General Hospital charges $3.25 per half hour, which
means a 24-hour stay costs $156.
11JANUARY 2013 VOLUME 109 NUMBER 1

THE
RES
EAR
CH F
ILE
Shift work and risk for type 2 diabetes
CRITICAL READ
SUMMARY
Purpose: To determine the relationship between duration of rotating night shift work and the risk of developing type 2 diabetes in two cohorts of female nurses in the U.S.
Design: Prospective longitudinal study
Participants: 69,269 women, age 42 to 67, in the Nurses’ Health Study (NHS) 1 and 107,915 women, age 25 to 42, in NHS 2, without diabetes at baseline, were followed for 18-20 years
Methods: Participants completed detailed questionnaires every two to four years. The total years of shift work was defined as the number of years that women had worked rotating night shifts — classified as at least three nights per month in addition to other shifts in the same month. If participants self-reported diabetes, they completed a supplementary questionnaire to confirm this diagnosis. Important covariates potentially associated with diabetes, including body weight, smoking, physical activity, family history, menopausal status and diet quality, were considered. The researchers determined the incidence of
new type 2 diabetes, using Cox proportional hazard models adjusted for known diabetic risk factors.
Results: When the researchers controlled for age and the other covariates, they found that the women who had done shift work for at least 20 years were 1.58 times more likely to develop type 2 diabetes in comparison to those who had no shift work history. The longer women worked in shift work positions, the more likely they were to develop diabetes. The researchers also found that rotating night shift work may be associated with increased weight gain.
COMMENTARY AND PRACTICE IMPLICATIONS
The major strengths of this study are its prospective design and large population-based sample, which allowed researchers to conclude with confidence that exposure to shift work was related to women actually developing diabetes, when factors related to diabetes development were also considered. However, the study has limitations, as the researchers acknowledge. They had no detailed information on patterns of night shift work rotations. Historically, these have included long stretches of eight-hour shifts; more recently, shorter stretches of 12-hour shifts are more common. Furthermore, other work-related characteristics such as employment status (full time or part time) and work strain were not taken into account. A nurse working full time in a stressful setting may have greater exposure to the potential harmful effects of shift work.
The important take-home messages are that specific factors associated with rotating night shift work may be increasing some women’s risk for developing type 2 diabetes and that maintaining a healthy weight and lifestyle is protective. The findings support the need for effective workplace health strategies designed to screen for chronic diseases and contributing factors and to promote healthy lifestyle behaviours. From a research perspective, there is a need to understand the underlying mechanisms that may link rotating night shift work to increased risk for chronic diseases. ■
Pan, A., Schernhammer, E. S., Sun, Q., & Hu, F. B. (2011). Rotating night shift work and risk of type 2 diabetes: Two prospective cohort studies in women. PLoS Med 8(12):e1001141. doi:10.1371/journal.pmed.1001141
JOAN TRANMER, RN, BScN, M.Sc., PhD, IS A PROFESSOR IN THE SCHOOL OF NURSING AND COMMUNITY HEALTH AND EPIDEMIOLOGY, QUEEN’S UNIVERSITY, KINGSTON, ONT.
RESOURCES ON THIS TOPIC EBSCO-CINAHL AND MEDLINE full-text articles
Szosland, D. (2010). Shift work and metabolic syndrome, diabetes mellitus and ischaemic heart disease. International Journal of Occupational Medicine and Environmental Health, 23(3), 287-291. doi:10.2478/v10001-010-0032-5
Scientists discover how shift work may threaten health. (2009). Harvard Women’s Health Watch, 16(10), 7.
Esquirol, Y., Bongard, V., Mabile, L., onnier, B., Soulat, .-M., & Perret, B. (2009). Shift work and metabolic
syndrome: Respective impacts of job strain, physical activity, and dietary rhythms. Chronobiology International, 26(3), 544-559.
Biggi, N., Consonni, D., Galluzzo, V., Sogliani, M., & Costa, G. (2008). Metabolic syndrome in permanent night workers. Chronobiology International, 25(2), 443-454.
12 CANADIAN-NURSE.COM

Bio-Oil® is a skincare oil that helps improve the appearance of scars,stretch marks and uneven skin tone. It contains natural oils, vitamins andthe breakthrough ingredient PurCellin Oil™. For comprehensive productinformation and results of clinical trials, please visit bio-oil.com. Bio-Oil isthe No.1 selling scar and stretch mark product in 11 countries.

Working for nurses, working for Canadians
As a new year begins, I am excited about the opportunities to show you that CNA is your strong national association through which you can support each other and speak with a powerful, unified voice.
The results from our member and nursing student surveys have given us great insight into your wants, needs and expectations, which will be reflected in our work. Here’s a
sampling of our plans for 2013:The recommendations from CNA’s independent
National Expert Commission will be front and centre in much of our work. If you haven’t yet, I urge you to read A Nursing Call to Action, expertcommission.cna-aiic.ca, a report that contains forward-thinking ideas and nursing-led solutions to today’s health-care challenges. You can get even more insight by checking out our special Globe and Mail feature, globeandmail.com/canadiannurses.
We’ll also shine the spotlight on you, Canada’s RNs. We plan to unveil a dynamic campaign that promotes the remarkable depth and breadth of RNs and we’ll work to raise the profile of clinical nurse specialists. We’re also bringing our Nurse Practitioners: It’s About Time! campaign to new jurisdictions.
CNA’s efforts to influence health policy will continue in full force through initiatives like our participation in the health-care innovation working group, led by the provincial/territorial premiers.
We have plans to celebrate 30 fantastic nurses by honouring them with Queen Elizabeth II Diamond Jubilee medals.
We’ll support CNA past president Judith Shamian in her bid to be president of the International Council of Nurses. And in June, CNA and our partners at the National Health Leadership Conference will bring you the first-ever nursing leadership stream.
2013 will be action-packed… to get the most out of it, remember to read the Commission’s report!
Rachel Bard, RN, [email protected]
CEO OUTLOOK Remembering a remarkable nurse
The nursing community came together in November to celebrate the life of Dr. Helen K. Mussallem, a remarkable nurse leader who passed away in Ottawa on Nov. 9 at age 97.
We were privileged at CNA to have this strong visionary leader as our executive director from 1963 to 1981. Over her lifetime, she had a stellar international career, becoming one of the most influential figures in Canada’s nursing history. Mussallem’s numerous honorary doctorates and prestigious awards, including the International Red Cross’s Florence Nightingale Medal and the Companion of the Order of Canada, made her Canada’s most decorated nurse.
TEC
KLE
S P
HO
TOG
RA
PH
Y IN
C.
CNA YOUR L INK TO THE CANADIAN NURSES ASSOCIATION
YOUR L INK TO THE CANADIAN NURSES ASSOCIATION
Members encouraged to submit resolutionsCNA encourages nurse members to raise issues of national concern and make your views known. One way to do so is to submit resolutions.
To submit a resolution, you must fill out a submission form outlining the connection between the motion and CNA’s mission and goals and send it to CNA’s governance coordinator. The contact information, resolution guidelines and the submission form are found on CNA’s website, cna-aiic.ca.
The deadline for submissions from individual nurse members is March 26, 2013. For CNA jurisdictional and associate members, the deadline is May 14, 2013. Resolutions will be presented at the 2013 annual meeting in Ottawa on June 19.
Dr. Helen K. Mussallem
1915-2012
14 CANADIAN-NURSE.COM

cna-aiic.ca
CNA’s board of directors
1. Maggie Danko, president, CNSA
2. Karima Velji, president-elect, CNA
3. Barb Mildon, president, CNA
4. Rachel Bard, CEO, CNA
5. Susan Duncan, president, ARNBC
6. Cathy Stratton, president, ARNNL
7. France Marquis, president, NANB
8. Robert Nevin, president, RNANT/NU
9. Peggy Heynen, president, YRNA
10. Vincent MacLean, public representative
11. Claire Betker, associate member representative
12. Cheryl Banks, president, ARNPEI
13. Rhonda Seidman-Carlson, president, RNAO
14. Kandice Hennenfent, president, SRNA
15. Dianne Dyer, president, CARNA
16. Cathy Rippin-Sisler, president, CRNM
17. Jocelyn Reimer-Kent, associate member
representative
18. Peter MacDougall, president, CRNNS
Missing from photo:
Joseph Mapa, public representative
TEC
KLE
S P
HO
TOG
RA
PH
Y IN
C.
9
1 2 3 4 56
7
816
17
18
15
14
13
12
11
10
RNs join call to end povertyCNA recently joined members of an anti-poverty coalition to call for an end to poverty, part of our ongoing efforts to raise awareness of the social determinants of health.
As a way to bring attention to the International Day for the Eradication of Poverty, Oct. 17, a number of media and public activities took place, including a press conference on Parliament Hill, the release of the Citizen for Public Justice’s report on the state of poverty
in Canada, and a panel discussion with people with lived experiences of poverty and members of an all-party anti-poverty caucus.
CNA participated in some of the events through our membership in Dignity for All, a non-partisan coalition of provincial and national organizations, individuals, and MPs and Senators who are dedicated to eliminating poverty. Joyce Douglas, CNA nurse advisor and coalition representative, said RNs are
encouraged to join the campaign at dignityforall.ca.
“This work fits well with our own priority to address the social determinants of health that are fundamental to one’s health, such as socio-economic status,” Douglas said. For more information on CNA’s social determinants work, e-mail [email protected].
The board of directors met at CNA House, Nov. 26-28
15JANUARY 2013 VOLUME 109 NUMBER 1

Annual meetings and conferencesJanuary-June 2013
Canadian Nursing Students’ Association Jan. 23-26 Halifax, N.S. www.cnsa.ca
Canadian Association of Neonatal Nurses Feb. 10-12 Montreal, Que. www.neonatalcann.ca
Canadian Respiratory Health Professionals April 11-13 Quebec City, Que. www.lung.ca/crhp-pcsr/
home-accueil_e.php
Operating Room Nurses Association of Canada April 21-25 Ottawa, Ont. www.ornac.ca
Canadian Association of Nurses in AIDS Care April 25-28 Toronto, Ont. www.canac.org
Canadian Occupational Health Nurses Association Inc. April 30-May 2 Edmonton, Alta. www.cohna-aciist.ca
Canadian Association for Enterostomal Therapy May 9-12 Toronto, Ont. www.caet.ca
Canadian Orthopaedic Nurses Association May 27-29 Vancouver, B.C. www.cona-nurse.org
Canadian Association of Rehabilitation Nurses May 29-31 Vancouver, B.C. www.carn.ca
National Emergency Nurses’ Affiliation May 29-31 Vancouver, B.C. www.nena.ca
Canadian Gerontological Nursing Association May 29-June 1 Richmond, B.C. www.cgna.net
Canadian Association for the History of Nursing June 1-3 Victoria, B.C. www.cahn-achn.ca
Community and Hospital Infection Control Association – Canada June 1-5 Ottawa, Ont. www.chica.org
Canadian Association of Neuroscience Nurses June 11-14 Montreal, Que. www.cann.ca
Community Health Nurses of Canada June 17-19 Kelowna, B.C. www.chnc.ca
16 CANADIAN-NURSE.COM

cna-aiic.ca
Supporting your practice: CNA’s new tools and resources
CNA Webinar Series: Progress in PracticeOur winter 2013 lineup is here. Register online!
Strengthening Nursing Practice Through Information and Communication Technologies
Stay the Course! Be Prepared for the 2013 CNA Certification Exams
What if Interprofessional Care Teams were the Norm in Canada?
Get Ready for the CRNE
New Resources Position Statement on Influenza Immunization of Registered Nurses
In this new statement, CNA outlines its position in detail and provides important supporting evidence. It is CNA’s position that all RNs should receive the influenza vaccine annually to protect themselves, their families and those in their care, with the exception of RNs for whom influenza immunization is contraindicated.
Report Shows Record-high Number of RN Grads
The 2010-2011 Registered Nurses Education in Canada Statistics report, published by CNA and the Canadian Association of Schools of Nursing, reveals the number of graduates of entry-to-practice RN programs has risen steadily in the past decade. In 2011, there were 10,827 graduates, a 6.9 per cent increase from 2010 and a record high. Visit cna-aiic.ca for the full picture.
New on NurseONE.ca Webliographies
Nursing leaders share solutions with parliamentariansCNA leaders descended on Parliament Hill on Nov. 27 to convince over 40 MPs and senators that taking action on CNA’s recent National Expert Commission report can improve Canadians’ health.
The day of meetings was part of our ongoing advocacy and policy work to improve health and keep people well.
During CNA’s Parliament Hill Day, more than 30 nurse leaders — including members of CNA’s board of directors — spoke to parliamentarians about ways to improve the nation’s health and the importance of sustaining Canada’s publicly funded, not-for-profit health-care system. Two of the Commission’s action items were particularly influential throughout the day.
We asked MPs and senators to commit to achieving a top-five global ranking on five priority health and systems performance goals in the next five years. “What gets measured gets managed,” president Barb Mildon said. “As one of the top spenders in the world on health, we need to rank among the best for key indicators, including infant mortality and diabetes rates, but we don’t.”
Secondly, CNA’s leadership urged MPs and senators to bring health into all policies by applying an equity-based health impact assessment to evaluate the health benefit and consequences of all future decisions. Results from a nationwide Nanos Research poll, conducted for CNA prior
should consider the positive and negative impacts on people’s health. Participants were enthusiastic about the day, noting it provided
great opportunities to bring nursing solutions and perspectives to the attention of parliamentarians.
Health Minister Leona Aglukkaq and CNA president Barb Mildon discussed the federal government’s new regulations that grant more prescribing authority to nurse practitioners (NPs), midwives and podiatrists. CNA welcomed this as a milestone for NPs and their patients.
NEI
L VA
LOIS
17JANUARY 2013 VOLUME 109 NUMBER 1

An online team of diabetes experts will guide your patients through videos, articles and tools
Pharmacists to help with the ins and outs of blood glucose monitoring
Nurses to help navigate the healthcare system and better manage their diabetes
Nutritionists to explain how to eat with pleasure and still manage blood glucose
Kinesiologists to show how physical activity doesn’t have to mean spending hours at the gym
Psychologists to help with the emotional aspects of diabetes
Recommend STARsystem
Introducing
STARsystem
Free health coaching*
With STARsystem™ your patients will benefi t from free health coaching sessions that include 90 minutes of health coaching* by phone and 6 months of unlimited online support. The health coach will be there to provide the motivation your patients need while helping set personal goals and a plan of action to achieve them.
Finally, a personalized, step-by-step diabetes management system
* Health coaching will be provided by Health Interaction™, a Sanofi Canada program.
STARsystem™ and Health Interaction™ are trademarks of Sanofi .
iBGStar™ and BGStar™ are trademarks of Sanofi .
iPhone and iPod touch are trademarks of Apple Inc., registered in the U.S. and other countries.
Copyright © 2012 sanofi -aventis Canada Inc. All rights reserved.
Monitoring Management

The only bloodglucose meters
that give
access to STARsystem
Intelligent, accurate technology made simple.
Because it takes more than a meterto manage blood glucose
starsystem.sanofi.ca
The meter that seamlessly connects to the iPhone or iPod touch.
NEW!
CD
N.B
GM
.11.10
.04E
Nutrition Physical activity
Emotional well-being

n average, insulin pumps cost approximately $7,000, with ongoing annual costs of about $3,000. In 2006, the Ontario government announced that funding would be provided for insulin pumps and supplies for children in the province. Many families and patients who had not previously considered pump therapy for diabetes management were now in a position to consider this option, and there
was a surge of interest in switching from multiple daily injections to insulin pump therapy.
In our pediatric diabetes program, at the Diabetes Care Centre, Credit Valley Hospital site in Mississauga, Ont., we follow approximately 210 children and adolescents with type 1 diabetes. (The centre’s patients also include adults with type 1, type 2 and gestational diabetes.) Patients in the pediatric program have a clinic visit every three to four months, where they are seen by a diabetes nurse educator, a diabetes dietitian educator, a social worker and a pediatrician.
Prior to December 2006, children and adolescents were started on insulin
Group insulin pump starts in a pediatric diabetes program
PRO
MIS
ING
PR
ACT
ICES
Diabetes educators at the Credit Valley Hospital adapted their approach to accommodate increases in the numbers of patients and families interested in starting pump therapy
Diabetes nurse educator Monica Smith (centre) shows young
patients and their parents how to operate an insulin pump.
SA
ND
RA
TAVA
RES
20 CANADIAN-NURSE.COM

pumps during one-on-one training sessions with the nurse educator and the dietitian educator. Following the funding announcement, we needed to come up with a way to continue to provide timely access to pump therapy while accommodating the increased numbers of patients and families who require training and support to prepare for pump initiation. Facilitating insulin pump starts in a group setting and creating a more structured education program was the answer. A pilot initiative involving adult patients proved very
successful. By January 2007, we were ready to implement this idea for patients in the pediatric diabetes program.
Between the beginning of January 2007 and the end of 2011, 84 of our patients, ranging in age from three to 18, were started on insulin pumps. We scheduled monthly group pump starts, with a maximum of three patients and their families per class. As interest grew, we were able to accommodate two group pump starts per month. We also developed a plan for group lessons to help patients and their families maximize use of the pump and the bolus calculator features.
Patients are not booked for a pump start until they have had several appointments with the dietitian educator to learn to carbohydrate count and to establish insulin-to-carbohydrate ratios. Each patient is booked for a trial cannula insertion and is encouraged to wear a pump for several days with saline, rather than insulin, in the reservoir. For younger children, in particular, the saline trial is beneficial in reducing any anxiety they might have about inserting the cannula in a group setting on pump start day.
Age group and type of pump being used is considered when deciding what class is appropriate for a patient. The classes are three hours in duration and take place on two consecutive Monday mornings. Family members attend both sessions. Before the sessions,
The advantages of continuous
subcutaneous insulin
infusion include customized,
flexible basal and bolus
dosing, reduction in severe
hypoglycemia, reductions of the
risk of nocturnal hypoglycemia,
and, most importantly, the
consistent and precise delivery
of insulin that is required for
optimal glucose control and
reduced risk of the development
of complications of diabetes.
Source: Scheiner, G., Sobel, R.J., Smith, D. E., Pick, A., Kruger, D., King, J., & Green, K. (2009). Insulin pump therapy: Guidelines for successful outcomes.
Insulin pump therapy
participants are expected to have watched educational material on a CD, reviewed basic pump programming instructions, inserted the battery into the pump and set the date and time. In the first session, we go over the pump’s features and operating menus and how to insert a cannula and fill a reservoir with saline. Depending on the age of the patients, we ask them or family members to do a cannula change independently during the first week and instruct them on the use of the bolus wizard calculator for mealtime boluses. On the following Monday, everyone is feeling confident and ready to get started on the insulin pump. During this lesson, we also discuss strategies for preventing diabetic ketoacidosis (DKA) and hand out blood ketone testing meters. The symptoms and management of hypoglycemia are reviewed. Families receive an insulin pump therapy booklet, which we developed, outlining their responsibilities for successful pumping as well as the centre’s responsibilities in pump management. The booklet guides them through the formula for determining insulin doses for starting on the pump, sick day and DKA management, glucagon, hypoglycemia, exercise management and how to manage the pump when admitted to hospital.
At the end of the second session, all participants have an opportunity to share information and their own experiences of living with diabetes in
21JANUARY 2013 VOLUME 109 NUMBER 1

the family. Family members have been enthusiastic about the benefits of the group approach, which is viewed as both supportive and empowering.
The nurse educator follows up by phone with patients after the first class. We decided that it was important for each patient to also have an individual visit with the educators one month after pump start. Regular phone and e-mail contacts are made at timely intervals throughout the first few months. We also help families complete the documentation required to maintain eligibility to renew the annual grant for supplies. Most families report that pump therapy improves their children’s quality of life and that they plan to continue with pumps, rather than injections, for managing diabetes.
The nurse educator is responsible for collecting data related to glycemic control and diabetes management as part of our patients’ regular visits to
the clinic. These data, which include three-month blood sugar average (A1C), incidents of hypoglycemia and any emergency department visits, are routinely collected in pediatric diabetes centres as part of the ongoing assessment of patients’ diabetes management skills.
The data collected between 2007 and 2011 on 78 of the 84 patients started on pumps showed stable glycemic control with a range in average blood sugar control of 8.2-8.5 per cent. There were no incidents of severe hypoglycemia or hypoglycemia requiring glucagon administration and only 11 documented visits to the emergency department for DKA; most were related to site issues, which include dislodged or inadvertently
MONICA SMITH, RN, BScN, CDE, IS A DIABETES NURSE EDUCATOR AT THE CREDIT VALLEY HOSPITAL SITE, THE CREDIT VALLEY HOSPITAL AND TRILLIUM HEALTH CENTRE, MISSISSAUGA, ONT.
ANGELA ROODE, RN, BScN, CDE, IS A DIABETES NURSE CLINICIAN AT HALTON HEALTHCARE SERVICES, OAKVILLE SITE, OAKVILLE, ONT.
removed cannulas and infection at the site. These results are consistent with the evidence in the literature on the safety and efficacy of insulin pumps in reducing trips to the ED for hypoglycemia and DKA. Twelve patients discontinued use of the pump, which suggests that, overall, there is a high level of satisfaction with this type of therapy.
We believe that these positive outcomes may, in part, be a reflection of the support and structure of our education initiative. Furthermore, we suggest that when young patients experience less glucose variability, they are likely to have positive long-term outcomes related to possible delay or prevention of diabetes complications. ■
22 CANADIAN-NURSE.COM

Extend your Professional Reach
A Master of Science in Nursing should advance your career, not interrupt it. The MSN at Trinity Western University offers flexible, convenient graduate educa-tion for the working nurse. Complete a MSN at Trinity Western University without leaving your current position, and specialize in Nursing Education, Nursing Leadership, or Advanced Practice.
Visit us online at www.twu.ca/MSN to find out more.
Scholarships are available!
MASTER OF SCIENCE IN NURSING AT TWU
76 0 0 GLOV ER RD L A NGLE Y, BC V2Y 1Y1
6 0 4 513 2019gradadmiss ions@ t wu.ca
twu.ca/graduate
The Legal Nurse Consultants Association of Canada presents
their
4th Annual Conference
“ Legal Nurse Consulting — Conquering New Challenges ”
April 26 – 28, 2013 Century Plaza Hotel,
1015 Burrard St., Vancouver, BC
Member registration $125 before Feb 15, 2013;
$150 after. Non-members $175
Go to www.lncac.ca to register
23JANUARY 2013 VOLUME 109 NUMBER 1
Centre for Professional
Nursing Education
MacEwan.ca/PeriopRN
The operating room. Get the skills you need.
Perioperative Nursing at
MacEwan University will
get you there.
Take this post-diploma
certificate online
at your pace.

FEAT
UR
E
ick up any newspaper on any given day and it’s a good bet at least one article will feature an indicator — maybe flu vaccination rates or the most recent wait times for MRIs. If it’s particularly compelling, the stat may even make the headlines. But what do all these numbers really mean? And how do we know when to pay attention to them?
The Canadian Institute for Health Information defines a health indicator as “a single measure (usually expressed in quantitative terms) that captures a key dimension of health, such as how many people suffer from chronic disease or have had a heart attack. Indicators also capture various determinants of health, such as income, or key dimensions of the health care system, such as how often patients return to hospital for more care after they are treated.” Commonly reported health indicators include BMI, smoking prevalence, diabetes rates, incidence of hospital-acquired infections, percentage of births that are caesarean sections, and infant mortality rates, to name just a few.
The collection of health indicators has increased in recent years in the pursuit of accountability and
quality improvement. But an overabundance of measurements without a coordinated plan
can lead to indicator chaos
Making Sense
Indicatorsof
By SUE CAVANAUGH
“We are drowning in information and starved for knowledge.”
– John Naisbitt, American futurist
24

Indicators can provide information about people, such as their life expectancy, or about systems, such as pharmaceutical drug coverage rates. Indicators are extremely useful for capturing what is happening, but they do not explain why those things are happening. Without a back story or context, indicators have no real significance.
Indicator collection has increased in recent years to satisfy the demand for accountability and quality improvement in the health-care system. But along with all of this measurement comes a challenge — a challenge experts are calling indicator chaos. The term refers to both the overwhelming amount of data being collected and the lack of a coordinated plan across the health system on what numbers to collect and how to interpret and use them. Without a plan, there can be duplication of effort and a waste of already scarce resources. Even worse, money may be spent on developing programs and services that aren’t useful or appropriate because the data has been interpreted incorrectly.
“It’s an issue everyone should be thinking about and aware of,” says John Abbott, CEO of the Health Council of Canada. “We have all these data coming at us, in both our professional and our personal lives, and we have to try to make sense of them so we can make the right decisions, whether in the workplace or in our own family.” Abbott gives the example of childhood obesity indicators. While most in the health sector, he says, agree on how to measure childhood obesity, mere knowledge of the national child obesity rate doesn’t tell us much. “We need to look behind the indicators to see what the contributing factors are.” A closer look, says Abbott, is likely to reveal that children from poorer families, lower-income neighbourhoods and aboriginal communities have much higher levels of obesity than children from urban, middle-class neighbourhoods. “It’s important to put the numbers in context; otherwise we’re masking the real issues and challenges, and we end up spending a lot of resources pitching the wrong message to the wrong audience.”
But that doesn’t mean we shouldn’t be measuring those numbers. “The indicator can be used to draw people into the conversation,” says Abbott. “We can let everyone know we have a problem with childhood obesity and within what specific circumstances and context. Then, we can
In 2011, the provincial health quality councils, along with national agencies such as Accreditation Canada and the Canadian Patient Safety Institute, held a national summit on the topic of indicator chaos. According to the summit report, Think Big, Start Small, Act Now: Tackling Indicator Chaos, participants supported a vision for a pan-Canadian health measurement system that is structured, transparent and accessible, and they identified key steps for working toward it:
Start with the patient. A nationwide system for developing and disseminating health-care indicators should be shaped and guided by patients’ needs, priorities and potential bene ts.
Don’t talk. Act. Success in tackling indicator chaos demands quick action on two or three pilot projects to gure out how to set priorities, build frameworks for creating indicators and test the validity and usefulness of the indicators we develop.
Name leaders. Success depends on establishing a national consortium of dedicated stakeholders who will keep momentum from the summit going. Choosing the people to work together and providing a small and exible secretariat to support them needs to be done quickly.
Create a clearing house. Our collective failure to communicate is causing tremendous waste. Efforts are duplicated, good ideas aren’t shared, and work done nationally may never lter down to people and organizations that could use it.
Agree on priorities. Indicator chaos comes from a lack of common priorities and coordination and the impossibility of planning without them. Always ask: Who are we measuring for? Why are we measuring this?
Source: Think Big, Start Small, Act Now: Tackling Indicator Chaos,
Saskatchewan’s Health Quality Council, 2011. Used with permission.
National summit calls for action
25JANUARY 2013 VOLUME 109 NUMBER 1
target the appropriate communities and their support systems.”
Health-care organizations, and particularly their overloaded managers and staff who are tasked with collecting data, are on the front lines of indicator chaos. Some may lack the necessary expertise to properly analyze and interpret the information once it’s collected. One thing they all need to ensure is that they use the most appropriate indicators for
their circumstances; a program manager has to look at specific data sets that will help her accurately determine whether the outcomes for clients are positive or negative and whether any changes to the program are warranted.
If organizations can’t answer why they are measuring something, they should question whether they should be collecting the data at all. This opinion was echoed by attendees during a colloquium on indicators at CNA last spring for leaders from many national health-
“Understanding how to be a critical user of health indicators is a key part of health literacy.”
– Health Council of Canada, A Citizen’s Guide
to Health Indicators
Since 2005, the Ottawa Neighbourhood Study has used a combination of health, environmental and safety indicators to provide public health, city planners and residents themselves with valuable information about the overall health of their neighbourhoods. The ongoing collaborative project, led by Elizabeth Kristjansson of the school of psychology and the Institute of Population Health at the University of Ottawa, has spawned programs and services tailored to the needs of individual neighbourhoods. The city’s community health and resource centres have created a strategy called No Community Left Behind, which helps residents develop solutions to address the issues identi ed in the study. One community was able to use the indicators to get support to create new playgrounds, reduce gang activity, make its streets safer and rejuvenate its community association.
In 2012, the study received the prestigious CIHR Partnership Award.
The Ottawa Neighbourhood Study
26

care associations. There was agreement that the information indicators provide has to be relevant for all levels of the health system.
When indicators are developed from self-reported data, their reliability may be questionable. For example, the Canadian Index of Wellbeing, which tracks multiple quality-of-life indicators, found an interesting disconnect between self-rated health and clinical data collected by Statistics Canada in 2003. People from Newfoundland and Labrador had the lowest life expectancy and among the highest rates
In 1662, John Graunt published a booklet of indicators of the health and size of the population of London, U.K. Natural and Political Observations Mentioned in a Following Index, and Made upon the Bills of Mortality was the rst publication of its kind. Using the christening and burial records (bills of mortality) for each parish in London for the previous 70 years, Graunt produced a clear picture of the health issues of the population by tracking the causes of death. In his ndings, he argued for policies that would combine medicine and social responsibility with good government. One of his recommendations was that beggars should be taken care of with public funds.
Graunt was concerned about the reliability of the causes of death stated in the records, whether through the ignorance or the corruption of the recording clerks or the inspectors who determined the causes. For example, he was convinced that consumption was often recorded as cause of death to cover up for the far more shameful “infection of the Spermatick parts.” He also knew that the christening records did not accurately capture the number of births in a parish because Catholics and Puritans, in particular, were reluctant to have their children baptized into the Church of England.
Graunt also published a collection of the bills of mortality for 1665, the year of the Great Plague of London. Week by week, parish by parish, he tallied the rise of the plague, from its first real appearance in May (28 recorded cases) to June (340), July (4,400), August (13,000), September (32,300), October (13,300), November (4,100) and December (1,060).
For his work, Graunt was elected to the Royal Society of London — quite an achievement for a man who was a haberdasher by trade.
The father of modern indicators
27JANUARY 2013 VOLUME 109 NUMBER 1

of diabetes and obesity in the country, yet they were most likely of all Canadians to consider themselves to be in excellent or very good health. Residents of British Columbia, who had the longest life expectancy, lowest rate of obesity and average levels of diabetes, had given a much lower self-rating of their health.
In her job as a senior epidemiologist with Ottawa Public Health, Amira Ali analyzes and interprets data sets to ensure that public health programs and services are evidence informed and address local population health needs. She acknowledges that using self-reported measurements of health can be problematic. “For example, we know that self-reported BMI likely underestimates the true BMI. So we have to keep an error or inflation factor in mind and be conservative in how we use those types of data sets.” However, Ali believes there is a place for self-reporting: “If we didn’t allow for it, we would have next to no data on behavioural risk factors — because how else are we going to determine them?”
There’s no question that indicators can be manipulated for various purposes, political and otherwise; numbers are often thrown around to place blame for poor system performance or patient outcomes. Certainly, political parties have been known to interpret data selectively to
score points or to bolster their own platforms. For example, if data showed that 25 per cent of Canadians had difficulty accessing health care, one politician might say this means that most Canadians do not have difficulty with access; another, that one in four Canadians have problems accessing care.
Ali has some advice on how to make sense of indicators reported in the media. First, look to see whether a source is provided. If the source is not reputable or is missing, be suspicious of the accuracy of the data. Second, keep an eye out for words like astronomical, skyrocketing, of epidemic proportions — over-the-top descriptors like these should be interpreted with caution. Third, look for the context. If no context is provided, the data should be disregarded or, at least, investigated further. “We often have people calling our information line after they’ve read a story that quotes an alarming statistic,” says Ali. “We make sure the public health nurses operating the lines have access to the right information to explain how the article was misleading or what the number really means.” ■
SUE CAVANAUGH IS STAFF WRITER, CANADIAN NURSE.
28 CANADIAN-NURSE.COM
From rhetoric to action:
Achieving person and family-centered
health systems
Don’t delay, register today! | Ne tardez pas, inscrivez-vous dès aujoud’hui.
June 10 -11, 2013Niagara Falls, Ontario
Les 10 et 11 juin 2013Niagara Falls (Ontario)
Join health leaders from across Canada to explore and discuss how to take concrete steps to move person and family-centered health systems from rhetoric to reality.
Joignez-vous à des leaders en santé de toutes les régions du Canada afin d’explorer et discuter des mesures concrètes à prendre pour passer de la parole aux actes afin que les systèmes de santé centrés sur la personne et la famille deviennent réalité.
Nationally and internationally renowned speakers include: / Les conférenciers de renommée nationale et internationale comprennent : Margaret Trudeau, Brian Goldman, Shirlee Sharkey and /et Durhane Wong-Rieger.
NEW: NURSING LEADERSHIP STREAM
NOUVEAU : VOLET SUR LE LEADERSHIP DANS LA PROFESSION INFIRMIÈRE
www.nhlc-cnls.ca
De la rhétorique à l’action :
des systèmes de santé centrés sur
la personne et la famille
2013 National Health Leadership Conference
Conférence nationale sur le leadership en santé 2013

et me give you a hand with that.” A crew member was helping a passenger fasten his life-jacket and adjust his helicopter seatbelt. I was impressed with the keen observation skills and offer of assistance to a newbie like me, before the ocean voyage had even started.
On Aug.7, we had arrived in Kugluktuk, Nunavut, and were being shuttled by helicopter to the Canadian coast guard Ship Sir Wilfrid Laurier, anchored in the harbour nearby. The Laurier is a high-endurance multi-tasked icebreaker, 83 metres long with six decks, and the flagship of the Coast Guard’s Western fleet.
For the next six weeks, I would be a health officer aboard the Laurier, travelling through the Northwest Passage, far north of the Arctic Circle’s 66 degrees latitude. I was feeling apprehensive, in spite of going through a three-month screening process and completing a four-day orientation, conducted by the coast guard’s national health officer program coordinator.
I am comfortable working in unusual environments and working independently; I am an occupational health nurse with Health Canada and a former army nurse. My clients, who include coast guard crews in the Atlantic region, work in high-risk occupations. It was a crew member who
ON
TH
E JO
B
The Laurier is a high-endurance multi-tasked icebreaker, 83 metres long with six decks, and
the coast guard’s
Six weeks on an Arctic icebreaker
As a health of cer on the Canadian Coast Guard Ship Sir Wilfrid Laurier, Theresa McGuire provided primary care, counselling, health and safety promotion and emergency treatment for the ship’s crew and passengers
BR
IAN
CA
SE
29JANUARY 2013 VOLUME 109 NUMBER 1

passenger to conduct a confidential health survey and brief physical assessment. Cardiac, diabetic and neurological emergencies can occur suddenly and necessitate critical evacuations.
My sick bay hours were 8 a.m. to 4 p.m., seven days a week. At all other times, I was on standby to be “piped” for emergencies. I quickly got to know crew members and earned their trust as I started assessing and treating infections and minor injuries. It warmed my heart when someone would say, “We’re glad you’re here.” A small metal particle embedded in an eye proved to be one of the most serious of my challenges. The patient was in significant pain and distress. If not resolved quickly, an eye injury can mean medical evacuation. After numbing the eye, I used every gentle procedure at my disposal, along with calm hands and reassuring words, to help me remove the particle.
A few weeks into the voyage, archeological divers with Parks Canada joined the Laurier to search for the ill-fated Franklin expedition ships. I reviewed emergency medical
treatment procedures with them; the nearest hyperbaric chamber is many hours away, even by helicopter or charter plane. Fortunately for me, the divers were well trained and safety conscious.
The Arctic Ocean, as beautiful as it is at this time of year, can
be deathly cold and unpredictable. Having a well-prepared, self-sufficient team is critical, and the coast guard certainly practises what it preaches when it comes to marine safety and emergency response. Briefed by an experienced ship safety officer, all newcomers receive instruction regarding fire stations, lifeboats, abandon-ship drills and full immersion suits. Life-jackets are inspected and maintained regularly and are always worn when boarding and when travelling in Zodiacs and survey vessels. Steady in hand, foot and eye, the Laurier crew are respectful of the
suggested I “come aboard” on one of the Arctic voyages. I wanted to know more about the challenges of this work environment and knew that I had the required qualifications for a position as a health officer: a background in community health, advanced practice skills and experience in primary care nursing in remote areas.
Once we lost sight of land, I went through a hatch door to investigate my workplace. The sight of a brand-new Stryker stretcher, an automated external defibrillator, oxygen and Entonox therapy cylinders and an abundance of IV, suture, and dressing supplies was reassuring. I knew then that I could handle all but major surgery quite independently. A full burn-dressing kit, hypothermia kit, mass casualty triage kit, a basic supply of pharmaceuticals and access to an onboard helicopter and experienced pilot for medevac completed the picture.
The First Nations and Inuit Health Branch Clinical Practice Guidelines for Nurses in Primary Care was a trusted resource, and I could reach a medical consult service on the satellite
phone. All coast guard crew are certified in emergency first aid; three are designated as rescue specialists while on board and have advanced medical treatment training. We did additional training together to practise and enhance their skills.
After about a week, my sea legs kicked in and I began to feel comfortable in my new environment. Fortunately, the Laurier is a stable ship, and there were few cases of seasickness. I needed to be aware of existing medical conditions, and I met with each crew member and
stocked, the sick bay
three metres by three metres, with a large
BR
IAN
CA
SE
Today, the coast guard has a much expanded role in supporting
maintaining marine communication beacons and responding Laurier’s
passengers included scientists, hydrographers and media
30 CANADIAN-NURSE.COM

THERESA McGUIRE, RN, DOHN, COHN(C), CRSP, IS AN OCCUPATIONAL HEALTH NURSE WITH HEALTH CANADA, IN HALIFAX.
challenge of working on a moving platform. It was a relief to see everyone safely back on board each night, after long days spent surveying on open water, flying in the helicopter, climbing remote beacons and placing large buoys. Of course, we were always ready for search and rescue calls, which could range from other vessels in distress to downed aircraft.
There were no critical emergencies on my leg of the voyage. However, medical evacuations took place on other coast guard ships over the summer. There are usually six ships underway in the Arctic during this season (July through October), in various areas throughout the North.
The amazing level of cleanliness onboard rivalled that of any hospital I had worked in. We took additional sanitation measures when a rogue upper respiratory virus appeared early on in the voyage. Disinfectant wipe down of all common areas and increased handwashing soon stalled the spread. Later on in the voyage, and with my captive audience in mind, I put together information sessions on positive coping strategies for shift work, blood pressure and blood sugar monitoring, back safety and hearing protection.
Life on board was often fun, even when the seas and weather were rough. The weekly menus on the Laurier were varied and well balanced. Barbecues were held on the aft deck to mark the arrival of visitors, a rotation of captains and the end of our voyage. After hours, we took turns calling bingo, organizing card games and playing music. Our hydrographers and archeologists gave presentations on their fascinating work. CBC’s The National was documenting these research activities, and we gathered in the lounge to watch clips from the show on satellite TV. Basic e-mail service meant that I could keep in touch with family and friends. For me, the day’s best entertainment was the breathtaking sunset from high on the bridge. I never tired of watching the multitude of ways that waves can shimmer and reflect light.
On trips ashore, I met community health nurses in the Inuit communities of Cambridge Bay, Taloyoak and Gjoa Haven, to discuss the resources we had available to us. Making connections with nursing colleagues was essential — I might have needed local help, and any of them might have required disaster response assistance from me or the Laurier. When I met students at a high school in Cambridge Bay, I encouraged them to consider the Canadian coast guard and nursing as career options.
This assignment at sea was a time of reflection and learning and an opportunity to validate my values and knowledge. I would highly recommend the experience to any nurse seeking an out-of-the-ordinary challenge. ■
31JANUARY 2013 VOLUME 109 NUMBER 1
Université d’Ottawa | Faculté des sciences de la santé
L’École des sciences infirmières de la Faculté des sciences de la santé de l’Université d’Ottawa souligne la contribution des infirmières et infirmiers au mieux-être de la population.
Joignez-vous à l’équipe!
Programmes d’études de 2e et 3e cycles :Ph.D. (Sc.Inf.)
M.Sc. (Sc.Inf.) (Composantes majeures d’enseignement à distance)*
M.Sc. (Sc.Inf.) / Diplôme en soins de santé primaire pour infirmières et infirmiers praticiens (Composantes majeures d’enseignement à distance)*
M.Sc. (Sc.Inf.) / Spécialisation en études des femmes
Diplôme en soins de santé primaires pour infirmières et infirmiers praticiens
Renseignements :www.sante.uOttawa.ca
* À l’Université d’Ottawa, le Consortium national de formation en santé (CNFS) contribue à offrir un accès accru à des programmes d’études dans le domaine de la santé, aux francophones issus des collectivités en situation minoritaire.

Straight talk:
REFLECTION
he nursing profession is ailing, and RNs are in denial. We claim to be healthier than we really are. In some ways, we are not unlike those patients who tell us, “I feel fine,” when it’s evident that they aren’t fine at all.
Negative relationships and lack of adherence to our standards of practice and code of ethics are threatening our very survival as a profession. How have unprofessional behaviours (bullying and disrespecting colleagues) and confusion about professional identity managed to thrive? When did it become OK to have no nursing plan of care, to switch patients if we did not “like” the assignment, to disregard continuity of care and to fail to engage in therapeutic nurse-patient relationships (the cornerstone of professional practice)? When did we start accepting that leadership is missing in action?
For the past several years, I have spoken to thousands of nurses, in all areas of practice, at conferences, workshops and workplace consultations across this country. Their responses to my concerns have left me with a sense that there are many who agree we are in trouble and that it’s time to do something about it.
When was the last time you reflected on what nursing means to you? As I prepare to leave the profession I love, my own thoughts are increasingly turning to the ways in which the profession has changed over the years. And I am feeling a modicum of unease. Separation anxiety? Possibly, but I believe it is more than that.
From the day I first entered nursing, it has been a
As she approaches retirement, after 42 years as a registered nurse, Barb Fry nds that she is thinking more and more about the state of the profession — and its future. In upcoming issues, she will share her thoughts on scopes of practice, leadership and the art of nursing, in the hope of creating awareness and inspiring positive change
Why we need to do better
dominant influence in my life. But three fairly recent events put the experiences I’ve had over four decades of nursing into focus and launched me on a new professional quest.
The first event occurred after watching a movie last summer about Florence Nightingale. I wept tears of sadness, an acknowledgment of how far we’ve strayed from the ideals of the art of nursing.
Months later, I visited the Florence Nightingale museum in London. The modern structure and cheerful interior belie the dark and difficult history of nursing over the centuries. At one point, the quiet of the museum was shattered by the excited voices of elementary students arriving for a tour, a scavenger hunt, interactive learning and stories told by a “live” Florence, in period costume. I learned that this visit is a requirement of the school curriculum. And that interest triggered more questions: how is the nursing profession really perceived here at home? How much do Canadians truly know or care about what nursing practice can offer? How much do nurses value their profession and one another? Why do they struggle when trying to describe their scopes of practice?
The third event unfurled after my husband became seriously ill. Thankfully, he is thriving today because of the expert care he received during his hospitalization and followup treatment. His nurses (a different one assigned each day), although pleasant, seemed primarily focused on attending to tasks associated with his physical needs. There was little continuity of care and no time for the psychosocial and spiritual aspects of his care. Not one nurse was able to
32 CANADIAN-NURSE.COM

BARB FRY, BN, M.Ad.Ed., IS A PROFESSIONAL SPEAKER, BUSINESS OWNER AND AUTHOR.
find the time to talk to my husband or me about the devastating impact of this illness. There is something wrong with a system and a management that places such pressure on nurses to focus exclusively on tasks, when task-oriented care prevents nurses from fulfilling their full scope of practice.
While many of us typically blame our governments and cost-cutting measures for putting us in this situation, lack of professionalism in our professional relationships is an equal culprit. We have turned on one another and become
unsupportive. We have stopped dealing with one another in a professional manner. And so, the conditions are ripe for a profession breakdown, one from which we may not survive. Make no mistake: when RNs cannot, or choose not to, function to the full extent of their scopes of practice, they will be replaced.
I’ve given you lots of bad news, but there is good news, too! We have the ability, individually and collectively, to eliminate these threats. What’s
more, I have witnessed tremendous hope, a fervent desire for change and a “can do” attitude in nurses who want to create a better future for nursing practice. We already
possess the knowledge and tools to repair what is broken and to become the unstoppable force we are meant to be in our health system.
Am I issuing a professional wake-up call? Yes...if that’s how you want to see it. A few of you will be ready to jump up and get started. Some will politely acknowledge the call; others will roll over and go back to sleep. The remainder will howl, “She needs to retire!” It is up to you to decide if I am right and if so, to determine what actions you are willing to take to change things for the better.
Within our nursing culture, we are inclined to do things in the same way we always have. But I’m not buying that thinking. I feel ethically bound to do what I can to bring about positive change. Here’s my plan:
I will continue to speak, write and promote awareness about professionalism in practice.
I will initiate a call to action to enshrine standards of practice and the code of ethics in all we do.
I will advocate for the return of the therapeutic relationship.
I will remind nurses that those who focus exclusively on tasks are reduced to being technicians of care.
I will encourage nurses to believe in themselves and to step up and assume their rightful place in the health system. ■
Negative relationships and lack of adherence to our standards of practice and code of ethics are threatening our very survival as a profession
MIK
E D
EMB
ECK
PH
OTO
GR
AP
HY
Eliminating long-standing, harmful practices in the profession is no longer optional, Barb Fry says.
33JANUARY 2013 VOLUME 109 NUMBER 1

NU
RS
E TO
KN
OW
Lynda McLeod encourages nurses to practise self-care through art
ynda McLeod doesn’t mince words about the importance of art in her life.“Without it, I couldn’t be involved in nursing,” says the 54-year-old
educator and artist. “I couldn’t take the pain and the sadness and the discord you encounter as a nurse without having a place to leave it all behind at the end of the day.”
McLeod points to research showing that simply being exposed to art can provide a host of benefits for patients — among them are lower levels of
in abundance Creative expression
By DAVID McDONALD
TEC
KLE
S P
HO
TOG
RA
PH
Y IN
C.
anxiety, a reduced need for pain m e d i c a t i o n a n d i m p ro v e d postoperative recovery times.
“And in actually doing art,” she says, “the same kind of healing happens. You’re in a sweet spot… a happy, joyful place.”
McLeod was born into a creative family in Orillia, Ont. Her father pa inte d ; her mother was an accomplished craftsperson.
A self-described “predominantly right-brained” person, McLeod struggled in high school. “I’m a 100 per cent visual learner,” she says. “The only course I really did well in was biology, because I could draw it.”
She loved art but didn’t display exceptional talent and was dissuaded from pursuing it as a career. Instead, after graduation, she found work at the Huronia Regional Centre in Orillia, helping to care for kids with Down syndrome and other developmental disabilities. The head nurse, struck by the young woman’s compassionate way with children, suggested she might have the makings of a good nurse.
After earning her diploma in 1979, McLeod landed a job in the ICU at a Toronto hospital.
“It was intense,” she says of the working environment in which she and her fellow newbies found themselves. “We didn’t know what to do with our feelings about what had happened on a typical day. We’d go out for a drink and try to talk about it and unwind. But I couldn’t get rid of the images.” Mental snapshots of patients in pain and distress haunted her sleep.
Instinctively, McLeod sought out a pottery class. Her instructor told her there was literature to support the notion that creative expression can help people process troubling events. Sure enough, McLeod’s nightmares subsided. It was her first direct experience with the therapeutic powers of art.
For the Art by Nurses founder, it isn’t about how good someone is at art; it’s about bringing nurses together to make art and have a conversation about what’s happening in the profession.
34 CANADIAN-NURSE.COM

What is one word you would use to describe yourself? Imaginative
If you could change one thing about yourself, what would it be?My impatience
What are you most proud of having accomplished?Being a mother. I am so proud of my two daughters; they have become spirited, creative, independent freethinkers who are grounded in social justice
“If I had more free time, I would….” Draw more, read more and paint every day
Where did you go on your last vacation?I kayaked in Newfoundland. It is a hauntingly beautiful region
What is the one place in the world you’d most like to visit?I want to visit some of the pristine places that are left in our world. Bhutan is rst on my list
What is your biggest regret?I should have travelled right after nursing school
If there was a single person who inspired you to become a nurse, who was it?My mum. She was my biggest fan. She saw something in me that I didn’t
What was the best piece of career advice you’ve received?In my rst job, a feisty head nurse encouraged me to move around and get different experiences under my belt
What do you like least about being a nurse?The slow pace of change philosophically within our profession. We could be so powerful if we joined hands in de ning to the public what nursing is
10 QUESTIONS
with Lynda McLeodMcLeod continued her career in ICU. But, by
the late 1980s, she was ready for a change. Again, her artistic side came to the rescue. Up against a more experienced colleague for a nurse educator position in a hemodialysis unit, McLeod demonstrated how she’d use her own drawings as a teaching tool. She believes that’s what earned her the job.
In 1997, the McLeods — Lynda, her husband and their two young daughters — moved to Victoria, where Peter had landed a position as director of outdoor education at a boarding school. Lynda joined Camosun College’s nursing faculty. It’s a job she loved from the start. “When I close the classroom door, I know something exciting is going to happen.”
McLeod is equally enthusiastic about the family’s West Coast lifestyle. Their home is located a few blocks from Juan de Fuca Strait. “We’ve never looked back. We can actually ski and kayak on the same day, and maybe do a little fishing.”
Although McLeod had dabbled in watercolours over the years, it was a series of wilderness adventures in her adoptive province that pushed her art to a whole new level. Somewhere around this time, she also became a proponent of art’s salutary effects. What really motivated her to spread the word, she says, were the results of the 2005 National Survey of the Work and Health of Nurses, detailing what she refers to as the “terrible” state of nurses’ health in this country. “I didn’t want to become a statistic,” she says. “So I started thinking of ways to use self-care to help build healthier work environments. And using art seemed so natural.”
In 2007, McLeod launched Art by Nurses, a website to foster artistic expression and reflection among her professional colleagues — and promote their ideas and endeavours. Four years later, she mounted a group show by nurse artists, at Victoria’s Royal Jubilee Hospital. Healing Hallways was slated to run a month or two. A year later, it’s still there, providing a respite for patients and staff from the exigencies of hospital life. Her dream, she says, is to have similar shows in hospitals across the country. “If I can get funding,” she says, “I’ll put them in every province.”
In day-to-day discussions McLeod has with undergrads, she hammers home the importance of self-care and talks up the role art can play.
“I weave it into every class I teach,” she says. In recent years, McLeod has taken her message beyond the
classroom. Operating out of her home studio, she has begun a second career as a co-active coach, guiding clients in identifying and developing their creativity. These aspiring artists and writers want to get in touch with their inner Emily Carr or Alice Munro. Currently, she is working with seven nurses, a number she hopes will grow over time.
“I try to walk my talk,” McLeod says. “I truly believe in self-care as the way to stay in nursing and remain engaged and healthy.” ■
DAVID McDONALD IS AN OTTAWA WRITER AND FILMMAKER.
35JANUARY 2013 VOLUME 109 NUMBER 1

Have you ever thought about becoming a Registered Nurse for Princess Cruises? You would travel the world on board one of our 17 luxury cruise ships whilst working within a team of maritime medicine experts, treating patients in our accredited medical centres.
We are looking for highly skilled registered nurses with Emergency or Urgent Care experience with the commitment to deliver the highest standards of patient care. Additional openings for Japanese speaking nurses and temporary or permanent contracts of two to four months are also available. Take your nursing career in a new and exciting direction. Visit www.pmcmarine.com or email [email protected]
A S A C R U I S E S H I P R E G I S T E R E D N U R S E
CANADIAN-NURSE.COM36

Sign up for NurseNewsline and receive:
1. Go to www.CanadianHealthcareNetwork.ca
2. Hit the Register Now! Button
3. Complete the brief online registration
4. Validate your registration via the activation email
5. Start enjoying NurseNewsline!
NurseNewsline is available @
Registration is FREE and EASY TO DO
Check out
the latest nurse news by joining
NurseNewsline
INTERESTED IN SHARING YOUR PASSION FOR NURSING?
The Bachelor of Science in Nursing (BScN) program at MacEwan University, Edmonton, Alberta, emphasizes development of a strong knowledge base, acquisition of diverse nursing practice skills and demonstration of professional attributes.
We invite applications for full-time continuing or sessional faculty positions.
To view the available appointments and required qualifications, please refer to www.MacEwan.ca/careers
For general inquiries please contact:Sharon Bookhalter, DeanFaculty of Health and Community [email protected]
Faculty Positions Available with the MacEwan University BScN Program
37JANUARY 2013 VOLUME 109 NUMBER 1

38 CANADIAN-NURSE.COM
TENURE-TRACK NURSING FACULTY POSITIONS:
UNIVERS ITY OF BR IT ISH COLUMBIA OKANAGAN
The University of British Columbia’s Okanagan campus in Kelowna, B.C. seeks four tenure-track academic researchers at the assistant, associate, or full professor levels to join our School of Nursing (http://www.ubc.ca/okanagan/nursing/welcome.html). Review of applications is underway. We offer undergraduate and masters’ programs in nursing and an interdisciplinary PhD program; UBC is consistently ranked among the world’s top 40 universities.
Applicants require a relevant PhD and eligibility for registration with the College of Registered Nurses of British Columbia; postdoctoral research training is preferred. Teaching potential in undergraduate and graduate medical-surgical nursing, public health, mental health, gerontology, statistics, and/or leadership are desirable. Research foci in knowledge translation, aboriginal health, rural health, global health, mental health, or other Tri-Council funding areas are advantageous. For more information on how to apply, please see http://www.ubc.ca/okanagan/hr/careers/faculty/tenuretrack.html#hsd
To find out more and to apply,
visit: jobs.vch.caPhone: 604.675.2500Toll-Free in North America: 1.800.565.1727
Come for the job.Stay for the team.
Incredible Lifestyle
Outstanding Career Move
Attractive Relocation Assistance
Photo: VCH ICU Richmond Hospital Employees.
Tertiary
Resident Care Continence Nurse Clinicians
Immediate opportunities in the following areas: Advanced Practice positions:
www.alzheimer.ca
Let’s start seeing people with dementia
for who they are.
Test your attitude towards dementia at
www.alzheimer.ca/ letstalkaboutdementia

39JANUARY 2013 VOLUME 109 NUMBER 1
CLA
SSIF
IED
SCLASSIFIEDSEVENTS AND COURSES LEGAL NURSE CONSULTING TRAINING — CALGARY, APRIL 2013 OR ONLINE ANYTIME!Use your nursing knowledge in a new way.
Developed specifically for Canadian Nurses and our
medical-legal environment. LNC training benefits all
nurses in all areas of practice. Presented by CanLNC,
Canada’s most experienced and successful LNC firm.
Go to www.CanLNC.ca for more information.
FOOT CARE NURSE PROGRAMLearn nursing foot care with a mentor in your
own community, complete workbook (Lazenby)
assignments from your home and do your final
clinical at a community college. Also online
continuing education programs available such
as a Foot Care Nurse Educator Program, monthly
Webinars and a Private Practice Program. Our Foot
Care Nurse Educators are also willing to travel to
your local college! www.footcarekingston.com
MISCELLANEOUS
LIVE THE LIFE OF YOUR DREAMSWould you like freedom to live the life of your
dreams while helping others succeed?
Call 1-877-260-6636 for free information on a part-
time home-based business in the wellness industry
with unlimited income potential.
CANADA IT’S A GREAT TIME TO BE A NURSE!* It’s about Choices!
* It’s about Freedom!
* It’s about Money!
Canada’s leaders in relief staffing for healthcare
professionals are seeking experienced ER and
Outpost nurses. Urgent needs for OR Transplant
Nurses. Some of the highest rates of pay in Canada,
fabulous assignment locations, flexible scheduling,
exceptional clinical support and paid travel and
housing. Where is your career taking you next?
www.travelnurse.ca or call 1-866-355-8355
TRAVEL NURSING IN CANADASelect Medical Connections offers travel nursing
assignments across Western Canada. Since 1999
we have delivered:
TOP PAY — up to $10,000 monthly
FLEXIBILITY — work on your own terms
ADVENTURE — explore Canada
NEW EXPERIENCES, hospitals and friends
FREE housing and travel
JOBS in Canada, USA and Australia
Visit www.topnursejobs.com or call 877-525-3870
to launch your adventure today!
Bayer .......................................... OBC
Bio-Oil ............................................ 13
Covidien ........................................... 9
Government of Nunavut .................. 36
Grant MacEwan University ......... 23, 37
Legal Nurse Consultants Association of Canada ..................... 23
National Health Leadership Conference ..................................... 28
National Nursing Week .................... 39
Princess Cruises ............................. 36
.......................... 18, 19
Trinity Western University ................ 23
University of British Columbia ......... 38
University of Calgary ...................... IBC
University of Calgary-Qatar ............. IFC
Université d’Ottawa ........................ 31
Vancouver Coastal Health ................ 38
EXPLORING PROFESSIONAL ISSUES SINCE 1905
INDEX OF ADVERTISERS
Publication does not constitute CNA endorsement of, or an assumption of liability for, any claims made in advertisements.
We’re looking for stories of nurse-led innovation
in primary care. If you have a story to share, e-mail us!

RODNEY LOEPPKY IS AN ASSOCIATE PROFESSOR OF AMERICAN POLITICS AND THE POLITICS OF HEALTH AT YORK UNIVERSITY IN TORONTO. HIS WORK INCLUDES STUDIES OF THE HUMAN GENOME PROJECT AND HEALTH-CARE SYSTEMS IN CANADA, THE U.S. AND GERMANY.
The U.S. has just come through the longest and most exhausting election cycle in its history, with campaigns stretching back almost two years! The decisive victory for the Obama administration has been interpreted also as a ringing endorsement of health-care reform in America. Although it seems unlikely now that Republicans in Congress will continue to wage all-out war against the Affordable Care Act (ACA), a number of the 30 Republican state governors are likely to drag their feet on — or even issue challenges to — implementing the act in 2014. Nonetheless, advocates of health reform see a
clear path forward. The ACA (often referred
to as Obamacare) has several objectives: it will prohibit both the denial of coverage based on pre-existing conditions and the nasty practice of rescission (revoking coverage in the wake of catastrophic medical needs). It will provide coverage to some 32 million additional Americans by way of
expanded Medicaid and the individual mandate (which makes insurance coverage a legal responsibility). And it will encourage affordable premiums with health exchanges (online portals through which consumers can compare basic insurance packages) while also offering subsidies for those who cannot afford what the industry offers. There is much more to say about the ACA, but from our vantage point north of the border, what might be its unintended consequences for Canadians?
On one level, there are practical considerations
for provinces and territories in which a shortage of care providers remains a serious concern. Extending health-care coverage to millions of Americans will require, quite simply, more care providers. Numerous regions of the U.S. are already underserviced, and there can be no doubt about where recruiters will come looking. This dynamic is not new, and policy-makers and professional associations will have to pay close attention as 2014 approaches.
There will be other pressures, not the least of which may involve a stronger push for systemic change. It’s worth noting that the ACA is not a step toward either a single-payer or a universal system — rather, it simply mandates access for more Americans to the patchwork of private care options in the existing system. Along the way, several new “experimental” forms of private care will be proposed, and these will undoubtedly serve as justification for advocates here who want to challenge principles of universality in the Canada Health Act. Despite the fact that an endless river of evidence points to higher care costs — much higher costs — in privatized systems, those intent on experimentation will point out that expanded forms of private care in the U.S. are evidence that such programs can work here in Canada. But we need to be clear: health-care costs for Americans (on a per capita basis) are twice what they are for Canadians, and, thanks to lobbying efforts by the insurance and pharmaceutical industries, the ACA contains no mechanisms to rein in those costs. That’s the bottom line. Restructuring the Canadian system to provide better access and care is a noble goal, but anyone who thinks privatized care is the answer, à la Obamacare, is taking Canadian patients and care providers alike down a dangerous path. ■
THE
LAS
T W
OR
D
Some will view expanded forms of private care in the U.S. as evidence that they can work here
U.S. health-care reform
What will
mean for Canada?
40 CANADIAN-NURSE.COM

Research Chair/Professor
The University of Calgary is a leading Canadian university located in the nation’s most enterprising city. The university has a clear strategic direction—Eyes High—to
become one of Canada’s top five research universities by 2016, grounded in innovative learning and teaching and fully integrated with the community of Calgary.
Named a cultural capital of Canada and one of the best places to live in the world, Calgary enjoys more days of sunshine than any other major Canadian city and is less
than an hour’s drive from the majestic Rocky Mountains.
The Faculty of Nursing at the University of Calgary is launching an exciting initiative to support research development by offering 2 research chairs and 4 research
professorships beginning July 1, 2013. All positions are tenured/tenure-track continuing appointments with significant research support for establishment of research
teams and initiatives upon recruitment to Calgary. These research leaders will join an exciting faculty team poised for impact on health care across the country, and
will position the University of Calgary for prominence as a research university.
Candidates for research chairs will be nationally or internationally acclaimed mid- to senior career nursing scholars, preferably at the rank of full professor.
Applicants will have demonstrated success in implementation of an outstanding program of research, a compelling profile of research publication and dissemination,
demonstrated leadership in their field of research, and a significant track record of graduate student supervision. Funding support for research chairs will complement
other competitive external funds garnered in support of their research programs in the following areas:
1. Chair in Knowledge Translation
2. Chair in Simulation Education
Candidates for research professorships will normally be at an early phase of their research career (to be appointed at assistant or associate professoriate rank).
They will already have established an emerging research program and will demonstrate an excellent beginning research funding and publication record, potential
to become leaders in their field, and beginning experience in graduate student supervision. Funds provided in support of the professorship will complement other
competitive external funds in support of establishment of research programs in the following areas:
1. Professorship in Cancer Care
2. Professorship in Gerontological Nursing
3. Professorship in Health Technology
4. Professorship in Teaching and Learning
Please refer to the website at www.ucalgary.ca for position profiles and additional information on these positions.
Applications will be accepted until January 15, 2013 or until positions are filled.
Please provide a cover letter, a curriculum vitae, a summary of the research program, and 3 examples of relevant publications or knowledge translation materials.
Inquiries and materials can be directed to:
Dr. Dianne Tapp
Dean and Professor
Faculty of Nursing
University of Calgary
2500 University Drive NW
Calgary, AB T2N 1N4
The University of Calgary respects, appreciates and encourages diversity.
F A C U L T Y O F N U R S I N G
ucalgary.ca

=+
bayerdiabetes.ca
Bayer’s CONTOUR® NEXT EZ meter usesonly Bayer’s CONTOUR® NEXT test strips
© 2012 Bayer Inc. ®/TMCONTOUR®, CONTOUR® NEXT, CONTOUR® NEXT EZ and No CodingTM & Design are trademarks of Bayer HealthCare LLC,
used under license by Bayer Inc. Bayer and Bayer Cross are registered trademarks of Bayer AG, used under license by Bayer Inc. DD2534-0712E
Easy and accurate:A powerful combination
Easy-to-use features and next-generation accuracy for confidence in patient test results
Bayer’s CONTOUR® NEXT EZ andBayer’s CONTOUR® NEXT Test StripsNEW
Related Documents











