Situating Disability and Diversity: A Spatial Science Strategy Presenter Hamish Robertson Faculty of Medicine University of NSW

Situating Disability and Diversity PacRim Presentation 2014
Aug 14, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Situating Disability and Diversity: A Spatial Science Strategy
PresenterHamish Robertson
Faculty of MedicineUniversity of NSW

Contents
• Introduction• Convergence issues at a global level• Ageing, disability and diversity in context• Spatial science as a key contributor• Building a model• Discussion• Conclusion

Introduction
• Doctoral candidate on the geography of Alzheimer's disease
• Experience in multicultural/diversity health, patient safety, health/medical geography, ageing research and disability
• Focus on spatial science applications in support and critique of responses to above issues
• Exploration of value and utility of geographies of health and medicine to emerging issues
• This is a large topic and only intended as a partial overview

Global Convergence of Ageing Disability and Diversity
• Ageing, disability and diversity are converging now and into the future - locally, nationally and globally -> spatial differentiation and inequalities
• Rising aged population = rise in people with disabling conditions (physical, psychological and neurological -> cognitive problems) – variable patterns
• Diversity of ageing means disability paradigm will continue to expand e.g. neurological conditions – identitification versus medicalisation
• Understanding the complexities of age and ageing are still very developmental – and still mainly women who survive longest
• Social diversity (difference) problematic and problematised since inception e.g. the uniform ethnic state, racism and eugenics – social categories as problems
• PWD construct not necessarily the basis for self-identification in older people whose conditions are often slow and progressive
• Politics of ageing and aged care funding will converge with disability as governments, NGO’s, families and individuals attempt to cope
• E.g. Diana Coole, 2012 on neoliberal discourse and new social risks (NSRs) and Monique Lanoix on dependency aversion in bioethics

Persistent Vulnerabilities in AustraliaSource: Travaglia, 2009
• The elderly• People of Aboriginal and Torres Strait Islander background• Immigrants - especially non-English speaking background• People with disabilities, especially cognitive impairments• Children and youth• Patients with literacy and communication problems• People from lower SES• Geographically isolated individuals• Socially isolated individuals• The homeless• The frail and malnourished• Patients with co-morbidities and chronic illness• Patients with high acuity• Patients with liminal status (social, physical, geographic)• Patients without an advocate in the system
Travaglia (2009)

Disability Rate by Age in Australia 2009 and 2012

0–4 5–14 15–24 25–34 35–44 45–54 55–59 60–64 65–69 70–74 75–79 80–84 85–89 90 and over
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
Age and Total Disability (%)
0–4 5–14 15–24 25–34 35–44 45–54 55–59 60–64 65–69 70–74 75–79 80–84 85–89 90 and over
0.0
20.0
40.0
60.0
80.0
100.0
120.0
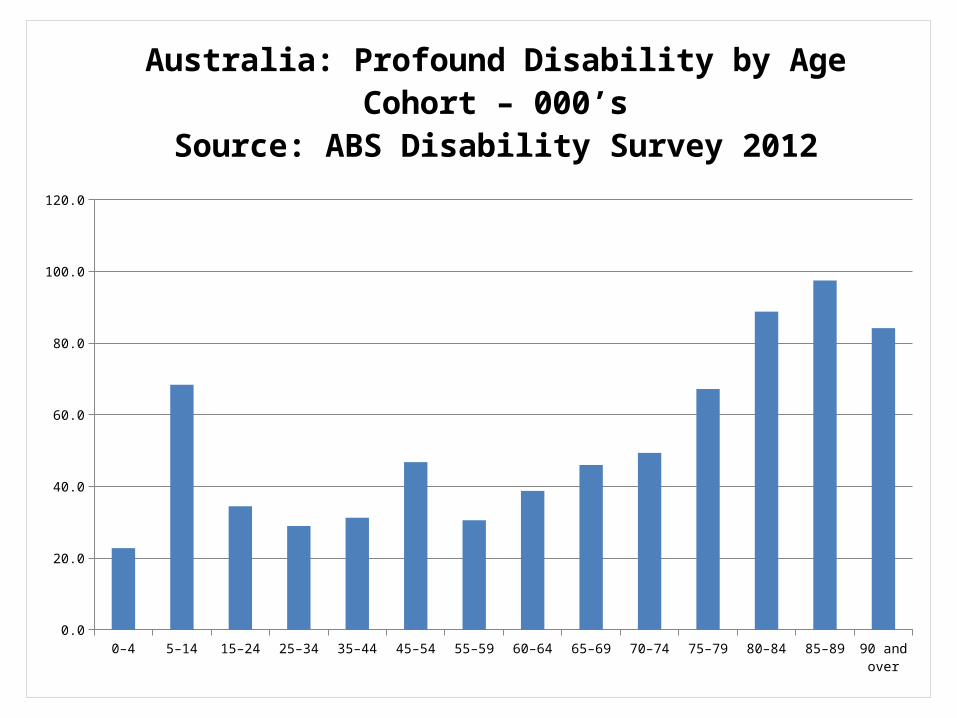
Australia: Profound Disability by Age Cohort – 000’sSource: ABS Disability Survey 2012

0–4 5–14 15–24 25–34 35–44 45–54 55–59 60–64 65–69 70–74 75–79 80–84 85–89 90 and over
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
Profound Disability Status by Age and Sex
MaleFemale

ACT Northern TerritoryWestern Australia NSW Queensland South Australia Victoria Tasmania0.0
10.0
20.0
30.0
40.0
50.0
60.0
Total Disability by State/Territory (%)
0-6465+

Spatial Science in a Rapidly Changing Disability Environment
• Dynamics of the disability sector (inc. advocacy) require an increasingly sophisticated evidence base – competition, rationing, corporatisation
• Adaptation to an ageing world means conceptual and epistemic dynamism – not the past re-packaged and re-presented
• Spatial science a rapidly expanding and highly interdisciplinary field of practice and theory
• This has value for disability/diversity/ageing paradigms and their convergence
• Space and place are central to positions taken and utility/value of responses

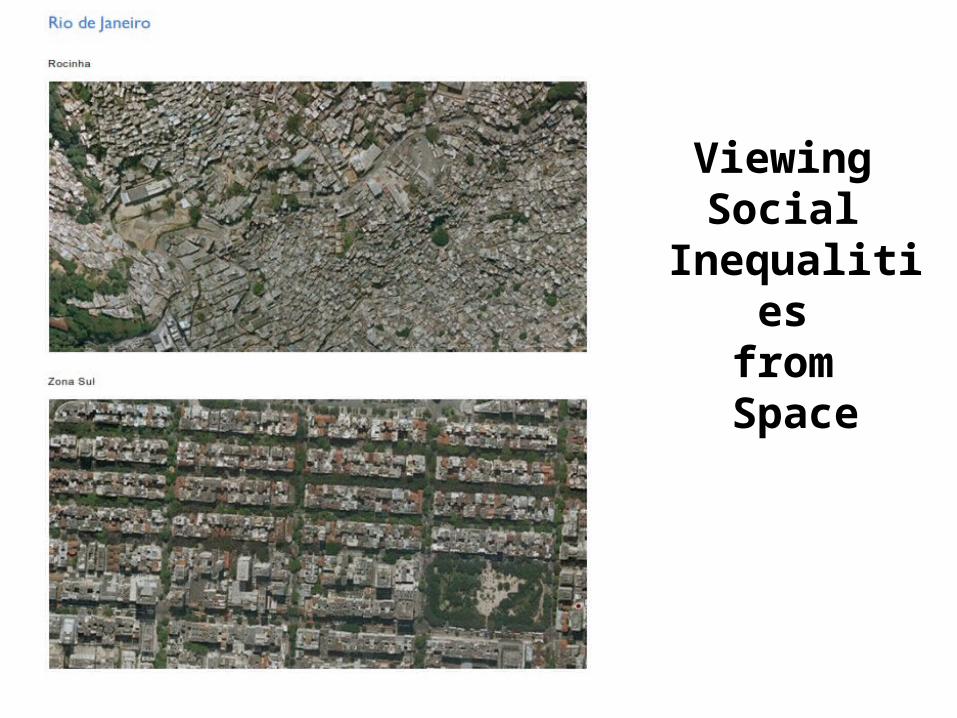
Viewing Social
Inequalities from Space
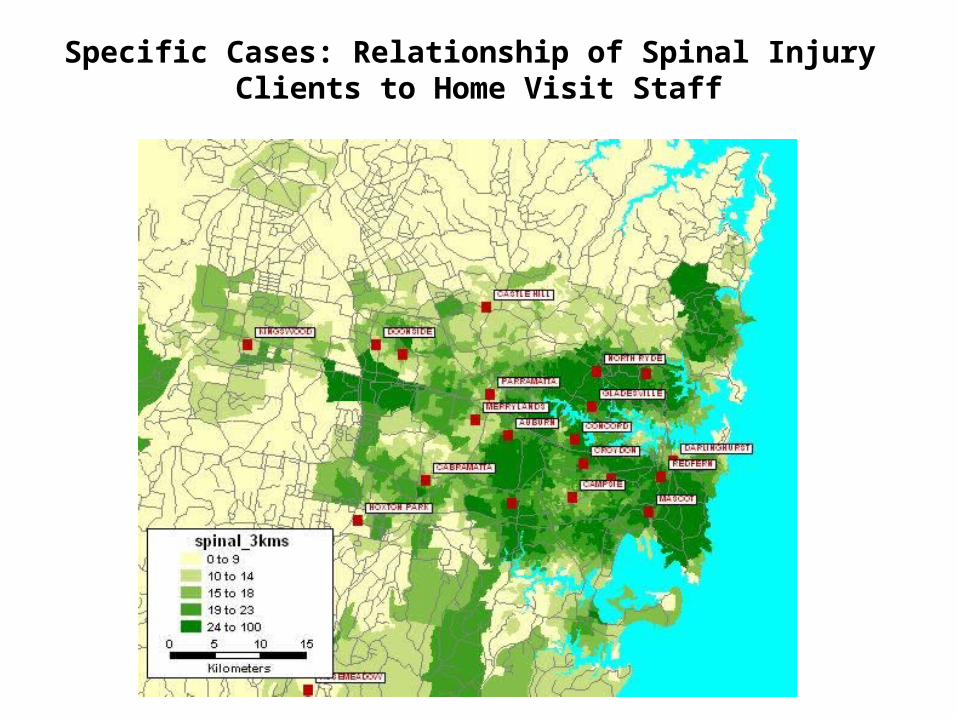
Specific Cases: Relationship of Spinal Injury Clients to Home Visit Staff

Building a Model
• Demographic variables – age cohorts, country of birth, languages spoken, disability status
• Expanding the model of disability – physical, psychological, behavioural, movement, cognitive, pain etc (age-adjusted disability)
• Mapping the data analysis• Visualising the outputs• Making the evidence accessible

Discussion• Ageing, diversity and disability are place-specific
constructs and experiences• Non-teleological definitions and processes needed i.e.
not referenced to an ideal/idealised state or group or entity
• Population ageing is adding to the complexity of disability and diversity constructs
• Spatial science and technology can represent these complexities in visual formats (2D, 3D, 4D etc) – soon 3D printing will add tangible
• Disability is conceptually, temporally and spatially contingent

Conclusion
• Ageing, disability and diversity all have key contextual characteristics – place matters
• Convergence of these phenomena will increase diversity of experiences and outcomes
• Responses by governments appear increasingly problematic – blame, rationing, category games etc
• Spatial science and can support individual and collective capacity to respond and inform your evidence base – lobbying, negotiation etc
• Visualisation and a capacity to share approaches are central to spatial science strategies
• Disability is a multi-dimensional experience, a spatially informed approach supports disability in a complex and changing world
Related Documents











