SINUS OF VALSALVA ANEURYSM Moderator- Dr.RV KUMAR Presenter- Dr.Jyotindra Singh

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

SINUS OF VALSALVA ANEURYSM
Moderator- Dr.RV KUMARPresenter- Dr.Jyotindra Singh

INTRODUCTIONThin walled, saccular or tubular outpouchings, usually always in the right sinus or adjacent half of the noncoronary sinus.
Generally have an - Intracardiac course
May protrude into the pericardial space and they may rupture into the right (or rarely left) heart chambers to form --- Aorta-cardiac fistula.
5 times higher in Asian countries.
Male preponderence – 4:1
0.15-1.5% surgeries correspond to SVA repair

HISTORICAL ASPECT 1839 -1st description by Hope
1840- 1st important paper published by Thurman
1949- Jones and Langley -the subject of congenital and acquired lesion .
1951- 1st diagnosis of rupture during life by Venning
1956- 1st. successful repair with CPB at Mayo Clinic using CPB.
1957-Morrow & colleagues –closed ruptured SOVA using mild hypothermia
SAKAKIBARA & KONNO
- Studied association with VSD & AR
- First to provide comprehensive classification

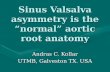
AORTIC ROOT- ANATOMY
Young adults
AA>STJ
AdultsAA = STJ
ElderlyAA<STJ

.
The 2 trigones underneath the commissures of the noncoronary leaflet are fibrous structures, whereas the other underneath the commissure between the right and the left leaflets is mostly a muscular structure.
ROOT ANATOMY

Anatomic and Echocardiographic Relationship Between the Components of the Normal Aortic Root
Systole
Diastole
120 degree - LAX
ST junctionAnnulus
Tubular aortaSinuses

SINUS OF VALSALVAring.

SINUS OF VALSALVA
3 sinuses named after- Antonio Valsalva.
Provide space behind the open aortic leaflets so that the leaflets do not occlude the coronary artery orifices.
Secondly, this space favours the development of eddy currents behind the leaflets when they are open.
Magnetic resonance imaging has shown- in aiding leaflet opening through the creation of a low-pressure system by means of the Venturi effect.
In valve sparing aortic valve surgery, maintenance or recreation of the sinuses has been beneficial in terms of normal leaflet movement and valve durability

MORPHOLOGY1 Separation of the aortic media of the
sinus from the media adjacent to the hinge line of the AV valve
cusp .
Results from the absence of normal aortic elastic tissue and media in two region.
2 Congenitally weak area gradually gives way under aortic pressure to
form an aneurysm.
3 The aneurysm appears an excavation of the sinus which protrudes into the underlying cardiac chamber.


CONGENITAL ACQUIRED
Connective tissue disorders-
Rheumatoid arthritis,
Ehlers-Danhlos syndrome,
Marfan’s syndrome,
Klippel Feil syndrome,
Turner’s syndrome,
Trisomies 13 and 15,
Loeys-Dietz syndrome,
Arachnodactyly,
Osteogenesis imperfecta.
Infectious diseases –
bacterial endocarditis,
syphilis, and tuberculosis;
Degenerative conditions
atherosclerosis
cystic medial necrosis;
Injury from deceleration trauma.
Iatrogenic pseudoaneurysms hematoma formation after AVR
removal of aortic valve calcifcations

ACQUIRED


Type I: the aneurysm originates in the left portion of the right sinus, protrudes forward and ruptures into the right ventricle near the pulmonary valve.
The concurrent presence of VSD under the pulmonary valve is frequent.
Type II: the aneurysm originates in the mid portion of the right sinus, protrudes and ruptures in the right ventricle. A concurrent VSD is uncommon.
Type III: the aneurysm originates in the mid portion of the right coronary leaflet and protrudes towards the tricuspid valve. It often ruptures into the right atrium and sometimes into the right ventricle, just below the septal leaflet of the tricuspid valve. VSD is rarely encountered.
Type IV: the aneurysm originates in the right portion of the non-coronary leaflet and ruptures into the right atrium. A combined VSD is uncommon.

Congenital Heart Surgery Database Committee of the Society of Thoracic Surgeons


RSOVA-VariantsLeftward portion of sinus
WINDSOCK projecting into the adjacent RVOT just below the pulmonary valve.
Arising CENTRALLY
project in the outlet portion of the
RV aspect of the ventricular septum
RIGHTWARD
Entering RV beneath the parietal band in the region of Membranous septum

Non coronary sinus- VARIANTSNon coronary sinus
originate from –ANTERIOR PORTION
---- Project into RIGHT ATRIUM
---- Rarely into RV or RA+ RV, muscular ventricular septum.
POSTERIOR PORTION
RUPTURE INTO PERICARDIUM

Associated cardiac anomalies - VSD
Prevalence – 30 to 50 %
Incidence higher in Rt.sinus
Left third of right aortic sinus- JUXTA – ARTERIAL
RIGHT THIRD – conoventricular /peri membranous
Centrally – Juxta aortic / outlet portion of the septum.
Hinge line of aortic leaflet separates aneurysm from VSD
Supracristal VSD & RSOVA
Incomplete fusion of the truncal swellings at the time of the division of the common truncus from the bulbar septum during the 5th week of embryogenesis

VSD - CLASSIFICATION
Type-I - VSD is present immediately below the commissure of the left & right semilunar cusp of pulmonary valve .Aneurysm ruptures into the RVOT forming aortico –right ventricular fistula.
Type-II- VSD rests on the crista supraventricularis,not in contact with the tricuspid or pulmomary valves.
Type-III- VSD lies just below crista supraventricularis and the corresponding sinus of valsalva.
Type –IV – VSD rests on the paramembranacea

OTHER ANOMALIESAortic regurgitation results from prolapsed aortic cusp
Bicuspid aortic valve leading to AR.
Pulmonary stenosis
Aortic coarctation
PDA
ASD
Subaortic stenosis
TOF

ANEURYSM RUPTURERuptured aneurysms originate most frequently from the right coronary sinus (65–85%),
Less frequently from the noncoronary sinus (10–30%), and
Rarely from the left coronary sinus ( 5%)
The right ventricle is the most common receiving chamber (about 80–90%), due to rupture of either right or noncoronary SVA

RUPTURE RIGHT CORONARY SINUS
Develop localized “ WINDSOCK ”
Rupture into adjacent low pressure chamber
INTRA CARDIAC FISTULOUS PORTION
NIPPLE LIKE projection into cardiac chamber with one or more points of rupture at its apex
Non coronary sinus origin - have no WINDSOCK deformity , direct fistulous communication between aortic sinus & heart
Left sinus origin – Extra cardiac aneurysm

ANEURYSM RUPTURE
occur.
SITES OF RUPTURE ASIANS Non- Asians
RIGHT ATRIUM 13 35
RIGHT VENTRICLE 84 57
RV + RA <1 <1
LEFT ATRIUM <1 <1
LEFT VENTRICLE <1 2
RA+ LA+ LV <1 <1
VENTRICULAR SEPTUM <1 <1
PULMONARY TRUNK <1 <1
RV + Pulmonary trunk <1 <1
PERICARDIUM <1 2

Presentation
SOVA clinically presents based on
Depending on the size of the aneurysm,
the rapidity with which it ruptures,
the cardiac chamber with which it communicates
RUPTURED SOVA
20% no symptoms develop.
45%- gradual onset of effort dyspnea
35% - acute symptoms
sudden breathlessness & pain
Pain- precordial/ epigastric
Sudden death
precipitated by – heavy exertion/ IE / Marfan syndrome.

UNRUPTURED ANEURYSM - Tricuspid valve dysfunction
- RVOT obstruction
- Severe MI – by compressing
right or left coronary artery.
- Conduction abnormalities
- Embolization from unruptured aneurysm.
ST-elevation in leads V1–V3

Rupture into the Right ventricle-
the severe diastolic ventricular volume-overload causes
Obliteration of the y-descent
Rupture into the right atrium
obliterates the x-descent.
The high Right atrial pressure-
Early tricuspid opening
Premature v-wave,
High peaked a-wave
with a fourth heart sound.
JVP in Ruptured aneurysm

Sudden appearance of a continuous murmur in an otherwise healthy individual.
Heard at a maximum at the lower sternal border or xiphoid.
Diastolic accentuation of this murmur is an important sign to differentiate ruptured sinus from PDA or arteriovenous fistula.
Systolic suppression of the murmur is caused by both mechanical narrowing of the fistulous tract during systole as well as the probable
Venturi effect created by the rapid ejection of blood past the aortic origin of the fistula
Ruptured aneurysm

Tamponade
Myocardial ischemia,
Conduction disturbances and/or arrhythmias.
Rupture into the pericardial space, a very rare complication (2% of noncoronary SVA ruptures), almost invariably leads to fatal cardiac tamponade
Rupture causes compression of the ostium of the left main coronary artery, resulting in myocardial ischemia and arrhythmic death
SUDDEN CARDIAC DEATH

ECG
ECG showing sinus tachycardia with 1st degree AV block and right bundle branch block.
Ventricular tachycardias arising from the aortic sinus of Valsalva: An under-recognized variant of left outflow tract ventricular tachycardia
Compression of the His bundle occurs when the ruptured SVA penetrates the base of the interventricular septum and results in atriovenricular conduction defects and arrhythmias


X RAYIt is uncommon to find the aneurysm abnormality on x ray as they are intracardiac.
However, the evidence of aortic atherosclerosis is a clue to the etiology as evidenced in this patient.
Rarely these aneurysms can cause heart border abnormalities depending upon the cusp involved.
Marked cardiomegaly can be visualized if aortic root dilation and aortic insufficiency are present

IMAGING GUIDELINES


35


AORTOGRAM
occur.
Right-sided pressures were elevated with a right atrial pressure of 12 mmHg,
Pulmonary artery pressure of 47/31 mmHg with a mean of 37 mmHg, a pulmonary wedge pressure of 20 mmHg and a left ventricular end-diastolic pressure is 24 mmHg.
There was a significant 14% rise in oxygen saturation between the right atrial and vena caval oxygen saturations.
A single injection was done at the aortic root which demonstrated a communication between the origin of the right sinus of Valsalva into the right atrium (RA), with eventual opacification of the right atrium, right ventricle (RV) and pulmonary arteries. -


CT vs CMRThe advantages of performing MR imaging in the setting of a known or suspected Valsalva sinus aneurysm include the
-evaluate the LV hemodynamic pattern,
- identify aortic regurgitation and quantify aorto-cardiac shunt or fistulous blood flow.
CT is less time consuming and the preferred investigation compared to MRI in case of acute setting of aneurysmal rupture
Conventional angiography is the
gold standard and can be used for both diagnostic and therapeutic purposes.

Indications for Surgery

Indications for surgeryEnlargement beyond 5.5 cm,
Progression of greater >1.0 cm/year.
Aortic regurgitation from distraction of the commissural posts with ventricular enlargement
Unruptured aneurysms encroaching on nearby structures, causing myocardial ischemia, or having the potential to rupture warrant repair.
Family history of aortic dissection or rupture.
Asymptomatic patients – Serial follow- up . If high likelihood of progressive increase in size and the possibility of rupture or endocarditis.

Approach is by a median sternotomy using cardiopulmonary bypass.
The arterial cannula is placed distally in the ascending aorta.
Bicaval venous cannulation using right angle cannulas should be used.
A moderate degree hypothermia,e.g. 28°C, is appropriate.
CARDIOPLEGIA- Retrograde
STEPS OF SURGERY

A transverse aortotomy is performed, and the root anatomy assessed.
An oblique right atriotomy is performed next, allowing for identification of both ends of the aneurysm or of the fistulous tract in case of rupture .
In case of protrusion or rupture into the right ventricle, exposure can be obtained through a right atriotomy or a limited ventriculotomy .
When the fistulous tract or diverticulum is in the right ventricular infundibulum, the lesion can also be exposed through a transverse pulmonary arteriotomy.
STEPS OF SURGERY

The defect must be repaired through the aortic root, using a patch of autologous or bovine pericardium to exclude the aortic inlet into the aneurysm.
Primary closure predisposes to a higher risk of recurrence (as high as 20%) or aortic valve regurgitation from deformation of the root. - CONDEMNED
The ventricular or atrial aspect of the fistula can be closed primarily,
a patch should be used to incorporate closure of a coexisting ventricular septal defect
Great care should be taken in avoiding the atrioventricular conduction system at the time of VSD closure.
Single/Double patch repair


Aneurysm is in Right ward position of Right sinus - Perimembranous VSD
RIGHT ATRIAL APPROACH with detachment of antr & septal leaflet of TV
Leftward portion of the Right sinus-
Vsd is juxta arterial - approach is through the RV or pulmonary trunk.
Combined Approach- Aortic & RV pulmonary trunk or right atrial approach.
RSOVA + VSD

RSOVA + VSD
Thinned out windsock containing one or more perforation – resected creating a large defect in Rt. sinus of valsalva.
Defect separated from VSD by hinge line of right aortic cusp.

Origin- usually non coronary sinus but occasionally from right coronary sinus.
Approach- Aorta alone or right atrium.
Clamp placed across windsock.
A coexisting VSD is always sought.
Windsock is excised –based on hinge line of valve cusp.
Windsock is narrow & bordering edges are of good quality- direct closure
RSOVA to RA ,No VSD

Approach through ascending aorta.
CPB- through single canula in RA.
Venting catheter in LA
Cardioplegia
Aorta – opened transversely
Site of origin of aneurysm defined.
Orifice closed with pericardial / dacron patch
Unruptured sinus of valsalva aneurysm


SOVA- RESULTS

Most patients survive the early post op period.
Hospital mortality – max. 5% reported.
Severe AR with marked LV enlargement is a risk factor for premature death in late postop period.
Direct closure – 20 to 30 % prevalence for reoperation for reoperation for recurrence of the fistula.
Heart block occurs in 2 % to 3% of patients.
Complications

DEVICE CLOSURE

DEVICE CLOSURE

Related Documents