Shwachman–Diamond syndrome is associated with low-turnover osteoporosis Sanna Toiviainen-Salo a , Mervi K. Mäyränpää b , Peter R. Durie c , Nicole Richards d , Marc Grynpas e , Lynda Ellis c , Shiro Ikegawa f , William G. Cole g , Johanna Rommens d , Eino Marttinen a , Erkki Savilahti h , Outi Mäkitie h,i, ⁎ a Helsinki Medical Imaging Center, Helsinki University Hospital, Helsinki, Finland b Department of Surgery, Hospital for Children and Adolescents, Helsinki University Hospital, Helsinki, Finland c Division of Gastroenterology and Nutrition, Hospital for Sick Children, University of Toronto, Toronto, Ontario, Canada d Programmes in Genetics and Genomic Biology, and Integrative Biology, Research Institute, University of Toronto, Toronto, Ontario, Canada e Department of Pathology and Laboratory Medicine, Mount Sinai Hospital, Toronto, Ontario, Canada f Laboratory for Bone and Joint Diseases, SNP Research Center, RIKEN, Tokyo, Japan g Division of Orthopaedic Surgery, Hospital for Sick Children, University of Toronto, Toronto, Ontario, Canada h Department of Pediatrics, Hospital for Children and Adolescents, Helsinki University Hospital, Helsinki, Finland i Folkhälsan Institute of Genetics, Helsinki, Finland Received 2 May 2007; revised 27 July 2007; accepted 21 August 2007 Available online 5 September 2007 Abstract Introduction: Shwachman–Diamond syndrome (SDS) is an autosomal recessive disorder characterized by exocrine pancreatic insufficiency and bone marrow dysfunction. These result in malabsorption and hematological abnormalities. A skeletal dysplasia is also an integral feature of SDS. The present study assessed prevalence and determinants of osteopenia and osteoporosis in patients with SDS and disease-causing mutations in the SBDS gene. Materials and methods: Eleven patients (8 males) aged from 5 to 37 years (median 16.7 years) with a genetically confirmed diagnosis of SDS were assessed for fracture history, bone mineral content (BMC), lean tissue mass (LTM) and bone mineral density (BMD) (Hologic Discovery A), osteoporotic vertebral changes, and for blood biochemistry and hematological parameters. Iliac crest bone biopsies were obtained from four patients for histology and histomorphometry. Results: The main findings were: (1) markedly reduced BMD Z-scores at the lumbar spine (median − 2.1, range − 4.4 to − 0.8), proximal femur (median − 1.3, range − 2.2 to − 0.7) and, whole body (median − 1.0, range − 2.8 to +0.6), and reduced Z-scores for height-adjusted BMC/LTM ratio (median − 0.9, range − 3.6 to + 1.1); (2) vertebral compression fractures in three patients; and (3) blood biochemistry suggestive of mild vitamin D and vitamin K deficiency. Bone biopsies in four patients showed significant low-turnover osteoporosis with reduced trabecular bone volume, low numbers of osteoclasts and osteoblasts, and reduced amount of osteoid. Conclusions: The results suggest that in addition to the skeletal dysplasia, SDS is associated with a more generalized bone disease characterized by low bone mass, low bone turnover and by vertebral fragility fractures. Osteoporosis may result from a primary defect in bone metabolism, and could be related to the bone marrow dysfunction and neutropenia. © 2007 Elsevier Inc. All rights reserved. Keywords: Shwachman–Diamond syndrome; SBDS; Osteoporosis; Neutropenia; Malabsorption Bone 41 (2007) 965 – 972 www.elsevier.com/locate/bone Abbreviations: SDS, Shwachman–Diamond syndrome; SBDS, Shwachman–Bodian–Diamond Syndrome gene; BMD, bone mineral density; BMC, bone mineral content; LTM, lean tissue mass; DXA, dual-energy X-ray absorptiometry; 25-OHD, 25-hydroxyvitamin-D; PTH, parathyroid hormone; CF, cystic fibrosis. ⁎ Corresponding author. Hospital for Children and Adolescents, Metabolic Bone Clinic, Helsinki University Hospital, P.O. Box 281, FIN-00029 Helsinki, Finland. Fax: +358 9 71 75299. E-mail address: [email protected] (O. Mäkitie). 8756-3282/$ - see front matter © 2007 Elsevier Inc. All rights reserved. doi:10.1016/j.bone.2007.08.035

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

965–972www.elsevier.com/locate/bone
Bone 41 (2007)
Shwachman–Diamond syndrome is associatedwith low-turnover osteoporosis
Sanna Toiviainen-Salo a, Mervi K. Mäyränpää b, Peter R. Durie c, Nicole Richards d,Marc Grynpas e, Lynda Ellis c, Shiro Ikegawa f, William G. Cole g, Johanna Rommens d,
Eino Marttinen a, Erkki Savilahti h, Outi Mäkitie h,i,⁎
a Helsinki Medical Imaging Center, Helsinki University Hospital, Helsinki, Finlandb Department of Surgery, Hospital for Children and Adolescents, Helsinki University Hospital, Helsinki, Finland
c Division of Gastroenterology and Nutrition, Hospital for Sick Children, University of Toronto, Toronto, Ontario, Canadad Programmes in Genetics and Genomic Biology, and Integrative Biology, Research Institute, University of Toronto, Toronto, Ontario, Canada
e Department of Pathology and Laboratory Medicine, Mount Sinai Hospital, Toronto, Ontario, Canadaf Laboratory for Bone and Joint Diseases, SNP Research Center, RIKEN, Tokyo, Japan
g Division of Orthopaedic Surgery, Hospital for Sick Children, University of Toronto, Toronto, Ontario, Canadah Department of Pediatrics, Hospital for Children and Adolescents, Helsinki University Hospital, Helsinki, Finland
i Folkhälsan Institute of Genetics, Helsinki, Finland
Received 2 May 2007; revised 27 July 2007; accepted 21 August 2007Available online 5 September 2007
Abstract
Introduction: Shwachman–Diamond syndrome (SDS) is an autosomal recessive disorder characterized by exocrine pancreatic insufficiency andbone marrow dysfunction. These result in malabsorption and hematological abnormalities. A skeletal dysplasia is also an integral feature of SDS.The present study assessed prevalence and determinants of osteopenia and osteoporosis in patients with SDS and disease-causing mutations in theSBDS gene.Materials and methods: Eleven patients (8 males) aged from 5 to 37 years (median 16.7 years) with a genetically confirmed diagnosis of SDSwere assessed for fracture history, bone mineral content (BMC), lean tissue mass (LTM) and bone mineral density (BMD) (Hologic Discovery A),osteoporotic vertebral changes, and for blood biochemistry and hematological parameters. Iliac crest bone biopsies were obtained from fourpatients for histology and histomorphometry.Results: The main findings were: (1) markedly reduced BMD Z-scores at the lumbar spine (median −2.1, range −4.4 to −0.8), proximal femur(median −1.3, range −2.2 to −0.7) and, whole body (median −1.0, range −2.8 to +0.6), and reduced Z-scores for height-adjusted BMC/LTMratio (median −0.9, range −3.6 to +1.1); (2) vertebral compression fractures in three patients; and (3) blood biochemistry suggestive of mildvitamin D and vitamin K deficiency. Bone biopsies in four patients showed significant low-turnover osteoporosis with reduced trabecular bonevolume, low numbers of osteoclasts and osteoblasts, and reduced amount of osteoid.Conclusions: The results suggest that in addition to the skeletal dysplasia, SDS is associated with a more generalized bone disease characterizedby low bone mass, low bone turnover and by vertebral fragility fractures. Osteoporosis may result from a primary defect in bone metabolism, andcould be related to the bone marrow dysfunction and neutropenia.© 2007 Elsevier Inc. All rights reserved.
Keywords: Shwachman–Diamond syndrome; SBDS; Osteoporosis; Neutropenia; Malabsorption
Abbreviations: SDS, Shwachman–Diamond syndrome; SBDS, Shwachman–Bodian–Diamond Syndrome gene; BMD, bone mineral density; BMC, bone mineralcontent; LTM, lean tissue mass; DXA, dual-energy X-ray absorptiometry; 25-OHD, 25-hydroxyvitamin-D; PTH, parathyroid hormone; CF, cystic fibrosis.⁎ Corresponding author. Hospital for Children and Adolescents, Metabolic Bone Clinic, Helsinki University Hospital, P.O. Box 281, FIN-00029 Helsinki, Finland.
Fax: +358 9 71 75299.E-mail address: [email protected] (O. Mäkitie).
8756-3282/$ - see front matter © 2007 Elsevier Inc. All rights reserved.doi:10.1016/j.bone.2007.08.035

966 S. Toiviainen-Salo et al. / Bone 41 (2007) 965–972
Introduction
Shwachman–Diamond syndrome [1,2] (MIM# 260400) is arare autosomal recessive disorder in which the symptoms arisingfrom pancreatic insufficiency and bone marrow dysfunctiondominate. The pancreatic dysfunction presents as impairedenzyme output and malabsorption of fat-soluble nutrients [3–5];imaging studies show a fatty pancreas [6,7]. Bone marrowdysfunction is characterized by persistent or intermittentneutropenia, anemia or thrombocytopenia, and in bone marrowstudies by hypocellular marrow, aplastic anemia, myelodyspla-sia and leukemia [8,9]. The SBDS gene that is associated withSDS has been recently identified [10] and several disease-causing mutations have been described [11–13]. Recent data[14–17] suggest that the SBDS protein is associated with RNAmetabolism and ribosomal function, but the specific role ofSBDS remains to be elucidated.
The association of a skeletal dysplasia with SDS has beenreported in several studies [6,18–23]. According to a recentstudy [24], all patients with SDS and SBDS mutations havefindings consistent with skeletal dysplasia but the localizationand severity of these features vary with age, and even in patientswith identical genotypes.
In addition to skeletal dysplasia, generalized osteopenia andeven spinal compression fractures at an early age have beendescribed in occasional case reports in children and adults withSDS [7,19,24–27]. Patients with SDS have several risk factorsfor osteoporosis. These include malabsorption and compro-mised nutrition due to pancreatic insufficiency, vitamin D andvitamin K deficiency, delayed puberty and infections. How-ever, no previous studies have assessed the overall bone healthin patients with SDS. In order to gain knowledge on the pre-valence, etiology and characteristics of osteopenia andosteoporosis in SDS, we assessed 11 patients with SDS forseveral parameters of skeletal health. The results suggest thatin addition to the previously characterized epiphyseal andmetaphyseal skeletal changes, SDS is often associated withsymptomatic osteoporosis.
Materials and methods
Patients
Study subjects were ascertained through the pediatric units of all fiveuniversity hospitals in Finland. The inclusion criteria for this study were(i) exocrine pancreatic dysfunction associated with fatty pancreas in imagingstudies, (ii) hematologic abnormalities, characterized by persistent or intermit-tent neutropenia, (iii) age N4 years, and (iv) verified mutations in the SBDSgene. All 11 patients meeting these criteria consented to participate. The studyprotocol was approved by the Research Ethics Board, Helsinki UniversityHospital and a written informed consent was obtained from each patient and/orguardian.
Clinical data
Data on the patients' previous medical history were collected from hospitalrecords. A detailed history on present health, nutrition status, stature, growth andlevel of physical exercise, puberty, gastrointestinal and skeletal symptoms,history of fractures and medications, including vitamin substitutions, wasobtained by patient interview and from hospital records. All the patients were
clinically assessed for phenotypic features by a pediatric endocrinologist (OM).Height was measured with a Harpenden stadiometer (Holtain Limited, UK) andweight with an electric scale; values were compared with Finnish growth charts[28]. Height standard deviation score (height Z-score) was defined as deviationof height, in SD units, from mean height for age and sex [29].Weights wereexpressed as body mass index (BMI), derived from [weight (in kg)/by height2
(in m2)]. Pubertal maturation was assessed according to Tanner [30]. Thepresence or absence of pancreatic insufficiency was classified on the basis ofserum trypsinogen concentration [25,31]; patients with values b6 μg/L wereclassified as having pancreatic insufficiency (PI) and patients with intermediate(6 to 16.6 μg/L) or normal (N16.6 μg/L) values were classified as havingpancreatic sufficiency (PS). The pancreatic phenotype was confirmed with themeasurement of serum isoamylase level [4].
Bone mineral density and radiographic assessment
Areal bone mineral density (aBMD) for the lumbar spine (L1–L4), proximalfemur and whole body were measured with dual-energy X-ray absorptiometry(DXA, Hologic Discovery A®, Bedford, USA). The aBMDs were transformedinto Z-scores by using age- and sex-specific reference data for the equipment. Inaddition, T-scores were calculated for adult patients by comparing the aBMDresults with sex-specific reference data for the equipment. The Z-score is thenumber of standard deviations a given BMDmeasurement differs from the meanfor age-, sex- and race-matched reference population. .The T-score is the numberof standard deviations a given BMDmeasurement differs from the mean for sex-matched normal young adult reference population. Body composition, includingbone mineral content (BMC), fat mass and lean tissue mass (LTM), was obtainedwith the same DXA scanner. Height-adjusted Z-scores for BMC/LTM werecalculated using previously published reference data for children and youngadults [32].
Standard anterior–posterior and lateral neutral radiographs of the thoracicand lumbar spine were taken in supine position. All thoracic and lumbar radio-graphs were reviewed by two radiologists. Changes in vertebral morphologywere graded by inspection of digitized images (AGFA ImPacs System®) andclassified according to the grading methods of Genant [33] for adults and ofMäkitie [34] for children to identify vertebral morphological changes suggestiveof osteoporosis. Compression of 20% or more in the anterior, middle or posteriorvertebral height was considered significant.
Bone biopsy
A transiliac bone biopsy was obtained from four patients with a bone biopsyneedle of 7.5 mm inner diameter (Rochester Bone Biopsy, Medical InnovationsIncorporation Inc., USA) following a double-labeling course with oraltetracycline, with a 10-day interval period. The biopsy was performed 4 daysafter the end of tetracycline administration. Bone histomorphometry analyseswere conducted at the Bone and Cartilage Research Unit, University of Kuopio,Kuopio, Finland. All parameters were analyzed using a semiautomatic imageanalyzer (Bioquant Osteo, Bioquant Image Analysis Corporation, Nashville,TN, USA) and the results compared with normative data [35–37]. Allnomenclature, abbreviations, and standard formulas follow the recommenda-tions of the American Society for Bone and Mineral Research.
Mutation analysis
The SBDS coding regions were screened for mutations by restrictionenzyme digestion of amplified exon 2 or by direct sequencing of PCR-amplifiedproducts of genomic DNA as previously described [10].
Biochemistry
Peripheral blood counts were obtained to assess hematological dysfunction.Anemia was defined as a hemoglobin concentration below the normal age and sex-specific reference range [38], neutropenia as a neutrophil count b1500×106 cells/L, and thrombocytopenia as a platelet count of b150×109 cells/L. Serumconcentration of cationic trypsinogen (S-Tryp, reference range 16.6–42.6 μg/L)was determined by a double-antibody radioimmunoassay [39]. Serum pancreatic

967S. Toiviainen-Salo et al. / Bone 41 (2007) 965–972
isoamylase activity (S-AmylP, reference range 13–53 U/L) was determined withthe use of a commercial test kit (Randox Laboratories, Co Antrim, UnitedKingdom), which utilizes ethylidene-p-nitrophenyl maltoheptaoxide as substratewith two monoclonal antibodies to synergistically inhibit salivary amylase. Afterhydrolysis by amylase, the reaction end-product p-nitrophenyl is detected by itsabsorbance at 450 nm (Cobas Mira Analyzer, Roche, Switzerland). Fecal pan-creatic elastase (reference range N200 μg/L) was quantified by ELISA (PancreaticElastase ELISA, Bioserv Analytics andMedical Devices Ltd. Rostock, Germany).
Serum concentrations of 25-OH-vitamin D (S-25-OHD), vitamin A (usingretinol, Sigma R-7632, UK as standard) and vitamin E (using alpha-tocopherol,Sigma T-3634, UK, as standard) were determined by HPLC followed by UVdetection (HP 1100 Liquid Chromatograph for 25(OH)D and HP1090 LiquidChromatograph for vitamins A and E). S-25-OHD values below 38 nmol/L wereregarded consistent with hypovitaminosis D. The reference range for vitamin Awas 1–3 μmol/L and for vitamin E 12–40 μmol/L. Prothrombin time (P-PT) wasmeasured by Owrens prothrombin complex assay method (Nycotest PT, AXIS-SHIELD PoC AS, Oslo, Norway) and the coagulation activity was expressed aspercentage of normal value (reference range N70%). Plasma concentrations ofcreatinine (P-Crea, reference range 50–90 μmol/L), calcium (P-Ca, referencerange 2.15–2.51 mmol/L), phosphate (P-Pi), and alkaline phosphatase (P-ALP)were determined by standard assays. The reference range for S-Pi was age-dependent and for P-ALP age- and sex-dependent. The reference values of theyoungest and the oldest patients ranged for S-Pi from 1.2–1.8 mmol/L to 0.8–1.4 mmol/L, respectively, and for P-ALP from 250–1000 U/L to 60–275 U/L,respectively.
Plasma parathyroid hormone (P-PTH) was measured by solid-phaseenzyme-labelled chemiluminescent immunometric assay (IMMULITE 2000,DPD, Diagnostic Products Corporation, Los Angeles, CA), the reference rangewas 8–73 ng/L. Serum concentrations of follicle-stimulating hormone (FSH),luteinizing hormone (LH) and estradiol in adult females and testosterone in adultmales were measured by standard assays.
Statistical analysis
Simple regression analysis, Student's t-test and Chi square test were used, asappropriate, for statistical analysis (Statview® 5.0.1 for Macintosh, © 1992–1998 SAS Institute Inc.). A P-value of less than 0.05 was considered statisticallysignificant.
Results
Clinical characteristics
Eleven patients (8 males) aged 5.2–37.1 years (median16.7 years) from 10 families, all of Finnish ancestry, were
Table 1Clinical characteristics, vertebral and peripheral fractures and DXA findings in the 1
Patient # Gender,age (years)
Height(SD)
BMI(kg/m2)
Enzyme substitutionduration (years)
Vitamin Dsubstitution(IU/day)
Perfrac
#1 M 5.2 −2.7 14.4 4.5a 1200 0#2 M 6.0 −2.3 16.1 0 – 0#3 F 6.7 −0.7 14.9 4.5a Occasional 0#4 F 10.9 −2.5 13.4 6a 1200 0#5 M 14.6 −1.5 27.7 0 – 0#6 M 16.7 −3.1 17.7 16a 800 0#7 M 24.5 −2.8 22.4 19 200–400 2#8 M 25.9 −2.0 22.7 25a 800 1#9 F 31.1 −1.0 20.9 30a 600 0#10 M 32.4 −0.9 24.9 28 – 1#11 M 37.1 −2.3 25.2 10 – 1
Patients marked with a were on pancreatic enzyme substitution at the time of the sF, proximal femur; WB, whole body; LTM, lean tissue mass; BMC, bone mineral c
included in the study. They were diagnosed with SDS at amedian age of 1.5 years (range 4 months to 14.5 years). Allpatients had neutropenia and malabsorption due to exocrinepancreatic insufficiency at the time of diagnosis, and nine hadbeen on pancreatic enzyme supplements. Two non-supplemen-ted patients were diagnosed with SDS during the course of thestudy. Patient #2 was diagnosed at the age of 6 years after hisolder brother (#6), who was previously diagnosed with SDS,participated in the study. Patient #5 was referred to theMetabolicBone Clinic at the age of 14 years by an orthopedic surgeonbecause of lower limb deformities and metaphyseal changes. Allthe patients reported compliance with the prescribed medicaltreatment including enzyme supplements and vitamins. At thetime of the study, six patients were on enzyme supplements andthree had discontinued the medication 2, 3 and 26 years prior tothe study assessment. Eight patients had been supplementedwith vitamin D, six patients with vitamin E and vitamin A andtwo patients with calcium. At the time of the study, six patientswere on vitamin D supplements (median dose 800 IU/day), fivepatients on vitamin A and four patients on vitamin E supple-ments. None of the patients had been supplemented with vitaminK. Based on dietary interview, all the patients had sufficientintake of calcium (diet and supplements included). None of thepatients had received G-CSF treatment for neutropenia.
One patient (#7) had a known diagnosis of osteoporosis andhad received a single intravenous dose of zoledronic acid 12months prior to the study. This treatment was discontinued afterthe first dose because of prolonged fever and bone pain after theinfusion. One patient (#8) had been diagnosed with a symp-tomatic vertebral compression fracture following a low-energyfall. Four patients had sustained peripheral fractures; in three ofthese patients fractures (2 wrist fractures, 1 hip fracture and 1femoral shaft fracture) resulted from a low-impact trauma. Noneof the patients had motor disabilities and the level of physicalactivity was considered to be normal. Only one patient par-ticipated actively in sports. None of the patients reported bonepain.
The median Z-score for height at study assessment was −2.3(−3.1 to −0.7) and seven patients had a height Z-score below
1 patients with SDS
ipheraltures
Vertebralfractures
BMD LSZ-score
BMD LST-score
BMD FZ-score
BMD WBZ-score
BMC/ LTMZ-score
0 −2.8 – −1.3 +0.6 1.10 −2.1 – −1.6 +0.3 0.90 −1.6 – −1.2 −0.3 −0.70 −2.1 – −1.6 −0.2 0.53 −1.7 – −2.5 −2.8 −0.94 −1.9 – −1.7 –1.0 0.00 −3.7 −3.7 −1.2 −3.4 −3.61 −4.4 −4.4 −2.2 −2.8 −3.50 −2.1 −2.2 −1.3 −1.1 −1.90 −3.0 −3.0 −1.3 −2.7 −3.40 −0.8 −0.8 −0.7 –1.7 −3.4
tudy. BMI, body mass index; BMD, bone mineral density; LS, lumbar spine;ontent.

Fig. 1. BMD Z-scores in the 11 patients with SDS at the lumbar spine, proximalfemur and whole body. The bottom of each box indicates the first, the cross linethe second (median), and the top the third quartile of the variables. Whiskersextend from the box to the highest and lowest values, excluding outliers.
968 S. Toiviainen-Salo et al. / Bone 41 (2007) 965–972
−2.0. The median BMI was 20.9 kg/m2 (13.4–27.7 kg/m2).Pubertal maturation (Tanner stage and hormonal parameters)was appropriate for age in all patients.
Clinical features and radiological findings are summarized inTable 1.
Genetic findings
Eight patients were compound heterozygotes for the twocommon SBDS mutations 258+2TNC and 183TANCT. Thethree remaining patients were all heterozygous for 258+2TNC;one of them had a complex rearrangement in the other allele,one had a mutation IVS2-124GNA and in one patient the otherSBDS mutation could not be identified (Table 2).
Laboratory findings
Ten of 1l patients had neutropenia at the time of assessment;the median neutrophil count was 810×106 cells/L (range 380–1600×106 cells/L). Two patients also had thrombocytopenia.Based on the serum trypsinogen concentration (median16.9 μg/L, range 1.2–60.9 μg/L) seven patients werepancreatic sufficient (not assessed in one patient) (Table 2).Serum pancreatic isoamylase activity was below the referencerange in all the assessed patients (n=10). Fecal elastase value(median 169 μg/L, range 50–500 μg/L, n=9) was below thereference range (200 μg/L) in five patients. Plasma concentra-tions of Ca, Pi and ALP were within reference range in all thepatients. None of the patients had severe vitamin D deficiency(median 37 nmol/L, range 17–76 nmol/L) but six patients(54%) had values consistent with hypovitaminosis D (S-25-OHD below 38 nmol/L) (Table 2). Three patients hadsecondary hyperparathyroidism. In two patients, the elevatedP-PTH was probably secondary to vitamin D deficiency, in thethird patient the reason was unknown. Vitamin A and Econcentrations were normal in all the patients. The P-PT whichreflects vitamin K status, was below the reference range in sixpatients (median 73%, range 58–109%).
Table 2Genetic and biochemical findings in the 11 patients with SDS
Patient SBDS mutations Neutrophil (×106/L) S-Tryp (μg/L) S-AmylP
#1 C/unknown 450a 3.2a 4a
#2 C/D 500a 30.9 5a
#3 C/D 1300a NA NA#4 C/D 1300a 35.5 5a
#5 C/X 1100a 59.2 3a
#6 C/D 750a 1.2a 6a
#7 C/complex 1150a 7.8a 9a
#8 C/D 1600 1.9a 9a
#9 C/D 400a 14.4a 6a
#10 C/D 800a 19.3 5a
#11 C/D 1400a 60.9 7a
Normal N1500 16.6–42.6 13–53
C, 258+2TNC; D, 183TANCT; X, IVS2-124GNA; S-Tryp, serum cationic trypsinogvitamin D; P-PT, plasma prothrombin time; fP-PTH, serum parathyroid hormone;supranormal values with b.
Radiographic findings
BMD results were available for all the patients (Table 1 andFig. 1). The median Z-scores were for the lumbar spine −2.1(range −4.4 to −0.8), for the proximal femur −1.3 (−2.2 to−0.7), and for the whole body −1.0 (−2.8 to +0.6). The lumbarspine BMD Z-score was below −1.0 in ten patients (91 %) andbelow −2.0 in seven patients (63%). The median Z-score forheight-adjusted BMC/LTM was −0.9 (range −3.6 to +1.1); itwas below −1.0 in five patients and below −2.0 in four patients(Table 1). According to the WHO classification for adults[40], which is based on the lumbar spine and femoral neckBMD T-scores, four of the five adults had either osteopenia(T-score b−1.0) or osteoporosis (T-score b−2.5). There wasno correlation between the degree of neutropenia and any ofthe BMD values.
Spinal radiographs of all eleven patients were available forassessment. Three patients had a total of eight compressedvertebrae (Table 1) all of which were located in the thoracic
(U/L) S-25-OHD (nmol/L) P-PT (%) P-PTH (ng/L) P-ALP (U/L)
75 58a 45 21733a 59a 26 15245 84 25 28176 69a 94b 26836a 109 40 27855 58a 43 21937a 73 51 11017a 64a 38 6639 74 86b 7826a 65a 80b 8931a 83 50 80
≥38 N70 8–73 Age-specific
en; S-AmylP, serum pancreatic isoamylase activity; S-25-OHD, serum 25-OH-P-ALP, plasma alkaline phosphatase. Subnormal values are marked with a and
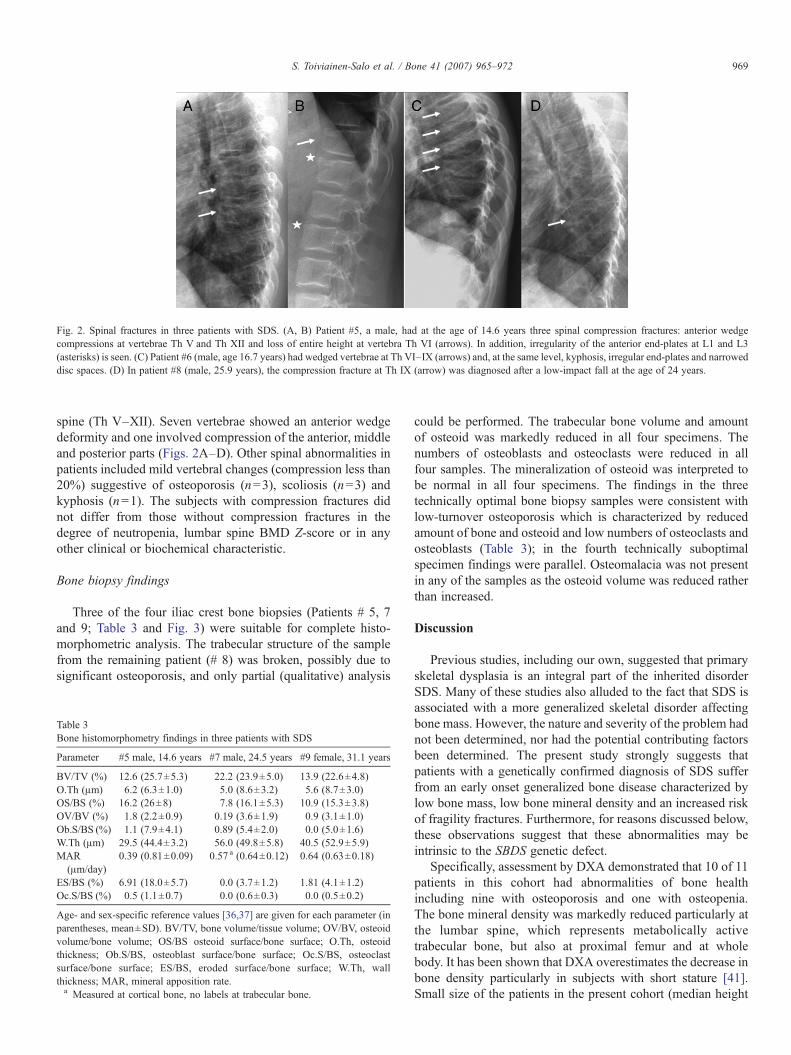
Fig. 2. Spinal fractures in three patients with SDS. (A, B) Patient #5, a male, had at the age of 14.6 years three spinal compression fractures: anterior wedgecompressions at vertebrae Th V and Th XII and loss of entire height at vertebra Th VI (arrows). In addition, irregularity of the anterior end-plates at L1 and L3(asterisks) is seen. (C) Patient #6 (male, age 16.7 years) had wedged vertebrae at Th VI–IX (arrows) and, at the same level, kyphosis, irregular end-plates and narroweddisc spaces. (D) In patient #8 (male, 25.9 years), the compression fracture at Th IX (arrow) was diagnosed after a low-impact fall at the age of 24 years.
969S. Toiviainen-Salo et al. / Bone 41 (2007) 965–972
spine (Th V–XII). Seven vertebrae showed an anterior wedgedeformity and one involved compression of the anterior, middleand posterior parts (Figs. 2A–D). Other spinal abnormalities inpatients included mild vertebral changes (compression less than20%) suggestive of osteoporosis (n=3), scoliosis (n=3) andkyphosis (n=1). The subjects with compression fractures didnot differ from those without compression fractures in thedegree of neutropenia, lumbar spine BMD Z-score or in anyother clinical or biochemical characteristic.
Bone biopsy findings
Three of the four iliac crest bone biopsies (Patients # 5, 7and 9; Table 3 and Fig. 3) were suitable for complete histo-morphometric analysis. The trabecular structure of the samplefrom the remaining patient (# 8) was broken, possibly due tosignificant osteoporosis, and only partial (qualitative) analysis
Table 3Bone histomorphometry findings in three patients with SDS
Parameter #5 male, 14.6 years #7 male, 24.5 years #9 female, 31.1 years
BV/TV (%) 12.6 (25.7±5.3) 22.2 (23.9±5.0) 13.9 (22.6±4.8)O.Th (μm) 6.2 (6.3±1.0) 5.0 (8.6±3.2) 5.6 (8.7±3.0)OS/BS (%) 16.2 (26±8) 7.8 (16.1±5.3) 10.9 (15.3±3.8)OV/BV (%) 1.8 (2.2±0.9) 0.19 (3.6±1.9) 0.9 (3.1±1.0)Ob.S/BS (%) 1.1 (7.9±4.1) 0.89 (5.4±2.0) 0.0 (5.0±1.6)W.Th (μm) 29.5 (44.4±3.2) 56.0 (49.8±5.8) 40.5 (52.9±5.9)MAR
(μm/day)0.39 (0.81±0.09) 0.57 a (0.64±0.12) 0.64 (0.63±0.18)
ES/BS (%) 6.91 (18.0±5.7) 0.0 (3.7±1.2) 1.81 (4.1±1.2)Oc.S/BS (%) 0.5 (1.1±0.7) 0.0 (0.6±0.3) 0.0 (0.5±0.2)
Age- and sex-specific reference values [36,37] are given for each parameter (inparentheses, mean±SD). BV/TV, bone volume/tissue volume; OV/BV, osteoidvolume/bone volume; OS/BS osteoid surface/bone surface; O.Th, osteoidthickness; Ob.S/BS, osteoblast surface/bone surface; Oc.S/BS, osteoclastsurface/bone surface; ES/BS, eroded surface/bone surface; W.Th, wallthickness; MAR, mineral apposition rate.a Measured at cortical bone, no labels at trabecular bone.
could be performed. The trabecular bone volume and amountof osteoid was markedly reduced in all four specimens. Thenumbers of osteoblasts and osteoclasts were reduced in allfour samples. The mineralization of osteoid was interpreted tobe normal in all four specimens. The findings in the threetechnically optimal bone biopsy samples were consistent withlow-turnover osteoporosis which is characterized by reducedamount of bone and osteoid and low numbers of osteoclasts andosteoblasts (Table 3); in the fourth technically suboptimalspecimen findings were parallel. Osteomalacia was not presentin any of the samples as the osteoid volume was reduced ratherthan increased.
Discussion
Previous studies, including our own, suggested that primaryskeletal dysplasia is an integral part of the inherited disorderSDS. Many of these studies also alluded to the fact that SDS isassociated with a more generalized skeletal disorder affectingbone mass. However, the nature and severity of the problem hadnot been determined, nor had the potential contributing factorsbeen determined. The present study strongly suggests thatpatients with a genetically confirmed diagnosis of SDS sufferfrom an early onset generalized bone disease characterized bylow bone mass, low bone mineral density and an increased riskof fragility fractures. Furthermore, for reasons discussed below,these observations suggest that these abnormalities may beintrinsic to the SBDS genetic defect.
Specifically, assessment by DXA demonstrated that 10 of 11patients in this cohort had abnormalities of bone healthincluding nine with osteoporosis and one with osteopenia.The bone mineral density was markedly reduced particularly atthe lumbar spine, which represents metabolically activetrabecular bone, but also at proximal femur and at wholebody. It has been shown that DXA overestimates the decrease inbone density particularly in subjects with short stature [41].Small size of the patients in the present cohort (median height

Fig. 3. Bone biopsies in two patients with SDS (patient #9, A and B; patient #7, C and D) show significant osteoporosis with low bone volume, reduced amount ofosteoid and reduced numbers of osteoblasts and osteoclasts. Magnification: ×20 in panels A and C, ×100 in panels B and D.
970 S. Toiviainen-Salo et al. / Bone 41 (2007) 965–972
Z-score −2.3) could thus partly explain the observed reductionsin BMD. However, the height-corrected BMC/LTM ratio,which has been regarded a more accurate method to assess bonehealth especially in subjects with short stature [32] was alsoreduced in seven patients. The low BMC and BMD results,history of low-impact peripheral fractures, signs of osteoporoticvertebral deformities in spinal radiographs in some patients aswell as the bone biopsy findings all suggest that patients withSDS have true osteoporosis with reduced bone mass andimpaired bone quality.
Bone biopsies in four patients showed significant low-turnover osteoporosis with reduced trabecular bone volume,low numbers of osteoclasts and osteoblasts, and reducedamount of osteoid. These differ from bone histomorphometryfindings in CF which have shown decreased osteoblastic, butincreased osteoclastic activity [42]. Our findings suggest thatpatients with SDS suffer from a primary defect in bone metab-olism. The expression and role of SBDS in bone and in variouscell types essential for normal bone formation and turnover areunknown. Since macrophage/osteoclast and neutrophil lineageshave a common precursor stem cell, the granulocyte/macro-phage colony-forming cell, the reduction in osteoclasts andneutropenia in SDS may be due to marrow hypofunction at thelevel of stem cell. Low-turnover osteoporosis with reducednumbers of both osteoclasts and osteoblasts may be directlyrelated to the SBDS defect in stem cell proliferation ordifferentiation. This however remains to be evaluated in futurestudies.
Malabsorption due to exocrine pancreatic insufficiency is themain manifestation of SDS. Thus it could be speculated that thereductions in bone density in our cohort were at least partlysecondary to compromised nutrition and decreased absorptionof fat-soluble vitamins, of which especially vitamin D andvitamin K are known to play an important role in skeletal health.At the latitude of Finland (situated 60°N and higher), low
vitamin D status is commonly observed even in healthyindividuals and vitamin status varies according to the season,being lowest in the winter [43,44]. Of our study cohort, six outof 11 patients had hypovitaminosis D when using the cut-offvalue of 38 nmol/L, and three patients had an increased P-PTHvalue. In two patients, the elevated P-PTH was probablysecondary to vitamin D deficiency; in the third patient, thereason was unknown. Despite adequate S-25-OHD and calciumintake calcium absorption may be subnormal and contribute tosecondary hyperparathyroidism. None of the patients had a S-25-OHD concentration above 80 nmol/L, a value that has oftenbeen regarded as the target concentration when direct positiveimpact on bone health is desired [45]. These observed vitamin Dvalues are comparable to those recently observed in healthyFinnish military recruits [44]. Furthermore, none of the studiedpatients with SDS had osteomalacia characteristic of vitamin Ddeficiency in bone biopsies. Taken together, vitamin D defi-ciency seems not to be a significant cause of impaired bonehealth in SDS.
Several studies have demonstrated that low dietary vitaminK intake is associated with low BMD and increased fractures[46,47]. Vitamins K and D may have synergistic effects on boneloss [48] and deficiency of both vitamins could be more harmfulthan deficiency of only one of them. Vitamin K status in thepresent cohort was assessed indirectly by prothrombin timeassay. The results are in accordance with suboptimal intake and/or absorption of vitamin K in some of the patients. Althoughprobably having a negative influence on bone, vitamin Kdeficiency does not alone cause osteoporosis, as was seen inPatient #5, who had normal vitamin K and D status, but severeclinical and biopsy confirmed osteoporosis.
Regarding the nutritional risk factors associated withpancreatic insufficiency and malabsorption, SDS patients sharesimilarities with patients with cystic fibrosis (CF) who also havebeen reported to be at risk of osteopenia and osteoporosis [49–

971S. Toiviainen-Salo et al. / Bone 41 (2007) 965–972
52]. Based on our observations SDS patients do, however, haveeven lower BMDs than reported for CF patients even though thelatter group has additional risk factors such as the use of steroids,chronic inflammation, more severe malnutrition, more severemalabsorption and reduced physical activity.
In conclusion, the present study shows that osteoporosis is anintegral feature of Shwachman–Diamond syndrome. SDSosteoporosis is characterized by reduced numbers of osteoclastsand osteoblasts and low bone turnover and may be directlyrelated to the bone marrow dysfunction and neutropenia.Malabsorption could be an additional risk factor. The findingsof the present study expand the SDS-related bone disease toinclude, in addition to abnormalities in metaphyseal andepiphyseal development, also primary osteoporosis. Furtherstudies are necessary to elucidate the role of the SBDS protein inthe function of chondrocytes, osteoblasts, osteoclasts and theirprecursors. While no therapeutic means to target the primarydefect are presently available, efforts should bemade to optimizegeneral preventive measures such as nutrition and intake of fatsoluble vitamins, and weight-bearing exercise. The role ofbisphosphonates and anabolic agents in the treatment of SDS-associated low-turnover osteoporosis needs to be addressed infuture studies.
Acknowledgments
We would like to thank RN Päivikki Rissanen for assistancein clinical evaluations and Prof. Heikki Kröger for helpfulcomments regarding the bone biopsy findings. Funding: Thestudy was financially supported by the Päivikki and SakariSohlberg Foundation, the Foundation for Pediatric Research,the Sigrid Juselius Foundation, the Finnish Medical SocietyDuodecim, the Helsinki University Hospital research fund allHelsinki, Finland, and Canadian Institutes of Health Research,Canada.
References
[1] Shwachman H, Diamond LK, Oski FA, Khaw KT. The syndrome ofpancreatic insufficiency and bone marrow dysfunction. J Pediatr 1964;65:645–63.
[2] Bodian M, Sheldon W, Lightwood R. Congenital hypoplasia of theexocrine pancreas. Acta Paediatr 1964;53:282–93.
[3] Mack DR, Forstner GG, Wilschanski M, Freedman MH, Durie PR.Shwachman syndrome: exocrine pancreatic dysfunction and variablephenotypic expression. Gastroenterology 1996;111:1593–602.
[4] Ip WF, Dupuis A, Ellis L, Beharry S, Morrison J, Stormon MO, et al.Serum pancreatic enzymes define the pancreatic phenotype in patients withShwachman–Diamond syndrome. J Pediatr 2002;141:259–65.
[5] Berrocal T, Simon MJ, Al-Assir I, Prieto C, Pastor I, de Pablo L, et al.Shwachman–Diamond syndrome: clinical, radiological and sonographicaspects. Pediatr Radiol 1995;25:289–92.
[6] Berrocal T, Simon MJ, Al-Assir I, Prieto C, Pastor I, de Pablo L, et al.Shwachman–Diamond syndrome: clinical, radiological and sonographicfindings. Pediatr Radiol 1995;25:356–9.
[7] Lacaille F, Mani TM, Brunelle F, Lallemand D, Schmitz J. Magneticresonance imaging for diagnosis of Shwachman's syndrome. J PediatrGastroenterol Nutr 1996;23:599–603.
[8] Dror Y, Freedman MH. Shwachman–Diamond syndrome: an inheritedpreleukemic bone marrow failure disorder with aberrant hematopoietic
progenitors and faulty marrow microenvironment. Blood 1999;94:3048–54.
[9] Dror Y, Freedman MH. Shwachman–Diamond syndrome. Br J Haematol2002;118:701–13.
[10] Boocock GR, Morrison JA, Popovic M, Richards N, Ellis L, Durie PR, etal. Mutations in SBDS are associated with Shwachman–Diamondsyndrome. Nat Genet 2003;33:97–101.
[11] Nicolis E, Bonizzato A, Assael BM, Cipolli M. Identification of novelmutations in patients with Shwachman–Diamond syndrome. HumanMutat 2005;25:410.
[12] Nakashima E, Mabuchi A, Makita Y, Masuno M, Ohashi H, Nishimura G,et al. Novel SBDS mutations caused by gene conversion in Japanesepatients with Shwachman–Diamond syndrome. Hum Genet 2004;114:345–8.
[13] Kawakami T, Mitsui T, Kanai M, Shirahata E, Sendo D, Kanno M, et al.Genetic analysis of Shwachman–Diamond syndrome: phenotypic hetero-geneity in patients carrying identical SBDS mutations. Tohoku J Exp Med2005;206:253–9.
[14] Savchenko A, Krogan N, Cort JR, Evdokimova E, Lew JM, YeeAA, et al. The Shwachman–Bodian–Diamond syndrome proteinfamily is involved in RNA metabolism. J Biol Chem 2005;280:19213–20.
[15] Austin KM, Leary RJ, Shimamura A. The Shwachman–Diamond SBDSprotein localizes to the nucleolus. Blood 2005;106:1253–8.
[16] Boocock GR, Marit MR, Rommens JM. Phylogeny, sequence conserva-tion, and functional complementation of the SBDS protein family.Genomics 2006;87:758–71.
[17] Menne TF, Goyenechea B, Sanchez-Puig N, Wong CC, Tonkin LM,Ancliff PJ, et al. The Shwachman–Bodian–Diamond syndrome proteinmediates translational activation of ribosomes in yeast. Nat Genet 2007;39:486–95.
[18] Burke V, Colebatch JH, Anderson CM, Simons MJ. Association ofpancreatic insufficiency and chronic neutropenia in childhood. Arch DisChild 1967;42:147–57.
[19] Aggett PJ, Cavanagh NP, Matthew DJ, Pincott JR, Sutcliffe J, Harries JT.Shwachman's syndrome. A review of 21 cases. Arch Dis Child 1980;55:331–47.
[20] Taybi H, Mitchell AD, Friedman GD. Metaphyseal dysostosis and theassociated syndrome of pancreatic insufficiency and blood disorders.Radiology 1969;93:563–71.
[21] Danks DM, Haslam R, Mayne V, Kaufmann HJ, Holtzapple PG.Metaphyseal chondrodysplasia, neutropenia, and pancreatic insufficiencypresenting with respiratory distress in the neonatal period. Arch Dis Child1976;51:697–702.
[22] McLennan TW, Steinbach HL. Shwachman's syndrome: the broadspectrum of bony abnormalities. Radiology 1974;112:167–73.
[23] Nishimura G, Nakashima E, Hirose Y, Cole T, Cox P, Cohn DH, et al. TheShwachman–Bodian–Diamond syndrome gene mutations cause a neona-tal form of spondylometaphysial dysplasia (SMD) resembling SMDSedaghatian type. J Med Genet 2007;44:e73.
[24] Mäkitie O, Ellis L, Durie PR, Morrison JA, Sochett EB, Rommens JM, etal. Skeletal phenotype in patients with Shwachman–Diamond syndromeand mutations in SBDS. Clin Genet 2004;65:101–12.
[25] Ginzberg H, Shin J, Ellis L, Morrison J, Ip W, Dror Y, et al. Shwachmansyndrome: phenotypic manifestations of sibling sets and isolated cases in alarge patient cohort are similar. J Pediatr 1999;135:81–8.
[26] Fellman K, Kozlowski K, Senger A. Unusual bone changes in exocrinepancreas insufficiency with cyclic neutropenia. Acta Radiol Diagn(Stockh) 1972;12:428–32.
[27] Rosendahl J, Teich N, Mossner J, Edelmann J, Koch CA. Compoundheterozygous mutations of the SBDS gene in a patient with Shwachman–Diamond syndrome, type 1 diabetes mellitus and osteoporosis. Pancrea-tology 2006;6:549–54.
[28] Sorva R, Lankinen S, Tolppanen EM, Perheentupa J. Variation of growthin height and weight of children: II. After infancy. Acta Paediatr Scand1990;79:498–506.
[29] Pere A. Comparison of two methods for transforming height and weight tonormality. Ann Hum Biol 2000;27:35–45.

972 S. Toiviainen-Salo et al. / Bone 41 (2007) 965–972
[30] Tanner JM, Whitehouse RH. Clinical longitudinal standards for height,weight, height velocity, weight velocity, and stages of puberty. Arch DisChild 1976;51:170–9.
[31] Moore DJ, Forstner GG, Largman C, Cleghorn GJ, Wong SS, Durie PR.Serum immunoreactive cationic trypsinogen: a useful indicator of severeexocrine dysfunction in the paediatric patient without cystic fibrosis. Gut1986;27:1362–8.
[32] Hogler W, Briody J, Woodhead HJ, Chan A, Cowell CT. Importance oflean mass in the interpretation of total body densitometry in children andadolescents. J Pediatr 2003;143:81–8.
[33] Genant HK, Wu CY, van Kuijk C, Nevitt MC. Vertebral fracture assess-ment using a semiquantitative technique. J Bone Miner Res 1993;8:1137–48.
[34] Mäkitie O, Doria AS, Henriques F, Cole WG, Compeyrot S, Silverman E,et al. Radiographic vertebral morphology: a diagnostic tool in pediatricosteoporosis. J Pediatr 2005;146:395–401.
[35] Recker RR, Kimmel DB, Parfitt AM, Davies KM, Keshawarz N, HindersS. Static and tetracycline-based bone histomorphometric data from 34normal postmenopausal females. J Bone Miner Res 1988;3:133–44.
[36] Rehman MT, Hoyland JA, Denton J, Freemont AJ. Age relatedhistomorphometric changes in bone in normal British men and women.J Clin Pathol 1994;47:529–34.
[37] Glorieux FH, Travers R, Taylor A, Bowen JR, Rauch F, Norman M, et al.Normative data for iliac bone histomorphometry in growing children.Bone 2000;26:103–9.
[38] Dallman PR, Siimes MA. Percentile curves for hemoglobin and red cellvolume in infancy and childhood. J Pediatr 1979;94:26–31.
[39] Geokas MC, Largman C, Brodrick JW, Johnson JH. Determination ofhuman pancreatic cationic trypsinogen in serum by radioimmunoassay.Am J Physiol 1979;236:E77–83.
[40] Genant HK, Cooper C, Poor G, Reid I, Ehrlich G, Kanis J, et al. Interimreport and recommendations of the World Health Organization task-forcefor osteoporosis. Osteoporos Int 1999;10:259–64.
[41] Wren TA, Liu X, Pitukcheewanont P, Gilsanz V. Bone densitometry inpediatric populations: discrepancies in the diagnosis of osteoporosis byDXA and CT. J Pediatr 2005;146:776–9.
[42] Haworth CS, Webb AK, Egan JJ, Selby PL, Hasleton PS, Bishop PW, et al.Bone histomorphometry in adult patients with cystic fibrosis. Chest2000;118:434–9.
[43] Lamberg-Allardt CJ, Outila TA, Kärkkäinen MU, Rita HJ, Valsta LM.Vitamin D deficiency and bone health in healthy adults in Finland: couldthis be a concern in other parts of Europe? J Bone Miner Res 2001;16:2066–73. 39.
[44] Välimaki VV, Alfthan H, Lehmuskallio E, Löyttyniemi E, Sahi T, StenmanUH, et al. Vitamin D status as a determinant of peak bone mass in youngFinnish men. J Clin Endocrinol Metab 2004;89:76–80.
[45] Dawson-Hughes B, Heaney RP, Holick MF, Lips P, Meunier PJ, Vieth R.Estimates of optimal vitamin D status. Osteoporos Int 2005;16:713–6.
[46] Hodges SJ, PilkingtonMJ, Stamp TC, Catterall A, Shearer MJ, Bitensky L,et al. Depressed levels of circulating menaquinones in patients withosteoporotic fractures of the spine and femoral neck. Bone 1991;12:387–9.
[47] Weber P. Vitamin K and bone health. Nutrition 2001;17:880–7 Review.[48] Matsunaga S, Ito H, Sakou T. The effect of vitamin K and D supplemen-
tation on ovariectomy-induced bone loss. Calcif Tissue Int 1999;65:285–9.[49] Haworth CS, Selby PL, Webb AK, Dodd ME, Musson H, McLNiven R,
et al. Low bone mineral density in adults with cystic fibrosis. Thorax1999;54:961–7.
[50] Conway SP, Morton AM, Oldroyd B, White H, Smith AH, Haigh I.Osteoporosis and osteopenia in adults and adolescents with cystic fibrosis:prevalence and associated factors. Thorax 2000;55:798–804.
[51] Conway SP, Wolfe SP, Brownlee KG, White H, Oldroyd B, Truscott JG, etal. Vitamin K status among children with cystic fibrosis and its relationshipto bone mineral density and bone turnover. Pediatrics 2005;115:1325–31.
[52] Shead EF, Haworth CS, Gunn E, Bilton D, Scott MA, Compston JE.Osteoclastogenesis during infective exacerbations in patients with cysticfibrosis. Am J Respir Crit Care Med 2006;174:306–11.
Related Documents











