Please cite this article in press as: Saccol MF, et al. Shoulder rotator strength and torque steadiness in athletes with anterior shoulder instability or SLAP lesion. J Sci Med Sport (2013), http://dx.doi.org/10.1016/j.jsams.2013.10.246 ARTICLE IN PRESS G Model JSAMS-955; No. of Pages 6 Journal of Science and Medicine in Sport xxx (2013) xxx–xxx Contents lists available at ScienceDirect Journal of Science and Medicine in Sport j our na l ho me page: www.elsevier.com/locate/jsams Original research Shoulder rotator strength and torque steadiness in athletes with anterior shoulder instability or SLAP lesion Michele Forgiarini Saccol a,∗ , Gisele Garcia Zanca a , Benno Ejnisman b , Marco Túlio de Mello c , Stela Márcia Mattiello a a Department of Physical Therapy, Federal University of São Carlos, São Carlos, Brazil b Department of Orthopaedic Surgery and Sports Medicine, Federal University of São Paulo, São Paulo, Brazil c Center of Studies on Psychobiology and Exercise, Department of Psychobiology, Federal University of São Paulo, São Paulo, Brazil a r t i c l e i n f o Article history: Received 18 April 2013 Received in revised form 7 October 2013 Accepted 13 October 2013 Available online xxx Keywords: Shoulder joint Muscle strength Sensory motor performance Joint instability SLAP lesion a b s t r a c t Objectives: To investigate shoulder rotator strength and steadiness in athletes with anterior instability and superior labrum anterior posterior (SLAP) lesion. Design: Cross-sectional laboratory study. Methods: Athletes with anterior shoulder instability (instability group, n = 10) and a SLAP lesion (SLAP group, n = 10) were compared with healthy athletes matched by age, anthropometrics and sport (control group for shoulder instability, n = 10 and control group for SLAP, n = 10). Torque steadiness was evaluated with three 10 s submaximal isometric contractions (35% of peak torque) with the arm at 90 ◦ of shoulder abduction and 90 ◦ of external rotation. The mean isometric torque, standard deviation and coefficient of variation were measured from the steadiness trials. To evaluate shoulder rotator strength, concentric isokinetic tests (90 ◦ /s, 180 ◦ /s) were performed at the 90–90 ◦ position and peak torque to body mass and shoulder external to internal rotation ratio variables were analyzed. The variables were tested with the instability and control groups with respect to shoulder instability and between the SLAP and control groups for SLAP lesion using the Mann–Whitney test. Results: The SLAP group presented a higher coefficient of variation than the SLAP control group (p = 0.003). Regarding shoulder strength, the internal and external shoulder rotators were weaker in the instability group than in the instability control group (p < 0.05). Conclusions: Athletes with anterior shoulder instability presented shoulder rotation weakness, while athletes with a SLAP lesion showed higher torque fluctuation during internal rotation. These results indicate that there are different alterations to strength and sensory motor control in each condition. © 2013 Published by Elsevier Ltd on behalf of Sports Medicine Australia. 1. Introduction During sports activities, shoulder joint ligaments and muscles are constantly challenged to maintain glenohumeral joint stability via passive bony and soft-tissue restraints and dynamic stability via the rotator cuff and scapular muscle. 1,2 If any disruption occurs in the static restraints, the synergistic relationship that results in glenohumeral stability can be compromised, overloading the dynamic stabilizers. 3 Losses in static stability are present in superior labrum ante- rior posterior (SLAP) lesions and in recurrent shoulder instability after traumatic first-time shoulder dislocation, 4–6 which are the most common injuries among young athletes. 7–9 These lesions represent a real challenge in sports medicine rehabilitation, ∗ Corresponding author. E-mail address: [email protected] (M.F. Saccol). since they produce persistent symptoms that interfere in reg- ular sports participation. 8,9 Considering that these conditions are associated with deficits in the static stabilizers of the shoulder, 5,6 it follows that the dynamic stabilizers would also present some adaptation in order to maintain functional joint sta- bility. Rotator cuff muscles are essential to dynamic shoulder stabil- ity by preventing excessive translations of the humeral head at the glenoid fossa. 3 Studies have found a tendency toward a lower shoulder external-to-internal rotation ratio, 10 as well as rotator cuff weakness 11 in athletes with recurrent anterior shoulder instabil- ity. With respect to SLAP lesions, however, there are only reports on shoulder rotator strength after arthroscopic repair. 7,12 Besides muscle strength, joint stability also depends on proper muscle balance, 8 which can be evaluated during steady submaximal iso- metric contractions. 13,14 The ability to perform muscle contractions with a minimum of force fluctuation during a constant-force task, i.e., torque steadiness, is considered an integrated sensorimotor 1440-2440/$ – see front matter © 2013 Published by Elsevier Ltd on behalf of Sports Medicine Australia. http://dx.doi.org/10.1016/j.jsams.2013.10.246

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

G
J
O
Sa
MMa
b
c
ARRAA
KSMSJS
1
avviid
ramr
1h
ARTICLE IN PRESS Model
SAMS-955; No. of Pages 6
Journal of Science and Medicine in Sport xxx (2013) xxx– xxx
Contents lists available at ScienceDirect
Journal of Science and Medicine in Sport
j our na l ho me page: www.elsev ier .com/ locate / j sams
riginal research
houlder rotator strength and torque steadiness in athletes withnterior shoulder instability or SLAP lesion
ichele Forgiarini Saccola,∗, Gisele Garcia Zancaa, Benno Ejnismanb,arco Túlio de Melloc, Stela Márcia Mattielloa
Department of Physical Therapy, Federal University of São Carlos, São Carlos, BrazilDepartment of Orthopaedic Surgery and Sports Medicine, Federal University of São Paulo, São Paulo, BrazilCenter of Studies on Psychobiology and Exercise, Department of Psychobiology, Federal University of São Paulo, São Paulo, Brazil
a r t i c l e i n f o
rticle history:eceived 18 April 2013eceived in revised form 7 October 2013ccepted 13 October 2013vailable online xxx
eywords:houlder jointuscle strength
ensory motor performanceoint instabilityLAP lesion
a b s t r a c t
Objectives: To investigate shoulder rotator strength and steadiness in athletes with anterior instabilityand superior labrum anterior posterior (SLAP) lesion.Design: Cross-sectional laboratory study.Methods: Athletes with anterior shoulder instability (instability group, n = 10) and a SLAP lesion (SLAPgroup, n = 10) were compared with healthy athletes matched by age, anthropometrics and sport (controlgroup for shoulder instability, n = 10 and control group for SLAP, n = 10). Torque steadiness was evaluatedwith three 10 s submaximal isometric contractions (35% of peak torque) with the arm at 90◦ of shoulderabduction and 90◦ of external rotation. The mean isometric torque, standard deviation and coefficientof variation were measured from the steadiness trials. To evaluate shoulder rotator strength, concentricisokinetic tests (90◦/s, 180◦/s) were performed at the 90–90◦ position and peak torque to body massand shoulder external to internal rotation ratio variables were analyzed. The variables were tested withthe instability and control groups with respect to shoulder instability and between the SLAP and controlgroups for SLAP lesion using the Mann–Whitney test.
Results: The SLAP group presented a higher coefficient of variation than the SLAP control group (p = 0.003).Regarding shoulder strength, the internal and external shoulder rotators were weaker in the instabilitygroup than in the instability control group (p < 0.05).Conclusions: Athletes with anterior shoulder instability presented shoulder rotation weakness, whileathletes with a SLAP lesion showed higher torque fluctuation during internal rotation. These resultsindicate that there are different alterations to strength and sensory motor control in each condition.. Introduction
During sports activities, shoulder joint ligaments and musclesre constantly challenged to maintain glenohumeral joint stabilityia passive bony and soft-tissue restraints and dynamic stabilityia the rotator cuff and scapular muscle.1,2 If any disruption occursn the static restraints, the synergistic relationship that resultsn glenohumeral stability can be compromised, overloading theynamic stabilizers.3
Losses in static stability are present in superior labrum ante-ior posterior (SLAP) lesions and in recurrent shoulder instability
Please cite this article in press as: Saccol MF, et al. Shoulder rotator strengtor SLAP lesion. J Sci Med Sport (2013), http://dx.doi.org/10.1016/j.jsams.201
fter traumatic first-time shoulder dislocation,4–6 which are theost common injuries among young athletes.7–9 These lesions
epresent a real challenge in sports medicine rehabilitation,
∗ Corresponding author.E-mail address: [email protected] (M.F. Saccol).
440-2440/$ – see front matter © 2013 Published by Elsevier Ltd on behalf of Sports Medttp://dx.doi.org/10.1016/j.jsams.2013.10.246
© 2013 Published by Elsevier Ltd on behalf of Sports Medicine Australia.
since they produce persistent symptoms that interfere in reg-ular sports participation.8,9 Considering that these conditionsare associated with deficits in the static stabilizers of theshoulder,5,6 it follows that the dynamic stabilizers would alsopresent some adaptation in order to maintain functional joint sta-bility.
Rotator cuff muscles are essential to dynamic shoulder stabil-ity by preventing excessive translations of the humeral head atthe glenoid fossa.3 Studies have found a tendency toward a lowershoulder external-to-internal rotation ratio,10 as well as rotator cuffweakness11 in athletes with recurrent anterior shoulder instabil-ity. With respect to SLAP lesions, however, there are only reportson shoulder rotator strength after arthroscopic repair.7,12 Besidesmuscle strength, joint stability also depends on proper muscle
h and torque steadiness in athletes with anterior shoulder instability3.10.246
balance,8 which can be evaluated during steady submaximal iso-metric contractions.13,14 The ability to perform muscle contractionswith a minimum of force fluctuation during a constant-force task,i.e., torque steadiness, is considered an integrated sensorimotor
icine Australia.

ARTICLE IN PRESSG Model
JSAMS-955; No. of Pages 6
2 M.F. Saccol et al. / Journal of Science and Medicine in Sport xxx (2013) xxx– xxx
espec
ctko
fbTSrsiebtit
rsAano
2
rtsE
istltSpjsrt
Fig. 1. Injured athletes and r
ontrol evaluation.13 Although restoring neural and muscle func-ion is essential to shoulder rehabilitation,15 no study, to ournowledge, has yet described the steadiness pattern in SLAP lesionsr shoulder instability.
Strength, stability and motion are the components of shoulderunction that should be focused on rehabilitation, which shoulde specifically directed to the alterations present in an injury.he damaged structures and the referred symptoms are diverse inLAP lesions and anterior shoulder instability.1,5 However, currentecommendations for conservative treatment of these lesions areimilar, including rotator cuff resistance and sensorimotor train-ng to improve dynamic joint stability.16–18 The lack of studiesvaluating muscle strength and control in SLAP and shoulder insta-ility makes specific rehabilitation planning more difficult. In ordero establish specific rehabilitation strategies, it is fundamental tonvestigate possible alterations in the strength and control of rota-or cuff muscles in these injuries.
Therefore, the aim of this study was to investigate shoulderotation strength and torque steadiness in athletes with anteriorhoulder instability or SLAP lesion compared with healthy athletes.
better understanding of possible alterations in maximal strengthnd submaximal strength control of these muscles may help cli-icians plan specific rehabilitation strategies for each injury, thusptimizing recovery and sports participation.
. Methods
Athletes with anterior shoulder instability or SLAP lesion wereecruited at an orthopedic clinic. All of them agreed to participate inhe study on a voluntary basis and provided written informed con-ent. This study was approved by the University Human Researchthics Committee.
The inclusion criteria for participants of the anterior instabil-ty group were a minimum of one episode of traumatic anteriorhoulder dislocation, a positive apprehension test, sulcus sign andhe anterior load-and-shift test.5 The inclusion criteria for the SLAPesion group were a clinical diagnosis based on a positive O’Brienest, anterior tenderness to palpation and MRI documentation ofLAP type II, III, IV or V.8 All diagnoses were given by the same ortho-edic shoulder surgeon. The exclusion criteria included generalized
Please cite this article in press as: Saccol MF, et al. Shoulder rotator strengtor SLAP lesion. J Sci Med Sport (2013), http://dx.doi.org/10.1016/j.jsams.201
oint laxity, bilateral shoulder lesion, multidirectional instability,igns of rotator cuff lesion, degenerative arthritis, systemic or neu-ological illnesses, previous shoulder or neck surgery or physicalherapy treatment in the 12 months prior to the study. Athletes
tive control group selection.
with limited external shoulder rotation (less than 95◦) and withmore than 10 episodes of shoulder dislocation were excluded, sincethey were unable to achieve the shoulder positions used in thestudy without pain or apprehension.
Healthy athletes with no history of shoulder pain or injury werepaired with injured participants by anthropometric characteristicsand sport type. Fig. 1 describes the group selection.
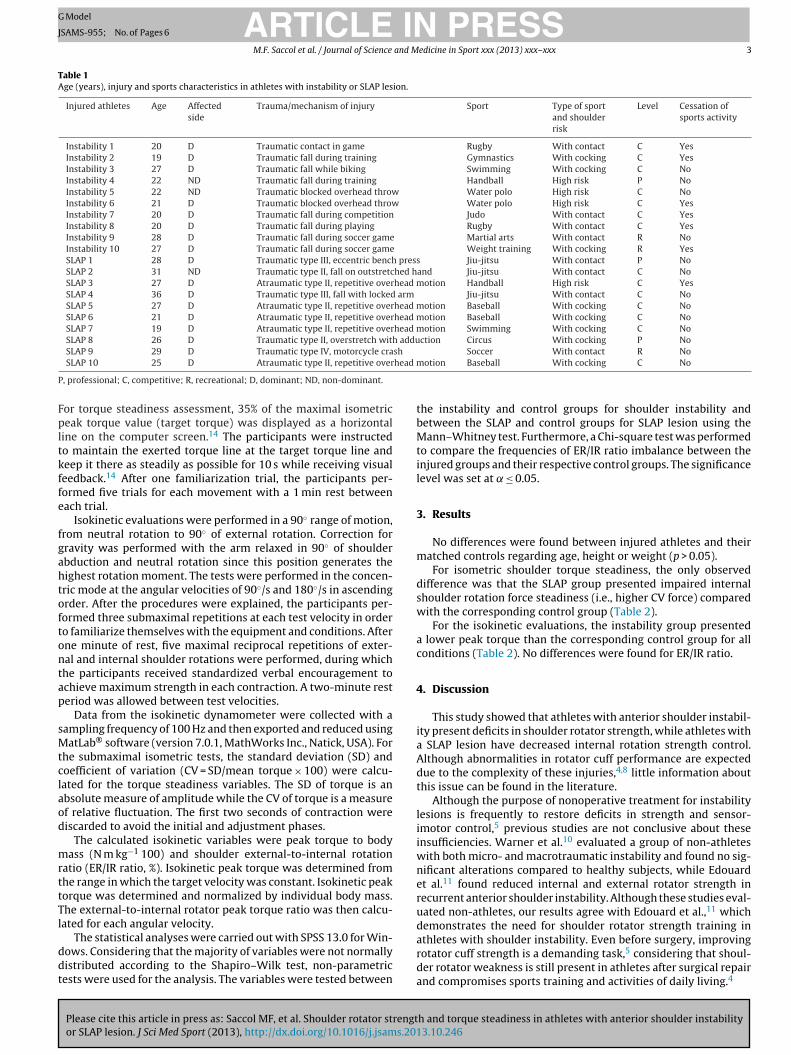
Four groups of male athletes were evaluated: an instabilitygroup (n = 10; 22.6 ± 3.4 years; 1.8 ± 0.05 m; 83.8 ± 7.7 kg); a shoul-der instability control group (n = 10; 22 ± 3.4 years; 1.8 ± 0.08 m;82 ± 9.2 kg); a SLAP group (n = 10; 26.9 ± 4.7 years; 1.7 ± 0.05 m;77.4 ± 14.9 kg) and a SLAP control group (n = 10; 26.4 ± 4.5 years;1.7 ± 0.04 m; 78.1 ± 8.5 kg). Information regarding age, affectedside (dominant side = preferred arm during sports), trauma andsport type from the instability and SLAP groups are presented inTable 1.
Athletes involved in different sports were included from pro-fessional (15%), competitive (70%) and recreational (15%) levels.According the Walch (1987)19 classification for shoulder risk insport, 60% of the athletes in our sample were involved in sports withcocking or high risk (cocking and blocking) and 40% were involvedin contact sports.
The isometric and isokinetic evaluations were performed duringinternal and external shoulder rotations with a Biodex Multi-Joint System 3 isokinetic dynamometer (Biodex Medical SystemInc., New York). Evaluations were preceded by a series of shoul-der warm-up exercises consisting of 15 free flexion–extension,adduction–abduction and circumduction movements that weresupervised by the principal investigator.14
For the instability and SLAP groups, the injured shoulder wastested. The arm evaluated in healthy athletes was paired with theinjured (dominant or non-dominant) arm of the matched injuredathlete. Athletes were assessed in the seated position, and trunkstabilization was provided by diagonal and pelvic straps. The evalu-ated arm was positioned with the shoulder abducted to 90◦ and theelbow flexed to 90◦. The olecranon was aligned over the machine’srotational axis. This 90–90◦ position was chosen because it chal-lenges the dynamic stabilization of shoulder.20
The isometric maximal and submaximal tests were performedbefore the isokinetic tests. The internal and external isometric rota-
h and torque steadiness in athletes with anterior shoulder instability3.10.246
tions were assessed with the shoulder positioned at 90◦ of externalrotation. For both rotation movement types, three 5 s maximal vol-untary isometric contractions were performed with a 1 min intervalbetween each contraction to determine the isometric peak torque.
ARTICLE IN PRESSG Model
JSAMS-955; No. of Pages 6
M.F. Saccol et al. / Journal of Science and Medicine in Sport xxx (2013) xxx– xxx 3
Table 1Age (years), injury and sports characteristics in athletes with instability or SLAP lesion.
Injured athletes Age Affectedside
Trauma/mechanism of injury Sport Type of sportand shoulderrisk
Level Cessation ofsports activity
Instability 1 20 D Traumatic contact in game Rugby With contact C YesInstability 2 19 D Traumatic fall during training Gymnastics With cocking C YesInstability 3 27 D Traumatic fall while biking Swimming With cocking C NoInstability 4 22 ND Traumatic fall during training Handball High risk P NoInstability 5 22 ND Traumatic blocked overhead throw Water polo High risk C NoInstability 6 21 D Traumatic blocked overhead throw Water polo High risk C YesInstability 7 20 D Traumatic fall during competition Judo With contact C YesInstability 8 20 D Traumatic fall during playing Rugby With contact C YesInstability 9 28 D Traumatic fall during soccer game Martial arts With contact R NoInstability 10 27 D Traumatic fall during soccer game Weight training With cocking R YesSLAP 1 28 D Traumatic type III, eccentric bench press Jiu-jitsu With contact P NoSLAP 2 31 ND Traumatic type II, fall on outstretched hand Jiu-jitsu With contact C NoSLAP 3 27 D Atraumatic type II, repetitive overhead motion Handball High risk C YesSLAP 4 36 D Traumatic type III, fall with locked arm Jiu-jitsu With contact C NoSLAP 5 27 D Atraumatic type II, repetitive overhead motion Baseball With cocking C NoSLAP 6 21 D Atraumatic type II, repetitive overhead motion Baseball With cocking C NoSLAP 7 19 D Atraumatic type II, repetitive overhead motion Swimming With cocking C NoSLAP 8 26 D Traumatic type II, overstretch with adduction Circus With cocking P No
sh
head m
P
Fpltkffe
fgahtoftontap
sMtclaod
mrttTl
ddt
SLAP 9 29 D Traumatic type IV, motorcycle craSLAP 10 25 D Atraumatic type II, repetitive over
, professional; C, competitive; R, recreational; D, dominant; ND, non-dominant.
or torque steadiness assessment, 35% of the maximal isometriceak torque value (target torque) was displayed as a horizontal
ine on the computer screen.14 The participants were instructedo maintain the exerted torque line at the target torque line andeep it there as steadily as possible for 10 s while receiving visualeedback.14 After one familiarization trial, the participants per-ormed five trials for each movement with a 1 min rest betweenach trial.
Isokinetic evaluations were performed in a 90◦ range of motion,rom neutral rotation to 90◦ of external rotation. Correction forravity was performed with the arm relaxed in 90◦ of shoulderbduction and neutral rotation since this position generates theighest rotation moment. The tests were performed in the concen-ric mode at the angular velocities of 90◦/s and 180◦/s in ascendingrder. After the procedures were explained, the participants per-ormed three submaximal repetitions at each test velocity in ordero familiarize themselves with the equipment and conditions. Afterne minute of rest, five maximal reciprocal repetitions of exter-al and internal shoulder rotations were performed, during whichhe participants received standardized verbal encouragement tochieve maximum strength in each contraction. A two-minute resteriod was allowed between test velocities.
Data from the isokinetic dynamometer were collected with aampling frequency of 100 Hz and then exported and reduced usingatLab® software (version 7.0.1, MathWorks Inc., Natick, USA). For
he submaximal isometric tests, the standard deviation (SD) andoefficient of variation (CV = SD/mean torque × 100) were calcu-ated for the torque steadiness variables. The SD of torque is anbsolute measure of amplitude while the CV of torque is a measuref relative fluctuation. The first two seconds of contraction wereiscarded to avoid the initial and adjustment phases.
The calculated isokinetic variables were peak torque to bodyass (N m kg−1 100) and shoulder external-to-internal rotation
atio (ER/IR ratio, %). Isokinetic peak torque was determined fromhe range in which the target velocity was constant. Isokinetic peakorque was determined and normalized by individual body mass.he external-to-internal rotator peak torque ratio was then calcu-ated for each angular velocity.
Please cite this article in press as: Saccol MF, et al. Shoulder rotator strengtor SLAP lesion. J Sci Med Sport (2013), http://dx.doi.org/10.1016/j.jsams.201
The statistical analyses were carried out with SPSS 13.0 for Win-ows. Considering that the majority of variables were not normallyistributed according to the Shapiro–Wilk test, non-parametricests were used for the analysis. The variables were tested between
Soccer With contact R Nootion Baseball With cocking C No
the instability and control groups for shoulder instability andbetween the SLAP and control groups for SLAP lesion using theMann–Whitney test. Furthermore, a Chi-square test was performedto compare the frequencies of ER/IR ratio imbalance between theinjured groups and their respective control groups. The significancelevel was set at ̨ ≤ 0.05.
3. Results
No differences were found between injured athletes and theirmatched controls regarding age, height or weight (p > 0.05).
For isometric shoulder torque steadiness, the only observeddifference was that the SLAP group presented impaired internalshoulder rotation force steadiness (i.e., higher CV force) comparedwith the corresponding control group (Table 2).
For the isokinetic evaluations, the instability group presenteda lower peak torque than the corresponding control group for allconditions (Table 2). No differences were found for ER/IR ratio.
4. Discussion
This study showed that athletes with anterior shoulder instabil-ity present deficits in shoulder rotator strength, while athletes witha SLAP lesion have decreased internal rotation strength control.Although abnormalities in rotator cuff performance are expecteddue to the complexity of these injuries,4,8 little information aboutthis issue can be found in the literature.
Although the purpose of nonoperative treatment for instabilitylesions is frequently to restore deficits in strength and sensor-imotor control,5 previous studies are not conclusive about theseinsufficiencies. Warner et al.10 evaluated a group of non-athleteswith both micro- and macrotraumatic instability and found no sig-nificant alterations compared to healthy subjects, while Edouardet al.11 found reduced internal and external rotator strength inrecurrent anterior shoulder instability. Although these studies eval-uated non-athletes, our results agree with Edouard et al.,11 whichdemonstrates the need for shoulder rotator strength training in
h and torque steadiness in athletes with anterior shoulder instability3.10.246
athletes with shoulder instability. Even before surgery, improvingrotator cuff strength is a demanding task,5 considering that shoul-der rotator weakness is still present in athletes after surgical repairand compromises sports training and activities of daily living.4

ARTICLE IN PRESSG Model
JSAMS-955; No. of Pages 6
4 M.F. Saccol et al. / Journal of Science and Medicine in Sport xxx (2013) xxx– xxx
Table 2Results of maximal and submaximal shoulder rotator strength test in athletes with anterior shoulder instability and SLAP lesion compared with their paired controls. Dataare presented as median (minimum–maximum).
Instability group(n = 10)
Instability controlgroup (n = 10)
p value SLAP group(n = 10)
SLAP controlgroup (n = 10)
p value
Isometric peak torque (Nm)External rotation 23.5 (19–47) 29.5 (23–43) 0.353 28.5 (14–39) 26 (16–35) 0.436Internal rotation 41.5 (26–78) 41.5 (30–70) 0.579 35 (24–70) 37 (19–63) 0.684
Standard deviationExternal rotation 0.36 (0.16–0.68) 0.39 (0.22–0.59) 0.739 0.43 (0.2–1.05) 0.36 (0.23–0.43) 0.190Internal rotation 0.51 (0.24–0.95) 0.59 (0.38–1.71) 0.393 0.54 (0.35–1.18) 0.48 (0.28–1.17) 0.113
Coefficient of variation (%)External rotation 4.07 (2.28–7.56) 3.89 (2.26–5.77) 0.631 4.62 (3.36–8.55) 4.22 (2.16–5.73) 0.393Internal rotation 3.55 (2.06–5.05) 4.48 (3.0–7.05) 0.529 4.61 (2.94–8.43) 3.72 (2.33–6.45) 0.003
Peak torque to body weight at 90◦/s (Nm kg−1 100)External rotation 39.5 (17.5–55.1) 53.8 (41.1–58.4) 0.007 45.9 (28.7–66.1) 46.7 (33.6–58.6) 0.853Internal rotation 50.6 (29.3–74.4) 67.3 (49.2–81.9) 0.043 62.8 (38.5–79.4) 50.5 (40.4–62.5) 0.089External rotation to internal rotation ratio 0.77 (0.47–1.10) 0.79 (0.67–0.92) 0.971 0.80 (0.43–1.1) 0.95 (0.72–1.08) 0.247% of ER/IR ratio imbalancea 70 70 0.639 80 90 0.531
Peak torque to body weight at 180◦/s (Nm kg−1 100)External rotation 38.4 (29.8–55.6) 50 (36.6–62.8) 0.009 45.3 (26.6–57.4) 43.8 (33.3–55.5) 0.579Internal rotation 44.2 (37.1–72.4) 67.5 (45–84.4) 0.019 57.9 (30.5–86.7) 46.8 (35.1–59.1) 0.063External rotation to internal rotation ratio 0.79 (0.61–0.98) 0.76 (0.6–0.94) 0.529 0.78 (0.6–1.0) 0.91 (0.76–1.04) 0.052% of ER/IR ratio imbalancea 90 70 0.121 70 100 0.060
pwapdwsiwmi(iitCpt
atsapastsSfascd
wTtt
a Considering the adequate ratio between 66% and 75%.20
Despite the fact that athletes with anterior shoulder instabilityresented deficits in maximal isokinetic strength, no alterationsere found in their torque steadiness pattern. Some studies evalu-
ting passive joint repositioning and kinesthesia have reported thatatients with anterior shoulder instability present proprioceptioneficits.21,22 Recently, Hung and Darling23 found that individualsith anterior shoulder dislocation did not exhibit joint position
ense deficits in active repositioning but had greater errors dur-ng passive repositioning. The authors suggested that individuals
ith unstable shoulders may be able to exert proper shoulderuscle activation to stabilize the glenohumeral joint when mov-
ng into vulnerable positions such as the one used in our studyabduction and external rotation). Since the torque steadiness tests considered an integrated sensory-motor control evaluation,13 its possible that our volunteers presented deficits in propriocep-ion, but active stabilizers compensated for them during the test.omplementary proprioceptive evaluation for kinesthesia and jointosition sense could have contributed to the sensory-motor controlest results in our study.
Regarding the SLAP lesion, studies evaluating muscle strengthnd control are scarce, we were able to find only two retrospec-ive studies. Pillai et al.12 evaluated external rotation strength afterurgical repair in patients with isolated SLAP lesions compared to
group with SLAP and spinoglenoid cyst. Ellenbecker et al.7 com-ared shoulder strength between injured and uninjured sides afterrthroscopic superior labrum repair and found a small (10% or less)trength deficit in internal and external rotators. If we consider thathe SLAP lesion is a fairly recent diagnosis that is mainly treated byugery,6,8 planning intervention strategies relies on determiningLAP lesion deficiencies compared to healthy controls. Our studyound that the SLAP group did not present maximal strength alter-tions compared with a matched healthy control group. We canpeculate that, although SLAP lesions lead to sports limitations andomplaints, they do not decrease strength in the way that instabilityoes.
However, in submaximal strength control test, the athletes
Please cite this article in press as: Saccol MF, et al. Shoulder rotator strengtor SLAP lesion. J Sci Med Sport (2013), http://dx.doi.org/10.1016/j.jsams.201
ith SLAP lesions showed decreased internal rotator steadiness.his increase in torque fluctuation could influence their capacityo achieve the desired force or produce the intended limb trajec-ory since it could reduce their ability to apply precise force.24
Previous studies have also found neuromuscular alterations ininternalrotator muscles among asymptomatic overhead athletes14
and athletes with shoulder pain.25 Internal rotator musclesare fundamental for dynamic shoulder stability and joint pro-tection mechanisms, improving the passive barrier to anteriortranslation25 and assisting with centering in humeral headmotion.15 Our results reinforce the importance of internal rotatormuscles for shoulder joint support as well as their impairment inshoulder injuries.
This is the first study to evaluate torque steadiness in athleteswith a SLAP lesion. A previous study found that healthy athletespresent higher fluctuation in internal rotation torque than non-athletes, which was considered an adaptation to sports activity thatcould have helped prevent shoulder injuries.14 Although highervariability can be considered a positive factor in overuse preven-tion, excessive variability can be considered pathological.26 Sinceinjured athletes were compared with matched controls who canbe considered to represent the normal pattern for their respectivesports, we believe that an increase in torque fluctuation in this casecan be considered harmful.
Despite impairment of internal rotator muscle control, most ofthe SLAP athletes maintained a regular training regimen, unlike theathletes with anterior instability. Considering that the stability ofthe labrum is increased by muscle activity and capsuloligamen-tous integrity,27 their continued shoulder rotator strength allowedthe athletes with SLAP to continue training. In athletes with ante-rior shoulder instability, it is possible that the inherent loss ofcapsuloligamentous stability limited their participation in sports.However, whether the shoulder rotator weakness observed in theseathletes is a cause or a consequence of such instability11 or evenresultant from decreased sports participation remains unclear. Ourfindings demonstrate that these injury types may cause differentimpairments in sports activity.
There were no differences in the ER/IR strength ratio betweenthe injured and control groups. The ER/IR ratio has been widely
h and torque steadiness in athletes with anterior shoulder instability3.10.246
reported in shoulder strength profiles and is considered a predictorof shoulder injuries.10,11,28 The proportion of athletes with ER/IRratio imbalance was also similar between the injured and controlgroup. Therefore, despite the high intra-group variability, our study

ING Model
J
and M
riiti
csandn
Wotoaalbiit
isiiilc
vaataeatsil
5
SaWda
P
•
•
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
ARTICLESAMS-955; No. of Pages 6
M.F. Saccol et al. / Journal of Science
einforces that this variable alone should not represent shouldernjury risk. We suggest that it can be altered by other factors besidesnjury. This is also supported by a recent study29 that demonstratedhe necessity of more than one isokinetic parameter to indicate anncrease in injury risk.
Previous studies have compared the injured shoulder with theontralateral one, despite the use of a control group.10,11 Side-to-ide differences may be present independent of shoulder injury,s has been shown in healthy athletes between the dominant andondominant arm.28 Since the present study included athletes fromifferent types of sports, each one with a different overload on theondominant side, the contralateral was not used for comparisons
There are some limitations to this study that should be noted.e should be careful in generalizing the results for all severities
f shoulder instability, considering that only athletes able to con-rol the shoulder in abduction and external rotation without painr apprehension were included in this study. Since most sublux-tions and dislocations occur in this position, we had to excludethletes with more severe instability (more than 10 episodes) andimited external rotation motion. Even though it limited the num-er of subjects in our injured groups, we chose this position since
t challenges the dynamic stabilization of shoulder muscles20 and,n this position, subscapularis, infraspinatus and the long head ofhe biceps tendon contract to stabilize the glenohumeral joint.30
Additionally, these results are limited to athletes with instabil-ty or SLAP lesion that present symptoms and, finally, the smallample size should be emphasized as a limitation. Further stud-es are necessary to investigate these patterns in asymptomaticnjured athletes. Additionally, although we used validated clin-cal examination tests and imaging studies for diagnosing SLAPesions, arthroscopy remains the definitive means of diagnosis andharacterization.8
Finally, this study has some clinical implications for the conser-ative treatment of the shoulders of athletes. Our results show thatnterior shoulder instability and SLAP lesion are related to differentlterations in shoulder rotator strength and control. Consideringhat shoulder rotator weakness was more apparent in athletes withnterior instability, external and internal rotator strengtheningxercises should be prominent in their treatment. For athletes with
SLAP lesion, rehabilitation should focus on functional exerciseshat require internal rotation force control. These results demon-trate that specific shoulder muscle adaptations are related to eachnjury type and should be considered in the rehabilitation of ath-etes.
. Conclusion
In conclusion, athletes with anterior shoulder instability andLAP lesions presented different impairments regarding strengthnd sensory motor control compared to matched healthy athletes.hile athletes with anterior shoulder instability demonstrated
eficits in shoulder rotation strength, athletes with SLAP presentedltered shoulder internal rotation force control.
ractical implications
Although current practice for treating anterior instability andSLAP lesions is similar regarding improvement in the dynamicstability of the rotator cuff, these lesions present different musclestrength and force control patterns.Anterior shoulder instability involves an overall deficit in rotator
Please cite this article in press as: Saccol MF, et al. Shoulder rotator strengtor SLAP lesion. J Sci Med Sport (2013), http://dx.doi.org/10.1016/j.jsams.201
cuff strength without alterations in submaximal force control.This finding reinforces the need for internal and external rotatorresistance strength training as a principal component of conser-vative treatment.
2
PRESSedicine in Sport xxx (2013) xxx– xxx 5
• SLAP lesion results included internal rotation force control alter-ations without strength deficits compared to matched controls.This indicates a reduced ability to apply precise force and com-promises sports performance. Physical therapy for such athletesshould focus on functional exercises involving strength control.
Acknowledgments
The authors gratefully acknowledge the research fellow-ships from São Paulo Research Foundation (FAPESP), grants#2008/02076-6 and #2009/05219-5.
References
1. Hudson VJ. Evaluation, diagnosis, and treatment of shoulder injuries in athletes.Clin Sports Med 2010; 29(1):19–32.
2. Borsa PA, Laudner KG, Sauers EL. Mobility and stability adaptations in the shoul-der of the overhead athlete: a theoretical and evidence-based perspective. SportsMed 2008; 38(1):17–36.
3. Myers JB, Lephart SM. Sensorimotor deficits contributing to glenohumeral insta-bility. Clin Orthop Relat Res 2002; 400:98–104.
4. Meller R, Krettek C, Gosling T et al. Recurrent shoulder instability among ath-letes: changes in quality of life, sports activity, and muscle function followingopen repair. Knee Surg Sports Traumatol Arthrosc 2007; 15(3):295–304.
5. Bak K, Wiesler ER, Poehling GG. Consensus statement on shoulder instability.Arthroscopy 2010; 26(2):249–255.
6. Gorantla K, Gill C, Wright RW. The outcome of type II SLAP repair: a systematicreview. Arthroscopy 2010; 26(4):537–545.
7. 7.Ellenbecker TS, Sueyoshi T, Winters M et al. Descriptive report of shoulderrange of motion and rotational strength six and 12 weeks following arthroscopicsuperior labral repair. N Am J Sports Phys Ther 2008; 3(2):95–106.
8. Edwards SL, Lee JA, Bell JE et al. Nonoperative treatment of superior labrumanterior posterior tears: improvements in pain, function, and quality of life. AmJ Sports Med 2010; 38(7):1456–1461.
9. Castagna A, Delle Rose G, Borroni M et al. Arthroscopic stabilization of theshoulder in adolescent athletes participating in overhead or contact sports.Arthroscopy 2012; 28(3):309–315.
0. Warner JJ, Micheli LJ, Arslanian LE et al. Patterns of flexibility, laxity, and strengthin normal shoulders and shoulders with instability and impingement. Am J SportsMed 1990; 18(4):366–375.
1. Edouard P, Degache F, Beguin L et al. Rotator cuff strength in recurrent anteriorshoulder instability. J Bone Joint Surg Am 2011; 93(8):759–765.
2. Pillai G, Baynes JR, Gladstone J et al. Greater strength increase with cyst decom-pression and SLAP repair than SLAP repair alone. Clin Orthop Relat Res 2011;469(4):1056–1060.
3. Bandholm T, Rasmussen L, Aagaard P et al. Force steadiness, muscle activity, andmaximal muscle strength in subjects with subacromial impingement syndrome.Muscle Nerve 2006; 34(5):631–639.
4. Zanca GG, Saccol MF, Oliveira AB et al. Shoulder internal and external rota-tions torque steadiness in overhead athletes with and without impingementsymptoms. J Sci Med Sport 2013; 16(5):433–437.
5. Myers JB, Wassinger CA, Lephart SM. Sensorimotor contribution to shoulderstability: effect of injury and rehabilitation. Man Ther 2006; 11(3):197–201.
6. Dodson CC, Altchek DW. SLAP lesions: an update on recognition and treatment.J Orthop Sports Phys Ther 2009; 39(2):71–80.
7. Kirkely A, Werstine R, Ratjek A et al. Prospective randomized clinical trialcomparing the effectiveness of immediate arthroscopic stabilization versusimmobilization and rehabilitation in first traumatic anterior dislocations of theshoulder. Arthroscopy 2005; 21(1):55–63.
8. Burns TC, Owens BD. Management of shoulder instability in in-season athletes.Phys Sportsmed 2010; 38(3):55–60.
9. Walch G. Directions for the use of the quotation of anterior instabilities of theshoulder, Abstracts of the First Open Congress of the European Society of Surgery ofthe Shoulder and Elbow, Paris, 1987, p. 51–55.
0. Glousman R, Jobe F, Tibone J et al. Dynamic electromyographic analysis of thethrowing shoulder with glenohumeral instability. J Bone Joint Surg Am 1988;70(2):220–226.
1. Lephart SM, Warner JJ, Borsa PA et al. Proprioception of the shoulder joint inhealthy, unstable, and surgically repaired shoulders. J Shoulder Elbow Surg 1994;3(6):371–380.
2. Zuckerman JD, Gallagher MA, Cuomo F et al. The effect of instability and subse-quent anterior shoulder repair on proprioceptive ability. J Shoulder Elbow Surg2003; 12(2):105–109.
3. Hung YJ, Darling WG. Shoulder position sense during passive matching andactive positioning tasks in individuals with anterior shoulder instability. PhysTher 2012; 92(4):563–573.
4. Enoka RM, Christou EA, Hunter SK et al. Mechanisms that contribute to dif-
h and torque steadiness in athletes with anterior shoulder instability3.10.246
ferences in motor performance between young and old adults. J ElectromyogrKinesiol 2003; 13(1):1–12.
5. Hess SA, Richardson C, Darnell R et al. Timing of rotator cuff activation duringshoulder external rotation in throwers with and without symptoms of pain. JOrthop Sports Phys Ther 2005; 35(12):812–820.

ING Model
J
6 and M
2
2
2
29. Edouard P, Degache F, Oullion R et al. Shoulder strength imbalances as injuryrisk in handball. Int J Sports Med 2013; 34(7):654–660.
ARTICLESAMS-955; No. of Pages 6
M.F. Saccol et al. / Journal of Science
6. Harbourne RT, Stergiou N. Movement variability and the use of nonlinear tools:principles to guide physical therapist practice. Phys Ther 2009; 89(3):267–282.
Please cite this article in press as: Saccol MF, et al. Shoulder rotator strengtor SLAP lesion. J Sci Med Sport (2013), http://dx.doi.org/10.1016/j.jsams.201
7. Lippitt SB, Vanderhooft JE, Harris SL et al. Glenohumeral stability from concavity-compression: a quantitative analysis. J Shoulder Elbow Surg 1993; 2(1):27–34.
8. Ellenbecker TS, Davies GJ. The application of isokinetics in testing and rehabili-tation of the shoulder complex. J Athl Train 2000; 35(3):338–350.
3
PRESSedicine in Sport xxx (2013) xxx– xxx
h and torque steadiness in athletes with anterior shoulder instability3.10.246
0. Kuhn JE, Huston LJ, Soslowsky LJ et al. External rotation of the glenohumeraljoint: ligament restraints and muscle effects in the neutral and abducted pos-itions. J Shoulder Elbow Surg 2005; 14:39S–48S.
Related Documents











