Shoulder Injuries By: Nathaniel Patterson Clavicle

Shoulder Injuries By: Nathaniel Patterson Clavicle.
Dec 27, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Shoulder Injuries
By: Nathaniel Patterson
Clavicle
Anatomy Of the Shoulder
• There are Three Main Bones in the Shoulder– The Clavicle– The Scapula– Humoreus

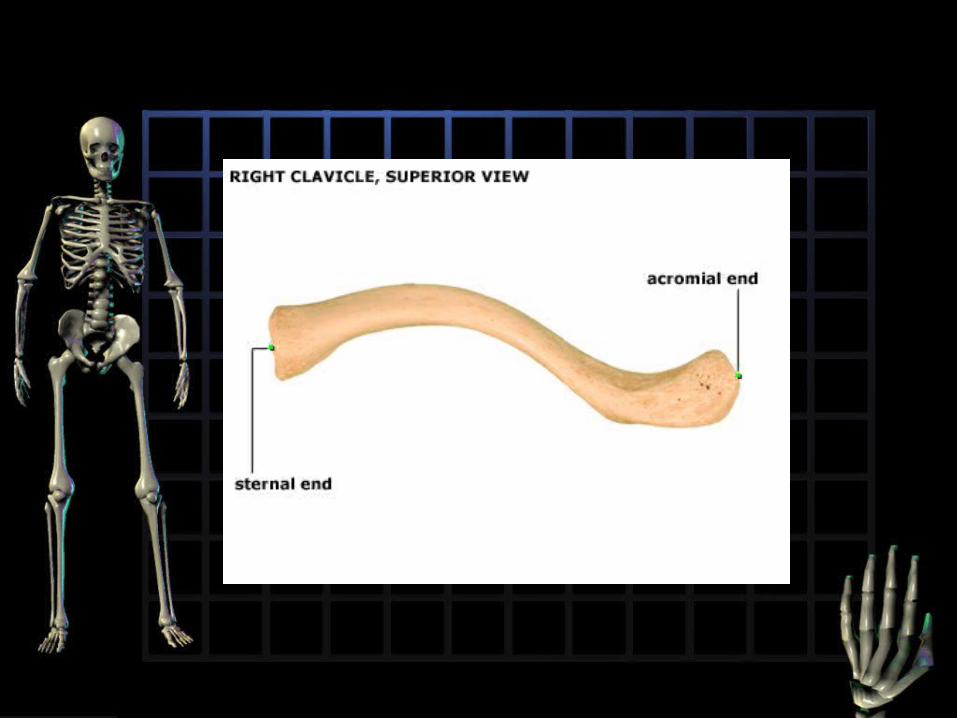
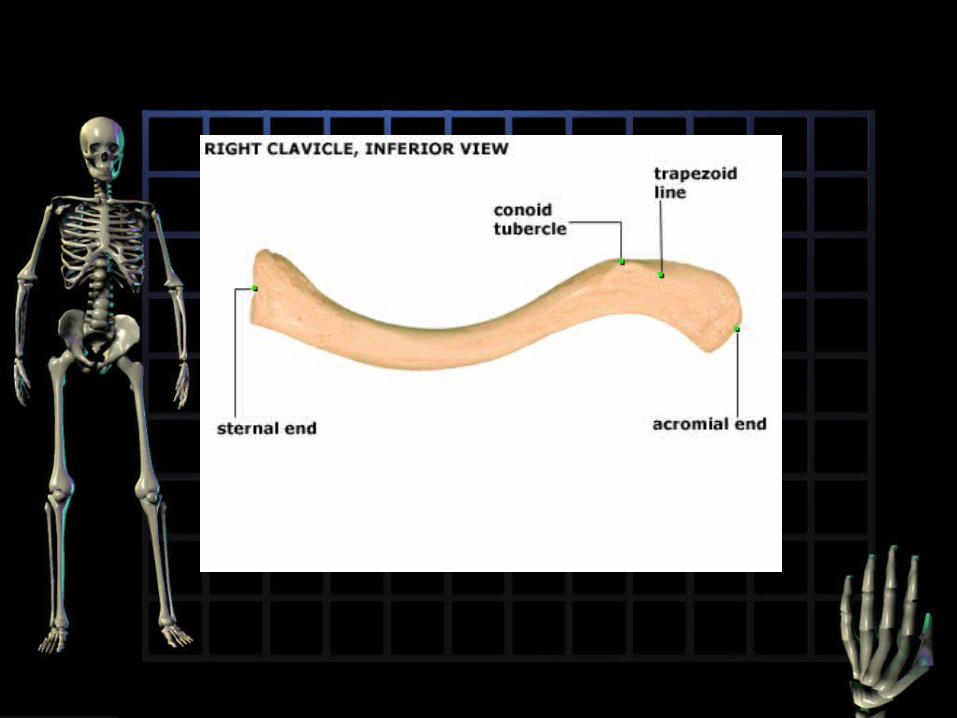
The Clavicle
• The clavicle is an S-shaped bone that attaches the trunk to the upper extremity (the only bone to do so through bony articulations).

The Scapula
• The Scapula (Shoulder Blade)– The Scapula forms the posterior part of the
shoulder girdle.


The Humerus
• The Humerus is the bone that connects to the lower arm, and to the shoulder.

Muscles
• The Rotator Cuff– The rotator cuff is a set of four muscles that
are responsible for the movement of the arm and gives the shoulder stability.
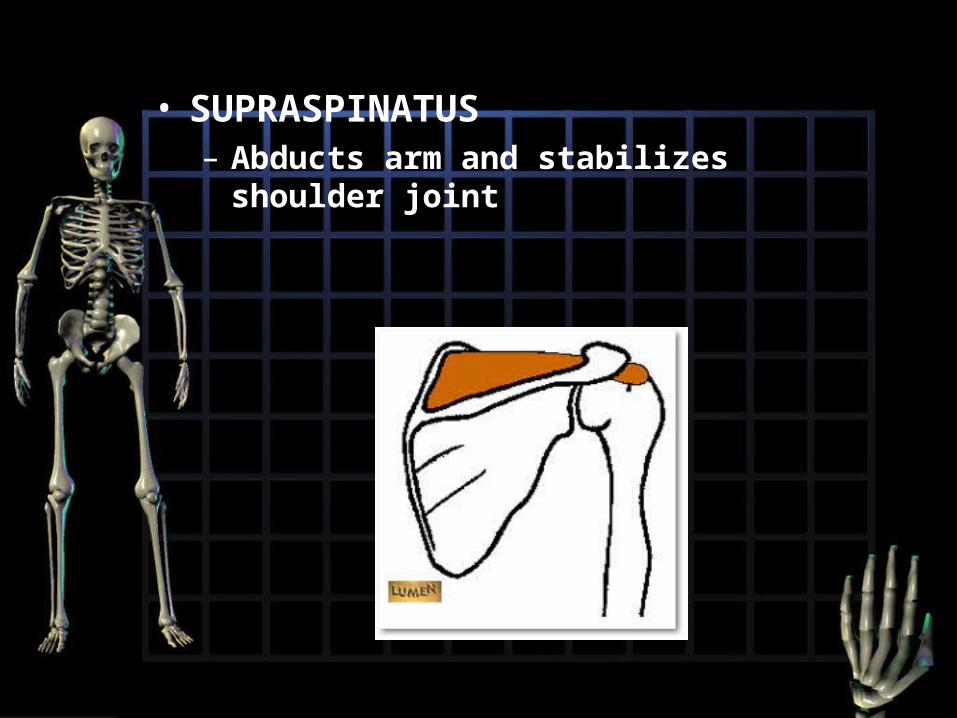
• SUPRASPINATUS– Abducts arm and stabilizes shoulder
joint
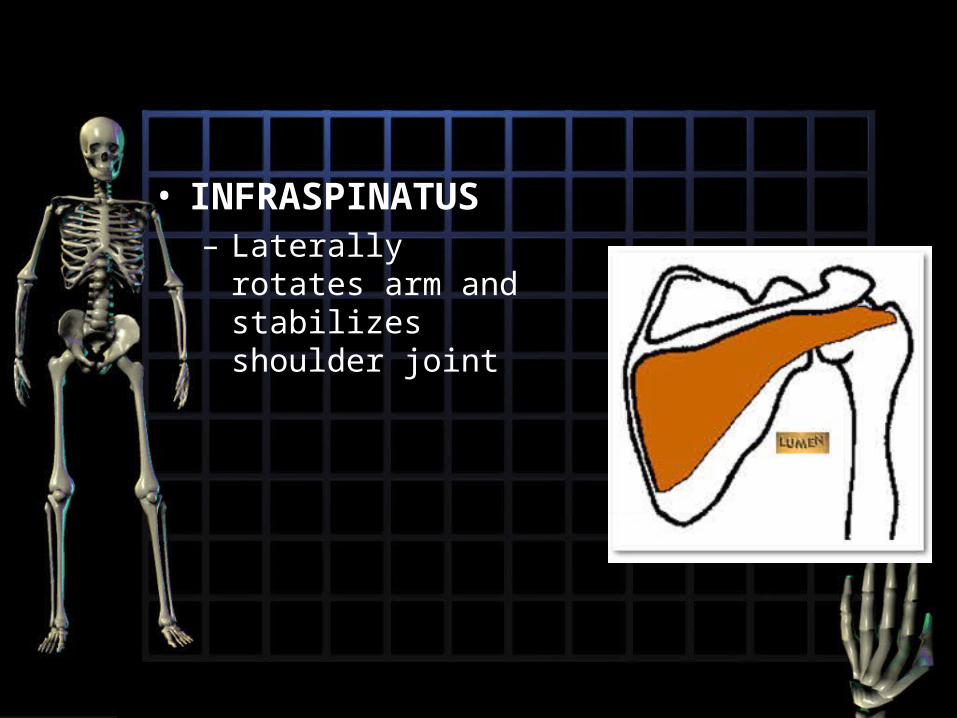
• INFRASPINATUS– Laterally rotates arm
and stabilizes shoulder joint
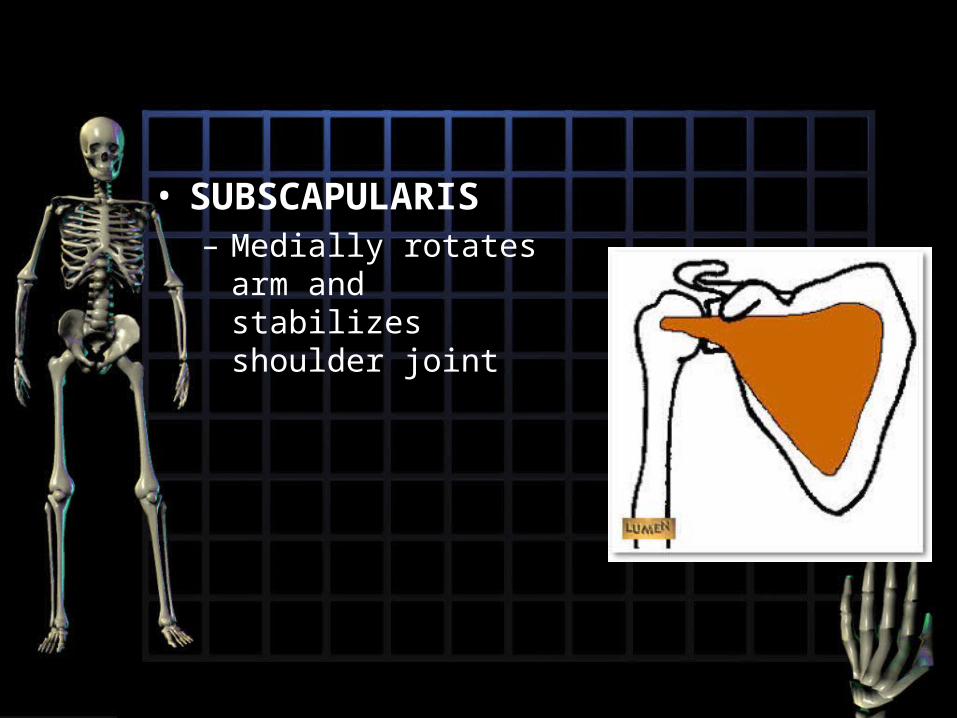
• SUBSCAPULARIS– Medially rotates arm
and stabilizes shoulder joint

• TERES MINOR– laterally rotates arm
and stabilizes shoulder joint
Deltoid and Teres Major
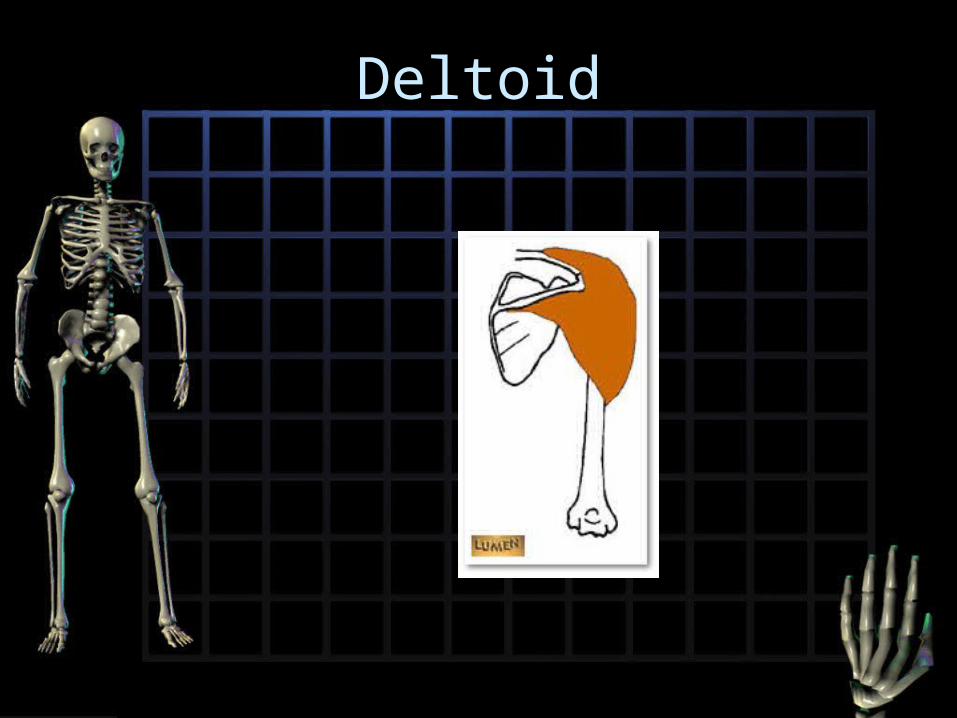
• Deltoid– Abducts arm, anterior fibers flex and medial
rotate, posterior fibers extend and lateral rotate
• Teres Major– Medially rotates and adducts arm. Stabilizes
shoulder joint
Deltoid

Teres Major

Ligaments
• the acromioclavicular ligament is superior to the joint and links the lateral end of the clavicle and the acromion.
• the coracoclavicular ligament, a stronger ligament, does not attach to the acromion, but rather attaches the clavicle to the scapula at the coracoid process. – the conoid ligament lies medially. It spans from
the conoid tubercle of the clavicle to the coracoid process.
– the trapezoid ligament is the lateral portion of the ligament. It spans from the trapezoid line on the clavicle to the coracoid process.
Bursae
• Bursae reduce friction in areas where tendons (or skin) slide across bones, ligaments or other tendons.

Dislocated Shoulder
• There are 2 types of dislocations – A partial dislocation (subluxation) means the
head humerus is partially out of the socket (glenoid).
– A complete dislocation means it's all the way out.

• Both partial and complete dislocation cause pain and unsteadiness in your shoulder. Your muscles may have spasms from the disruption, and this can make it hurt more. When your shoulder dislocates time and again, you have shoulder instability

Signs and Symptoms
• swelling
• numbness
• weakness
• Bruising
• Sometimes dislocation may tear ligaments or tendons in your shoulder. Once in awhile, the dislocation may damage your nerves.
Treatment
• A Doctor or trained Professional will place the ball of the humerus back in the socket.
Rehab
• Immobilization
• A sling
• Ice
• If it happens consistently the doctor might prescribe a brace, sometimes surgery is needed to correct the problem

Rotator cuff tear
• Are a common source of shoulder pain.
• Damage increases with age.

Surgical and Non Surgical Options
• Non-operative (conservative) treatment
• Operative - Rotator cuff repair • Open • Mini-open • All-arthroscopic

Non-Operative
• Injections – Injecting medicines to help strengthen
the area.
• Activity modification (avoidance of activities that cause symptoms)

• Advantages• Patient avoids surgery and its inherent
risks: • Infection • Permanent stiffness • Anesthesia complications
• Disadvantages • Strength does not improve • Tears may increase in size over time • Patient may need to decrease activity
level

Operative
• The 3 Main Types • Open repair • Mini-open repair • All-arthroscopic repair
• After rotator cuff repair, 80 percent to 95 percent of patients achieve a satisfactory result, defined as adequate pain relief, restoration or improvement of function, improvement in range of motion

Potential Complications
• Nerve injury (1 percent to 2 percent)
• Infection (1 percent):
• Deltoid Detachment (less than 1 percent):
• Stiffness (less than 1 percent):
• Tendon re-tear (6 percent
Rehab.
• Following rotator cuff surgery, therapy progresses in stages. Passive range of motion exercises are begun with a therapist; pendulum exercises may be taught as well. Progressive strengthening and range of motion exercises continue during the next 6 to 12 weeks. Most patients have a functional range of motion and adequate strength by 4 to 6 months after surgery.
Related Documents











