Shoulder and Shoulder and Knee Injury: Knee Injury: Treatment and Treatment and Prevention Prevention Samir Sharma MD Board Certified Fellowship Trained Sports Medicine Head Team Physician San Jose Sabercats

Shoulder and Knee Injury: Treatment and Prevention Samir Sharma MD Board Certified Fellowship Trained Sports Medicine Head Team Physician San Jose Sabercats.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Shoulder and Knee Shoulder and Knee Injury: Treatment Injury: Treatment and Preventionand Prevention
Samir Sharma MD Board CertifiedFellowship Trained Sports MedicineHead Team Physician San Jose Sabercats

Shoulder InjuriesShoulder Injuries

AnatomyAnatomy
The shoulder has the greatest degree of movement of any joint in the body
It is a multiaxial ball and socket joint

AnatomyAnatomy
The Rotator Cuff is a set of four muscles that surround the humeral head.
They function to help abduct and rotate the arm and also function as dynamic stabilizers of the joint.
Instability, Impingement & DJDInstability, Impingement & DJD
Think of all soft tissue shoulder disorders tofall in three broad categories:
1) Instability2) Impingement3) DJD
The Age of the patient generally places them in each of these categories

Shoulder InstabilityShoulder Instability
Mostly cccurs in younger patients <30 years of age
The extreme form of this is a shoulder dislocation
Can cause secondary tendonitis and labrum and cartilage tears
Anterior instability is the most common 95 %
Usually occurs when the patient raises their arm overhead in a throwing position
Subluxation vs Dislocation Dislocation has to be reduced

Shoulder InstabilityShoulder Instability
History, the patient is “apprehensive” about putting their arm overhead
History of previous anterior dislocations
Physical Exam positive apprehension test improved when posterior pressure is applied over the anterior aspect of the shoulder

Apprehension SignApprehension Sign

Shoulder DislocationShoulder Dislocation

Shoulder Instability < 20 Shoulder Instability < 20 YearsYears
For dislocators < 20 years old there is a 90% chance of redislocation. As one ages the chance of redislocation lessens
In this high risk group, surgical repair and capsular tightening is recommended
Arthroscopic techniques have advanced significantly over the past several years

Shoulder Instability > 30 YearsShoulder Instability > 30 Years
Anterior Dislocations for first time dislocators over the age of 30, a trial of physical therapy followed by reevaluation
After a course of PT, On PE if the pt still has a positive apprehension sign this is an indicator that the capsule is stretched and the IGHL complex is not functioning properly

Shoulder Instability > 50 YearsShoulder Instability > 50 Years
In patients older than 50 who have a dislocation, concomitant rotator cuff tear at the time of injury needs to be ruled out
If there is a small tear, a trial of therapy can still be initiated to regain motion and strengthen the periscapular muscles
In older patients >65 with a dislocation surgery is usually not necessary and the treatment is physical therapy with rehab
ImpingementImpingement
Overuse type injuries which occur in the middle aged 40-60 individual
As the arm is abducted the rotator cuff tendons and biceps tendon abut (impinge) against the acromion causing inflammation in the bursa and wear of the RTC tendon
As this happens thousands of times the rotator cuff starts to fray and tear

ImpingementImpingement

Rotator Cuff TendonitisRotator Cuff Tendonitis
Gradual onset of pain along anterolateral shoulder
Difficulty sleeping on the affected side
May be preceded by an antecedent trauma
Patients complain of difficulty with overhead lifting

Rotator Cuff TendonitisRotator Cuff Tendonitis
Physical exam may include a painful arc from 60-120 degrees of abduction
Weakness on supraspinatus muscle strength testing
Positive impingement tests

Painful Arc Associated with Painful Arc Associated with ImpingementImpingement
Rotator Cuff TendonitisRotator Cuff Tendonitis
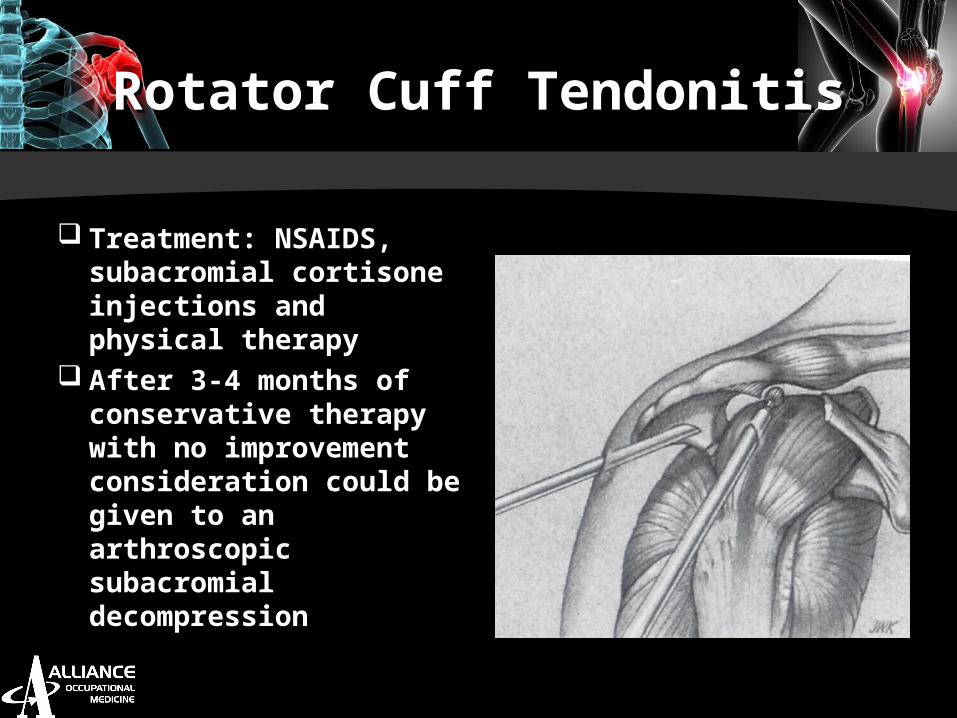
Treatment: NSAIDS, subacromial cortisone injections and physical therapy
After 3-4 months of conservative therapy with no improvement consideration could be given to an arthroscopic subacromial decompression

Rotator Cuff TendonitisRotator Cuff Tendonitis
Arthroscopic Subacromial Decompression involves removal of any subacromial bone spurs, inflamed subacromial bursa, and direct assessment of the status of the rotator cuff and glenohumeral joint
Open subacromial decompression achieves the same purpose however the deltoid muscle is detached and reattached and a larger incision is involved

Rotator Cuff TearRotator Cuff Tear
History is similar to RTC tendonitis Physical exam may show increased
supraspinatus weakness and atrophy of the supraspinatus fossa
MRI is the study of choice Arthrogram is also a good study to
just look at whether there is a tear in the rotator cuff

Rotator Cuff TearRotator Cuff Tear
Treatment- In a patient who is <50 years of age immediate referral to an orthopedist
Key point is that degenerative rotator cuff tears occur in patients greater than 50
years
A tear in a patient less than 50 years of age is a traumatic tear unless proven
otherwise

Rotator Cuff TearRotator Cuff Tear
Traumatic rotator cuff tears require operative fixation
Degenerative Rotator Cuff Tears treatment is controversial
May initiate physical therapy, NSAIDs and 1-2 cortisone injections
If no improvement consider surgical repair

Rotator Cuff TearRotator Cuff Tear

Rotator Cuff RepairRotator Cuff Repair

DJDDJD
Degenerative Joint Disease of the shoulder (Osteoarthritis)
Commonly occurs in older patients >60 years of age
History of stiffness and pain
Radiologic Diagnosis

Degenerative Shoulder Degenerative Shoulder DiseaseDisease
History Pain and Stiffness May be preceded by antecedent
trauma Physical Exam Marked loss of motion Diffuse muscle atrophy Crepitus on ROM

Degenerative Shoulder Degenerative Shoulder DiseaseDisease
Xray: Grashey Xray true AP xray of the shoulder shows loss of joint space and humeral osteophytes
Treatment Gentle ROM and Strengthening NSAIDS Intrarticular cortisone injection

Degenerative Shoulder Degenerative Shoulder DiseaseDisease

Degenerative Shoulder Degenerative Shoulder DiseaseDisease
Surgery is indicated when pain is not amenable to conservative management
Surgery include a hemiarthroplasty vs a Total Shoulder Replacement
Surgery can predictably relieve pain. Functional improvement is not as predictable

Case Study # 1
Pt. is a 57 yr old male seen for consultation in regards to rt. shoulder. Pt. injured rt. shoulder at work climbing in and out of truck using steering wheel to pull himself up & diagnosed w/rt. shoulder impingement syndrome with AC joint arthritis. Initial treatment of PT and NSAIDS, improving slower than expected. MRI conducted, showed moderate supraspinatus and infraspinatus tendinosis with a small-to-moderate sized interstitial tear and detachment of the tendons.
Treatment: Pt. underwent shoulder arthroscopy and debridement with distal clavicle resection. Pt. went back to full duty and was made MMI with 0% impairment. Future medical provided to include antiinflammatory medications and cortisone injectsion as needed for flare ups.

Case Study # 2
Pt. is a 53 yr old male who injured rt shoulder by a compactor smashing rt shoulder. Had severe rt shoulder pain and difficulty with use of arm. Started on ibuprofin 600 mg & Soma. MRI was performed and showed a supraspinatus complete tear with retraction & AC joint arthritis. Conservative treatment of PT and cortisone injection failed.
Treatment: Pt. underwent rt shoulder arthroscopy, rotator cuff tendon repair and resection. Patient returned to full duty., made MMI with no permanent restrictions and 0% impairment rating. Future medical to include antiinflammatory medications and cortisone injection as needed for flare ups.

Case Study #3
Pt. is a 42 yr old female injured lt shoulder while picking up towels. Also undergoing treatment for RMI for hand/wrist/forearm. Pt had difficulty with overhead use, use of her arm and difficulty sleeping at night. MRI was performed and showed anterior superior labrum signal with mild arthrosis of AC joint.
Treatment: Pt underwent lt shoulder cortisone injection and improved with ROM. Still has some residual lt shoulder pain. Made MMI with no permanent restrictions, 0 % whole body impairment and future medical to include follow up visits, antiinflammatory medications, and cortisone injections as needed for flare ups.

Case Study # 4
Pt. is 46 yr old plumber who injured rt shoulder by using too much force while using cordless drill. Complains of pain, reduced strength and ROM. STAT MRI requested which showed rotator cuff tear.
Treatment: right shoulder arthroscopy with subacromial decompression, debridement of labrum, and repair of the partial thickness articular surface tear. Pt fell 1 week after surgery, aggravated injury and delayed recovery. WCE completed which showed Pt will benefit from work hardening program. After completion, Pt was able to return to work full duty, range of motion increased significantly, and pain factors decreased to point where medication no longer needed. Pt extremely happy with outcome.

Shoulder Injury PreventionShoulder Injury Prevention
Lift items close to the body
Only lift items below shoulder level
When using a mouse keep in front of you at fingertip level so you do not have to reach with your arm outstretched
Take posture breaks when repetitively using the arm and shoulder
Shoulder Injury PreventionShoulder Injury Prevention
If performing a job which requires repetitive lifting, conditioning with rotator cuff strengthening exercises maybe beneficial
Stretch before performing lifting tasks
Take breaks to prevent muscle fatigue

Knee InjuriesKnee Injuries

AnatomyAnatomy
Think of the knee source of pain in 4 basic
areas.1. Medial (inner)2. Lateral (outer)3. Anterior (front)4. Posterior (back)

Medial Aspect of KneeMedial Aspect of Knee
Important Structures
1. MCL2. Medial
Meniscus3. Pes Anserine
tendons4. Medial Condyle
/ Medial Tibial Plateau

Lateral Aspect of KneeLateral Aspect of Knee
1) Lateral meniscus
2) ACL3) Lateral
Condyle/ Lateral Plateau
4) Iliotibial Band

Anterior & Posterior Aspects of KneeAnterior & Posterior Aspects of Knee

Anterior Knee PainAnterior Knee Pain
Patellar Chondromalacia Essentially softening and wear of the
patellar cartilage due to overuse or maltracking
Patients complain of pain while climbing stairs
MRI shows mild thinning of the cartilage Treatment is NSAIDS/ Cortisone injection
Anterior Knee PainAnterior Knee Pain
Patellofemoral Arthritis Diagnosed by decreased ROM with crepitus
on PE Lateral Xray shows diffuse narrowing of the
patellofemoral compartment with osteophytes Treatment - Cortisone Injection/
Viscosupplementation Injections Newer Trials of Isolated Patellofemoral
Replacement

Patellofemoral ArthiritisPatellofemoral Arthiritis

Medial Compartment PainMedial Compartment Pain
1. Degenerative meniscal tear2. Osteoarthritis3. Pes Anserine tendonitis4. MCL

Degenerative Meniscal Degenerative Meniscal TearsTears
Patients c/o of catching and locking
Degenerative tears can occur with minimal trauma
Complaints of knee giving way
Distinguish from bucket handle tear of the meniscus

Mcmurray ExamMcmurray Exam
Pt is supine with the knee flexed
The examiner internally and externally rotates the leg
A positive test is a snap or click felt along the joint line that is accompanied by pain

Types of Meniscus TearsTypes of Meniscus Tears

Bucket Handle Meniscus Bucket Handle Meniscus TearTear
Pt cannot achieve full extension
Moderate to large effusion in knee
There is a block to extension when passively trying to extend knee
Urgent referral

Degenerative Joint DiseaseDegenerative Joint Disease
Weight Bearing x-rays are crucial! They show the functional space in the
knee Always specify on the prescription to
obtain weight bearing x-rays Radiographically joint space
narrowing with osteophytes are classic Otherwise known as osteoarthritis

Degenerative Joint DiseaseDegenerative Joint Disease

Degenerative Joint DiseaseDegenerative Joint Disease
Patients c/o of catching and locking of the knee due to the friction caused by the rough surfaces rubbing against each other
History of stiffness
PE: May have effusion, decreased ROM and crepitus
TreatmentTreatment
Depends on amount of cartilage wear
If there is joint space narrowing on xray (greater than 1 cm) this correlates with a large amount of osteochondral wear
Consideration should be given for intrarticular cortisone injection
Also viscosupplementation is an option

Medial Collateral Ligament Medial Collateral Ligament TearTear
History of trauma Valgus force to knee Medial Joint tenderness Reproduction of pain with valgus
load to knee Test against opposite knee

Valgus Stress Test (MCL)Valgus Stress Test (MCL)

Radiologic Findings of MCL Radiologic Findings of MCL TearTear
Medial Collateral Ligament Medial Collateral Ligament TearTear
Treat with crutches and bracing for 4-6 weeks depending on severity of tear
Usually PT will help regain Post injury muscle strength and ROM

ACL TearACL Tear
Usually occurs with pivoting and twisting
Patients describe a “Pop” when injury occurs
Marked swelling with an effusion
Positive Lachman exam

Lachman Test (ACL test)Lachman Test (ACL test)
With the patient supine and the knee flexed approximately 30 degrees
Stabilize the proximal thigh and apply an anterior directed force on the tibia

ACL TearACL Tear
Initial treatment goal is to regain ROM of knee and decrease swelling
Knee is initially swollen
PT sessions to teach ROM and strengthening exercises is helpful

ACL TreatmentACL Treatment
Surgery reserved for active individuals or those with functional instability
Arthroscopic procedure
Different types of graft options

Case Study # 1Case Study # 1
Pt. is 68 year old male, injured left knee when he slipped and twisted his knee at work. Diagnosed with Arthrofibrosis, maceration of the meniscus, and left knee marked articular cartilage along weight bearing surface of medical compartment. Returned to work full duty, PT prescribed. Improving slower than expected. MRI ordered revealed medial meniscus maceration and tearing. Ortho consult requested.
Treatment: Left knee cortisone injection relieved pain. No permanent work restrictions, 0% impairment. Made MMI with future medical (antiinflammatory medications and cortisone injections) for flare ups.

Case Study # 2Case Study # 2
Pt. is 53 yr old male, injured rt. knee when he tripped over some tied wire. Had increased rt. knee pain, swelling, catching & locking. MRI performed which showed full thickness chondral defect along latereral patellar face ad intrasubstance degeneration of anterior and posterior horn of medical meniscus. Pt had continued rt. knee pain, difficulty weightbearing & use of rt. knee.
Treatment: Pt. underwent antiinflammatory medications and activity restriction. Reached maximum medical improvement and made MMI with no permanent work restrictions and 0% impairment. Given future medical to include antiinflammatory medication and cortisone injection as needed for future flare ups of knee.

Knee Injury PreventionKnee Injury Prevention
Every pound of weight is 4-6 pounds of force on the knee
Avoid activities in which the employee is bending or squatting for prolonged periods of time
Design the space so that the employee can work from a seated position instead of a kneeling one

Knee Injury PreventionKnee Injury Prevention
If you have to kneel for prolonged periods wear well designed knee pads
Well designed breaks to allow employees to relieve pressure on the knees and stretch
Important to prevent deconditioning with good quadriceps and hamstring strengthening exercises

Questions?Questions?
Thank you!Thank you!
Dr. Samir SharmaDr. Samir SharmaAlliance Occupational MedicineAlliance Occupational Medicine
2737 Walsh Ave. Santa Clara, CA.2737 Walsh Ave. Santa Clara, CA.315 S. Abbott Ave. Milpitas, CA.315 S. Abbott Ave. Milpitas, CA.
1901 Monterey Rd. Ste 10 San Jose, 1901 Monterey Rd. Ste 10 San Jose, CA.CA.
Related Documents











