SHOCK AND RESUSCITATION Hugh M. Foy, MD Harborview Medical Center University of Washington

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
SHOCK AND RESUSCITATION
Hugh M. Foy, MD
Harborview Medical Center
University of Washington

Shock and Resuscitation
Goal: understand the pathophysiology of shock and it’s treatment
• Objectives:– Be able to categorize types of shock– Understand mechanisms of adapting to
volume loss of blood loss– Demonstrate shock treatment:
• lines, sites, types of fluid• End points of resuscitation• Complications of treatment

SHOCK: Definition
• Commonly misused– “psychogenic”– Webster: 12 different definitions
• 4: “the state of profound depression of the vital processes associated with reduced blood volume and pressure and caused usually by severe esp. crushing injuries, hemorrhage, or burns.”
“The rude unhinging of the machinery of life” Gross 1872

Types of Shock
• “Classic” Blalock 1937
– Hematogenic– Neurogenic– Vasogenic– Cardiogenic

Classification of Shock• Low Cardiac Output states
– Hypovolemic shock• volume loss• Internal volume loss
– Cardiac shock• Impaired inflow• Primary pump
dysfunction• Impaired outflow
– Low peripheral resistance states
• Neurogenic shock– Loss of sympathetic
tone• Vasogenic Shock
– Septic– Anaphylactic
Carrico: ACS Early Care of the Injured Patient 4th Ed.

The Circulatory System
• Components:– Heart (pump)– Blood Vessels– Blood

Circulation and Electricity
• Circulation– The flow of blood
• Electricity – The flow of electrons
• Ohms law: V= IR (Voltage = Current x
Resistance)
BP = CO x SVR • (Cardiac Output x System
Vascular Resistance)

Circulation Schematic
• The Pump (heart)– 2 sided
• Anatomically looks parallel, BUT:
• Physiologically and in Actuality
– Supplies 2 systems connected in series

2-Sided Pump
• Right Side– Compliant, flexible– Low pressure,
variable volume• Left Side
– Stiff, strong– High pressure,
fixed volume
Like the colon?
The Heart:

The Circulatory System
• Multiple Parallel Circuits– Organized
teleologically: • Prioritized supply
– Closest circuits get supplied first and foremost
» Coronaries, Brain, Kidneys
– Distal circuits get shut down when volume low
» Gut/Muscle, Skin

Circulatory Control Mechanisms
• Closest, fastest– Carotid Bodies (Baroreceptors)
• Stimulate Sympathetic Nervous System
• Mid-level– Kidneys- Juxtaglomerular
Apparatus• Sense low flow and stimulate
Renin resulting in vasoconstriction (splancnic)
• Down-line– Adrenal Cortex
• Senses need for more Sodium and Fluid Re-absorbtion to deal with upright posture volume needs

Acute Volume Loss
• Shock - Classes:
I 0-15% blood lossII 15-30% blood lossIII 30-40% blood lossIV >40% blood loss
SHOCK

Response to Volume Loss
Type % blood loss HR BP Postural Cap Ref
• I 0-15% nl nl maybe nl• II 15-30% + maybe yes nl• III 30-40% +++ decr moot incr• IV >40% ++++ <60Sys “ incr

Shock Resuscitation StudyShires, et al
• Bled dogs 40% blood volume– 100% mortality
untreated• Bled, then gave back
blood– 80% mortality– Autopsy study
• Swollen muscle cells despite total volume loss
• Tagged RBCs, Na+, K+, Alb., and repeated the experiment
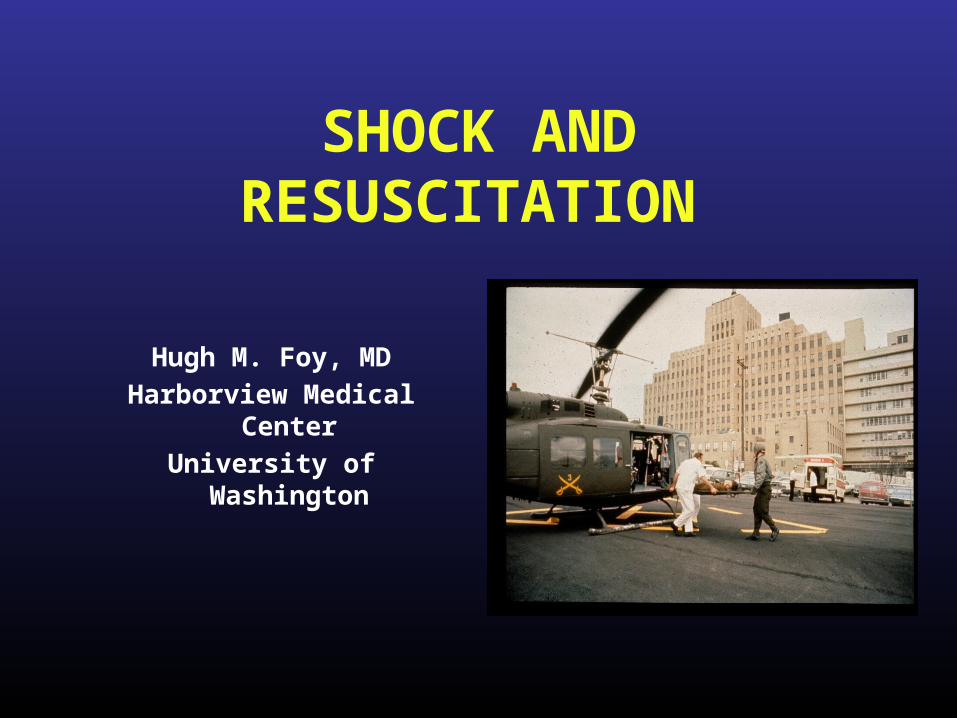
Results
• Na+ leaked into cells• K+ leaked out of
cells• Albumin leaked into
interstitial space• Water followed Na+ • Translocated fluid 3
times the shed blood• Measured
composition of transloc. fluid
Shires Shock Study

Conclusions
• Translocated Fluid composition is LR • Inadequate O2 delivery shuts down Na+/K+
pumps, making cells leaky
• Repeated the Experiment:– Gave Shed Blood plus 3 times volume of LR
• Mortality decreased from 80 to 30%
Shires Shock Study

Treatment of Shock
• Recognize Type of Shock
• If definite pump failure and cardiogenic shock institute cardiac protocols
• Otherwise: 2 large bore, upper extremity lines and:– Volume– Volume– Volume
When in doubt, try a little more volume

Treatment of Shock
• Goal: Restore perfusion
• Method: Depends on type of Shock– Basically 2 kinds:
• Hypovolemic (hemorrhagic, septic, neurogen.)
• Cardiogenic (Impedence or primary Cardiac Failure)

Treatment:Cardiogenic Shock
• Oxygen by nasal cannula• IV access
– Pain medication– Nitrates prn-
• may need unloading only after volume status addressed
– Treat arrythmias– CPR as needed

Treatment of Shock
• Prioritized approach• Must address and treat sequentially:
– PRELOAD– AFTERLOAD– PUMP
• QUESTIONs:– What type of fluid– How Much– End Point of Resuscitation

Resuscitation Fluids
• Blood• Lactated Ringers• Normal Saline• Colloids• Hypertonic Saline• Blood Substitutes

Treatment: Hemorrhagic Shock
• Large bore access – 2 upper extremity IVs– 16 gauge or larger
• Bolus therapy– 20 cc/kg– Adults- 2 liters
• Monitor Effect• Repeat if necessary• After 2nd bolus: need
blood txn – 10cc/kg

End Points of Resuscitation:
• Restoration of normal vital signs• Adequate Urine output
– 0.5 - 1.0 cc/kg/hr• Tissue Oxygenation measurement• Adequate Cardiac Index• Normalization of Oxygen delivery DO2I• Normal Serum Lactate levels
none proven helpful, some deleterious
Englehart; Curr Op Crit Care; Vol 12(6), Dec 06, p 579-574

Evolution in Treatment Strategies
• Auto transfusion (“Cell Saver”)• Hyperdynamic “Supranormal”
Resuscitation (Shoemaker)• Less is More - Mattox• Trauma Vaccine - Vedder, et al.• Hypertonic Saline• Glue Grant-
– standardization, endpoints, genetics

Alternatives to Transfusion:• Autotransfusion
– Safe, warm, better 2-3 DPG levels
– Coagulation factors present
– 2 methods• Passive collection and
anti-coagulant (chest tubes)
• “Cell Saver”- washes Red Cells
– Contamination and Time issues in trauma
• Expensive, fussy, too slow in trauma, • Okay in elective, clean cases

Hyperdynamic “Supranormal” Resuscitation• Swan Ganz Catheter• Measure ratio of O2 delivery
and consumption• Push fluid resuscitation until
no longer “flow dependent”• Massive Edema can be lethal
– (DaNang Lung, ARDS, MSOF, SIRS, Abdominal Comp. Syn.
Multiple synergistic factors: some influenced by ventilator strategy

Mattox in HoustonQ: Is less fluid better?
• Randomized pts. QOD • LR vs 250 cc. Hypertonic Saline/Dextran• 3% increase in survival in HSD (not significant)• Trend in increase survival in penetrating trauma
victims only • Prospective trial showed only a trend in
improvement, with low n of 48 pts• May be beneficial with head injuries only
• Ann Surg 1991;213:482-491• Am J Surg 1989;157:528-34

“We’ll see”

Trauma Vaccine Trials
• Shock-
“Ischemia-Reperfusion Injury”
* WBCs “up-regulated”
adhere to endothelium
* Damaged endothelium leaky
Create massive edema
Blocking adherence -mAb 60.3
-neutropenia protective against ARDS
- WBC surface adhesion molecules when blocked
decreases the edema and injury
- animal data encouraging
Human Trials unsuccessful
Vedder, et al: Blood, 15 2002, Vol 100, No. 6, pp 2077-80

HYPERTONIC SALINE WITH DEXTRAN (HSD)
7.5%saline with 6% dextran-70
• Less volume and weight to carry
• May reduce mortality• Limits secondary
brain injury• Less activation of
inflammatory cells

Harborview Study
• Double blind, randomized study• N = 209• Endpoint: ARDS free survival
– 250 ml 7.5% HTS/ 6% Dextran70 vs LR• Findings:
– No difference in population overall– Improvement in sickest patients (19%)
• > 10 units PCs required
• Bulger et al: Arch Surg. 2008; 143(2); 139-148
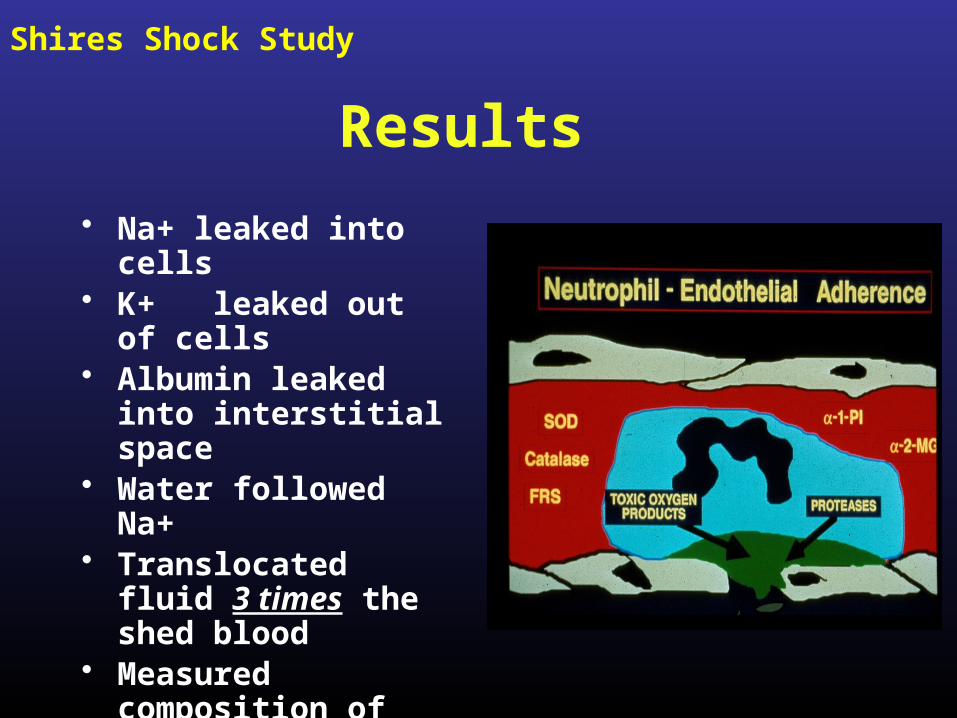
Shock-Treatment Algorithm

Transcutaneous O2 Sat Monitoring

Tissue Oxygenation Measurements
Cohn SM, Nathens AB, Moore FA, Rhee P, Puyana JC, Moore EE, Beilman GJ. J Trauma. 2007 Jan;62(1):44-54; discussion 54-5.
*StO2 <75 severe shock
78% MODS91% Dead
StO2 <75% in 1st hr.
* StO2 >7588%
MODS free survival
Similar to Base Deficit measurement

Blood Transfusion
• Blood Banks safer• Some risk
unavoidable– New viruses are
inevitable– False negative
screening tests• Independent risk
factor for MSOD• Time for cross-match
delays RxThe Search for
Alternatives continues

Alternatives to Transfusion:
• Blood Substitutes: – Immediately available, storage easier, no need
for compatibility testing, disease free– Polymerized, Stroma-free Hemoglobin
• 50 gm in 500 ml• No adverse effects up to 6 units• Slight increase in Bilirubin• Studies small, more needed
Gould:J Am Coll Surg 1998: 187:113-122

SUMMARY
• The Circulation is a Circuit• Volume is most often the answer• Lactated Ringers still the standard• More is better than less, maybe• New techniques:
– Hypertonic Saline- • okay in Head Injury• Less immunosuppression• Helpful in the sickest patients
– Better Indicators & Endpoints of Resuscitation
Shock and Resuscitation:
Related Documents




![Group presentation child care[1].pptx 2 (1).pptx 104first semester](https://static.cupdf.com/doc/110x72/546f3359b4af9ff50b8b4625/group-presentation-child-care1pptx-2-1pptx-104first-semester.jpg)





![ID 1 SESSION 4.pptx [Autoguardado].pptx](https://static.cupdf.com/doc/110x72/55cf8c675503462b138c00e6/id-1-session-4pptx-autoguardadopptx.jpg)