+ Shock R-9.16.19 Chapter 67

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

+
Shock R-9.16.19
Chapter 67
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Shock
n Syndrome = decreased tissue perfusion and impaired cellular metabolism
n Imbalance in supply/demand for O2 and nutrients

Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Diagnostic Studies
n Thorough H & Pn No single study
n Blood studies n Elevation of lactaten Base deficit
n 12-lead ECGn Chest x-rayn Hemodynamic monitoring
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Shock
n Classification of shockn Cardiogenic – see handout
n Hypovolemic
n Distributive
n Obstructive
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Low Blood FlowHypovolemic Shock
n Absolute hypovolemia: loss of intravascular fluid volume n Hemorrhage
n GI loss (e.g., vomiting, diarrhea)
n Fistula drainage
n Diabetes insipidus
n Hyperglycemia
n Diuresis
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Low Blood FlowHypovolemic Shock
n Relative hypovolemian Results when fluid volume moves out of the vascular space into
extravascular space (e.g., intracavitary space)
n Termed third spacing
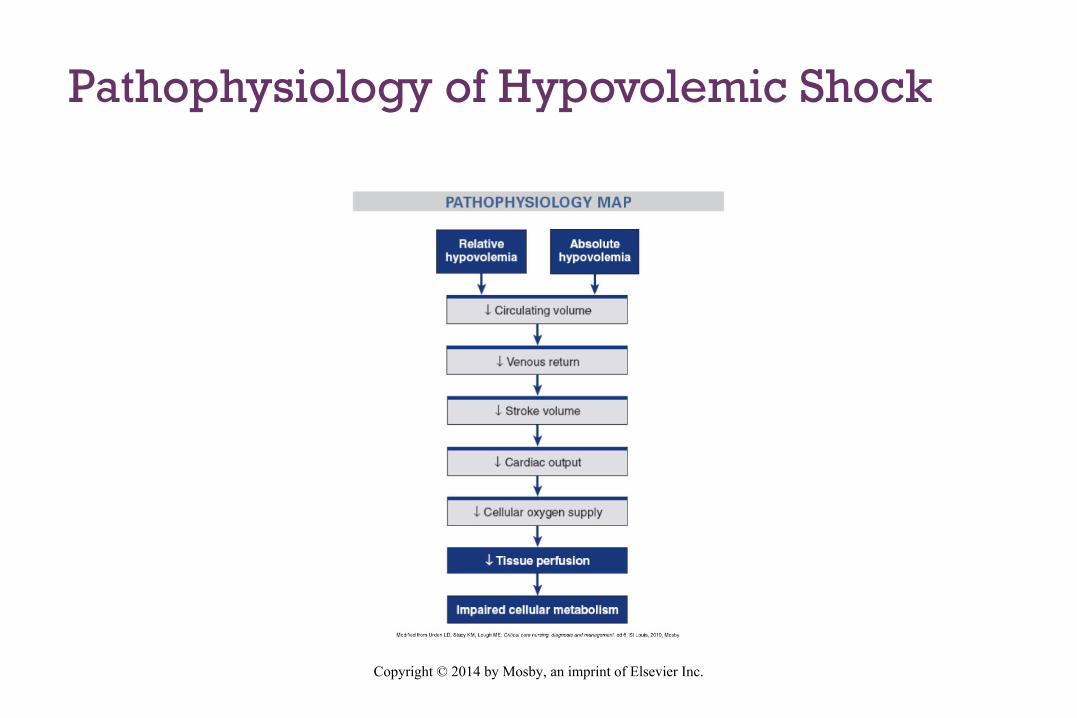
Pathophysiology of Hypovolemic Shock
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Low Blood FlowHypovolemic Shock
n Clinical manifestationsn Anxiety
n Tachypnea
n Increase in CO, heart rate
n Decrease in stroke volume, PAWP, urinary output
n If loss is >30%, blood volume is replaced
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Collaborative CareHypovolemic Shock
n Stop loss of fluid and restoring the circulating volume
n Fluid replacement: 3:1 rule (3 mL of isotonic crystalloid for every 1 mL of estimated blood loss)
Type of fluid?
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Distributive ShockNeurogenic Shock
n Hemodynamic phenomenon
n S/P 30 minutes of a spinal cord injury at the fifth thoracic (T5) vertebra or above
n Response to spinal anesthesia
n massive vasodilation, leading to pooling of blood in vessels
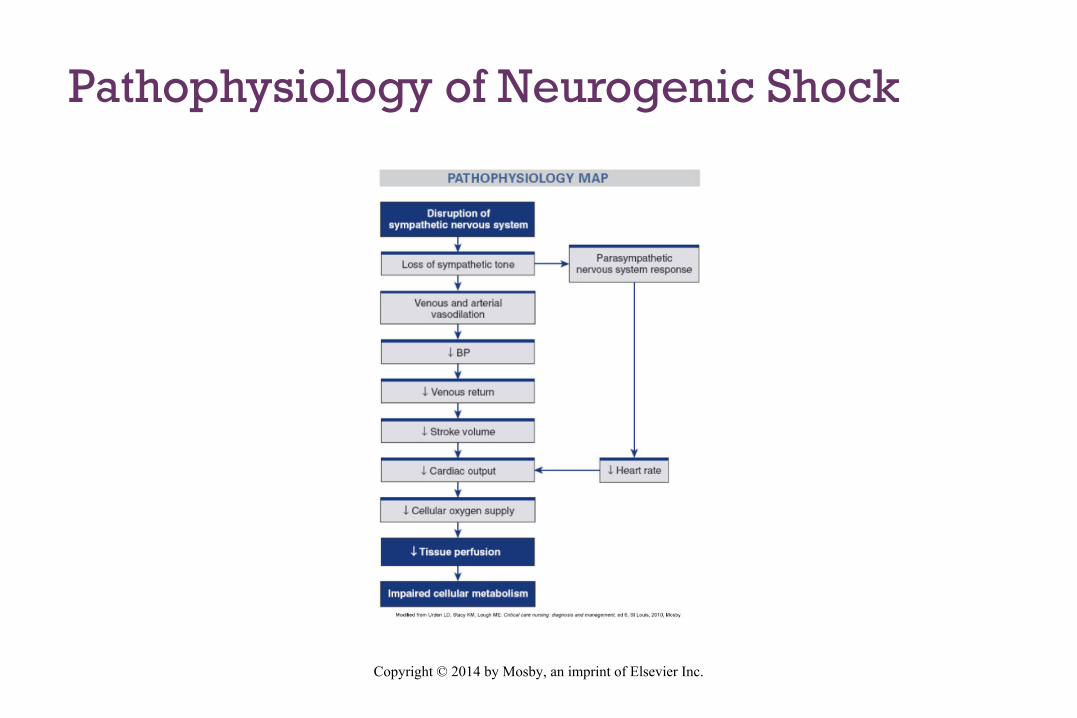
Pathophysiology of Neurogenic Shock
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Distributive ShockNeurogenic Shock
n Clinical manifestations n Hypotension
n Bradycardia
n Temperature dysregulation (resulting in heat loss)
n Dry skin
n Poikilothermia (taking on the temperature of the environment)
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Collaborative CareNeurogenic Shock
n In spinal cord injury: spinal stabilityn Vasopressors
n Atropine
n Fluids cautiously
n Monitor for hypothermia

Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Distributive ShockAnaphylactic Shock
n Acute, life-threatening hypersensitivity (allergic) reactionn Massive vasodilation
n Release of vasoactive mediators
n ↑ Capillary permeability
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Distributive ShockAnaphylactic Shock
n Clinical manifestationsn Anxiety, confusion, dizziness
n Sense of impending doom
n Chest pain
n Incontinence
n Swelling of the lips and tongue, angioedema
n Wheezing, stridor
n Flushing, pruritus, urticaria
n Respiratory distress and circulatory failure

Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Collaborative CareAnaphylactic Shock
n Epinephrine
n diphenhydramine
n Maintain a patent airway n Nebulized bronchodilators
n Aerosolized epinephrine
n Endotracheal intubation or cricothyroidotomy may be necessary
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Collaborative CareAnaphylactic Shock
n Aggressive fluid replacement
n IV corticosteroids
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Distributive ShockSeptic Shock
n Sepsis: systemic inflammatory response to documented or suspected infection
n Severe sepsis = sepsis + organ dysfunction
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Distributive ShockSeptic Shock
n Septic shock n hypotension despite fluid resuscitation
n hypoxia
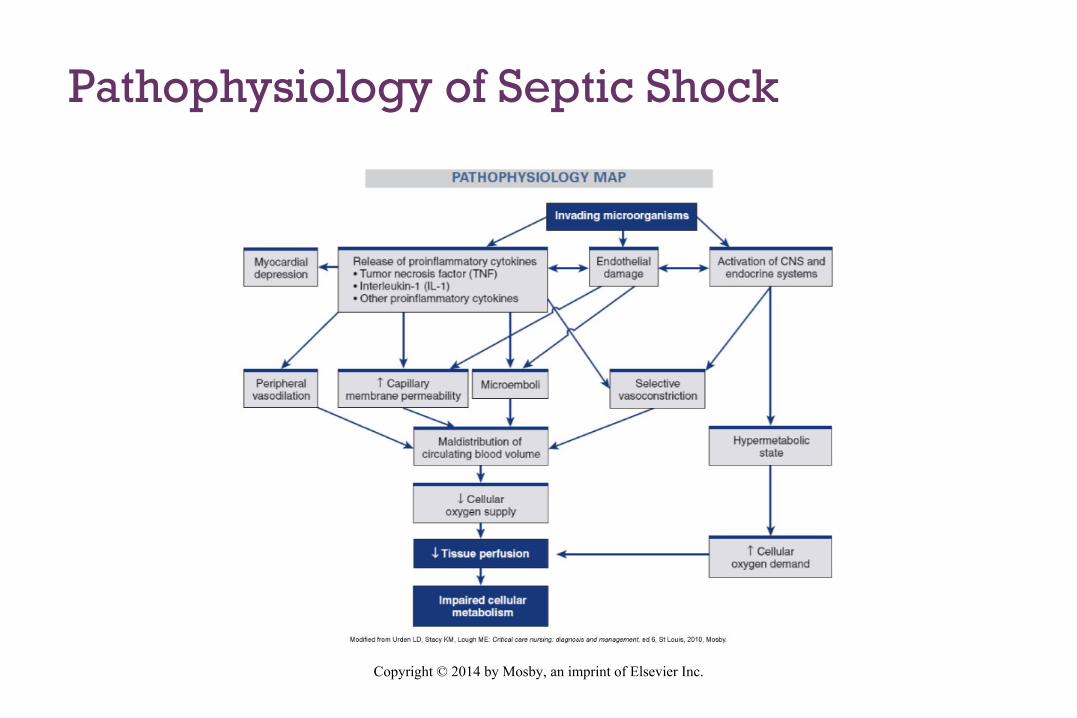
Pathophysiology of Septic Shock
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Distributive ShockSeptic Shock
n Clinical manifestationsn ↑ Coagulation and inflammation
n ↓ Fibrinolysis
n Formation of microthrombi
n Obstruction of microvasculature
n Hyperdynamic state: increased CO and decreased SVR
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Distributive ShockSeptic Shock
n Three major pathophysiologic effectsn Vasodilation
n Maldistribution of blood flow
n Myocardial depression
n Decreased ejection fraction
n Ventricular dilation
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Distributive ShockSeptic Shock
n Clinical manifestationsn Tachypnea/hyperventilation
n Temperature dysregulation
n ↓ Urine output
n Altered neurologic status
n GI dysfunction
n Respiratory failure is common
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Collaborative CareSeptic Shock
n Code Sepsis- Protocol handout
n Fluid replacement n Hemodynamic monitoring - Target CVP (8-12 mm Hg)
n Vasopressor drug therapy (CVP >8mm hg)
n Vasopressin for patients refractory to vasopressor therapy
n IV corticosteroids if vasopressor therapy not able to maintain BP
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Collaborative Care Septic Shock
n Antibiotics after cultures are obtained (e.g., blood, wound exudate, urine, stool, sputum)
n 1st Broad-spectrum antibiotics
n More specific antibiotics are then given based on the organism identified
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Collaborative Care Septic Shock
n Glucose levels <180 mg/dL
n Stress ulcer prophylaxis with histamine (H2)-receptor blockers
n DVT prophylaxis with low-dose unfractionated heparin or low-molecular-weight heparin
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Collaborative Care
n Cornerstone of therapy for septic, hypovolemic, and anaphylactic shock = volume expansion n Isotonic crystalloids (e.g., normal saline) for initial resuscitation of shock
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Collaborative Care
n Volume expansion- If no response to 2–3 L of crystalloids n blood administration
n CVP
n Monitor for Complications of fluid resuscitation
n Hypothermia
n Coagulopathy
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Collaborative Care
n Primary goal of drug therapy = correction of decreased tissue perfusionn Vasopressor drugs (e.g., norepinephrine)
n Achieve/maintain MAP >60 to 65 mm Hg
n unresponsive to fluid resuscitation
n Continuously monitor end-organ perfusion
n Vasodilator therapy (e.g., nitroglycerin, nitroprusside)
n Achieve/maintain MAP >65 mm Hg
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Collaborative Care
n Nutrition is vital to decreasing morbidity n Initiate enteral nutrition within the first 24 hours
n Initiate parenteral nutrition if enteral nutrition contraindicated or fails to meet at least 80% of caloric requirements
n Monitor protein, nitrogen balance, BUN, glucose, electrolytes
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+Nursing Assessment
n ABCs n Airway
n Breathing
n Circulation
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+
When assessing a patient in shock, the nurse recognizes that the hemodynamics of shock include:
a. Normal cardiac output in cardiogenic shock.
b. Increase in central venous pressure in hypovolemic shock.
c. Increase in systemic vascular resistance in all types of shock.
d. Variations in cardiac output and decreased systemic vascular resistance in septic shock.
Audience Response Question

Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+
The nurse is caring for a critically ill patient. The nurse suspects that the patient has progressed beyond the compensatory stage of shock if what occurs?
a. Increased blood glucose levelsb. Increased serum sodium levelsc. Increased serum calcium levelsd. Increased serum potassium levels
Audience Response Question
Copyright © 2014 by Mosby, an imprint of Elsevier Inc.
+
The nurse is caring for a patient in septic shock. Which hemodynamic change would the nurse expect?
a. Increased ejection fraction.b. Increased mean arterial pressure.c. Decreased central venous pressure.d. Decreased systemic vascular resistance.
Audience Response Question
Related Documents











