SHOCK

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

SHOCK

Definition
Shock is defined as: A physiologic state in which there is
inadequate blood flow to tissues and cells of the body –Brunner & Suddarth, 2004
A condition in which systemic blood pressure is inadequate to deliver oxygen and nutrients to support vital organs and cellular functions –Mikhail, 1999

Definition of Shock
“A clinical state in which blood flow is inadequate for tissue requirements or oxygen utilization is impaired. There is either insufficient oxygen delivery, maldistribution of oxygen delivery or impaired utilization”

SHOCK: AN OVERVIEW
SIGNIFICANCE OF SHOCK: Shock affect all body systems. It may
develop rapidly or slowly, depending on the underlying cause.
Nursing care of the patient in shock requires ongoing systemic assessment.

Types of Shock
Cardiogenic (intracardiac vs extracardiac)
Hypovolemic Distributive
Septic neurogenic (spinal shock) anaphylactic
SHOCK: AN OVERVIEW
STAGES OF SHOCK 1. INITIAL STAGE
2. COMPENSATORY STAGE 3. PROGRESSIVE STAGE 4. IRREVERSIBLE STAGE

SHOCK: AN OVERVIEW1.INITIAL STAGE Cells deprived of O2 mitochondria cannot produce ATP
anaerobic respiration lactic acid builds up metabolic acidosis harmful to cells
Hypoxia occur due to hypo perfusion state
Cell membrane damage
Anaerobic respiration
Build up of lactic and pyruvic acid
Metabolic acidosis

SHOCK: AN OVERVIEW
2. COMPENSATORY STAGE This stage is characterised by the body employing
the physiological mech, indusial, hormonal, neural, bio chemical in an attempt to reverse the condition
Hyperventillation to correct acidosis
baroreceptor reflexes sympathetic stimulation constrict arteriols in most parts of the body and venous reservoirs protection of coronary and cerebral blood flow
angiotensin-aldosteron, ADH vasoconstriction, water and salt retention by the kidneysabsorption of fluid from ISF and GIT, increased thirst
In this compensatory stage of shock, the patient’s blood pressure remains within normal limits.
This results from stimulation of the sympathetic nervous system.
The patient displays signs of fight-or-flight response There is blood shunting

SHOCK: AN OVERVIEW
COMPENSATORY STAGE CLINICAL MANIFESTATIONS
Blood pressure▪ normal
Heart rate▪ >100 bpm
Respiratory status▪ >20 breaths/minute
Skin▪ cold and clammy
Urinary output (UO)▪ decreased
Mentation▪ confusion
Acid-base balance▪ Respiratory alkalosis

SHOCK: AN OVERVIEW
Compensatory stage NURSING MANAGEMENT
▪ Monitoring tissue perfusion▪ Changes in LOC▪ V/S▪ UO▪ Skin▪ Lab values▪ Hemodynamic status▪ Administer IVF and meds
▪ Reducing anxiety▪ Promoting safety

SHOCK: AN OVERVIEW
2. PROGRESSIVE STAGE it should cause the crisis not been
successfully treat the shock will proceed to the progressive stage and the compensatory mechanism begins to fail
In the progressive stage of shock, the mechanisms that regulate blood pressure can no longer compensate and the mean arterial pressure (MAP) falls below normal limits, with an average systolic blood pressure of less than 90 mm/Hg.
- circulatory system themselves begin to deteriorate, without therapy shock becomes steadily worse until death
- positive feedback mechanisms are developed and can cause vicious circle of progressively decreasing CO
- Cardiac depression - coronary blood flow, contractility
- Vasomotor failure - cerebral blood flow Release of toxins by ischemic tissues: histamine,
serotonin, tissue enzymes Intestines hypoperfusion mucosal barrier
disturbance endotoxin formation and absorption vasodilatation,
cardiac depression
Vasodilation in precapillary bed
Generalised cellular deterioration: K+ , ATP, release of hydrolases – first signs of multiorgan failure

SHOCK: AN OVERVIEW
PROGRESSIVE STAGE: PATHOPHYSIOLOGY Although all organ system suffer from
hypoperfusion at this stage, two events perpetuate the shock syndrome:▪ (1)Cardiac dysfunction and;▪ (2) Failure of the autoregulatory function of
the microcirculation▪ Even if the underlying cause of the shock is
reversed, the breakdown of the circulatory system itself perpetuates the shock state, and a visual cycle ensues.

SHOCK: AN OVERVIEW
PROGRESSIVE STAGE: ASSESSMENT AND DIAGNOSTIC FINDINGS As shock progresses, organs systems
decompensate RESPIRATORY EFFECTS
▪ Rapid and shallow respirations▪ Crackles▪ Decreased O₂ levels and increased CO₂ levels▪ Alveolar collapse▪ Pulmonary edema▪ Interstitial inflammation and fibrosis▪ ARDS

SHOCK: AN OVERVIEW
PROGRESSIVE STAGE: ASSESSMENT AND DIAGNOSTIC FINDINGS cont’d.. CARDIOVASCULAR EFFECTS
Dysrhythmias and ischemia Rapid heart rate Chest pain Rise in cardiac enzyme levels Further impairment of the heart’s pumping
capacity

SHOCK: AN OVERVIEW
PROGRESSIVE STAGE: ASSESSMENT AND DIAGNOSTIC FINDINGS cont’d.. NEUROLOGIC EFFECTS
Confusion Subtle change in behaviour Lethargy Sluggish pupillary reactions

SHOCK: AN OVERVIEW
PROGRESSIVE STAGE: ASSESSMENT AND DIAGNOSTIC FINDINGS cont’d.. RENAL EFFECTS
Acute Renal Failure (ARF) Increase in BUN Increase in serum creatinine Fluid and electrolyte shifts Acid-base imbalances Decrease in urinary output

SHOCK: AN OVERVIEW
PROGRESSIVE STAGE: ASSESSMENT AND DIAGNOSTIC FINDINGS cont’d.. HEPATIC EFFECTS
Increased liver enzymes Decreased metabolic and phagocytic
actions Elevated bilirubin levels

SHOCK: AN OVERVIEW
PROGRESSIVE STAGE: ASSESSMENT AND DIAGNOSTIC FINDINGS cont’d.. GASTROINTESTINAL EFFECTS
Gastric stress ulcers Bloody diarrhea Increased risk of bleeding and infection

SHOCK: AN OVERVIEW
PROGRESSIVE STAGE: ASSESSMENT AND DIAGNOSTIC FINDINGS cont’d.. HEMATOLOGIC EFFECTS
Disseminated intravascular coagulation (DIC)
Bruises Bleeding Prolonged coagulation times

SHOCK: AN OVERVIEW
PROGRESSIVE STAGE: MEDICAL MANAGEMENT Depends on the kind of shock and its
underlying cause IV fluids and medications Early enteral nutritional support and use
of drugs to prevent GI ulcers and bleeding

SHOCK: AN OVERVIEW
PROGRESSIVE STAGE: NURSING MANAGEMENT Patient in the progressive stage are often cared for in the
ICU.▪ Proper documentation▪ Preventing complications
▪ Monitoring▪ Maintaining aseptic technique▪ Positioning and repositioning▪ Preventing pulmonary and integumentary complications
▪ Promoting rest and comfort▪ Efforts are made to minimize cardiac workload by reducing
patient’s physical activity and fear or anxiety.▪ Protection from excessive warmth or cold
▪ Supporting family members▪ The nurse should make sure that the family is comfortably
situated and kept informed about the patient’s status.

SHOCK: AN OVERVIEW
PROGRESSIVE STAGE: SUMMARY OF CLINICAL FINDINGS Blood pressure
Systolic <80-90 mmHg Heart rate
>150 bpm Respiratory status
Rapid, shallow respirations; crackles Skin
Mottled, petechiae Urinary output
0.5 mL/kg/hr Mentation
Lethargy Acid-base balance
Metabolic acidosis

SHOCK: AN OVERVIEW
3. IRREVERSIBLE STAGE / REFRACTORY STAGE Represents the point along the shock
continuum at which organ damage is so severe that the patient does not respond to treatment and cannot survive
Blood pressure remains low despite treatment Presence of an overwhelming metabolic
acidosis Multiple organ dysfunction has occured and
death is imminent

- despite therapy circulatory system continues to deteriorate and death ensues
marked hypoxic tissue damage endothelial dysfunction adhesive
molecules, neutrophils, macrophages inflammation progressive acidosis microcirculation failure plasma proteins leak to interstitium advanced disseminated intravascular
coagulation

SHOCK: AN OVERVIEW
IRREVERSIBLE STAGE: SUMMARY OF CLINICAL FINDINGS Blood pressure
Requires mechanical or pharmacological support Heart rate
Erratic or asystole Respiratory status
Requires intubation Skin
Jaundice Urinary output
Anuric, requires dialysis Mentation
Unconscious Acid-base balance
Profound acidosis

SHOCK: AN OVERVIEW
IRREVERSIBLE STAGE: MEDICAL MANAGEMENT Usually the same as for the progressive
stage Experimental strategies may also be
employed Antibiotic agents
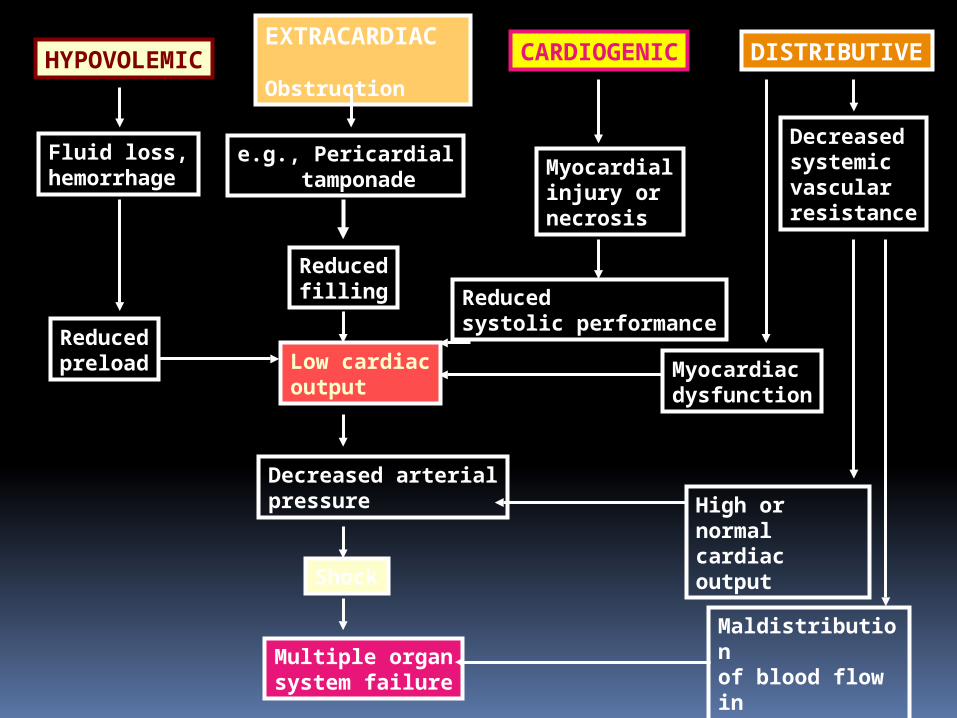
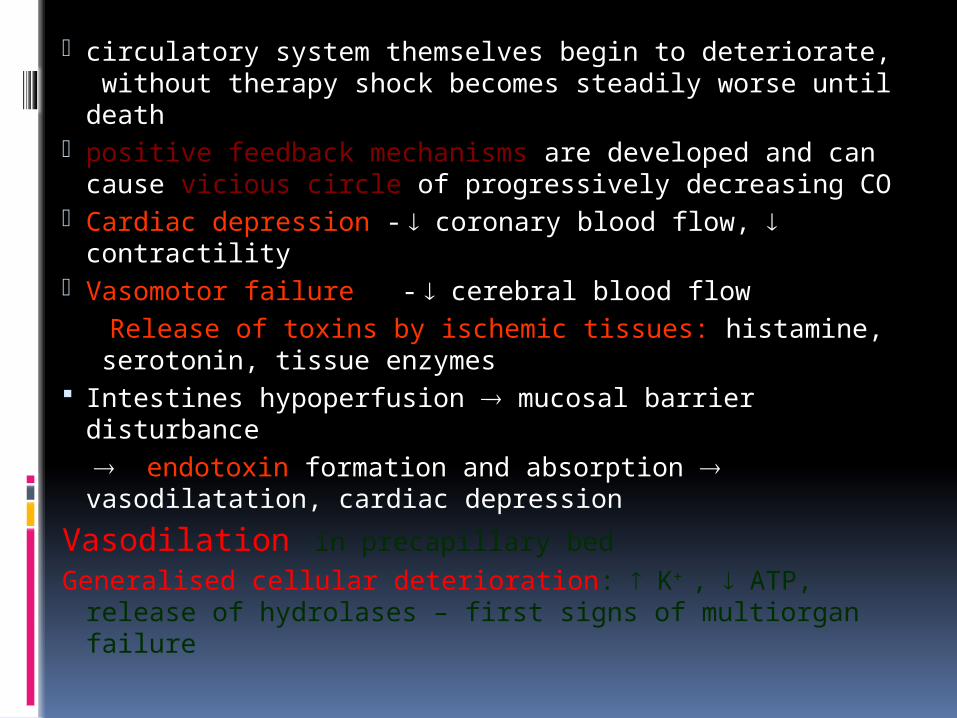
HYPOVOLEMICEXTRACARDIAC Obstruction
CARDIOGENIC DISTRIBUTIVE
Fluid loss,hemorrhage
e.g., Pericardial tamponade
Myocardialinjury ornecrosis
Decreasedsystemicvascularresistance
Myocardiacdysfunction
Reducedsystolic performance
Reducedfilling
Low cardiacoutput
Reducedpreload
Decreased arterialpressure
Shock
Multiple organsystem failure
High or normalcardiac output
Maldistributionof blood flow inmicrocirculation

DIFFERENT TYPES OF SHOCK

CARDIOGENIC SHOCK
CARDIOGENIC SHOCK
CARDIOGENIC SHOCK Occurs when the heart’s ability to
contract and pump blood is impaired and the supply of oxygen is inadequate
Causes: Coronary
Myocardial Infarction

• MI (most common)• Aortic dissection• PE• Cardiac tamponade• Ruptured viscus• Hemorrhage• Sepsis• Cardiomyopathy (restrictive or dilated),
myocarditis• Medication overdose (beta/calcium-channel
blockers)• Cardiotoxic drugs (doxorubicin)• Electrolyte abnormalities (calcium, phosphate)• Valvular abnormalities (mitral/aortic stenosis)• Papillary muscle or ventricular free wall rupture

Risk Factors for Developing CS• Older age• Multivessel CAD• Anterior MI location• STEMI or LBBB• HTN• DM• Prior MI• Prior CHF
33
Cardiogenic Shock, intracardiac Myocardial Injury or Obstruction to
Flow Arrhythmias valvular lesions AMI Severe CHF VSD Hypertrophic Cardiomyopathy

Cardiogenic Shock, extracardiac(Obstructive)
Pulmonary Embolism Cardiac Tamponade Tension Pneumothorax Presentation will be according to
underlying disease process.

CARDIOGENIC SHOCK CLINICAL MANIFESTATIONS
Angina pain Dysrhythmias Hemodynamic stability Rapid thready pulse JVD Pulmonary Edema oliguria Restless Hypotension Increase cvp Dependent edema Skin- pale, cyanotic, cold & moist

Differential Diagnoses (limited)
MI Tension PTX Aortic dissection PE Cardiac tamponade Ruptured viscus Valvular abnormalities (mitral/aortic
stenosis)
37

Diagnosis
ECG ECHO Chest X-Ray Cardiac enzymes

MEDICAL MANAGEMENT Goals:
1. Limit further myocardial damage and preserve the healthy myocardium
2. Improve the cardiac function
CARDIOGENIC SHOCK
MEDICAL MANAGEMENT Correction of underlying causes
▪ Coronary cardiogenic shock: thrombolytic therapy, angioplasty, CABG
▪ Non coronary: cardiac valve replacement, or correction of a dysrhythmia
Initiation of first-line treatment▪ Supplying supplemental O₂▪ Controlling chest pain▪ Providing selected fluid support▪ Administering vasoactive medications
▪ Dobutamine, dopamine, ▪ Controlling heart rate with medication or by implantation of
a transthoracic or intravenous pacemaker▪ Implementing mechanical cardiac support

CARDIOGENIC SHOCK
MEDICAL MANAGEMENT: FIRST-LINE TREATMENTS Pain control: MORPHINE Hemodynamic monitoring
▪ Measures:▪ Pulmonary artery pressures▪ Cardiac output▪ Pulmonary and systemic resistance
Pharmacologic therapy▪ Dobutamine
▪ Increases strength of myocardial contraction▪ Decreases pulmonary and systemic resistance
▪ Nitroglycerin▪ Venous dilator▪ Arterial dilator
▪ Dopamine▪ Low-dose▪ Medium-dose▪ High-dose
▪ Other Vasoactive medications
CARDIOGENIC SHOCK
MEDICAL MANAGEMENT: FIRST-LINE TREATMENTS cont’d.. Fluid therapy Mechanical assistive devices
Intra-aortic balloon counterpulasation Left and right ventricular assist devices
Pharmacologic Treatment of Cardiogenic Shock
• SBP <70 mm Hg + shock → Norepinephrine
• SBP 70-100 mm Hg + shock→ Dopamine
• SBP 70-100 mm Hg – shock→ Dobutamine
• Refractory hypotension + shock→ Amrinone or milrinone may improve
cardiac output
43

CARDIOGENIC SHOCK
NURSING MANAGEMENT Preventing cardiogenic shock Monitoring hemodynamic status Administering medications and IV fluids Maintaining Intra-aortic balloon counter
pulsation Enhancing safety and comfort

HYPOVOLEMIC SHOCK

Hypovolemic Shock
Definition:Reduction in intravascular volume
leading to insufficient oxygen delivery to cells (mitochondria)

HYPOVOLEMIC SHOCK
1. HYPOVOLEMIC SHOCK Characterized by a decrease in
intravascular volume Occurs when there is a reduction in
intravascular volume of 15% to 25% Can be caused by:
External fluid losses Internal fluid losses

PATHOPHYSIOLOGY
Loss of blood
decreased filling of the right heart( dec. in venous return)
decrease of filling of the pulmonary vasculature
decreases filling of the left atrium and ventricle
left ventricular stroke volume decreases
Drop in arterial pressure which leads to reduced perfusion to vital organs leading to multiple organ failure and
finally death if untreated

Etiology Reduced circulating blood volume with
secondary decreased cardiac output Acute hemorrhage Vomiting/Diarrhea Dehydration Burns Peritonitis/Pancreatitis Third spacing Diabetics diuretics
Etiology
Non haemorrhagic Vomitting,diarrhoea Bowel obstruction ,pancreatitis Burns Neglect ,environmental(dehydration)
Haemorrhagic Gl bleed Trauma Massive haemoptysis Ectopic pregnancy ,PPH

Clinical manifestation
Hypotensive flat neck veins clear lungs cool, cyanotic extremities evidence of bleeding?
Anticoagulant use trauma, bruising
oliguria

Clinical features Skin: cool, moist, pale
skin
Resp. rate: rate and depth are increased
Heart rate: pulse is weak and thready, MAP is decreased, pulse pressure is narrow
Blood pressure: increases then decreases
Urine output: decreased
Mentation: Loss of consciousness, restlessness, agitation, mild confusion

HYPOVOLEMIC SHOCK MEDICAL MANAGEMENT
Major goals▪ Restore intravascular volume▪ Redistribute fluid volume▪ Reverse the underlying cause
Treatment of the underlying cause▪ Haemorrhage▪ Diarrhoea/vomiting
Fluid and blood replacement▪ Insert two large-gauge IV line▪ Administration of isotonic crystalloids▪ Administration of blood and blood products
Redistribution of fluid Pharmacologic therapy
▪ Drugs used in cardiogenic shock▪ Also depends on the cause of hypovolemia
Management : A,B,C,D IMMEDIATE MANAGEMENT RESUSCITATION : EXTRACELLULAR FLUID REPLACEMENT :-maintenance of
circulation and B.P
maintenance of patent airway(A), and breathing(B) IMMEDIATE CONTROL OF BLEEDING QUICK ASSESSMENT EXTRACELLULAR FLUID REPLACEMENT :-maintenance of
circulation and B.P DRUGS : (D)
SEDATIVES CHRONOTROPIC AGENTS INOTROPIC AGENTS VASODILATORS VASOCONSTRICTORS BETA-BLOCKERS DIURETICS
PHYSICAL EXAMINATION AND MONITORING

Immediate Management : POSITION

Immediate control of bleeding
Compression bandages/pressure packs
Local haemostatic agents
ElectroCautery Ligature of
vessels

Surgical management vascular repair surgical haemostasis closure of bleeding ulcer

Quick examination
The patients clothing is cut away & the whole body is visualized, palpated & examined for other injuries or bleeding sites.
Assessment of blood loss :
Blood loss with fractures considered as :- 1,000 to 2,000 mL for pelvic fractures, 500 to 1,000 mL for femur fractures,
250 to 500 mL for tibia or humerus fractures,
125 to 250 mL for fractures of smaller bones.
A hematoma the size of an apple usually contains at least 500 mL of blood.

Neurological examination :
Glasgow coma scale

Fluid replacement
Crystalloids : Fluid replacement should be started with a crystalloid
3 liters. Over a time of 45 min is sufficient or depends on the vital signs(pulse, b.p, CVP,urine output)
In the mean time blood should be sent for cross matching
Colloids: (ex: albumin) – Will increase osmotic pressure, watch for
pulmonary edema – Remains in vascular space longer (several hrs)

How much Fluid?
1. Calculate total blood volume2. Determine the % of blood loss3. Multiple total blood volume by the %
loss4. Replacement by:5. Colloid fluids, 1.5 times the result in
step 3.6. Crystalloid fluids, 4 times the result
in step 3.
Blood: – 500 ml whole blood increases Hct 2-
3%, 250ml Packed RBC’s increases Hct 3-4%
Drugs (common in all types)
• Sedatives : to reduce pain– Morphine : 10 mg IM– Pethidine : 100 mg IM
• Chronotropic agents : increases H.R– Adrenaline : 1-8 mcg/min
• Ionotropic agents : inc. cardiac contractility– Dopamine : 3-10 mcg/min
• Vasoconstrictors– Phenylephrine : 20 mcg/min

Central Venous Pressure
Normal value : 10-15 mm of Hg In hypovolemic shock, the blood volume is
decreased, so is the CVP is also decreased. In cardiogenic shock there is no depletion of
blood volume and the CVP remains normal.
Urine
Urine output is a good indication of severity of shock. Urine output is affected quite early even in moderate shock. It is also a good index of adequacy of replacement therapy.
Normal output : 60-70 ml/hr. In shock : <30 ml/hr

HYPOVOLEMIC SHOCK
NURSING MANAGEMENT Primary focus: prevention of shock, if possible Otherwise, nursing interventions focus on
assisting with treatment targeted at treating its cause and restoring intravascular volume.▪ Administering blood and fluids safely
▪ Obtain blood specimens▪ Monitor for potential complications▪ Hemodynamic monitoring, vital signs, ABG,
Hgb&Hct, temp., physical assessment▪ Implementing other measures
▪ O₂ administration

CIRCULATORY SHOCK

CIRCULATORY/DISTRIBUTIVE SHOCKCIRCULATORY SHOCK
Occurs when blood volume is abnormally displaced in the vasculature – for example, when blood volume pools in peripheral blood vessels.
The displacement causes a relative hypovolemia Causes:
▪ Loss of sympathetic tone▪ Release of biochemical mediators by cells
Three types:▪ 1. Septic shock▪ 2. Neurogenic shock▪ 3. Anaphylactic shock

Septic Shock

Definition
Shock:- When the cardiovascular system fails to deliver enough oxygen and nutrients to meet cellular metabolic needs.
Sepsis:- Presence of bacteria in the blood stream.
Septic Shock:- Begins with the development of septicaemia usually from bacterial infections, but can be viral in origin.
This is the most common type of Distributive Shock.

CIRCULATORY SHOCK:SEPTIC SHOCK
1. SEPTIC SHOCK Most common type; caused by widespread
infection The greatest risk of sepsis occurs in patients
with bacteraemia and pneumonia Risk factors in the increased incidence of septic
shock:▪ Increased number of immunocompromised
patients▪ Increased incidence of invasive procedures▪ Increased number of resistant microorganisms▪ Increase in the older population

Septic Shock
Results due to a severe infections Usually a bacterial infection(gram-negative bacteria)
Definitions: SIRS (Systemic inflammatory response
syndrome Severe SIRS Sepsis Severe Sepsis Septic Shock

Septic Shock
Systemic inflammatory response syndrome (SIRS): The systemic inflammatory response to a wide variety of severe clinical insults manifests by 2 or more of the following conditions:
Temperature greater than 38°C or less than 36°C
Heart rate greater than 90 beats per minute (bpm)
Respiratory rate greater than 20 breaths per minute or PaCO2 less than 32 mm Hg
White blood cell count greater than 12,000/mL, less than 4000/mL, or 10% immature (band) forms

Septic Shock
Causes 1)Lower respiratory tract infections >Streptococcus pneumonia >Klebsiella pneumonia >Staphylococcus aureus >Escherichia coli >Legionella species >Haemophilus species >Anaerobes >Gram-negative bacteria >Fungi

Septic Shock
2)Urinary tract infections >E coli
>Proteus species
>Klebsiella species
>Pseudomonas species
>Enterobacter species
>Serratia species

Septic Shock3) GI tract infections E coli Streptococcus faecalis Bacteroides fragilis Acinetobacter species Pseudomonas species Enterobacter species Salmonella species

Septic Shock
5) Invasive procedures Catheters Intravascular devices Prosthetic devices Hemodialysis and peritoneal dialysis catheters Endotracheal tube6) Prior antibiotic treatment7) Prolonged hospitalization8) Childbirth, abortion9) Other factors Malnutrition

Pathophysiology
MO invades body tissues immune response release of chemical mediators vasodilatation & micro thrombi formation obstruction of blood flow to tissue & organs hypoxia lactic acidosis
Dignosis
Vital signs
Narrow pulse pressure and tachycardia
Peripheral vasodilatation warm shock
Stroke volume and cardiac out put decrease
Altered mental status and oliguria

Work up
Lab Studies
Imaging Studies

Lab studies
Serum chemistry Serum electrolyte Platelet WBC PT &APTT LFT Blood & urine culture Gram staining

Imaging studies
CT X-RAY MRI

Diagnosis
To diagnose septic shock, the following two criteria must be met:
Evidence of infection, through a positive blood test.
Hypotension, despite adequate fluid replacement.
In addition, two out of four of the following must be present also:
Heart rate > 90bpm. Body Temp < 36 or > 38˚C. Hyperventilation. White blood cell count < 4000 cells/ mm3 or
>12000 cells/mm3.

Diagnostic Criteria
SIRSRequires 2 of the following:
Severe SIRSMust meet criteria for SIRS, plus 1 of the
following:a. Temp >38.3° or <36.0° Cb. Tachypnea (RR>20 )c. Tachycardia (HR>90, in the
absence of intrinsic heart disease)
d. WBC > 10,000/mm3
a. Altered mental statusb. SBP<90mmHg or fall of >40mmHg from
baselinec. Impaired gas exchanged. Lactic acidosis (pH<7.30 & lactate > 1.5 x
upper limit of normal)e. Oliguria or renal failure (<0.5mL/kg/hr)f. Hyperbilirubinemiag. Coagulopathy (platelets < 80,000-100,000/mm3, INR >2.0, PTT >1.5 x control, or elevated fibrin degredation products)
Management of Septic Shock Early goal directed therapy Identification of source of infection Broad Spectrum Antibiotics IV fluids Vasopressors Steroids ?? Recombinant human activated protein
C ( Xygris) Bicarbonate if pH < 7.1
Treatments
Fluid resuscitation Vasopressors Antibiotics initially : empirical antibiotics later : specific antibiotics(based on appropriate culture
and sensitivity test) Empirical therapy Cephalothin (6 to 8 Gm/day I.V. in 4 to 6 divided
doses), Gentamicin ( 5 mg/Kg./,day ), Clindamycin (particularly when infecting organism is
Bacteroids) Nutritional therapy
Enteral rather than parenteral route

Respiratory Support Transfusions Recombinant Activated Protein C Corticosteroids Glycemic Control

CIRCULATORY SHOCK:SEPTIC SHOCK
SEPTIC SHOCK: NURSING MANAGEMENT Use strict septic technique in all procedures Monitor for signs of infection Obtain appropriate specimens for C&S Address an elevated body temperature
▪ Administer acetaminophen as prescribed▪ Provide hypothermia blankets▪ Monitor for shivering▪ Provide comfort
Adminidtration of prescribed IV fluids and medications Monitor blood levels of medications, BUN, creatinine, WBC Monitor other values
▪ Hemodynamic status▪ I&O▪ Nutritional status
Complication
Septic shock Acute respiratory distress syndr
ome Arrhythmias DIC Hepatic and renal failure Fetal and maternal death

Neurogenic shock

Definition
Definition: hypotension as a result of the loss of sympathetic vascular tone below the level of spinal cord injury
*Hemodynamic phenomenon- * Loss of vasomotor tone & Loss of sympathetic nervous system tone > impaired cellular metabolism
Occurs Within 30 min cord injury level T 5 or above; last up to 6 weeks; also due to effect some drugs that effect vasomotor center of medulla as opioids, benzodiazepines

Spinal shock & neurogenic shock can in same patient-BUT not same disorder
Mechanism: Loss of autonomic innervation of the cardiovascular system (arterioles, venules, small veins, including the heart)
-it occur after acute spinal shock-sympathetic outflow is disrupted leaving unopposed vagal tone-result in hypotension and bradycardiaspinal shock – temporary loss of spinal reflex activity below a total spinal cord injury
Neurogenic Shock
Causes:
1. Spinal cord injury
2. Drugs
3. Regional anesthesia
4. Neurological disorders

Imbalance bet: sympathetic & parasympathetic stimulation
Massive vasodilation
Decreased SVR
Reduction in vascular tone
Inadequate CO, falling BP
Tissus perfusion of O2&nutri
Impared cellular metabolism
Fig 3: NEUROGENIC SHOCK

Clinical manifestation
- Hypotension (due to massive vasodilatation - Bradycardia- due to unopposed parasympathetic stimulation - Poikilothermia; *Unable to regulate temperature- - CVP decrease - skin- pale and cool -oliguria to anuria -Flaccid paralysis below level of spinal cord injury

Risk factors
Spinal cord injury Spinal anaesthesia Depressed action of medication

Neurogenic Shock- Management
fluid replacement Resuscitation initiation of
vasopressor drugs to counteract vasodilatation.
Administer atropine if bradycardia occurs

management• -keep MAP at 85-90mm Hg for first 7 days
-thought to minimize secondary cord injury -if crystalloid is insufficient use vasopressure-search for other cause of hypotension-for bradycardia -atropine -pacemakermethylprednisolone -used only for blunt injury - high dose therapy for 23 hrs - must be started within 8 hrscontroversial –risk for infection ,GI bleed-monitor temp-provide supplementary o2- Alpha agonist to augment tone if perfusion still inadequatedopamine at alpha doses (> 10 mcg/kg per min)ephedrine (12.5-25 mg IV every 3-4 hour)
-

Nursing Management
Elevate bed atleast 30 degree when patient receiving spinal or epidural anaesthesia
Carefully immoblize the patient to prevent complication Support cardiovascular and neurologic
function▪ Apply elastic compression stockings▪ Monitor for and prevent complications
associated with immobilty

Anaphylactic Shock
CIRCULATORY SHOCK:ANAPHYLACTIC SHOCK
ANAPHYLACTIC SHOCK: A circulatory shock state resulting from a
severe allergic reaction producing an overwhelming systemic vasodilation and reactive hypovolemia
There is widespread vasodilation and capillary permeability
Can be prevented
Anaphylaxis- rapid generalized immunologically mediated events involving an antigen specific IgE mediated mechanism that occur after exposure to foreign substances in previously sensitized person
IgE mediated Anaphylatoid reaction –clinically
indistinguishable from anaphylaxis ,do not require a sensitizing exposure
not IgE mediated

Anaphylactic Shock
Results from severe allergic reaction
Body responds to allergen by releasing histamine
Histamine causes vessels to dilate and become “leaky”

Anaphylactic Shock

Anaphylactic Shock
Patients with anaphylaxis develop:
o Hypotentiono hives (urticaria)o Itcho wheezing and
difficulty breathing (bronchospasm)
o angioedema
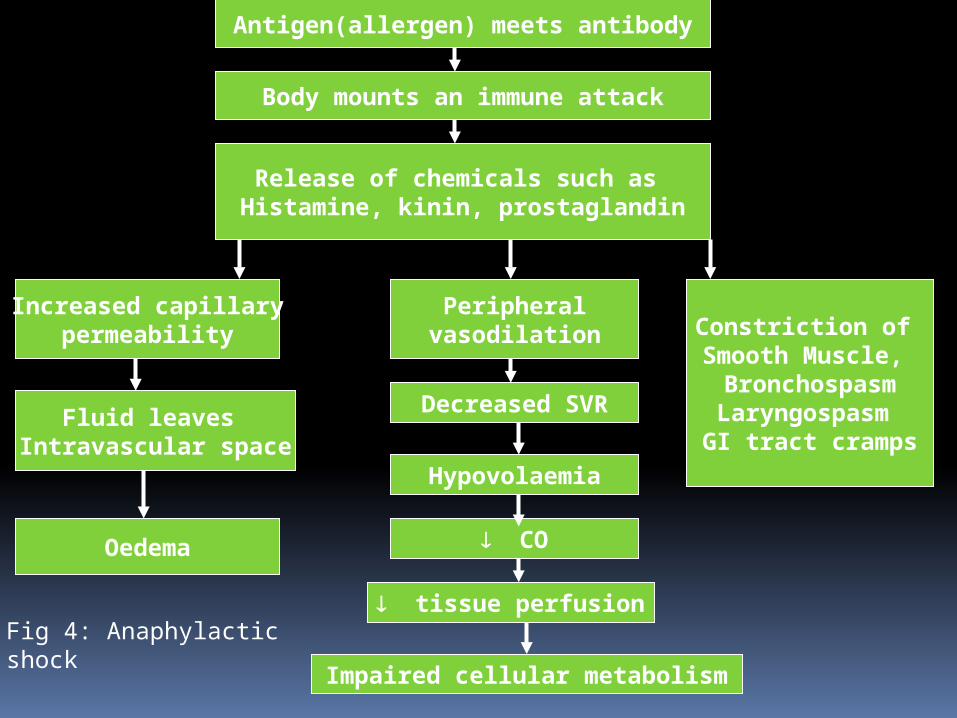
Antigen(allergen) meets antibody
Body mounts an immune attack
Release of chemicals such as Histamine, kinin, prostaglandin
Increased capillarypermeability
Peripheralvasodilation Constriction of
Smooth Muscle, BronchospasmLaryngospasm GI tract cramps
Fluid leaves Intravascular space
Oedema
Decreased SVR
Hypovolaemia
CO
tissue perfusion
Impaired cellular metabolism
Fig 4: Anaphylacticshock

symptoms of anaphylaxis
• First- Pruritus, flushing, urticaria appear• Next- Throat fullness, anxiety, chest tightness,
shortness of breath and lightheadedness
• Finally- Altered mental status, respiratory distress and circulatory collapse
• Hypotension• Pulmonary edema• Warm skin• Restless• Anxious• Abdominal cramp• diarrhoea


management
• ABC’s• Angioedema and respiratory compromise
require immediate intubation• Removing the causative antigen
• IV, cardiac monitor, pulse oximetry• IVFs, oxygen• Epinephrine• Second line
• Corticosteriods• H1 and H2 blockers

Anaphylactic Shock Management 1. basic and circulatory management.2. Specific management. Includes immediate
and late.Immediate Stop administering suspected agent and call
for help Early intubation Client to be placed immediately in supine or
Trendelenburg position with leg elevation to increase venous return.
Start epinephrine IM. Repeat every 5-15 min. until improvement occurs in blood pressure. if need IV in severe cases.

Replacement with crystalloids solution for rapid intravascular fluid volume expansion.
Advanced life support measures if cardiac arrest occurs.
Secondary (late)- Management IV epinephrine if hypotension persist. Atropine in cases with significant
bradycardia IV salbutamol if brancho spasm persist. If
need Anti histamines preferable Refer to critical care centers
• Epinephrine• 0.3-0.5 mg IM• Repeat every 5-10 min as needed• Caution with patients taking beta blockers-
can cause severe hypertension due to unopposed alpha stimulation
• For CV collapse, 1 mg IV• If refractory, start IV drip

• Corticosteroids• Methylprednisolone 125 mg IV • Prednisone 60 mg PO
• Antihistamines• H1 blocker- Diphenhydramine 25-50 mg
IV• H2 blocker- Ranitidine 50 mg IV
• Bronchodilators• Albuterol nebulizer• Atrovent nebulizer• Magnesium sulfate 2 g IV over 20 minutes
• Glucagon• For patients taking beta blockers and with
refractory hypotension• 1 mg IV q5 minutes until hypotension
resolves

CIRCULATORY SHOCK:ANAPHYLACTIC SHOCK
NURSING MANAGEMENT Assess all patients for allergies Observe patient for allergic reaction when
administering new medications Identify patients at risk for anaphylaxis in
diagnostic testing sites Be adept with the clinical signs of anaphylaxis,
CPR and other emergency measures Teaching the client and the family about
preventing future anaphylacticc episodes and administering emergency medications to treat anaphylaxis
Related Documents