
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Shock is a life threatening clinical syndrome of cardiovascular collapse characterised by
Hypotension: acute reduction in circulating blood volume
Hypoperfusion: inadequate perfusion of cells & tissues

Shock is a life-threatening medical
emergency and one of the most
common causes of death for critically ill
people.
One of the key dangers of shock is that it
progresses by a positive feedback
mechanism. Once shock begins, it tends
to make itself worse. This is why
immediate treatment of shock is critical.

◊ Pallor- paleness
◊ Sweating
◊ Clammy limbs-Cold extremities
◊ Tachycardia
◊ Low blood pressure (sometimes not seen)
◊ Decreased urine output
◊ Weak & rapid pulse
◊ Unconsciousness
◊ Sighing & shallow breath

Reduced effective circulating blood volume
Reduced venous return to heart
Reduced cardiac output
Reduced blood flow
Reduced supply of oxygen
Anoxia
Inflammatory mediators
SHOCK

Compensated/Initial/Reversible shock
Progressive decompensated shock
Irreversible shock
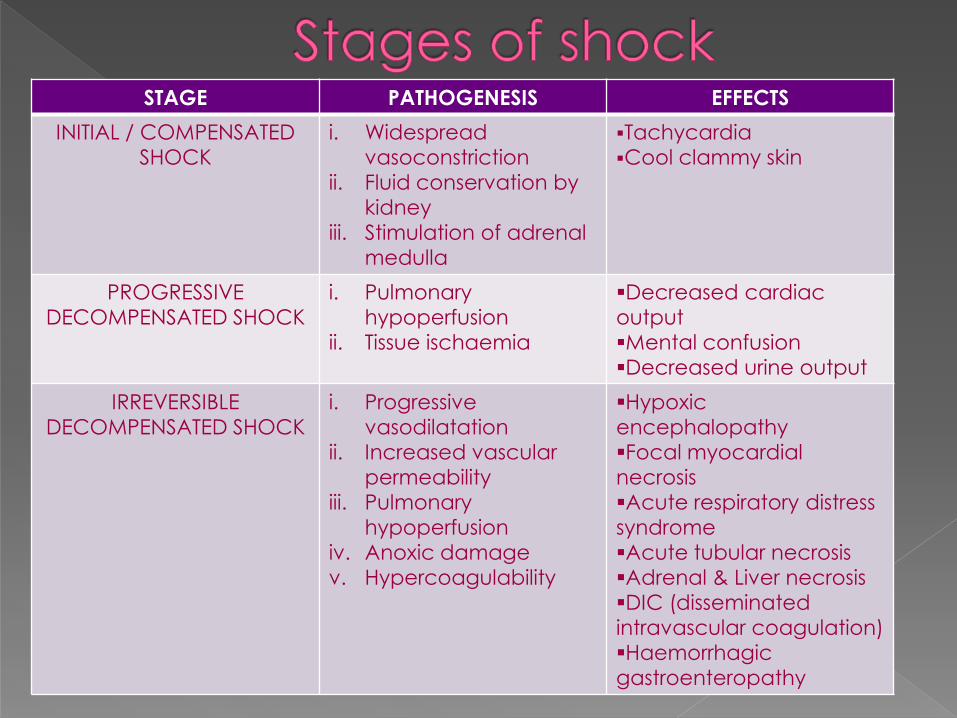
STAGE PATHOGENESIS EFFECTS
INITIAL / COMPENSATED
SHOCK
i. Widespread
vasoconstriction
ii. Fluid conservation by
kidney
iii. Stimulation of adrenal
medulla
Tachycardia
Cool clammy skin
PROGRESSIVE
DECOMPENSATED SHOCK
i. Pulmonary
hypoperfusion
ii. Tissue ischaemia
Decreased cardiac
output
Mental confusion
Decreased urine output
IRREVERSIBLE
DECOMPENSATED SHOCK
i. Progressive
vasodilatation
ii. Increased vascular
permeability
iii. Pulmonary
hypoperfusion
iv. Anoxic damage
v. Hypercoagulability
Hypoxic
encephalopathy
Focal myocardial
necrosis
Acute respiratory distress
syndrome
Acute tubular necrosis
Adrenal & Liver necrosis
DIC (disseminated
intravascular coagulation)
Haemorrhagic
gastroenteropathy

Hypovolaemic shock
Cardiogenic shock
Septic shock
Anaphylactic shock
Neurogenic shock Hypoadrenal shock
Traumatic shock
Shock of any type requires immediate treatment

Form of shock resulting from inadequate
blood volume
Either the RBCs along with plasma are
reduced or plasma volume alone
Causes: Acute haemorrhage
Dehydration (vomitings, diarrhoea)
Burns
Excessive use of diuretics
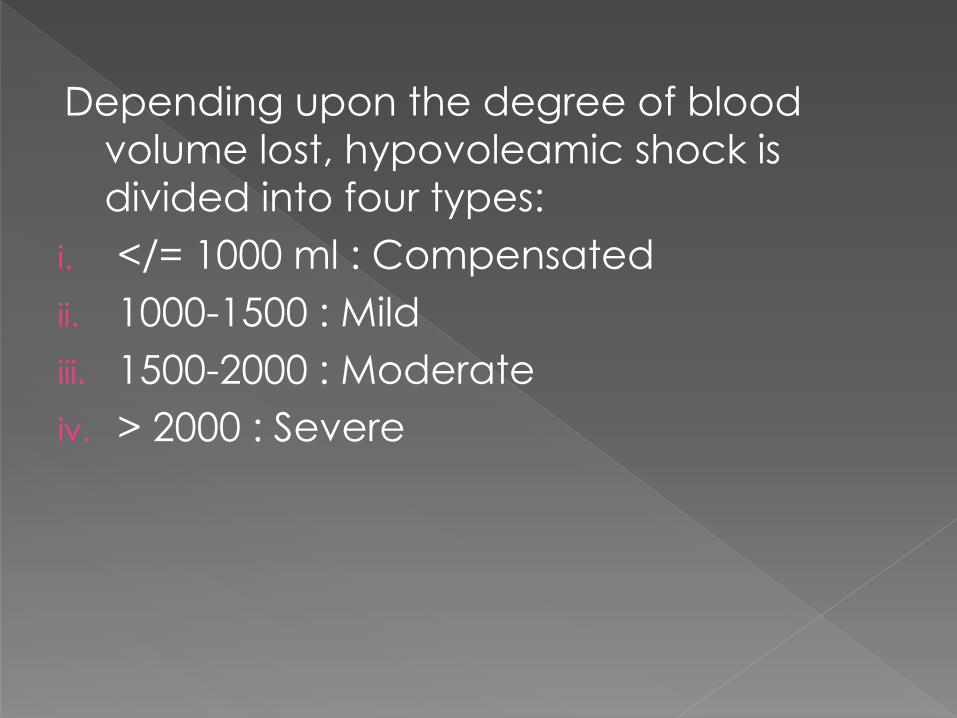
Depending upon the degree of blood
volume lost, hypovoleamic shock is
divided into four types:
i. </= 1000 ml : Compensated
ii. 1000-1500 : Mild
iii. 1500-2000 : Moderate
iv. > 2000 : Severe

Resulting from sudden fall in cardiac
output due to severe left ventricular
dysfunction
Normovoleamic shock
Causes : Myocardial infarction
Cardiomyopathies
Cardiac arrhythmias
Pulmonary embolism

Precipitated by severe bacterial infection
May be due to release of bacterial toxins
There is immune system activation &
severe systemic inflammatory response
Causes : Gram negative septicaemia (endotoxic shock) eg.E.coli,
Klebsiella, Pseudomonas
Gram positive septiceamia(exotoxic shock) eg.Streptococci,
Pneumococci
Due to inflammation, there is : Vasodilatation - profound vasodilatation causes
peripheral pooling of blood & hyperdynamic
circulation,
Increased vascular permeability - causes inflammatory
oedema
Disseminated Intravascular Coagulation
is prone to develop due to endothelial
cell injury by toxins

Type I hypersensitivity reaction
Caused by a severe anaphylactic
reaction to an allergen, antigen, drug or
foreign protein
Causes release of histamine which
causes widespread vasodilatation,
hypotension, & increased capillary
permeability

results from Slow heart rate due to
interruption of sympathetic vasomotor
supply
Causes :
High cervical spinal cord injury
Accidental high spinal anaesthesia
Severe head injury Should not be confused with SPINAL SHOCK which is a
recoverable loss of function of the spinal cord after injury and does not refer to the haemodynamic instability

Occurs from unknown adrenal
insufficiency
Patient fails to respond normally to stress
of trauma, surgery or illness
Causes : Administration of high doses of glucocorticoids
Secondary adrenal insufficiency eg . tuberculosis, idiopathic
adrenal trauma
Initially hypovoleamic shock
Even after hemorrhage control, patient
continues to suffer plasma loss into
interstitium of injured tissue
Causes : Severe injuries
Surgeries with marked blood loss
Obstetrical trauma


Cause should be identified & treated
Foot end of the bed should be elevated to increase venous return, this raises the BP to some extent
BP & plasma should be maintained with appropriate intra venous fluids
Vasopressors like Dopamine may be given intravenously when BP cannot be maintained by IV fluids.
Plasma expanders may help in cases of severe hypovleamia

Acid base & electrolyte disturbances should be corrected
Adequate urine output should be ensured
To restore the intravascular volume, the component that is lost should be ideally replaced-like plasma in burns, blood in haemorrhage. But in emergency, immediate volume replacement is important. In such cases, plasma expanders and IV fluids are used
Apart from restoration of intravascular volume, the specific cause of shock should be identified, and treated
Adrenaline
Morphine
Drotrecogin alpha (Activated
Protein C)
Vasopressors & inotropes
Plasma expanders

Adrenaline is the drug of choice in anaphylactic shock
0.3 – 0.5 ml of 1:1000 solution is used
Promptly reverses hypotension, laryngeal edema & bronchospasm and is life saving in presence of anaphylactic shock
Absorption by SC route is not reliable in presence of shock, hence IM route is preferred
Anaphylaxis can occur following the use of any drug, even in dental practice

IV morphine is the drug if choice in cardiogenic shock
Dose : 10-20 mg IM
Morphine affords symptomatic relief of pain without affecting the underlying disease
In MI morphine relieves pain & apprehension. As a result reflex sympathetic stimulation is reduced & shock is minimised

Drotrecogin alpha (Activated human protein C) is a drug recently introduced found to be useful in the treatment of septic shock
In septic shock, bacterial toxins evoke inflammatory response associated with impairment of coagulation & fibrinolysis
Protein C inhibits coagulation & improves fibrinolysis
May also inhibit TNF synthesis
Obtained by recombinant DNA technology
Very expensive

High molecular weight substances,
which when infused intravenously, exert
osmotic pressure and remain in the body
for long time
Colloids
•Dextrans
•Gelation polymer
•Polyvinyl pyrrolidine
•Hydroxyethyl starches
Crystalloids
•Normal saline
•dextrose
Substances causing vasoconstriction are called vasopressors
Vasopressors are used when BP cannot maintained by IV fluids
Vasopressors are administered only when the patient is normovoleamic
Norepinephrine is considered first line vasopressor, dobutamine first line inotrope
Epinephrine is second line catecholamine in shock that is unresponsive to other catecholamines

Itntravenous fluids are sterile solutions
meant for intravenous administration
IV fluids are used for the replacement of
fluid, electrolytes, & nutrition
IV fluids are given in almost all types of
shock. Therefore, a knowledge of
different IV fluids available is important
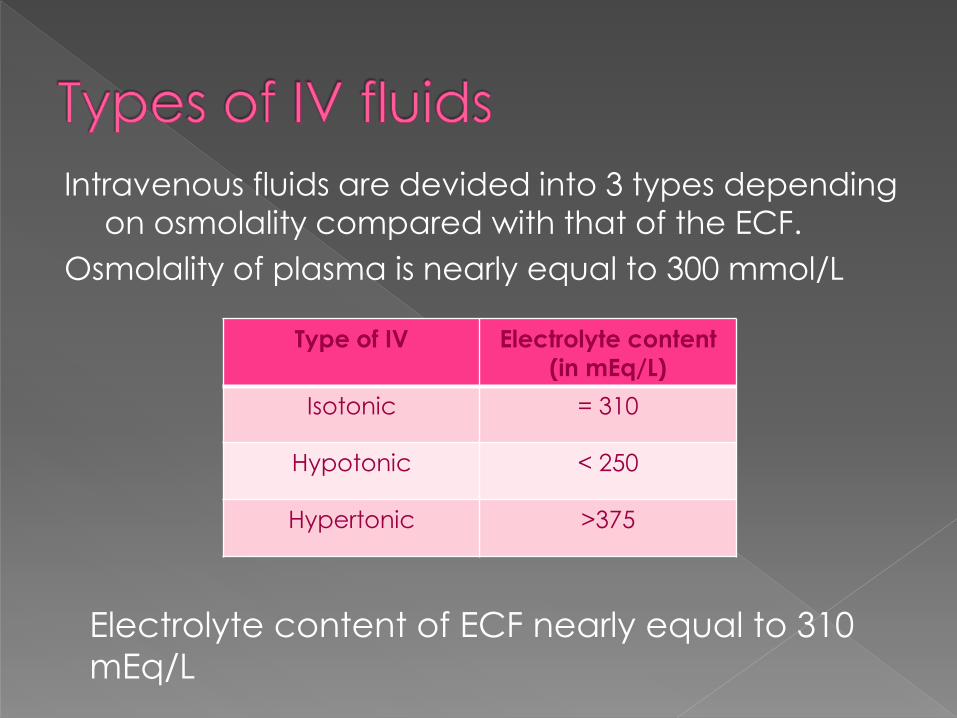
Intravenous fluids are devided into 3 types depending
on osmolality compared with that of the ECF.
Osmolality of plasma is nearly equal to 300 mmol/L
Type of IV Electrolyte content
(in mEq/L)
Isotonic = 310
Hypotonic < 250
Hypertonic >375
Electrolyte content of ECF nearly equal to 310
mEq/L
Osmolality is almost equal to that of ECF, hence does not alter the of shape of RBCs.
One liter of this solution expands ECF by one liter
But, quickly diffuses into ECF, & therefore three liters of isotonic fluid is required to replenish one liter of lost blood
Patients with hypertension & cardiac failure should be carefully monitered to avoid fluid overload
Isotonic solutions include normal saline & lactated ringer solution

Normal saline solution :
0.9% sodium chloride. It is used in
hyponatraemia . It should be avoided in
heart failure, pulmonary edema and
renal impairment.
Lactated ringer solution :
Contains potassium, calcuim, and sodium
chloride. It is used to correct
dehydration, hyponatraemia and to
replace gastrointestinal fluids.
Replace cellular fluids as they are
hypotonic to plasma
Half normal saline (0.45 % NaCl sol.) is the
one normally used
Used in hypeynatraemia and other
hyperosmolar conditions
Over dosage can result in intravascular
fluid depletion, hypotension, cellular
edema, and later cell damage

5% dextrose in normal saline or lactated ringer solution or in hypotonic solution has osmolality more than ECF
45 – 50% dextrose solution may be administered in hypoglyceamia or to supplement calories
Being strongly hypertonic, these fluids should be injected into central veins foe rapid dilution
They are injected slowly and carefully to avoid cell shrinkage and ECF volume overload

Related Documents










