Shift work and its impact upon nurse performance: current knowledge and research issues Joanne M. Fitzpatrick BSc PhD RGN Lecturer Alison E. While BSc MSc PhD RGN RHV Cert. Ed. Professor of Community Nursing and Julia D. Roberts BA MA Cert. Ed. RGN RNT Lecturer, Research in Nursing Studies Section, Florence Nightingale Division of Nursing and Midwifery, King’s College London, London, England Accepted for publication 8 December 1997 FITZPATRICK J.M., WHILE A.E. & ROBERTS J.D. (1999) Journal of Advanced Nursing 29(1), 18–27 Shift work and its impact upon nurse performance: current knowledge and research issues Previous research investigating shift work and its impact upon the quality of registered nurse performance and outcomes (including biological, psychosocial and organizational) is reviewed. The present study, which involved non- participant observation of staff nurses (n 34) within their first year of practice (Part 1 or Part 12 of the United Kingdom Professional Register), is described. The findings demonstrated support for earlier research which suggested that 12 1 2 hour shifts are associated with less effective performance. This study, together with previous research, highlights important indicators for the design and management of future empirical work which is required to investigate the influence of shift work upon process as well as outcomes for nurses, service users and the employing organization. This is particularly pertinent in the light of recent changes in work patterns. The well-being and effectiveness of the nursing workforce requires enhancement, and the effective management of shift-work is a key strategy in achieving this. Key words: shift work, process, outcomes, nursing INTRODUCTION Within health care provision, the need for 24-hour nursing care requires nurses to work shift systems. Health care management must address the needs of the nursing workforce in order to maximize the efficiency and effectiveness of care-delivery. Research in the field of shift work and its influence upon nurses is limited, with researchers having tended to focus upon different aspects of shift work, and with conflicting findings emerging. Further, the research has been conducted in different countries, so that differences in the nature of nursing work within the various health care systems further limits the generalizability of the findings. It is also likely that Correspondence: Joanne M. Fitzpatrick, Research in Nursing Studies Section, Florence Nightingale Division of Nursing and Midwifery, King’s College London, Cornwall House, Waterloo Road, London SE1 8WA, England. Journal of Advanced Nursing, 1999, 29(1), 18–27 Experience before and throughout the nursing career 18 Ó 1999 Blackwell Science Ltd

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Shift work and its impact upon nurseperformance: current knowledge andresearch issues
Joanne M. Fitzpatrick BSc PhD RGN
Lecturer
Alison E. While BSc MSc PhD RGN RHV Cert. Ed.
Professor of Community Nursing
and Julia D. Roberts BA MA Cert. Ed. RGN RNT
Lecturer, Research in Nursing Studies Section, Florence Nightingale Division
of Nursing and Midwifery, King's College London,
London, England
Accepted for publication 8 December 1997
FITZPATRICK J.M., WHILE A.E. & ROBERTS J.D. (1999) Journal of Advanced Nursing
29(1), 18±27
Shift work and its impact upon nurse performance: current knowledge and
research issues
Previous research investigating shift work and its impact upon the quality of
registered nurse performance and outcomes (including biological, psychosocial
and organizational) is reviewed. The present study, which involved non-
participant observation of staff nurses (n � 34) within their ®rst year of practice
(Part 1 or Part 12 of the United Kingdom Professional Register), is described.
The ®ndings demonstrated support for earlier research which suggested that
1212 hour shifts are associated with less effective performance. This study,
together with previous research, highlights important indicators for the design
and management of future empirical work which is required to investigate the
in¯uence of shift work upon process as well as outcomes for nurses, service
users and the employing organization. This is particularly pertinent in the light
of recent changes in work patterns. The well-being and effectiveness of the
nursing workforce requires enhancement, and the effective management of
shift-work is a key strategy in achieving this.
Key words: shift work, process, outcomes, nursing
INTRODUCTION
Within health care provision, the need for 24-hour nursing
care requires nurses to work shift systems. Health care
management must address the needs of the nursing
workforce in order to maximize the ef®ciency and
effectiveness of care-delivery. Research in the ®eld of
shift work and its in¯uence upon nurses is limited, with
researchers having tended to focus upon different aspects
of shift work, and with con¯icting ®ndings emerging.
Further, the research has been conducted in different
countries, so that differences in the nature of nursing work
within the various health care systems further limits the
generalizability of the ®ndings. It is also likely that
Correspondence: Joanne M. Fitzpatrick, Research in Nursing Studies
Section, Florence Nightingale Division of Nursing and Midwifery, King's
College London, Cornwall House, Waterloo Road, London SE1 8WA,
England.
Journal of Advanced Nursing, 1999, 29(1), 18±27 Experience before and throughout the nursing career
18 Ó 1999 Blackwell Science Ltd

nursing work has changed over time, with greater use of
technology and increased patient turnover requiring
cautious interpretation of earlier research ®ndings.
LITERATURE REVIEW
Variables in¯uencing performance
It is well established that human performance is in¯u-
enced by a variety of extrinsic and intrinsic variables
(McCloskey 1983, Feldt & Brennan 1989). Encompassed
within the former category is the individual's working
environment, which includes factors such as: shift work
(Todd et al. 1989, Skipper et al. 1990); expectations of the
health care institution, reference groups, and own
expectations (Benne & Bennis 1959); the attitudes and
expectations of superiors; the system of work organiza-
tion; quality and amount of work-related communications
(Harrington & Theis 1968); and the nurturing of innova-
tion, expression of individuality and morale (While 1994).
In view of the current interest in working patterns and the
recent European Community Directive on working time
(Institute of Personal Development 1993), it is the impact
of shift work upon nurse performance which is the focus
of this paper.
Previous research investigating shift work
A review of the literature has revealed that shift work has
been examined from a variety of perspectives, including
its in¯uence upon the biological and psychosocial systems
(i.e. outcomes) as well as its impact upon the quality of
performance (i.e. process).
Biological and psychosocial outcomes of shift work
Several studies have investigated biological and psycho-
social outcomes of shift work in general, while other
research has focused upon particular features of shift work
such as rostering and duration of shift.
Biological and psychosocial issues associated withshift work in generalSkipper et al.'s (1990) US questionnaire survey sought to
examine the effect of shift work on the physical and
mental health of a census sample of female nurses
(n � 482, 54á6% response rate) in ®ve hospitals (which
included general and psychiatric settings). The question-
naire consisted of seven scales which focused upon:
physical health; mental depression; family relations;
informal social participation; voluntary organization
participation; job performance; and job-related stress.
Internal consistency testing using Cronbach's alpha coef-
®cient revealed that ®ve of the seven scales reached
Nunally's (1978) criterion of 0á80: mental depression scale
(r � 0á903); family relations scale (r � 0á909); voluntary
organization participation scale (r � 0á828); job
performance scale (r � 0á909); and job-related stress scale
(r � 0á893). The coef®cient alphas for the physical health
scale (r � 0á671) and informal social participation scale
(r � 0á447) were more modest and should be borne in
mind when considering the study ®ndings, as should be
the absence of reported validity testing. While there was
no signi®cant association between shift work and nurses'
physical and mental health, signi®cant associations
emerged between shift work and voluntary organization
participation (P < 0á001) and hours spent in solitary
(P < 0á009), with afternoon nurses participating least in
voluntary organizations and spending the greatest
proportion of time in solitary activities. Similarly, social
isolation was identi®ed as a key problem for nurses
(n � 1087) in a questionnaire survey conducted in the
Netherlands (Bosch & Lange 1987), particularly for those
working weekend and night shifts. The nurse sample
worked in a variety of settings (including general hospi-
tals, psychiatric hospitals and nursing homes for older
adults), but selection of setting and subjects are not
detailed in the published paper.
Details of the impact of shift on job-related stress were
presented in a separate paper by the North American
researchers (Coffey et al. 1988). Using Swiercz's (1983)
tool to measure participants' job-related stress, ®ndings
indicated that the instrument's ®ve sub-scales were
signi®cantly related to shift: inadequate knowledge and
technical skills (P < 0á0046); nature of direct patient care
(P < 0á0012); interpersonal con¯icts (P < 0á0001); physical
working conditions (P < 0á0006); and management of the
unit (P < 0á0001), with nurses working the rotating shift
experiencing greater stress by comparison with those
working ®xed shifts. Further, nurses working rotating
shifts experienced signi®cantly more job-related stress
overall than those working ®xed afternoon, day and night
shifts (P < 0á001) which may in part re¯ect the experience
of working with a variety of different personnel and caring
for different patients at different times of the day. The
authors also suggested that this stress was related in part
to the disruption of circadian rhythms due to irregular
working hours. Lanuza (1976 p. 583) has suggested that
circadian rhythm disturbance due to factors such as shift
rotation may result in: `subjective feelings of fatigue,
imbalances of homeostatic mechanisms and decrements
in performance'. Further, Bosch and Lange (1987) found
that mental stress was not conducive to mental well-being
and contributed to sleeping problems and fatigue. In this
regard, it is interesting that Skipper et al. (1990) found no
signi®cant association between shift work and physical
and mental health.
By contrast with these ®ndings, Barton and Folkard's
(1991) questionnaire study involving a census sample of
psychiatric night nurses (n � 280) in one United King-
Experience before and throughout the nursing career Shift work
Ó 1999 Blackwell Science Ltd, Journal of Advanced Nursing, 29(1), 18±27 19

dom (UK) hospital reported signi®cantly higher stress
levels (P < 0á05) than the day shift nurses (n � 98). In
particular, temporary night nurses (i.e. permanent day
staff who had to undertake a 12-week period of night duty
every 12±18 months) reported the highest stress levels
(P < 0á05). Healy's (1997) more recent UK study of second
year student nurses (n � 100) undertaking their ®rst
allocation of night work found that the majority of the
sample (73%) were depressed on completion. Night work
also resulted in disturbances to sleep, appetite, energy,
concentration and an increase in psychosomatic com-
plaints such as irritability and feelings of helplessness.
Such ®ndings highlight the issue of self-selection which is
explored later in the paper. Healy's sample was drawn
from ®ve teaching hospitals. No further details of the
sample design are provided in the published paper.
RosteringThe impact of particular features of shift work, for
example rostering, has been investigated to a limited
extent. Contrary to the ®ndings of Skipper and colleagues
(1990), nurses and midwives in Barton's (1995) larger
study (n � 1082), who worked internal rotation and
irregular systems of duty rostering, experienced poorer
psychological health (P < 0á05), chronic fatigue (P < 0á05),
more social and domestic disruption (P < 0á01), more
disrupted sleep (P < 0á01), and more job dissatisfaction,
than those nurses working ¯exible systems (P < 0á01).
These ®ndings concur with the earlier Belgian work of
Verhaegen et al. (1987) which found that rotating nurses
(n � 44) (i.e. nurses who worked morning and afternoon
shifts in a weekly rotating scheme as well as periodic
night shifts) reported more health complaints than both
full time (n � 29) and part-time (n � 94) permanent
night nurses, although only the difference between the
rotating and part-time permanent night nurses was statis-
tically signi®cant (P < 0á01). Similarly, Jamal (1981) found
that nurses (n � 180) working on rotating shifts in two
Quebec hospitals obtained lower scores for mental health,
job satisfaction, social involvement and organization
commitment than nurses (n � 245) working ®xed shifts,
and scored higher on anticipated turnover, absenteeism
and lack of punctuality. In Niedhammer et al.'s (1994)
longitudinal study of the effects of shift work on sleep
among French nurses (n � 469), those who worked
alternating schedules and particularly those who
alternated with night shifts, were more likely to experi-
ence sleep disorders (de®ned by the authors as premature
awakening and dif®culties in getting to sleep) than those
on permanent schedules (P < 0á05). Sleep disorders
predicted nurses' transfer to permanent days, and a
signi®cant decrease in sleep disturbance was subsequent-
ly reported. Similarly, in Gold et al.'s (1992) cross-
sectional study, in the United States of America (USA),
nurses (n � 119) working rotating shifts were 2á8 times as
likely to report poor quality sleep, as were nurses working
day/evening shifts (n � 61).
Such ®ndings suggest that rostering constitutes an
important variable when examining the in¯uence of shift
work on employees. Empirical evidence in this ®eld,
however, is not unequivocal. Barton (1995) found that
regular rostering (a ®xed roster which is repeated when
the cycle of shifts ®nishes) and ¯exible rostering (the duty
roster is drawn up in consulation with individuals) had no
in¯uence upon permanent night nurses. However, Barton
has suggested that this may be due to the fact that many
permanent night nurses have chosen to work the night
shift and are less concerned with the details of their shifts.
In an earlier study (Barton 1994) 81% (n � 194) of
permanent night shift nurses, by comparison with 20%
(n � 69) of rotating shift nurses, had chosen to work their
present shift system. Those who had not chosen to work
their shift system displayed more symptoms of cardiovas-
cular disease and more non- domestic disruption (e.g.
dealing with dental, doctor or banking matters).
Duration of shiftTodd et al.'s (1993) two-phase survey which focused upon
duration of shift, investigated British nurses' satisfaction
with the introduction of a 12-hour shift (n � 234, 73%
response rate for phase 1; and n � 205, 64% response rate
for phase 2). All quali®ed and unquali®ed grades from 10
wards in two hospitals were recruited to the study. The
®ndings revealed overwhelming dissatisfaction among
quali®ed and unquali®ed nursing staff, with the majority
of nurses (83%) indicating a preference for returning to the
8-hour shift system. The 12-hour shift was regarded as
impacting negatively upon nurses' personal lives
(P £ 0á0001) and family commitments (P £ 0á0001), and
participants reported feeling more mentally (P £ 0á0001)
and physically (P £ 0á004) tired. However, the rostering
system was not examined by Todd et al. Similarly, in
Mills et al.'s (1983) earlier US pilot study involving a
census sample of nurses (n � 30) in one surgical inten-
sive care unit working 1212 hour shifts, a signi®cant
association emerged between drowsiness (P < 0á05) and
physical impairment (P < 0á05), and length of shift. A
methodological strength of Mills et al.'s study was that the
majority of the sample (n � 24) had not previously
worked a 1212 hour schedule (Bohle & Tilley 1989). Fatigue
was measured using: the Subjective Symptoms of Fatigue
Checklist (Yoshitake 1978); a reasoning test; and a vital
signs form test. Although not statistically signi®cant,
participants' mental reasoning increased over time, while
performance on a paper and pencil exercise at the ®rst,
sixth and twelfth hours revealed signi®cantly more errors
over time (P < 0á001), with the greatest increase occurring
between the ®rst and sixth hours.
Less effective performance over time may re¯ect the fact
that optimum mental and physical performance coincides
J.M. Fitzpatrick et al.
20 Ó 1999 Blackwell Science Ltd, Journal of Advanced Nursing, 29(1), 18±27

with peak temperature, the latter corresponding with the
time of day when individuals feel most alert; so, for
example, `day-active' people tend to feel at their best
during the middle of their waking period (Lanuza 1976
p. 584). Interestingly, the majority of Mills et al.'s (1983)
nurse sample (96%) preferred not to return to an 8-hour
shift. This may be attributed partly to having more leisure
time away from work, which the nurses regarded as
advantageous. In addition, they reported that their own
performance (P < 0á001) as well as communication within
the practice unit (P < 0á05) had improved signi®cantly
since working the 1212 hour shift.
Self-selection and adaptation
The above studies have identi®ed some of the biological
and psychosocial issues associated with shift work. These
factors impinge upon ef®ciency and effectiveness of
performance, which in turn has implications for the
individual worker, service users and the employing
organization. Similarly, affective, motivational and atten-
tional variables may in¯uence an individual's response to
shift work (Messick 1984, Vries-Griever & Meijman 1987,
Feldt & Brennan 1989). Thus attitude towards and com-
mitment to a particular shift system constitute potentially
confounding variables. Bauer (1993 p. 933) noted that:
`Only when nurses had the choice of different work
patterns that matched their family responsibilities did
these physiological stress symptoms occur less frequently'.
Further, the results of Alward and Monk's (1990) US
study of nurses who worked 812 hours rotating shifts
(n � 30) (i.e. worked day and night shifts on an irregular
basis) or a ®xed shift schedule (permanent nights)
(n � 30) indicated that the latter perceived the ®rst shift
as requiring less overall effort than did the rotating shift
nurses (P < 0á01). The authors suggested that lifestyle
differences between the two groups rather than biological
factors alone may have accounted for the ®xed shift
group's more favourable response. Thus nurses' self-
selection for permanent night work may have positively
in¯uenced the study ®ndings. Indeed, this is a plausible
explanation for the ®ndings of other empirical work
(e.g. Verhaegen et al. 1987, Todd et al. 1989). In Verhaegen
et al.'s (1987) study investigating Belgian night nurses'
(n � 29) adaptation to different work schedules, the
sample was found to comprise people who were more
evening-oriented, and who demonstrated less rigidity of
sleep pattern and evaluated night work more positively
than nurses working a rotating system. Barton (1994)
reported that tolerance to night work increased when
individuals made the decision to work at night, for
whatever reason.
From an organizational perspective, Findlay's (1994)
pilot system of self-scheduling in a British continuing care
psychiatric ward resulted in: increased morale and job
satisfaction; greater continuity of client care; more effec-
tive use of nursing resources; and ®nancial savings.
Research in other employment spheres has yielded
interesting ®ndings. Reduced absenteeism was also a
reported advantage in Krausz and Freibach's (1983)
comparative study of ¯exible versus non-¯exible working
time for women (n � 277) in an Israeli insurance com-
pany, although comparability of ®ndings is limited due to
the different nature of the work. Work context variables,
which include hours and shifts worked (Redfern 1978),
may also be associated with unplanned absence which has
disruptive effects upon organizational productivity and
continuity of care (Beil-Hildebrand 1996). In this regard, a
proactive management approach is essential. Indeed,
Bosch and Lange (1987), as a result of their large study
of shift work for nurses in the Netherlands, recommended
that adjustment of work patterns to meet workers' needs
was an important measure in enhancing their well-being
as well as improving care delivery.
The Royal College of Nursing (RCN) (1997 p. 2) has
clearly indicated its position regarding shift working,
starting that: `all nurses should have the opportunity and
ability to review their own work patterns and to secure the
working arrangements which best suit their professional
and personal interests and their commitment to patients
care'. This is made more emphatic by the recent European
ruling requiring a 48-hour working week for non-ex-
empted staff (Institute of Personal Development 1993),
which will provide greater need for negotiation between
employers and nurses regarding shift work.
As well as the notation of self-selection, individual
coping strategies may in¯uence adaptability to working
different shift systems. A small British questionnaire
study to examine the effects of shift rotation on nurses'
stress, coping and strain (n � 18), conducted by Milne
and Watkins (1986), revealed that despite the introduction
of internal rotation, stress was perceived as being fairly
constant during the study and was managed by the use of
coping strategies such as: active cognition (drawing upon
past experience); active behaviour (adopting positive
action); and, less positively, `avoidance' (in this study,
trying to reduce tension by an increase in smoking). The
overall result was a signi®cant reduction in reported
strain.
Support for the positive effect of self-selection, how-
ever, is not conclusive. In addition, the issue of adaptation
and coping strategies of nurses working shifts warrants
further in-depth study.
The impact of shift work on quality of performance
The paucity of research investigating the in¯uence of shift
work upon the quality of performance (i.e. process) is
noteworthy. American nurses (n � 463) in Coffey et al.'s
(1988) study self-rated their clinical performance on items
Experience before and throughout the nursing career Shift work
Ó 1999 Blackwell Science Ltd, Journal of Advanced Nursing, 29(1), 18±27 21

drawn from Schwirian's (1988) instrument. The number of
items selected was not indicated in Coffey et al.'s pub-
lished paper. The items focused upon ®ve practice areas
which achieved acceptable levels of internal consistency:
leadership (r � 0á748); teaching/collaboration (r �0á818); planning/evaluation (r � 0á882); interpersonal
relations/communication (r � 0á795); and professional
development (r � 0á858). Coffey et al. (1988) found a
signi®cant relationship between overall performance and
shift, with self-rated quality of performance being highest
for nurses working the day shift, followed by night,
afternoon and rotating shifts (P < 0á0001). Further, within
the subscales of performance, professional development
was signi®cantly related to the type of shift worked
(P < 0á004), with those working nights rating themselves
signi®cantly higher than their counterparts. Coffey et al.
did not, however, examine actual performance in the
practice setting.
Using a repeated measure design, Todd et al. (1989)
explored the in¯uence of 8- and 12-hour nursing shifts
upon quality of care on wards (n � 10) within two
hospitals in Northern Ireland. Quality of care was mea-
sured using Monitor (Goldstone et al. 1983), 1 month prior
to the introduction of the 12-hour shift and 6 months after
it had been in operation. However, the homogeneity of the
Monitor instrument was found to be low in Redfern et al.'s
(1994) study examining the validity of three popular
generic quality assessment instruments in use in the UK,
and this should be borne in mind when considering Todd
et al.'s (1989) ®ndings. The Wilcoxon matched pairs
signed rank test yielded a signi®cant difference between
total Monitor scores for the wards (P < 0á01), with those
wards operating 8-hour shifts obtaining higher scores.
Eight-hour shift wards also obtained signi®cantly higher
scores for: planning of nursing care (P < 0á05); attending to
patient's psychosocial needs (P < 0á02); and evaluation of
nursing care objectives (P < 0á01).
Todd et al. concluded that the 12-hour shift appeared to
be associated with less effective care. The researchers also
found that with under 12-hour shifts, there was a signi®cant
decrease in the percentage of time spent by students
working with trained nursing staff (P < 0á001), with 46%
of their time being spent working alone (Reid et al. 1991).
This has implications for pre-registration nurse education,
particularly in the UK in view of the establishment of the
diploma registered nurse (RN) programme and the ensuing
demands of large student cohorts upon clinical placement
areas (Jowett et al. 1994, White et al. 1994). Reid et al. (1991)
also found that in contrast to the 8-hour shift, when
approximately 50% of observations of students working
with quali®ed staff possessed an educational content, only
16á3% were coded under the 12-hour shift system
(P < 0á05).
Reduced performance capacity owing to the in¯uence
of extraneous variables such as duration and pattern of
shift may be compensated for by the investment of greater
effort on the part of the individual (Vries-Griever &
Meijman 1987), although impaired performance may still
occur. British transplant co-ordinators (n � 61) in Smi-
ther's (1995) study which examined the pattern and effect
of on-call work, reported sub-optimal performance owing
to tiredness, lack of concentration, stress, intolerance and
irritability. Similar ®ndings have been reported in other
areas of work. For example, Budnick et al.'s (1994) US
study of sleep and alertness among industrial workers
(n � 25) working a 12-hour rotating shift revealed ad-
verse behaviours for individuals on both day and night
shifts. On the day shift, the third and fourth days of the 4-
day rotation were perceived to be less safe, less produc-
tive and demanded more effort. The number of consecu-
tive shifts worked therefore represents an important
variable. (Northcott & Facey 1995). Workers in Budnick
et al.'s (1994) study also reported a variety of adverse
effects including: dif®culty in staying awake; falling
asleep on the job; and being more accident prone on their
journeys home from work. The authors suggested that
reduced alertness and/or fatigue as a consequence of
circadian rhythm desynchronization and sleep loss con-
tributed to these ®ndings.
Within the health service, such ®ndings have poten-
tially serious implications, for example, ineffective in-
formation processing (Vries-Griever & Meijman 1987) and
ineffective psychomotor skills performance (e.g. drug
administration errors). Similarly, Gold et al.'s (1992)
survey of all nurses in one Massachusetts hospital found
that nurses working rotating shifts (n � 119) were twice
as likely to report any accident (including car accidents,
medication errors, on-the-job procedural errors and on-
the-job personal injuries owing to tiredness) or error by
comparison with those working day/evening shifts
(n � 61). In the UK, such ®ndings raise concerns in view
of recent changes to the scope of professional practice
(United Kingdom Central Council for Nursing, Midwifery
and Health Visiting, UKCC 1992), with many registered
nurses now required to take on an extended role as a
means of reducing junior doctors' hours (Bradshaw 1995,
Dowling et al. 1995).
Contrary to more recent work (Todd et al. 1989), Mills
et al.'s (1983) North American study found no signi®cant
differences between the quality of patient care delivered
on wards operating 8 and 1212 hour shift systems. Quality
of patient care was measured using a tool which drew
upon a previously developed instrument (Jelinek et al.
1974) and focused upon: documentation of patient care;
observation of patient care; protection from infection;
special treatments; emotional needs; and special needs.
The authors tested the content validity of the instrument
and also reported high inter-item correlations with
Jelinek et al.'s criteria, although no further details are
presented in the published paper.
J.M. Fitzpatrick et al.
22 Ó 1999 Blackwell Science Ltd, Journal of Advanced Nursing, 29(1), 18±27

Gillespie and Curzio's (1996) small British question-
naire study of all nurses (n � 47) from two medical wards
located in one hospital revealed that 70% (n � 23) of the
nurses working a 12-hour shift system reported increased
opportunity for patient contact and a greater proportion of
time being spent in direct patient care. Having more time
off was also regarded positively by 61% (n � 14), which
contrasted starkly with nurses working the 8-hour shift
who identi®ed less time off between shifts as a major
disadvantage. A majority of those working the 12-hour
shift (64%), however, reported that communication be-
tween colleagues could be further improved. Only 40%
(n � 7) of those working the 8-hour shift identi®ed the
opportunity for increased patient contact to be an advan-
tage. Despite this ®nding, 76% of the nurses (n � 14)
indicated that they had adequate time for direct patient
care. The authors also reported that, regardless of shift
duration, nursing documentation was adequate and that
patients (n � 10) were generally satis®ed with the nur-
sing staff. The ®ndings of Gillespie and Curzio's (1996)
study, however, must be considered with caution in view
of the small sample sizes and poor response rate (48á5%).
THE PRESENT STUDY
The principal aim of the study was to re®ne and validate
the King's Nurse Performance Scale (Fitzpatrick et al.
1997), an empirically derived generic instrument which
permits detailed examination of nurses' practice within
the institutional setting. Contextual information included
data regarding the duration of participants' working shift.
Method
The performance of 34 purposively selected staff nurses
(all were within the ®rst year of practice, Part 1 or Part 12
of the UKCC Professional Register) was observed continu-
ously for 212 hours on three separate occasions (preferably
during a morning, afternoon and evening shift) using the
King's Nurse Performance Scale. Observation was not
conducted during the night shift, since the purpose of the
study was to test the reliability and validity of the
instrument and not to examine which nursing activities
occurred during the periods of day and night. The sample
was recruited from two hospitals within one London
Trust. Ethical approval was obtained from both
participating institutions and informed consent was
gained from all participants. Participants were observed
within the hospital setting on a variety of wards within the
medical, surgical, gynaecology, oncology and cardiology
directorates. For just over half of the observation sessions
(52á5%), participants worked shifts of 8 hours duration or
less, and for the remainder participants worked 12±1212
hour shifts.
Data analysis was conducted on completion of the data
collection process. A total mean performance score and
mean scores for the scale's ®ve practice domains (physical
domain; psychosocial domain; professional domain; com-
munication domain; and care management domain) were
derived for each participating nurse using the formula: the
sum of the weighted totals divided by the total number of
ratings. The Kruskal-Wallis test was used to explore the
relationship between duration of shift and clinical perfor-
mance as well as time of shift (that is, morning, afternoon,
or evening observations) and nurse performance.
Findings
Table 1 indicates that the median total performance score
was 3á6. The median values for each of the practice
domain scores were: `physical domain' 3á4; `psychosocial
domain' 3á7; `professional domain' 3á5; `communication
domain' 3á6; and `care management domain' 3á7. The
minimum scores for the different domains of practice
ranged from 3á2 (care management domain) to 2á6 (psy-
chosocial domain) and the maximum scores for the
domains ranged from 4á0 (psychosocial domain) to 3á9(physical, professional, communication and care manage-
ment domains).
A signi®cant relationship was found between duration
of shift and total performance score (P � 0á04), with those
working a shift of 8 hours or less achieving a higher total
performance score than those working 12±1212 hour shifts
(Table 2). Signi®cant differences were also found between
the two categories of shift in the physical (P � 0á03) and
professional (P � 0á01) domains of practice, with those
Table 1 Total median score and sub-section median scores
Median Minimum Maximum Q1 Q3
Total score 3á6 3á0 3á9 3á4 3á7Physical domain score 3á4 2á7 3á9 3á1 3á6Psychosocial domain score 3á7 2á6 4á0 3á5 3á8Professional domain score 3á5 2á9 3á9 3á2 3á7Communication domain score 3á6 3á0 3á9 3á5 3á8Care management domain score 3á7 3á2 3á9 3á5 3á8
Experience before and throughout the nursing career Shift work
Ó 1999 Blackwell Science Ltd, Journal of Advanced Nursing, 29(1), 18±27 23
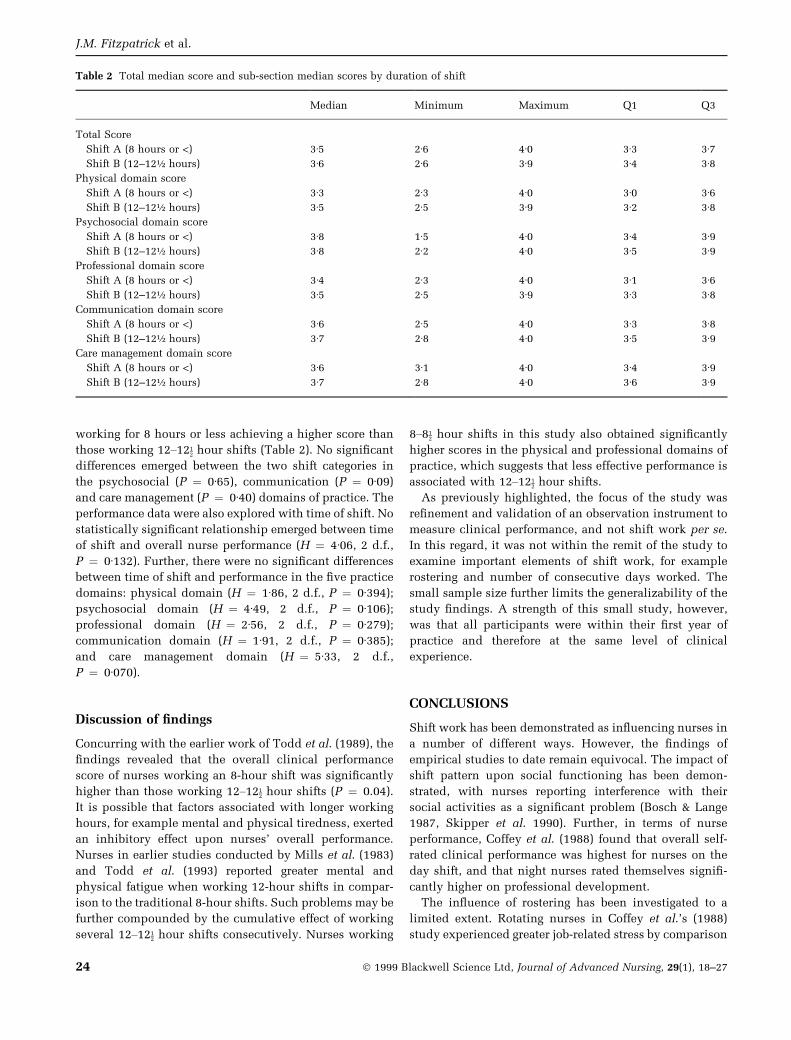
working for 8 hours or less achieving a higher score than
those working 12±1212 hour shifts (Table 2). No signi®cant
differences emerged between the two shift categories in
the psychosocial (P � 0á65), communication (P � 0á09)
and care management (P � 0á40) domains of practice. The
performance data were also explored with time of shift. No
statistically signi®cant relationship emerged between time
of shift and overall nurse performance (H � 4á06, 2 d.f.,
P � 0á132). Further, there were no signi®cant differences
between time of shift and performance in the ®ve practice
domains: physical domain (H � 1á86, 2 d.f., P � 0á394);
psychosocial domain (H � 4á49, 2 d.f., P � 0á106);
professional domain (H � 2á56, 2 d.f., P � 0á279);
communication domain (H � 1á91, 2 d.f., P � 0á385);
and care management domain (H � 5á33, 2 d.f.,
P � 0á070).
Discussion of ®ndings
Concurring with the earlier work of Todd et al. (1989), the
®ndings revealed that the overall clinical performance
score of nurses working an 8-hour shift was signi®cantly
higher than those working 12±1212 hour shifts (P � 0.04).
It is possible that factors associated with longer working
hours, for example mental and physical tiredness, exerted
an inhibitory effect upon nurses' overall performance.
Nurses in earlier studies conducted by Mills et al. (1983)
and Todd et al. (1993) reported greater mental and
physical fatigue when working 12-hour shifts in compar-
ison to the traditional 8-hour shifts. Such problems may be
further compounded by the cumulative effect of working
several 12±1212 hour shifts consecutively. Nurses working
8±812 hour shifts in this study also obtained signi®cantly
higher scores in the physical and professional domains of
practice, which suggests that less effective performance is
associated with 12±1212 hour shifts.
As previously highlighted, the focus of the study was
re®nement and validation of an observation instrument to
measure clinical performance, and not shift work per se.
In this regard, it was not within the remit of the study to
examine important elements of shift work, for example
rostering and number of consecutive days worked. The
small sample size further limits the generalizability of the
study ®ndings. A strength of this small study, however,
was that all participants were within their ®rst year of
practice and therefore at the same level of clinical
experience.
CONCLUSIONS
Shift work has been demonstrated as in¯uencing nurses in
a number of different ways. However, the ®ndings of
empirical studies to date remain equivocal. The impact of
shift pattern upon social functioning has been demon-
strated, with nurses reporting interference with their
social activities as a signi®cant problem (Bosch & Lange
1987, Skipper et al. 1990). Further, in terms of nurse
performance, Coffey et al. (1988) found that overall self-
rated clinical performance was highest for nurses on the
day shift, and that night nurses rated themselves signi®-
cantly higher on professional development.
The in¯uence of rostering has been investigated to a
limited extent. Rotating nurses in Coffey et al.'s (1988)
study experienced greater job-related stress by comparison
Table 2 Total median score and sub-section median scores by duration of shift
Median Minimum Maximum Q1 Q3
Total Score
Shift A (8 hours or <) 3á5 2á6 4á0 3á3 3á7Shift B (12±12� hours) 3á6 2á6 3á9 3á4 3á8
Physical domain score
Shift A (8 hours or <) 3á3 2á3 4á0 3á0 3á6Shift B (12±12� hours) 3á5 2á5 3á9 3á2 3á8
Psychosocial domain score
Shift A (8 hours or <) 3á8 1á5 4á0 3á4 3á9Shift B (12±12� hours) 3á8 2á2 4á0 3á5 3á9
Professional domain score
Shift A (8 hours or <) 3á4 2á3 4á0 3á1 3á6Shift B (12±12� hours) 3á5 2á5 3á9 3á3 3á8
Communication domain score
Shift A (8 hours or <) 3á6 2á5 4á0 3á3 3á8Shift B (12±12� hours) 3á7 2á8 4á0 3á5 3á9
Care management domain score
Shift A (8 hours or <) 3á6 3á1 4á0 3á4 3á9Shift B (12±12� hours) 3á7 2á8 4á0 3á6 3á9
J.M. Fitzpatrick et al.
24 Ó 1999 Blackwell Science Ltd, Journal of Advanced Nursing, 29(1), 18±27

with their counterparts. Further, nurses working internal
rotation and irregular systems of duty rostering in Barton's
(1995) study experienced poorer psychological health,
chronic fatigue, more social and domestic disruption,
more disrupted sleep, and more job dissatisfaction than
those working ¯exible systems. Rotating nurses in Ver-
haegen et al.'s (1987) study reported more health com-
plaints than full- and part-time night nurses and nurses
who worked alternating schedules. In particular, those
who alternated with nights were more likely to experience
sleep disorders, according to Niedhammer et al.'s (1994)
study. Such ®ndings underline the potentially negative
impact of rotation and irregular systems of rostering for
nurses' well being, with Seccombe and Smith (1996)
noting an increasing number of nurses working internal
rotation within the health service.
Con¯icting ®ndings have emerged for those studies
which have examined the in¯uence of duration of shift.
The 12-hour shift system has been demonstrated as having
a negative impact upon nurses' personal lives (Todd et al.
1989) and mental and physical ability (Mills et al. 1983,
Todd et al. 1989). Nurses in Todd et al.'s (1989) study
indicated a preference for returning to the 8-hour shift
system. In contrast, the nurse cohort in Mills et al.'s (1983)
and Gillespie and Curzio's (1996) studies preferred to work
the 12-hour shift.
Limited empirical investigation of the impact of shift
duration upon quality of care has been conducted,
and disparity between ®ndings is evident. The work of
Todd et al. (1989) and the present study ®ndings revealed
that quality of care decreased with the 12-hour shift.
Further, Reid et al. (1991) reported that educational
activity also decreased under the 12-hour shift. By
contrast, Mills et al.'s (1983) earlier US study reported
no signi®cant differences between the quality of care
delivered during 8- and 12-hour shifts. Interpretation of
such ®ndings demands caution in view of noted
methodological limitations. Moreover, it is dif®cult to
compare the ®ndings of such studies since different
measures of quality have been utilized and researchers
have focused upon different aspects of shift work. Of
further signi®cance, as Bohle and Tilley (1989) have
identi®ed, many studies examining shift work have
adopted a cross-sectional design, with inadequate use of
control groups. Such issues provide an important focus for
the design and management of future research. A
prospective longitudinal study is required, to examine
the impact of 8- and 12-hour shift systems upon nurses.
Sample design should be considered carefully, with
adequate control for the effects of extraneous variables.
Taking into consideration previous work (Todd et al.
1989, Barton et al. 1993), pattern, rostering, duration of
shift and number of consecutive shifts worked should be
incorporated into the research design. The impact of shift
work upon process (i.e. examination of the quality of care)
as well as outcomes for nurses (e.g. personal and
professional), consumers (e.g. satisfaction, length of stay)
and the organization (e.g. unplanned absenteeism, cost-
effectiveness and productivity) should also be investi-
gated.
In conclusion, every attempt should be made to
enhance the well-being and effectiveness of the nursing
workforce, and it is argued that effective management of
nurses' shift work represents a key strategy for achieving
this. The latter also has the potential to generate positive
outcomes for consumers and for employing organizations.
Research evidence, however, regarding the strengths and
limitations of different systems of shift work remains
ambiguous. In the meantime, Seccombe and Smith's
(1996) large survey of Royal College of Nursing members
(n � 4347; 73% response rate) has revealed the increas-
ing workload stress being experienced by nurses, with
almost three-®fths of the sample claiming to have worked
in excess of their contracted hours in their latest working
week. This survey also noted an increased proportion of
nurses working internal rotation although it was not their
desired working pattern (Seccombe et al. 1993). Twelve-
hour shifts were only worked by a minority of the
respondents, but Seccombe and Smith (1996) noted that
their use had increased from 2% in 1993 to 5% in 1996.
The ®ndings highlight the need for sound research in this
area and the incorporation of relevant ®ndings into
management policy, if the ef®ciency and the effectiveness
of the nursing workforce is to be maximized.
Acknowledgement
The authors were engaged in a study to re®ne and validate
the King's Nurse Performance Scale commissioned by
Miss Wilma MacPherson, Director of Quality and Nursing,
Guy's and St Thomas' Hospitals NHS Trust and assisted
by the generosity of Guy's and St Thomas' Trustees. This
paper draws upon this work.
References
Alward R.R. & Monk T.H. (1990) A comparison of rotating shift
and permanent night nurses. International Journal of Nursing
Studies 27(3), 297±302.
Barton J. (1994) Choosing to work at night: a moderating in¯uence
on individual tolerance to shift work. Journal of Applied
Psychology 79(3), 449±454.
Barton J. (1995) Is ¯exible rostering helpful? Nursing Times 91(7),
32±35.
Barton J. & Folkard S. (1991) The response of day and night nurses
to their work schedules. Journal of Occupational Psychology
64, 207±218.
Bauer I. (1993) Nurses' perceptions of the ®rst hour of the morning
shift (06á00±07á00) in a German hospital. Journal of Advanced
Nursing 18, 932±937.
Experience before and throughout the nursing career Shift work
Ó 1999 Blackwell Science Ltd, Journal of Advanced Nursing, 29(1), 18±27 25
Beil-Hildebrand M. (1996) Nurse absence Ð the causes and the
consequences. Journal of Nursing Management 4, 11±17.
Benne K.D. & Bennis W. (1959) Role of the professional nurse.
American Journal of Nursing 59(2), 196±198.
Bohle P. & Tilley A.J. (1989) The impact of night work on
psychological well-being. Ergonomics 32(9), 1089±1099.
Bosch L.H.M. & Lange W.A.M. (1987) Shift work in health care.
Ergonomics 30(5), 773±791.
Bradshaw P. (1995) The recent health reforms in the United
Kingdom: some tentative observations on their impact on
nurses in hospital. Journal of Advanced Nursing 21(5), 975±
979.
Budnick L.D., Lerman S.E., Baker T.L., Jones H. & Czeisler C.A.
(1994) Sleep and alertness in a 12 hour rotating shift work
environment. Journal of Occupational Medicine 36(12), 1295±
1300.
Coffey L.C., Skipper J.K. & Jung F.D. (1988) Nurses and shift work:
effects on job performance and job-related stress. Journal of
Advanced Nursing 13, 245±254.
Dowling S., Barrett S. & West R. (1995) With nurse practitioners,
who needs house of®cers? British Medical Journal 311(7000),
309±313.
Feldt L.S. & Brennan R.L. (1989) Reliability. In Educational
Measurement (Linn R.L. ed.), Macmillan, Phoenix, pp. 105±
146.
Findlay J. (1994) Shifting time. Nursing Times 90(2), 42±44.
Fitzpatrick J.M., While A.E. & Roberts J.D. (1997) Measuring
clinical performance: development of the King's Nurse Perfor-
mance Scale. International Journal of Nursing Studies 34(3),
222±230.
Gillespie A. & Curzio J. (1996) A comparison of a 12 hour and
eight hour shift system. Nurses Times 96(39), 36±39.
Gold D.R., Rogacz S., Tosteson T.D., Baum T.M., Speizer F.E. &
Czeisler C.A. (1992) Rotating shift work, sleep and accidents
related to sleepiness in hospital nurses. American Journal of
Public Health 82(7), 1011±1014.
Goldstone L.A., Ball J.A. & Collier M.M. (1983) MONITOR: An
Index of the Quality of Nursing Care for Acute Medical and
Surgical Wards. Newcastle upon Tyne Polytechnic Products,
Newcastle upon Tyne.
Harrington H.A. & Thesis E.C. (1968) Institutional factors per-
ceived by baccalaureate graduates as in¯uencing their perfor-
mance as staff nurses. Nursing Research 17(3), 228±235.
Healy D. (1997) Blues in the night. Nursing Times 93(15), 26±
28.
Institute of Personnel Development (1993) The Adaptation of
Working Time: EU Directive on Working Time (93/104). IPD,
London.
Jamal M. (1981) Shift work related to job attitudes, social
participation and withdrawal behaviour: a study of nurses
and industrial workers. Personnel Psychology 34, 535±547.
Jelinek R.C., Hausman R.N., Hegyvary S.T. & Newman J.F. (1974)
A Methodology for Monitoring Quality of Nursing Care. US
Department of Health, Education and Welfare, Bethesda, Mary-
land.
Jowett S., Walton I. & Payne S. (1994) Challenges and Change in
Nurse Education: A Study of the Implementation of Project
2000. NFER, Slough.
Krausz M. & Freibach N. (1983) Effects of ¯exible working time for
employed women upon satisfaction, strains, and absenteeism.
Journal of Occupational Psychology 56, 155±159.
Lanuza D.M. (1976) Circadian rhythms of mental ef®ciency and
performance. Nursing Clinics of North America 11(4), 583±594.
McCloskey J.C. (1983) Nursing education and job effectiveness.
Nursing Research 32(1), 53±59.
Messick S. (1984) The psychology of educational measurement.
Journal of Educational Measurement 21(3), 215±238.
Mills M.E., Arnold B. & Wood C.M. (1983) Core-12: a controlled
study of the impact of 12-hour scheduling. Nursing Research
32(6), 356±361.
Milne D. & Watkins F. (1986) An evaluation of the effects of shift
rotation on nurses' stress, coping and strain. International
Journal of Nursing Studies 23(2), 139±146.
Niedhammer I., Lert F. & Marne M.J. (1994) Effects of shift work
on sleep among French nurses. Journal of Occupational
Medicine 36(6), 667±674.
Northcott N. & Facey S. (1995) Twelve-hour shifts: helpful or
hazardous to patients? Nursing Times 91(7), 29±31.
Nunally J.C. (1978) Psychometric Theory. McGraw-Hill, New
York.
Redfern S.J. (1978) Absence and wastage in trained nurses: a
selective review of the literature. Journal of Advanced Nursing
3, 231±249.
Redfern S.J. & Norman I.J. with Tomalin D.A., Oliver S. & Jacka K.
(1994) The Validity of Quality Assessment Instruments in
Nursing. Department of Health, London.
Reid N., Todd C. & Robinson G. (1991) Educational activities on
wards under 12 hour shifts. International Journal of Nursing
Studies 28(1), 47±54.
Royal College of Nursing (1997) Health and Safety at Work 6 Ð
Shifting the Balance: Towards the Best Practice in Shift
Working and Patient Care. RCN, London.
Schwirian P. (1978) Evaluating the performance of nurses: a
multidimensional approach. Nursing Research 27, 347±351.
Seccombe I. & Smith G. (1996) In the Balance: Registered Nurse
Supply and Demand. Report No. 315. Institute of Employment
Studies, University of Sussex.
Seccombe I., Ball J. & Patch A. (1993) The Price of Commitment:
Nurses' Pay, Careers and Prospects. Report No. 251. Institute of
Manpower Studies, University of Sussex, Brighton.
Skipper J.K., Jung F.D. & Coffey L.C. (1990) Nurses and shift work:
effects on physical and mental depression. Journal of Advanced
Nursing 15, 835±842.
Smithers F. (1995) The pattern and effect of on call work in
transplant co-ordinators in the United Kingdom. International
Journal of Nursing Studies 32(5), 469±483.
Swiercz P.M. (1983) Determinants of registered nurses attitudes
toward collective bargaining. Unpublished PhD Dissertation,
VPI & SU, Blacksburg, Virginia.
Todd C., Reid N.& RobinsonG. (1989) The qualityofnursing care on
wards working eight and twelve hour shifts: a repeated measures
study using the MONITOR index of quality of care. International
Journal of Nursing Studies 26(4), 359±368.
Todd C., Robinson G. & Reid N. (1993) 12 hour shifts: job
satisfaction of nurses. Journal of Nursing Management 1, 215±
220.
J.M. Fitzpatrick et al.
26 Ó 1999 Blackwell Science Ltd, Journal of Advanced Nursing, 29(1), 18±27

United Kingdom Central Council for Nursing, Midwifery and
Health Visiting (1992). The Scope of Professional Practice.
UKCC, London.
Verhaegen P., Cober R., De Smedt M., Dirkx J., Kerstens J.,
Ryvers D. & Van Daele P. (1987) The adaptation of night nurses
to different work schedules. Ergonomics 30(9), 1301±1309.
Vries-Griever A.H.G. & Meijman T.F. (1987) The impact of
abnormal hours of work on various modes of information
processing: a process model on human costs of performance.
Ergonomics 30(9), 1287±1299.
While A.E. (1994) Competence versus performance: which is the
more important? Journal of Advanced Nursing 20, 525±531.
White E., Riley E., Davies S. & Twinn S. (1994) A Detailed Study
of the Relationship between Teaching, Support, Supervision
and Role Modelling in Clinical Areas within the Context of
P2000 Courses. English National Board for Nursing, Midwifery
and Health Visiting, London.
Yoshitake H. (1978) Three characteristic patterns of subjective
fatigue symptoms. Ergonomics 10, 341.
Experience before and throughout the nursing career Shift work
Ó 1999 Blackwell Science Ltd, Journal of Advanced Nursing, 29(1), 18±27 27
Related Documents











![[Nurse Transition Coach Model] · Reducing Readmissions • Upon admission we establish a mutually responsible relationship with patient and ... – Readmission Review Weekly Meeting](https://static.cupdf.com/doc/110x72/5fe062e33bda0230f53bf352/nurse-transition-coach-model-reducing-readmissions-a-upon-admission-we-establish.jpg)