Sex cord-stromal tumors of the testis in children. A clinicopathologic report from the Italian TREP project ☆ Giovanni Cecchetto a, ⁎ , Rita Alaggio b , Gianni Bisogno c , Calogero Virgone a , Patrizia Dall'Igna a , Monica Terenziani d , Renata Boldrini e , Vittoria D'Onofrio f , Andrea Ferrari d , Gabriella Bernini g a Department of Pediatrics, Division of Pediatric Surgery, University of Padua, Italy b Department of Medical and Diagnostic Sciences and Special Therapies, University of Padua, Italy c Division of Hematology Oncology, Department of Pediatrics, University Hospital of Padua, Italy d Pediatric Oncology Unit, Istituto Tumori of Milan, Italy e Department of Pathology, Pediatric Hospital “Bambino Gesù,” Rome, Italy f Department of Pathology, Pediatric Hospital Santo Bono, Naples, Italy g Division of Pediatric Hematology Oncology, Pediatric Hospital Meyer, Florence, Italy Received 30 November 2009; revised 26 February 2010; accepted 27 February 2010 Key words: Children; Testicular neoplasm; Sex cord-stromal tumors Abstract Purpose: Testicular sex cord-stromal tumors (SCSTs) are very rare in children and include a variety of neoplasms with different clinical features and biologic behavior. Aim of the study was to report the clinical findings and results observed in a series of patients with testicular SCST, registered in a multi- institutional Italian network on rare tumors in children and adolescents. Materials and Methods: The records of 11 patients, enrolled in 6 Italian centers from January 2000 to December 2008, were reviewed. The Children's Oncology Group (COG) staging system was adopted. Chemotherapy was recommended in patients with incomplete surgery or metastatic disease. Results: A testicular mass was the most common symptom. All patients underwent primary removal of the tumor; orchiectomy with high ligation of spermatic cord was performed in 7 and tumor enucleation in 4. At histology, 4 patients had Leydig cell tumors, 4 juvenile granulosa cell tumors, 1 Sertoli cell tumor, 1 incompletely differentiated SCST, and 1 SCST with an intermediate pattern Sertoli cell tumor/ mixed form. The histology of 8 of 11 cases was reviewed and investigated through immunohisto- chemical stains. Ten children were in stage I; 1 patient, who did not undergo hemiscrotectomy after enucleation through a transscrotal access, was considered stage II. All the patients are in first complete remission (mean follow-up, 59 months; range, 8-94). ☆ Partially supported by a Grant from “Fondazione Cassa Di Risparmio Di Padova e Rovigo” and from the “Fondazione Citta' della Speranza”, Padova. ⁎ Corresponding author. Department of Pediatrics, Pediatric Surgery, University of Padua, 35128 Padua, Italy. Tel.: +39 049 8213681; fax: +39 049 8211781. E-mail address: [email protected] (G. Cecchetto). www.elsevier.com/locate/jpedsurg 0022-3468/$ – see front matter © 2010 Elsevier Inc. All rights reserved. doi:10.1016/j.jpedsurg.2010.02.120 Journal of Pediatric Surgery (2010) 45, 1868–1873

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

www.elsevier.com/locate/jpedsurg
Journal of Pediatric Surgery (2010) 45, 1868–1873
Sex cord-stromal tumors of the testis in children.A clinicopathologic report from the ItalianTREP project☆
Giovanni Cecchetto a,⁎, Rita Alaggio b, Gianni Bisogno c, Calogero Virgone a,Patrizia Dall'Igna a, Monica Terenziani d, Renata Boldrini e, Vittoria D'Onofrio f,Andrea Ferrari d, Gabriella Bernini g
aDepartment of Pediatrics, Division of Pediatric Surgery, University of Padua, ItalybDepartment of Medical and Diagnostic Sciences and Special Therapies, University of Padua, ItalycDivision of Hematology Oncology, Department of Pediatrics, University Hospital of Padua, ItalydPediatric Oncology Unit, Istituto Tumori of Milan, ItalyeDepartment of Pathology, Pediatric Hospital “Bambino Gesù,” Rome, ItalyfDepartment of Pathology, Pediatric Hospital Santo Bono, Naples, ItalygDivision of Pediatric Hematology Oncology, Pediatric Hospital Meyer, Florence, Italy
Received 30 November 2009; revised 26 February 2010; accepted 27 February 2010
8
0d
Key words:Children;Testicular neoplasm;Sex cord-stromal tumors
AbstractPurpose: Testicular sex cord-stromal tumors (SCSTs) are very rare in children and include a variety ofneoplasms with different clinical features and biologic behavior. Aim of the study was to report theclinical findings and results observed in a series of patients with testicular SCST, registered in a multi-institutional Italian network on rare tumors in children and adolescents.Materials and Methods: The records of 11 patients, enrolled in 6 Italian centers from January 2000 toDecember 2008, were reviewed. The Children's Oncology Group (COG) staging system was adopted.Chemotherapy was recommended in patients with incomplete surgery or metastatic disease.Results: A testicular mass was the most common symptom. All patients underwent primary removal ofthe tumor; orchiectomy with high ligation of spermatic cord was performed in 7 and tumor enucleationin 4. At histology, 4 patients had Leydig cell tumors, 4 juvenile granulosa cell tumors, 1 Sertoli celltumor, 1 incompletely differentiated SCST, and 1 SCST with an intermediate pattern Sertoli cell tumor/mixed form. The histology of 8 of 11 cases was reviewed and investigated through immunohisto-chemical stains. Ten children were in stage I; 1 patient, who did not undergo hemiscrotectomy afterenucleation through a transscrotal access, was considered stage II. All the patients are in first completeremission (mean follow-up, 59 months; range, 8-94).
☆ Partially supported by a Grant from “Fondazione Cassa Di Risparmio Di Padova e Rovigo” and from the “Fondazione Citta' della Speranza”, Padova.⁎ Corresponding author. Department of Pediatrics, Pediatric Surgery, University of Padua, 35128 Padua, Italy. Tel.: +39 049 8213681; fax: +39 049
211781.E-mail address: [email protected] (G. Cecchetto).
022-3468/$ – see front matter © 2010 Elsevier Inc. All rights reserved.oi:10.1016/j.jpedsurg.2010.02.120

1869SCSTs of the testis in children
Conclusions: Our experience confirmed the rarity of testicular SCST. They have to be considered in thedifferential diagnosis of testicular solid masses, taking into account that hormonal signs are present in aminority of cases. All patients were cured with surgery alone. The sparing surgery represented a choicein selected cases.© 2010 Elsevier Inc. All rights reserved.
Testicular sex cord-stromal tumors (SCSTs) are very rarein children and adolescents. They include a heterogeneousgroup of neoplasms developing from nongerminative tissue,with different clinical features and biologic behavior. Leydigcell tumors (LCTs), Sertoli cell tumors (SCTs), juvenilegranulosa cell tumors (JGCTs), and undifferentiated celltumors are the main histologic types, accounting for about6% to 8% of all testicular neoplasms in children, with 2 peaksof incidence, within few months after birth and aroundpuberty, respectively [1,2].
All these forms generally present with a painless testicularmass, whereas hormonal manifestations, such as isosexualpseudoprecocity or estrogenic manifestations, occur in 10%to 20% of the cases [2-4]. They generally have a benignbehavior [2,5,6]; however, rare cases with malignant featuresare reported in literature [7,8].
Since 2000, the patients with testicular SCST have beenregistered within the Tumori Rari in Etá Pediatrica (TREP)project, an Italian multi-institutional network on rare tumorsin children and adolescents, which was launched under theauspices of the Italian Association of Pediatric Oncology andthe Italian Society of Pediatric Surgery. We report theclinical findings, treatment, and outcome observed inpatients with testicular SCST, with the purposes to evaluatethe efficacy of our clinical approach and to offer acontribution to the literature data.
1. Materials and methods
The Italian Study on Rare Tumors in children is calledTREP project, an acronym that in Italian indicates TumoriRari in Etá Pediatrica. This study represents the first Italianmulti-institutional network on rare tumors and was intendedto register all children and adolescents up to the age of18, affected by tumors with an incidence of less than 2 casesper million, and not treated in the current national orinternational protocols [9]. Besides the registration of cases,the TREP project offered diagnostic and therapeuticrecommendations for every histotype according to the recentdata of the literature and helped physicians in approachingrare neoplasms.
The recommended diagnostic workup for testicular SCSTwas similar to that adopted for germ cell tumors. Patientswith a mass of the testis had to be evaluated with scrotalultrasound, abdominal computed tomographic (CT) scan,and serologic markers (α-fetoprotein and β-human chorionic
gonadotropin [HCG]). When endocrinologic abnormalitieswere suspected, an accurate hormonal assessment withevaluation of serologic levels of testosterone, androstene-dione, dehydroepiandosterone sulfate, and 17-hydroxypro-gesterone was mandatory.
The surgical complete excision of the tumor was thetreatment of choice; if this was not feasible, a surgical biopsywas indicated. The inguinal orchiectomy with high ligationof the spermatic cord was the suggested approach, afterfrozen biopsy examination of the tumor. When thepreoperative serologic levels of α-fetoprotein and β-HCGcould rule out a malignant germ cell tumor, an enucleation ofthe mass through an inguinal approach was accepted; thefeasibility of such a procedure depended upon tumor size andsite in the gonad. A reexcision was recommended in case aprimary scrotal approach had been performed or whenneoplastic residuals were left. The surgical exploration ofretroperitoneal lymph nodes was not indicated if abdominalCT scan was normal.
Information concerning each patient was obtainedprospectively through special printed forms from thephysicians in charge, but the records of all the cases werereviewed for this analysis. Informed consent was obtainedfor all patients enrolled into the study.
All patients were grouped after the first surgical approachaccording to the COG staging system proposed for germ celltumors (Fig. 1). Although testicular SCST do not have anaggressive behavior and generally are cured with surgery, acisplatinum-based chemotherapy (cisplatin, 25 mg/m2 days1-4; etoposide, 100 mg/m2 days 1-4; bleomycin, 15 mg/m2
day 2) was provided for patients with malignant localizeddisease, who had undergone incomplete excision or initialbiopsy, or in the presence of metastatic spread. Three courseswere suggested for stage II patients and 4 courses for stage IIIand IV.
A revision of the histologic specimens by the pathologistsof the TREP panel was highly recommended. The H&E-stained slides, paraffin blocks, and/or unstained sectionswere requested. All available H&E-stained sections andimmunostains were reviewed, and tumors were categorizedusing standard criteria according to the current World HealthOrganization classification [10]. Only if further materialcould be available, other immunostains had to be performedaccording to standardized protocols. The immunohistochem-ical panel included the classic markers, such as cytokeratins(AE1-3, CAM5.2), smooth muscle actin, and vimentin;inhibin and Wilms' tumor protein 1 (WT1), recentlyidentified as markers of SCSTs, were also analyzed, as
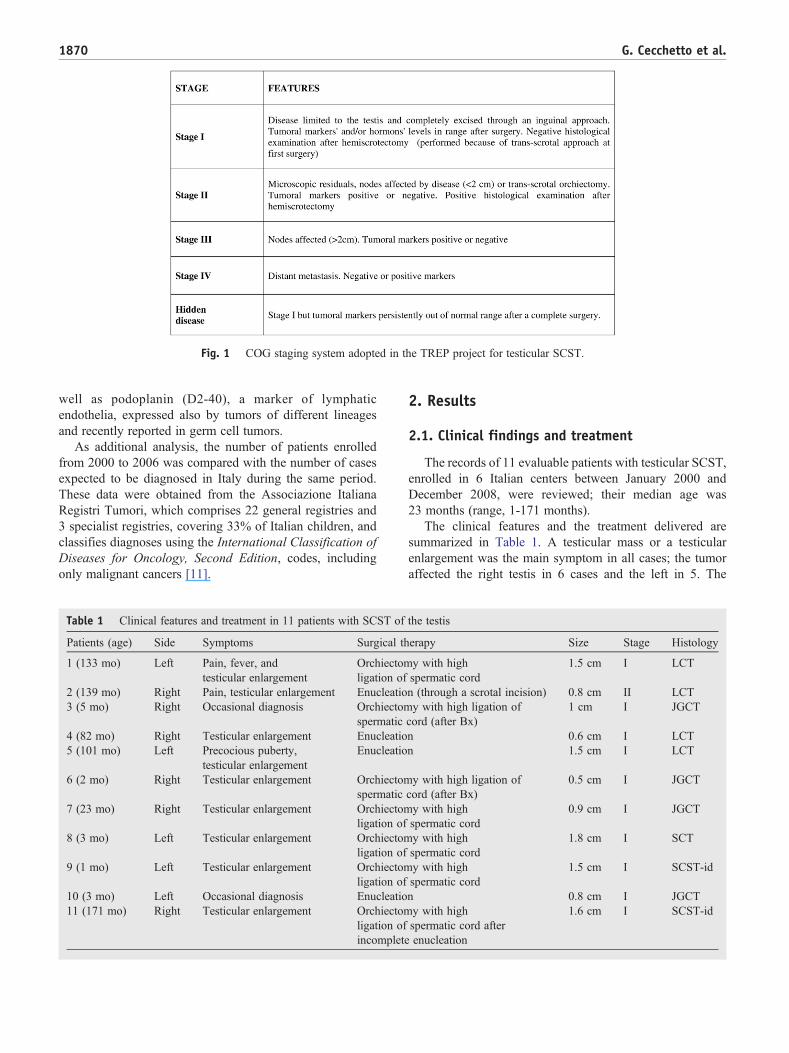
Fig. 1 COG staging system adopted in the TREP project for testicular SCST.
1870 G. Cecchetto et al.
well as podoplanin (D2-40), a marker of lymphaticendothelia, expressed also by tumors of different lineagesand recently reported in germ cell tumors.
As additional analysis, the number of patients enrolledfrom 2000 to 2006 was compared with the number of casesexpected to be diagnosed in Italy during the same period.These data were obtained from the Associazione ItalianaRegistri Tumori, which comprises 22 general registries and3 specialist registries, covering 33% of Italian children, andclassifies diagnoses using the International Classification ofDiseases for Oncology, Second Edition, codes, includingonly malignant cancers [11].
Table 1 Clinical features and treatment in 11 patients with SCST of
Patients (age) Side Symptoms Surgical th
1 (133 mo) Left Pain, fever, andtesticular enlargement
Orchiectomligation of
2 (139 mo) Right Pain, testicular enlargement Enucleatio3 (5 mo) Right Occasional diagnosis Orchiectom
spermatic4 (82 mo) Right Testicular enlargement Enucleatio5 (101 mo) Left Precocious puberty,
testicular enlargementEnucleatio
6 (2 mo) Right Testicular enlargement Orchiectomspermatic
7 (23 mo) Right Testicular enlargement Orchiectomligation of
8 (3 mo) Left Testicular enlargement Orchiectomligation of
9 (1 mo) Left Testicular enlargement Orchiectomligation of
10 (3 mo) Left Occasional diagnosis Enucleatio11 (171 mo) Right Testicular enlargement Orchiectom
ligation ofincomplete
2. Results
2.1. Clinical findings and treatment
The records of 11 evaluable patients with testicular SCST,enrolled in 6 Italian centers between January 2000 andDecember 2008, were reviewed; their median age was23 months (range, 1-171 months).
The clinical features and the treatment delivered aresummarized in Table 1. A testicular mass or a testicularenlargement was the main symptom in all cases; the tumoraffected the right testis in 6 cases and the left in 5. The
the testis
erapy Size Stage Histology
y with highspermatic cord
1.5 cm I LCT
n (through a scrotal incision) 0.8 cm II LCTy with high ligation of
cord (after Bx)1 cm I JGCT
n 0.6 cm I LCTn 1.5 cm I LCT
y with high ligation ofcord (after Bx)
0.5 cm I JGCT
y with highspermatic cord
0.9 cm I JGCT
y with highspermatic cord
1.8 cm I SCT
y with highspermatic cord
1.5 cm I SCST-id
n 0.8 cm I JGCTy with highspermatic cord afterenucleation
1.6 cm I SCST-id

Table 2 Immunohistochemical and pathologic findings in 8/11 cases
Patients (age) Histology α-Inhibin Podoplanin WT-1 Cytokeratin Vimentin Smooth muscle actin Protein-S 100
1 (133 mo) LCT Positive Negative Positive Positive Not available Not available Not available2 (139 mo) LCT Positive Negative Positive Positive Not available Not available Positive3 (5 mo) JGCT Positive Not available Not available Not available Not available Positive Not available4 (82 mo) LCT Positive Not available Not available Not available Positive Not available Not available8 (3 mo) SCT Positive Negative Positive Not available Positive Not available Not available9 (1 mo) SCST-id Negative Negative Negative Negative Positive Not available Not available10 (3 mo) JGCT Positive Negative Positive Positive Not available Not available Positive11 (171 mo) SCST-id Positive Not available Not available Not available Positive Positive Positive
1871SCSTs of the testis in children
testicular enlargement was the first sign in 9 and wasassociated with pain in 2, fever in 1, and suspected precociouspuberty in 1. In 2 patients, the tumor was occasionallydetected during ultrasound (US) performed because ofundescended testis at the age of 3 and 5 months, respectively.No pathologic levels of serologic markers (α-fetoprotein andβ-HCG) were detected in any case; the endocrinology profileperformed in the case with suspected precocious pubertyresulted normal. Besides the US, which showed a solid massin the testis in all the cases, no other instrumentalinvestigations were performed before the surgical approach.
All patients underwent primary surgery with differentapproaches. An inguinal orchiectomy with high ligation ofthe spermatic cord was performed in seven (in 3 of them, aninguinal approach had been done before, consisting in abiopsy of the mass in two and enucleation with suspectedresiduals in one). A tumor enucleation was done in four(through an inguinal approach in three, through a scrotalincision in one); after that, no other procedures wereperformed. The mean diameter of the mass was 1.1 cm(range, 0.5-1.8 cm).
The staging evaluation, including abdominal CT scan ormagnetic resonance imaging and chest x-ray, was completedafter surgery; no regional or distant spread was detected. Tenchildren were considered stage I and did not receive furthertherapy. The patient in whom the tumor enucleation had beenperformed through a transscrotal access, but hemiscrotect-omy was not performed, was cautiously classified as stage II;however, he did not receive chemotherapy because ofphysician decision.
At the time of this report, all patients are alive in firstcomplete remission with a mean follow-up of 59 months(range, 8-94 months).
2.2. Pathologic findings
The histologic diagnosis was LCT in 4 patients, JGCT in4, incompletely differentiated SCST in 2, and SCT in 1. Thehistologic review was performed in 8 of 11 cases andconfirmed the diagnosis in 7 cases; in one case, a JGCT hadbeen originally misdiagnosed as a mixed gonadal stromaltumor. Juvenile granulosa cell tumors were characterizedby a typical follicular pattern showing large follicles
bordered by medium-sized cells with pale eosinophiliccytoplasm and oval nuclei with occasional nucleoli.Focally, there were areas of hyalinization with evidenceof cells arranged in a trabecular pattern. Mitoses wereabsent or rare. Leydig cell tumor displayed nests and sheetsof cells with abundant eosinophilic cytoplasm and frequentcytoplasmic vacuoles, round nuclei, and small nucleoli. Inone case, an abundant fibrous stroma with discreetinflammatory lymphocytic infiltrate was present, and thecells were focally arranged in a trabecular pattern. Reinke'scrystals were not observed in any case. Mitoses were absentin all cases. Two tumors showed elongated cells withround-oval nuclei and finely dispersed chromatin arrangedin short fascicles with evidence, at the periphery, ofscattered cords and tubules characteristic of SCTs. Thesemorphological findings were typical of an incompletelydifferentiated SCST. Mitoses were only rare or absent inone case. A single SCT showed tubules lined by a layer ofcells with amphophilic cytoplasm frequently containingsmall vacuoles. In these cases, the mitotic rate was high(40/10 high-power field).
Results of the immunostains are summarized in Table 2.Vimentin, smooth muscle actin, and protein S-100 weredetectable in all specimen examined; α-inhibin and WT-1were positive in all tumors that were evaluated, except in oneincompletely differentiated SCST (SCST-id); in this tumor,the only positive immunohistochemical marker was vimen-tin. On the other hand, podoplanin was negative in all the5 cases studied. Calretinin immunostains were performedonly in 2 cases, 1 SCST-id and 1 LCT, and both were positive.
2.3. Comparison between observed andexpected cases
According to the Associazione Italiana Registri Tumoridata, 80 patients younger than 18 years with a diagnosis ofgonadal SCST (ovarian and testicular) were to be expected inItaly for the 6-year period considered (2000-2006), that is,41 cases aged 0 to 14 and 39 cases aged 15 to 17 years.The ratio between observed and expected cases was 0.66(95% confidence interval, 0.39-1.10) in the population ofless than 15 years and 0.08 (0.02-0.24) in the 15 to 17-year-old group [11].

1872 G. Cecchetto et al.
3. Discussion
Sex cord-stromal tumors of the testes are a heterogeneousgroup of neoplasms, which are rarely encountered in thedaily pediatric surgery and pediatric oncology practice. Ourseries of 11 cases registered between 2000 and 2009demonstrate the rarity of these tumors. The recent analysisof tumor accrual included in the TREP project [11] showedthat most patients were enrolled into the study because theywere observed in prepubertal age; the older patients mayhave been treated in adult centers, and this could explain thetendency to underreport testicular SCSTs.
In most SCST, the clinical presentation is similar to that oftesticular germ cell tumors, being a mass of the testis the onlysymptom, whereas hormonal signs are evident in a minorityof cases [12-14]. Leydig cell tumors represent the mostcommon histotype; they appear between 5 and 10 years ofage or in pubertal boys and are bilateral in 10% of the cases[15,16]; hormonal activity is observed in 20% of patients andis characterized by symptoms of isosexual pseudoprecocitybecause of androgenic hormone production [17,18]. Sertolicell tumors are more commonly diagnosed before 1 year ofage and are considered to be hormonally silent, butoccasionally, they can produce gynecomastia because ofestrogenic secretion; they may occur in association withPeutz-Jeghers syndrome and Carney complex [19]. Juvenilegranulosa cell tumors arise predominantly in neonates andinfants [12,20,21] and may be associated with ambiguousgenitalia or abnormal sex chromosomes [22]. The group ofundifferentiated tumors, composed by Sertoli, Leydig, andundifferentiated cells, are characterized by mixed clinicaland histologic features [23].
In our series, the 4 patients with JGCT and those with STwere younger than 1 year; the age in the group of patientswith LCT was between 82 and 139 months. Symptoms werenonspecific in almost all the patients, and only in one case,slight endocrine signs were suspected preoperatively but notconfirmed at serologic evaluation.
In the last years, serum inhibin B has obtainedconsideration as a marker for stromal ovarian and testicularSCST [12,24] also in pediatric patients. Its evaluation hasbeen recently introduced in our study.
Testicular SCST generally do not have an aggressivebehavior; LCTs are less aggressive in children than in adults,and only few malignant forms are described [2]. Juvenilegranulosa cell tumors are considered borderline tumors; nolocally advanced, metastatic, or relapsed cases are reported.Also, SCTs are considered low-grade tumors; however, 4cases with a metastatic relapse were described [8]. Sporadiccases of metastatic undifferentiated stromal tumors are alsoreported in some series [2,7].
Some authors defined an SCST as malignant only whenspecific histologic features were detected, such as vascularinvasion, high mitotic index, and tumor necrosis [2,8]. Thewide morphological range of SCST makes their diagnosisdifficult and represents a possible diagnostic pitfall,
mimicking various other tumors including both germ cellstumors and mesenchymal lesions.
Most of our cases showed the typical morphology of thedifferent subtypes that made the diagnosis straightforward.The 2 SCST-id, instead, were characterized by areascomposed by elongated cells, arranged in short fascicles,mimicking mesenchymal tumors. Immunohistochemistryplayed an important role for these tumors; vimentin wasexpressed in both cases, whereas inhibin and WT1 werenegative in one case, as already reported in other series[25,26]. In the other histotypes, inhibin and WT-1 confirmedtheir liability as markers of SCST in analogy to their ovariancounterpart. Podoplanin, a proved marker of germ celltumors [27,28], resulted to be constantly negative in theseneoplasms, suggesting its possible role in ruling out theseforms. Its negativity may be useful in differential diagnosiswith mixed gonadal stromal tumors. Cytokeratins werevariously expressed in the different subtypes of SCST. Thelimited number of available section did not allow performingother immunostain such as melan-A and calretinin, which areexpressed in most stromal gonadal tumors. Two of 2 casestested for calretinin were positive.
A debated point regards the surgical approach of SCST. Inour study, the suggested treatment has been the inguinalorchiectomy with high ligation of the spermatic cord, whichis similar to the one adopted for huge or malignant testiculargerm cell tumors. However, when preoperative normal levelsof α-fetoprotein can rule out a malignant germ cell tumor andUS shows a small and encapsulated mass, a testis-sparingsurgery should be taken into consideration. In our group, 3patients were treated with enucleation of the tumor, throughan inguinal approach, and the residual testis was left in situ.Many authors suggest indeed that SCST should be managedwith a conservative procedure, with the help of intraoperativefrozen section examination [6,12,14,29,30]. If residuals areleft, an inguinal orchiectomy is indicated. Moreover,Henderson et al [31] state that if the diagnosis of an LCTin a child can be hormonally determined before surgery, theenucleation might be done also through a scrotal incision,which is generally not accepted for testicular tumors inchildren. In our opinion, larger experiences are needed toconfirm the adequacy of a transscrotal approach for SCST.
After surgery, a strict follow-up is warranted, includingphysical evaluation of the scrotum, US and CT scan ofretroperitoneal nodes and hormonal evaluation if pathologicat diagnosis [17]. Platinum-based chemotherapy is generallysuggested when residuals are left after surgery and in thoserare cases with metastatic spread [2,5].
Our experience on a multi-institutional series hasconfirmed the rarity of SCST in children and adolescentsand their favorable outcome. They have to be considered inthe differential diagnosis of testicular solid masses takinginto account that hormonal signs are present in a minority ofcases. All our patients were cured with surgery alone,including the one who underwent the removal of the tumorthrough a scrotal approach. These results confirm the

1873SCSTs of the testis in children
nonaggressive behavior of testicular SCST. Internationalcooperation is warranted to improve our understanding ofclinical behavior and biology of these tumors in childhood;the TREP experience demonstrated that cooperative studiesare feasible even on very rare tumors and may be consideredas a model for this collaboration.
Acknowledgments
The authors thank Mrs Elisa Mancini for data manage-ment. The TREP Project is partially supported by a grantfrom Fondazione Cassa Di Risparmio Di Padova e Rovigoand from the Fondazione Citta' della Speranza, Padova.
References
[1] Masiakos PT, Flynn CE, Donahue PK. Tumors causing masculizingand feminizing syndromes. Semin Pediatr Surg 1977;6(3):147-55.
[2] Thomas JC, Ross JH, Kay R. Stromal testis tumors in children: a reportfrom the Prepubertal Testis Tumor Registry. J Urol 2001;166:2338-40.
[3] Cortez JC, Kaplan GW. Gonadal stromal tumors, gonadoblastoma,epidermoid cysts, and secondary tumors of the testis in children. UrolClin North Am 1993;20(1):15-26.
[4] Ross JH, Rybicki L, Kay R. Clinical behaviour and contemporarymanagement algorithm for prepubertal testis tumors: a summary of thePrepubertal Testis Tumor Registry. J Urol 2002;168:1675-9.
[5] Talon I, Moog R, Kaufmann I, et al. Sertoli cell tumor of the testis inchildren. J Pediatr Hematol Oncol 2005;27:491-4.
[6] Treiyer A, Blanc G, Stark E, et al. Prepubertal testicular tumors:frequently overlooked. J Pediatr Urol 2007;3:480-3.
[7] Rosvoll VD, Woodard JR. Sertoli cell tumor of the testis. Cancer 1968;22:8-13.
[8] Kolon TF, Hochman HI. Malignant Sertoli cell tumor in aprepubescent boy. J Urol 1997;158:608-9.
[9] Ferrari A, Bisogno G, De Salvo GL, et al. The challenge of very raretumors in childhood: the Italian TREP Project. Eur J Cancer 2007;43:654-9.
[10] Eble JN, Sauter G, Epstein JI, Sesterhenn IA, editors. World HealthOrganization Classifications of Tumours. Pathology and Genetics ofTumours of the Urinary Tract and Male Genital Organs. Lyon: IARCPress; 2004.
[11] Pastore G, De Salvo GL, Bisogno G, et al. Evaluating access to pediatriccancer care centers of children and adolescents with rare tumors in Italy:the TREP Project. Pediatr Blood Cancer 2009;53:152-5.
[12] Shukla AR, Huff DS, Canning DA, et al. Juvenile granulosa tumor ofthe testis: contemporary clinical management and pathologicaldiagnosis. J Urol 2004;171:1900-2.
[13] Garrett JE, Cartwight PC, Snow BW, et al. Cystic testicular lesions inthe pediatric population. J Urol 2000;63(3):928-36.
[14] Metcalfe PD, Farivar-Mohseni H, Farhat W, et al. Pediatric testiculartumors: contemporary incidence and efficacy of testicular preservingsurgery. J Urol 2003;170(6):2412-5.
[15] Papatsoris AG, Triantafyllidis A, Gekas A, et al. Leydig cell tumor ofthe testis. New cases and review of the current literature. Tumori 2004;90:422-3.
[16] Ciftci AO, Bingol-Kologlu M, Senocak ME, et al. Testicular tumors inchildren. J Pediatr Surg 2001;36(12):1796-801.
[17] Petkovic V, Salemi S, Vassella E, et al. Leydig cell tumor in children:variable clinical presentation, diagnostic features, follow-up andgenetic analysis of four cases. Horm Res 2007;67:89-95.
[18] Ponce de Leon RJ, Algaba AF, Bassas AL, et al. Leydig cell tumor ofthe testis. Arch Esp Urol 2000;53:453-8.
[19] Brown B, Ram A, Clayton P, Humprey G. Conservative managementof bilateral Sertoli cell tumors of the testicle in association with theCarney complex: a case report. J Pediatr Surg 2007;42:E13-5.
[20] Peterson C, Skoog S. Prenatal diagnosis of juvenile granulosa celltumor of the testis. J Ped Urol 2008;4:472-4.
[21] Bryan DE, Cain MP, Casale AJ. Juvenile granulosa-theca cell(sex cord-stromal) tumor of the infant testis. J Urol 2003;169:1497-8.
[22] Alexiev BA, Alaish SM. Chen-Chih Sun testicular juvenile granulosacell tumor in a newborn: case report and review of the literature. Int JSurg Pathol 2007;15(3):321-5.
[23] Breckelbaum CE, Abreo F, Fowler M, et al. Undifferentiated sex cord/stromal testis tumor. Urology 2000;55(3):436.
[24] Bergadà I, Del Toro K, Katz O, et al. Serum inhibin B concentration ina prepubertal boy with gynecomastia and Peutz-Jeghers syndrome.J Pediatr Endocrinol Metab 2000;13(1):101-3.
[25] Zhao C, Bratthauer GL, Barner L, et al. Diagnostic utility of WT-1immunostaining in ovarian Sertoli cell tumors. Am J Surg Pathol 2007;31(9):1378-86.
[26] Goswitz JJ, Pettinato G, Manivel JG. Testicular sex cord-stromaltumors in children: clinicopathologic study of sixteen children andreview of the literature. Pediatr Pathol Lab Med 1996;16(3):451-70.
[27] Ordoňez NG. Podoplanin: a novel diagnostic immunohistochemicalmarker. Adv Anat Pathol 2006;13:83-8.
[28] Schacht V, Dadras SS, Johnson LA, et al. Up-regulation of thelymphatic marker podoplanin, a mucin-type transmembrane glyco-protein, in human squamous cell carcinomas and germ cell tumors. AmJ Pathol 2005;166(3):913-21.
[29] Pohl HS, Shukla AR, Metcalf PD, et al. Prepubertal testis tumors:actual prevalence rate of histological types. J Urol 2004;172:2370-2.
[30] Valla JS. Testis-sparing surgery for benign testicular tumors inchildren. J Urol 2001;165:2280-3.
[31] Henderson CG, Ahmed AA, Sesterhenn I, et al. Enucleation forprepubertal Leydig cell tumor. J Urol 2006;176:703-5.
Related Documents











