Serum ferritin is associated with markers of insulin resistance in Japanese men but not in women Ngoc Minh Pham a, ⁎ , Akiko Nanri a , Siyan Yi b , Kayo Kurotani a , Shamima Akter a , Leng Huat Foo c , Nobuo Nishi d , Masao Sato e , Hitomi Hayabuchi f , Tetsuya Mizoue a a Department of Epidemiology and Prevention, Clinical Research Center, National Center for Global Health and Medicine, Tokyo 162-8655, Japan b Walter H. Shorenstein Asia-Pacific Research Center, Standford University, USA c School of Health Sciences, Universiti Sains Malaysia, Kelantan, Malaysia d Center for International Collaboration and Partnership, National Institute of Health and Nutrition, Tokyo, Japan e Department of Applied Biological Chemistry, Graduate School of Bioresource and Bioenvironmental Sciences, Kyushu University, Fukuoka, Japan f Faculty of Human Environmental Science, Fukuoka Women's University, Fukuoka, Japan ARTICLE INFO ABSTRACT Article history: Received 9 April 2012 Accepted 31 July 2012 Objective. Several epidemiological studies have reported that high concentrations of circulating ferritin, a marker of iron stores, are related to insulin resistance (IR); however, questions remain regarding inconsistent data between Asian men and women and the inadequate consideration of potential confounding effects on the relationship between ferritin and IR. Our aim was to examine the relationship between serum ferritin concentrations and IR markers in the Japanese population. Materials/Methods. We analyzed data (n = 493) from a cross-sectional survey conducted in 2009 among a Japanese working population aged 20–68 years. Fasting serum ferritin and insulin levels and fasting plasma glucose levels were determined, and the homeostatic model assessment of IR (HOMA-IR) was calculated. Multiple regression analysis was performed with adjustments for demographic and lifestyle factors, body mass index and serum C-reactive protein. Results. Fasting insulin and HOMA-IR significantly increased with increasing levels of serum ferritin after adjustment for covariates in men (P for trend=.005 and .001, respectively). Compared with men in the lowest tertile of serum ferritin, those in the highest tertile had a 24% higher HOMA-IR score. Additional data suggested a positive association between iron intake and HOMA-IR (P for trend = .07) in men. Neither serum ferritin nor iron intake was related to IR markers in women, even in postmenopausal women. Conclusions. Serum ferritin concentrations were positively associated with fasting insulin and HOMA-IR in men but not in women, suggesting an important role of iron storage in the pathogenesis of IR in Japanese men. © 2013 Elsevier Inc. All rights reserved. Keywords: Iron stores Glucose Insulin Japanese METABOLISM CLINICAL AND EXPERIMENTAL 62 (2013) 561 – 567 Abbreviations: BMI, body mass index; CI, confidence interval; CRP, C-reactive protein; HOMA, homeostatic model assessment; IR, insulin resistance; MET, metabolic equivalent. ⁎ Corresponding author. Tel.: +81 3 3202 7181; fax: +81 3 3202 7364. E-mail address: [email protected] (N.M. Pham). 0026-0495/$ – see front matter © 2013 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.metabol.2012.07.025 Available online at www.sciencedirect.com Metabolism www.metabolismjournal.com

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 2 ( 2 0 1 3 ) 5 6 1 – 5 6 7
Ava i l ab l e on l i ne a t www.sc i enced i r ec t . com
Metabolismwww.metabo l i sm jou rna l . com
Serum ferritin is associated with markers of insulin resistance
in Japanese men but not in womenNgoc Minh Phama,⁎, Akiko Nanri a, Siyan Yib, Kayo Kurotani a, Shamima Aktera,Leng Huat Foo c, Nobuo Nishi d, Masao Sato e, Hitomi Hayabuchi f, Tetsuya Mizouea
a Department of Epidemiology and Prevention, Clinical Research Center, National Center for Global Health andMedicine, Tokyo 162-8655, Japanb Walter H. Shorenstein Asia-Pacific Research Center, Standford University, USAc School of Health Sciences, Universiti Sains Malaysia, Kelantan, Malaysiad Center for International Collaboration and Partnership, National Institute of Health and Nutrition, Tokyo, Japane Department of Applied Biological Chemistry, Graduate School of Bioresource and Bioenvironmental Sciences, Kyushu University, Fukuoka, Japanf Faculty of Human Environmental Science, Fukuoka Women's University, Fukuoka, Japan
A R T I C L E I N F O
Abbreviations: BMI, body mass index; CI,insulin resistance; MET, metabolic equivalen⁎ Corresponding author. Tel.: +81 3 3202 7181
E-mail address: [email protected] (N.M
0026-0495/$ – see front matter © 2013 Elsevihttp://dx.doi.org/10.1016/j.metabol.2012.07.02
A B S T R A C T
Article history:Received 9 April 2012Accepted 31 July 2012
Objective. Several epidemiological studies have reported that high concentrations ofcirculating ferritin, a marker of iron stores, are related to insulin resistance (IR); however,questions remain regarding inconsistent data between Asian men and women and theinadequate consideration of potential confounding effects on the relationship betweenferritin and IR. Our aim was to examine the relationship between serum ferritinconcentrations and IR markers in the Japanese population.
Materials/Methods. We analyzed data (n=493) from a cross-sectional survey conducted in2009 among a Japanese working population aged 20–68 years. Fasting serum ferritin andinsulin levels and fasting plasma glucose levels were determined, and the homeostaticmodel assessment of IR (HOMA-IR) was calculated. Multiple regression analysis wasperformed with adjustments for demographic and lifestyle factors, body mass index andserum C-reactive protein.
Results. Fasting insulin and HOMA-IR significantly increased with increasing levels ofserum ferritin after adjustment for covariates in men (P for trend=.005 and .001,respectively). Compared with men in the lowest tertile of serum ferritin, those in thehighest tertile had a 24% higher HOMA-IR score. Additional data suggested a positiveassociation between iron intake and HOMA-IR (P for trend=.07) in men. Neither serumferritin nor iron intakewas related to IRmarkers inwomen, even inpostmenopausalwomen.
Conclusions. Serum ferritin concentrations were positively associated with fasting insulinand HOMA-IR in men but not in women, suggesting an important role of iron storage in thepathogenesis of IR in Japanese men.
© 2013 Elsevier Inc. All rights reserved.
Keywords:Iron storesGlucoseInsulinJapanese
confidence interval; CRP, C-reactive protein; HOMA, homeostatic model assessment; IR,t.; fax: +81 3 3202 7364.. Pham).
er Inc. All rights reserved.5

562 M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 2 ( 2 0 1 3 ) 5 6 1 – 5 6 7
1. Introduction
The health effects caused by iron overload have receivedincreasing attention [1]. There is accumulating evidence tosuggest that elevated concentrations of circulating ferritin, amarker of iron stores, are associated with the prevalence andrisk of metabolic syndrome [2–5] and type 2 diabetes [6].Metabolic syndrome and type 2 diabetes are multifactorialdisorders in which insulin resistance (IR) is closely involved.Thus, high concentrations of circulating ferritin may berelated to IR. Most observational studies have shown thatelevated levels of circulating ferritin are associated with IR asassessed by the homeostatic model assessment (HOMA)[2,5,7–11] and decreased insulin sensitivity [12,13]. However,a very recent study among a Latin American populationfound no association between circulating ferritin and HOMA-IR [14]. As with intervention studies, the association betweeniron depletion and insulin sensitivity has been inconsistent[15–17].
Although the majority of epidemiological studies supportsa positive association between circulating ferritin and IRamong Westerners [2,8,10] and Asians [5,7,9,11], severalquestions remain to be resolved. One is the lack of consistencyin the association between circulating ferritin and IR accord-ing to gender and menopausal status [2,5,7,11]. Anotherconcern is the inadequate consideration given to the potentialconfounding effect of inflammation. Ferritin is an acute-phasereactant [18], i.e., its concentration increases during inflam-mation, and numerous studies have suggested that inflam-mation is related to IR [19]; however, some [2,11], but not all[5,7,9], studies accounted for inflammation by showingadjustments in circulating C-reactive protein (CRP), a sensitivemarker of low-grade inflammation. Moreover, most Asianstudies [5,7,9,11] did not control for important lifestyle factorsthat potentially affect the association between circulatingferritin and HOMA-IR. Thus, there is a need for furtherepidemiological studies to elucidate the association betweenferritin and IR among Asians.
The present study was conducted to examine the associ-ation between serum ferritin and IR markers among aJapanese working population. We hypothesized that higherconcentrations of serum ferritin are associated with highervalues of IR markers.
2. Methods
2.1. Study procedure and subjects
We conducted a cross-sectional survey in July and November2009 among municipal employees in two workplaces innortheastern Kyushu, Japan. At the time of the periodichealth checkup, all full-time workers (n=605) except thosewho were on long sick or maternity leave were invited toparticipate. Of the invited participants, 567 (325 men and 242women aged 20–68 years) consented to take part in the study(response rate 94%). Participants were asked to fill in asurvey questionnaire before the health checkup. The surveyquestionnaire was then checked by research staff for
completeness, and where necessary, clarifications weremade with the subjects on the day of their health examina-tion. We also obtained data that were routinely collectedduring the health examination, including anthropometricmeasurements, biochemical data and information on med-ical history, smoking and alcohol consumption. We excludedparticipants who reported having a history of diabetes (n=8),cancer (n=13), cardiovascular disease (n=11) and thosereceiving medical care for chronic hepatitis (n=3). We furtherexcluded individuals without fasting status (n=25) and thosewho had missing values for the insulin measurement (n=16)and covariates (n=1). After exclusion, 493 total participants(283 men and 210 women) were eligible for the study. Thestudy protocol was reviewed and approved by the EthicsCommittee of the National Center for Global Health andMedicine, Japan. Written informed consent was obtainedfrom all subjects prior to the survey.
2.2. Laboratory measurements
Blood samples were obtained on the day of the healthcheckup. Venous blood (7 mL) was drawn into vacuum tubesand then transported in a cooler box to the laboratory. Theblood was centrifuged for 10 min, and the separated serumwas divided into a maximum of six tubes (0.5 mL each) andkept at −30 °C during the survey for each workplace. One ofthese tubes was sent, immediately after the survey period, toan external laboratory (Mitsubishi Chemical Medience Corpo-ration, Tokyo, Japan) for the measurement of high-sensitivityCRP and folate, whereas the remaining ones were stored at −80 °C until analysis for other items including ferritin andinsulin. High-sensitivity CRP was measured using a latexnephelometry (N-Latex CRPII; Dade Behring, Tokyo, Japan) ona BN II Nephelometer (Dade Behring), with the lower limit ofdetection being 0.04 mg/L and the coefficients of variationwere 6.3% at 0.05 mg/L and 1.7% at 0.98 mg/L. Ferritin wasdetermined using a chemiluminescence immunoassay (Che-milumi ACS-Ferritin II; Siemens Healthcare Diagnostics,Tokyo, Japan) on an ADVIA Centaur (Bayer), with the lowerlimit of detection being 0.5 μg/L and the coefficients ofvariation were 3.4% at 36.7 μg/L, 3.4% at 83.3 μg/L and 4.2%at 255 μg/L. Insulinwasmeasured using a chemiluminescenceimmunoassay (Architect Insulin; Abbott Japan, Tokyo, Japan)on an ARCHITECT i2000 (Abbott Diagnostics), and the co-efficients of variation were 2.5% at 6.2 μU/mL and 1.2% at60.9 μU/mL. Plasma glucose concentration was measured as apart of the regular health checkup using enzymatic methods(Glucose CII-test Wako, Wako Pure Chemical Industries,Osaka, Japan) and an OLYMPUS AU640 measuring device.We computed the homeostatic model assessment of IR(HOMA-IR) using the following formula: [fasting insulin(μU/mL) × fasting glucose (mmol/L)]/22.5 [20].
2.3. Other variables
Marital status, job position, alcohol and tobacco use,occupational and non-occupational physical activities andparental history of type 2 diabetes were elicited in thequestionnaire. Occupational physical activity was classified

563M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 2 ( 2 0 1 3 ) 5 6 1 – 5 6 7
as sedentary work (managerial and clerical jobs) and activework (childcare work, school lunch preparation and technicaljobs). Questions on non-occupational physical activity ascer-tained the time (in minutes) spent for walking or cycling tocommute to or from work and for five recreational activities(walking, low-, moderate-, and high-intensity activities, andgardening). Non-occupational physical activity was estimat-ed as a metabolic equivalent (MET) value and expressed asthe sum of MET multiplied by the time (in hours) spentperforming each activity [21]. Body height was measured tothe nearest 0.1 cm with subjects standing without shoes.Body weight in light clothes was measured to the nearest0.1 kg. Body mass index (BMI) was calculated by dividingweight by squared height (kg/m2). Iron intake was assessedusing a validated brief self-administered diet history ques-tionnaire, which ascertained the consumption frequency of56 food items, beverages and 9 dishes in the previous month.Correlations between iron intake according to the above-mentioned validated questionnaire and those from 16-dayweighted dietary records were 0.35 and 0.36 in men andwomen, respectively [22].
2.4. Statistical analysis
Data on subject characteristics were expressed as the mean±standard deviation, median (interquartile range) and per-centage according to the tertile of the serum ferritinconcentration; their trend associations were evaluated usinglinear regression analysis for continuous variables withordinal numbers 1–3 assigned to the tertiles of serum ferritin,or Mantel–Haenszel chi-squared tests for categorical vari-ables. Fasting insulin and glucose concentrations as well asHOMA-IR were log-transformed before analysis because theywere not distributed normally. Analysis of covariance wasperformed to calculate geometric means and 95% confidenceintervals (CI) of IR markers across the tertiles of serumferritin. Multiple linear regressions were used to test thetrend of association between serum ferritin and IR markersby assigning ordinal numbers 1–3 to increasing tertiles ofserum ferritin. We first adjusted for age (continuous) andstudy site (survey in July 2009 or November 2009) (model 1). Inaddition, we adjusted for job position (low or middle andhigh), occupational physical activity (active or sedentary),non-occupational physical activity (<5 or≥5 MET-h/week),parental history of type 2 diabetes (yes or no), currentsmoking (yes or no), alcohol consumption (yes or no),hypertension (yes or no) defined as systolic blood pressureof≥140 mmHg or diastolic blood pressure of≥90 mmHg orcurrent use of antihypertensive drugs, menopausal status(yes or no) and BMI (continuous) (model 2). Further adjust-ment was made for log-transformed serum CRP (continuous)(model 3). We also conducted analyses after excludingsubjects with clinically elevated serum ferritin concentra-tions (≥ 300 μg/L and≥200 μg/L for men and women, respec-tively) [23] and limited analyses to postmenopausal women.In addition, we examined the association between dietaryiron intake and IR markers. Statistical analyses were per-formed using Stata version 12.0 (StataCorp, College Station,TX). Two-sided P values of less than .05 were consideredstatistically significant.
3. Results
We presented data for men and women separately becausemen had much higher concentrations of serum ferritin thandid women (geometric mean: men, 130.5 μg/L; women,32.3 μg/L; P for difference< .001) and because significantinteractions were detected between sex and serum ferritinon fasting insulin, glucose and HOMA-IR (P for interaction=.006, .025 and .0002, respectively) using a likelihood ratio test,which compared models with and without a multiplicativeinteraction term between sex (dichotomous) and log-trans-formed serum ferritin (continuous) in the full model (model 3).Mean concentrations of serum ferritin were significantlylower in premenopausal women (23.4 μg/L, 95% CI 19.9–27.5)compared with postmenopausal women (75.4 μg/L, 95% CI61.0–93.3) and lower in postmenopausal women comparedwith men (130.5 μg/L, 95% CI 119.5–142.6). Subject character-istics across the tertiles of serum ferritin concentrations inmen and women are summarized in Table 1. Men with higherserum ferritin concentrations tended to have a significantlyhigher BMI and serum CRP concentration. In women, subjectswith higher serum ferritin concentrations were older, lesslikely to be in a low job position and more likely to bepostmenopausal. Women with higher serum ferritin concen-trations tended to consume more dietary iron and have asignificantly higher serum CRP concentration. The Spearmancorrelation coefficient between serum ferritin and CRPwas 0.3.
Higher concentrations of serum ferritin were significantlyassociatedwith higher values for all IRmarkers after adjustingfor age, study site, occupational and non-occupational phys-ical activity, parental history of type 2 diabetes, currentsmoking, alcohol consumption, hypertension and BMI(model 2) in men (Table 2). Further adjustment for CRP(model 3) did not materially change the association of serumferritin with fasting insulin (P for trend=.005) and HOMA-IR (Pfor trend=.001), although the association with fasting glucosebecame statistically non-significant (P for trend=.08). In fullyadjusted models (model 3), compared with men in the lowesttertile of serum ferritin, those in the highest tertile had a 19%higher concentration of fasting serum insulin, 3% higherconcentration of fasting plasma glucose, and 24% higher scoreof HOMA-IR. In women, serum ferritin concentrations werenot associated with any IR marker.
In sensitivity analysis, after excluding individuals withclinically elevated serum concentrations of ferritin, ≥300 μg/Lin men (n=26) and≥200 μg/L in women (n=3), the positiveassociation between serum ferritin and IR markers in men didnot alter appreciably, and the null association in womenremained (data not shown). Additional analyses limited topostmenopausal subjects (n=58) showed no associationbetween serum ferritin and IR markers (data not shown). Werepeated our analyses using dietary iron intake as theexposure variable and observed a suggestion of a positiveassociation between iron intake and fasting insulin (P fortrend=.08) as well as HOMA-IR (P for trend=.07) in men, butnot in women (P for trend=.25 and .45 for fasting insulin andHOMA-IR, respectively) after adjustments for potential con-founders (except serum ferritin). Additional adjustment for

Table 1 – Characteristics of the study subjects by tertile of serum ferritin concentration.
Men Women
Tertile 1 Tertile 2 Tertile 3 P fortrend a
Tertile 1 Tertile 2 Tertile 3 P fortrend a
n 95 94 94 70 71 69Serum ferritin (μg/L) b 7.2–108 109–191 192–623 3.2–<21.2 21.2–<57 57–248Age (years) c 45.9±11.1 43.7±11.1 44.5±11.1 .37 38.9±8.1 41.6±9.6 47.6±10.7 <.001Study site Ad, % 25.3 30.9 40.4 .03 30.0 15.5 18.8 .11Job position (low), % 49.5 52.1 53.2 .61 80.0 67.6 46.4 <.001Sedentary work, % 86.3 89.4 93.6 .10 77.1 63.4 65.2 .13Non-occupationalphysical activity(≥5 MET-h/week) e, %
46.3 38.3 43.6 .71 22.9 21.1 27.5 .52
BMI (kg/m2) c 22.7±2.9 23.0±3.1 24.0±3.4 .02 21.1±2.6 20.7±3.1 21.7±3.0 .16Current cigarettesmokers, %
36.8 45.7 39.4 .72 1.43 8.45 2.90 .66
Current alcoholdrinkers, %
46.3 38.3 43.6 .22 52.9 49.3 42.0 .20
Hypertension, % 13.7 14.9 16.0 .66 2.9 4.2 7.3 .23Parental history oftype 2 diabetes, %
13.7 14.9 17.0 .52 28.6 21.1 17.4 .11
Postmenopausalwomen, %
― ― ― ― 5.7 22.5 55.1 <.001
Total iron intake(mg/day) f
4.6 (4.0–5.2) 6.9 (6.3–7.7) 9.8 (9.1–11.2) .21 5.0 (4.1–5.8) 6.9 (6.6–7.4) 9.5 (8.7–10.4) .02
CRP (mg/L) f 0.32 (0.19–0.77) 0.46 (0.21–1.10) 0.60 (0.30–1.11) .002 0.18 (0.10–0.37) 0.26 (0.11–0.52) 0.39 (0.12–0.97) .002
Abbreviations: BMI, body mass index; CRP, high-sensitivity C-reactive protein; MET-h, metabolic equivalent-hour.a Based on linear regression analysis for continuous variables with ordinal numbers 1–3 assigned to the tertiles of serum ferritin or Mantel–Haenszel test for trends for categorical variables.b Range.c Mean±SD.d Survey conducted in July 2009.e Including walking or cycling to commute to or from work and recreational activities.f Median (interquartile range).
564 M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 2 ( 2 0 1 3 ) 5 6 1 – 5 6 7
serum ferritin (log-transformed continuous variable) did notmeasurably change the results.
4. Discussion
In the present study, we examined the association betweenserum ferritin concentrations and IR markers as assessed byfasting insulin, glucose and HOMA-IR in Japanese adults, andfound a positive association of serum ferritin with fastinginsulin and HOMA-IR inmen, but not in women. This is one ofthe few studies among Asians [5,7,9,11] to address theassociation between serum ferritin concentration and IR.
Our results for men concur with several previous studiesshowing that elevated ferritin concentrations were associatedwith higher fasting insulin [2,5,24–26] and HOMA-IR [2,5,8–11].Similarly, serum ferritin has been inversely related to insulinsensitivity as assessed by the minimal model method [12] orthe hyperinsulinemic–euglycemic clamp technique [13], andpositively correlated with IR as evaluated with the insulinsuppression test [27]. The present findings also agree with aChinese study [7] reporting a positive association betweenserum ferritin and HOMA-IR, albeit the association wasconfined towomen. The fact that no associationwas observedfor men in the Chinese study may be due to a low statisticalpower (n=140) and the lack of control for lifestyle factors such
as smoking, alcohol intake and physical activity and noadjustment for CRP levels. In addition, it has been reportedthat frequent blood donation [28] and bloodletting [15] arerelated to increased insulin sensitivity, and phlebotomytherapy decreases fasting glucose and insulin [29] as well asHOMA-IR [16]. Taken together, our data and those of previousstudies [2,5,8–11,24–29] support an adverse association be-tween elevated body iron stores and IR in men regardless ofrace or ethnicity.
Unlike inmen, thepresent study failed to findanassociationbetween serum ferritin and IR markers in women. Consistentwith our findings, two previous studies [2,5] showed noassociation between circulating ferritin concentrations andHOMA-IR in premenopausal women. Similarly, a Korean study[11] found that serum ferritin was unrelated to HOMA-IR ineither premenopausal or postmenopausal women. However, apositive association between circulating ferritin and HOMA-IRhas been reported among postmenopausal women [2,5]. Thenull association amongwomen in thepresent studymaybedueto limited sample size and a relatively small proportion ofpostmenopausal women (28%) compared with the 42% [5] to43% [2] inclusion rate reported previously. Thus, the statisticalpower may not be sufficient to detect an association amongwomen in the present study. Moreover, the mean concentra-tions of serum ferritin in thewomen in our studywere nearly 4-fold lower than those inmen, and the corresponding data were
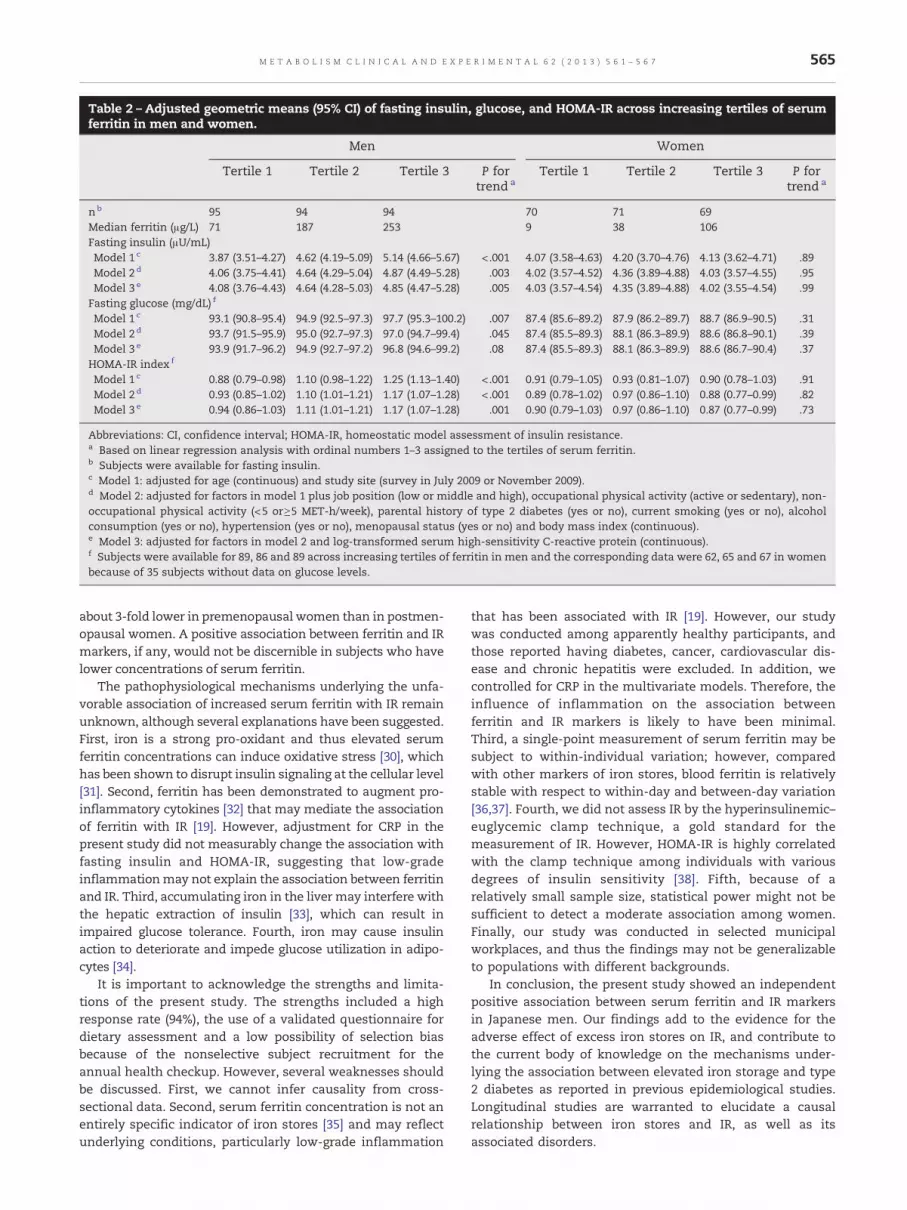
Table 2 – Adjusted geometric means (95% CI) of fasting insulin, glucose, and HOMA-IR across increasing tertiles of serumferritin in men and women.
Men Women
Tertile 1 Tertile 2 Tertile 3 P fortrend a
Tertile 1 Tertile 2 Tertile 3 P fortrend a
nb 95 94 94 70 71 69Median ferritin (μg/L) 71 187 253 9 38 106Fasting insulin (μU/mL)Model 1 c 3.87 (3.51–4.27) 4.62 (4.19–5.09) 5.14 (4.66–5.67) <.001 4.07 (3.58–4.63) 4.20 (3.70–4.76) 4.13 (3.62–4.71) .89Model 2 d 4.06 (3.75–4.41) 4.64 (4.29–5.04) 4.87 (4.49–5.28) .003 4.02 (3.57–4.52) 4.36 (3.89–4.88) 4.03 (3.57–4.55) .95Model 3 e 4.08 (3.76–4.43) 4.64 (4.28–5.03) 4.85 (4.47–5.28) .005 4.03 (3.57–4.54) 4.35 (3.89–4.88) 4.02 (3.55–4.54) .99
Fasting glucose (mg/dL) f
Model 1 c 93.1 (90.8–95.4) 94.9 (92.5–97.3) 97.7 (95.3–100.2) .007 87.4 (85.6–89.2) 87.9 (86.2–89.7) 88.7 (86.9–90.5) .31Model 2 d 93.7 (91.5–95.9) 95.0 (92.7–97.3) 97.0 (94.7–99.4) .045 87.4 (85.5–89.3) 88.1 (86.3–89.9) 88.6 (86.8–90.1) .39Model 3 e 93.9 (91.7–96.2) 94.9 (92.7–97.2) 96.8 (94.6–99.2) .08 87.4 (85.5–89.3) 88.1 (86.3–89.9) 88.6 (86.7–90.4) .37
HOMA-IR index f
Model 1 c 0.88 (0.79–0.98) 1.10 (0.98–1.22) 1.25 (1.13–1.40) <.001 0.91 (0.79–1.05) 0.93 (0.81–1.07) 0.90 (0.78–1.03) .91Model 2 d 0.93 (0.85–1.02) 1.10 (1.01–1.21) 1.17 (1.07–1.28) <.001 0.89 (0.78–1.02) 0.97 (0.86–1.10) 0.88 (0.77–0.99) .82Model 3 e 0.94 (0.86–1.03) 1.11 (1.01–1.21) 1.17 (1.07–1.28) .001 0.90 (0.79–1.03) 0.97 (0.86–1.10) 0.87 (0.77–0.99) .73
Abbreviations: CI, confidence interval; HOMA-IR, homeostatic model assessment of insulin resistance.a Based on linear regression analysis with ordinal numbers 1–3 assigned to the tertiles of serum ferritin.b Subjects were available for fasting insulin.c Model 1: adjusted for age (continuous) and study site (survey in July 2009 or November 2009).d Model 2: adjusted for factors in model 1 plus job position (low or middle and high), occupational physical activity (active or sedentary), non-occupational physical activity (<5 or≥5 MET-h/week), parental history of type 2 diabetes (yes or no), current smoking (yes or no), alcoholconsumption (yes or no), hypertension (yes or no), menopausal status (yes or no) and body mass index (continuous).e Model 3: adjusted for factors in model 2 and log-transformed serum high-sensitivity C-reactive protein (continuous).f Subjects were available for 89, 86 and 89 across increasing tertiles of ferritin in men and the corresponding data were 62, 65 and 67 in womenbecause of 35 subjects without data on glucose levels.
565M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 2 ( 2 0 1 3 ) 5 6 1 – 5 6 7
about 3-fold lower in premenopausal women than in postmen-opausal women. A positive association between ferritin and IRmarkers, if any, would not be discernible in subjects who havelower concentrations of serum ferritin.
The pathophysiological mechanisms underlying the unfa-vorable association of increased serum ferritin with IR remainunknown, although several explanations have been suggested.First, iron is a strong pro-oxidant and thus elevated serumferritin concentrations can induce oxidative stress [30], whichhas been shown to disrupt insulin signaling at the cellular level[31]. Second, ferritin has been demonstrated to augment pro-inflammatory cytokines [32] that may mediate the associationof ferritin with IR [19]. However, adjustment for CRP in thepresent study did not measurably change the association withfasting insulin and HOMA-IR, suggesting that low-gradeinflammationmay not explain the association between ferritinand IR. Third, accumulating iron in the liver may interfere withthe hepatic extraction of insulin [33], which can result inimpaired glucose tolerance. Fourth, iron may cause insulinaction to deteriorate and impede glucose utilization in adipo-cytes [34].
It is important to acknowledge the strengths and limita-tions of the present study. The strengths included a highresponse rate (94%), the use of a validated questionnaire fordietary assessment and a low possibility of selection biasbecause of the nonselective subject recruitment for theannual health checkup. However, several weaknesses shouldbe discussed. First, we cannot infer causality from cross-sectional data. Second, serum ferritin concentration is not anentirely specific indicator of iron stores [35] and may reflectunderlying conditions, particularly low-grade inflammation
that has been associated with IR [19]. However, our studywas conducted among apparently healthy participants, andthose reported having diabetes, cancer, cardiovascular dis-ease and chronic hepatitis were excluded. In addition, wecontrolled for CRP in the multivariate models. Therefore, theinfluence of inflammation on the association betweenferritin and IR markers is likely to have been minimal.Third, a single-point measurement of serum ferritin may besubject to within-individual variation; however, comparedwith other markers of iron stores, blood ferritin is relativelystable with respect to within-day and between-day variation[36,37]. Fourth, we did not assess IR by the hyperinsulinemic–euglycemic clamp technique, a gold standard for themeasurement of IR. However, HOMA-IR is highly correlatedwith the clamp technique among individuals with variousdegrees of insulin sensitivity [38]. Fifth, because of arelatively small sample size, statistical power might not besufficient to detect a moderate association among women.Finally, our study was conducted in selected municipalworkplaces, and thus the findings may not be generalizableto populations with different backgrounds.
In conclusion, the present study showed an independentpositive association between serum ferritin and IR markersin Japanese men. Our findings add to the evidence for theadverse effect of excess iron stores on IR, and contribute tothe current body of knowledge on the mechanisms under-lying the association between elevated iron storage and type2 diabetes as reported in previous epidemiological studies.Longitudinal studies are warranted to elucidate a causalrelationship between iron stores and IR, as well as itsassociated disorders.
566 M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 2 ( 2 0 1 3 ) 5 6 1 – 5 6 7
Author contributions
N.M.P. analyzed data andwrote themanuscript. A.N. planned,coordinated field survey and contributed to discussion. S.Y.contributed to discussion. K.K. contributed to data interpre-tation and discussion. S.A. contributed to data interpretationand discussion. L.H. contributed to discussion. N.N. contrib-uted to data presentation and discussion. M.S. planned,coordinated field survey and contributed to discussion. H.H.planned, coordinated field survey and contributed to discus-sion. T.M. edited the manuscript and is the principalinvestigator of the present study.
Funding
This study was supported by a Grant-in-Aid for ScientificResearch (B) (21390213) from the Japan Society for thePromotion of Science (To Dr Mizoue), a Grant-in-Aid forYoung Scientists (B) (21790598) from theMinistry of Education,Culture, Sports, Science and Technology and a Grant ofNational Center for Global Health and Medicine (To Dr Nanri).
Conflict of interest
The authors declare no conflict of interest.
Acknowledgments
We are grateful to the study participants for their cooperationand participation.We also thank SeikoMiyazaki and YasutakaHoriuchi (Kyushu University); Emi Tanaka, Youko Tsuruda,Misaki Hirose, Meishu Sai, Miho Isayama, Midori Sasaki, MieShimomura, andAzumiUehara (FukukaWomen'sUniversity);Yaeko Nagano (retired nurse); and Yumi Matsushita, AkikoHayashi, Yu Teruyama, Kae Saito, Kayoko Washizuka, andYuhoMizoue (National Center for Global Health andMedicine)for their help in data collection.
R E F E R E N C E S
[1] Heath AL, Fairweather-Tait SJ. Health implications of ironoverload: the role of diet and genotype. Nutr Rev 2003;61:45–62.
[2] Jehn M, Clark JpM, Guallar E. Serum ferritin and risk of themetabolic syndrome in U.S. adults. Diabetes Care 2004;27:2422–8.
[3] Vari IS, Balkau B, Kettaneh A, et al. Ferritin and transferrin areassociated with metabolic syndrome abnormalities and theirchange over time in a general population: data from anEpidemiological Study on the Insulin Resistance Syndrome(DESIR). Diabetes Care 2007;30:1795–801.
[4] Sun L, Franco OH, Hu FB, et al. Ferritin concentrations,metabolic syndrome, and type 2 diabetes in middle-aged andelderly Chinese. J Clin Endocrinol Metab 2008;93:4690–6.
[5] Lee BK, Kim Y, Kim YI. Association of serum ferritin withmetabolic syndrome and diabetes mellitus in the South
Korean general population according to the Korean NationalHealth and Nutrition Examination Survey 2008. Metabolism2011;60:1416–24.
[6] Rajpathak SN, Crandall JP, Wylie-Rosett J, et al. The role ofiron in type 2 diabetes in humans. Biochim Biophys Acta2009;1790:671–81.
[7] Sheu WH, Chen YT, Lee WJ, et al. A relationship betweenserum ferritin and the insulin resistance syndrome is presentin non-diabetic women but not in non-diabetic men. ClinEndocrinol (Oxf) 2003;58:380–5.
[8] Chen J, Wildman RP, Hamm LL, et al. Association betweeninflammation and insulin resistance in U.S. nondiabeticadults: results from the Third National Health andNutrition Examination Survey. Diabetes Care 2004;27:2960–5.
[9] Iwasaki T, Nakajima A, Yoneda M, et al. Serum ferritin isassociated with visceral fat area and subcutaneous fat area.Diabetes Care 2005;28:2486–91.
[10] Syrovatka P, Kraml P, Potockova J, et al. Relationshipbetween increased body iron stores, oxidative stress andinsulin resistance in healthy men. Ann Nutr Metab 2009;54:268–74.
[11] Kim CH, Kim HK, Bae SJ, et al. Association of elevated serumferritin concentration with insulin resistance and impairedglucose metabolism in Korean men and women. Metabolism2011;60:414–20.
[12] Fernández-Real JM, Ricart-Engel W, Arroyo E, et al. Serumferritin as a component of the insulin resistance syndrome.Diabetes Care 1998;21:62–8.
[13] Haap M, Fritsche A, Mensing HJ, et al. Association of highserum ferritin concentration with glucose intolerance andinsulin resistance in healthy people. Ann Intern Med2003;139:869–71.
[14] Suárez-Ortegón MF, Arbeláez A, Mosquera M, et al. Body ironstores as predictors of insulin resistance in apparentlyhealthy urban Colombian men. Biol Trace Elem Res 2012;145:283–5.
[15] Fernández-Real JM, Peñarroja G, Castro A, et al. Bloodlettingin high-ferritin type 2 diabetes: effects on insulin sensitivityand beta-cell function. Diabetes 2002;51:1000–4.
[16] Valenti L, Fracanzani AL, Dongiovanni P, et al. Iron depletionby phlebotomy improves insulin resistance in patients withnonalcoholic fatty liver disease and hyperferritinemia:evidence from a case–control study. Am J Gastroenterol2007;102:1251–8.
[17] Houschyar KS, Ludtke R, Dobos GJ, et al. Effects of phlebot-omy-induced reduction of body iron stores on metabolicsyndrome: results from a randomized clinical trial. BMC Med2012;10:54.
[18] Weiss G, Goodnough LT. Anemia of chronic disease. N Engl JMed 2005;352:1011–23.
[19] Shoelson SE, Lee J, Goldfine AB. Inflammation and insulinresistance. J Clin Invest 2006;116:1793–801.
[20] Wallace TM, Levy JC, Matthews DR. Use and abuse of HOMAmodeling. Diabetes Care 2004;27:1487–95.
[21] Ainsworth BE, Haskell WL, Whitt MC, et al. Compendium ofphysical activities: an update of activity codes and METintensities. Med Sci Sports Exerc 2000;32:S498–516.
[22] Sasaki S. Development and evaluation of dietaryassessment methods using biomarkers and diet historyquestionnaires for individuals (in Japanese). In: Tanaka H,editor. Research for evaluation methods of nutrition anddietary lifestyle programs held on healthy Japan 21. Summaryreport. Tokyo: Ministry of Health, Welfare, and Labor; 2004.p. 11–44.
[23] Fairbanks VF. Laboratory testing for iron status. Hosp Pract(Off Ed) 1991;26(Suppl. 3):17–24.
[24] Tuomainen TP, Nyyssönen K, Salonen R, et al. Body ironstores are associated with serum insulin and blood glucose

567M E T A B O L I S M C L I N I C A L A N D E X P E R I M E N T A L 6 2 ( 2 0 1 3 ) 5 6 1 – 5 6 7
concentrations. Population study in 1,013 eastern Finnishmen. Diabetes Care 1997;20:426–8.
[25] Ford ES, Cogswell ME. Diabetes and serum ferritinconcentration among U.S. adults. Diabetes Care 1999;22:1978–83.
[26] Fumeron F, Péan F, Driss F, et al. Ferritin and transferrin areboth predictive of the onset of hyperglycemia in men andwomen over 3 years: the data from an epidemiological studyon the Insulin Resistance Syndrome (DESIR) study. DiabetesCare 2006;29:2090–4.
[27] Hua NW, Stoohs RA, Facchini FS. Low iron status andenhanced insulin sensitivity in lacto-ovo vegetarians. Br JNutr 2001;86:515–9.
[28] Fernández-Real JM, López-Bermejo A, Ricart W. Iron stores,blood donation, and insulin sensitivity and secretion. ClinChem 2005;51:1201–5.
[29] Facchini FS. Effect of phlebotomy on plasma glucose andinsulin concentrations. Diabetes Care 1998;21:2190.
[30] Fernández-Real JM, López-Bermejo A, Ricart W. Cross-talkbetween iron metabolism and diabetes. Diabetes 2002;51:2348–54.
[31] Rains JL, Jain SK. Oxidative stress, insulin signaling, anddiabetes. Free Radic Biol Med 2011;50:567–75.
[32] Ruddell RG, Hoang-Le D, Barwood JM, et al. Ferritin functionsas a proinflammatory cytokine via iron-independent proteinkinase C zeta/nuclear factor kappaB-regulated signaling in rathepatic stellate cells. Hepatology 2009;49:887–900.
[33] Ferrannini E. Insulin resistance, iron, and the liver. Lancet2000;355:2181–2.
[34] Green A, Basile R, Rumberger JM. Transferrin and iron induceinsulin resistance of glucose transport in adipocytes.Metabolism 2006;55:1042–5.
[35] Taher AT, Musallam KM, Inati A. Iron overload:consequences, assessment, and monitoring. Hemoglobin2009;33(Suppl. 1):S46–57.
[36] Dale JC, Burritt MF, Zinsmeister AR. Diurnal variation ofserum iron, iron-binding capacity, transferrin saturation, andferritin levels. Am J Clin Pathol 2002;117:802–8.
[37] Pilon VA, Howanitz PJ, Howanitz JH, et al. Day-to-dayvariation in serum ferritin concentration in healthy subjects.Clin Chem 1981;27:78–82.
[38] Bonora E, Targher G, Alberiche M, et al. Homeostasis modelassessment closely mirrors the glucose clamp technique inthe assessment of insulin sensitivity: studies in subjects withvarious degrees of glucose tolerance and insulin sensitivity.Diabetes Care 2000;23:57–63.
Related Documents











