Serum ferritin and transferrin levels as serologic markers of methylene diphenyl diisocyanate–induced occupational asthma Gyu-Young Hur, MD, PhD, a Gil-Soon Choi, MD, a Seung-Soo Sheen, MD, PhD, b Hyun-Young Lee, MS, a Han-Jung Park, MD, a Sung-Jin Choi, MD, a Young-Min Ye, MD, a and Hae-Sim Park, MD, PhD a Suwon, South Korea Background: Although methylene diphenyl diisocyanate (MDI) may induce occupational asthma in the workplace, the pathogenic mechanisms are unclear. Objectives: By using bronchoalveolar lavage fluid, we sought to identify proteins that were differentially expressed between subjects with MDI-induced occupational asthma (MDI-OA) and asymptomatic exposed controls (AECs). Methods: To find proteins that were differentially expressed between the MDI-OA and AEC groups, 2-dimensional electrophoresis was performed by using bronchoalveolar lavage fluid obtained from subjects after MDI-specific inhalation challenge. The selected protein spots were then identified by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry. The clinical relevance of the differentially expressed spots was compared by ELISA using sera from the MDI-OA/eosinophilic bronchitis, AEC, and unexposed healthy control groups. Receiver operating characteristic curves were then plotted, and the sensitivity and specificity were determined. Results: Twenty-three protein spots were identified that distinguished the subjects with MDI-OA from those in the AEC group. Among them, ferritin expression was downregulated whereas transferrin expression was upregulated in subjects with MDI-OA compared with AEC; these results were validated by ELISA using sera from the MDI-OA/EB and AEC groups. To identify subjects with MDI-OA, the optimal serum cutoff levels were 69.84 ng/mL for ferritin and 2.48 mg/mL for transferrin. When these 2 parameters were combined, the sensitivity was 71.43% and the specificity was 85.71%. Conclusion: Serum ferritin and transferrin levels are associated with the phenotype of MDI-OA. (J Allergy Clin Immunol 2008;122:774-80.) Key words: MDI, occupational asthma, ferritin, transferrin, proteome Diisocyanates, which are widely used in the manufacture of polyurethane foams, elastomers, adhesives, coatings, insecti- cides, paints, plastics, and varnishes, may cause occupational asthma as a low-molecular-weight antigen, 1,2 and several efforts have been made to develop serologic markers for isocyanate-in- duced asthma. In the case of toluene diisocyanate–induced occu- pational asthma (TDI-OA), specific IgE and IgG antibodies to toluene diisocyanate (TDI)–human serum albumin conjugate were found to be good diagnostic tools. 3-5 In addition, serum-spe- cific IgG to cytokeratin 19 was suggested as a possible serologic marker of TDI-OA, but the sensitivity of these 2 parameters was too low to be applied. 3-6 In methylene diisocyanate–induced oc- cupational asthma (MDI-OA), although the level of serum spe- cific IgE and IgG antibodies was found to be increased in some patients, 7 it was not high enough to be used for diagnostic pur- poses. Considering that permanent impairment of lung function was reported in long-term follow-up studies of isocyanate-in- duced asthma, 8 developing relevant serologic markers to identify susceptible subjects among exposed workers is essential. Proteomic analysis is a complex process involving the purifi- cation and identification of individual proteins from all of the proteins expressed in a cell or tissue. 9 To clarify the pathogenic mechanisms of asthma with proteomic technology, many studies have used human samples such as bronchoalveolar lavage fluid (BALF) 10 and plasma. 11,12 From a the Department of Allergy and Rheumatology, and b Pulmonary and Critical Care Medicine, Ajou University School of Medicine. Supported by a grant from the Korean Health 21 R&D Project of the Ministry of Health and Welfare, Republic of Korea (A050571). G.-Y. Hur is currently with the Department of Internal Medicine, Korea University College of Medicine, Seoul, South Korea. Disclosure of potential conflict of interest: The authors have declared that they have no conflict of interest. Received for publication February 19, 2008; revised July 28, 2008; accepted for publica- tion July 29, 2008. Reprint requests: Hae-Sim Park, MD, PhD, Department of Allergy and Rheumatology, Ajou University School of Medicine, San-5, Wonchun-dong, Youngtong-gu, Suwon, 443-721, South Korea. E-mail: [email protected]. 0091-6749/$34.00 Ó 2008 American Academy of Allergy, Asthma & Immunology doi:10.1016/j.jaci.2008.07.034 Abbreviations used 2-DE: 2-Dimensional electrophoresis AEC: Asymptomatic exposed control ANCOVA: Analysis of covariance ARDS: Acute respiratory distress syndrome AUC: Area under the curve BALF: Bronchoalveolar lavage fluid DBP: Vitamin D–binding protein precursor EB: Eosinophilic bronchitis MALDI-TOF/TOF MS: Matrix-assisted laser desorption ionization time-of-flight/time-of-flight mass spectrometry MDI: Methylene diisocyanate MDI-EB: Methylene diisocyanate–induced eosinophilic bronchitis MDI-OA: Methylene diisocyanate–induced occupational asthma MS: Mass spectrometry NC: Nonatopic healthy control ROC: Receiver operating characteristic TDI: Toluene diisocyanate TDI-OA: Toluene diisocyanate–induced occupational asthma WRRS: Work-related lower respiratory symptom 774

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Serum ferritin and transferrin levels as serologic markers ofmethylene diphenyl diisocyanate–induced occupationalasthma
Gyu-Young Hur, MD, PhD,a Gil-Soon Choi, MD,a Seung-Soo Sheen, MD, PhD,b Hyun-Young Lee, MS,a Han-Jung Park,
MD,a Sung-Jin Choi, MD,a Young-Min Ye, MD,a and Hae-Sim Park, MD, PhDa Suwon, South Korea
Background: Although methylene diphenyl diisocyanate (MDI)may induce occupational asthma in the workplace, thepathogenic mechanisms are unclear.Objectives: By using bronchoalveolar lavage fluid, we sought toidentify proteins that were differentially expressed betweensubjects with MDI-induced occupational asthma (MDI-OA) andasymptomatic exposed controls (AECs).Methods: To find proteins that were differentially expressedbetween the MDI-OA and AEC groups, 2-dimensionalelectrophoresis was performed by using bronchoalveolar lavagefluid obtained from subjects after MDI-specific inhalationchallenge. The selected protein spots were then identified bymatrix-assisted laser desorption/ionization time-of-flight massspectrometry. The clinical relevance of the differentiallyexpressed spots was compared by ELISA using sera from theMDI-OA/eosinophilic bronchitis, AEC, and unexposed healthycontrol groups. Receiver operating characteristic curves werethen plotted, and the sensitivity and specificity were determined.Results: Twenty-three protein spots were identified thatdistinguished the subjects with MDI-OA from those in the AECgroup. Among them, ferritin expression was downregulatedwhereas transferrin expression was upregulated in subjects withMDI-OA compared with AEC; these results were validated byELISA using sera from the MDI-OA/EB and AEC groups. Toidentify subjects with MDI-OA, the optimal serum cutoff levelswere 69.84 ng/mL for ferritin and 2.48 mg/mL for transferrin.When these 2 parameters were combined, the sensitivity was71.43% and the specificity was 85.71%.Conclusion: Serum ferritin and transferrin levels are associatedwith the phenotype of MDI-OA. (J Allergy Clin Immunol2008;122:774-80.)
Key words: MDI, occupational asthma, ferritin, transferrin,proteome
From athe Department of Allergy and Rheumatology, and bPulmonary and Critical Care
Medicine, Ajou University School of Medicine.
Supported by a grant from the Korean Health 21 R&D Project of the Ministry of Health
and Welfare, Republic of Korea (A050571).
G.-Y. Hur is currently with the Department of Internal Medicine, Korea University
College of Medicine, Seoul, South Korea.
Disclosure of potential conflict of interest: The authors have declared that they have no
conflict of interest.
Received for publication February 19, 2008; revised July 28, 2008; accepted for publica-
tion July 29, 2008.
Reprint requests: Hae-Sim Park, MD, PhD, Department of Allergy and Rheumatology,
Ajou University School of Medicine, San-5, Wonchun-dong, Youngtong-gu, Suwon,
443-721, South Korea. E-mail: [email protected].
0091-6749/$34.00
� 2008 American Academy of Allergy, Asthma & Immunology
doi:10.1016/j.jaci.2008.07.034
774
Diisocyanates, which are widely used in the manufacture ofpolyurethane foams, elastomers, adhesives, coatings, insecti-cides, paints, plastics, and varnishes, may cause occupationalasthma as a low-molecular-weight antigen,1,2 and several effortshave been made to develop serologic markers for isocyanate-in-duced asthma. In the case of toluene diisocyanate–induced occu-pational asthma (TDI-OA), specific IgE and IgG antibodies totoluene diisocyanate (TDI)–human serum albumin conjugatewere found to be good diagnostic tools.3-5 In addition, serum-spe-cific IgG to cytokeratin 19 was suggested as a possible serologicmarker of TDI-OA, but the sensitivity of these 2 parameters wastoo low to be applied.3-6 In methylene diisocyanate–induced oc-cupational asthma (MDI-OA), although the level of serum spe-cific IgE and IgG antibodies was found to be increased in somepatients,7 it was not high enough to be used for diagnostic pur-poses. Considering that permanent impairment of lung functionwas reported in long-term follow-up studies of isocyanate-in-duced asthma,8 developing relevant serologic markers to identifysusceptible subjects among exposed workers is essential.
Proteomic analysis is a complex process involving the purifi-cation and identification of individual proteins from all of theproteins expressed in a cell or tissue.9 To clarify the pathogenicmechanisms of asthma with proteomic technology, many studieshave used human samples such as bronchoalveolar lavage fluid(BALF)10 and plasma.11,12
Abbreviations used
2-DE: 2-Dimensional electrophoresis
AEC: Asymptomatic exposed control
ANCOVA: Analysis of covariance
ARDS: Acute respiratory distress syndrome
AUC: Area under the curve
BALF: Bronchoalveolar lavage fluid
DBP: Vitamin D–binding protein precursor
EB: Eosinophilic bronchitis
MALDI-TOF/TOF MS: Matrix-assisted laser desorption ionization
time-of-flight/time-of-flight mass spectrometry
MDI: Methylene diisocyanate
MDI-EB: Methylene diisocyanate–induced
eosinophilic bronchitis
MDI-OA: Methylene diisocyanate–induced
occupational asthma
MS: Mass spectrometry
NC: Nonatopic healthy control
ROC: Receiver operating characteristic
TDI: Toluene diisocyanate
TDI-OA: Toluene diisocyanate–induced
occupational asthma
WRRS: Work-related lower respiratory symptom
J ALLERGY CLIN IMMUNOL
VOLUME 122, NUMBER 4
HUR ET AL 775
In this study, we sought to identify new serologic markers usinga proteomic approach and to validate them for screeningsuspected subjects from among MDI-exposed individuals.
METHODSThe protocol for this study was reviewed and approved by the Ajou
University Institute Review Board, and informed consent was obtained from
each study subject.
Study subjectsSeven subjects with MDI-OA and/or eosinophilic bronchitis (EB), 51
asymptomatic exposed controls (AECs), and 74 nonatopic healthy controls
(NCs) were enrolled in this study. Among 7 subjects of the MDI-OA/EB
group, 5 had MDI-OA and 2 had MDI-induced EB (MDI-EB). All subjects
with MDI-OA/EB and AECs were selected from among 58 previously studied
MDI-exposed workers in a single car upholstery factory.7 First, 58 subjects
were screened by respiratory questionnaire, and 26 subjects who had com-
plained of work-related lower respiratory symptoms (WRRSs) underwent
methacholine challenge test. Then, 11 subjects showing a positive response
to methacholine challenge test underwent the MDI-specific inhalation tests
subsequently, except 2 subjects who refused the MDI-specific inhalation
test. Five symptomatic workers who had positive responses to both methacho-
line challenge test and MDI-specific inhalation challenge were defined as hav-
ing MDI-OA, and their clinical features are summarized in Table I. WRRS was
defined as lower respiratory symptoms aggravated during the work, but im-
proved after the work or during holidays, including cough, sputum, wheezing
episodes, or shortness of breath.7,13 The subjects with MDI-EB were defined
as complaining of WRRS with increased sputum eosinophilia (>3%) after
MDI bronchial challenges, but having negative responses to the methacholine
bronchial challenge and MDI-specific inhalation challenge tests.14 Subjects
with AEC were defined as subjects who did not have MDI-OA/EB although
they had worked in the same workplace. Two subjects who had positive
responses to methacholine challenge tests but refused further studies were
excluded from the AEC group. The NCs were healthy nonatopic volunteers
who had never been exposed to MDI. The detailed results of MDI-specific in-
halation challenge were reported in our previous article.7
Skin prick test and bronchial challenge testingThe skin prick test, which included 9 common inhalant allergens (tree
mixture, grass mixture, mugwort, ragweed, cat fur, dog fur, Dermatophagoides
pteronyssinus, Dermatophagoides farinae, and Alternaria; Bencard, Bradford,
United Kingdom), was performed on all subjects. The result of each test was
reported as the ratio of the mean wheal diameter of the allergen to histamine.
For values above 1, the reaction was defined as positive. Atopy was defined
as more than 1 positive response to the common inhalant allergens on the
skin prick test.
Airway responsiveness to methacholine was tested in those 26 subjects who
had WRRS by using the 5-breath dosimeter protocol.15 MDI-specific inhala-
tion challenge testing was performed on 15 subjects with definite WRRS or
positive responses to the methacholine challenge test by using a modified ver-
sion of a previously described method.7,16 In brief, 20 mL polymeric MDI
(Desmodur 44V20; Bayer, Leverkusen, Germany) was heated to 1808C in a
beaker on a hot plate to approach the optimal MDI exposure conditions for
bronchial provocation. The atmospheric concentration of MDI was measured
serially by using personal samplers (GilAir; Sensidyne Inc, Clearwater, Fla)
placed 60 cm away from the hot plate. The initial exposure lasted 20 minutes,
and another was performed after a 1-hour break. During the break, the booth
was thoroughly ventilated. Spirometric measurements were recorded before
the challenge, at 10-minute intervals for 1 hour after the challenge, and subse-
quently at 1-hour intervals for the next 4 hours. Peak flow measurements were
collected at 2-hour intervals for 24 hours. The test was performed in a booth
equipped with a ventilating fan and transparent windows through which the
subjects were observed. All subjects with MDI-OA had positive results of
methacholine challenge, and their PC20 values ranged from 2.76 to 21.93
mg/mL.
Bronchoscopy and bronchoalveolar lavageFiber optic bronchoscopy was performed 24 hours after the MDI-specific
challenge test. Bronchoalveolar lavage was performed through a flexible
bronchoscope (Olympus BF-P240; Olympus Corp, Tokyo, Japan), which was
wedged into the subsegmental bronchus of the right middle lobe. Three 30-mL
aliquots of sterile saline solution were instilled through the bronchoscope. The
fluid was immediately recovered by gentle suction after each instillation. The
harvested BALF was centrifuged at 1000 rpm for 10 minutes, and the
supernatant was collected for proteomic analysis according to the MDI-
specific inhalation challenge test result. Serum was obtained from each subject
after MDI-specific inhalation challenge testing.
Two-dimensional electrophoresis and image
analysisTo evaluate differential protein expression in the MDI-OA and AEC
groups, we chose 2 subjects with a more than 25% decrease in FEV1 after the
MDI-specific inhalation challenge test (typical MDI-OA) and 2 subjects with
no decrease in FEV1 after the MDI-specific inhalation challenge test (AECs),
and collected BALF for 2-DE.
Each sample was prepared by trichloroacetic acid/acetone precipitation
for desalting and concentrating. Immubilized pH gradient (IPG) strips (Immobi-
line DryStrip, pH 3-10 NL, Amersham Pharmacia Biotech, Uppsala, Sweden)
and Pharmalytes (pH 3-10; Amersham Pharmacia Biotech) were used for
isoelectric focusing. For the first-dimensional analysis, 1 mg protein was
focused on IPG strips as described except that a total of 80,000 voltage-hours
was applied.17,18 For second-dimensional separation, electrophoresis was per-
formed by using 9% to 16% gradient polyacrylamide gels until the dye front
reached the lower end of the gel. To quantify the relative abundance of the pro-
teins, the gels were stained with Coomassie Brilliant Blue G-250 (Bio-Rad, Her-
cules, Calif). The stained gels were then scanned using a GS-710 imaging
densitometer (Bio-Rad) and analyzed with Image Master Platinum 5 (GE
Healthcare, Piscataway, NJ).
In-gel digestion and mass spectrometric analysisProtein spots that increased or decreased more than 2-fold between the
positive and negative groups were selected for mass spectrometry (MS)
TABLE I. Clinical features of the study subjects
MDI-OA/EB
(n 5 7)
AEC
(n 5 49)
NC
(n 5 74)
P
value
Age (y) 46.43 6 4.43 39.94 6 9.49 29.34 6 6.63 <.001
Sex
(male/female)
2/5 26/23 22/52 .056
Working duration
(y)
5.56 6 1.28 4.02 6 2.43 NA .205
% Predicted
FEV1*
105.17 6 13.56 99.92 6 17.78 99.91 6 10.16 .778
PC20 (mg/mL) 15.05 6 9.82 22.83 6 7.77� ND NA
Log total IgE
(IU/mL)
2.13 6 0.63 2.00 6 0.65 1.80 6 0.53 .513
Geometric mean 134.52 99.41 62.79
95% CI 34.9-518.3 64.7-152.7 27.7-142.2
Atopy (%) 0 (0) 15 (30.6) 0 (0) NA
Smoking history
(%)
1 (14.3) 21 (41.2) 16 (21.6) .150
NA, Not applicable; ND, not done.
*Performed before methacholine challenge test.
�Derived from 17 individuals taking the test.
J ALLERGY CLIN IMMUNOL
OCTOBER 2008
776 HUR ET AL
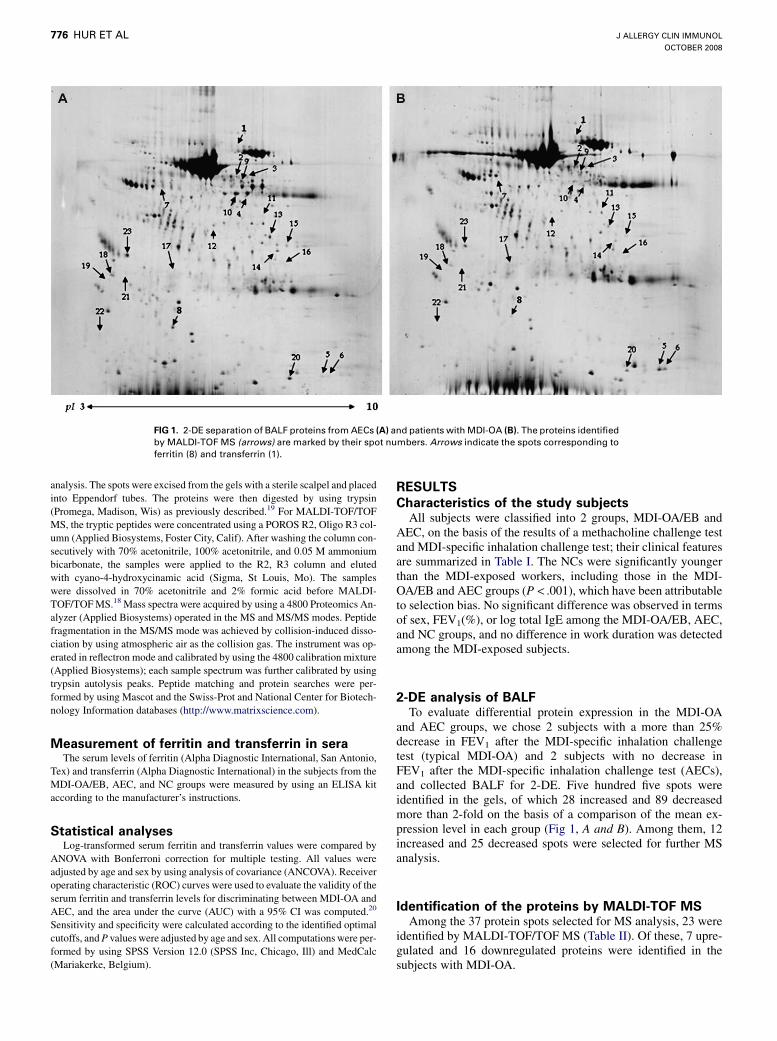
FIG 1. 2-DE separation of BALF proteins from AECs (A) and patients with MDI-OA (B). The proteins identified
by MALDI-TOF MS (arrows) are marked by their spot numbers. Arrows indicate the spots corresponding to
ferritin (8) and transferrin (1).
analysis. The spots were excised from the gels with a sterile scalpel and placed
into Eppendorf tubes. The proteins were then digested by using trypsin
(Promega, Madison, Wis) as previously described.19 For MALDI-TOF/TOF
MS, the tryptic peptides were concentrated using a POROS R2, Oligo R3 col-
umn (Applied Biosystems, Foster City, Calif). After washing the column con-
secutively with 70% acetonitrile, 100% acetonitrile, and 0.05 M ammonium
bicarbonate, the samples were applied to the R2, R3 column and eluted
with cyano-4-hydroxycinamic acid (Sigma, St Louis, Mo). The samples
were dissolved in 70% acetonitrile and 2% formic acid before MALDI-
TOF/TOF MS.18 Mass spectra were acquired by using a 4800 Proteomics An-
alyzer (Applied Biosystems) operated in the MS and MS/MS modes. Peptide
fragmentation in the MS/MS mode was achieved by collision-induced disso-
ciation by using atmospheric air as the collision gas. The instrument was op-
erated in reflectron mode and calibrated by using the 4800 calibration mixture
(Applied Biosystems); each sample spectrum was further calibrated by using
trypsin autolysis peaks. Peptide matching and protein searches were per-
formed by using Mascot and the Swiss-Prot and National Center for Biotech-
nology Information databases (http://www.matrixscience.com).
Measurement of ferritin and transferrin in seraThe serum levels of ferritin (Alpha Diagnostic International, San Antonio,
Tex) and transferrin (Alpha Diagnostic International) in the subjects from the
MDI-OA/EB, AEC, and NC groups were measured by using an ELISA kit
according to the manufacturer’s instructions.
Statistical analysesLog-transformed serum ferritin and transferrin values were compared by
ANOVA with Bonferroni correction for multiple testing. All values were
adjusted by age and sex by using analysis of covariance (ANCOVA). Receiver
operating characteristic (ROC) curves were used to evaluate the validity of the
serum ferritin and transferrin levels for discriminating between MDI-OA and
AEC, and the area under the curve (AUC) with a 95% CI was computed.20
Sensitivity and specificity were calculated according to the identified optimal
cutoffs, and P values were adjusted by age and sex. All computations were per-
formed by using SPSS Version 12.0 (SPSS Inc, Chicago, Ill) and MedCalc
(Mariakerke, Belgium).
RESULTS
Characteristics of the study subjectsAll subjects were classified into 2 groups, MDI-OA/EB and
AEC, on the basis of the results of a methacholine challenge testand MDI-specific inhalation challenge test; their clinical featuresare summarized in Table I. The NCs were significantly youngerthan the MDI-exposed workers, including those in the MDI-OA/EB and AEC groups (P < .001), which have been attributableto selection bias. No significant difference was observed in termsof sex, FEV1(%), or log total IgE among the MDI-OA/EB, AEC,and NC groups, and no difference in work duration was detectedamong the MDI-exposed subjects.
2-DE analysis of BALFTo evaluate differential protein expression in the MDI-OA
and AEC groups, we chose 2 subjects with a more than 25%decrease in FEV1 after the MDI-specific inhalation challengetest (typical MDI-OA) and 2 subjects with no decrease inFEV1 after the MDI-specific inhalation challenge test (AECs),and collected BALF for 2-DE. Five hundred five spots wereidentified in the gels, of which 28 increased and 89 decreasedmore than 2-fold on the basis of a comparison of the mean ex-pression level in each group (Fig 1, A and B). Among them, 12increased and 25 decreased spots were selected for further MSanalysis.
Identification of the proteins by MALDI-TOF MSAmong the 37 protein spots selected for MS analysis, 23 were
identified by MALDI-TOF/TOF MS (Table II). Of these, 7 upre-gulated and 16 downregulated proteins were identified in thesubjects with MDI-OA.

J ALLERGY CLIN IMMUNOL
VOLUME 122, NUMBER 4
HUR ET AL 777
TABLE II. List of proteins identified by MALDI-TOF MS analysis
No. Protein Exp gi No. Score Peptide match Theory-mass (kD) pI Cov %
1 Transferrin, human serum [ 7245524 58 7 37241 6.49 20
2 Immunoglobulin heavy chain [ 3819788 92 9 24238 5.56 30
3 Human FcaRI [ 31615936 96 8 23642 7.12 37
4 Unnamed protein product [ 34530195 70 15 87805 9.56 20
5 Human hemoglobin [ 56967333 86 6 15018 8.07 46
6 Hemoglobin a1 globin chain [ 13650074 66 9 15292 7.96 66
7 DBP [ 139641 68 13 52929 5.40 35
8 Ferritin light subunit Y 182516 79 8 16441 5.65 49
9 Human salivary amylase Y 15988375 94 12 56411 6.21 27
10 Aldehyde dehydrogenase [NAD(P)] Y 283971 127 13 50703 5.99 27
11 Aldo-keto reductase family 7 Y 19343681 102 11 37553 6.50 45
12 Gelsolinlike capping protein Y 63252913 47 8 38474 5.82 31
13 Fructose-1,6-bisphosphatase 1 Y 57165050 121 16 37190 6.54 27
14 Annexin A1 Y 119582952 74 12 40057 7.60 38
15 Annexin A2 Y 4757756 65 8 38580 7.57 37
16 Rho guanine nucleotide exchange factor 4 Y 15011981 65 22 76372 6.00 34
17 Hypothetical protein Y 119613232 65 14 37160 6.17 40
18 Immunoglobulin heavy chain Y 112700812 53 6 10870 6.34 82
19 Bullous pemphigoid antigen Y 2134838 64 15 76452 6.15 23
20 hCG2042874 Y 119605532 61 15 90369 5.86 17
21 Pulmonary surfactant apoprotein precursor Y 190565 83 6 26836 5.17 29
22 Chain H, chrystal structure of the MRP14 (S100A9) Y 20150236 72 6 13159 5.71 74
23 Annexin V Y 809185 154 20 35783 4.94 56
Cov, Coverage; gi No., genInfo identifier; pI, isoelectric point.
Measurement of the serum ferritin and transferrin
levels by ELISATo validate the proteins identified by MALDI-TOF/TOF MS,
we measured the serum ferritin and transferrin levels in the MDI-OA/EB, AEC, and NC groups (Fig 2), which was adjusted by ageand sex. Table III showed both unadjusted and adjusted P valuesof serum ferritin and transferrin, which indicated that both ferritinand transferrin levels had significant difference between thegroups after age and sex adjustment (P 5 .005 and <.001,respectively).
Determination of the optimal cutoff levels for serum
ferritin and transferrinWe next evaluated the diagnostic value of serum ferritin (Fig 3,
A) and transferrin (Fig 3, B) in discriminating between subjectswith MDI-OA/EB and the AECs using the AUC, which was com-puted from a ROC curve. We then selected the appropriate cutoffvalues for each ROC curve. Using the cutoff for ferritin (69.84 ng/mL; Table III), the sensitivity and specificity were 85.71% and71.48%, respectively, with 0.786 (95% CI, 0.614-0.957; P 5
.053) of the AUC value. When we applied the transferrin cutoffvalue (�2.48 mg/mL), the sensitivity and specificity decreasedto 71.43% and 51.02%, with 0.612 (95% CI, 0.396-0.829; P 5
.400) of the AUC value. When both parameters were combinedto improve the discriminating power,21 the AUC value increasedto 0.789 (95% CI, 0.580-0.991; P 5 .020), whereas the sensitivityand specificity increased to 71.43% and 85.71%, respectively(Table IV).
DISCUSSIONTo elucidate the pathogenic mechanisms of MDI-OA, we
adopted a proteomic approach as a screening tool. First, 2-DE was
used to screen for target proteins in BALF collected from subjectswith MDI-OA and the AECs, and 23 protein spots that wereupregulated or downregulated more than 2-fold were selected.Among those spots, transferrin (spot 1), immunoglobin (spot 2),hemoglobin (spots 5 and 6), and vitamin D–binding proteinprecursor (DBP; spot 7) were upregulated, whereas ferritin lightchain (spot 8), gelsolinlike capping protein (spot 12), and multipleannexins (spots 14, 15, and 23) were downregulated.
We found that the ferritin light chain was downregulatedwhereas transferrin was upregulated in the MDI-OA groupcompared with the AEC group by using a proteomic approach.Both ferritin and transferrin are regarded as markers of ironmetabolism, and they are fully associated with one another.Ferritin is an iron storage protein consisting of 2 subunits, a heavyand light chain, encoded by separate genes that sequester iron inthe ferric (Fe31) state. Ferritin is an acute-phase reactant withclinical implications as a serologic marker of acute and chronicinflammation. It often increases during periods of oxidative stresssuch as acute respiratory distress syndrome (ARDS)22,23 or cysticfibrosis24 for the detoxification of free iron, because free iron fa-cilitates the formation of highly toxic hydroxyl radicals from hy-drogen peroxide.25,26 In addition, polymorphisms within the genethat encodes the ferritin light chain are associated with the devel-opment of ARDS.27 Thus, altered intracellular and extracellularferritin expression may have implications in the development oflung inflammation, including ARDS. Consistent with our results,a recent study reported that epithelial cells treated with carbonmonoxide (CO) gas, which has a high affinity for ferrous ironand can alter iron metabolism in bronchial epithelial cells,28 ex-hibited a decreased ferritin concentration. Some studies haveshown reduced ferritin levels29 and increased transferrin levels30
in the sera of patients with asthma. Transferrin is an antioxidantthat binds iron in the plasma. The iron delivered by transferrinmay be associated with increased oxidative cell injury,31 because
J ALLERGY CLIN IMMUNOL
OCTOBER 2008
778 HUR ET AL
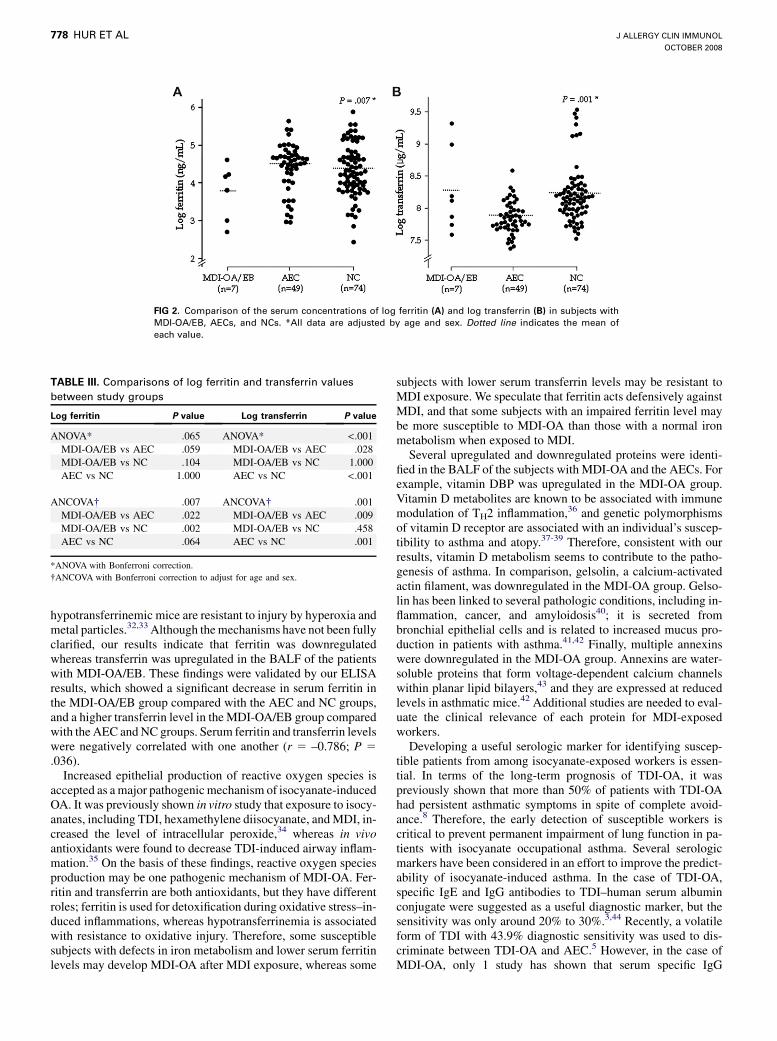
FIG 2. Comparison of the serum concentrations of log ferritin (A) and log transferrin (B) in subjects with
MDI-OA/EB, AECs, and NCs. *All data are adjusted by age and sex. Dotted line indicates the mean of
each value.
hypotransferrinemic mice are resistant to injury by hyperoxia andmetal particles.32,33 Although the mechanisms have not been fullyclarified, our results indicate that ferritin was downregulatedwhereas transferrin was upregulated in the BALF of the patientswith MDI-OA/EB. These findings were validated by our ELISAresults, which showed a significant decrease in serum ferritin inthe MDI-OA/EB group compared with the AEC and NC groups,and a higher transferrin level in the MDI-OA/EB group comparedwith the AEC and NC groups. Serum ferritin and transferrin levelswere negatively correlated with one another (r 5 –0.786; P 5
.036).Increased epithelial production of reactive oxygen species is
accepted as a major pathogenic mechanism of isocyanate-inducedOA. It was previously shown in vitro study that exposure to isocy-anates, including TDI, hexamethylene diisocyanate, and MDI, in-creased the level of intracellular peroxide,34 whereas in vivoantioxidants were found to decrease TDI-induced airway inflam-mation.35 On the basis of these findings, reactive oxygen speciesproduction may be one pathogenic mechanism of MDI-OA. Fer-ritin and transferrin are both antioxidants, but they have differentroles; ferritin is used for detoxification during oxidative stress–in-duced inflammations, whereas hypotransferrinemia is associatedwith resistance to oxidative injury. Therefore, some susceptiblesubjects with defects in iron metabolism and lower serum ferritinlevels may develop MDI-OA after MDI exposure, whereas some
TABLE III. Comparisons of log ferritin and transferrin values
between study groups
Log ferritin P value Log transferrin P value
ANOVA* .065 ANOVA* <.001
MDI-OA/EB vs AEC .059 MDI-OA/EB vs AEC .028
MDI-OA/EB vs NC .104 MDI-OA/EB vs NC 1.000
AEC vs NC 1.000 AEC vs NC <.001
ANCOVA� .007 ANCOVA� .001
MDI-OA/EB vs AEC .022 MDI-OA/EB vs AEC .009
MDI-OA/EB vs NC .002 MDI-OA/EB vs NC .458
AEC vs NC .064 AEC vs NC .001
*ANOVA with Bonferroni correction.
�ANCOVA with Bonferroni correction to adjust for age and sex.
subjects with lower serum transferrin levels may be resistant toMDI exposure. We speculate that ferritin acts defensively againstMDI, and that some subjects with an impaired ferritin level maybe more susceptible to MDI-OA than those with a normal ironmetabolism when exposed to MDI.
Several upregulated and downregulated proteins were identi-fied in the BALF of the subjects with MDI-OA and the AECs. Forexample, vitamin DBP was upregulated in the MDI-OA group.Vitamin D metabolites are known to be associated with immunemodulation of TH2 inflammation,36 and genetic polymorphismsof vitamin D receptor are associated with an individual’s suscep-tibility to asthma and atopy.37-39 Therefore, consistent with ourresults, vitamin D metabolism seems to contribute to the patho-genesis of asthma. In comparison, gelsolin, a calcium-activatedactin filament, was downregulated in the MDI-OA group. Gelso-lin has been linked to several pathologic conditions, including in-flammation, cancer, and amyloidosis40; it is secreted frombronchial epithelial cells and is related to increased mucus pro-duction in patients with asthma.41,42 Finally, multiple annexinswere downregulated in the MDI-OA group. Annexins are water-soluble proteins that form voltage-dependent calcium channelswithin planar lipid bilayers,43 and they are expressed at reducedlevels in asthmatic mice.42 Additional studies are needed to eval-uate the clinical relevance of each protein for MDI-exposedworkers.
Developing a useful serologic marker for identifying suscep-tible patients from among isocyanate-exposed workers is essen-tial. In terms of the long-term prognosis of TDI-OA, it waspreviously shown that more than 50% of patients with TDI-OAhad persistent asthmatic symptoms in spite of complete avoid-ance.8 Therefore, the early detection of susceptible workers iscritical to prevent permanent impairment of lung function in pa-tients with isocyanate occupational asthma. Several serologicmarkers have been considered in an effort to improve the predict-ability of isocyanate-induced asthma. In the case of TDI-OA,specific IgE and IgG antibodies to TDI–human serum albuminconjugate were suggested as a useful diagnostic marker, but thesensitivity was only around 20% to 30%.3,44 Recently, a volatileform of TDI with 43.9% diagnostic sensitivity was used to dis-criminate between TDI-OA and AEC.5 However, in the case ofMDI-OA, only 1 study has shown that serum specific IgG

J ALLERGY CLIN IMMUNOL
VOLUME 122, NUMBER 4
HUR ET AL 779
FIG 3. ROC curves for the serum levels of ferritin (A) and transferrin (B), as well as the combined value (C)
used to determine the optimal cutoffs for MDI-OA. Arrows indicate the optimal value for ferritin, transferrin,
and the combined value (ferritin � 69.84 ng/mL and transferrin � 2.48 mg/mL). Gray regions represent the
sensitivity range (60-100) and specificity range (50-100).
antibodies may be a useful predictive factor (57.1% sensitivity).7
In this study, we evaluated the diagnostic value of serum ferritinand transferrin measurements in identifying MDI-OA/EB. We ap-plied ROC curves to compute the optimal values and selectedthose areas with more than 60% sensitivity and more than 50%specificity (Fig 3). We obtained the optimal AUC values basedon those values, although the serum ferritin cutoff value affordedsuperior sensitivity and specificity compared with the serumtransferrin cutoff value (sensitivity, 85.71% vs 71.43%; specific-ity, 71.48% vs 51.02%). When we combined ferritin with transfer-rin, however, the P value improved (P value, ferritin only, 0.053;vs ferritin with transferrin, .020). Although a follow-up longitudi-nal study will be essential to confirm whether these 2 markers willbe useful for predicting development of MDI-induced asthma in alarger cohort, on the basis of these findings, we suggest that the 2combined serologic markers (serum ferritin �69.84 ng/mL andserum transferrin �2.48 mg/mL) can be used to discriminate be-tween subjects with MDI-OA/EB and the AECs from amongMDI-exposed workers with 71.43% sensitivity and 85.71%specificity.
In conclusion, this study is the first to consider differentialprotein expression in the BALF of subjects with MDI-OA andAECs. We found 23 differentially expressed (more than 2-fold)protein spots after a MDI-specific inhalation challenge test inpatients with MDI-OA. Among them, the ferritin light chain wasdownregulated and whereas transferrin was upregulated, andthese results were validated by using sera from exposed workers.Our findings suggest that combined serum ferritin and transferrin(ferritin�69.84 ng/mL and transferrin�2.48 mg/mL) testing canbe used to identify cases of MDI-OA from among the MDI-exposed workers.
TABLE IV. Sensitivity, specificity, and the values of the area
under the ROC with 95% CI and P values
Cutoffs
Sensitivity
(%)
Specificity
(%) AUC (95% CI)
P
value*
Ferritin
� 69.84 ng/mL
85.71 71.48 0.786 (0.614-0.957) .053
Transferrin � 2.48
mg/mL
71.43 51.02 0.612 (0.396-0.829) .400
Ferritin � 69.84 ng/
mL and transferrin
� 2.48 mg/mL
71.43 85.71 0.786 (0.580-0.991) .020
*Values are adjusted by age and sex.
We thank Dr Eun-Young Lee (Yonsei Proteome Research Center, Seoul,
Korea) for assistance with the proteomic analysis.
Clinical implications: Serum ferritin and transferrin can beused as serologic markers for identifying MDI-OA in MDI-ex-posed workers.
REFERENCES
1. Mapp CE. Agents, old and new, causing occupational asthma. Occup Environ Med
2001;58:354-60.
2. Mapp CE, Boschetto P, Maestrelli P, Fabbri LM. Occupational asthma. Am J Re-
spir Crit Care Med 2005;172:280-305.
3. Park HS, Kim HY, Nahm DH, Son JW, Kim YY. Specific IgG, but not specific IgE,
antibodies to toluene diisocyanate-human serum albumin conjugate are associated
with toluene diisocyanate bronchoprovocation test results. J Allergy Clin Immunol
1999;104:847-51.
4. Park HS, Lee SK, Kim HY, Nahm DH, Kim SS. Specific immunoglobulin E and
immunoglobulin G antibodies to toluene diisocyanate-human serum albumin con-
jugate: useful markers for predicting long-term prognosis in toluene diisocyanate-
induced asthma. Clin Exp Allergy 2002;32:551-5.
5. Ye YM, Kim CW, Kim HR, Kim HM, Suh CH, Nahm DH, et al. Biophysical
determinants of toluene diisocyanate antigenicity associated with exposure and
asthma. J Allergy Clin Immunol 2006;118:885-91.
6. Choi JH, Nahm DH, Kim SH, Kim YS, Suh CH, Park HS, et al. Increased levels of
IgG to cytokeratin 19 in sera of patients with toluene diisocyanate-induced asthma.
Ann Allergy Asthma Immunol 2004;93:293-8.
7. Hur GY, Koh DH, Choi GS, Park HJ, Choi SJ, Ye YM, et al. Clinical and immu-
nologic findings of methylene diphenyl diisocyanate-induced occupational asthma
in a car upholstery factory. Clin Exp Allergy 2008;38:586-93.
8. Park HS, Cho SH, Hong CS, Kim YY. Isocyanate-induced occupational asthma in
far-east Asia: pathogenesis to prognosis. Clin Exp Allergy 2002;32:198-204.
9. Crameri R. The potential of proteomics and peptidomics for allergy and asthma
research. Allergy 2005;60:1227-37.
10. Wu J, Kobayashi M, Sousa EA, Liu W, Cai J, Goldman SJ, et al. Differential pro-
teomic analysis of bronchoalveolar lavage fluid in asthmatics following segmental
antigen challenge. Mol Cell Proteomics 2005;4:1251-64.
11. Lee SH, Rhim T, Choi YS, Min JW, Kim SH, Cho SY, et al. Complement C3a and
C4a increased in plasma of patients with aspirin-induced asthma. Am J Respir Crit
Care Med 2006;173:370-8.
12. Murphy VE, Johnson RF, Wang YC, Akinsanya K, Gibson PG, Smith R, et al. Pro-
teomic study of plasma proteins in pregnant women with asthma. Respirology
2006;11:41-8.
13. Hur GY, Koh DH, Kim HA, Park HJ, Ye YM, Kim KS, et al. Prevalence of work-
related symptoms and serum-specific antibodies to wheat flour in exposed workers
in the bakery industry. Respir Med 2008;102:548-55.
14. Quirce S. Eosinophilic bronchitis in the workplace. Curr Opin Allergy Clin Immu-
nol 2004;4:87-91.
15. Crapo RO, Casaburi R, Coates AL, Enright PL, Hankinson JL, Irvin CG, et al.
Guidelines for methacholine and exercise challenge testing-1999. This official
statement of the American Thoracic Society was adopted by the ATS Board of Di-
rectors, July 1999. Am J Respir Crit Care Med 2000;161:309-29.

J ALLERGY CLIN IMMUNOL
OCTOBER 2008
780 HUR ET AL
16. Zammit-Tabona M, Sherkin M, Kijek K, Chan H, Chan-Yeung M. Asthma caused
by diphenylmethane diisocyanate in foundry workers: clinical, bronchial provoca-
tion, and immunologic studies. Am Rev Respir Dis 1983;128:226-30.
17. Cho YM, Bae SH, Choi BK, Cho SY, Song CW, Yoo JK, et al. Differential expres-
sion of the liver proteome in senescence accelerated mice. Proteomics 2003;3:
1883-94.
18. Choi BK, Cho YM, Bae SH, Zoubaulis CC, Paik YK. Single-step perfusion
chromatography with a throughput potential for enhanced peptide detection by
matrix-assisted laser desorption/ ionization-mass spectrometry. Proteomics 2003;
3:1955-61.
19. Shevchenko A, Wilm M, Vorm O, Mann M. Mass spectrometric sequencing of pro-
teins silver-stained polyacrylamide gels. Anal Chem 1996;68:850-8.
20. Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating
characteristic (ROC) curve. Radiology 1982;143:29-36.
21. Grube E, Bootsveld A, Buellesfeld L, Yuecel S, Shen JT, Imhoff M. Computerized
two-lead resting ECG analysis for the detection of coronary artery stenosis after
coronary revascularization. Int J Med Sci 2008;5:50-61.
22. Connelly KG, Moss M, Parsons PE, Moore EE, Moore FA, Giclas PC, et al. Serum
ferritin as a predictor of the acute respiratory distress syndrome. Am J Respir Crit
Care Med 1997;155:21-5.
23. Ghio AJ, Carter JD, Richards JH, Richer LD, Grissom CK, Elstad MR. Iron and
iron-related proteins in the lower respiratory tract of patients with acute respiratory
distress syndrome. Crit Care Med 2003;31:395-400.
24. Reid DW, Carroll V, O’May C, Champion A, Kirov SM. Increased airway iron as a
potential factor in the persistence of Pseudomonas aeruginosa infection in cystic
fibrosis. Eur Respir J 2007;30:286-92.
25. Ghio AJ, Turi JL, Yang F, Garrick LM, Garrick MD. Iron homeostasis in the lung.
Biol Res 2006;39:67-77.
26. Turi JL, Yang F, Garrick MD, Piantadosi CA, Ghio AJ. The iron cycle and oxida-
tive stress in the lung. Free Radic Biol Med 2004;36:850-7.
27. Lagan AL, Quinlan GJ, Mumby S, Melley DD, Goldstraw P, Bellingan GJ, et al.
Variation in iron homeostasis genes between patients with ARDS and healthy con-
trol subjects. Chest 2008;133:1302-11.
28. Ghio AJ, Stonehuerner JG, Dailey LA, Richards JH, Madden MD, Deng Z, et al.
Carbon monoxide reversibly alters iron homeostasis and respiratory epithelial cell
function. Am J Respir Cell Mol Biol 2008;38:715-23.
29. Vural H, Uzun K, Uz E, Kocyigit A, Cigli A, Akyol O. Concentrations of copper,
zinc and various elements in serum of patients with bronchial asthma. J Trace Elem
Med Biol 2000;14:88-91.
30. Brogan TD, Ryley HC, Neale L, Yassa J. Soluble proteins of bronchopulmonary secre-
tions from patients with cystic fibrosis, asthma, and bronchitis. Thorax 1975;30:72-9.
31. Breuer W, Greenberg E, Cabantchik ZI. Newly delivered transferrin iron and oxi-
dative cell injury. FEBS Lett 1997;403:213-9.
32. Ghio AJ, Carter JD, Richards JH, Crissman KM, Bobb HH, Yang F. Diminished
injury in hypotransferrinemic mice after exposure to a metal-rich particle. Am J
Physiol Lung Cell Mol Physiol 2000;278:L1051-61.
33. Yang F, Coalson JJ, Bobb HH, Carter JD, Banu J, Ghio AJ. Resistance of hypotrans-
ferrinemic mice to hyperoxia-induced lung injury. Am J Physiol 1999;277:L1214-23.
34. Elms J, Beckett PN, Griffin P, Curran AD. Mechanisms of isocyanate sensitisation:
an in vitro approach. Toxicol In Vitro 2001;15:631-4.
35. Kim SH, Park HJ, Lee CM, Choi IW, Moon DO, Roh HJ, et al. Epigallocatechin-3-
gallate protects toluene diisocyanate-induced airway inflammation in a murine
model of asthma. FEBS Lett 2006;580:1883-90.
36. Wittke A, Weaver V, Mahon BD, August A, Cantorna MT. Vitamin D receptor-
deficient mice fail to develop experimental allergic asthma. J Immunol 2004;
173:3432-6.
37. Poon AH, Laprise C, Lemire M, Montpetit A, Sinnett D, Schurr E, et al. Associ-
ation of vitamin D receptor genetic variants with susceptibility to asthma and at-
opy. Am J Respir Crit Care Med 2004;170:967-73.
38. Raby BA, Lazarus R, Silverman EK, Lake S, Lange C, Wjst M, et al. Association
of vitamin D receptor gene polymorphisms with childhood and adult asthma. Am J
Respir Crit Care Med 2004;170:1057-65.
39. Vollmert C, Illig T, Altmuller J, Klugbauer S, Loesgen S, Dumitrescu L, et al.
Single nucleotide polymorphism screening and association analysis: exclusion of
integrin beta 7 and vitamin D receptor (chromosome 12q) as candidate genes for
asthma. Clin Exp Allergy 2004;34:1841-50.
40. Spinardi L, Witke W. Gelsolin and diseases. Subcell Biochem 2007;45:55-69.
41. Candiano G, Bruschi M, Pedemonte N, Caci E, Liberatori S, Bini L, et al. Gelsolin
secretion in interleukin-4-treated bronchial epithelia and in asthmatic airways. Am
J Respir Crit Care Med 2005;172:1090-6.
42. Houtman R, Krijgsveld J, Kool M, Romijn EP, Redegeld FA, Nijkamp FP, et al.
Lung proteome alterations in a mouse model for nonallergic asthma. Proteomics
2003;3:2008-18.
43. Kourie JI, Wood HB. Biophysical and molecular properties of annexin-formed
channels. Prog Biophys Mol Biol 2000;73:91-134.
44. Cartier A, Grammer L, Malo JL, Lagier F, Ghezzo H, Harris K, et al. Specific
serum antibodies against isocyanates: association with occupational asthma. J
Allergy Clin Immunol 1989;84:507-14.
Related Documents











