This article was downloaded by:[HEAL-Link Consortium] On: 15 May 2008 Access Details: [subscription number 772810551] Publisher: Informa Healthcare Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Scandinavian Journal of Gastroenterology Publication details, including instructions for authors and subscription information: http://www.informaworld.com/smpp/title~content=t713690387 Serum adipokine levels in chronic liver diseases: Association of resistin levels with fibrosis severity Emmanuel Tsochatzis a ; George V. Papatheodoridis a ; Emilia Hadziyannis a ; Anastasia Georgiou a ; Georgia Kafiri b ; Dina G. Tiniakos c ; Emanuel K. Manesis a ; Athanasios J. Archimandritis a a Second Department of Internal Medicine, Athens University Medical School, Hippokration General Hospital, Athens, Greece b Department of Pathology, Hippokration General Hospital, Athens, Greece c Laboratory of Histology & Embryology, Athens University Medical School, Greece First Published on: 30 April 2008 To cite this Article: Tsochatzis, Emmanuel, Papatheodoridis, George V., Hadziyannis, Emilia, Georgiou, Anastasia, Kafiri, Georgia, Tiniakos, Dina G., Manesis, Emanuel K. and Archimandritis, Athanasios J. (2008) 'Serum adipokine levels in chronic liver diseases: Association of resistin levels with fibrosis severity', Scandinavian Journal of Gastroenterology, To link to this article: DOI: 10.1080/00365520802085387 URL: http://dx.doi.org/10.1080/00365520802085387 PLEASE SCROLL DOWN FOR ARTICLE Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf This article maybe used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

This article was downloaded by:[HEAL-Link Consortium]On: 15 May 2008Access Details: [subscription number 772810551]Publisher: Informa HealthcareInforma Ltd Registered in England and Wales Registered Number: 1072954Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Scandinavian Journal ofGastroenterologyPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t713690387
Serum adipokine levels in chronic liver diseases:Association of resistin levels with fibrosis severityEmmanuel Tsochatzis a; George V. Papatheodoridis a; Emilia Hadziyannis a;Anastasia Georgiou a; Georgia Kafiri b; Dina G. Tiniakos c; Emanuel K. Manesis a;Athanasios J. Archimandritis aa Second Department of Internal Medicine, Athens University Medical School,Hippokration General Hospital, Athens, Greeceb Department of Pathology, Hippokration General Hospital, Athens, Greecec Laboratory of Histology & Embryology, Athens University Medical School, Greece
First Published on: 30 April 2008
To cite this Article: Tsochatzis, Emmanuel, Papatheodoridis, George V., Hadziyannis, Emilia, Georgiou, Anastasia,Kafiri, Georgia, Tiniakos, Dina G., Manesis, Emanuel K. and Archimandritis, Athanasios J. (2008) 'Serum adipokinelevels in chronic liver diseases: Association of resistin levels with fibrosis severity', Scandinavian Journal ofGastroenterology,
To link to this article: DOI: 10.1080/00365520802085387URL: http://dx.doi.org/10.1080/00365520802085387
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article maybe used for research, teaching and private study purposes. Any substantial or systematic reproduction,re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expresslyforbidden.
The publisher does not give any warranty express or implied or make any representation that the contents will becomplete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should beindependently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings,demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with orarising out of the use of this material.

Dow
nloa
ded
By:
[HE
AL-
Link
Con
sorti
um] A
t: 17
:37
15 M
ay 2
008
ORIGINAL ARTICLE
Serum adipokine levels in chronic liver diseases: Association of resistinlevels with fibrosis severity
EMMANUEL TSOCHATZIS1, GEORGE V. PAPATHEODORIDIS1,
EMILIA HADZIYANNIS1, ANASTASIA GEORGIOU1, GEORGIA KAFIRI2,
DINA G. TINIAKOS3, EMANUEL K. MANESIS1 & ATHANASIOS J. ARCHIMANDRITIS1
1Second Department of Internal Medicine, Athens University Medical School, Hippokration General Hospital, Athens,
Greece, 2Department of Pathology, Hippokration General Hospital, Athens, Greece, and 3Laboratory of Histology &
Embryology, Athens University Medical School, Greece
AbstractObjective. Leptin and adiponectin have been implicated in the pathogenesis and progression of non-alcoholicsteatohepatitis (NASH) and chronic hepatitis C (CHC), but little is known about the role of resistin in chronic liverdiseases. The objective of this study was to investigate serum levels of the above three adipokines in relation to the etiology ofliver disease and to determine their associations with histological severity. Material and methods. We prospectivelyevaluated 146 patients (HBeAg-negative chronic hepatitis B (CHB): 52, CHC: 70, NASH: 24) who consecutivelyunderwent liver biopsy. Detailed epidemiological, anthropometric and laboratory data were recorded. Histological lesionswere evaluated blindly according to the Ishak and the Brunt classifications for CHB/CHC and NASH, respectively.Results. Serum adipokine levels were similar between CHB and CHC patients, while CHB/CHC patients had significantlylower leptin levels compared with NASH patients (8.397.3 versus 17.6916.6 ng/ml, p�0.012) and higher adiponectin(10.295.1 versus 7.594 mg/ml, p�0.018) and resistin levels (7.192.5 versus 5.792.8 ng/ml, p�0.016). In CHB/CHC,there was no significant association between steatosis or necroinflammation and levels of adipokines, while the presence ofmoderate/severe fibrosis (stages 4�6) was associated with higher leptin and adiponectin levels in male but not in femalepatients and with lower resistin levels irrespective of gender or other factors (adjusted odds ratio�0.788, p�0.035).Conclusions. Serum adipokine levels depend on the etiology of liver disease differing between chronic viral hepatitis andNASH, but not between CHB and CHC. In CHB/CHC, resistin levels are independently associated with fibrosis severity,whereas in the association of leptin and adiponectin levels with fibrosis, it seems to be a gender effect.
Key Words: Adipokines, adiponectin, chronic hepatitis B, chronic hepatitis C, leptin, non-alcoholic steatohepatitis, resistin
Introduction
In recent years, adipose tissue has gained attention
as a metabolically active tissue that secretes bioactive
proteins, called adipokines. The adipokines, which
include leptin, adiponectin and resistin, participate
in energy homeostasis and the inflammatory re-
sponse. Leptin is an anorexigenic hormone and is
increased in obesity as a consequence of leptin
resistance [1]. It has pro-inflammatory actions and
is involved in fibrogenesis in various in vitro and
animal models [2]. Adiponectin is an anti-inflam-
matory cytokine that reduces body fat, ameliorates
insulin resistance (IR) and has hepatoprotective
actions [2]. Finally, resistin primarily causes hepatic
IR in rodents but its role in human disease is still
unclear [3].
Hepatic steatosis is a hallmark of non-alcoholic
fatty liver disease (NAFLD), but its role seems to be
crucial as a co-factor of disease progression in other
liver diseases, most importantly in chronic hepatitis
C (CHC), whereas it does not seem to influence
fibrosis severity in chronic hepatitis B (CHB) [4�6].
Since adipokines regulate lipogenesis, lipolysis and
fat distribution, they were initially studied in NAFLD
and suggested to participate in its pathogenesis.
Correspondence: George V. Papatheodoridis, MD, Second Department of Internal Medicine, Athens University Medical School, Hippokration General
Hospital of Athens, 114 Vas. Sophias Ave., GR-115 27 Athens, Greece. Tel: �30 210 7774 742. Fax: �30 210 7706 871. E-mail: [email protected]
Scandinavian Journal of Gastroenterology
2008, 1�9, iFirst article
(Received 10 December 2007; accepted 26 March 2008)
ISSN 0036-5521 print/ISSN 1502-7708 online # 2008 Taylor & Francis
DOI: 10.1080/00365520802085387

Dow
nloa
ded
By:
[HE
AL-
Link
Con
sorti
um] A
t: 17
:37
15 M
ay 2
008
When their involvement in inflammatory and fibro-
genic response became evident, leptin and adiponec-
tin were studied as markers of fibrosis and disease
severity mainly in CHC, but also in cholestasis and
cirrhosis [2]. Results, however, were contradictory,
possibly reflecting the heterogeneity of study popula-
tions or small-size samples. Resistin has not been
adequately studied in chronic liver diseases to date
[7,8].
In this study, we evaluated the metabolic and
adipokine profiles in patients with CHB, CHC and
non-alcoholic steatohepatitis (NASH). In particular,
our aims were a) to study the serum adipokine levels
in relation to the etiology of liver disease and b) to
clarify the associations of leptin and adiponectin
levels and to investigate the potential associations of
resistin levels with liver histology and with para-
meters of IR and metabolic syndrome in a well-
defined cohort of patients with chronic liver disease.
Material and methods
Patient population
We prospectively included 146 treatment-naı̈ve pa-
tients who consecutively underwent liver biopsy at
our Department between August 2004 and August
2006. Fifty-two patients had HBeAg-negative CHB,
70 CHC and 24 had NASH. Patients with HBeAg-
positive CHB, NAFLD and histological findings of
simple fatty liver, any type of therapy for their liver
disease, alcohol abuse, concomitant chronic HBV
and HCV infection, antibodies against hepatitis D
virus (anti-HDV), antibodies against human immu-
nodeficiency virus (anti-HIV), evidence of autoim-
mune liver disease or an inadequate liver biopsy were
excluded. None of the patients had decompensated
liver disease (evidence or history of ascites, variceal
bleeding, hepatic encephalopathy or jaundice from
hepatic failure) or evidence of hepatocellular carci-
noma (HCC).
The local ethics committee approved the study
protocol and all patients gave informed consent.
HBeAg-negative CHB was diagnosed in patients
with positive hepatitis B surface antigen (HBsAg),
negative hepatitis B e antigen (HBeAg) and positive
for its antibody (anti-HBe) for at least 6 months,
increased alanine aminotransferase (ALAT) on at
least two monthly occasions, detectable serum
hepatitis B virus (HBV) DNA, histological lesions
compatible with chronic viral hepatitis (CVH) and
absence of any other possible cause of liver injury.
CHC was diagnosed in patients with positive anti-
bodies against HCV (anti-HCV), detectable serum
hepatitis C virus (HCV) RNA and histological
lesions compatible with CVH. NASH was diagnosed
in patients with NAFLD and histological lesions
compatible with NASH. The diagnosis of NAFLD
was made in patients with increased ALAT activity
(�40 IU/l) on ]3 separate monthly determinations
within the last 6 months and evidence of hepatic
steatosis on liver biopsy provided that any other
possible cause of liver injury including alcohol abuse
had been excluded.
Epidemiological data were obtained from all
patients. Alcohol consumption during the past 5
years was taken into account and alcohol abuse was
excluded by careful questioning conducted by two
independent physicians, including interrogation of
family members, where possible. Alcohol abuse was
considered as a mean daily alcohol consumption of
�30 g for males and �20 g for females for CVH and
�20 g/day regardless of gender for NAFLD patients.
The presence of diabetes mellitus was also recorded
in known diabetics or patients with fasting glucose
�126 mg/dl on more than one occasion. Weight and
height were measured and body mass index (BMI)
(kg/m2) was calculated on the liver biopsy day. Waist
circumference was measured at the midpoint be-
tween the lower border of the rib cage and the iliac
crest, whereas hip circumference was measured at
the widest point between hip and buttock.
Metabolic syndrome was diagnosed in the pre-
sence of 3 or more out of 5 criteria, as defined by the
Adult Treatment Panel III [9], namely: 1) fasting
glucose ]110 mg/dl, 2) central adiposity, defined as
waist circumference �102 cm in men or �88 cm in
women, 3) hypertension, defined as systolic blood
pressure ]135 mmHg, diastolic blood pressure ]
85 mmHg or antihypertensive treatment 4) serum
triglycerides �150 mg/dl and 5) serum high-density
lipoprotein (HDL) cholesterol B40 mg/dl in men or
B50 mg/dl in women.
Laboratory methods
Blood chemistry values including complete blood
count, prothrombin time and levels of serum glu-
cose, cholesterol, HDL and low-density lipoprotein
(LDL), triglycerides and liver enzymes (ALAT,
aspartate aminotransferase (ASAT), alkaline phos-
phatase (ALP), gamma-glutamyl transpeptidase
(GGT)) were determined using commercially avail-
able assays on the liver biopsy day. Insulin levels were
also measured with the INS-EASIA kit (BioSource
Europe S.A., Nivelles, Belgium). IR was determined
by the homeostasis model assessment (HOMA)
method using the following equation: Insulin resis-
tance (HOMA)�Fasting insulin (mU/ml)�fasting
glucose (mmol/l)/22.5 [10]; IR was considered to be
present in cases with HOMA ]3.0.
2 E. Tsochatzis et al.

Dow
nloa
ded
By:
[HE
AL-
Link
Con
sorti
um] A
t: 17
:37
15 M
ay 2
008
Commercially available enzyme immunoassays
were used for detection of HBsAg, HBeAg, anti-
HBe, anti-HCV, anti-HDV and anti-HIV. In patients
with CHB, serum HBV DNA levels were deter-
mined with a commercially available quantitative
polymerase chain reaction (PCR) assay (Amplicor
HBV Monitor; Roche Molecular Diagnostics Sys-
tems, Branchburg, N.J., USA). In patients with
CHC, serum HCV RNA was detected using a
commercially available qualitative PCR assay (Am-
plicor; Roche Molecular Diagnostic Systems, sensi-
tivity: 30 IU/ml) and HCV genotype was determined
with a commercially available assay (HCV Genotype
Assay; LIPA, Versant, Bayer Healthcare, Tarrytown,
N.Y., USA).
All serum adipokine levels were determined in
stored serum samples using immunoenzymometric
assays. Serum samples were obtained after overnight
fasting on the liver biopsy day and were stored in
aliquots at �608C until assayed. Leptin was mea-
sured with the LEPTIN EASIA kit (BioSource
Europe S.A.), adiponectin with the Adiponectin
Elisa kit (Asbach Medical Products (AMP), Obrigh-
eim, Germany) and resistin with the Human Resistin
ELISA kit (Biovendor, Heidelberg, Germany).
Liver histology
All 146 liver biopsy specimens were of adequate
length (]1.5 cm). All biopsies from CVH patients
were evaluated blindly by one liver pathologist
(G.K.) in accordance with the classification system
proposed by Ishak et al. [11]. All biopsies from
NAFLD patients were evaluated blindly by another
liver pathologist (D.G.T.) according to the classifica-
tion system proposed by Brunt et al. [12]. NASH
was considered to be present in NAFLD cases with
grade score ]2 and/or fibrosis score ]1. In both
CVH and NASH, hepatic steatosis was assessed as
the percentage of hepatocytes containing fat droplets
and it was graded as 0 (B5% steatosis), 1 (mild, 5�33% of hepatocytes affected), 2 (moderate, 33�66%
of hepatocytes affected) and 3 (severe, �66% of
hepatocytes affected).
Statistical analysis
All data were analyzed using the statistical package
SPSS (version 14.0; SPSS Inc., Chicago, Ill., USA).
Statistical analysis was performed using the t-test,
ANOVA, the Mann-Whitney test or the Kruskal-
Wallis test for comparisons of continuous variables
between or among groups, the corrected x2 method
or the Fisher two-tailed exact test for comparisons of
qualitative data and Spearman’s coefficient for
correlations of quantitative data, when appropriate.
A two-tailed p-value of less than 0.05 was considered
to be statistically significant. In the univariate
analysis including multiple (K) comparisons, a
p-value of 0.05/K was considered to be statistically
significant. The multivariate analysis was performed
using backward logistic regression models. Only
variables with a p-value 50.10 at univariate analysis
were entered in the multivariate analysis models.
Results
Baseline characteristics
The patients’ baseline characteristics are presented
in Table I. The patients were middle-aged and
overweight, with a slight predominance of males.
Males and females were comparable in terms of age,
BMI, steatosis, necroinflammation grade and fibro-
sis stage. NASH patients had significantly higher
BMI values, higher values of triglycerides, more
severe steatosis and a more frequent presence of
glucose intolerance, central adiposity and metabolic
syndrome compared with patients with CVH. In-
sulin resistance was present in 44% and 46% of
patients with CVH and NASH, respectively.
Associations of serum adipokines with demographic and
metabolic parameters
The associations between each adipokine level and
all patients’ characteristics are summarized in
Table II. Higher serum leptin levels were signifi-
cantly associated with increasing age (r�0.173, p�0.029), increasing BMI (r�0.417, pB0.001), fe-
male gender (PB0.001), presence of IR (p�0.012),
central adiposity (pB0.001), diabetes mellitus
(p�0.025), presence of metabolic syndrome (pB
0.001), increasing serum adiponectin (r�0.263,
p�0.002) and decreasing serum resistin levels
(r��0.164, p�0.049). Higher serum adiponectin
levels were significantly associated with increasing
age (r�0.298, pB0.001), female gender (pB0.001)
and increasing leptin levels. Finally, higher serum
resistin levels significantly correlated only with
female gender (p�0.001) and decreasing leptin
levels. No association was noted between any
adipokine and viral load in CHB or CHC patients.
Serum adipokines and etiology of chronic liver disease
Serum adipokine levels did not significantly differ
between patients with CHB and CHC (Table III).
Patients with CVH had significantly lower leptin
levels (8.397.3 versus 17.6916.6 ng/ml, p�0.012)
and higher adiponectin (10.295.1 versus 7.594.0
mg/ml, p�0.018) and resistin levels (7.192.5 versus
5.792.8 ng/ml, p�0.016) compared with patients
Adipokines in chronic liver diseases 3

Dow
nloa
ded
By:
[HE
AL-
Link
Con
sorti
um] A
t: 17
:37
15 M
ay 2
008
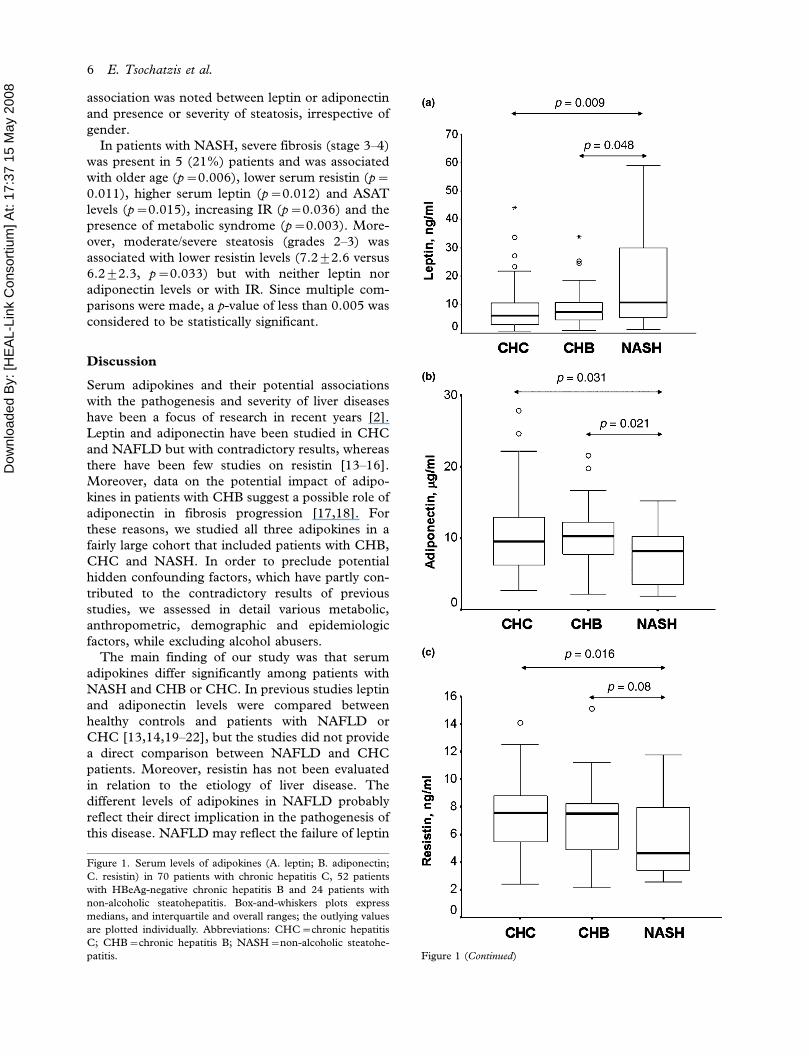
with NASH. Leptin, adiponectin and resistin levels
in patients with CHC, CHB and NASH are depicted
in Figure 1. Among patients with CHC, 11 had
infection with genotype 3 and 59 with genotype non-
3. Serum leptin levels were significantly higher and
serum resistin significantly lower in genotype non-3
compared with genotype 3 CHC patients, while
no difference was noted for adiponectin levels
(Figure 2). In CHB patients without steatosis
(n�16), who may be considered as cases with
chronic liver disease unrelated to disturbances in
fat metabolism, serum adiponectin levels were
higher than those in the remaining CVH patients
(12.693.8 versus 9.995.2, p�0.018), while no
significant difference was noted for leptin and
resistin levels. Insulin resistance did not significantly
differ among patients with CHB, CHC and NASH.
All the above associations did not significantly
change after adjustment for age, gender and BMI.
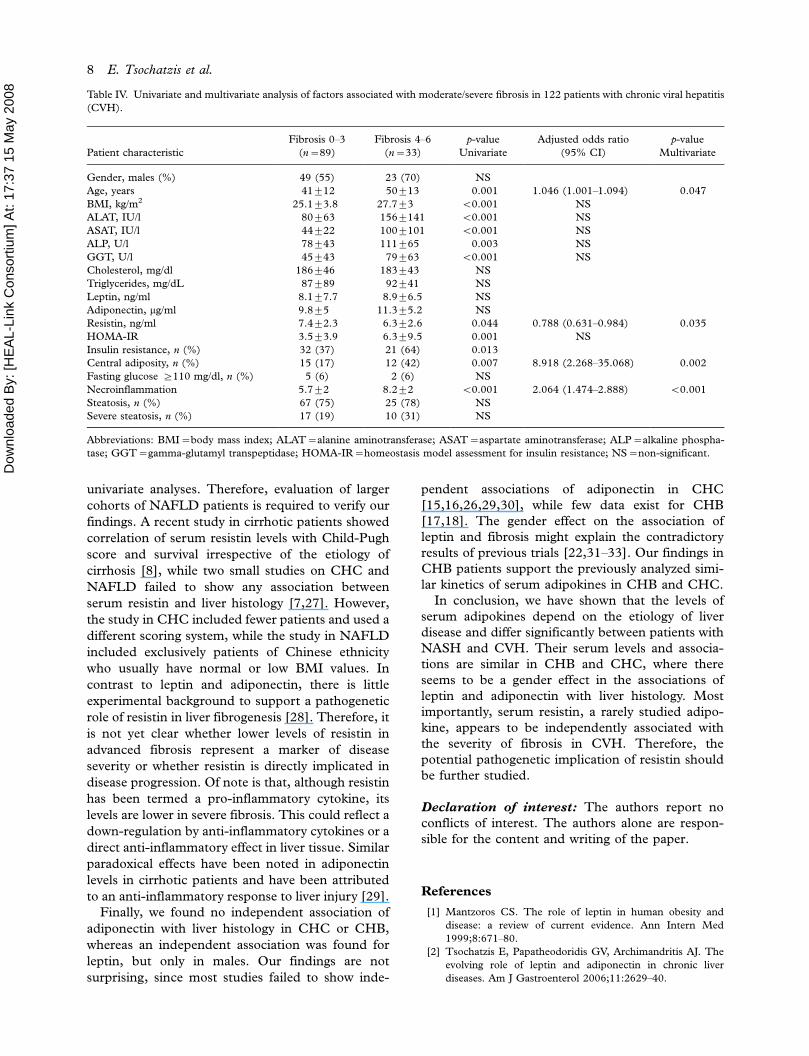
Serum adipokines and liver histology
As serum adipokine levels did not significantly differ
between CHB and CHC patients, we addressed
their potential associations with liver histology in the
whole cohort of 122 CVH patients (Table IV).
Severe fibrosis (stages 4�6) was detected in 33
(27%) of the CVH patients. In the univariate
analysis, severe fibrosis was associated with advanced
age, increased BMI, higher necroinflammation
grade, higher HOMA index, increased serum
ASAT, ALAT, ALP and GGT levels and decreased
serum resistin levels, but not with leptin or adipo-
nectin levels. In the multivariate analysis, lower
serum resistin was, among others, an independent
predictor of severe fibrosis (OR: 0.788, 95% CI:
0.631�0.984, p�0.035) (Table IV). No significant
association between steatosis or necroinflammation
and serum adipokine levels was noted (data not
shown). Similar findings were observed when an
analysis was done separately for CHB and CHC or
for genotype 3 and non-3 CHC or when patients
with CHC and diabetes mellitus were excluded (data
not shown).
When males and females were analyzed separately,
some additional associations between adipokine
levels and histological parameters were found. In
particular, leptin levels were higher only in males
with severe fibrosis than in those without severe
fibrosis (7.495.1 versus 4.593.5 ng/ml, p�0.013)
but not in females. Similarly, serum adiponectin
levels correlated with the severity of necroinflamma-
tion only in males (r�0.29, p�0.016) and were
higher only in male patients with than in those
without severe fibrosis (11.195.0 versus 8.194.3
mg/ml, p�0.021). In contrast, serum resistin levels
Table I. Baseline characteristics of 146 patients with chronic liver disease, chronic viral hepatitis (CVH): 122, non-alcoholic steatohepatitis
(NASH): [24].
Patient characteristics CHB (n�52) CHC (n�70) CVH (n�122) NASH (n�24) p-value1
Gender, males (%) 36 (69) 36 (51) 72 (59) 13 (54) NS
Age, years 41.5912.9 44.5911.9 43.2912.4 45.2916.5 NS
BMI, kg/m2 26.593.9 25.393.6 25.893.8 29.294.5 0.002
ALAT, IU/l 1089129 95964 101997 74956 NS
ASAT, IU/l 65990 56933 60964 44924 NS
ALP, U/l 94964 84943 88952 101949 0.057
GGT, U/l 57961 54944 55951 999107 0.061
Cholesterol, mg/dl 194946 179944 185945 202942 0.085
HDL, mg/dl 48918 46915 47916 46912 NS
LDL, mg/dl 126945 114934 119939 134943 NS
Triglycerides, mg/dl 90943 88963 89955 118942 0.006
HOMA-IR 5.598.7 3.492.5 4.396 492.9 NS
Insulin resistance, n (%) 26 (50) 27 (39) 53 (44) 11 (46) NS
Central adiposity, n (%) 9 (17) 15 (21) 29 (24) 13 (54) 0.005
Fasting glucose ]110 mg/dl, n (%) 1 (2) 6 (9) 7 (6) 6 (25) 0.008
Metabolic syndrome, n (%) 2 (4) 5 (7) 7 (6) 9 (37) B0.001
Necroinflammation* 6.192.7 6.592 6.492.3 2.090.7 �Fibrosis* 2.991.8 2.991.4 2.991.5 2.391.1 �Steatosis, n (%) 36 (71) 56 (80) 92 (76) 24 (100) 0.004
Severe steatosis, n (%) 8 (16) 19 (27) 27 (22) 15 (62) B0.001
Abbreviations: CHB�HBeAg-negative chronic hepatitis B; CHC�chronic hepatitis C; BMI�body mass index; ALAT�alanine
aminotransferase; ASAT�aspartate aminotransferase; ALP�alkaline phosphatase; GGT�gamma-glutamyl transpeptidase; HDL�high-density lipoprotein; LDL�low-density lipoprotein; HOMA-IR�homeostasis model assessment for insulin resistance; NS�non-
significant.
*Necroinflammation and fibrosis were evaluated using the Ishak classification system [11] in CVH patients and the Brunt classification
system [12] in NASH patients; 1p-values for comparisons between CVH and NASH patients.
4 E. Tsochatzis et al.
Dow
nloa
ded
By:
[HE
AL-
Link
Con
sorti
um] A
t: 17
:37
15 M
ay 2
008
were lower in patients with than in those without
severe fibrosis, irrespective of gender. In the multi-
variate analysis including only male patients, in-
creased serum leptin levels but not adiponectin levels
were independently associated with severe fibrosis
(OR: 1.231, 95%CI 1.029�1.473, p�0.023) No
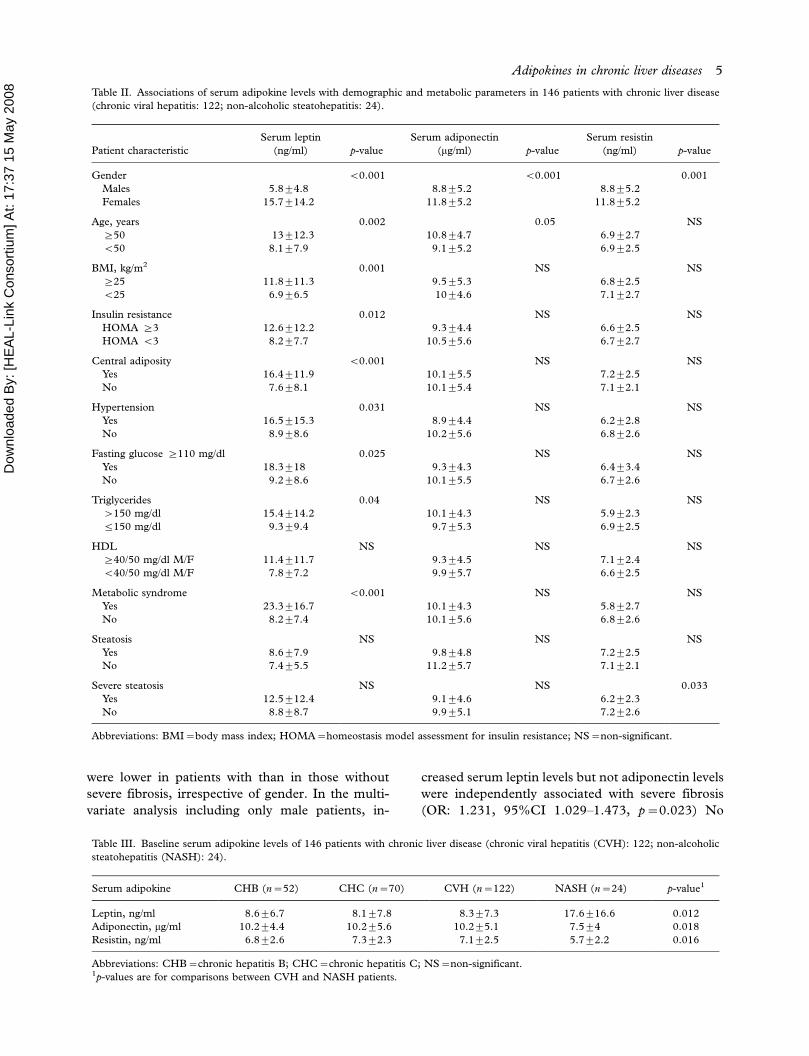
Table II. Associations of serum adipokine levels with demographic and metabolic parameters in 146 patients with chronic liver disease
(chronic viral hepatitis: 122; non-alcoholic steatohepatitis: 24).
Patient characteristic
Serum leptin
(ng/ml) p-value
Serum adiponectin
(mg/ml) p-value
Serum resistin
(ng/ml) p-value
Gender B0.001 B0.001 0.001
Males 5.894.8 8.895.2 8.895.2
Females 15.7914.2 11.895.2 11.895.2
Age, years 0.002 0.05 NS
]50 13912.3 10.894.7 6.992.7
B50 8.197.9 9.195.2 6.992.5
BMI, kg/m2 0.001 NS NS
]25 11.8911.3 9.595.3 6.892.5
B25 6.996.5 1094.6 7.192.7
Insulin resistance 0.012 NS NS
HOMA ]3 12.6912.2 9.394.4 6.692.5
HOMA B3 8.297.7 10.595.6 6.792.7
Central adiposity B0.001 NS NS
Yes 16.4911.9 10.195.5 7.292.5
No 7.698.1 10.195.4 7.192.1
Hypertension 0.031 NS NS
Yes 16.5915.3 8.994.4 6.292.8
No 8.998.6 10.295.6 6.892.6
Fasting glucose ]110 mg/dl 0.025 NS NS
Yes 18.3918 9.394.3 6.493.4
No 9.298.6 10.195.5 6.792.6
Triglycerides 0.04 NS NS
�150 mg/dl 15.4914.2 10.194.3 5.992.3
5150 mg/dl 9.399.4 9.795.3 6.992.5
HDL NS NS NS
]40/50 mg/dl M/F 11.4911.7 9.394.5 7.192.4
B40/50 mg/dl M/F 7.897.2 9.995.7 6.692.5
Metabolic syndrome B0.001 NS NS
Yes 23.3916.7 10.194.3 5.892.7
No 8.297.4 10.195.6 6.892.6
Steatosis NS NS NS
Yes 8.697.9 9.894.8 7.292.5
No 7.495.5 11.295.7 7.192.1
Severe steatosis NS NS 0.033
Yes 12.5912.4 9.194.6 6.292.3
No 8.898.7 9.995.1 7.292.6
Abbreviations: BMI�body mass index; HOMA�homeostasis model assessment for insulin resistance; NS�non-significant.
Table III. Baseline serum adipokine levels of 146 patients with chronic liver disease (chronic viral hepatitis (CVH): 122; non-alcoholic
steatohepatitis (NASH): 24).
Serum adipokine CHB (n�52) CHC (n�70) CVH (n�122) NASH (n�24) p-value1
Leptin, ng/ml 8.696.7 8.197.8 8.397.3 17.6916.6 0.012
Adiponectin, mg/ml 10.294.4 10.295.6 10.295.1 7.594 0.018
Resistin, ng/ml 6.892.6 7.392.3 7.192.5 5.792.2 0.016
Abbreviations: CHB�chronic hepatitis B; CHC�chronic hepatitis C; NS�non-significant.1p-values are for comparisons between CVH and NASH patients.
Adipokines in chronic liver diseases 5
Dow
nloa
ded
By:
[HE
AL-
Link
Con
sorti
um] A
t: 17
:37
15 M
ay 2
008
association was noted between leptin or adiponectin
and presence or severity of steatosis, irrespective of
gender.
In patients with NASH, severe fibrosis (stage 3�4)
was present in 5 (21%) patients and was associated
with older age (p�0.006), lower serum resistin (p�0.011), higher serum leptin (p�0.012) and ASAT
levels (p�0.015), increasing IR (p�0.036) and the
presence of metabolic syndrome (p�0.003). More-
over, moderate/severe steatosis (grades 2�3) was
associated with lower resistin levels (7.292.6 versus
6.292.3, p�0.033) but with neither leptin nor
adiponectin levels or with IR. Since multiple com-
parisons were made, a p-value of less than 0.005 was
considered to be statistically significant.
Discussion
Serum adipokines and their potential associations
with the pathogenesis and severity of liver diseases
have been a focus of research in recent years [2].
Leptin and adiponectin have been studied in CHC
and NAFLD but with contradictory results, whereas
there have been few studies on resistin [13�16].
Moreover, data on the potential impact of adipo-
kines in patients with CHB suggest a possible role of
adiponectin in fibrosis progression [17,18]. For
these reasons, we studied all three adipokines in a
fairly large cohort that included patients with CHB,
CHC and NASH. In order to preclude potential
hidden confounding factors, which have partly con-
tributed to the contradictory results of previous
studies, we assessed in detail various metabolic,
anthropometric, demographic and epidemiologic
factors, while excluding alcohol abusers.
The main finding of our study was that serum
adipokines differ significantly among patients with
NASH and CHB or CHC. In previous studies leptin
and adiponectin levels were compared between
healthy controls and patients with NAFLD or
CHC [13,14,19�22], but the studies did not provide
a direct comparison between NAFLD and CHC
patients. Moreover, resistin has not been evaluated
in relation to the etiology of liver disease. The
different levels of adipokines in NAFLD probably
reflect their direct implication in the pathogenesis of
this disease. NAFLD may reflect the failure of leptin
Figure 1. Serum levels of adipokines (A. leptin; B. adiponectin;
C. resistin) in 70 patients with chronic hepatitis C, 52 patients
with HBeAg-negative chronic hepatitis B and 24 patients with
non-alcoholic steatohepatitis. Box-and-whiskers plots express
medians, and interquartile and overall ranges; the outlying values
are plotted individually. Abbreviations: CHC�chronic hepatitis
C; CHB�chronic hepatitis B; NASH�non-alcoholic steatohe-
patitis. Figure 1 (Continued)
6 E. Tsochatzis et al.

Dow
nloa
ded
By:
[HE
AL-
Link
Con
sorti
um] A
t: 17
:37
15 M
ay 2
008
to prevent ectopic lipid accumulation, referred to as
lipotoxicity, and is thus a leptin-resistant state [14].
Furthermore, the hepatoprotective adiponectin that
improves insulin sensitivity and regulates triglyceride
metabolism seems to be down-regulated and its
effects thus negated [20]. Although resistin has
been associated with IR, no experimental data exist
on its potential association with the pathogenesis of
liver disease. In a recent study of 80 Asian patients
with NAFLD and 48 controls, serum resistin levels
did not differ between NAFLD and controls or
NAFLD and NASH, although unmatched controls
were used and adjustments were not made [7]. Our
findings suggest that resistin may participate in the
pathogenesis of NAFLD, as its levels were found to
correlate with both steatosis and fibrosis severity in
our NASH patients. It is not clear whether the
adipokine deregulation is part of the ‘‘first’’ or
‘‘second’’ hit in NASH development [23], as few
studies have directly compared controls, patients
with simple steatosis and patients with NASH [20].
Adipokine profiles and all their associations did
not differ significantly between patients with CHB
and CHC. Of note is the difference observed in
serum leptin and resistin levels between CHC
patients with genotype 3 and non-3. Genotype-3
CHC has unique virological features, as it is
steatogenic per se and does not cause IR, in sharp
contrast to genotype non-3 [4,6,24,25]. We and
others have implied that patients with genotype 3
have different adipokine profiles and this is probably
attributed to the absence of IR [2,26]. Our findings,
although restricted in a small group of genotype-3
patients, further support this hypothesis.
Another finding of our study is a possible gender
effect in the associations between serum adipokines
and liver histology. Interestingly, we found positive
correlations between serum leptin and adiponectin
levels and fibrosis only in male patients with CHB or
CHC. On the one hand, this finding cannot be
directly attributed to confounding factors, as male
and female patients did not differ significantly in any
of the metabolic and histological parameters. On the
other hand, gender has previously been found to
affect the serum levels of adipokines. In particular, a
gender effect in the association between leptin [27]
and adiponectin levels [15] with the severity of
steatosis has been demonstrated in CHC patients.
This observation, although recorded, was not further
analyzed. Estrogen effects or gender-mediated adi-
pokine-receptor activities might be a possible ex-
planation of this finding, which needs further study
and verification.
Serum resistin levels were found to be indepen-
dently associated with fibrosis severity in patients
with CHB or CHC. They were also associated with
the severity of steatosis and fibrosis in NASH, but
only a small number of these patients were included
in the multivariate analysis, and multiple compar-
isons errors might have affected our results from
Figure 2. Serum levels of adipokines (A. leptin; B. adiponectin;
C. resistin) in relation to the hepatitis C virus (HCV) genotype.
Box- and-whiskers plots express medians, and interquartile and
overall ranges; the outlying values are plotted individually.
Adipokines in chronic liver diseases 7
Dow
nloa
ded
By:
[HE
AL-
Link
Con
sorti
um] A
t: 17
:37
15 M
ay 2
008
univariate analyses. Therefore, evaluation of larger
cohorts of NAFLD patients is required to verify our
findings. A recent study in cirrhotic patients showed
correlation of serum resistin levels with Child-Pugh
score and survival irrespective of the etiology of
cirrhosis [8], while two small studies on CHC and
NAFLD failed to show any association between
serum resistin and liver histology [7,27]. However,
the study in CHC included fewer patients and used a
different scoring system, while the study in NAFLD
included exclusively patients of Chinese ethnicity
who usually have normal or low BMI values. In
contrast to leptin and adiponectin, there is little
experimental background to support a pathogenetic
role of resistin in liver fibrogenesis [28]. Therefore, it
is not yet clear whether lower levels of resistin in
advanced fibrosis represent a marker of disease
severity or whether resistin is directly implicated in
disease progression. Of note is that, although resistin
has been termed a pro-inflammatory cytokine, its
levels are lower in severe fibrosis. This could reflect a
down-regulation by anti-inflammatory cytokines or a
direct anti-inflammatory effect in liver tissue. Similar
paradoxical effects have been noted in adiponectin
levels in cirrhotic patients and have been attributed
to an anti-inflammatory response to liver injury [29].
Finally, we found no independent association of
adiponectin with liver histology in CHC or CHB,
whereas an independent association was found for
leptin, but only in males. Our findings are not
surprising, since most studies failed to show inde-
pendent associations of adiponectin in CHC
[15,16,26,29,30], while few data exist for CHB
[17,18]. The gender effect on the association of
leptin and fibrosis might explain the contradictory
results of previous trials [22,31�33]. Our findings in
CHB patients support the previously analyzed simi-
lar kinetics of serum adipokines in CHB and CHC.
In conclusion, we have shown that the levels of
serum adipokines depend on the etiology of liver
disease and differ significantly between patients with
NASH and CVH. Their serum levels and associa-
tions are similar in CHB and CHC, where there
seems to be a gender effect in the associations of
leptin and adiponectin with liver histology. Most
importantly, serum resistin, a rarely studied adipo-
kine, appears to be independently associated with
the severity of fibrosis in CVH. Therefore, the
potential pathogenetic implication of resistin should
be further studied.
Declaration of interest: The authors report no
conflicts of interest. The authors alone are respon-
sible for the content and writing of the paper.
References
[1] Mantzoros CS. The role of leptin in human obesity and
disease: a review of current evidence. Ann Intern Med
1999;8:671�80.
[2] Tsochatzis E, Papatheodoridis GV, Archimandritis AJ. The
evolving role of leptin and adiponectin in chronic liver
diseases. Am J Gastroenterol 2006;11:2629�40.
Table IV. Univariate and multivariate analysis of factors associated with moderate/severe fibrosis in 122 patients with chronic viral hepatitis
(CVH).
Patient characteristic
Fibrosis 0�3(n�89)
Fibrosis 4�6(n�33)
p-value
Univariate
Adjusted odds ratio
(95% CI)
p-value
Multivariate
Gender, males (%) 49 (55) 23 (70) NS
Age, years 41912 50913 0.001 1.046 (1.001�1.094) 0.047
BMI, kg/m2 25.193.8 27.793 B0.001 NS
ALAT, IU/l 80963 1569141 B0.001 NS
ASAT, IU/l 44922 1009101 B0.001 NS
ALP, U/l 78943 111965 0.003 NS
GGT, U/l 45943 79963 B0.001 NS
Cholesterol, mg/dl 186946 183943 NS
Triglycerides, mg/dL 87989 92941 NS
Leptin, ng/ml 8.197.7 8.996.5 NS
Adiponectin, mg/ml 9.895 11.395.2 NS
Resistin, ng/ml 7.492.3 6.392.6 0.044 0.788 (0.631�0.984) 0.035
HOMA-IR 3.593.9 6.399.5 0.001 NS
Insulin resistance, n (%) 32 (37) 21 (64) 0.013
Central adiposity, n (%) 15 (17) 12 (42) 0.007 8.918 (2.268�35.068) 0.002
Fasting glucose ]110 mg/dl, n (%) 5 (6) 2 (6) NS
Necroinflammation 5.792 8.292 B0.001 2.064 (1.474�2.888) B0.001
Steatosis, n (%) 67 (75) 25 (78) NS
Severe steatosis, n (%) 17 (19) 10 (31) NS
Abbreviations: BMI�body mass index; ALAT�alanine aminotransferase; ASAT�aspartate aminotransferase; ALP�alkaline phospha-
tase; GGT�gamma-glutamyl transpeptidase; HOMA-IR�homeostasis model assessment for insulin resistance; NS�non-significant.
8 E. Tsochatzis et al.

Dow
nloa
ded
By:
[HE
AL-
Link
Con
sorti
um] A
t: 17
:37
15 M
ay 2
008
[3] McTernan PG, Kusminski CM, Kumar S. Resistin. Curr
Opin Lipidol 2006;2:170�5.
[4] Bugianesi E, McCullough AJ, Marchesini G. Insulin resis-
tance: a metabolic pathway to chronic liver disease. Hepa-
tology 2005;5:987�1000.
[5] Tsochatzis E, Papatheodoridis GV, Manesis EK, Chry-
santhos N, Kafiri G, Archimandritis AJ. Hepatic steatosis
in chronic hepatitis B develops due to host metabolic factors:
a comparative approach with genotype 1 chronic hepatitis C.
Digest Liver Dis 2007;39:936�42.
[6] Tsochatzis E, Papatheodoridis GV, Manesis EK, Chry-
santhos N, Kafiri G, Petraki K, et al. Hepatic steatosis in
genotype 4 chronic hepatitis C is mainly because of meta-
bolic factors. Am J Gastroenterol 2007;3:634�41.
[7] Wong VW, Hui AY, Tsang SW, Chan JL, Tse AM, Chan KF,
et al. Metabolic and adipokine profile of Chinese patients
with nonalcoholic fatty liver disease. Clin Gastroenterol
Hepatol 2006;4:1154�61.
[8] Yagmur E, Trautwein C, Gressner AM, Tacke F. Resistin
serum levels are associated with insulin resistance, disease
severity, clinical complications, and prognosis in patients
with chronic liver diseases. Am J Gastroenterol 2006;6:1244�52.
[9] Executive Summary of the Third Report of The National
Cholesterol Education Program (NCEP) Expert Panel on
Detection, Evaluation, and Treatment of High Blood Cho-
lesterol in Adults (Adult Treatment Panel III). JAMA
2001;19:2486�97.
[10] Matthews DR, Hosker JP, Rudenski AS, Naylor BA,
Treacher DF, Turner RC. Homeostasis model assessment:
insulin resistance and beta-cell function from fasting plasma
glucose and insulin concentrations in man. Diabetologia
1985;7:412�9.
[11] Ishak K, Baptista A, Bianchi L, Callea F, De GJ, Gudat F, et
al. Histological grading and staging of chronic hepatitis.
J Hepatol 1995;6:696�9.
[12] Brunt EM, Janney CG, Di Bisceglie AM, Neuschwander-
Tetri BA, Bacon BR. Nonalcoholic steatohepatitis: a propo-
sal for grading and staging the histological lesions. Am J
Gastroenterol 1999;9:2467�74.
[13] Bugianesi E, Pagotto U, Manini R, Vanni E, Gastaldelli A,
de IR, et al. Plasma adiponectin in nonalcoholic fatty liver is
related to hepatic insulin resistance and hepatic fat content,
not to liver disease severity. J Clin Endocrinol Metab 2005;6:
3498�504.
[14] Chitturi S, Farrell G, Frost L, Kriketos A, Lin R, Fung C,
et al. Serum leptin in NASH correlates with hepatic steatosis
but not fibrosis: a manifestation of lipotoxicity? Hepatology
2002;2:403�9.
[15] Jonsson JR, Moschen AR, Hickman IJ, Richardson MM,
Kaser S, Clouston AD, et al. Adiponectin and its receptors in
patients with chronic hepatitis C. J Hepatol 2005;6:929�36.
[16] Liu CJ, Chen PJ, Jeng YM, Huang WL, Yang WS, Lai MY,
et al. Serum adiponectin correlates with viral characteristics
but not histologic features in patients with chronic hepatitis
C. J Hepatol 2005;2:235�42.
[17] Hui C, Zhang H, Lee N, Chan W, Yueng Y, Leung K, et al.
Serum adiponectin is increased in advancing liver fibrosis
and declines with reduction in fibrosis in chronic hepatitis B.
J Hepatol 2007;47:191�202.
[18] Siagris D, Vafiadis G, Michalaki M, Lekkou A, Starakis A,
Makri M, et al. Serum adiponectin in chronic hepatitis C
and B. J Viral Hepat 2007;14:577�83.
[19] Angulo P, Alba LM, Petrovic LM, Adams LA, Lindor KD,
Jensen MD. Leptin, insulin resistance, and liver fibrosis in
human nonalcoholic fatty liver disease. J Hepatol 2004;6:
943�9.
[20] Hui JM, Hodge A, Farrell GC, Kench JG, Kriketos A,
George J. Beyond insulin resistance in NASH: TNF-alpha or
adiponectin? Hepatology 2004;1:46�54.
[21] Crespo J, Rivero M, Fabrega E, Cayon A, Amado JA,
Garcia-Unzeta MT, et al. Plasma leptin and TNF-alpha
levels in chronic hepatitis C patients and their relationship to
hepatic fibrosis. Dig Dis Sci 2002;7:1604�10.
[22] Giannini E, Ceppa P, Botta F, Mastracci L, Romagnoli P,
Comino I, et al. Leptin has no role in determining severity of
steatosis and fibrosis in patients with chronic hepatitis C. Am
J Gastroenterol 2000;11:3211�7.
[23] Day CP, James OF. Steatohepatitis: a tale of two ‘‘hits’’?
Gastroenterology 1998;4:842�5.
[24] Fartoux L, Poujol-Robert A, Guechot J, Wendum D,
Poupon R, Serfaty L. Insulin resistance is a cause of steatosis
and fibrosis progression in chronic hepatitis C. Gut 2005;7:
1003�8.
[25] Muzzi A, Leandro G, Rubbia-Brandt L, James R, Keiser O,
Malinverni R, et al. Insulin resistance is associated with liver
fibrosis in non-diabetic chronic hepatitis C patients. J
Hepatol 2005;1:41�6.
[26] Wang AY, Hickman IJ, Richards AA, Whitehead JP, Prins JB,
Macdonald GA. High molecular weight adiponectin corre-
lates with insulin sensitivity in patients with hepatitis C
genotype 3, but not genotype 1 infection. Am J Gastro-
enterol 2005;12:2717�23.
[27] Lo Iacono O, Venezia G, Petta S, Mineo C, De LS, Di MV,
et al. The impact of insulin resistance, serum adipocytokines
and visceral obesity on steatosis and fibrosis in patients with
chronic hepatitis C. Aliment Pharmacol Ther 2007;10:
1181�91.
[28] Bertolani C, Sancho-Bru P, Failli P, Bataller R, Aleffi S,
DeFranco R, et al. Resistin as an intrahepatic cytokine:
overexpression during chronic injury and induction of
proinflammatory actions in hepatic stellate cells. Am J Pathol
2006;169:2042�53.
[29] Tietge UJ, Boker KH, Manns MP, Bahr MJ. Elevated
circulating adiponectin levels in liver cirrhosis are associated
with reduced liver function and altered hepatic hemody-
namics. Am J Physiol Endocrinol Metab 2004;1:E82�9.
[30] Sato S, Furuta K, Mishiro T, Miyake T, Kohge N, Akagi S,
et al. Serum adiponectin concentration in patients with
hepatitis C virus. J Clin Gastroenterol 2005;8:744�5.
[31] Piche T, Vandenbos F, Bakar-Mahamat A, Vanbiervliet G,
Barjoan EM, Calle G, et al. The severity of liver fibrosis is
associated with high leptin levels in chronic hepatitis C.
J Viral Hepatol 2004;1:91�6.
[32] Romero-Gomez M, Castellano-Megias VM, Grande L, Irles
JA, Cruz M, Nogales MC, et al. Serum leptin levels correlate
with hepatic steatosis in chronic hepatitis C. Am J Gastro-
enterol 2003;5:1135�41.
[33] Manolakopoulos S, Bethanis S, Liapi C, Stripeli F, Sklavos
P, Margeli A, et al. An assessment of serum leptin levels in
patients with chronic viral hepatitis: a prospective study.
BMC Gastroenterol 2007;1:17.
Adipokines in chronic liver diseases 9
Related Documents



![Research Article Relevance of Plasma Obestatin and Early ...adipokine (leptin, resistin, and adiponectin), ghrelin, and obestatin [ , ]. With the development of blood glucose-lowering](https://static.cupdf.com/doc/110x72/60ed7df13f35e412bb291e36/research-article-relevance-of-plasma-obestatin-and-early-adipokine-leptin.jpg)







