PLEASE SCROLL DOWN FOR ARTICLE This article was downloaded by: [University of York] On: 16 October 2008 Access details: Access Details: [subscription number 788765713] Publisher Informa Healthcare Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Journal of Mental Health Publication details, including instructions for authors and subscription information: http://www.informaworld.com/smpp/title~content=t713432595 Self-help books for people with depression: A scoping review Rachel Richardson a ; David A. Richards a ; Michael Barkham b a Department of Health Sciences, University of York, York b Centre for Psychological Services Research, University of Sheffield, Sheffield, UK Online Publication Date: 01 October 2008 To cite this Article Richardson, Rachel, Richards, David A. and Barkham, Michael(2008)'Self-help books for people with depression: A scoping review',Journal of Mental Health,17:5,543 — 552 To link to this Article: DOI: 10.1080/09638230802053334 URL: http://dx.doi.org/10.1080/09638230802053334 Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf This article may be used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [University of York]On: 16 October 2008Access details: Access Details: [subscription number 788765713]Publisher Informa HealthcareInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Journal of Mental HealthPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t713432595
Self-help books for people with depression: A scoping reviewRachel Richardson a; David A. Richards a; Michael Barkham b
a Department of Health Sciences, University of York, York b Centre for Psychological Services Research,University of Sheffield, Sheffield, UK
Online Publication Date: 01 October 2008
To cite this Article Richardson, Rachel, Richards, David A. and Barkham, Michael(2008)'Self-help books for people with depression: Ascoping review',Journal of Mental Health,17:5,543 — 552
To link to this Article: DOI: 10.1080/09638230802053334
URL: http://dx.doi.org/10.1080/09638230802053334
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.
Self-help books for people with depression: A scopingreview
RACHEL RICHARDSON1, DAVID A. RICHARDS1, &
MICHAEL BARKHAM2
1Department of Health Sciences, University of York, York, and 2Centre for Psychological Services
Research, University of Sheffield, Sheffield, UK
AbstractBackground: There has been little research into self-help books for people with depression, despite theapparent plethora of such titles. As an initial step, we undertook a scoping review of available books.Aim: To identify the number of self-help books for people with depression or mixed anxiety anddepression that are available in the UK and to describe their principle characteristics.Methods: We located publicly available self-help books for people with depression or mixed anxietyand depression. We extracted data from the books we located that included descriptive information(including the psychological approach used), readability statistics and popularity measures.Results: We analysed data from 97 books. These publications were diverse in both structure andcontent. Structure and readability data illustrated that many potential readers may have difficulty usingsome of them. Popularity proved to be an unreliable way of locating books that would fulfil NICEguidance for a CBT based self-help programme.Conclusions: Many of the available books are complex to read in terms of literacy levels and maypresent additional problems given the concentration problems of people with depression. There is norelationship between popularity and a book being evidence-based or readable.
Keywords: Self-help books, depression
Introduction
Depression is a significant cause of personal distress, social disability and economic cost for
patients, families and society at large (Layard, 2006). The condition is highly prevalent: at
any one time more than 10% of the British population are suffering from depression alone or
mixed anxiety and depression (Office for National Statistics, 2001). We know that patients
would often prefer talking treatments to medication (Rogers et al., 1993, p. 124). However,
despite the fact that the National Institute for Health and Clinical Excellence (NICE) has
recognized that psychological therapies are as effective as antidepressants for most
depression (NICE, 2004), the majority of patients do not have access to talking treatments.
A recent survey published by the Office for National Statistics showed that only 9% of
people assessed as having a neurotic disorder were having counselling or therapy (Office for
National Statistics, 2001).
Correspondence: Rachel Richardson, Research Fellow, Area 4, Seebohm Rowntree Building, Department of Health Sciences,
University of York, York YO10 5DD, UK. Tel: þ44 (0)1904 321863. E-mail: [email protected]
Journal of Mental Health,
October 2008; 17(5): 543–552
ISSN 0963-8237 print/ISSN 1360-0567 online � Shadowfax Publishing and Informa UK Ltd.
DOI: 10.1080/09638230802053334
Downloaded By: [University of York] At: 10:21 16 October 2008
This unsatisfactory situation has led to calls for the development of increased open access
to psychological therapies focussing on self-management rather than traditional therapy
(Lovell & Richards, 2000). This direction has been reflected in both policy, for example the
Expert Patients Programme (Department of Health, 2001) and the National Service
Framework for Mental Health (Department of Health, 1999), and clinical guidelines, for
example the NICE clinical guideline on depression (NICE, 2004). The NHS has responded
to this challenge with various initiatives whereby self-help materials are made available to
patients. These include ‘‘books on prescription’’ schemes where a range of self-help books
are ‘‘prescribed’’ by a health professional and borrowed from a local library (Dobson, 2003).
Importantly, this policy direction reflects a patient-driven agenda, with self-help strategies
cited by patients as being an important part of managing mental health problems (Faulkner
& Layzell, 2000).
Nonetheless, there remain considerable issues to be resolved in the use of self-help as an
intervention for common mental health problems. First, reviewers have conflicting opinions
regarding the efficacy of self-help, opinions which are often a result of definitional
differences, particularly in regard to the amount of therapeutic support patients should
receive when undertaking a programme of self-help (Bower et al., 2001; Cuijpers, 1997;
Lewis et al., 2003). A recent review has noted, however, that whilst guided self-help for
depression may be effective, ‘‘pure’’ self-help is not supported by the current evidence
(Gellatly et al., 2007).
Second, there is the issue of whether self-help materials should be considered as
separate products analogous to a group of drugs such as SSRIs or a type of therapy such
as cognitive behaviour therapy (CBT). This is a critical issue since results from trials of
one self-help product can only be generalized if all self-help manuals and materials are
regarded as a single class of product. This has recently been illustrated by guidance in
the UK on the adoption of computerized cognitive behaviour therapy systems for
depression – a form of self-help. NICE ruled that randomized trial evidence from the
testing of one product (Beating the Blues) could not be generalized to others, despite the
class argument that all were based on an identical CBT model (NICE, 2006). According
to Anderson et al. (2005) only two self-help books have been evaluated in randomized
controlled trials and are available to members of the public: Managing anxiety and
depression (Holdsworth & Paxton, 1999) and Feeling good – the new mood therapy (Burns,
1999). We are also aware of one other book, What should I do? A handy guide to
managing depression and anxiety (Kennedy & Lovell, 2002) that has been evaluated in a
randomized controlled trial (Mead et al., 2005). There are, however, many more such
products available in both general circulation and specifically recommended by mental
health professionals.
Third, there is the difficulty arising from the abundance of books available. People seeking
a self-help book are faced with an array of material and most people with depression will not
have access to advice from a specialist mental health professional on which resource might
be best for them. People may use bestseller lists to select products. However these are self-
fulfilling: best selling books are automatically recommended above other products,
prompting more sales and high sales do not necessarily mean that a book is a useful
resource.
A final difficulty is the integration of ‘‘specific’’ and ‘‘common’’ factors into self-help
materials. We have recently pointed out (Richardson & Richards, 2006) that although the
efficacy of specific CBT techniques and their ability to be manualized has led them to be
translated into self-help formats, the independent agency of the therapeutic alliance has been
given little attention in these materials. There is considerable evidence that a strong
544 R. Richardson et al.
Downloaded By: [University of York] At: 10:21 16 October 2008
therapeutic alliance can have a positive impact on patient outcomes (Norcross, 2002).
Hence, it is reasonable to hypothesize that books that can engage the reader are likely to
produce better outcomes. However self-help books may vary in their degree of engagement
with the reader.
These issues make it extremely difficult for both the public and professionals to choose
and recommend appropriate self-help books. Books adopt differing theoretical perspectives.
Even when efficacious techniques are included in a book, if they are delivered without
attention to the therapeutic alliance, the material may not be as engaging as it might have
been. For mental health professionals, if the class argument is not accepted, any evidence of
efficacy from certain books may not be used as a reason to prescribe another. Currently there
are no recommendations based on a systematic appraisal of the content and style of self-help
books. Therefore, we set out to analyse the nature of self-help books readily available to the
public in the UK. The first stage of this work was a scoping review to identify the number
and nature of self-help books. We describe this work below.
Aim
To identify the number of self-help books for people with depression or mixed anxiety and
depression that are available in the UK and to describe their priniciple characteristics.
Methods
Inclusion criteria
We included self-help books according to the following criteria:
. Availability. Books had to be available for loan from any UK library, or to download
from a publicly accessible website. We excluded materials that could only be accessed
by patients through consultation with a health professional.
. Audience. In order to identify books that had the widest possible relevance we specified
that books had to be aimed at a general adult audience and not targeted at a specific age
group, gender, ethnic or religious group.
. Language. Only those written in English were included.
. Approach. Books had to be based around psychological approaches. We interpreted
this as books whose content originated from one of the ‘talking therapies’ i.e were based
on a body of literature drawing upon psychological theory or theories. We excluded
books based on, for example, dietary supplements.
. Content. Books had to offer more than just information about depression. Authors had
to offer specific advice and/or self-help strategies.
There was no restriction on publication date.
Search
We have described the search methods used in detail elsewhere (Richardson & Richards,
2006). Our aim was to identify as many as possible of the books available in the UK that
would meet our inclusion criteria. Briefly, we searched on-line bookshops, the British
Library catalogue, patient and professional websites, and the lists from ‘Books on
Prescription’ schemes.
Self-help for depression: Scoping review 545
Downloaded By: [University of York] At: 10:21 16 October 2008
Data extraction and analysis
We extracted and analysed:
(1) Descriptive information on: the year of publication of the latest edition; geographic base
of author; number of chapters; average length of each chapter; psychological model used;
the use or not of case histories; level of interactivity through the extent that books
included worksheets to fill in or exercises to complete by the reader; use of research
evidence categorized as ‘formal’ for those books that included references to research
papers in the text and a formal reference list, ‘informal’ for those books that
mentioned research evidence but did not include a reference list and ‘none’ for those
that did not include either of these.
(2) Readability statistics expressed as reading age. We scanned a page of text from the first
five pages of each book and then analysed the readability using the Flesch-Kincaid
Grade Level. We then added 5 to the figure obtained to convert the result into a
reading age figure.
(3) Popularity of the included books was assessed using Amazon sales rankings for
depression as a proxy measure of popularity.
One reviewer extracted the data and discussed this with a second reviewer where areas of
uncertainty were clarified.
Results
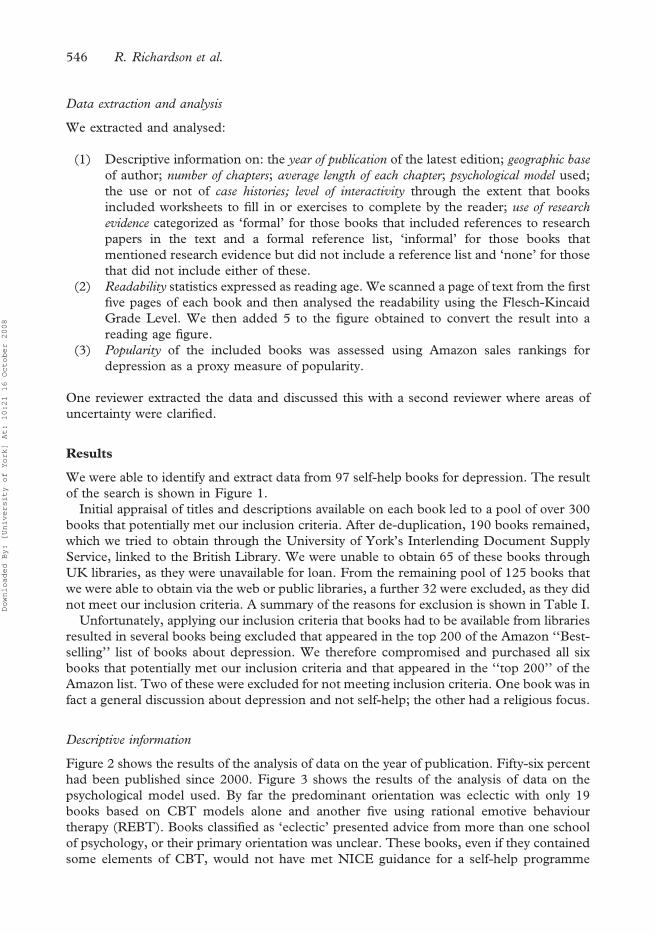
We were able to identify and extract data from 97 self-help books for depression. The result
of the search is shown in Figure 1.
Initial appraisal of titles and descriptions available on each book led to a pool of over 300
books that potentially met our inclusion criteria. After de-duplication, 190 books remained,
which we tried to obtain through the University of York’s Interlending Document Supply
Service, linked to the British Library. We were unable to obtain 65 of these books through
UK libraries, as they were unavailable for loan. From the remaining pool of 125 books that
we were able to obtain via the web or public libraries, a further 32 were excluded, as they did
not meet our inclusion criteria. A summary of the reasons for exclusion is shown in Table I.
Unfortunately, applying our inclusion criteria that books had to be available from libraries
resulted in several books being excluded that appeared in the top 200 of the Amazon ‘‘Best-
selling’’ list of books about depression. We therefore compromised and purchased all six
books that potentially met our inclusion criteria and that appeared in the ‘‘top 200’’ of the
Amazon list. Two of these were excluded for not meeting inclusion criteria. One book was in
fact a general discussion about depression and not self-help; the other had a religious focus.
Descriptive information
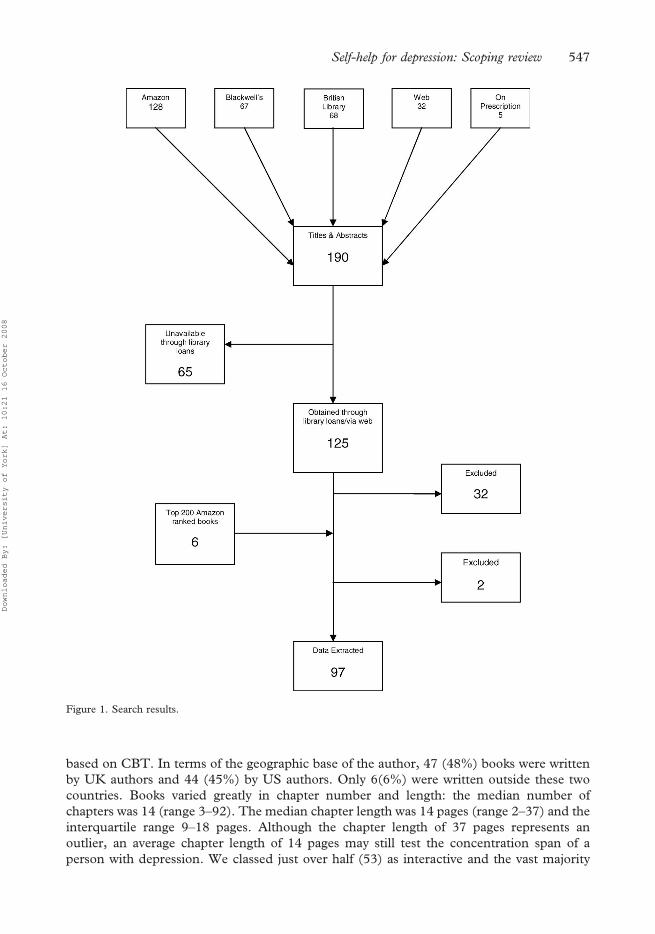
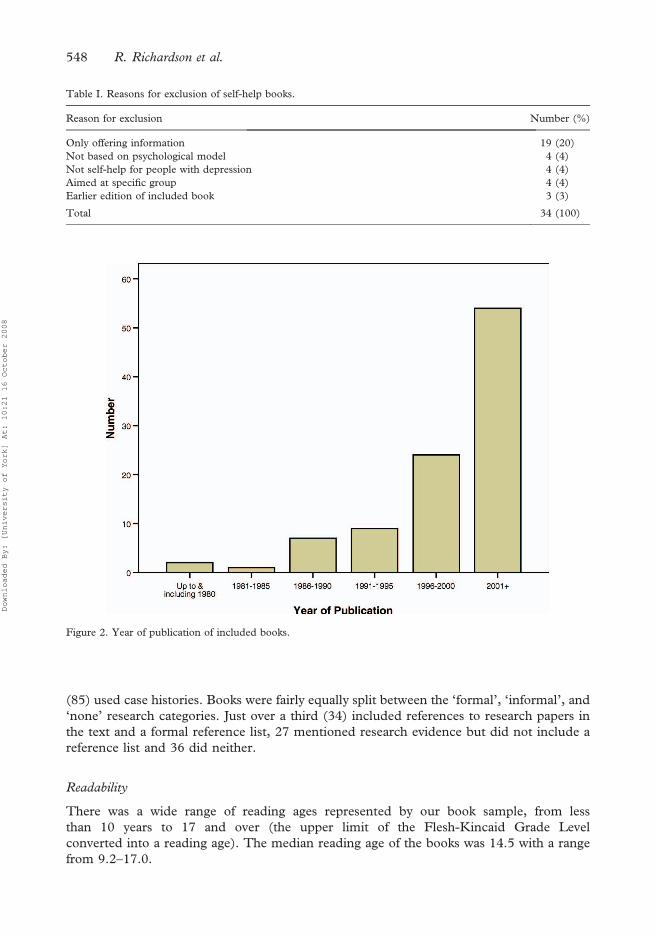
Figure 2 shows the results of the analysis of data on the year of publication. Fifty-six percent
had been published since 2000. Figure 3 shows the results of the analysis of data on the
psychological model used. By far the predominant orientation was eclectic with only 19
books based on CBT models alone and another five using rational emotive behaviour
therapy (REBT). Books classified as ‘eclectic’ presented advice from more than one school
of psychology, or their primary orientation was unclear. These books, even if they contained
some elements of CBT, would not have met NICE guidance for a self-help programme
546 R. Richardson et al.
Downloaded By: [University of York] At: 10:21 16 October 2008
based on CBT. In terms of the geographic base of the author, 47 (48%) books were written
by UK authors and 44 (45%) by US authors. Only 6(6%) were written outside these two
countries. Books varied greatly in chapter number and length: the median number of
chapters was 14 (range 3–92). The median chapter length was 14 pages (range 2–37) and the
interquartile range 9–18 pages. Although the chapter length of 37 pages represents an
outlier, an average chapter length of 14 pages may still test the concentration span of a
person with depression. We classed just over half (53) as interactive and the vast majority
Figure 1. Search results.
Self-help for depression: Scoping review 547
Downloaded By: [University of York] At: 10:21 16 October 2008
(85) used case histories. Books were fairly equally split between the ‘formal’, ‘informal’, and
‘none’ research categories. Just over a third (34) included references to research papers in
the text and a formal reference list, 27 mentioned research evidence but did not include a
reference list and 36 did neither.
Readability
There was a wide range of reading ages represented by our book sample, from less
than 10 years to 17 and over (the upper limit of the Flesh-Kincaid Grade Level
converted into a reading age). The median reading age of the books was 14.5 with a range
from 9.2–17.0.
Table I. Reasons for exclusion of self-help books.
Reason for exclusion Number (%)
Only offering information 19 (20)
Not based on psychological model 4 (4)
Not self-help for people with depression 4 (4)
Aimed at specific group 4 (4)
Earlier edition of included book 3 (3)
Total 34 (100)
Figure 2. Year of publication of included books.
548 R. Richardson et al.
Downloaded By: [University of York] At: 10:21 16 October 2008
Popularity
Table II shows the distribution of included books according to Amazon sales rankings. Just
under 50% of the books are in the Amazon top 500 with seven books occurring in the top
10. There are many other books listed under the Amazon depression ranking including
those concerning bipolar disorder, postnatal depression, complementary therapy for
depression and economic depression.
CBT versus Non- CBT Books
Given the focus on CBT in NICE guidelines we undertook some comparisons of the
characteristics of CBT/REBT versus non-CBT/REBT books. We did not find any difference in
the average chapter length of CBT/REBT versus non-CBT/REBT books (Independent
Samples T Test¼ 0.060, CI: –4.085 to 4.331, p¼ 0.953) nor in the average reading age
(Independent Samples T Test¼71.287, CI:71.667 to 0.371, p¼ 0.206). This would
suggest that books based on CBT/REBT models are no more difficult to read than books based
in other models. We also found that CBT/REBT books were no more likely to make overt use
Figure 3. Psychological model of included books.
Table II. Popularity: Amazon sales ranking.
Rank Number of books
1–500 46
501–1000 3
1001–1500 3
1501–2000 3
2001–2500 0
2501–3000 8
3001–3500 14
3501–4000 3
4000þ 0
Not listed 17
Total 97
Self-help for depression: Scoping review 549
Downloaded By: [University of York] At: 10:21 16 October 2008

of research than books based on other models (Chi-Square¼ 0.002, p¼ 0.964). However, not
unexpectedly, we found that CBT/REBT books were more likely to be interactive (Chi-
Square¼ 10.594, p¼ 0.001). We also analysed the position of CBT/REBT based self-help
books in the Amazon sales ranking. Twelve of these 24 books appeared in the top 500
positions, although seven were not listed at all in this category.
Discussion
We found 97 self-help books for depression that met our inclusion criteria, 93 of which could
be obtained from UK libraries. Whilst all purporting to be self-help books, these publications
are extremely diverse in both structure and content. Some of the techniques used (e.g., CBT)
have been the subject of rigorous clinical research whereas many of the others have not.
Indeed, despite the apparent growth in the rate of publication of self-help books since the year
2000 (although this could also be partly due to books published earlier going out of print),
there remain far fewer CBT books than one might expect.
Structure and readability data, including the average chapter length and the range of
reading ages required by these books, illustrate that many potential readers may have
difficulty using some of them. Even for people with a high reading age, an average chapter
length of 14 pages would require a span of concentration that may well be beyond people
with depression. The readability data is even more troubling. The majority of the books
require a reading age greater than 12 with 40% in the 15–17þ age range. To put this into
context A Tale of Two Cities (Dickens) has been calculated to have a reading age of 13 and
the Times Educational Supplement a reading age of 17 (Johnson, 1998, p. 7). The House of
Commons Public Accounts Committee recently estimated that there are about 12 million
people in employment with literacy skills at level 1 or below, which is equivalent to the level
expected of children 11 year old and younger (Public Accounts Committee, 2006). It is,
therefore, clear that due to literacy skill or because of the impact of the depression itself a
large proportion of adults would find the majority of currently available self-help books for
depression difficult to read. Similar difficulties are likely to be experienced for people whose
first language is not English. Books may be widely accessible, but their ability to be utilized
by the people they are aimed at may thus be limited. Interestingly, we did not find that CBT
based books were any more readable than books based on other psychological models. Being
based on an evidence-based model is no guarantee of superior readability.
With access to the internet becoming ever more ubiquitous, searching online book sellers
may become an ever more frequent means by which people find product information, even if
they subsequently purchase or borrow such products elsewhere. The included books in our
study spanned a wide range of positions on the ‘best-selling’ depression sales rankings on
Amazon, with some not listed at all. Although some of the CBT-based books appear in high
positions on the Amazon.co.uk ‘‘bestsellers’’ list, many do not appear at all. Relying on sales
figures-based popularity indices to identify an evidence-based book is not a reliable method.
Indeed, sales listings are self-reinforcing, independent of actual book quality or usability.
The average browser would be unlikely to scroll through more than a few pages of results
from an online bookstore and therefore those books at the top of the list listed in the first few
screens are likely to remain the ones selected for potential use.
Limitations
The major limitation of this review is that we had to exclude 59 of the 190 books identified
as potentially meeting the inclusion criteria, as we they were not obtainable from public
550 R. Richardson et al.
Downloaded By: [University of York] At: 10:21 16 October 2008
libraries. However, it is likely that several of these books would have failed to meet the
inclusion criteria once they had been obtained, so the deficit may not be that significant. We
are also confident that we have reviewed the most popular self-help books by obtaining all
those highest in the Amazon rankings.
It has sometimes proved difficult to apply the inclusion criteria relating to offering advice
rather than just information. There may be some books amongst those excluded whose
authors might argue that advice is offered and we had to make some difficult decisions.
Where we were in serious doubt, we erred towards including books. We are also not
implying that books just giving information about depression are unimportant and do not
have a therapeutic effect. However, we selected our inclusion criteria to try to find the books
that specifically offer self-help and thus might fall within the remit of the NICE guidelines
(NICE, 2004).
Conclusion and implications
The UK market for self-help books for depression is large and well supplied with a variety of
books, giving the consumer an apparently wide choice. However, on closer inspection, our
study has demonstrated that making a choice from such a large number of books is difficult.
. Many of the available books are complex to read in terms of literacy levels.
. Books may present additional problems given the concentration problems of people
with depression.
. There is no relationship between sales popularity and a book being evidence-based or
readable.
. Few books have been empirically tested.
Sales rankings are very influential in the commercial market but these are unrelated to
quality in terms of either an evidence-based (CBT) product or a readable one. Books are
never classified by either of these two criteria. Some readable and evidence based books
appear low down or not at all on sales rankings. Equally, whilst some evidence based books
appear high in the rankings, their readability statistics may render them unsuitable for many
potential readers. Libraries stock books that are popular or recommended by professionals.
In the same manner as the general public, professionals have little appraisal evidence with
which to recommend books. Indeed, lists used by ‘books on prescription schemes’ merely
tend to be very similar if not duplications of those used in other areas.
Given our findings, it is clearly inappropriate to apply the class argument, whereby all self-
help books for depression are considered to have similar therapeutic effects. This cannot be
true, even where books have the same psychological orientation, since they may vary along
so many other dimensions. The results of trials generated by one book, therefore, cannot be
generalized to others. Despite the proliferation of self-help books and the promotion of such
as a crucial element of modern mental health care (Rogers et al., 2004), we appear to have
little evidence with which to justify selection and use of specific self-help books more widely.
This has worrying implications for the people with depression who purchase and use these
books. We require an urgent research effort to develop and evaluate the use of specific
products in both a guided and self-managed form, similar to that currently being undertaken
in the UK for computerized CBT. These products should be developed to pay attention not
only to their core evidence base but also to their ease of use – including their readability,
their structure and their approach to engage readers. We need to replace the current
situation with one with a solid, and specific, evidence base.
Self-help for depression: Scoping review 551
Downloaded By: [University of York] At: 10:21 16 October 2008
Declaration of interest: The authors report no conflicts of interest. The authors alone are
responsible for the content and writing of the paper.
References
Anderson, L., Lewis, G., Araya, R., Elgie, R., Harrison, G., Proudfoot, J., Schmidt, U., Sharp, D., Weightman, A.
& Williams, C. (2005). Self-help books for depression: How can practitioners and patients make the right
choice? British Journal of General Practice, 55, 387–392.
Bower, P., Richards, D., & Lovell, K. (2001). The clinical and cost-effectiveness of self-help treatments for anxiety
and depressive disorders in primary care: A systematic review. British Journal of General Practice, 51, 838–845.
Burns, D.D. (1999). Feeling good – the new mood therapy. New York: Avon Books.
Cuijpers, P. (1997). Bibliotherapy in unipolar depression: A meta-analysis. Journal of Behavioural Therapy and
Experimental Psychiatry, 28, 139–147.
Department of Health. (1999). National service framework for mental health. London: Department of Health.
Department of Health. (2001). The expert patient: A new approach to chronic disease management for the 21st century.
London: Department of Health.
Dobson, R. (2003). GPs prescribe self-help books for mental health problems. British Medical Journal, 326, 1285.
Faulkner, A. & Layzell, S. (2000). Strategies for living: a report of user-led research into people’s strategies for living with
mental distress. London: The Mental Health Foundation.
Gellatly, J., Bower, P., Hennessy, S., Richards, D., Gilbody, S. & Lovell, K. (2007). What makes self-help
interventions effective in the management of depressive symptoms? Meta-analysis and meta-regression.
Psychological Medicine, 37, 1217–1228.
Holdsworth, N. & Paxton, R. (1999). Managing anxiety and depression. London: The Mental Health Foundation.
Johnson, K. (1998). Readability. Accessed 2 November 2006 from: http://www.timetabler.com/readable.pdf
Kennedy, A. & Lovell, K. (2005). What should I do? A handy guide to managing depression and anxiety. Southampton:
RTFB Publishing Limited.
Layard, R. (2006). The case for psychological treatment centres. British Medical Journal, 332, 1030–1032.
Lewis, G., Anderson, L., Araya, R., Elgie, R., Harrison, G., Proudfoot, J., Schmidt, U., Sharp, D., Weightman, A.,
& Williams, C. (2003). Self-help interventions for mental health problems. Bristol: University of Bristol.
Lovell, K. & Richards, D. (2000). Multiple access points and levels of entry (MAPLE): Ensuring choice,
accessibility and equity for CBT services. Behavioural and Cognitive Psychotherapy, 28, 379–391.
Mead, N., MacDonald, W., Bower, P., Lovell, K., Richards, D., Roberts, C., & Bucknall, A. (2005). The clinical
effectiveness of guided self-help versus waiting-list control in the management of anxiety and depression: a
randomized controlled trial. Psychological Medicine, 35, 1633–1643.
National Institute for Clinical Excellence. (2004). Depression: Management of depression in primary and secondary care.
Clinical Guideline 23. London: National Institute for Clinical Excellence.
National Institute for Health and Clinical Excellence. (2006). Computerised cognitive behaviour therapy for depression
and anxiety: review of Technology Appraisal 51. Technology Appraisal 97. London:National Institute for Health and
Clinical Excellence.
Norcross, J. (Ed.) (2002). Psychotherapy relationships that work: Therapist contributions and responsiveness to patients.
New York: Oxford University Press.
Office for National Statistics. (2001). Psychiatric morbidity amongst adults living in private households, 2000. London:
Office for National Statistics.
Public Accounts Committee. (2006). Skills for Life: Improving adult literacy and numeracy. Twenty-first report.
London: The Stationery Office.
Richardson, R. & Richards, D. (2006). Self-help: towards the next generation. Behavioural and Cognitive
Psychotherapy, 34, 13–23.
Richardson, R. & Richards, D. (2006). Designing a search strategy for locating self-help books for people with
depression. Health Information and Libraries Journal, 23, 294–295.
Rogers, A., Pilgrim, D., & Lacey, R. (1993). Experiencing psychiatry: users’ views of services. Basingstoke: The
Macmillan Press Ltd.
Rogers, A., Oliver, D., Bower, P., Lovell, K., & Richards, D. (2004). People’s understanding of a primary care-
based mental health self-help clinic. Patient Education and Counseling, 53, 41–46.
552 R. Richardson et al.
Downloaded By: [University of York] At: 10:21 16 October 2008
Related Documents











