Selected Strategies for Mitigation of Economic Impact Indrani Gupta Institute of Economic Growth Delhi Presented at the 7 th ICAAP, Kobe July 2005

Selected Strategies for Mitigation of Economic Impact Indrani Gupta Institute of Economic Growth Delhi Presented at the 7 th ICAAP, Kobe July 2005.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Selected Strategies for Mitigation of Economic Impact
Indrani GuptaInstitute of Economic Growth
Delhi
Presented at the 7th ICAAP, KobeJuly 2005
Impact has been studied, analyzed and discussed for several years now
Economy wide impact or
macroeconomic impact
Impact on sectors
Health
Education
Industry
Agriculture
Impact on households and individuals
Impact mitigation at the household and individual level
Integrating HIV/AIDS policies in the development and
poverty alleviation policies remain the most
important strategy of impact mitigation.
However, countries will continue to need more
specific policies that would meet the twin objectives
of impact mitigation and mainstreaming of HIV/AIDS
policies with other existing developmental efforts.
Mitigating impact at household and individual levels
would also help in mitigating impact at other levels.

Where is the economic impact the most on individuals and households?
While treatment costs have come down
drastically over the years, treatment of OIs and
ART continue to put serious strain on households
Therefore, making treatment available at reduced
costs to the maximum number continue to be one
of the most important strategies of impact
mitigation at the household and individual levels.
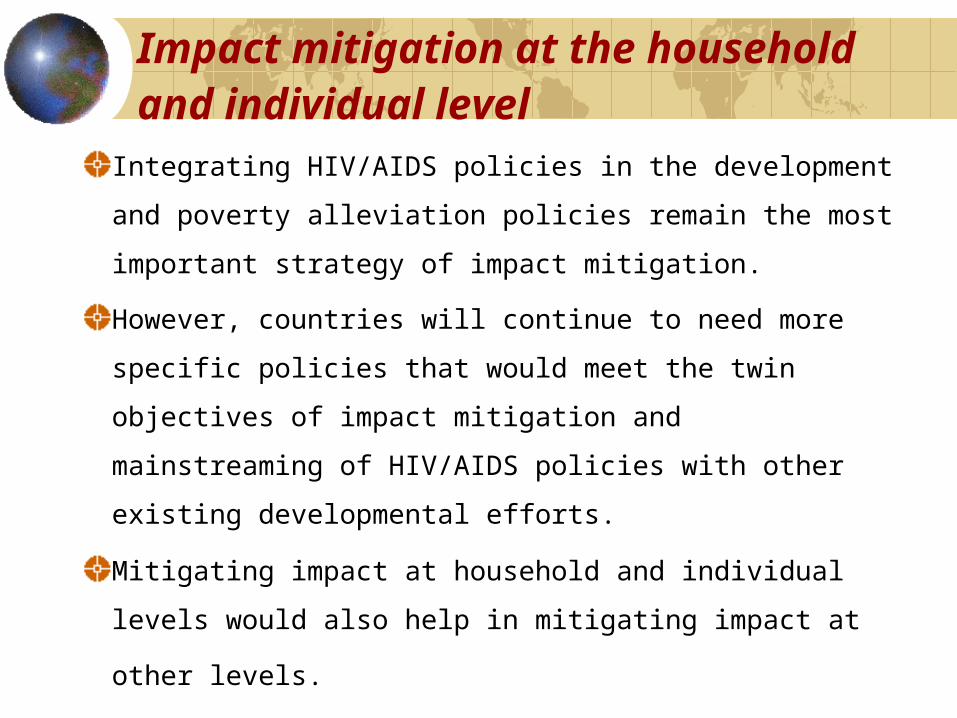
ART can mitigate impact of AIDS
Sectors
Impacts onHIV Positive
Impacts onHIV Negative
Affectedindividual
Saved healthy lifeyears
Averted years oforphanhood
Othersectors
Increased tenure,productivity ofHIV+ workers
E.g. Children whoare not orphanedwill have greaterdemand forschooling
Burden of treatment in India
In India, the price of the first line regimen has
come down significantly, but it is still around Rs.
1,200 per month.
Including monitoring tests, the burden of
treatment can be at least Rs. 2,000 per month.
This amount will be a burden not only for the
very poor households, but also for those in
higher economic categories.
The second line regimen plus tests would
impose a much greater burden on individuals.
Three ways of looking at coverage for ARV
Cover those who are HIV negative at inception
Amendments to existing insurance schemes initiated by
insurance companies
Cover those who are currently HIV positive in general
schemes for communities
Tailor-made schemes in collaboration with insurance companies,
and operated through organizations working in communities
Cover those who are HIV positive through specific
schemes
Tailor-made schemes for organisation working with HIV positive
individuals
Free ARV made available by other channels

Economic analysis can help governments in prioritizing and choosing the best alternative
Some examples of studies IEG has been involved in:
World Bank study on Modeling the Cost and Consequences of
HIV/AIDS treatment and prevention in India (Over, Heywood, Gold,
Gupta, Hira and Marseille 2004)
Factors Affecting Adherence to ARV: Analysis of economic factors
affecting adherence (Horizons/Population Council)
Access to Antiretrovirals in India - A Feasibility Study (Institute of
Economic Growth and Population Council 2004)
Feasibility of health insurance for clients of care and support centers
(Institute of Economic Growth, UNDP, Freedom Foundation, ongoing)
Costing of the free ART programme of the government: A feasibility
study (Institute of Economic Growth – World Bank 2005)
HIV/AIDS Treatment and Prevention in India: Modeling the Cost and
Consequences
Mead Over, Peter Heywood, Sudhakar Kurapati (World Bank)
Julian Gold, Indrani Gupta, Abhaya Indrayan, Subhash Hira, Elliot Marseille, Nico Nagelkerke, and Arni S.R. Srinivasa Rao(Consultants)
Policy options
Adhere: Support to help patients adhere
I.e. IEC, training, lab strengthening, subsidies for patient
monitoring in both private & public sectors
MTCT+: Structured ART for identified HIV+ mothers
and their partners
includes Adhere above
BPL: Structured ART for people below the poverty
line
includes Adhere above
TMART: Transmission-minimizing ART
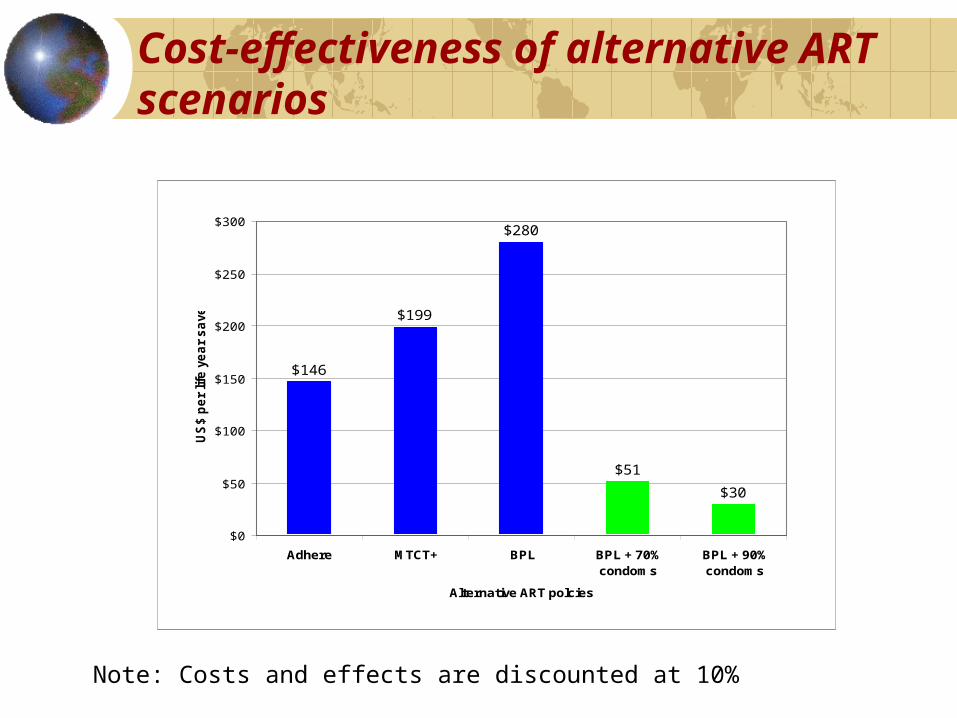
Cost-effectiveness of alternative ART scenarios
Note: Costs and effects are discounted at 10%
$146
$199
$280
$51
$30
$0
$50
$100
$150
$200
$250
$300
Adhere MTCT+ BPL BPL + 70%condoms
BPL + 90%condoms
Alternative ART polcies
US
$ p
er
life
ye
ar
sa
ved

India should proceed cautiously with the expansion of ART
In order to:
avoid the twin dangers of resistance and disinhibition and
enhance the beneficial synergy between ART and
prevention,
M & E must accompany rollout to an unprecedented
degree.
HIV/AIDS Treatment and Prevention in India: Modeling the Cost and Consequences, World Bank 2004
Free ARV programme of the Government of India
Govt. of India launched its free antiretroviral programme in April
2004 in seven high prevalence states: Andhra Pradesh, Karnataka,
Maharashtra, Tamil Nadu, Manipur, Nagaland and NCT of Delhi
through 8 government hospitals in the first phase.
In Phase I of implementation, the sub-groups among the PLHAs
being targeted on priority are :
Sero-positive mothers who have participated in the PPTCT programme;
Sero-positive children below the age of 15 years; and
People with AIDS who seek treatment in government hospitals.
Only first line regimen of drugs have been made available through
the free ART programme.
Population Council-Horizon’s study on Adherence, 2004
The study aimed to explore adherence levels among PLHA currently receiving ART, to better understand the factors that influence adherence to treatment, to explore sexual risk behavior among PLHA on ART, and to understand the financing mechanisms PLHA use to pay for their treatment.
Findings from this study provide important insights into adherence and sexual risk behaviour among PLHA on treatment that is of immediate relevance to the National ARV program as it scales up.

Some key findings from the economic analysis
The study found high economic burden of treatment on
those without any coverage, indicating the need to focus on
alternative financing mechanisms for treatment, which
should include drugs and test
However, lower adherence was observed among patients
receiving free ARVs even after controlling for economic
status
Subsidized programs like the free ART programme need to pay
careful attention to optimal pricing to maximize adherence

Future research that can inform policymaking on scaling up of ART
Costing of free ART programme of the GOI
How sustainable is the programme?
Evaluation of the on-going programme
How well is it doing?
How good is adherence?
Study on impact of the programme on the course
of the epidemic
Is behaviour changing in the right direction?

3 by 5 initiative
The latest WHO/UNAIDS report indicates that while
there has been progress on the 3 by 5 initiative of the
WHO, the coverage has not been as expected. Till June
2005, less than 1 million people have been covered, and
it seems unlikely that the target of 3 million will be met.
Initial evidence from India also indicates that there are
constraints to rapid scaling up and the initial target of
100,000 by 2005 has been now revised to 2007. To
date, less than 10,000 are being covered under the free
ART programme

Is the free ART initiative of the government sufficient?
Preliminary evidence indicates that it will be a while till all
those who are ARV-eligible will get free treatment (WHO
estimates that 700,000 individuals need ARV today)
In the meantime, economic impact of treatment will
continue to pose a burden on many households. Need to
find other ways of extending support for treatment
Health insurance or health coverage is one such option that
need to be given serious consideration.

Objectives of the study(Population Council-IEG)
To explore the feasibility of medical insurance for HIV
positive individuals in India to cover ARV drugs and
diagnostic tests.
To arrive at possible schemes of medical insurance
To point out the feasibility of each such scheme, with
issues and constraints with regard to implementation
Cover those who are HIV negative at inception
Amendments to Mediclaim Policy• National Insurance Company worked with Gujarat SACS to
formulate and pilot a health insurance policy with the following features:
– No HIV/AIDS exclusion– Coverage
– STDs– HIV/STD as OPD treatment including ARV– Tests like CD4 count
– Sum insured of Rs. 50000– Reimbursement through identified nodal agencies– Pre existing conditions including HIV not covered– Premium being worked out; likely to be around Rs.1,000
Critical illness policy with inclusion of HIV/AIDS as one of the diseases for the general population
• Amendment for healthcare workers in CI policy can be considered seriously by existing insurance companies
Cover those who are currently HIV positive in general schemes for communities
• Karuna Trust
– Successful low cost health insurance (with
NIC as partner)
– No exclusion in terms of diseases
Possible to amend the policy to cover HIV positive
individuals and cover cost of ARV

Cover those who are HIV positive through specific schemes
The global fund (GFATM) in its 2nd round has funded three
NGOs to provide ART on a cost recovery basis.
Certain care and support organisations have been exploring
ways of providing ARV to their clients through tailor-made
schemes (UNDP-IEG-Freedom Foundation).
These options involve significant funding and therefore has
implications about sustainability

Future directions
1. The dialogue with the insurance sector on an amendment to the Critical Illness Policy should be sustained.
2. The dialogue with the insurance sector on specific tailor-made policies for people living with HIV/AIDS (PLWHA) need to be continued.
3. Ways of amending community health insurance schemes to incorporate ARV treatment should be explored further.
4. The feasibility of including HIV-related conditions under Mediclaim and Universal Health Scheme needs to be further strengthened
5. The amendment to the critical illness policy, as currently being implemented needs to be closely monitored and evaluated to assess its feasibility and cost implications

A truly multi-sectoral approach is called for with the
different stakeholders involved:
Ministries of Health, Finance, Labour
Planning Commission
Insurance companies
NGOs including care and support organisations
Insurance Regulatory and Development Authority
Donors
NACO should take the initiative to organize such a meeting
This strategy will go a long way in mainstreaming the
response to impact alleviation and would also allow the
country to take another look at its existing health
insurance scenario
Future directions
Related Documents