Secondary Use of Clinical Data from Electronic Health Records William Hersh, MD Professor and Chair Department of Medical Informatics & Clinical Epidemiology School of Medicine Oregon Health & Science University Email: [email protected] Web: www.billhersh.info Blog: informaticsprofessor.blogspot.com References Anonymous (2007). Value‐driven Health Care: A Purchaser Guide, Version 2.0. Washington, DC, The Leapfrog Group. http://www.leapfroggroup.org/media/file/Employer_Purchaser_Guide_05_11_07.pdf. Anonymous (2010). For the Public’s Health: The Role of Measurement in Action and Accountability. Washington, DC, Institute of Medicine. http://www.iom.edu/Reports/2010/For‐the‐Publics‐ Health‐The‐Role‐of‐Measurement‐in‐Action‐and‐Accountability.aspx. Baker, D., Persell, S., et al. (2007). Automated review of electronic health records to assess quality of care for outpatients with heart failure. Annals of Internal Medicine, 146: 270‐277. Benin, A., Fenick, A., et al. (2011). How good are the data? Feasible approach to validation of metrics of quality derived from an outpatient electronic health record. American Journal of Medical Quality, 26: 441‐451. Benin, A., Vitkauskas, G., et al. (2005). Validity of using an electronic medical record for assessing quality of care in an outpatient setting. Medical Care, 43: 691‐698. Bernstam, E., Hersh, W., et al. (2009). Synergies and distinctions between computational disciplines in biomedical research: perspective from the Clinical and Translational Science Award programs. Academic Medicine, 84: 964‐970. Berwick, D., Nolan, T., et al. (2008). The triple aim: care, health, and cost. Health Affairs, 27: 759‐769. Blumenthal, D. (2011a). Implementation of the federal health information technology initiative. New England Journal of Medicine, 365: 2426‐2431. Blumenthal, D. (2011b). Wiring the health system‐‐origins and provisions of a new federal program. New England Journal of Medicine, 365: 2323‐2329. Botsis, T., Hartvigsen, G., et al. (2010). Secondary use of EHR: data quality issues and informatics opportunities. AMIA Summits on Translational Science Proceedings, San Francisco, CA. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3041534/. Bourgeois, F., Olson, K., et al. (2010). Patients treated at multiple acute health care facilities: quantifying information fragmentation. Archives of Internal Medicine, 170: 1989‐1995. Chan, K., Fowles, J., et al. (2010). Electronic health records and reliability and validity of quality measures: a review of the literature. Medical Care Research and Review, 67: 503‐527. Chapman, W., Christensen, L., et al. (2004). Classifying free‐text triage chief complaints into syndromic categories with natural language processing. Artificial Intelligence in Medicine, 33: 31‐40.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Secondary Use of Clinical Data from Electronic Health Records
William Hersh, MD
Professor and Chair
Department of Medical Informatics & Clinical Epidemiology
School of Medicine
Oregon Health & Science University
Email: [email protected]
Web: www.billhersh.info
Blog: informaticsprofessor.blogspot.com
References
Anonymous (2007). Value‐driven Health Care: A Purchaser Guide, Version 2.0. Washington, DC, The Leapfrog Group. http://www.leapfroggroup.org/media/file/Employer_Purchaser_Guide_05_11_07.pdf.
Anonymous (2010). For the Public’s Health: The Role of Measurement in Action and Accountability. Washington, DC, Institute of Medicine. http://www.iom.edu/Reports/2010/For‐the‐Publics‐Health‐The‐Role‐of‐Measurement‐in‐Action‐and‐Accountability.aspx.
Baker, D., Persell, S., et al. (2007). Automated review of electronic health records to assess quality of care for outpatients with heart failure. Annals of Internal Medicine, 146: 270‐277.
Benin, A., Fenick, A., et al. (2011). How good are the data? Feasible approach to validation of metrics of quality derived from an outpatient electronic health record. American Journal of Medical Quality, 26: 441‐451.
Benin, A., Vitkauskas, G., et al. (2005). Validity of using an electronic medical record for assessing quality of care in an outpatient setting. Medical Care, 43: 691‐698.
Bernstam, E., Hersh, W., et al. (2009). Synergies and distinctions between computational disciplines in biomedical research: perspective from the Clinical and Translational Science Award programs. Academic Medicine, 84: 964‐970.
Berwick, D., Nolan, T., et al. (2008). The triple aim: care, health, and cost. Health Affairs, 27: 759‐769. Blumenthal, D. (2011a). Implementation of the federal health information technology initiative. New
England Journal of Medicine, 365: 2426‐2431. Blumenthal, D. (2011b). Wiring the health system‐‐origins and provisions of a new federal program. New
England Journal of Medicine, 365: 2323‐2329. Botsis, T., Hartvigsen, G., et al. (2010). Secondary use of EHR: data quality issues and informatics
opportunities. AMIA Summits on Translational Science Proceedings, San Francisco, CA. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3041534/.
Bourgeois, F., Olson, K., et al. (2010). Patients treated at multiple acute health care facilities: quantifying information fragmentation. Archives of Internal Medicine, 170: 1989‐1995.
Chan, K., Fowles, J., et al. (2010). Electronic health records and reliability and validity of quality measures: a review of the literature. Medical Care Research and Review, 67: 503‐527.
Chapman, W., Christensen, L., et al. (2004). Classifying free‐text triage chief complaints into syndromic categories with natural language processing. Artificial Intelligence in Medicine, 33: 31‐40.

Chapman, W., Cooper, G., et al. (2003). Creating a text classifier to detect radiology reports describing mediastinal findings associated with inhalational anthrax and other disorders. Journal of the American Medical Informatics Association, 10: 494‐503.
Chapman, W., Dowling, J., et al. (2005). Classification of emergency department chief complaints into 7 syndromes: a retrospective analysis of 527,228 patients. Annals of Emergency Medicine, 46: 445‐455.
Chassin, M. and Loeb, J. (2011). The ongoing quality improvement journey: next stop, high reliability. Health Affairs, 30: 559‐568.
Christakis, N. and Fowler, J. (2010). Social network sensors for early detection of contagious outbreaks. PLoS ONE, 5(9): e12948. http://www.plosone.org/article/info%3Adoi%2F10.1371%2Fjournal.pone.0012948.
Chute, C., Pathak, J., et al. (2011). The SHARPn project on secondary use of Electronic Medical Record data: progress, plans, and possibilities. AMIA Annual Symposium Proceedings 2011, Washington, DC. 248‐256.
deLusignan, S. and vanWeel, C. (2005). The use of routinely collected computer data for research in primary care: opportunities and challenges. Family Practice, 23: 253‐263.
Denny, J., Miller, R., et al. (2009). Identifying QT prolongation from ECG impressions using a general‐purpose natural language processor. International Journal of Medical Informatics, 78(Suppl 1): S34‐42.
Denny, J., Peterson, J., et al. (2010). Extracting timing and status descriptors for colonoscopy testing from electronic medical records. Journal of the American Medical Informatics Association, 17: 383‐388.
Denny, J., Ritchie, M., et al. (2010a). PheWAS: Demonstrating the feasibility of a phenome‐wide scan to discover gene‐disease associations. Bioinformatics, 26: 1205‐1210.
Denny, J., Ritchie, M., et al. (2010b). Identification of genomic predictors of atrioventricular conduction: using electronic medical records as a tool for genome science. Circulation, 122: 2016‐2021.
Donabedian, A., ed. (2002). An Introduction to Quality Assurance in Health Care. Cambridge, MA. Oxford University Press.
Dougherty, D. and Conway, P. (2008). The "3T's" road map to transform US health care: the "how" of high‐quality care. Journal of the American Medical Association, 299(2319‐2321).
Doyle, T., Glynn, M., et al. (2002). Completeness of notifiable infectious disease reporting in the United States: an analytical literature review. American Journal of Epidemiology, 155: 866‐874.
Eden, J., Wheatley, B., et al., eds. (2008). Knowing What Works in Health Care: A Roadmap for the Nation. Washington, DC. National Academies Press.
Effler, P., Ching‐Lee, M., et al. (1999). Statewide system of electronic notifiable disease reporting from clinical laboratories: comparing automated reporting with conventional methods. Journal of the American Medical Association, 282: 1845‐1850.
Embi, P. and Payne, P. (2009). Clinical research informatics: challenges, opportunities and definition for an emerging domain. Journal of the American Medical Informatics Association, 16: 316‐327.
Finnell, J., Overhage, J., et al. (2011). All health care is not local: an evaluation of the distribution of emergency department care delivered in Indiana. AMIA Annual Symposium Proceedings, Washington, DC. in press.
Friedman, C., Wong, A., et al. (2010). Achieving a nationwide learning health system. Science Translational Medicine, 2(57): 57cm29. http://stm.sciencemag.org/content/2/57/57cm29.full.
Ginsberg, J., Mohebbi, M., et al. (2009). Detecting influenza epidemics using search engine query data. Nature, 457: 1012‐1014.

Goldenberg, A., Shmueli, G., et al. (2002). Early statistical detection of anthrax outbreaks by tracking over‐the‐counter medication sales. Proceedings of the National Academy of Sciences, 99: 5237‐5240.
Greene, S., Reid, R., et al. (2012). Implementing the learning health system: from concept to action. Annals of Internal Medicine, 157: 207‐210.
Hazlehurst, B., Sittig, D., et al. (2005). Natural language processing in the electronic medical record: assessing clinician adherence to tobacco treatment guidelines. American Journal of Preventive Medicine, 29: 434‐439.
Hogan, W., Tsui, F., et al. (2003). Detection of pediatric respiratory and diarrheal outbreaks from sales of over‐the‐counter electrolyte products. Journal of the American Medical Informatics Association, 10: 555‐562.
Hulth, A., Rydevik, G., et al. (2009). Web queries as a source for syndromic surveillance. PLoS ONE, 4(2): e4378.
Johnson, H., Wagner, M., et al. (2004). Analysis of Web access logs for surveillance of influenza. MEDINFO 2004 ‐ Proceedings of the Eleventh World Congress on Medical Informatics, San Francisco, CA. IOS Press. 1202‐1206.
Jollis, J., Ancukiewicz, M., et al. (1993). Discordance of databases designed for claims payment versus clinical information systems: implications for outcomes research. Annals of Internal Medicine, 119: 844‐850.
Kimia, A., Brownstein, J., et al. (2006). Lumbar puncture ordering and results in the pediatric population: a promising data source for surveillance systems. Academic Emergency Medicine, 13: 767‐773.
Klompas, M., McVetta, J., et al. (2012). Integrating clinical practice and public health surveillance using electronic medical record systems. American Journal of Preventive Medicine, 42(6S2): S154‐S162.
MacKenzie, S., Wyatt, M., et al. (2012). Practices and perspectives on building integrated data repositories: results from a 2010 CTSA survey. Journal of the American Medical Informatics Association: Epub ahead of print.
Maynard, A. (2012). The powers and pitfalls of payment for performance. Health Economics, 21: 3‐12. McCarty, C., Chisholm, R., et al. (2010). The eMERGE Network: a consortium of biorepositories linked to
electronic medical records data for conducting genomic studies. BMC Genomics, 4(1): 13. http://www.biomedcentral.com/1755‐8794/4/13.
Nightingale, F. (1863). Notes on Hospitals. London, England. Longman, Green, Roberts, Longman, and Green.
O'Connor, P. (2012). Quality improvement collaboratives in the age of health informatics‐‐new wine in new wineskins. BMJ Quality & Safety: Epub ahead of print.
Overhage, J., Grannis, S., et al. (2008). A comparison of the completeness and timeliness of automated electronic laboratory reporting and spontaneous reporting of notifiable conditions. American Journal of Public Health, 98: 344‐350.
Owens, D., Qaseem, A., et al. (2011). High‐value, cost‐conscious health care: concepts for clinicians to evaluate the benefits, harms, and costs of medical interventions. Annals of Internal Medicine, 154: 174‐180.
Pakhomov, S., Bjornsen, S., et al. (2008). Quality performance measurement using the text of electronic medical records. Medical Decision Making, 28: 462‐470.
Pakhomov, S., Hanson, P., et al. (2008). Automatic classification of foot examination findings using statistical natural language processing and machine learning. Journal of the American Medical Informatics Association, 15: 198‐202.
Pakhomov, S., Weston, S., et al. (2007). Electronic medical records for clinical research: application to the identification of heart failure. American Journal of Managed Care, 13: 281‐288.
Panackal, A., M'ikanatha, N., et al. (2002). Automatic electronic laboratory‐based reporting of notifiable infectious diseases at a large health system. Emerging Infectious Diseases, 8: 685‐691.
Parsons, A., McCullough, C., et al. (2012). Validity of electronic health record‐derived quality measurement for performance monitoring. Journal of the American Medical Informatics Association, 19: 604‐609.
Pawlson, L., Scholle, S., et al. (2007). Comparison of administrative‐only versus administrative plus chart review data for reporting HEDIS hybrid measures. American Journal of Managed Care, 13: 553‐558.
Payne, P., Embi, P., et al. (2009). Translational informatics: enabling high‐throughput research paradigms. Physiological Genomics, 39: 131‐140.
Proctor, M., Blair, K., et al. (1998). Surveillance data for waterborne illness detection: an assessment following a massive waterborne outbreak of Cryptosporidium infection. Epidemiology and Infection, 120: 43‐54.
Rea, S., Pathak, J., et al. (2012). Building a robust, scalable and standards‐driven infrastructure for secondary use of EHR data: The SHARPn project. Journal of Biomedical Informatics: Epub ahead of print.
Rhodes, E., Laffel, L., et al. (2007). Accuracy of administrative coding for type 2 diabetes in children, adolescents, and young adults. Diabetes Care, 30: 141‐143.
Richesson, R. and Andrews, J., eds. (2012). Clinical Research Informatics. New York, NY. Springer. Ritchie, M., Denny, J., et al. (2010). Robust replication of genotype‐phenotype associations across
multiple diseases in an electronic medical record. American Journal of Human Genetics, 86: 560‐572.
Rosenbloom, S., Denny, J., et al. (2011). Data from clinical notes: a perspective on the tension between structure and flexible documentation. Journal of the American Medical Informatics Association, 18: 181‐186.
Roski, J. and McClellan, M. (2011). Measuring health care performance now, not tomorrow: essential steps to support effective health reform. Health Affairs, 30: 682‐689.
Safran, C., Bloomrosen, M., et al. (2007). Toward a national framework for the secondary use of health data: an American Medical Informatics Association white paper. Journal of the American Medical Informatics Association, 14: 1‐9.
Shojania, K., Silver, I., et al. (2012). Continuing medical education and quality improvement: a match made in heaven? Annals of Internal Medicine, 156: 305‐308.
Silk, B. and Berkelman, R. (2005). A review of strategies for enhancing the completeness of notifiable disease reporting. Journal of Public Health Management and Practice, 11: 191‐200.
Tang, P., Ralston, M., et al. (2007). Comparison of methodologies for calculating quality measures based on administrative data versus clinical data from an electronic health record system: implications for performance measures. Journal of the American Medical Informatics Association, 14: 10‐15.
Tannen, R., Weiner, M., et al. (2008). Replicated studies of two randomized trials of angiotensin‐converting enzyme inhibitors: further empiric validation of the 'prior event rate ratio' to adjust for unmeasured confounding by indication. Pharmacoepidemiology and Drug Safety, 17: 671‐685.
Tannen, R., Weiner, M., et al. (2007). A simulation using data from a primary care practice database closely replicated the women's health initiative trial. Journal of Clinical Epidemiology, 60: 686‐695.
Weinberger, S. (2011). Providing high‐value, cost‐conscious care: a critical seventh general competency for physicians. Annals of Internal Medicine, 155: 386‐388.
Weiner, J., Fowles, J., et al. (2012). New paradigms for measuring clinical performance using electronic health records. International Journal for Quality in Health Care: Epub ahead of print.
Weiner, M. (2011). Evidence Generation Using Data‐Centric, Prospective, Outcomes Research Methodologies. San Francisco, CA, Presentation at AMIA Clinical Research Informatics Summit.
Wilke, R., Xu, H., et al. (2011). The emerging role of electronic medical records in pharmacogenomics. Clinical Pharmacology and Therapeutics, 89: 379‐386.
Zerhouni, E. (2007). Translational research: moving discovery to practice. Clinical Pharmacology and Therapeutics, 81: 126‐128.
1
Secondary Use of Clinical Data from Electronic Health Records
William Hersh, MDProfessor and Chair
Department of Medical Informatics & Clinical EpidemiologySchool of Medicine
Oregon Health & Science UniversityEmail: [email protected]: www.billhersh.info
Blog: informaticsprofessor.blogspot.com
1
Who said this and when?
• “I am fain to sum up with an urgent appeal for adopting … some uniform system of publishing the statistical records of hospitals. There is a growing conviction that in all hospitals, even in those which are best conducted, there is a great and unnecessary waste of life … In attempting to arrive at the truth, I have applied everywhere for information, but in scarcely an instance have I been able to obtain hospital records fit for any purposes of comparison … If wisely used, these improved statistics would tell us more of the relative value of particular operations and modes of treatment than we have means of ascertaining at present.”
2
2
Who and when...
• Florence Nightingale, Notes on Hospitals, London: Longman, Green, Roberts, Longman, and Green, 1863
• The first advocate for secondary use of clinical data?
• She does have a Web site (and museum in London)
– www.florence‐nightingale.co.uk
3
Overview
• Motivations for secondary use of clinical data
• Challenges for secondary use of clinical data
• Types of secondary use of clinical data
– Clinical and translational research
– Public health
– Quality measurement and improvement
4
3
Motivations for secondary use of clinical data
• Many “secondary uses” or re‐uses of electronic health record (EHR) data, including (Safran, 2007)– Clinical and translational research – generating hypotheses and facilitating research
– Public health surveillance for emerging threats– Healthcare quality measurement and improvement
• Opportunities facilitated by growing incentives for “meaningful use” of EHRs in the HITECH Act (Blumenthal, 2011; Blumenthal, 2011), aiming toward the “learning healthcare system” (Eden, 2008; Friedman, 2010)
5
Challenges for secondary use of clinical data
• EHR data does not automatically lead to knowledge– Data quality and accuracy is not a top priority for busy clinicians (de
Lusignan, 2005)– There is “tension” between structured and narrative documentation
(Rosenbloom, 2011)
• Many data idiosyncrasies (Weiner, 2011)– “Left censoring”: First instance of disease in record may not be when
first manifested– “Right censoring”: Data source may not cover long enough time
interval– Data might not be captured from other clinical (other hospitals or
health systems) or non‐clinical (OTC drugs) settings– Bias in testing or treatment– Institutional or personal variation in practice or documentation styles– Inconsistent use of coding or standards
6
4
Data in EHRs is incomplete
• Claims data failed to identify more than half of patients with prognostically important cardiac conditions prior to admission for catheterization (Jollis, 1993)
• Various approaches generated variable rate of retrieval of cases for quality measurement (Benin, 2005; Rhodes, 2007; Parsons, 2012); algorithmic methods can lead to improvement (Benin, 2011)
• At Columbia University Medical Center, 48.9% of patients with ICD‐9 code for pancreatic cancers did not have corresponding disease documentation in pathology reports, with many data elements incompletely documented (Botsis, 2010)
7
Patients get care in multiple places
• Study of 3.7M patients in Massachusetts found 31% visited 2 or more hospitals over 5 years (57% of all visits) and 1% visited 5 or more hospitals (10% of all visits) (Bourgeois, 2010)
• Study of 2.8M emergency department (ED) patients in Indiana found 40% of patients had data at multiple institutions, with all 81 EDs sharing patients in common (Finnell, 2011)
8

5
Despite these caveats, can we use secondary data from EHRs?
• Clinical and translational research
• Public health
• Quality measurement and improvement
9
Clinical research
• Clinical research comprises studies and trials in human subjects that fall into the three sub‐categories– Patient‐oriented research – research conducted with human subjects (or on material of human origin such as tissues, specimens and cognitive phenomena) for which an investigator (or colleague) directly interacts with human subjects
– Epidemiologic and behavioral studies
– Outcomes research and health services research
10
6
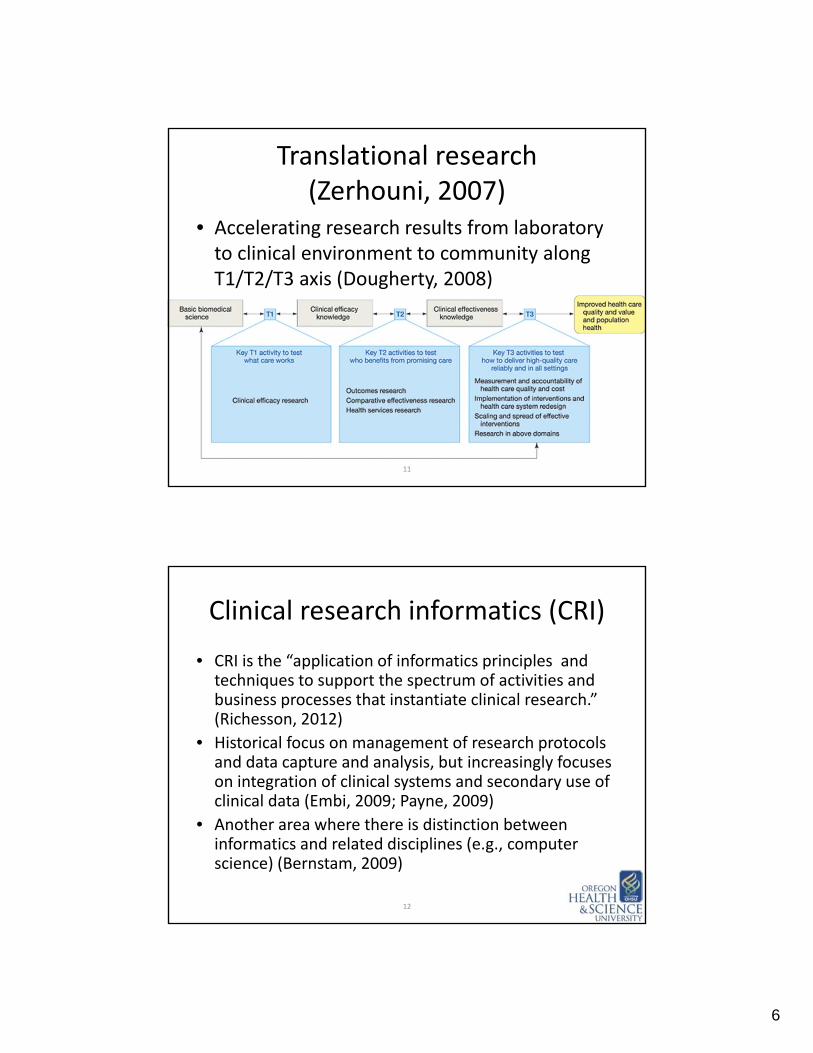
Translational research(Zerhouni, 2007)
• Accelerating research results from laboratory to clinical environment to community along T1/T2/T3 axis (Dougherty, 2008)
11
Clinical research informatics (CRI)
• CRI is the “application of informatics principles and techniques to support the spectrum of activities and business processes that instantiate clinical research.” (Richesson, 2012)
• Historical focus on management of research protocols and data capture and analysis, but increasingly focuses on integration of clinical systems and secondary use of clinical data (Embi, 2009; Payne, 2009)
• Another area where there is distinction between informatics and related disciplines (e.g., computer science) (Bernstam, 2009)
12
7
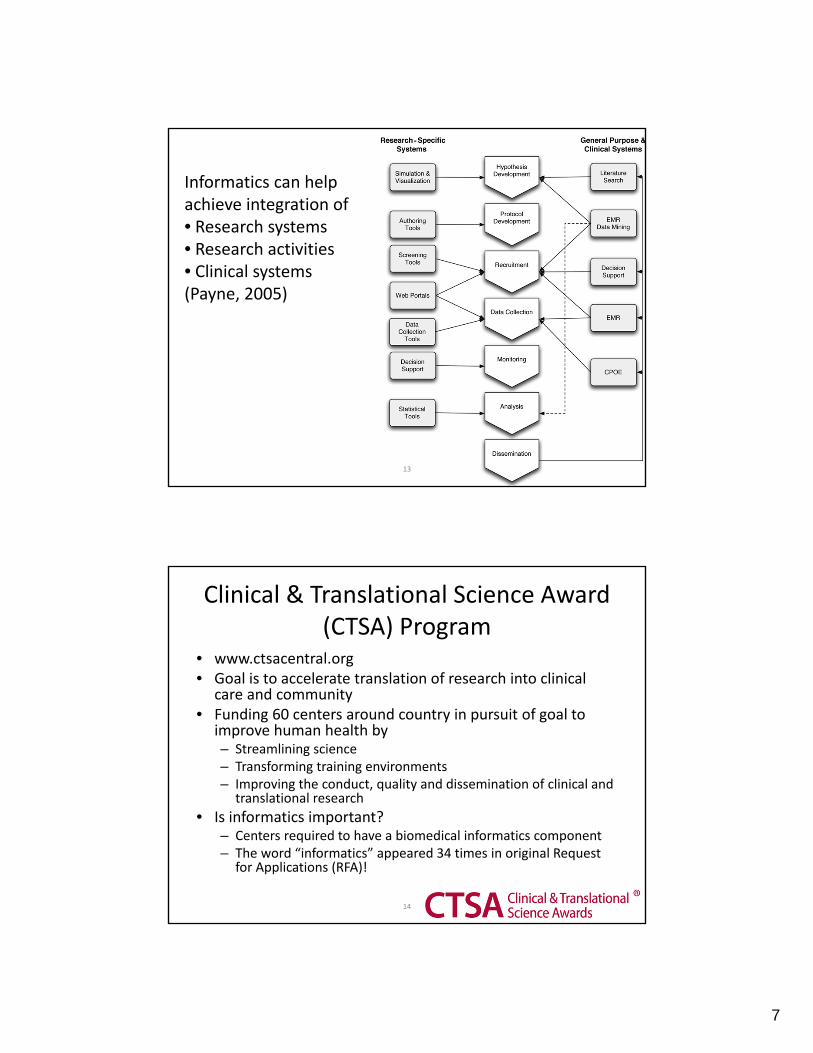
Informatics can helpachieve integration of• Research systems• Research activities• Clinical systems(Payne, 2005)
13
Clinical & Translational Science Award (CTSA) Program
• www.ctsacentral.org• Goal is to accelerate translation of research into clinical
care and community• Funding 60 centers around country in pursuit of goal to
improve human health by– Streamlining science– Transforming training environments– Improving the conduct, quality and dissemination of clinical and
translational research
• Is informatics important?– Centers required to have a biomedical informatics component– The word “informatics” appeared 34 times in original Request
for Applications (RFA)!
14

8
Common themes emerging among CTSA informatics programs
• Web portal to integrate research activities, people, etc.
• Informatics services and consultation for investigators
• Data warehousing for clinical, laboratory, and/or specimen data– Long‐term but difficult goal: data sharing
– Also difficult but being undertaken by many: clinical data warehouses from EHRs and other systems
• Facilitating collaboration and translation
• Educational programs for translational researchers– Some programs also focused on education for informaticians
15
Contents of research data warehouses in CTSA programs (MacKenzie, 2012)
16

9
Examples of research results from clinical data
• Identifying patients with heart failure for clinical research (Pakhomov, 2007)– Used natural language processing and predictive modeling to identify patients with heart failure for research studies
• Relationship of childhood obesity to hyperglycemia in pregnancy (Hillier, 2007)– Using data for nearly 10,000 patients, found association between hyperglycemia in pregnancy and subsequent childhood obesity
• “Replication” of clinical trials results by using techniques and measures, e.g., Women’s Health Initiative (Tannen, 2007) and hypertension studies (Tannen, 2008)
17
Including use of genomic data
• Electronic Medical Records and Genomics (eMERGE) Network – consortium that aims to link data in biorepositories with EHR systems (including clinical text processed by NLP) for “large‐scale, high‐throughput genetic research” (McCarty, 2011; Wilke, 2011)
• Results include– Replicating finding of known gene‐disease associations from research data in EHR data for several diseases (Denny, 2010; Ritchie, 2010)
– Discovering new gene‐disease associations (Denny, 2010)– Detection of clinical events, e.g., detection of electrocardiogram QT interval prolongation (Denny, 2009) and associated genomic predictors (Denny, 2010)
10.4b18
10
Public health
• Public health performs its missions through its core functions– Assessment– Policy Development – Assurance
• Public health activities include– Prevent epidemics and the spread of disease – Protect against environmental hazards – Prevent injuries – Promote and encourage healthy behaviors – Respond to disasters and assists communities in recovery – Assure the quality and accessibility of health services
• IOM (2010)• www.whatispublichealth.org
19
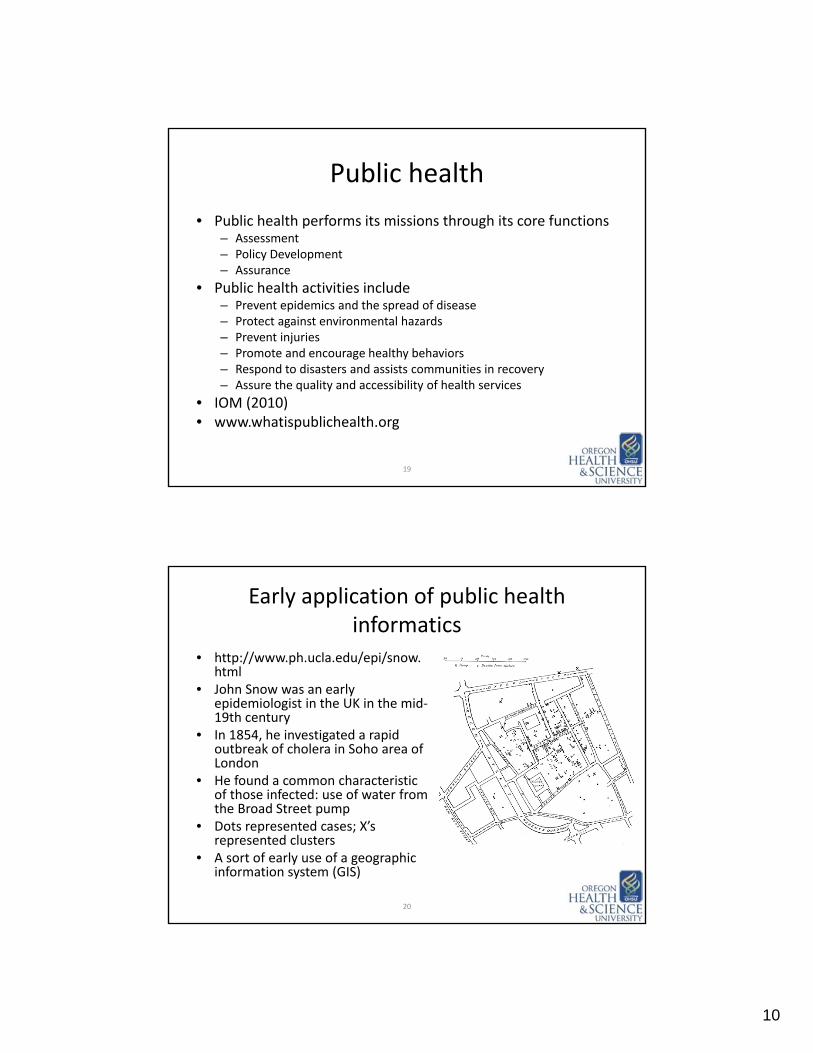
Early application of public health informatics
• http://www.ph.ucla.edu/epi/snow. html
• John Snow was an early epidemiologist in the UK in the mid‐19th century
• In 1854, he investigated a rapid outbreak of cholera in Soho area of London
• He found a common characteristic of those infected: use of water from the Broad Street pump
• Dots represented cases; X’s represented clusters
• A sort of early use of a geographic information system (GIS)
20

11
PatientSeeks Care
Clinical Encounter
Clinician Observes Disease
Local Health Department Reports to State Health Department and/or
State Health Department Reports to Local Health Department and to CDC
State or Local Public Health Reports De-identified cases to CDCPublished weekly in MMWR
Clinician Reports to Local or State Health
Department(1 to 3 days)
Clinician Orders Lab
Tests
Patient Presents to ED, urgent care, or
Hospital
or
Lab Reports Results to State or Local Public Health
(1 to 3 days)
Lab Tests Ordered
Hospital Reports to Local or State Health
Department(1 to 3 days)
or
or
and
or
Patient becomes ill.
May purchase non-
prescription meds.
Moderns public health reporting (courtesy, L. Snow, Utah DOH)
21
Despite laws, there is inadequate completeness of reporting
• Systematic review of 33 published reports between 1970‐1999 found variation from 9% to 99%, with completeness for AIDS, sexually transmitted infections, and TB higher (79%) than for all other diseases combined (49%) (Doyle, 2002)
• Reasons for clinicians not reporting– Unaware of legal requirement
– Lack of knowledge of which diseases reportable
– Do not understand how to report
– Assumption that someone else will report
– Intentional failure for privacy reasons
22

12
Efforts to improve reporting
• Emerging strategies for increasing reporting (Silk, 2005)– Active surveillance when appropriate– Automated, electronic laboratory‐based reporting– Strengthening ties with clinicians and other key partners– Increasing use of laboratory diagnostic tests in identifying new cases
• Automated electronic laboratory reporting– Shown to increase rate of reporting in a variety of settings (e.g., Effler, 1999; Panackal, 2002)
– Adding data from an electronic health information exchange identified 4.4 times as many cases as spontaneous paper‐based methods and identified those cases 7.9 days earlier (Overhage, 2008)
23
Amount of data to aid surveillance is increasing
• EHR data – e.g.,– Radiology reports (Chapman, 2003)– Chief complaints (Chapman, 2004)– Emergency Department chief complaint text (Chapman, 2005)
– Laboratory ordering and results, e.g., lumbar puncture (Kimia, 2006)
– All of the above (Klompas, 2012)
• Purchase of over‐the‐counter medications (e.g., cough suppressants, antidiarrheal medications, etc.) can foretell epidemics (Proctor, 1998; Goldenberg, 2002; Hogan, 2003)
24

13
Even more surveillance data in modern times
• Search engines– First major use: 2002 Winter Olympics in Salt Lake City, UT (Johnson, 2004)
– Google Flu Trends: http://www.google.org/flutrends/– Some flu‐related queries track closely with flu‐related visits to physicians, lagging by about a day (Ginsberg, 2009)
– Also shown with a search log submitted to a Swedish Web site (Hulth, 2009)
• Social networks, e.g., Facebook (Christakis, 2010)• Practical value?
25
Healthcare quality
• The Berwick “triple aim” (Berwick, 2008)– Improving experience of care– Improving health of population– Reducing costs
• Healthcare must strive to be “high‐value, cost‐conscious” (Owens, 2011), and “high reliability” (Chassin, 2011)– An essential physician competency (Weinberger, 2011) and
should be part of continuing medical education (Shojania, 2012)
• Investments in health IT can enable the “learning health system” (Friedman, 2010), allowing us to take advantage of data sources that already exist, such as administrative sources, registries, laboratories, and electronic health records (EHRs) (Roski, 2011)
26

14
Donabedian (2002) model of quality
• Three categories– Structural – factors that make it easier or harder to deliver high‐quality care, e.g., hospital location, volume, physician licensure, nurse staffing levels
– Process – factors describing healthcare content and activities, e.g., adherence to guidelines for screening, treatment, etc.
– Outcomes – changes attributable to care, e.g., mortality, morbidity, functional status
• Implemented and measured at different levels at an institution, e.g., individual, department, organization
27
Other definitions and issues
• Pay for performance (P4P) (Maynard, 2012)– Based on notion that healthcare should be held accountable financially and otherwise
– Sometimes called value‐based purchasing (Leapfrog, 2007)
• Public reporting (Mehrotra, 2012)– Publishing of information about quality, cost, and other aspects of healthcare performance
• Quality improvement collaboratives (O’Connor, 2012)– Putting the learning health system into action (Greene, 2012)
28
15
EHRs can augment data used in quality measures
• Coded information in EHR– Improves ability to assess diabetes quality measures (Tang, 2007)
– Administrative (or “claims”) data insufficient to calculate HEDIS measures – EHR data can improve accuracy of calculating HEDIS measures (Pawlson, 2007)
• Overall, EHR data quality is mixed for quality measurement; important attributes to improve include are granularity, timeliness, and comparability (Chan, 2010)
• EHR data for measuring quality requires transitions in collection and transformation of data (Weiner, 2012)
29
EHRs and quality measures
• Some measures in narrative text are harder to access– In heart failure, important data inaccessible in clinical notes, especially exclusion data for medications (Baker, 2007)
– Some data can be extracted by natural language processing (NLP) as effectively as manual abstractors in areas such smoking cessation advice (Hazlehurst, 2005), diabetic foot exam (Pakhomov, 2008), and congestive heart failure (CHF) (Pakhomov, 2008)
• Also impacted by workflow and documentation practices, which can result in underreporting of some preventive measures (Parsons, 2012)
30

16
Most prominent quality measures come from HITECH
• Eligible Professional (outpatient) – three required or alternate measures plus three of 13 others, e.g.,– Hypertension – blood pressure measurement– Tobacco use assessment and cessation intervention– Adult weight screening and follow‐up
• Eligible Hospital (inpatient) – 15 required measures, e.g.,– Diabetes: Hemoglobin A1c, low‐density lipoprotein, and blood
pressure control– Influenza immunization for patients > 50 years old– Pneumonia vaccination status for older adults– Breast cancer screening– Colorectal cancer screening
31
Secondary use of EHR data
• Offers potential to improve– Clinical and translational research– Public health– Quality measurement and improvement
• HITECH SHARP initiative investing in further work (Chute, 2011; Rea, 2012)
• Also many challenges– Quality and completeness of data – how to improve what clinicians enter?
– Privacy – how to protect?– Cost – who pays?
32
Related Documents











