Educators’ Conference Implementing the New Emergency Competencies into your Athletic Training Curriculum Ron Courson, ATC, PT, NREMT-I, CSCS Assistant Athletic Director – Sports Medicine University of Georgia

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

SEATA 4th Biennial Athletic Training Educators’ Conference
Implementing the New Emergency Competencies into your
Athletic Training Curriculum
Ron Courson, ATC, PT, NREMT-I, CSCSAssistant Athletic Director – Sports Medicine
University of Georgia
Objective
• Provide educational strategies to facilitate implementing NATA 5th edition athletic training education competencies related to acute care of injuries and illnesses
ATHLETIC TRAININGEDUCATION COMPETENCIES
5th Edition Released 2011
Professional Education Council: Lou Fincher, EdD, ATC- ChairDavid W. Carr, PhD, ATCRon Courson, ATC, PT, NREMT-I, CSCSJolene Henning, EdD, ATCMarsha Grant-Ford, PhD, ATCLuzita Vela, PhD, ATCAlice Wilcoxson, PhD, ATC, PT

ATHLETIC TRAININGEDUCATION COMPETENCIES
5th Edition Released 2011
• Content Areas– Evidence Based Practice– Prevention and Health Promotion– Clinical Examination and Diagnosis– Acute Care of Injury and Illness– Therapeutic Interventions– Psychosocial Strategies and Referral– Healthcare Administration– Professional Development and Responsibility
Preface• PEC orchestrated an initial open call for feedback on the 4th
edition of competencies• Groups of subject-matter experts were identified
– Acute Care of Injuries & Illnesses: • Ron Courson, ATC, PT, NREMT-I, CSCS: Team Leader• Dean Crowell, MA, ATC, NREMT-B• Gianluca Del Rossi, PhD, ATC• Michael Dillon, ATC• Jim Ellis, MD• Francis Feld, MEd, MS, ATC, CRNA• Kevin Guskiewicz, PhD, ATC• Glenn Henry, MS, NREMT-P• MaryBeth Horodyski, EdD, ATC• Jim Kyle, MD• Robb Rehberg, PhD, ATC, NREMT• Erik Swartz, PhD, ATC

Preface
• Acute Care (AC) content area substantially revised to reflect contemporary practice– addition of skill in assessing rectal temperature,
oxygen saturation, blood glucose levels, and use of a nebulizer and oropharyngeal and nasopharyngeal airways
– reflects recommendations of NATA position statements that are published or in development
– content areas now integrate knowledge and skills, instead of separate sections for cognitive and psychomotor competencies
Preface– action verb used in each
competency statement identifies the expected outcome; in some places, knowledge is the expectation and not skill acquisition
• acute care competency #9 (AC-9) requires that athletic training students be knowledgeable about the various types of airway adjuncts including OPA, NPA and supraglottic airways
• accompanying skill competency AC-10 does not require skill acquisition in the use of the supraglottic airways.

Acute Care of Injuries and Illnesses
• Athletic trainers are often present when injuries or other acute conditions occur or are the first healthcare professionals to evaluate a patient.
• For this reason, athletic trainers must be knowledgeable and skilled in the evaluation and immediate management of acute injuries and illnesses.

Acute Care of Injuries and Illnesses

Acute Care of Injuries and Illnesses

University of Georgia Sports Medicine
Background• Variety of healthcare
professionals may be involved in on-field management of suspected head and/or spine injury
• Important to develop standard guidelines to be used by all providers of pre-hospital care to ensure safe management

University of Georgia Sports Medicine
TEAMWORK• When dealing with a
potential life-threatening situation such as a head or c-spine injury, the scene of the injury is not the time nor the place for healthcare professionals to decide on appropriate treatment on such a controversial area

University of Georgia Sports Medicine
Emergency Preparation• Healthcare providers for
athletic competition (MDs, EMTs, ATCs) should develop emergency plan and protocol for dealing with such injuries when they occur and rehearse on regular basis

Change is a Constant in MedicineParadigm Shift
“No such thing as always and never”.
– James R. Andrews, MD
“A little controversy can be a good thing”.
– William Clancy, MD– oxygen– airway– c-spine management
• neutral alignment concept
– rectal temperature

Acute Care of Injuries and Illnesses• AC-9
– Differentiate the types of airway adjuncts (oropharygneal airways [OPA], nasopharyngeal airways [NPA] and supraglottic airways [King LT-D or Combitube]) and their use in maintaining a patent airway in adult respiratory and/or cardiac arrest.
• AC-10– Establish and maintain an airway, including the use of oro- and
nasopharygneal airways, and neutral spine alignment in an athlete with a suspected spine injury who may be wearing shoulder pads, a helmet with and without a face guard, or other protective equipment.
• AC-11– Determine when suction for airway maintenance is indicated
and use according to accepted practice protocols.

Acute Care of Injuries and Illnesses• AC-15
– Utilize a bag valve and pocket mask on a child and adult using supplemental oxygen.
• AC-16– Explain the indications, application, and treatment parameters for
supplemental oxygen administration for emergency situations.• AC-17
– Administer supplemental oxygen with adjuncts (eg, non-rebreather mask, nasal cannula).
• AC-18– Assess oxygen saturation using a pulse oximeter and interpret the
results to guide decision making.• AC-29
– Assess core body temperature using a rectal probe.
Acute Care of Injuries and Illnesses• AC-31
– Assist the patient in the use of a nebulizer treatment for an asthmatic attack.
• AC-32– Determine when use of a metered-dose inhaler is warranted
based on a patient’s condition.• AC-33
– Instruct a patient in the use of a meter-dosed inhaler in the presence of asthma-related bronchospasm.
• AC-35– Demonstrate the use of an auto-injectable epinephrine in the
management of allergic anaphylaxis. Decide when auto-injectable epinephrine use is warranted based on a patient’s condition.

Acute Care of Injuries and Illnesses
• AC-36– Identify the signs,
symptoms, interventions and, when appropriate, the return-to-participation criteria for:
• sudden cardiac arrest• exertional sickling
associated with sickle cell trait
• rhabdomyolysis

Acute Care of Injuries and Illnesses• University of Georgia
– KINS 4130: Athletic Training Emergency Care (ATEC) course
• spring semester• 4 hour course
– 3 hr. lecture, 1 hr. lab– Incorporate acute care
competencies and NATA emergency care related position statements
• guest instructors– physicians, paramedics
• bridge course for EMT– following completion of ATEC,
students have option of completing 1.5 month course and taking EMT national registry exam

Lecture/Laboratory Format
• Skill sheets– National Registry of
Emergency Medical Technicians
– www.nremt.org• Resources• Psychomotor exam
information

Pulse Oximetry

Core Temperature Assessment

Core Temperature Assessment
• DataTherm– monitor– 39 inch flexible probe– quick start card– instructional manual– sterile probe covers– Velcro® attachments– surgical paper tape – spare lithium battery

Core Temperature Assessment
• Rectal temperature is standard of care with exertional heat stroke
• Assess core body temperature with a rectal thermistor (thermistor implies flexible thermometer that stays in during cooling and allows for continuous monitoring of temperature during immersion therapy
Core Temperature Assessment
• NASCO enema simulator mannequin utilized at UGA for oral-practical simulations
Simulaids
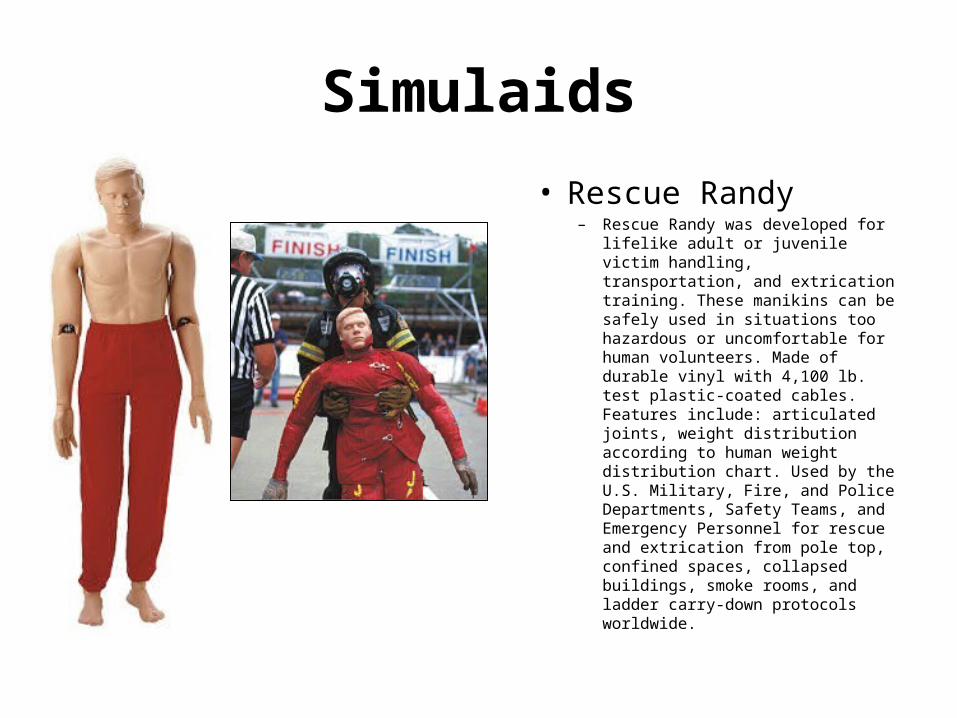
• Rescue Randy– Rescue Randy was developed for
lifelike adult or juvenile victim handling, transportation, and extrication training. These manikins can be safely used in situations too hazardous or uncomfortable for human volunteers. Made of durable vinyl with 4,100 lb. test plastic-coated cables. Features include: articulated joints, weight distribution according to human weight distribution chart. Used by the U.S. Military, Fire, and Police Departments, Safety Teams, and Emergency Personnel for rescue and extrication from pole top, confined spaces, collapsed buildings, smoke rooms, and ladder carry-down protocols worldwide.

Simulaids

Airway Management
• Manual manuevers• Basic airway• Aiway management
with BVM ventilation and suction
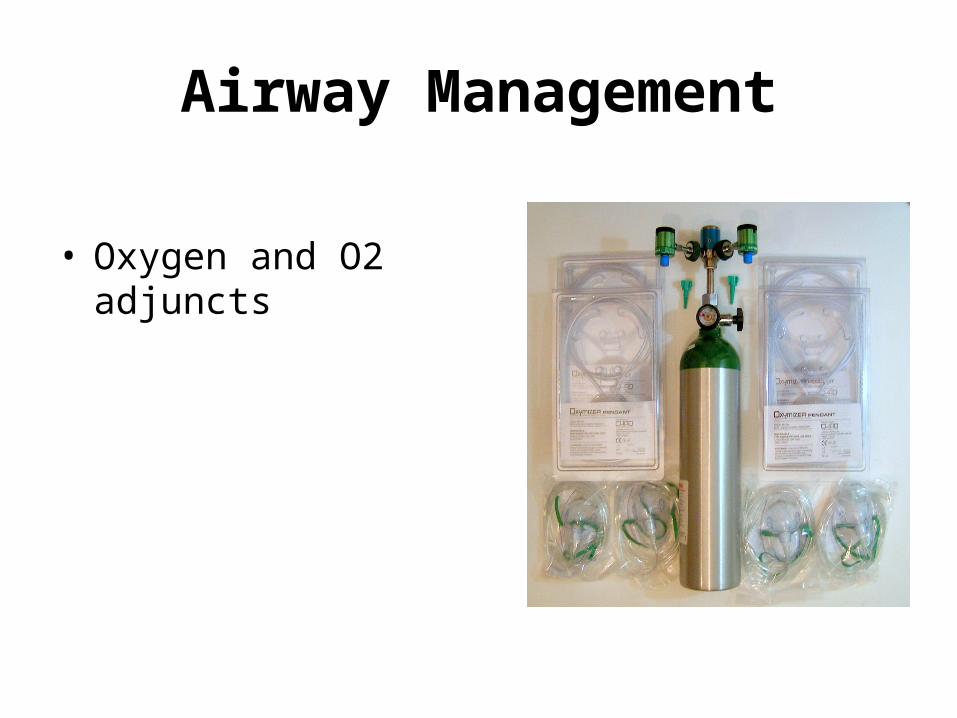
• Oxygen and O2 adjuncts• Advanced airway
Airway Management
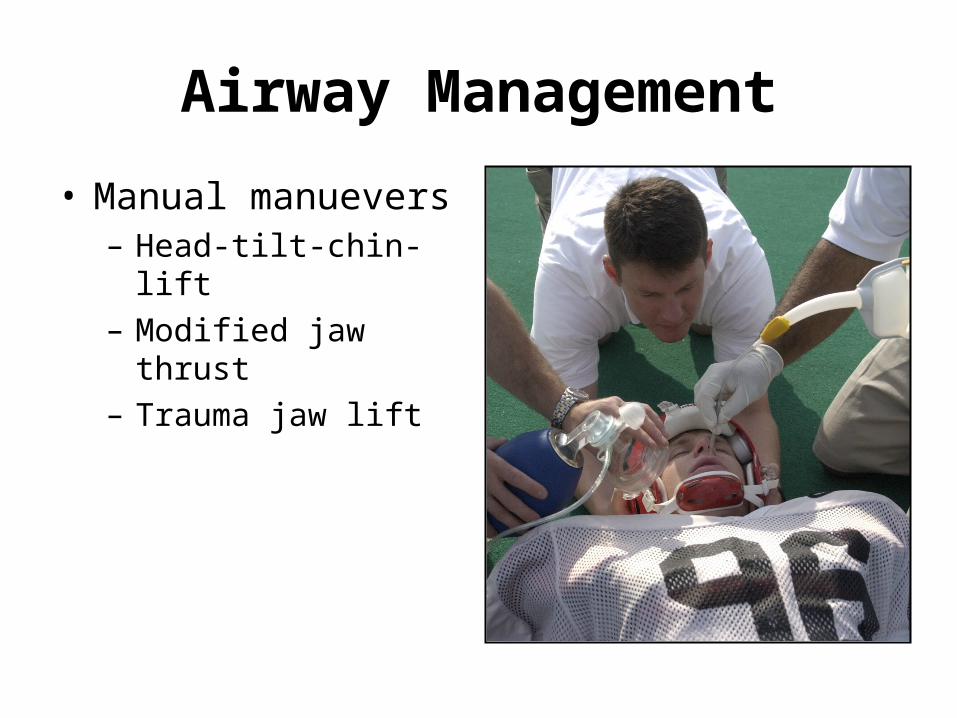
• Manual manuevers– Head-tilt-chin-lift– Modified jaw thrust– Trauma jaw lift
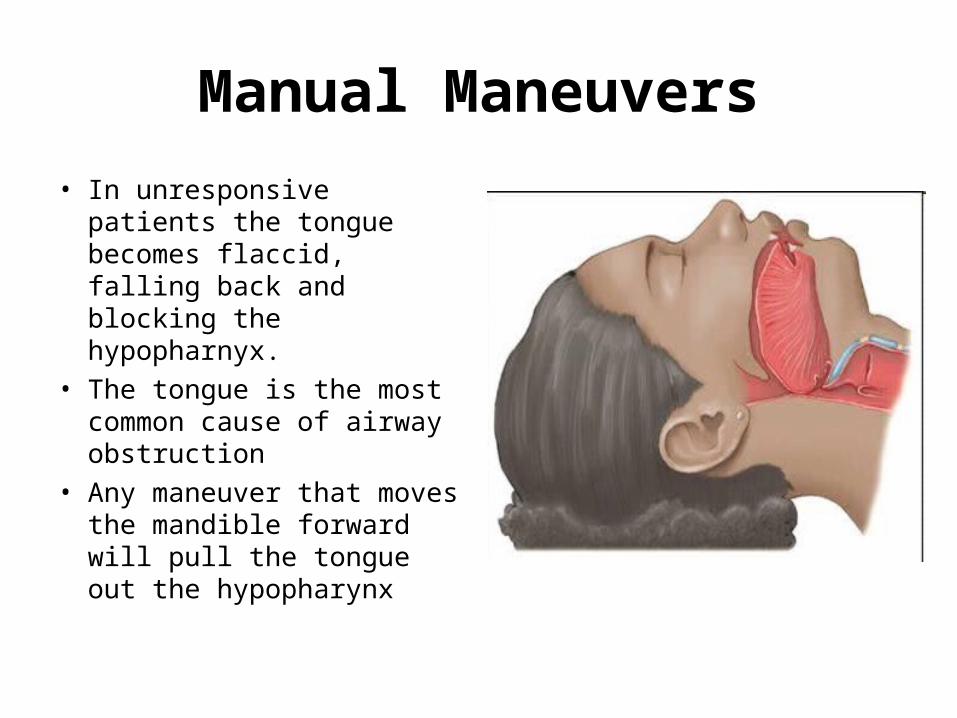
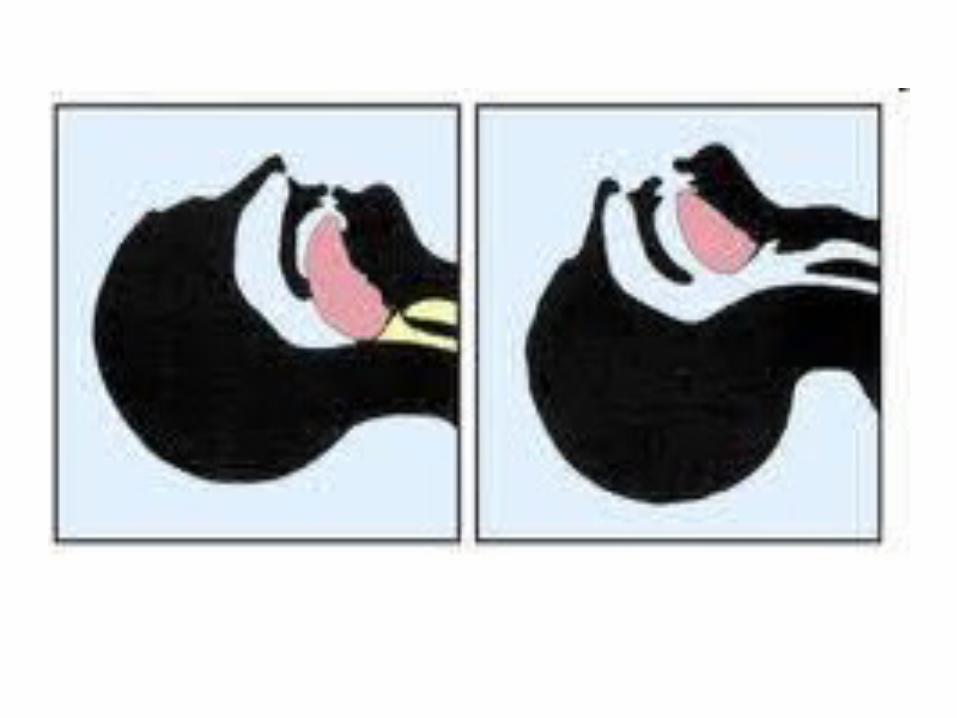
Manual Maneuvers
• In unresponsive patients the tongue becomes flaccid, falling back and blocking the hypopharnyx.
• The tongue is the most common cause of airway obstruction
• Any maneuver that moves the mandible forward will pull the tongue out the hypopharynx
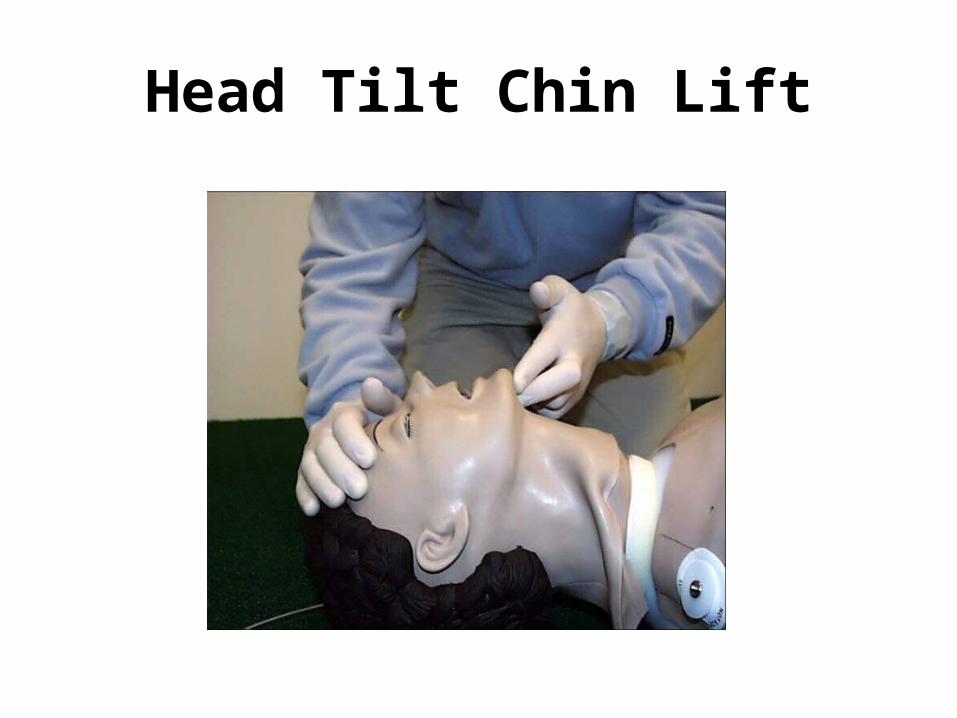
Head Tilt Chin Lift

Manual Maneuvers
• Trauma Jaw Thrust
• Trauma Chin Lift

Airway Management
•Basic mechanical airways– Oral pharyngeal airway
(OPA)
– Nasal pharyngeal airway (NPA)

Oropharyngeal Airway
Oropharyngeal Airway
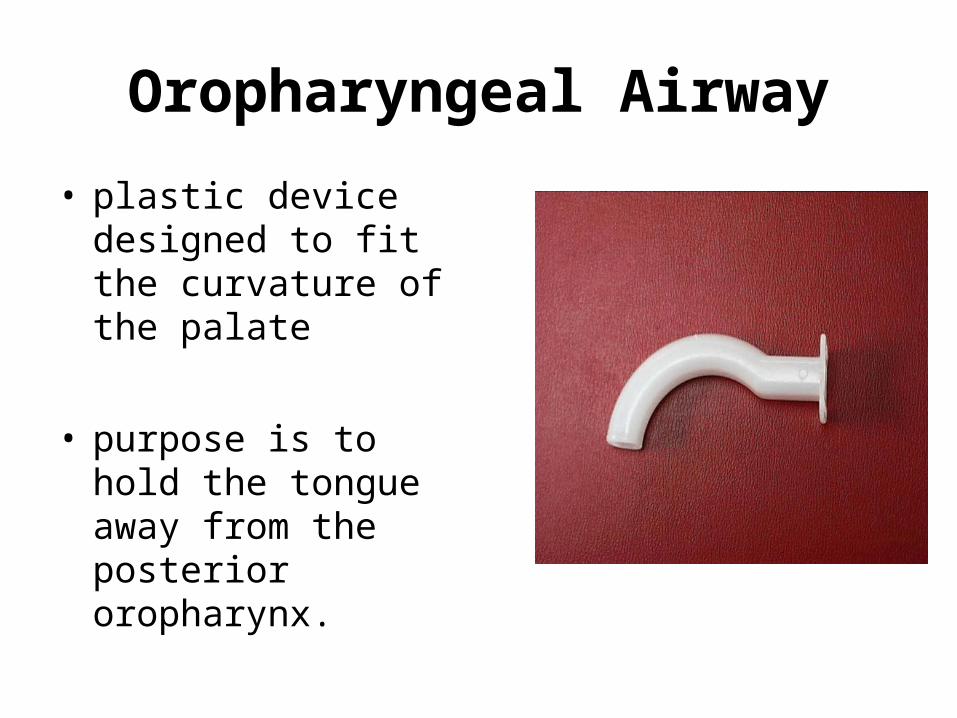
• plastic device designed to fit the curvature of the palate
• purpose is to hold the tongue away from the posterior oropharynx.

OPA Advantages
• allows air to pass around and through the device
• helps prevent obstruction by the teeth and lips
• helps manage unconscious patients who are breathing
• makes suctioning easier• serves as a bite block in case
of seizure
OPA Disadvantages
• does not isolate the trachea• cannot be inserted when the
teeth are clinched• may obstruct the airway if not
properly inserted• can be dislodged easily

OPA Measurement and Insertion


Nasopharyngeal Airway
• The NPA is a soft, rubberlike device that is inserted through one of the nares and then along the curvature of the posterior wall of the nasopharynx and oropharynx

Nasopharyngeal Airway
NPA Advantages• may be rapidly inserted• bypasses the tongue• may be used in presence of the
gag reflex• may be used when patient has
suffered damage to the oral cavity• may be used when patients teeth
are clenched
NPA Disadvantages• is smaller than the oropharyngeal
airway• does not isolate the trachea• difficult to suction through• may cause severe nosebleeds if
inserted too hard• may kink and clog• difficult to insert if any previous nasal
damage• cannot be used if there is a basilar
skull fracture

NPA Measurement and Insertion
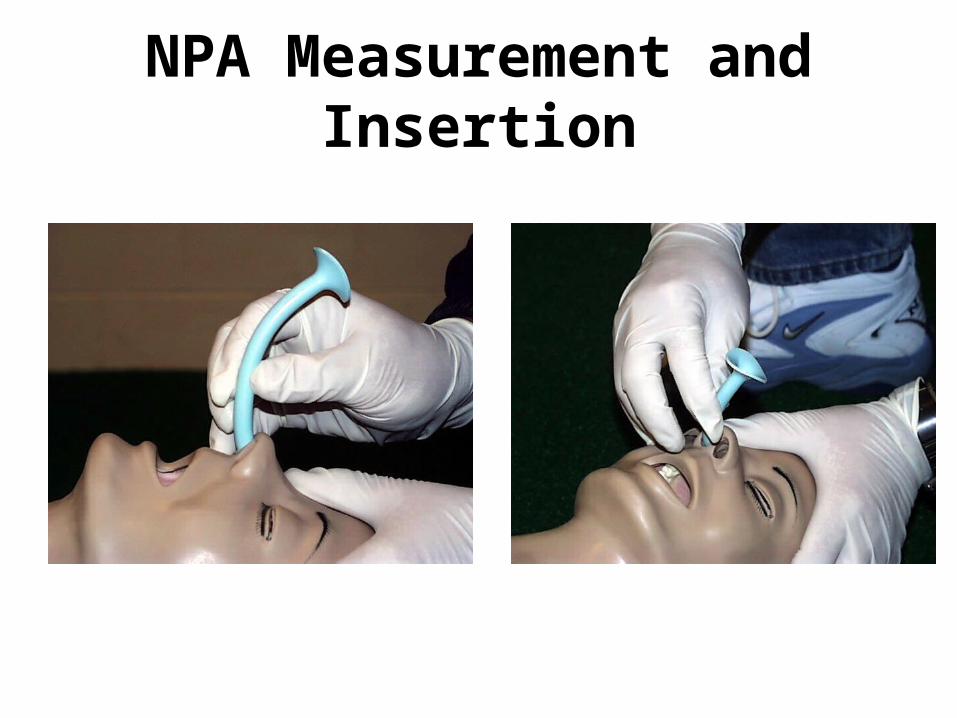
NPA Measurement and Insertion

Airway Management
• Pocket mask• Bag-valve-mask
– C-clamp technique– Res-Q-Pod
• Suction

Suction
• V-Vac manual suction• hand powered• disposable• ease of use• always suction on the
way out
Airway Management
• Oxygen and O2 adjuncts

Oxygen Delivery

Oxygen Adjuncts
• Non rebreather mask

Oxygen Adjuncts
• Bag-Valve-Mask
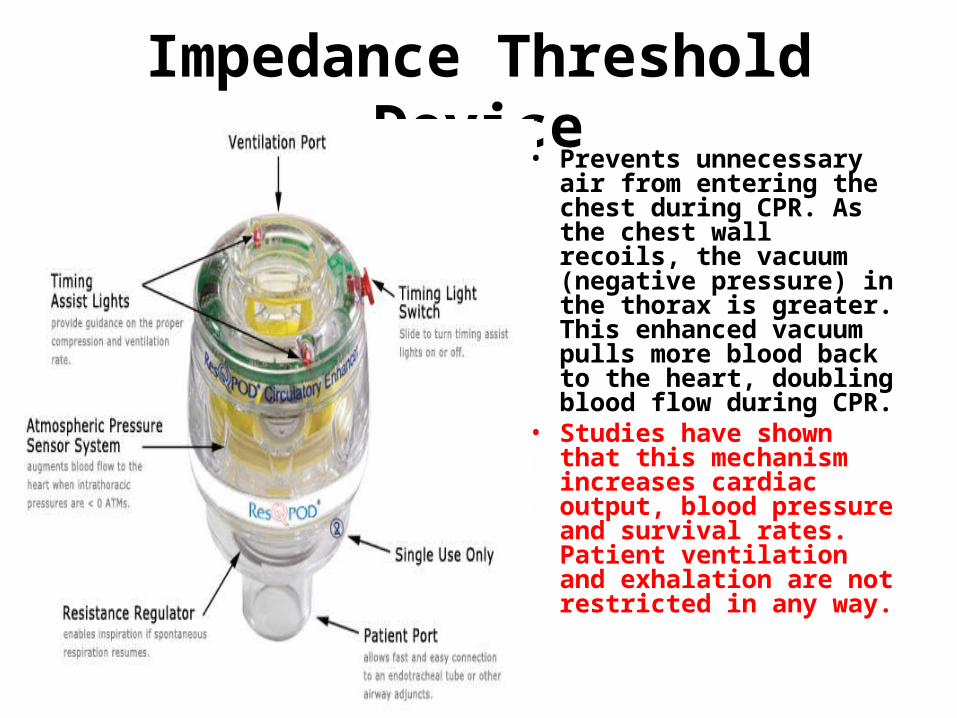
Impedance Threshold Device• Prevents unnecessary air
from entering the chest during CPR. As the chest wall recoils, the vacuum (negative pressure) in the thorax is greater. This enhanced vacuum pulls more blood back to the heart, doubling blood flow during CPR.
• Studies have shown that this mechanism increases cardiac output, blood pressure and survival rates. Patient ventilation and exhalation are not restricted in any way.

Airway Management
• Advanced airway– King LT– Combi-Tube– Endotracheal intubation

Advanced Airway Adjuncts
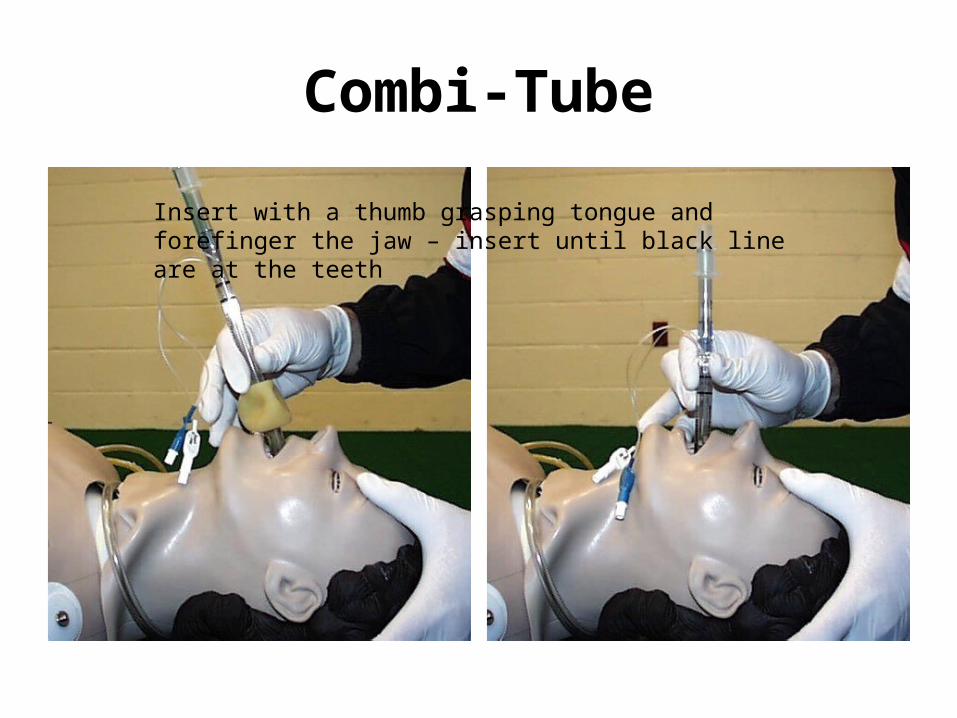
Combi-Tube
Insert with a thumb grasping tongue and forefinger the jaw – insert until black line are at the teeth

Combi-Tube
Combi-Tube Installed

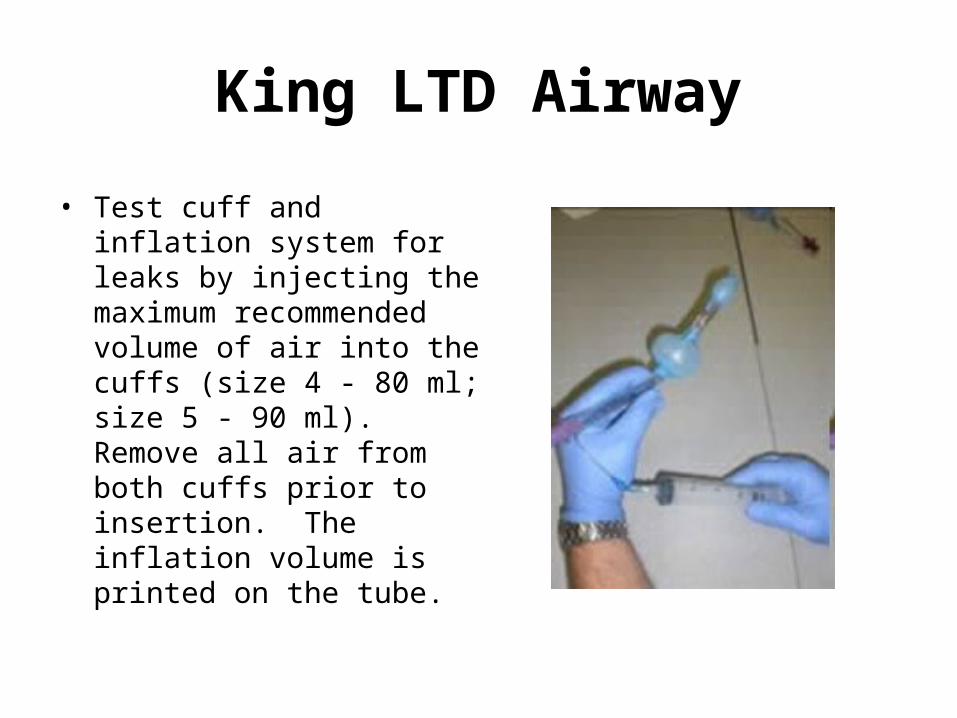
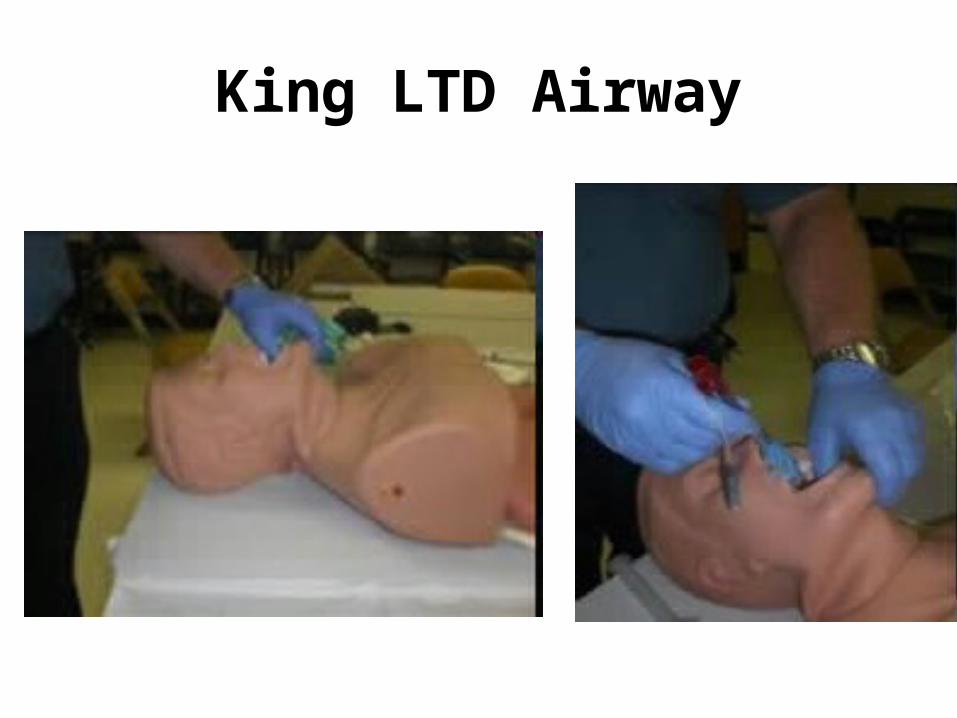
King LTD Airway
King LTD Airway
• Test cuff and inflation system for leaks by injecting the maximum recommended volume of air into the cuffs (size 4 - 80 ml; size 5 - 90 ml). Remove all air from both cuffs prior to insertion. The inflation volume is printed on the tube.
King LTD Airway

Simulaids
Laerdal Resusci Anne SkillGuide manikins

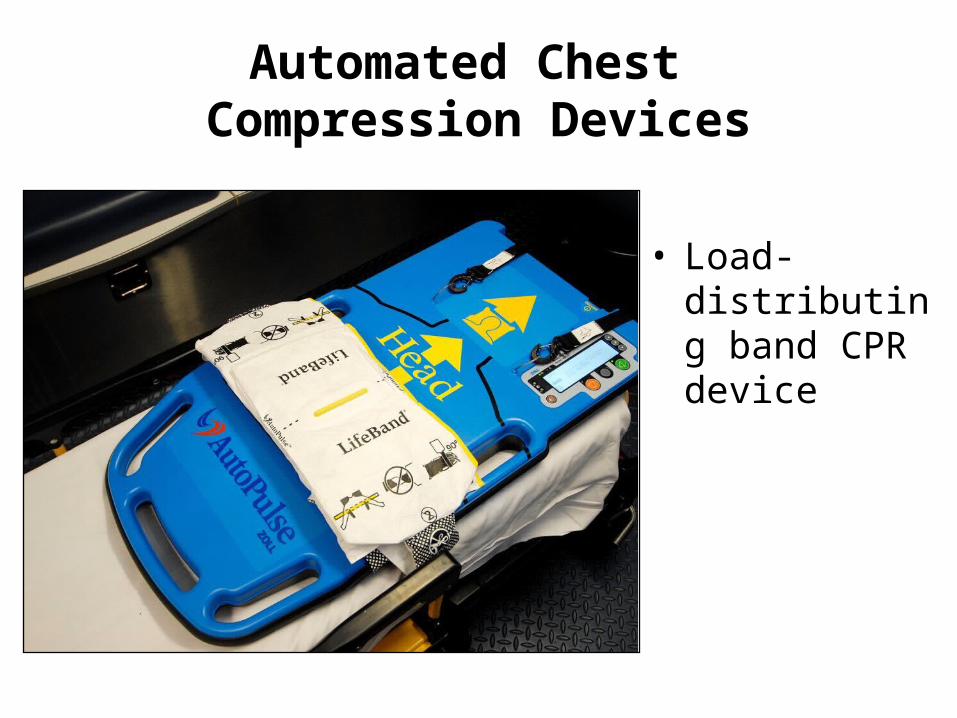
Automated Chest Compression Devices
• Mechanical piston device
Automated Chest Compression Devices
• Load-distributing band CPR device

Scenario Based Training
University of Georgia Sports Medicine
University of Georgia Sports Medicine
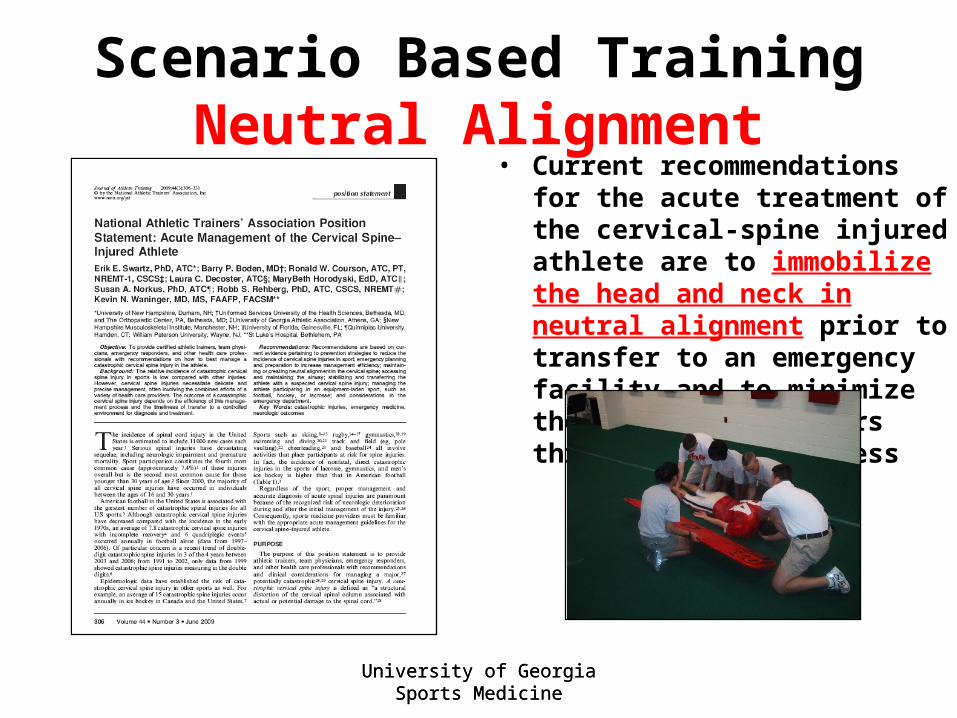
Scenario Based TrainingNeutral Alignment
• Current recommendations for the acute treatment of the cervical-spine injured athlete are to immobilize the head and neck in neutral alignment prior to transfer to an emergency facility and to minimize the motion that occurs throughout this process

Scenario Based Training

Scenario Based Training

Scenario Based Training
Scenario Based Training

Scenario Based Training

Scenario Based Training
Scenario Based Training
University of Georgia Sports Medicine
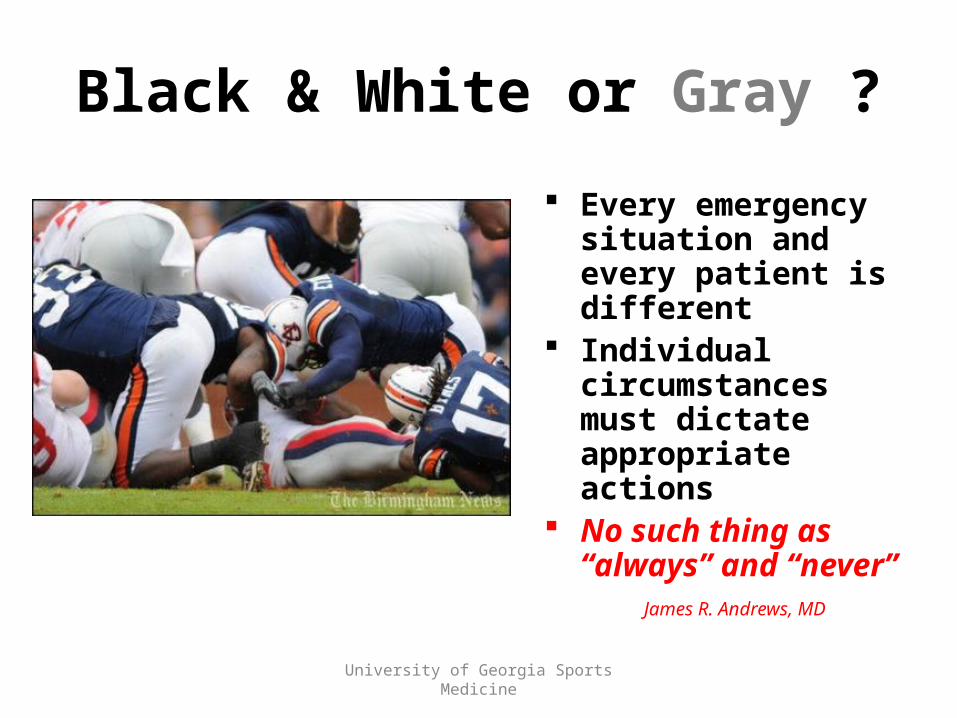
Black & White or Gray ?
Every emergency situation and every patient is different
Individual circumstances must dictate appropriate actions
No such thing as “always” and “never”
James R. Andrews, MD
Related Documents











