Accepted Manuscript Searching for cognitively optimal challenge point in physical activity for children with typical and atypical motor development Caterina Pesce, Claudia Crova, Rosalba Marchetti, Ilaria Struzzolino, Ilaria Masci, Giuseppe Vannozzi, Roberta Forte PII: S1755-2966(13)00030-6 DOI: 10.1016/j.mhpa.2013.07.001 Reference: MHPA 115 To appear in: Mental Health and Physical Activity Received Date: 28 December 2012 Revised Date: 18 June 2013 Accepted Date: 5 July 2013 Please cite this article as: Pesce, C., Crova, C., Marchetti, R., Struzzolino, I., Masci, I., Vannozzi, G., Forte, R., Searching for cognitively optimal challenge point in physical activity for children with typical and atypical motor development, Mental Health and Physical Activity (2013), doi: 10.1016/ j.mhpa.2013.07.001. This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Accepted Manuscript
Searching for cognitively optimal challenge point in physical activity for children withtypical and atypical motor development
Caterina Pesce, Claudia Crova, Rosalba Marchetti, Ilaria Struzzolino, Ilaria Masci,Giuseppe Vannozzi, Roberta Forte
PII: S1755-2966(13)00030-6
DOI: 10.1016/j.mhpa.2013.07.001
Reference: MHPA 115
To appear in: Mental Health and Physical Activity
Received Date: 28 December 2012
Revised Date: 18 June 2013
Accepted Date: 5 July 2013
Please cite this article as: Pesce, C., Crova, C., Marchetti, R., Struzzolino, I., Masci, I., Vannozzi,G., Forte, R., Searching for cognitively optimal challenge point in physical activity for children withtypical and atypical motor development, Mental Health and Physical Activity (2013), doi: 10.1016/j.mhpa.2013.07.001.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Searching for cognitively optimal challenge point in physical activity
for children with typical and atypical motor development
Caterina Pesce1, Claudia Crova 1, Rosalba Marchetti 1, Ilaria Struzzolino 1, Ilaria Masci1,
Giuseppe Vannozzi1, Roberta Forte 1
1Italian University Sport and Movement, Department of Human Motion and Sport Science, Italy
Correspondence concerning this article should be addressed to:
Caterina Pesce, University of Rome ‘Foro Italico’ Piazza L. De Bosis 15, 00135 Rome, Italy Phone: +39 06 36733366 Fax: +39 06 36733362 e-mail : [email protected]
E-mail addresses of the non-corresponding authors: . [email protected] [email protected] [email protected] [email protected] [email protected] [email protected]
This research has received financial support by the Advanced Distribution S.p.A. The sponsor had no role in study design; collection, analysis and interpretation of data; in writing of the report; and in decision to submit the article for publication. There are no interests or activities that might be seen as influencing the research.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 1
Searching for cognitively optimal challenge point in physical activity
for children with typical and atypical motor development
Date of submission: December 28, 2012
Date of resubmission: June 18, 2013
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 2
Abstract
Statement of problem. Growing evidence testifies that different types of physical activity (PA)
interventions promote cognitive development, but the specific impact of the cognitive demands inherent
in PA still remains underconsidered. This study investigated whether (1) increasing the cognitive
demands of PA positively impacts children’s executive function and (2) this ‘enrichment’ also matches
the ability/skill level of children with Developmental Coordination Disorder (DCD).
Methods. Two hundred and fifty children aged 5-10 years participated in different physical
education interventions, lasting six months, with or without special focus on cognitively demanding PA.
Before and after the intervention, children’s executive function was tested with the attention and
planning subscales of the Cognitive Assessment System and their motor developmental level classified
as typical, borderline, or DCD according to their performance evaluated by the Movement Assessment
Battery for Children.
Results. Among indices of executive function, those of Attention showed a differential effect of
PA type as a function of children’s motor developmental level: typically developing children gained
greatest attentional benefit from PA with additional cognitive demands, while children with
coordinative problems/impairment from the PA program without cognitive enrichment. Changes from
DCD to borderline or normal developmental status did not differ in frequency as a function of
intervention type.
Conclusions. Results showed that cognitively more or less challenging PA programs are
differently efficacious for promoting attention development and highlight the need to find and
continuously reset the degree of task complexity in PA to match the optimal challenge point of normal
and special children populations.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 3
Highlights
• We examine the cognitive benefits of physical activity (PA) interventions
• The qualitative aspects of physical exercise tasks may impact children’s cognition
• Adding cognitive demands to physical exercise promotes attention development
• Optimal challenge point depends on children’s typical/atypical motor development
• We need research on the ‘dose’ of cognitive demands in PA to gain greatest benefits
Key words: exercise, cognition, executive function, attention, developmental coordination
disorder, quality physical activity
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 4
Searching for cognitively optimal challenge point in physical activity
for children with typical and atypical motor development
Strong evidence supports the benefits of physical activity (PA) for children’s physical health, as
indicated by cardiovascular and musculoskeletal health outcomes (Kristensen et al., 2010; Strong et al.,
2005) and for their mental health, as shown by self-perception, emotional, and cognitive outcomes
(Ahn & Fedewa, 2011; Biddle & Aasare, 2011). In the last decade, developmental researchers have
devoted increasing attention to cognitive functioning as a relevant mental health outcome of PA and
particularly to executive cognitive functions, which are responsible for self-regulation, goal-oriented
and health-related behaviours (Tomporowski, Davis, Miller, & Naglieri, 2008; Tomporowski,
Lambourne, & Okumura, 2011).
While such evidence testifies the importance of PA at pediatric age, there is alarming evidence
of secular decremental trends in children’s PA levels (e.g., Dolmann, Norton, & Norton, 2005) and
physical fitness test performance (e.g., Tomkinson, Leger, Olds, & Carzola, 2003) and an emergent
health concern with ‘exercise-deficit disorder’ (Faigenbaum, Stracciolini, & Myer, 2011). Secular
trends of decline have been also documented in children’s coordination and fundamental motor skills
proficiency (Raczek, 2002) with onset as early as at preschool age (Roth et al., 2010; Vandorpe et al.,
2011), but research regarding these trends is still scarce and geographically limited. The scarce interest
for secular trends in motor coordination at pediatric age is surprising if we consider the close
interrelation existing between cognitive and motor development and, correspondingly, between the
development of the brain substrates responsible for executive function and motor behaviour (Diamond,
2000; Pennequin, Sorel, & Fontaine, 2010). Also from the perspective of atypical motor development,
several decades of research have evidenced that children with severe motor clumsiness and impairments
in motor control and perceptual-motor functioning (i.e., Developmental Coordination Disorder, DCD;
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 5
American Psychiatric Association, 2000) have co-occurring cognitive and attentional problems (Kirby
& Sudgen, 2007) and a strong association exists between DCD and deficits relying on executive
function impairment (i.e., Attention Deficit Hyperactivity Disorder, ADHD) (Sergeant, Piek, &
Oosterlaan, 2005).
As a consequence of the unbalanced attention devoted to secular trends in children’s fitness and
coordination, PA guidelines for young people scarcely consider aspects other than exercise quantity and
fitness-related health. This represents a problem particularly in childhood that has been defined as ‘skill
hungry years’ during which strongest emphasis should be put on PA experiences promoting motor and
cognitive development (Kirk, 2005). This problem may also reflect the general lack of specificity in
defining and measuring dimensions of PA for children from a qualitative point of view that goes beyond
the framework of intensity, duration and frequency of activity (Dwyer, Baur, & Hardy, 2009).
Recently, it has been pointed out that this unbalanced interest for PA quality and quantity in
favour of the latter extends to the area of exercise and cognition (Pesce, 2012). Also the attention of
investigators working on the relationship between PA and cognitive function during development still
mainly focuses on how the quantity of PA practiced by children and the resulting physical fitness affect
children’s cognition (Hillman, Erickson, & Kramer, 2008; Singh, Uijtdewilligen, Twisk, van Mechelen,
& Chinapaw, 2012). Instead, relatively little research has examined how the cognitive or social
interaction demands of PA (Best, 2012; Pesce, Crova, Cereatti, Casella, & Bellucci, 2009) and its motor
coordination demands (Budde, Voelcker-Rehage, Pietraßyk-Kendziorra, Ribeiro, & Tidow 2008;
Gallotta et al., 2011) impact children’s cognition independently of exercise intensity and duration (see
Best, 2010 for a review). These studies, exclusively regarding the transient effects of a single bout of
acute exercise, have lead to diverging results on the role of the amount of cognitive engagement by
movement. Cognitive engagement or effort may be conceived as the allocation of limited resources to
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 6
an ongoing task requiring mental operations and information processing. It is determined by executive
processes that draw on mental resources, as when individuals perform novel or complex tasks requiring
to consider multiple response pathways, but are only scarcely or not at all needed to perform repetitive
responses that have been highly learned with extended practice (Tomporowski, McCullick, & Horvat,
2010). It remains to be tested whether cognitive engagement by complex and variable movement tasks
in chronic exercise interventions may aid the development of executive functions in the preschool and
primary school years in which such functions ‘come online’ (Garon, Bryson, & Smith, 2008; Huizinga,
Dolan, & van der Molen, 2006).
This lack of developmental intervention studies in which the cognitive engagement in PA is
manipulated by varying the cognitive and motor coordination demands of the physical exercise tasks is
surprising. As a relevant review of interventions indicates (Diamond & Lee, 2011) executive function
development can be aided in playful ways by mindfulness PA and sport practices, such as martial arts.
However, attempts to deliberately apply executive function training by integrating specific cognitive
demands into physical education (PE) games are still rare (Kubesch & Walk, 2009), as well as attempts
to promote the development of executive function in children with motor developmental problems by
capitalizing on the cognitive challenges of sport activities such as table tennis (Tsai, 2009).
The present study investigated the effects, on children’s executive functions, of school-based PA
interventions led by PE specialist teachers which either (1) included or (2) did not include additional
cognitive demands specifically tailored to challenge executive function. Since in many countries PE in
the early school years still is the responsibility of the classroom generalist teacher, we also assessed the
cognitive outcomes of PE when it was (3) taught by generalist teachers. We verified whether the
cognitive ‘enrichment’ of PA matches the ability/skill level of children with or without motor
developmental problems. Since acute exercise studies in which the cognitive and coordinative
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 7
complexity of the PA tasks was manipulated have shown diverging effects on executive function (Best,
2012; Budde et al., 2008; Gallotta et al., 2012; Pesce et al., 2009), we hypothesized that the ‘dose’ of
cognitive and coordinative demands of the PA tasks may act as a moderator of the exercise-cognition
relationship and that the emergence of cognitive benefits depends on the interplay between individual
differences in motor development and amount of cognitive challenge in PA.
Methods
Participants
In the school year 2010/11, three kindergarten-primary schools of the Municipality of Rome
(Italy) participated in the study. They belonged to similar urban districts and had a homogeneous socio-
economic profile, as assessed using an area based measure. Within each school, seven gender-balanced
classes (two kindergarten classes with children aged 3-5 years and five first to fifth grade classes with
children aged 6 to 10 years) were selected according to teacher and class availability and randomly
assigned to different PE programs. Since in the school setting, random assignment of individuals to
different treatments is not feasible, we ‘traded’ the gold standard of fully randomized controlled trials
for the ecological validity of school class settings. The parents of all participants provided informed
written consent in conformity with the laws of the country and all children provided verbal assent
before involvement in the study. The study protocol was approved by the institutional ethics committee.
Of the total 530 children involved in the intervention, 250 (127 male and 123 female) children
aged 5-10 years, who were eligible for cognitive and/or motor coordination assessment, had no known
diagnosed disorder of cognition and no physical condition hindering them to participate in a school PE
program and did not miss any assessment session, represented the actual sample.
Baseline differences in PA levels and, given the young age of the children, differences in
spontaneous outdoor play between children assigned to the different PE interventions may influence the
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 8
intervention outcomes on cognitive functioning. Thus, outdoor play and PA levels were evaluated prior
to the intervention period on a subsample of children (n=76), stratified for schools and classes. Parents
completed the Children’s Outdoor Play Assessment Questionnaire (Veitch, Salmon, Ball, 2009) and
older primary school children completed, under the supervision of the researchers, the Physical Activity
Questionnaire for Children (PAQ_C) (Kowalski, Crocker, & Donen, 2004). No significant differences,
as assessed by means of t-test for independent samples, emerged among children assigned to the three
types of intervention (Table 1). Generalists and PE specialists volunteered in the study. The generalists
had a basic qualification for primary school teaching, but never participated in specific teacher training
for PE, whereas the specialists were licensed to teach PE.
Intervention and allocation procedures
There were two types of experimental PE intervention and one standard PE program. The two
experimental interventions were directed by PE specialist teachers (specialist-led, S-led), whereas
standard PE was directed by classroom generalist teachers (generalist-led, G-led). Both the generalists
and the PE specialists taught PE according to the age-related PE goals defined in the Italian curriculum
for kindergarten and primary school (basically motor and social skills development). However, the
generalists did not receive any particular instruction by the researchers. This was done to obtain an
ecologically valid control condition. Instead, the specialists were provided with guidelines for and
received training in the experimental interventions. The researchers devised two intervention programs
both made of similar PA games that emphasized variability of practice and widely challenged motor
control and perceptual-motor adaptation abilities.
The two specialist-led PE programs differed from one another in that in one of them, the PA
games were altered to involve a higher amount of mental engagement and were specifically tailored to
challenge executive functions (cognitively challenging specialist-led—ceS-led—intervention). This was
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 9
done by joining instructional principles of executive tasks used in cognitive developmental research
(Garon et al., 2008; Huizinga et al., 2006) with the principle of contextual interference as applied in
children’s motor learning (Tomporowski, et al., 2010). This principle, that following seminal research
(Shea and Morgan, 1979) has found large application in motor skill learning and sports training
(Vickers, 2007), affirms that learning is enhanced when interference during practice is high, as when
participants practice multiple tasks in a random order. In our intervention, for example, games were
altered in a way that children’s roles were no longer fixed, but fluctuated along the game. Also in
further games, children had to hold a rule in mind and respond according to this rule that randomly
required inhibiting a habitual response. Contextual interference is assumed to emerge because blocked
practice is not sufficiently demanding to produce optimal effort. Consistent with this view, contextual
interference is reduced or eliminated with more complex tasks (see Wulf & Shea, 2002). Therefore we
did not only use random practice as a mean to promote cognitive engagement, but also employed games
characterized by varying task complexity, with challenge incrementing, to keep children on the learning
curve (Tomporowski et al., 2010) and continuously stimulate executive control (Diamond & Lee,
2011). Also, open-ended tasks were employed in which only the starting point, the rule(s) and the task
goal were indicated and children were encouraged to find many possible solutions to perform it.
The intervention outcomes may depend on PE content and the delivery skills of the teachers as
well as on intensity and duration of physically active time in PE. Thus, PE sessions were observed
directly and videotaped in two randomly selected classes for each type of intervention to identify the
true characteristics of teachers’ individual instruction methods and teaching strategies and exercise
intensity was monitored by recording heart rate (HR) with HR monitors (Polar S610i) on a subsample
of children (n = 12 for each school) once a month. The qualitative intervention features were
categorized as teacher’s behavioural categories according to Rink’s Observation System for Content
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 10
Development-Physical Education (OSCD-PE) and teaching strategies (Rink, 2006) (Table 2). The
outcomes of the categorization, quantified as percentage (%) of events for time unit (20 sec) during PE,
were submitted to reliability computation. A satisfactory intra- and inter-observer agreement, indicated
by a percentage of agreement [Agreements/(Agreements + Disagreements) x 100] ≥ .80, was reached.
The time spent in moderate to vigorous physical activity (MVPA) was operationalized as HR > 139
bpm (Wang, Pereira, & Mota, 2005). The qualitative characteristics of PE teaching, the intensity and
duration of physically active time are reported on Table 3 separately for the three intervention types.
Each school was randomly allocated to receive two of the three interventions (first school: three G-led
and four S-led classes; second school: four G-led and three ceS-led classes; third school: three S-led and
four ceS-led classes). All children participated in PE for 1 hour once a week, corresponding to the
National curricular PE time, and the intervention duration was 6 months. The teacher-student ratio was
about 1:25. Following familiarization to tests protocols, participants were assessed two times: at
baseline and post-intervention. The same procedures and schedule were applied for pre- and post-
intervention testing, with cognitive and motor testing being administered by a trained experimenter in
the morning, within the same week in the same order (cognitive testing first) and not preceded by PA
lessons to avoid acute exercise effects.
Insert Tables 1-3 about here
Cognitive assessment
To assess children’s cognitive performance, the Cognitive Assessment System (CAS) (Naglieri &
Das, 1997, Italian version 2005) was used. The CAS consists of 12 subtests that assess 4 aspects of
cognition: Planning, Attention, Simultaneous and Successive processes (PASS theory) (Das, Naglieri,
& Kirby, 1994). For the present study, because of school time constraints, participants only performed
the Planning and Attention tasks which are the test performances most strongly relying on executive
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 11
functions. Also, we did not collect test-retest reliability data, since acceptable to good reliability data are
available for children of the age 5-10 years considered in this study (Naglieri & Das, 1997).
Planning. Planning is a cognitive process by which the individual determines, selects, and uses a
strategy to efficiently solve a problem.The Planning scale is composed of three subtests. The first
subtest, Matching Numbers, contains 4 items, each with 8 rows of numbers and 6 numbers per row,
with numbers increasing in digit length every four rows. The child must locate and underline the two
numbers in each row that are the same. The second subtest, Planned Codes, contains two items, each
within a matrix of 7 rows and 8 columns of letters with empty boxes. A caption is presented that shows
correspondence between letters and codes presented as a legend at the top of the page (e.g., A to OX
and B to XX). The child’s task is to fill in the empty boxes under each letter with the corresponding
codes discovering their internal organization to solve the task. The last subtest, Planned Connections,
contains 8 items. The first six require the child to join a series of numbers that are randomly distributed
in space in a sequential order, with an increasing length of numbers to be connected. The last two items
require the child to alternately connect numbers and letters serially (i.e., 1-A-2-B etc.). The items are
designed so that a child cannot complete a sequence by crossing one line over the other. To evaluate
performance on the first two subtests, the raw score is the ratio of the accuracy (total number correct)
and time to completion. For the third subtest, the raw score is the sum of the times required to complete
each item. All these scores are then converted to an age-based standard score and summed to obtain a
total scale value.
Attention. The Attention scale is composed of three subtests that require the child to use focal
attention to detect target stimuli and avoid distractions. The first subtest, Expressive Attention, is a
Stroop-like test composed of three items that measures attention selectivity and interference control
under time pressure. The first and the second items are without interference condition, while the third is
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 12
with interference. There are two age-specific sets of items. For example, in the version for children 8
years and older, the non-interference conditions are reading color words (Blue, Yellow, Green, and Red)
all written in dark ink and naming the colors of a series of rectangles (printed in blue, yellow, green, and
red). In the interference condition, the words Blue, Yellow, Green, and Red are printed in a different
color ink than the colors the words name and the child is instructed to name the color ink the word is
printed in, rather than to read the word. Only this last item is used as the measure of attention. The
second subtest, Number Detection, measures selectiveness and capacity to resist distraction under time
pressure. It is comprised of pages of numbers where the child must underline the correct numbers
among a large quantity of distracters in different formats. For example, the child must find a particular
stimulus (the number 1, 2, and 3 printed in an open font) on a page containing many distracters (the
same numbers printed in a different font style). The raw score is the ratio of the accuracy (total number
correct minus the number of false detections) and the time to completion summed across the items. The
third subtest, Receptive Attention, is a two-page subtest that measures the ability to focus and then shift
attention between different stimulus dimensions under time pressure. On the first page, children 8 years
and older must identify and underline pairs of target letters that are physically identical (e.g., TT but not
Tt), whereas on the second, pairs of letters that have the same name (e.g.,, Aa not Ba) are targets to be
underlined. For all subtests, the raw score is the ratio of the accuracy (total number correct in the first
subtest and total number correct minus the number of false detections in the second and third subtests)
and time to completion summed across items/pages. The raw score for each subtest is converted to an
age-based standard score and summed to obtain a total scale value.
Motor assessment
To assess children’s motor coordination performance, the Italian version of the Movement
Assessment Battery for Children (M-ABC) developed by Henderson and Sudgen (1992) was used. This
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 13
test evaluates movement competence providing objective quantitative data on both gross motor and fine
motor coordination of children aged from 4 to 12 years with eight tasks differentiated in four age-
related difficulty levels. The M-ABC has been proved to be a valid and reliable research and diagnostic
tool that covers the entire domain of motor ability and is used to identify motor problems and DCD
(Croce, Horvat, & McCarthy, 2001). The tasks are grouped under three subheadings: manual dexterity,
ball skills, and static and dynamic balance.
Manual dexterity. There are three tasks that slightly differ as a function of the child’s age. The
first is ‘posting coins’ (5 to 6 year-old), ‘placing pegs’ (7 to 8 year-old), or ‘shifting pegs by rows’ (9 to
10 year-old). The child must drop coins through the slot in a bank box, or place 12 plastic pegs in all
holes on a board, or move pegs from a given row to another, respectively, one at a time as quickly as
possible. The second task is ‘threading beads’ (5 to 6 year-old), ‘threading lace’ (7 to 8 year-old), or
‘threading nuts on bolt’ (9 to 10 year-old). The child must thread beads through a lace, or thread a lace
back and forth through the holes in a lacing board, or screw nuts down a bolt, respectively, one at a time
as quickly as possible. In both the first and second tasks, the examiner measures the seconds taken to
complete each task. The third task is ‘bicycle trail’ (5 to 6 year-old), or ‘flower trail’ (7 to 10 year-old).
The child must draw with the preferred hand one continuous line following the bicycle or flower trail on
a record form without crossing its boundaries. The examiner records the number of errors, i.e. the
number of times the drawn lines moves outside a boundary.
Ball skills. There are two tasks differing as a function of the child’s age. The first is ‘catching
bean bag’ (5 to 6 year-old), ‘one-hand bounce and catch’ (7 to 8 year-old), or ‘two-hand catch’ (9 to 10
year-old). The child must catch a bean bag tossed by the experimenter, or bounce a tennis ball on the
floor and catch it with the same hand, or throw a tennis ball at the wall form behind a marked distance
of 2 m and catch it at the return with both hands, respectively. The second task is ‘rolling ball into goal’
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 14
(5 to 6 year-old), or ‘throwing bean bag into box’ (7 to 10 year-old). The child must roll a tennis ball
along the floor between two stands, 40 cm apart from one another and 2 m apart from the child, to score
a ‘goal’, or throw a bean bag into a target box on the floor form behind a marked distance of 2 m (7 to 8
year-old) or 2,5 m (9 to 10 year old), respectively. In both types of tasks, the examiner records the
number of correctly executed trials (successful catches and throws) out of ten attempts.
Static and dynamic balance. There are three tasks differing as a function of the child’s age: one
for static balance and two for dynamic balance. The task evaluating static balance is ‘one-leg balance’
(5 to 6 year-old), ‘stork balance’ (7 to 8 year-old), or ‘one-board balance’ (9 to 10 year-old). The child
must stand on one leg, with the arms held at the sides, or stand on a foot, place the sole of the other foot
against the side of the supporting knee and the hands on the hips, or balance on one foot on a balance
board, respectively. The examiner records the number of seconds, up to 20, the child maintains balance
without moving the standing and the non-standing foot. The second task is ‘jumping over cord’ (5 to 6
year-old), ‘jumping in squares’ (7 to 8 year-old), or ‘hopping in squares’ (9 to 10 year-old). The child
must jump over the cord from a stationary position, landing with feet together, or make five continuous
jumps forward from a starting square to further five squares, or make five continuous hops forward
from square to square on one foot, respectively. The examiner records if the child performs a successful
jump (‘jumping over cord’) or the number of correct consecutive jumps/hops completed over five
without performance errors (‘jumping or hopping in squares’). The third task is ‘walking heels raised’
(5 to 6 year-old), ‘heel-to-toe walking’ (7 to 8 year-old), or ‘ball balance’ (9 to 10 year-old). The child
must walk along a 4.5 m line with heels raised without stepping off the line, or walk on a line placing
the heel of one foot against the toe of the other, or walk around the outside of two stands 2.7 m apart
and return to the starting point while steadying a board with a ball in the middle of it, respectively. The
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 15
examiner records the number of steps performed by the child without leaving space between toe and
heel or stepping off the line.
Data coding and scoring. The M-ABC data were standardized to compute average scores for the
three subheadings of manual dexterity, ball skills, and static and dynamic balance. The data were also
transformed into scores of impairment of motor function according to age-related normative data
(Henderson & Sudgen, 1992). Each impairment score indicates the extent to which a child falls below
the level of his/her age peers, while it does not differentiate between children who perform above this
level. A total score of impairment was computed as the sum of the scores obtained for each subheading
(manual dexterity, ball skills, and balance) in order to identify typically developing children and
children with movement problems or impairment. The 15th percentile is the threshold value for
coordinative developmental problems (borderline), the 5th percentile is the threshold value for
impairment (DCD). We did not collect test-retest reliability data, since high reliability results are
available for children across all age groups considered in this study (Croce et al., 2001; Henderson &
Sudgen, 1992).
Statistical analysis
Firstly, both physically active time in PE and percentage of active time spent in MVPA were
compared in the three intervention groups by means of univariate ANOVAs with group (G-led, S-led,
ceS-led) as factor followed by pairwise comparisons between groups (t-tests). Secondly, difference
values between pre- and post-intervention measures (pre-post delta) were computed for all CAS
measures of planning (Planning total score and Planned Codes, Matching Numbers, Planned
Connections scores) and attention (Attention total score and Expressive Attention, Number Detection
and Receptive Attention scores). Then a general linear model was applied to all delta scores with motor
developmental level (normal, borderline, DCD), group (G-led, S-led, ceS-led), and school (nested
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 16
within group) as factors and age and baseline planning or attention scores as covariates. These
covariates were included to exclude that any difference in age and baseline levels of planning and
attention ability might be responsible for differential intervention outcomes. In the case of significant
effects, planned pairwise comparisons (t-tests) were performed when appropriate and Bonferroni
correction was applied for multiple comparisons. Also, data were coded as a function of whether
children’s motor developmental classification changed from pre- to post-intervention from
DCD/borderline to borderline/typically developing. Then chi square statistics were applied to verify
whether the frequency of improvement cases differed as a function of the type of intervention.
Results
The overall percentages of typically developing, borderline and DCD children were 67.6%,
18.4%, and 14.8% respectively. The prevalence of children with DCD was consistent with the literature
and intermediate between that reported in European and American surveys (Tsiotra et al., 2006).
Children’s compliance to the CAS and M-ABC, as well as to PE classes was generally very good.
Adjusted analyses from general linear models of pre-post delta (∆) of cognitive performance
variables, with age and baseline score as covariates and school nested within group, did not show
differential intervention effects as a function of group and/or motor developmental level in the total
Planning scale or any of the Planning subtest scores. Instead, significant Group x Developmental Level
interactions emerged for ∆ total Attention scale, F(2, 239) = 5.16, p=.006, ηp2=.04, ∆ Expressive
Attention, F(2, 239) = 2.94, p=.05, ηp2=.03, and ∆ Receptive Attention, F(2, 239) = 7.19, p=.001,
ηp2=.06, subtest scores. Post-hoc analyses (adjusted p for six pairwise comparisons = .008) showed that
the different interventions exerted differential effects on the attention of typically developing and
borderline/DCD children.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 17
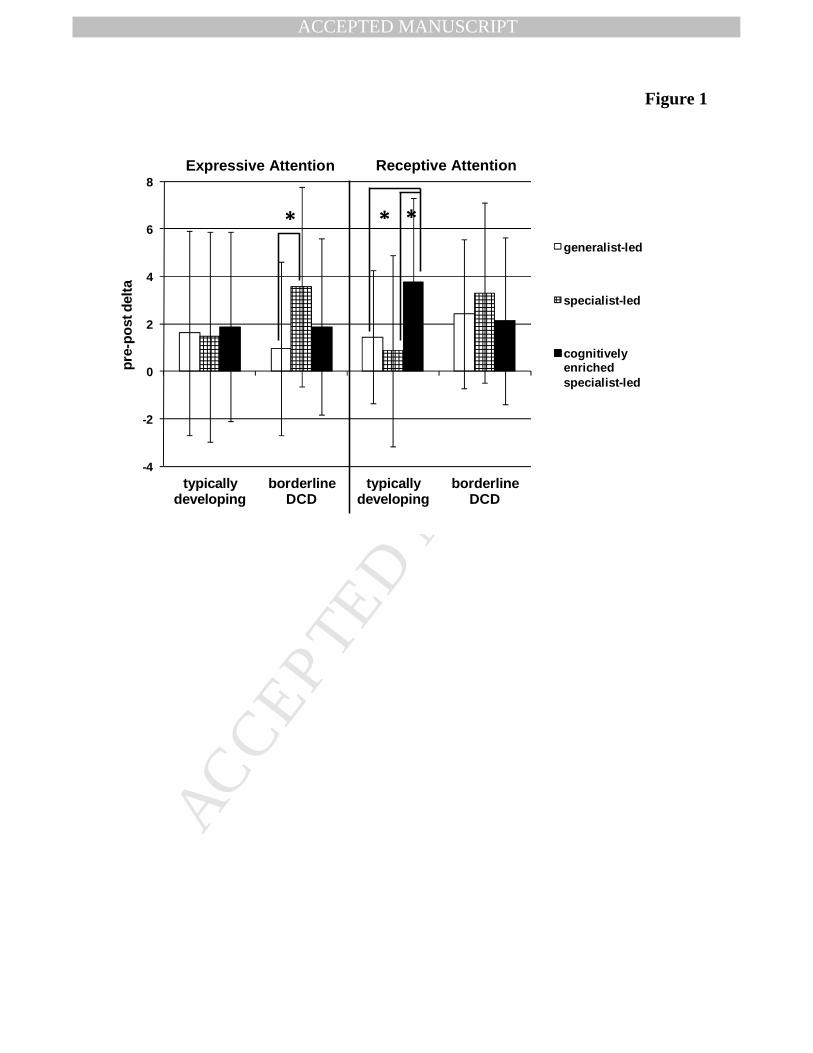
Typically developing children assigned to the ceS-led intervention showed more pronounced pre-
to-post improvements (positive ∆ values) in the total Attention scale (9.2±7.4), than typically
developing children in the G-led (5.5±7.6) and the S-led (4.2±9.9) groups. Analysis of attention
subscales showed that this advantage of the ceS-led group as compared to the other two intervention
groups was attributable to amelioration in Receptive Attention performance (Figure 1, right).
In contrast, borderline/DCD children did not show significant differences between intervention
groups in the total Attention scale (7.4±7.0, 9.1±9.4 and 7.8±9.3, for the G-led, S-led and ceS-led
groups, respectively). The non-significantly higher ∆ Attention of borderline/DCD children in the S-led
group reached significance, as compared to the G-led group, in the analysis of Expressive Attention data
(Figure 1, left), but not in that of Receptive Attention performance (Figure 1, right).
Insert figure 1 about here
Chi square tests performed on frequency of post-intervention ameliorations in M-ABC
performance showed that the amount of children whose classification changed from DCD/borderline to
borderline/typically developing did not significantly differ between intervention groups, although a non-
significant larger amount of improvement cases was observed in the ceS-led group (Table 1).
Among the three intervention types, there were significant differences in physically active time,
F(2, 33) = 36.85, p<.001, ηp2=.69, and in % of active time in MVPA, F(2, 33) = 3.63, p=.038, ηp
2=.18.
Post-hoc tests (adjusted p for three pairwise comparisons = .016) showed that the active time in the S-
led PE lessons was significantly longer than in the G-led and ceS-led PE lessons, whereas the
percentage of active time spent in MVPA only differed between S-led and G-led groups (Table 3).
Considering the relatively short physically active time (about half an hour per 1 hour PE lesson), the %
active time spent in MVPA equated to approximately only 12 and 15 minutes per PE lesson in the G-led
and ceS-led groups, respectively, but to 23 minutes in the S-led group. As compared to generalist
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 18
teachers, specialists – regardless of the presence or absence of additional cognitive demands – spent less
time for informing, but more for organizing the learning environment. As regards teaching styles, while
the generalist teachers made sometimes use of peer teaching, the PE specialists prioritized the
interactive style and, when they taught PA games with enhanced cognitive challenges, they also
adequately employed a cognitive teaching style (Table 3).
Discussion
The present study focused on whether qualitatively different types of PA interventions in school
settings may differently impact children’s executive function. The route by which PA impacts mental
functioning and particularly fosters executive function development is likely moderated by task
variables, such as physical exercise intensity, duration, and complexity, and individual characteristics,
such as physical fitness level, health status, and psycho-social factors (Pesce, 2009; Tomporowski et al.,
2011). We aimed to extend the notion of dose-response relationship (Pesce, 2012) examining whether
varying the amount of coordinative and cognitive complexity of the movement tasks we may meet the
need for an appropriate challenge point to induce executive function enhancement in children with
typical and atypical motor development.
On the whole, four main points emerged from the findings of this study.
(1) Attention development in the kindergarten and primary school years can be aided by specialist-
led PA experiences including targeted cognitive challenges. However, the efficacy of cognitive
engagement in PA for promoting attention development depends on the type and ‘dose’ of cognitive
challenges by movement and children’s motor developmental level.
(2) In typically developing children, attention selectivity and interference control, as reflected in
‘Expressive Attention’ data, did not show differential improvements following the three qualitatively
different types of intervention. PA per se, regardless of its cognitive challenges, increases physiological
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 19
arousal, which in turn allows for greater allocation of attention to exert cognitive control over
interference and avoid distractions (Best, 2012; Hillman et al., 2009).
(3) In children with motor developmental problems/impairment, this pathway seems to be
particularly effective at higher exercise intensity. In fact, they reaped larger ‘Expressive Attention’
benefits from the specialist-led interventions than from the generalist-led intervention which differed in
%MVPA. Moreover, children with motor developmental problems belonging to the specialist-led
classes obtained largest benefits when assigned to the PA intervention without additional cognitive
challenges.
(4) Only typically developing children, but not borderline children or those with DCD, benefited
mostly from the cognitively enriched PA program for improving their ability to focus and shift
attention, as reflected in the ‘Receptive Attention’ performance.
In summary, the different attentional outcomes of specialist-led PA as compared to generalist-led
PA may be due to the observed differences in both quantitative (i.e., intensity) and qualitative exercise
characteristics (i.e., content and delivery). Instead, the diverging response of children with or without
motor developmental problems to specialist-led PA interventions which differed in cognitive content
and delivery strategy, but not in exercise intensity, suggests the existence of a specific pathway through
which PA may aid executive function development: the direct stimulation by movement (Tomporowski
et al., 2011). This is in line with the potential of action to affect cognitive development (Rakison &
Woodward, 2008) especially during the sensitive periods in the development of neural structures
subtending high-level cognitive function (Thomas & Johnson, 2008).
Specifically, a specialist-led PA program without cognitive enrichment, but tailored to
emphasize variability of practice and widely challenging motor control and perceptual-motor adaptation
abilities is most appropriate for children with motor developmental difficulties, while a cognitively
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 20
enriched PA environment may represent an added value for typically developing children only.
Probably, children with atypical motor development need higher executive control to deal with
movement coordination difficulties and/or worse control over their gaze and visuospatial attention
underlying visuomotor control (Wilson, Miles, Vine, & Vickers, 2013). Since the games employed in
the cognitively challenging, specialist-led intervention often involved contextual interference and the
need to flexibly switch between visual stimulus-response associations, the low ability of children with
atypical motor development to pick-up task-relevant visual information may have led them to
ineffective task mastering and mental overload and challenged their executive function at a too high
degree. Carey, Bhatt, and Nagpal (2005) focused on the issue of proper level of cognitive engagement
and contextual interference in skill training, arguing that there may be a threshold above which any
increase in task complexity and cognitive effort is not beneficial. Our results suggest that such threshold
also exists in movement-based executive function training and must be fine-tuned with children’s motor
developmental level. This supports the importance to identify the optimal challenge point in PA as a
function of children’s typical/atypical motor development. The notion of optimal challenge point,
coined by Guadagnoli and Lee (2004), represents the degree of functional task difficulty an individual
of a specific skill level would need to optimize learning. Therefore, it takes into joint consideration the
skill level, task complexity, and task environment and will change as the individual’s abilities and skills
change. Our results suggest the opportunity to extend this notion from the challenges in the motor
domain to the cognitive challenges that may be inherent in movement tasks at different degrees.
The results obtained with children with atypical motor development confirm the appropriateness
to focus on PA intervention outcomes in the cognitive domain with this special children population
(Tsai, 2009). In adapted PA research, interventional studies with children with DCD are usually focused
on outcomes in the motor domain (Miyahara, Yamagichi & Green, 2008) also when the treatment is
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 21
cognitive in nature (Sudgen, 2007; Wilson, 2005) In the present study, the cognitively enriched PA did
not result to be especially advantageous in the motor domain for reducing cases of children with motor
problems (borderline) or impairment (DCD), since differences between intervention groups were
statistically negligible. Thus, the three intervention types were similarly useful for dampening
coordinative problems, or factors different from the PA intervention, such as growth, maturation, out-
of-school motor experiences, and habituation and learning of the motor assessment tasks may have been
responsible for general ameliorations in motor test performance.
The present findings showed the above described effects on children’s attention, but no effects
on planning ability as evaluated by the CAS. This is at odds with the outcomes of other developmental
chronic exercise studies employing the CAS and showing no differences between intervention and
control group changes in any CAS score (Fisher et al., 2011), or beneficial effects only on planning
performance (Davis et al., 2011). This divergence may be due to the type of PA interventions and
reconciled focusing on the concept of optimal challenge point. The above mentioned studies focused on
enhanced PA, either manipulating the duration of several weekly sessions (Davis et al., 2011), or
manipulating exercise intensity by enhancing the physically active time in PE and percentage of PE
lesson in MVPA within the curricular PE time (Fisher et al., 2011). The aim of these studies was to
search for the right ‘dose’ of quantitative exercise parameters for normal or overweight children. In
contrast, we manipulated the quality of PE experiences and particularly the amount and type of
cognitive stimulation inherent in the proposed activities while controlling for exercise intensity.
Our findings support the call for further research exploring whether the effects of PA on
executive functions differ as a function of task difficulty and cognitive demand (Hill et al., 2010).
However, it is to consider that we employed a low-dose PE intervention (1 hr/week), as it is prescribed
in the Italian preschool and primary school system, and the effect size was relatively small (.03 ≤ ηp2 ≤
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 22
.06). Thus on the one side, the evidence that even though embedded in a very low-dose PA program,
cognitively challenging movements may help obtain beneficial cognitive outcomes is encouraging. On
the other side, the small effect size calls for further interventional research exploring the cognitive
developmental outcomes that can be obtained joining high-dose PA (Davis et al., 2011) with an
appropriate level of cognitive challenge by movement (Crova et al., resubmitted after minor revisions).
In a recent study, Best (2012) examined the separate and combined effects of acute PA and
cognitive engagement on attentional interference control in children aged 6 to 10 years and found that
the combination of PA and cognitive effort did not have a stronger effect than PA alone. The
discrepancy of his results with the present findings may be due not only to differences between acute
and chronic exercise effects on cognition, but also to differences in attentional functions measured and
in manipulation of cognitive engagement. Best (2012) measured only one specific aspect of executive
attention (i.e., interference control) and used more interactive or repetitive video games to manipulate
children’s cognitive engagement. Instead in our study, we examined different aspects of attention and
tailored the PA games in the cognitively enriched program to elicit a specific engagement of executive
functions by matching the principles of neuropsychological executive function tasks (Garon et al., 2008;
Huizinga et al., 2006). The idea subtending our applied study on the cognitive outcomes of PA is that
cognitive engagement in PA should not be considered as a unitary construct. We consider the present
approach to the effects of exercise on cognition as a novel way to capitalize on quality PA, focusing on
cognitive functioning as a relevant mental health outcome of cognitively challenging PA.
A limitation of the study is the absence of a follow-up to control for the stability over time of the
benefits obtained by enhancing the cognitive challenges of the movement tasks in PA. To inform policy
development, more prospective field research is needed that joins measures of motor and cognitive
development to evaluate the goodness of quality PA interventions underpinned by sound theoretical
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 23
framework. The results could help re-focus actual guidelines for PA prescription for children,
grounding them not only on evidence of a dose-response relationship in the physiological domain, but
also on evidence of a ‘quality-response relationship’ in the cognitive domain (Pesce, 2012).
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 24
References
Ahn, S, Fedewa, A. L. (2011). A meta-analysis of the relationship between children’s physical activity
and mental health. Journal of Pediatric Psychology, 36, 385-397.
American Psychiatric Association (2000). Diagnostic and statistical manual of mental disorders (fourth
ed.). Washington, DC, USA: American Psychiatric Association.
Best, J. (2010). Effects of physical activity on children’s executive function: contributions of
experimental research on aerobic exercise. Developmental Review, 30, 331-351.
Best, J. (2012). Exergaming immediately enhances children’s executive function. Developmental
Psychology, 48, 1501–1510.
Biddle, S. J. H. & Asare, M. (2011). Physical activity and mental health in children and adolescents: a
review of reviews. British Journal of Sports Medicine, 45, 886–895.
Budde, H., Voelcker-Rehage, C., Pietraßyk-Kendziorra, S., Ribeiro, P., & Tidow, G. (2008). Acute
coordinative exercise improves attentional performance in adolescents. Neuroscience Letters,
441, 219-223.
Carey, J. R., Bhatt, E., & Nagpal, A. (2005). Neuroplasticity promoted by task complexity. Exercise and
Sport Sciences Review, 33, 24-31.
Croce, R. V., Horvat, M., & McCarthy, E. (2001). Reliability and concurrent validity of the movement
assessment battery for children. Perceptual and Motor Skills, 93, 275-280.
Crova, C., Struzzolino, I., Marchetti, R., Masci, I., Vannozzi, G., Forte, R., & Pesce, C. (resubmitted
after minor revisions). Benefits of cognitively challenging physical activity in overweight
children. Journal of Sports Sciences.
Das, J. P., Naglieri, J. A., & Kirby, J. R. (1994). Assessment of cognitive processes: the PASS theory of
intelligence. Needham Heights, MA: Allyn and Bacon.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 25
Davis, C. L., Tomporowski, P. D., Mc Dowell, J. E., Austin, B. P., Miller, P. H., Yanasak, N.
E.,…Naglieri, J. A. (2011). Exercise improves executive function and achievement and alters
brain activation in overweight children: a randomized, controlled trial. Health Psychology, 30, 91-
98.
Diamond, A. (2000). Close interrelation of motor development and cognitive development and of the
cerebellum and prefrontal cortex. Child Development, 71, 44-56.
Diamond, A., & Lee, K. (2011). Interventions shown to aid executive function development in children
4 to 12 years old. Science, 333, 954-969.
Dolmann, J., Norton K., Norton L. (2005). Evidence for the secular trends in children's physical activity
behavior. British Journal of Sports Medicine, 39, 892-897.
Dwyer, G., Baur, L. A., & Hardy, L. L. (2009). The challenge of understanding and assessing physical
activity in preschool-age children: thinking beyond the framework of intensity, duration and
frequency of activity. Journal of Science and Medicine in Sport, 12, 534-536.
Faigenbaum, A. Stracciolini, A., & Myer, G. D. (2011). Exercise deficit disorder in youth: a hidden
truth. Acta Paediatrica, 100, 1423–1425.
Fisher, A., Boyle, J. M. E., Paton, J. Y., Tomporowski, P., Watson, C., McColl, J. H., & Reilly, J. J.
(2011). Effects of a physical education intervention on cognitive function in young children:
randomized controlled pilot study. BMC Pediatrics, 11:97.
Gallotta, M. C., Guidetti, L., Franciosi, E., Emerenziani, G. P., Bonavolontà, V., & Baldari, C. (2012).
Effects of varying type of exertion on children’s attention capacity. Medicine & Science in Sports
& Exercise,44, 550-555.
Garon, N., Bryson, S., & Smith, I. M. (2008). Executive function in preschoolers: a review using an
integrative framework. Psychological Bulletin, 134, 31-60.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 26
Guadagnoli M. A., Lee T. D. (2004). Challenge point: a framework for conceptualizing the effects of
various practice conditions in motor learning. Journal of Motor Behavior, 36, 212-224.
Henderson, S.E., & Sudgen, D.A. (1992). Movement assessment battery for children. London, UK: The
Psychological Corporation. [Italian version (edited by Eu. Mercuri & El. Mercuri): Movement
ABC—Batteria per la valutazione motoria del bambino, 2000. Firenze (Italy): Giunti O.S.].
Hill, L., Williams, J. H. G., Aucott, L., Milne, J., Thomson, J., Greig, J,…Mon-Williams, M. (2010).
Exercising attention within the classroom. Developmental Medicine & Child Neurology, 52, 929-
934.
Hillman, C. H., Erickson, K. I., & Kramer, A. F. (2008). Be smart, exercise your heart: exercise effects
on brain and cognition. Nature Review Neuroscience, 8, 58-65.
Hillman, C. H., Pontifex, M. B., Raine, L. B., Castelli, D. M., Hall, E. E., & Kramer, A. F. (2009). The
effect of acute treadmill walking on cognitive control and academic achievement in preadolescent
children. Neuroscience, 159, 1044–1054.
Huizinga, M., Dolan, C. V., & van der Molen, M. W. (2006). Age-related change in executive function:
developmental trends and a latent variable analysis. Neuropsychoogia, 44, 2017-2036.
Kirby, A., & Sudgen, D. A. (2007). Children with developmental coordination disorders. Journal of the
Royal Society of Medicine, 100, 182-186.
Kirk, D. (2005). Physical education, youth sport and lifelong participation: the importance of early
learning experiences. European Physical Education Review, 11, 239-255.
Kowalski, K. C., Crocker, P. R. E., & Donen, R. M. (2004). The Physical Activity Questionnaire for
Older Children (PAQ-C) and Adolescents (PAQ-A) Manual. Canada: College of Kinesiology
University of Saskatchewan.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 27
Kristensen, P. L., Moeller, N. C., Korsholm, L., Kolle, E., Wedderkopp, N., Froberg, K., & Andersen,
L. B. (2010). The association between aerobic fitness and physical activity in children and
adolescents: the European youth heart study. European Journal of Applied Physiology, 110, 267–
275.
Kubesch, S., & Walk, L. (2009). Körperliches und kognitives Training exekutiver Funktionen in
Kindergarten und Schule [Physical and cognitive training of executive functions in preschool and
school]. Sportwissenschaft 39, 309-317.
Miyahara, M., Yamagichi, M., Green, C. (2008). A review of 326 children with developmental and
physical disabilities, consecutively taught at the movement development clinic: prevalence and
intervention outcomes of children with DCD. Journal of Developmental and Physical
Disabilities, 20, 353-363.
Naglieri, J.A., & Das, J.P. (1997). Cognitive Assessment System. Itaca, IL: Riverside Publishing. [Italian
version (edited by S. Taddei): CAS Das-Naglieri Cognitive Assessment System - Una misura
dell'intelligenza basata sul modello dei processi cognitivi PASS, 2005. Firenze (Italy): Giunti
O.S.]
Pennequin, V, Sorel, O., & Fontaine, R. (2010). Motor planning between 4 and 7 years of age: changes
linked to executive functions. Brain and Cognition, 74, 107–111.
Pesce C. (2009). An integrated approach to the effect of acute and chronic exercise on cognition: the
linked role of individual and task constraints. In T. McMorris, P.D. Tomporowski, & M.
Audiffren (Eds.), Exercise and cognitive function (pp. 213-226). West Sussex: Wiley and Sons.
Pesce, C. (2012). Shifting the focus from quantitative to qualitative exercise characteristics in exercise
and cognition research. Journal of Sport and Exercise Psychology, 34, 766 – 786.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 28
Pesce, C., Crova, C., Cereatti, L., Casella, R., & Bellucci, M. (2009). Physical activity and mental
performance in preadolescents: effects of acute exercise on free-recall memory. Mental Health
and Physical Activity, 2, 16–22.
Raczek, J. (2002). Entwicklungsveraenderungen der motorischen Leistungsfaehigkeit der Schuljugend
in drei Jahrzehnten (1965-1995) [Changes in motor capability development of school children
during three decades (1965-1995)]. Sportwissenschaft, 32, 201-216.
Rakison, D. H., & Woodward, A. L.(2008). New perspectives on the effects of action on perceptual and
cognitive development. Developmental Psychology, 44, 1209–1213.
Rink, J.E. (2006). Teaching physical education for learning (5th ed.). Boston: McGraw Hill.
Roth, K., Ruf, K., Obinger, M., Mauer, S., Ahnert, J., Schneider, W, … Hebestreit, H. (2010). Is there a
secular decline in motor skills in preschool children? Scandinavian Journal of Medicine and
Science in Sports, 20, 670–678.
Sergeant, J. A., Piek, J. P., & Oosterlaan, J. (2005). ADHD and DCD: A relationship in need of
research. Human Movement Science
Shea, J., & Morgan, R. (1979). Contextual interference effects on the acquisition, retention, and transfer
of a motor skill. Journal of Experimental Psychology: Human Learning and Memory, 5, 179-187.
Singh, A., Uijtdewilligen, L., Twisk, J. W. R., van Mechelen, W., & Chinapaw, M. J. M. (2012).
Physical activity and performance at school. A systematic review of the literature including
a methodological quality assessment. Archives of Pediatric and Adolescent Medicine, 166, 49-55.
Strong, W. B., Malina, R. M., Blimkie, C. J. R., Daniels, S. R., Dishman, R. K., Gutin, B., … &
Trudeau, F. (2005). Evidence based physical activity for school-age youth. The Journal of
Pediatrics, 146, 732-737.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 29
Sudgen, D. (2007). Current approaches to intervention in children with developmental coordination
disorder. Developmental Medicine and Child Neurology, 49, 467-471.
Thomas, M. S. C. & Johnson, M. H. (2008). New advances in understanding sensitive periods in brain
development. Current Directions in Psycholoogical Science, 17, 1-5.
Tomkinson G. R., Leger, L. A., Olds, T. S. & Carzola, G. (2003). Secular trend in the performance of
children and adolescent (1980-2000): an analysis of 55 studies of the 20m shuttle run test in 11
countries. Sports Medicine, 33, 285-300.
Tomporowski, P. D., Davis, C. L., Miller, P. H., & Naglieri, J. A. (2008). Exercise and children’s
intelligence, cognition, and academic performance. Educational Psychology Review, 20, 111-131.
Tomporowski, P. D., Lambourne, K., Okumura, M. S. (2011). Physical activity interventions and
children's mental function: An introduction and overview. Preventive Medicine, 52, 3-9.
Tomporowski, P. D., McCullick, B. A., & Horvat, M. (2010). Role of contextual interference and
mental engagement on learning. New York: Nova Science Publishers, Inc.
Tsai, C.-L. (2009). The effectiveness of exercise intervention on inhibitory control in children with
developmental coordination disorder: Using a visuospatial attention paradigm as a model.
Research in Developmental Disabilities, 30, 1268–1280.
Tsiotra, G. D., Flouris, A. D., Koutedakis, Y., Faught, B. E., Nevill, A. M., Lane, A. M., & Skenteris,
N. (2006). A comparison of Developmental Coordination Disorder prevalence rates in Canadian
and Greek children. Journal of Adolescent Health, 39, 125–127.
Vandorpe, B., Vandendriessche, J., Lefevre, J., Pion, J., Vaeyens, R., Matthys, S., … Lenoir, M.
(2011). The Körperkoordinations Test für Kinder: reference values and suitability for 6–12-year-
old children in Flanders Scandinavian Journal of Medicine and Science in Sports, 21, 378–388.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 30
Veitch, J., Salmon, J., & Ball, K. (2009). The validity and reliability of an instrument to assess
children’s outdoor play in various locations. Journal of Science and Medicine in Sport, 12, 579–
582.
Vickers, J. N. (2007). Perception, cognition and decision training. The quiet eye in action. Champaign,
IL : Human Kinetics (pp. 179-194).
Wang, G.Y., Pereira, B., & Mota, J. (2005). Indoor physical education measured by heart rate monitor:
a case study in Portugal. Journal of Sports Medicine and Physical Fitness, 45, 171-177.
Wilson, P.H. (2005). Practitioner review: approaches to assessment and treatment of children with
DCD: an evaluative review. Journal of Child Psychology and Psychiatry, 46, 806–823.
Wilson, M. R., Miles, C. A., Vine, S. J., Vickers, J. N. (2013). Quiet eye distinguishes children of high
and low motor coordination abilities. Medicine and Science in Sports and Exercise, 45, 1144-
1151.
Wulf, G., & Shea, C. H. (2002). Principles derived from the study of simple skills do not generalize to
complex skill learning. Psychonomic Bulletin & Review, 9, 185-211.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTRunning head: COGNITIVELY OPTIMAL CHALLENGE POINT IN PA FOR CHILDREN 31
Figure Captions
Figure 1. Pre-to-post intervention improvements (pre-post delta) in Expressive Attention (left) and
Receptive Attention (right) in 5 to 10 year-old children as a function of PA intervention type and motor
developmental level.
Acknowledgements
We thank the Guest Editor and two anonymous reviewers for helpful and insightful comments on a
previous version of the manuscript.
This research has received financial support by the Advanced Distribution S.p.A.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
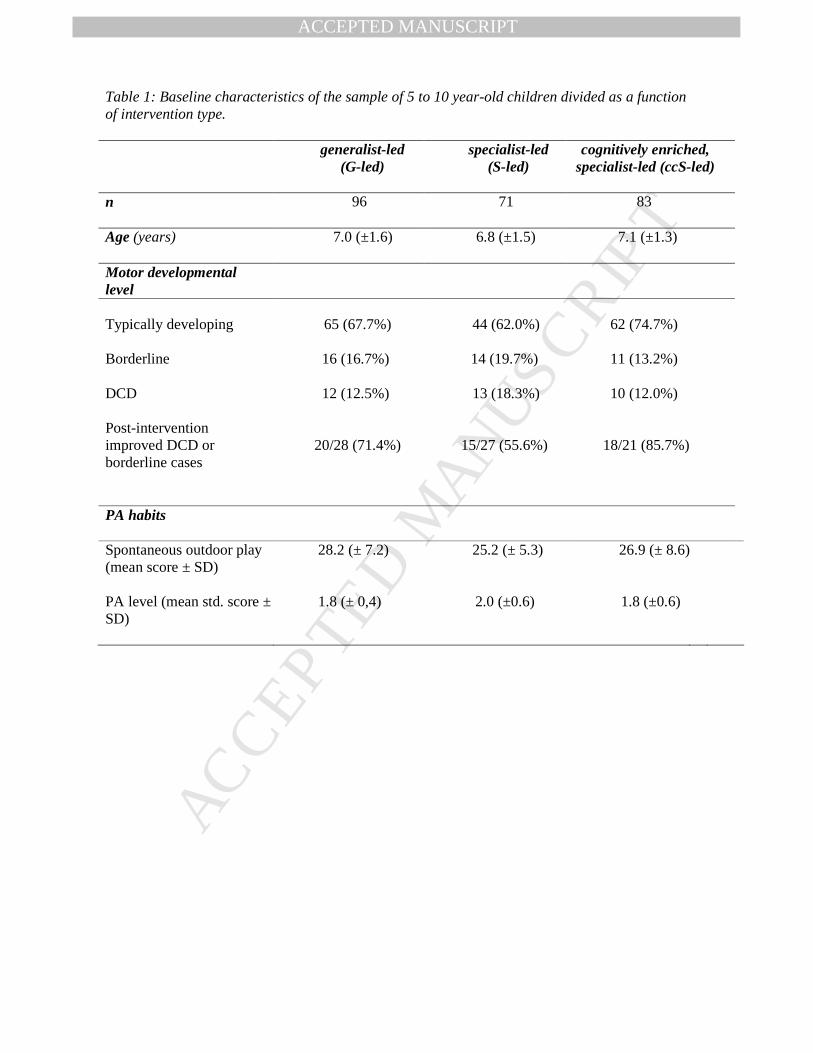
Table 1: Baseline characteristics of the sample of 5 to 10 year-old children divided as a function of intervention type.
generalist-led (G-led)
specialist-led (S-led)
cognitively enriched, specialist-led (ccS-led)
n 96 71 83
Age (years) 7.0 (±1.6) 6.8 (±1.5) 7.1 (±1.3)
Motor developmental level
Typically developing
65 (67.7%)
44 (62.0%)
62 (74.7%)
Borderline 16 (16.7%) 14 (19.7%) 11 (13.2%)
DCD 12 (12.5%) 13 (18.3%) 10 (12.0%) Post-intervention improved DCD or borderline cases
20/28 (71.4%) 15/27 (55.6%)
18/21 (85.7%)
PA habits
Spontaneous outdoor play (mean score ± SD)
28.2 (± 7.2) 25.2 (± 5.3) 26.9 (± 8.6)
PA level (mean std. score ± SD)
1.8 (± 0,4) 2.0 (±0.6) 1.8 (±0.6)
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
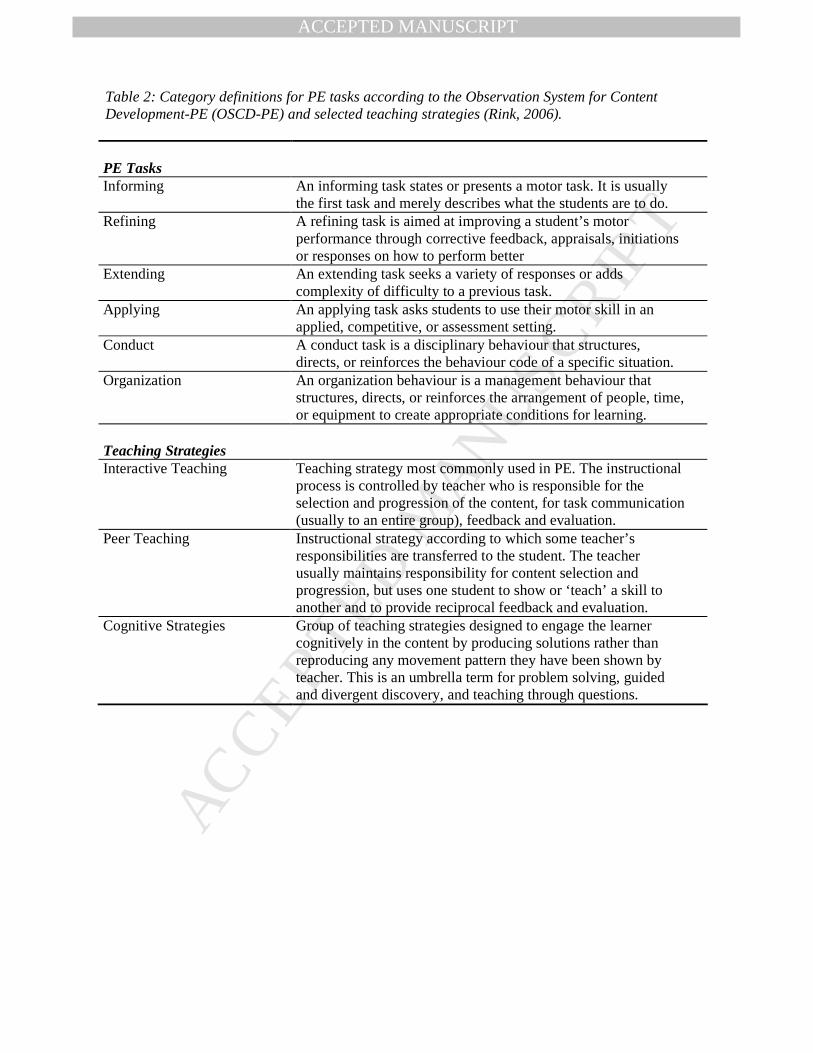
Table 2: Category definitions for PE tasks according to the Observation System for Content Development-PE (OSCD-PE) and selected teaching strategies (Rink, 2006). PE Tasks
Informing
An informing task states or presents a motor task. It is usually the first task and merely describes what the students are to do.
Refining A refining task is aimed at improving a student’s motor performance through corrective feedback, appraisals, initiations or responses on how to perform better
Extending
An extending task seeks a variety of responses or adds complexity of difficulty to a previous task.
Applying An applying task asks students to use their motor skill in an applied, competitive, or assessment setting.
Conduct A conduct task is a disciplinary behaviour that structures, directs, or reinforces the behaviour code of a specific situation.
Organization An organization behaviour is a management behaviour that structures, directs, or reinforces the arrangement of people, time, or equipment to create appropriate conditions for learning.
Teaching Strategies
Interactive Teaching Teaching strategy most commonly used in PE. The instructional process is controlled by teacher who is responsible for the selection and progression of the content, for task communication (usually to an entire group), feedback and evaluation.
Peer Teaching Instructional strategy according to which some teacher’s responsibilities are transferred to the student. The teacher usually maintains responsibility for content selection and progression, but uses one student to show or ‘teach’ a skill to another and to provide reciprocal feedback and evaluation.
Cognitive Strategies Group of teaching strategies designed to engage the learner cognitively in the content by producing solutions rather than reproducing any movement pattern they have been shown by teacher. This is an umbrella term for problem solving, guided and divergent discovery, and teaching through questions.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
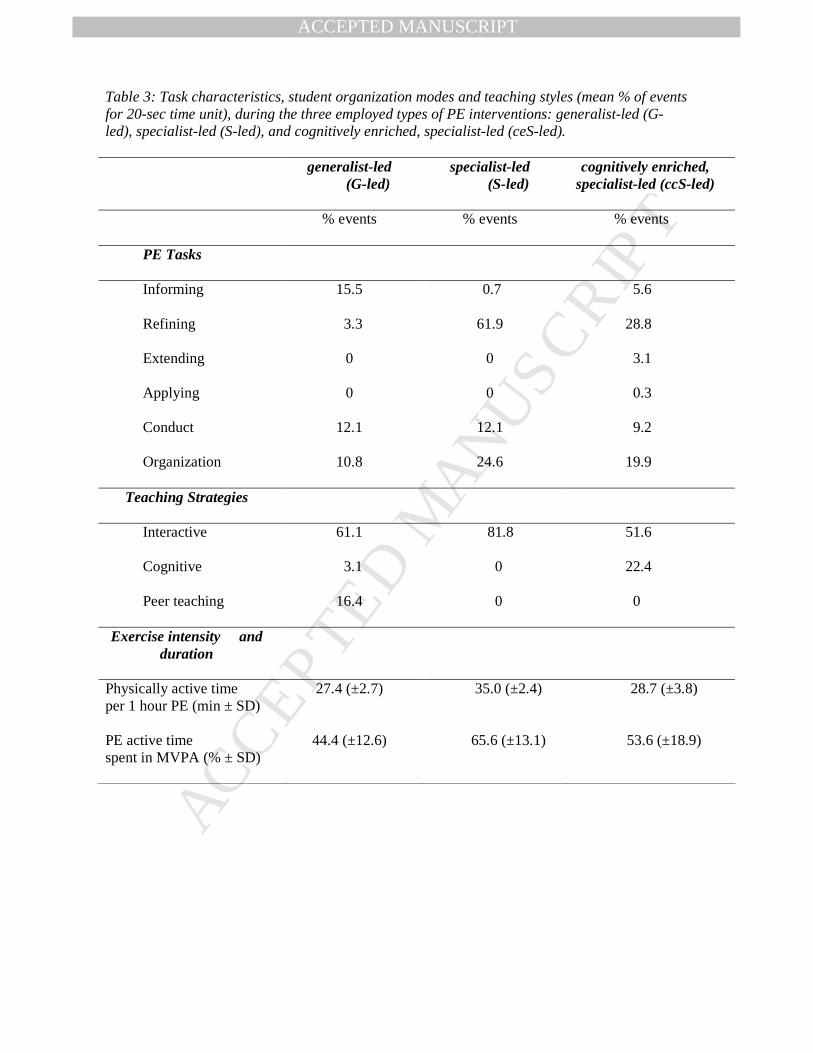
Table 3: Task characteristics, student organization modes and teaching styles (mean % of events for 20-sec time unit), during the three employed types of PE interventions: generalist-led (G-led), specialist-led (S-led), and cognitively enriched, specialist-led (ceS-led).
generalist-led (G-led)
specialist-led (S-led)
cognitively enriched, specialist-led (ccS-led)
% events % events % events
PE Tasks
Informing 15.5 0.7 5.6
Refining 3.3 61.9 28.8
Extending 0 0 3.1
Applying 0 0 0.3
Conduct 12.1 12.1 9.2
Organization 10.8 24.6 19.9
Teaching Strategies
Interactive 61.1 81.8 51.6
Cognitive 3.1 0 22.4
Peer teaching 16.4 0 0
Exercise intensity and duration
Physically active time per 1 hour PE (min ± SD)
27.4 (±2.7) 35.0 (±2.4) 28.7 (±3.8)
PE active time spent in MVPA (% ± SD)
44.4 (±12.6) 65.6 (±13.1) 53.6 (±18.9)
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figure 1
-4
-2
0
2
4
6
8
typically developing
borderline DCD
typically developing
borderline DCD
pre-
po
st d
elta
generalist-led
specialist-led
cognitively enriched specialist-led
*
*
*
Expressive Attention Receptive Attention
Related Documents











