Principles of Acid- Base Physiology Mazen Kherallah, MD, FCCP Internal Medicine, Infectious Disease and Critical Care Medicine

sdfds
Mar 21, 2016
englishdfdsdfdfdf
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Principles of Acid-Base Physiology
Mazen Kherallah, MD, FCCPInternal Medicine, Infectious Disease
and Critical Care Medicine
Note
• Acids are compound that are capable of donating a H+
• Bases are compound that are capable of accepting a H+
• When an acid HA dissociates, it yields a H+ and its conjugate base (anion, A-)
• HA H+ + A-

Valence
• The number of charges a compound or ion bears in solution, expressed in mEq/L.
• The term mEq reflects the number of charges or valences.
• Therefore multiply mmol by the valence to obtain mEq.
• Valence is especially important for albumin, which has a large valence on each molecule.
Characteristics of H+
• The free H+ is tiny and must be kept so for survival
• A very large accumulation of H+ may kill by binding to proteins in cells and changing their charge, shape, and possibly their function
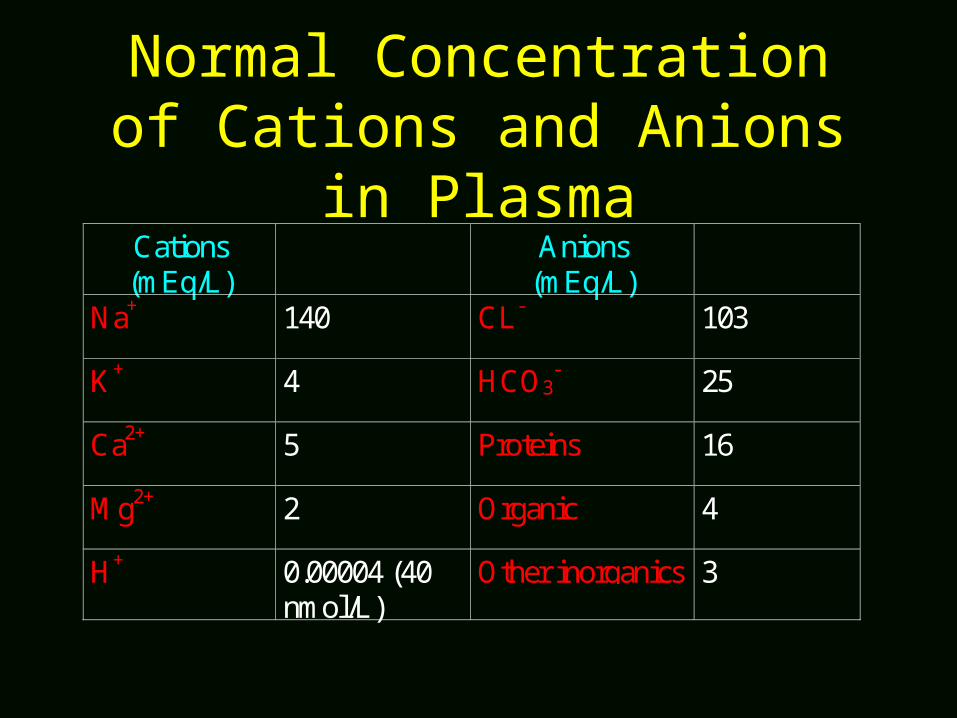
Normal Concentration of Cations and Anions in Plasma
Cations(mEq/L)
Anions(mEq/L)
Na+ 140 CL- 103
K+ 4 HCO3- 25
Ca2+ 5 Proteins 16
Mg2+ 2 Organic 4
H+ 0.00004 (40nmol/L)
Other inorganics 3

Number of H+ in the body• ECF: 15 L X 40 nmol/L = 600 nmol• ICF 30 L X 80 nmol/L = 2400 nmol• Total free H+ in the body is close to 3000 nmol/L• Close to 70.000.000 nmol of H+ is formed and
consumed daily• Affinity of H+ for chemical groups on organic and
inorganic compounds determine whether H+ will be bound or remain free (gastric)

Compartmental [H+]
ECF 40 nmol/L
ICF 80-100 nmol/L
Urine 10,000 nmol/L
Gastric fluid 70 mmol/L

Gastric [H+]• Very high concentration is needed to initiate digestion• The anion secreted by the stomach along with [H+] is Cl-
• Cl- will not bind H+ because HCl dissociates completely in aqueous solution and there are no major buffers in the gastric fluid
• H+ bind avidly when they come in contact with ingested proteins.• Binding of H+ makes the protein much more positively charged
and alters its shape so that pepsin can gain access to the sites it will hydrolyze in that protein.

Intracellular Buffers
• Binding to Proteins• Buffered by inorganic phosphate

Intracellular BuffersInorganic Phosphate
HPO42-
pH= pK + log ---------- H2PO4
-
HPO42-: divalent inorganic phosphate ion
H2PO4-: monovalent dihydrogen inorganic phosphate ion
pK for inorganic phosphate is close to 6.8

pH of Different Compartments
PH Compartment Ratio ofHPO4
2-/H2PO4-
7.4 ECF 4/1 (0.62)
7.1 ICF 2/1 (0.3)
5.8 Urine 1/10 (-1)

Physiology of Phosphate Buffers
Compartment TotalInorganicPhosphate
% as ofH2PO4
-Equation
ECF 1 mmol/L 20% H+ +HPO42- H2PO4
-
ICF 4-5 mmol/L 33% H+ +HPO42- H2PO4
-
Urine 30 mmol/L 90% H+ +HPO42- H2PO4
-

Definition of Metabolic Process
• A metabolic process starts with either dietary or stored fuels and ends with ATP or an energy store (glycogen, triglyceride)
• If part of the pathway generates H+ and is intimately linked to another part that removes H+, both parts can be ignored from an acid-base perspective
No Change in Net ChargeNeutrals to Neutrals
• Glucose Glycogen + CO2 + H2O• TG CO2 + H2O• Alanine Urea + Glucose
No Net Production or Removal of H+
At the Cellular Level
• H+ is formed when ATP is hydrolyzed to perform biologic work: reabsorb Na+
– ATP4- ADP3- + Pi2- + H+
• As soon as ATP is regenerated in the mitochondria of that cell, H+ are removed– ADP3- + Pi
2- + H+ ATP4-

No Net Production or Removal of H+
Multiple Organ Process
• Adipocyte: – TG 3 Palmitate- + 3 H+ + Glycerol
• Liver:– 3 Palmitate- + 3 H+ + 18 O2 12 ketoacid
anions + 12 H+
• Brain:– 12 ketoacid anions + 12 H+ CO2 + H2O + ATP

Reactions that Yield H+
• Glucose Lactate- + H+
• Fatty acid 4 Ketoacid anions + 4 H+
• Cysteine Urea + CO2 + H2O + SO42-
+ 2H+
• Lysine+ Urea + CO2 + H2O + H+
Reactions that Remove H+
• Lactate- + H+ Glucose• Citrate 3- + 3H+ CO2 + H2O• Glutamine Glucose + NH4+ + CO2
+ H2O + HCO3-

Dietary Acid-Base ImpactNutrient Product H+
(mEq/day)Reactions generating H+
Sulfur-containing amino acids: Cysteine/cystine, methionine
H+ 70
Cationic amino acids: Lysine, arginine, histidine
H+ 140
Organic phosphates HPO42-+H+ 30
Reactions removing H+
Anionic amino acids: Glutamate, aspartate
HCO3- -110
Organic anions (citrate3-) HCO3- -60
Posphate excretion H2PO4- -30
Net total H+ load to be excreted asNH4+
40

Sulfur-containing Amino AcidsCysteine/Cystine and Methionine
• Sulfur-containing amino acids can be oxidized to yield the terminal anion SO4
2- plus neutral end-product (glucose, urea, CO2 and and H2O)
• Because the affinity SO42- of for H+ is so low (SO4
2- has a very low pK), SO4
2- cannot help in removing H+ by urinary excretion• Hence other ways are needed to remove these H+ ( renal
excretion of NH4+)
• For each SO42- mEq of that accumulate or excreted without
NH4+, H+ accumulate

Cationic Amino AcidsLysine, Arginine, and Histidine
• Are metabolized to neutral end-products plus H+
• These H+ requires the excretion of NH4+ to prevent accumulation of protons
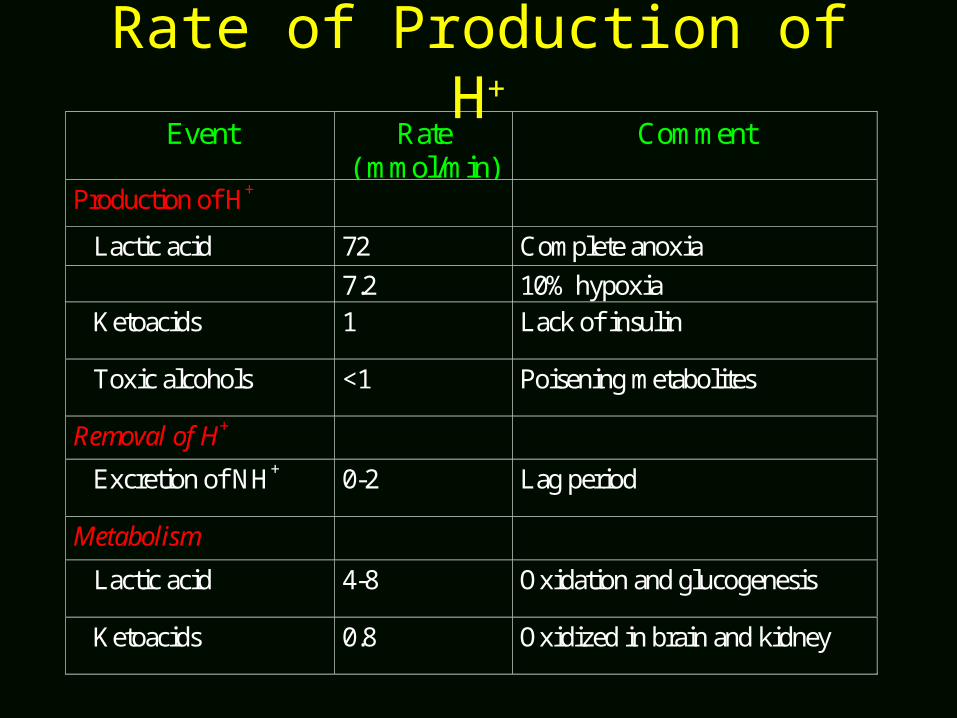
Rate of Production of H+
Event Rate( mmol/min)
Comment
Production of H+
Lactic acid 72 Complete anoxia7.2 10% hypoxia
Ketoacids 1 Lack of insulin
Toxic alcohols <1 Poisening metabolites
Removal of H+
Excretion of NH+ 0-2 Lag period
Metabolism
Lactic acid 4-8 Oxidation and glucogenesis
Ketoacids 0.8 Oxidized in brain and kidney

Y E s N o
W as H + p rod u cedat a m u ch fas te rra te th an it w as
rem oved
Y es N o
Is H + accu m ila tin g
R eac tion s th a t p rod u ce H +
Anions are metabolized to neutralproducts almost as fast as they areproduced:
Starvation KetoacidosisL-lactic acid: usual rate
Anions that are produced slowlyand excreted with H+ and NH4+
H2SO4 from proteinsDKAL-lactic acid: liver problemOrganic acids from gut: butyric acid, acetic, and propionicAnions from toxinsNH4 excretionproblem
L-lactic aciddue to low supply of O2: Exercise Shock
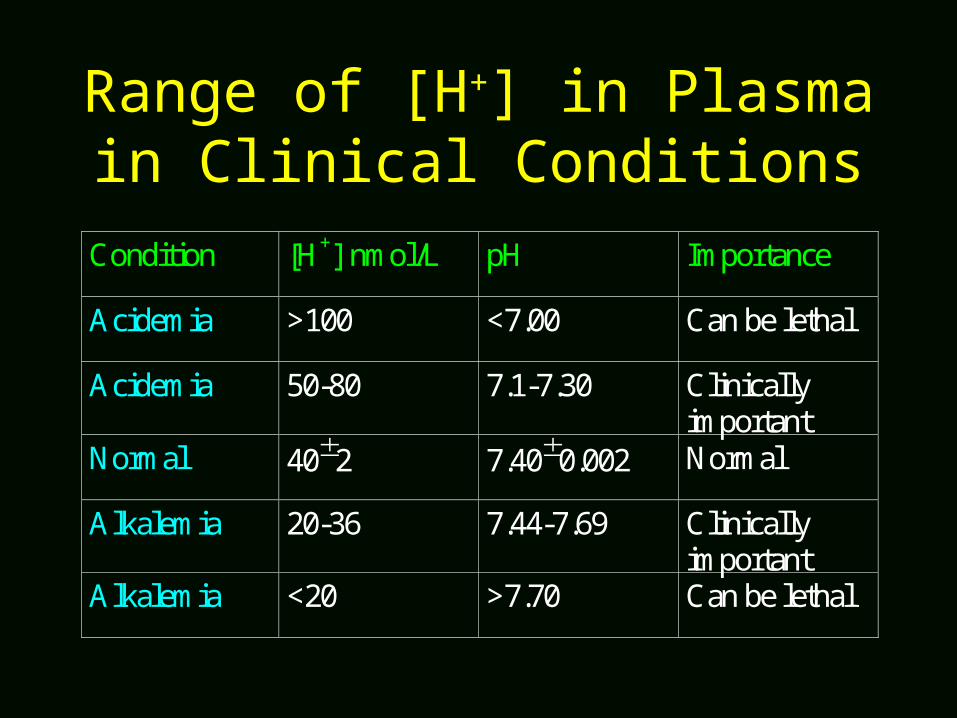
Range of [H+] in Plasma in Clinical Conditions
Condition [H+] nmol/L pH Importance
Acidemia >100 <7.00 Can be lethal
Acidemia 50-80 7.1-7.30 Clinicallyimportant
Normal 402 7.400.002 Normal
Alkalemia 20-36 7.44-7.69 Clinicallyimportant
Alkalemia <20 >7.70 Can be lethal

HCO3-
Fuels H+
CO2
Kidneys
Glutamine NH4+
Lungs
(70 mmol per day)
(Kidney must generate 70 mmol of HCO3 per day)
Generation of New HCO3-
• Each day 70 mmol is derived from the normal oxidative metabolism of dietary constituent and is buffered mainly by bicarbonate buffer system (BBS)
• To achieve acid-base balance, the kidney must generate 70 mmol of new HCO3- to replace the HCO3- consumed by the buffering process
• Should this process fails, the patient will become acidemic
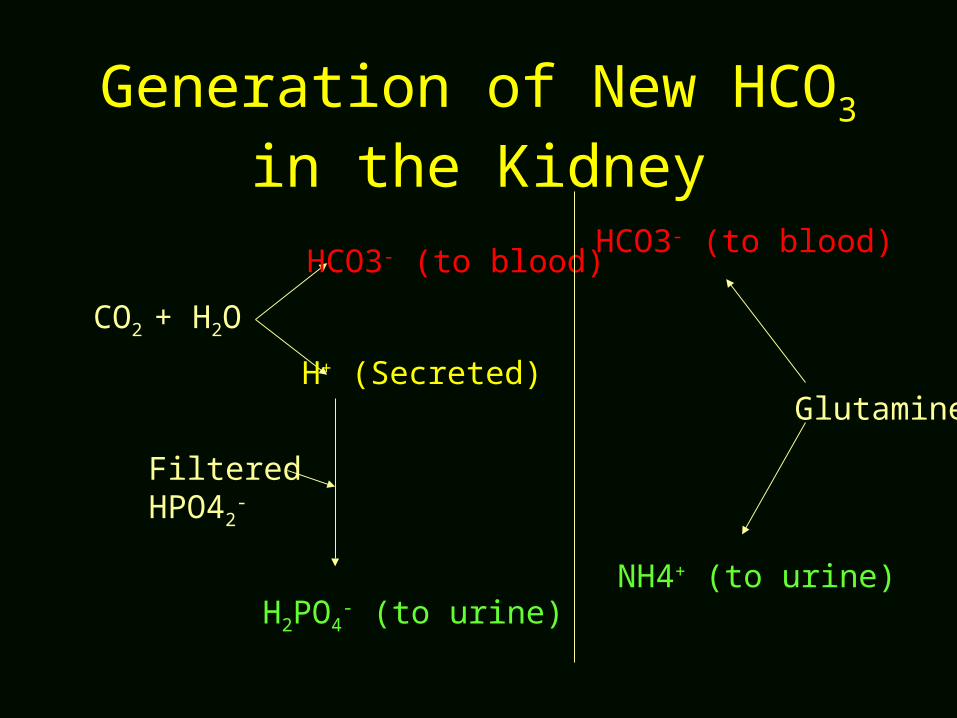
CO2 + H2O
HCO3- (to blood)
H+ (Secreted)
FilteredHPO42
-
H2PO4- (to urine)
Glutamine
NH4+ (to urine)
HCO3- (to blood)
Generation of New HCO3 in the Kidney
Concept
• Buffers work physiologically to keep added H+ from binding to proteins; instead H+ are forced to react with HCO3-
Chemistry of Buffers• Each buffer has its unique dissociation constant (pK),
which determine the range of [H+] at which the buffer is effective
• HAA- + H+
• pH= pK+ log HA/A-• A buffer is most effective at a [H+] or pH the is
equal to its pK• Strong acids have a lower pK, and weak acids have
higher pK.
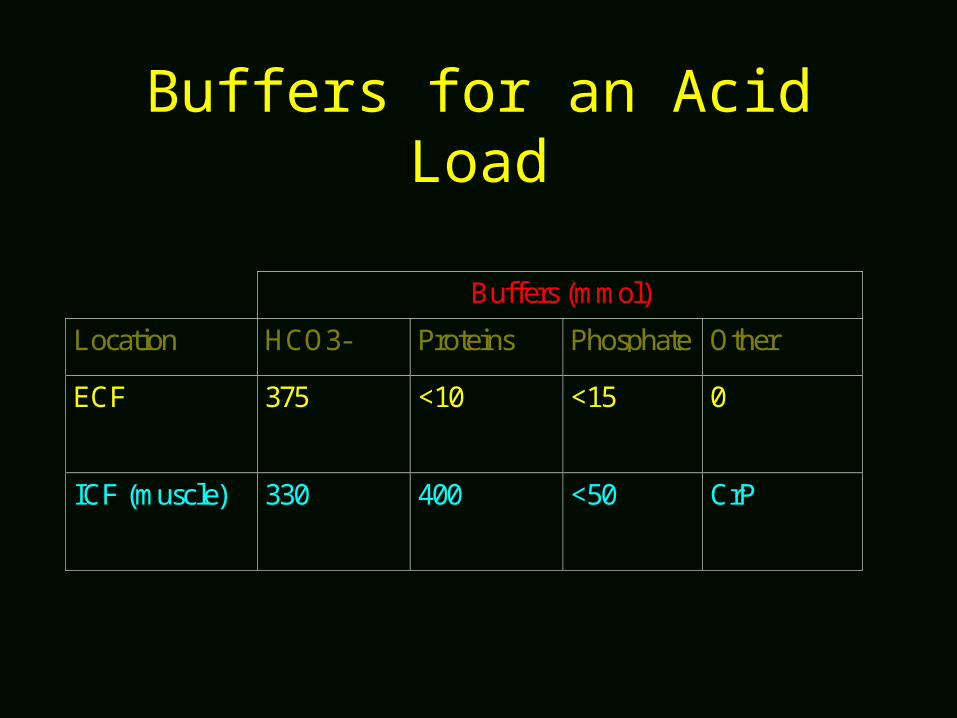
Buffers for an Acid Load
Buffers (mmol)
Location HCO3- Proteins Phosphate Other
ECF 375 <10 <15 0
ICF (muscle) 330 400 <50 CrP
Protein Buffer System
• The major non-BBS buffer is protein in the ICF (imidazole group in histidine)
• When H+ binds to proteins, the charge, shape, and possibly function of proteins may change
• Total content of histidines is close to 2400 mmol in 70-kg individual
• PH of ICF is close to pK of histidine• Only 1200 mmol of histidine are potential H+ acceptors

Bicarbonate Buffer System (BBS)
HCO3-
pH= pK + log ---------- H2CO3
H+ + HCO3- H2CO3 H2O + CO2
Each mmol of HCO3- remove 1 mmol of H+
[H+] = 24 X PCO2/HCO3-

Bicarbonate Buffer System Quantities
• Total content of HCO3- in the ECF is:– 25 mmol/L X 15 = 375 mmol
• Total content of HCO3- in the ICF is:– 13 mmol/L X 30 = 360 mmol
Bicarbonate Buffer System Physiology
• A function of the BBS is to prevent H+ from binding to proteins in the ICF
• The BBS is used first to remove a H+ load, providing that hyperventilation occurs
• The key to the operation of the BBS is the control of the PCO2
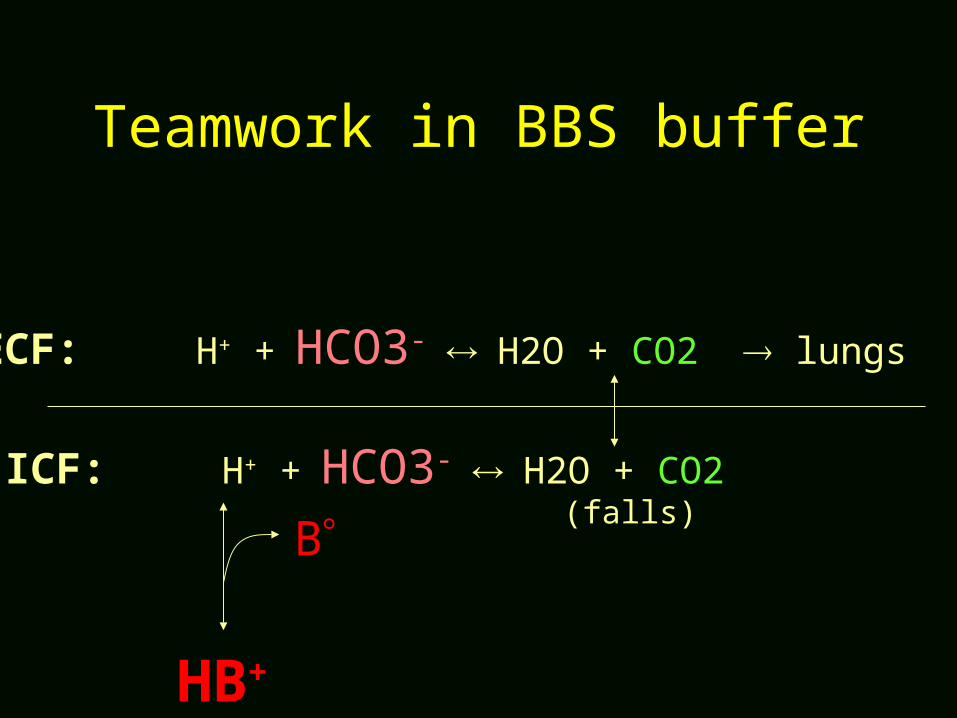
Teamwork in BBS buffer
ECF: H+ + HCO3- H2O + CO2 lungs
ICF: H+ + HCO3- H2O + CO2
HB+
B(falls)

Bicarbonate Buffer SystemImportance of CO2 Removal
Condition [H+](nmol/L)
PH PCO2(mm Hg)
HCO3-
(mmol/L)
Closed system(PCO2 rises)
871 6.06 455 12.5
No change inPCO2
77 7.11 40 12.5
Lower PCO2 52 7.29 27 12.5
Related Documents











