Screening in Disease Detection

Screening in Disease Detection. Natural history of disease Onset of symptoms Usual time of diagnosis Exposure Pathologic changes Stage of susceptibility.
Mar 26, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Screening in Disease Detection

Natural history of disease
Onset ofsymptoms
Usual time ofdiagnosis
Exposure
Pathologicchanges
Stage ofsusceptibility
Stage ofsubclinical
disease
Stage ofclinicaldisease
Stage ofrecovery,
disability ordeath
PRIMARYPREVENTION
SECONDARYPREVENTION
TERTIARYPREVENTION

“Screening is the application of a test to
people who are asymptomatic for the
purpose of classifying a person with respect
to their likelihood of having a particular
disease”
A Key Assumption of Screening Programs:
Early detection will lead to more favorable prognosis


Screening, in and of itself, does not diagnose disease.
• Persons who test positive are referred to physicians for more detailed
assessment
• Physicians determine the presence or absence of disease.
Screening is one of the most practical applications of epidemiology. It’s goal is to promote health and prevent disease.

When is it appropriate to initiate screening programs?
1. When the disease is serious
2. When the prevalence of pre-clinical disease is high
3. When medical care is available and health interventions are known to be effective
4. When failure to screen could be considered unethical

World Health Organization Criterion for Screening
Is it a health problem?
Is there treatment?
Are there facilities in place?
Is it detectable pre-clinically?
Is there a suitable screening test?
Is the screening test acceptable to people?
Is the natural history of disease understood?
Are the costs acceptable?
Wilson JMG, Junger G. (1967) The principles and practice of screening for Disease. Public Health Paper 34: Geneva, Switzerland: World Health Organization

Screening involves:
• Organizing a deployment of public health resources, policies, and procedures
• Defining the target population
• Setting priorities among diseases and conditions
• Choosing effective screening tests

It also involves:
• Assessing the effectiveness of screening procedures and programs
• Adopting practice guidelines to local needs
• Dealing with controversial and conflicting guidelines
• Translating guidelines into programs through public health departments, managed-care organizations, community based coalitions, and workplace coalitions.

Community
Media
Managed care
Health Departments
Universities
SchoolsWorkplaces
Community Based
Organizations(e.g. Churches)
Clinic- Patient- Provider- Community Liaison
Places ofRecreation
Conceptual framework relating screening at the individual, settings, and community levels

When examining a screening test we tend to look most
closely at its
Validity
Reproducibility
Efficacy

How do we judge the validity of a screening test?
We compare the screening test against some “gold standard”
Disease “gold standard”
Test Result Present Absent
Positive true positive false positive
Negative false negative true negative

As a measure of the validity of the test we calculate:
Sensitivity
= Probability that a person having the disease is detected by the test
= P (test positive | they have the disease)
Specificity
= Probability that a person who does not have the disease is classified that way by the test
= P(test negative | they don’t have the disease)

Disease “gold standard”
Test Result Present Absent Total
Positive TP FP all who test +
Negative FN TN all who test -
Total All with All without
Disease Disease
Sensitivity = TP Specificity = TN
TP + FN FP + TN

How do we examine the reproducibility?
We do the tests repeatedly in the same individuals
and calculate measures of:
Intrasubject Variation (Table 4-7 in Gordis)
Interobserver Variation (Figure 4-12 in Gordis)
Overall Percent Agreement
Kappa Statistic

For a measure of the efficacy of the test we use . . .
Positive Predictive Value
= Probability that someone who tests positive for the disease will actually have the disease
= P (have disease | positive test result)
Negative Predictive Value
= Probability that someone who tests positive for the disease will actually
have the disease
= P (don’t have disease | negative test result)

Disease “gold standard”
Test Result Present Absent Total
Positive TP FP all who test +
Negative FN TN all who test -
Total All with All without
Disease Disease
Positive predictive value = TP / TP + FP
Negative predictive value = TN / TN + FN

One of the reasons Positive Predictive Value is used as a measure of efficacy is because it depends on the prevalence of the disease
For a given screening test with sensitivity fixed at X% and specificity fixed at Y%,
if the prevalence then PPV
or
if the prevalence then PPV

For example, for a screening test with sens=99% and spec=95% (Gordis, 1996)
Disease
Prev Test Present Absent Total PPV
1% + 99 495 594 17%
- 1 9,405 9,406 =99/594
Totals 100 9,900 10,000
5% + 495 475 970 51%
- 5 9,025 9,030 =495/970
Totals 500 9,500 10,000

What if we want to screen for a quantitative risk factor?
Blood cholesterol levels Heart Disease
Plasma Glucose levelsDiabetes
Cognitive function Dementia
Body Mass Index Obesity
Blood pressure Hypertension

For quantitative tests, we have to think about screening a little differently
Truly
Diseased
Not
DiseasedTrue Negatives
False Negatives
False Positives
True Positives
“Disease Cutpoint” for screening
Risk factor level
Risk factor level

So what would happen if we lowered the cut off?
Truly
Diseased
Not
DiseasedTrue Negatives
False Negatives
False Positives
True Positives
“Disease Cutpoint”

Some notable features of sensitivity and specificity for a quantitative
test:
Lowering the cutpoint for the screening test will
true positives sensitivity
true negatives specificity
And of course, increasing the cutpoint will have the exact opposite effect.

Given that there will be trade-offs between sensitivity and specificity, how do we decide
which “errors” are more costly?
1. Failing to detect some true cases because of lower sensitivity
or
2. Misclassifying some people as diseased because of lower specificity

It depends . . .
On the prevalence of the disease
On the severity of the disease
On the potential fatality of the disease
On how good the test is
On the acceptability of the test to people

Sensitivity and Specificity for Fibrinogen Levels
00.20.40.60.8
1
1 2 3 4 5 6 7 8 9 10 11
Fibrinogen
Sen
Spec
What’s the most appropriate cutpoint? (What if it’s a marker for a lethal disease?
What its just a health indicator?)

What are other strategies for dealing with this tradeoff?
Use parallel tests
- here a positive result on any one test defines the person as a
probable case
Use serial tests
- here a positive result on a first test are re- evaluated on a second test
- individuals must test positive on both tests to be considered a probable case.

Biases when evaluating a screening program
There are three possible sources of bias when evaluating a screening program that may result in a false picture of its efficacy:
– 1. Volunteer bias
– 2. Lead time bias
– 3. Length time bias

Biases when evaluating a screening program
1. Compliance (volunteer) bias: Volunteers for screening are generally more health conscious/concerned than the general population, apt to assume greater responsibility for their own care, hence, more likely to comply with therapy.

Biases when evaluating a screening program
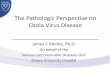
2. Lead time bias
Lead time is the amount of time by which the diagnosis was advanced due to screening. Lead time bias means that survival may erroneously appear to be increased among screen-detected cases simply because the diagnosis was made earlier in the course of the disease.

Fig. 1.—Natural history of disease. Diagram illustrates that preclinical phase begins at onset and ends when signs or symptoms develop. Clinical phase then starts, ending with death. Detectable preclinical phase (DPCP) begins when disease is detectable by a test. Detection (X) during DPCP advances time of diagnosis by duration of lead time.

Fig. 2.—Lead-time bias. Diagram shows that, with screening, time of diagnosis is advanced by lead time provided by positive test result. If earlier diagnosis has no effect on time of death from disease, then survival with testing is equal to survival without testing plus lead time.

Biases when evaluating a screening program
3. Length time bias
Less aggressive forms of a disease are more likely to be picked up in a screening program because they have a longer detectable pre-clinical phase. Less aggressive forms of disease usually have better survival.

Fig. 3.—Diagram shows how probability of detection is related to rate of disease progression. Length of each arrow represents length of detectable preclinical phase, from initial detectability to clinical diagnosis (Dx). Testing at a single moment detects four slowly progressive cases but only two rapidly progressive cases. Cases not detected by test (thin arrows) are diagnosed clinically either before or after time of testing. Thick arrows indicate detected cases.

Prostate Cancer Example

Prostate cancer
It is the second most common form of cancer among men in the United States.
It is also the second leading cause of cancer deaths.
American Cancer Society estimates that 179,300 new cases of prostate cancer were diagnosed in 1999 and 37,000 men died in 1999.
This cancer is most common among men 65 years and older.
http://www.cdc.gov/cancer/prostate/prostate.htm

Prostate cancer
At all ages, African American men
• have the highest incidence of PCA in the world
• diagnosed with the disease at later stages
• die of prostate cancers at higher rates
http://www.cdc.gov/cancer/prostate/prostate.htm

Incidence of Prostate Cancer
Recently, we’ve been better able to detect prostate cancer and hence our estimates of its incidence have increased
http://www.cdc.gov/cancer/prostate/prostate.htm

Death rates for Prostate Cancer
Death rates for African American men is twice what it is for White men.
http://www.cdc.gov/cancer/prostate/prostate.htm

Age-dependent Incidence and Death Rates
Incidence of PCA appears to level off above 70 yrs
but the death rate becomes exponentially worse at that age.
http://www.cdc.gov/cancer/prostate/prostate.htm

Early Detection
The benefits of early detection of prostate cancer
are thought to be the same as for any cancer.
However,
• Little is know about how to prevent the disease
• Scientific evidence is lacking about whether screening reduces deaths
• Evidence is lacking about whether current treatments really prolong men’s
lives.

Two commonly used methods for detecting prostate cancer
1. Digital rectal examination (DRE)
This has been used for years. . . But its ability to detect PCA is limited
• It can’t detect some small tumors
• It can’t distinguish between benign tumors and cancer

2. Prostate-specific antigen (PSA) test
PSA is an enzyme that increases with age and because of prostate abnormalities
• Its now used widely but medical consensus hasn’t been reached on its utility
• It also cannot distinguish between benign and cancerous tumors.

What are the treatment alternatives?
Radical prostatectomy
Radiation therapy
Watchful waiting

Criterion Prostate Cancer
Is it a health problem? Yes
Is there treatment? Probably
Are there facilities in place? Yes
Is it detectable pre-clinically? Yes
Is there a suitable screening test? Yes
Is the screening test acceptable? Yes
Is the disease understood?Partially
Are the costs acceptable?Possibly
Is continuous screening set up?PrematureMeyer F, Fradet Y. Clinical basics:Prostate Cancer:4. Screening. Can Med Assoc J; 1998 159(8):968-972

Data from American Cancer Society’s National Prostate Cancer Detection Project and the European Randomized Study of Screening for Prostate Cancer
Prostate Cancer
Test result Present AbsentTotal
Positive 197 1169 1366
Negative 29 5828 5857
Total 226 6997 7223
Positive test result = a PSA level >4ng/ml and DRE evidence
False negatives detected by biopsy after transurethal ultrasonography yielded abnormal findings.
Meyer F, Fradet Y. Clinical basics:Prostate Cancer:4. Screening. Can Med Assoc J; 1998 159(8):968-972

Data from Canadian National Breast Screening Study
Breast Cancer
Test result Present AbsentTotal
Positive 142 3,2303,372
Negative 15 16,324 16,339
Total 226 19,5554 19,711
Positive test result = a suspicious finding by mammogram and/or physical exam
False negatives are those in whom breast cancer was discovered in 1st yr follow-up
Meyer F, Fradet Y. Clinical basics:Prostate Cancer:4. Screening. Can Med Assoc J; 1998 159(8):968-972

Comparison of Breast and Prostate Cancer
Prostate BreastCancer Cancer
Sensitivity,% 87.2 90.4Specificity, % 83.3 83.5Positive test, % 18.9 17.1Prevalence, % 3.1 0.8Positive predictive 14.4 4.2value, %
Meyer F, Fradet Y. Clinical basics:Prostate Cancer:4. Screening. Can Med Assoc J; 1998
159(8):968-972

Other issues related to Screening Programs:
• Evaluating the effectiveness of the program
• Defining High Risk subgroups
- Those subgroups for whom the prevalence of asymptomatic disease is expected to be
higher
• Ethical considerations
- Who should be offered the test?
- Who should have access to the results?

Selected Examples of Prevention Effectiveness
Annual US % of personsPrevention Undesired Incidence without Prevention Economic at Risk CoveredType* Outcome Intervention Method % Effectiveness Analysis by Method
Primary Measles 4,000,000 Vaccination 95-98 $16.85 per By age 2, 50-80%;
case prevented by age 6, 98%
Secondary Breast cancer 50,000 Mammography 20-70 $45K to $165K per 15-38 deaths screening year of life saved
Tertiary Blindness from 24,000 Retinal screening, 50 $100 per year of 60-80 Diabetes treatment vision saved
* Primary prevention = directed at susceptible persons before they develop a particular disease (risk factor reduction); Secondary prevention = directed at persons who are symptomatic but who have developed biologic changes (early detection and treatment); Tertiary prevention = directed at preventing disability in persons who have symptomatic disease (prevent complications and rehabilitation).
SOURCE: Thacker et. Al. (1994)

Group Health Cooperative of Puget Sound’s Breast Cancer Risk Algorithm and Screening Protocol
Mammography Risk Relative PercentageFrequency Level Risk-Level Criteria Risk WomenAnnual
Every 2 Years
Every 3 Years
Not Recommended
1
2
3
4
Previous breast cancer or atypia on biopsy results; at least 2 first-degree relatives with breast cancer
One first-degree relative with breast cancer; >50 years of age and >2 MRF’s
>50 years of age and >1 MRF; or >50 years of age and > MRF
<50 years of age and no MRF
4-14
1.9-3.5
1.2-1.9
1.0
Source: Taplin et al. (1990)
1
15
66
17

Conditions for Which Screening Is Recommended, USPSTF 1996
Health Outcome Test(s) Populations(s) Age Group (years)
HIV
HbgSS/PKU/
Hypothyroidism
Anemia
Lead poisoning
Rubella
Tuberculosis
Hearing
Vision
Lab
Hgb/Phenylalanine
T4&TSH
Hgb/Hct
Blood lead
Lab
PPD
--
--
HR2/HR3
General/General
general
HR1/HR/P (female)HR7
General (female)
HR1/HR3/HR6/HR7
General
General
0-10/11+
Birth/Birth
Birth
0-10/11+
0-10
11-24, 25-64
65+/0-24/25-64
65+
0-10, 65+
Source: U.S. Preventive Services task Force [USPSTF] (1996)

More Conditions for Which Screening Is Recommended
Health Outcome Test(s) Populations(s) Age Group (years) Obesity
CVD/HBP
CVD
Injury/Liver disease
Colorectal cancer
Breast cancer
Cervical cancer
Chlamydia
Gonorrhea
Syphilis
Height/Weight
Blood pressure
Cholesterol
Alcohol overuse
Fecal Occult Blood TestSigmoidoscopy
Mammography/Clinical Breast Exam
Pap Smear
Lab
Lab
Lab
General
General
General/HR6
General
General
General
General
General/HR4
HR2
HR1/HR9
All
All
25-64/65+
11+
25+
50+ (female)
11+ (female)
11-24/11-64
11-24, 25-64
11-64/65+
Source: U.S. Preventive Services task Force [USPSTF] (1996)

Related Documents