Screening Guidelines and Treatment Options for Abdominal Aortic Aneurysms Allen Jeremias, MD Division of Cardiology Beth Israel Deaconess Medical Center Harvard Medical School

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Screening Guidelines and Treatment Options for Abdominal
Aortic Aneurysms
Allen Jeremias, MDDivision of Cardiology
Beth Israel DeaconessMedical Center
Harvard Medical School

AAA
• Normal size: 2 cm
• AAA: 3 cm
• Prevalence: 1.3% in men aged 45-54 BUT 12.5% in age 75-84
• Risk factors: Same as CAD but mainly hereditary and tobacco
• Natural history: Gradual expansion; mural thrombus
• Complications: Rupture; thromboembolism; compression or erosion of adjacent structures
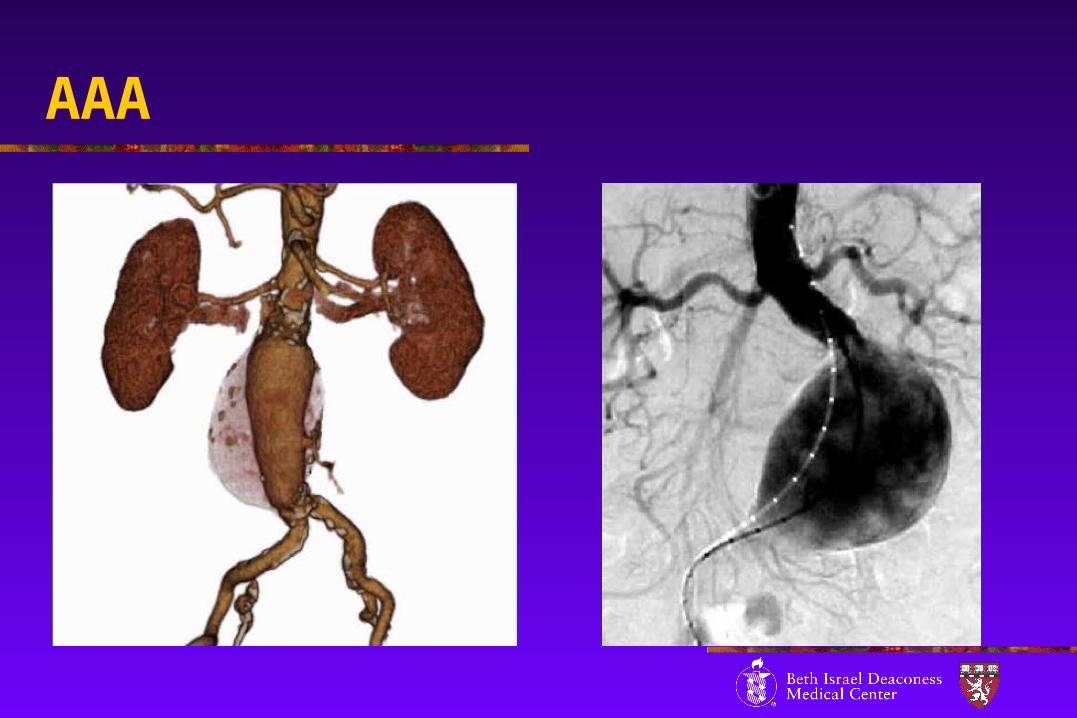
AAA
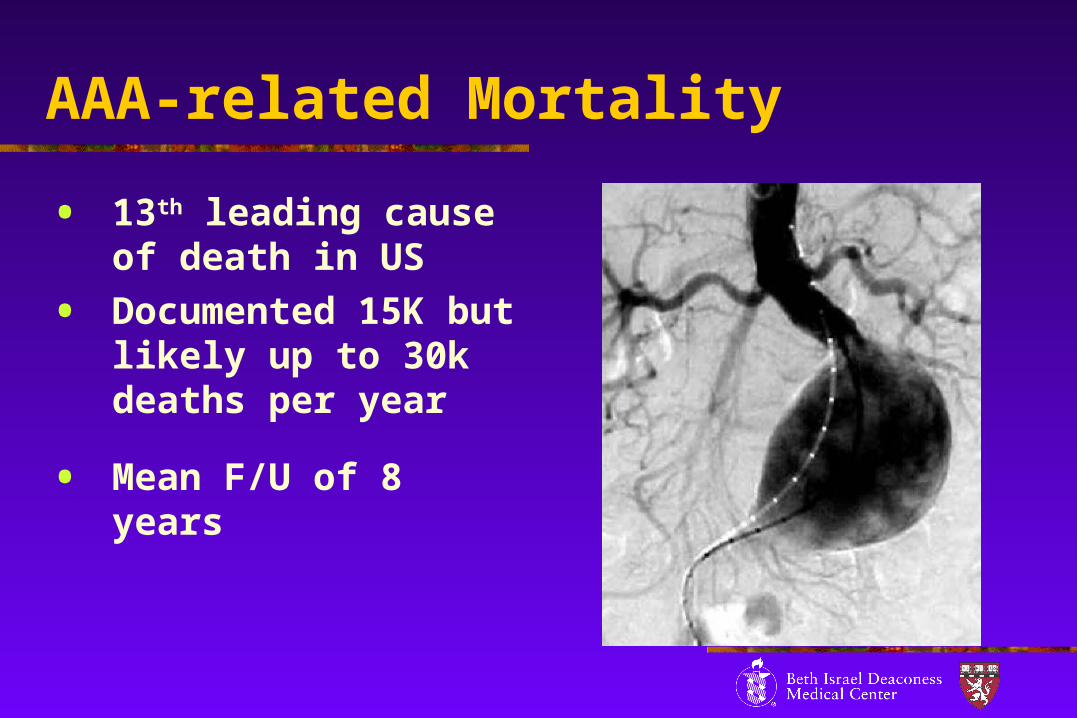
AAA-related Mortality
• 13th leading cause of death in US
• Documented 15K but likely up to 30k deaths per year
• Mean F/U of 8 years

Natural History
• Yearly Growth Rates:0.19 cm for AAA 2.8 to 3.9 cm 0.27 cm for AAA 4.0 to 4.5 cm0.35 cm for AAA 4.6 to 8.5 cm
• Rupture Rate at 5 years:AAA >6 cm – 43% vs. 20% for smaller AAA
• Estimated Risk of Rupture:0 in AAA less than 4.0 cm0.5 to 5% for AAA 4.0 to 4.9 cm 3 to 15% for AAA 5.0 to 5.9 cm 10 to 20% for AAA 6.0 to 6.9 cm20 to 40% for AAA 7.0 to 7.9 cm30 to 50% for AAA 8.0 cm
Clinical Presentation
• Most AAA quiescent until rupture
• Rarely Abd. pain or back pain
• New pain and tenderness indicate recent expansion
• Thromboembolism to lower extremities
• Ruptured AAA: Triad of Abd. or back pain, hypotension, and pulsatile Abd. mass

Physical Examination
• 30% of asymptomatic AAA discovered during routine PE
• Pulsatile large Abd. mass
• Sensitivity of PR 22-96%

Screening – Benefit?
• In men age 50+ 49% decrease in AAA rupture in 5 years
• In men age 50+ 64% decrease in AAA rupture in 9 years
Wilminek et al. JVS 2003

Screening – Benefit?
• Population based study of 67,800 men aged 65-74 with random allocation to Abd. US
• Yearly US for AAA> 3 cm and surgery for AAA> 5.5cm or 1 cm progression within 1 year
• 4-year aneurysm-related mortality in control group: 0.33% vs. 0.19% (RR reduction 42%)
• Total of 47 fewer deaths in screening group
MASS: BMJ 2002

Screening – Cost
• Additional cost in screening group: $3.5 million
• Incremental cost-effectiveness ratio: $45,000 per life-year gained
• 10-year estimate: $12,500 per life-year gained
• Recommendation: Screening for ‘high-risk’ groups
MASS: BMJ 2002

Screening Guidelines
Class I
• Men age 60+ with FHx of AAA PE and US
Class IIa
• Men age 65 – 75 with h/o tobacco PE and USx1
BUT: No screening for non-smokers and women! ACC/AHA Guidelines for PVD; JACC 2006
Imaging - US
• Optimal for screening – cheap, easy and no radiation exposure
• Sensitivity almost 100%
• No visualization of iliac arteries
• Dependence on sonographer
• 2-3% of patients cannot be imaged
Imaging – CT/MRI
• Better definition of AAA shape
• Better image suprarenal AAA
• Detection of other Abd. pathology
• Other vascular structures visible (renal, iliac arteries)

Follow-up Surveillance
Aortic diameter <3 cm — no further testing
Aneurysm 3 to 4 cm — annual ultrasound Aneurysm 4 to 4.5 cm — ultrasound every
six months Aneurysm >4.5 cm — referral to a
vascular specialist
Society for Vascular Surgery
Follow-up Surveillance
• AAA <4.0 cm annual US
• AAA 4.0 – 5.4 cm bi-annual US
• Consider intervention when AAA >5.5 cm or >0.5 cm expansion within 6 months
• Also, intervention with Abd./back pain or tenderness and embolism
ACC/AHA Guidelines for PVD; JACC 2006
Observational Management
Class I
• Peri-operative BB therapy for Pt. with CAD
Class IIb
• BB therapy to reduce rate of AAA expansion
ACC/AHA Guidelines for PVD; JACC 2006

Intermediate Size AAA (4-5.5 cm)
UK Small Aneurysm trial
• Randomized 1090 Pt. to surgery vs. US surveillance every 6 months
• Operative mortality 5.4%
• Mean F/U of 8 years Lancet 1998
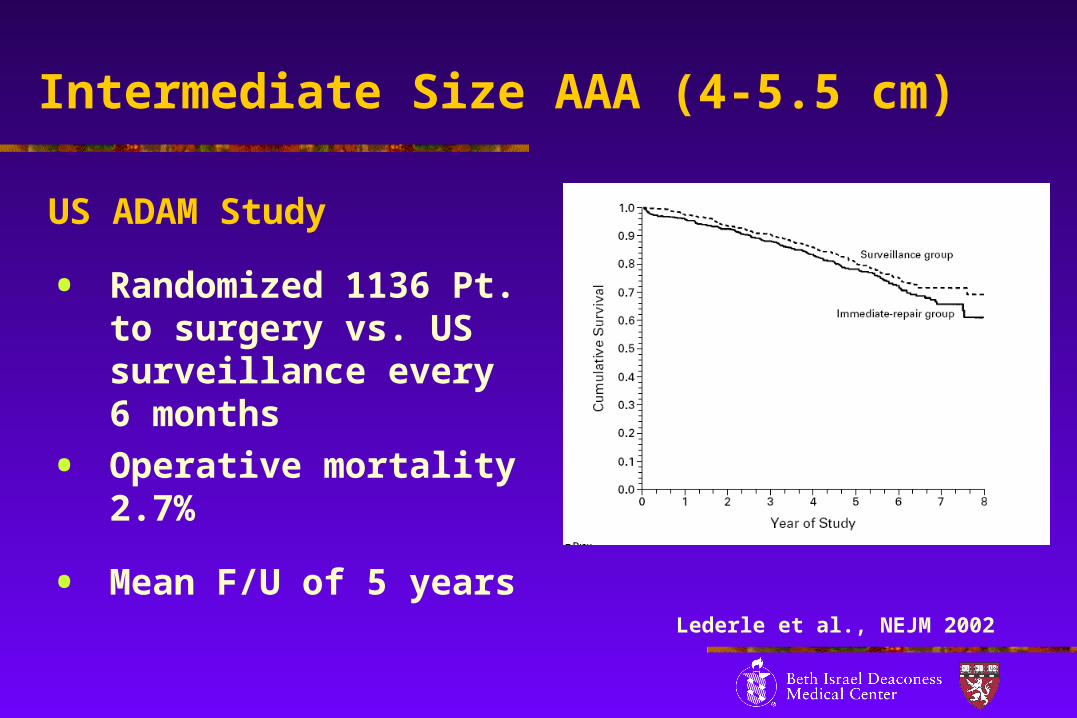
Intermediate Size AAA (4-5.5 cm)
US ADAM Study
• Randomized 1136 Pt. to surgery vs. US surveillance every 6 months
• Operative mortality 2.7%
• Mean F/U of 5 yearsLederle et al., NEJM 2002

Therapy
Surgery
• Peri-operative mortality 2.7-5.6%
• 40-70% mortality for ruptured AAA surgery
• Significant morbidity (5-12 weeks before returning to normal life style)

Therapy
EVAR
• Peri-operative mortality 1.0-2.4%
• May have lower mortality for ruptured AAA surgery
• Recovery within 1-3 days

Surgery vs. EVAR

Therapy - EVAR

Therapy - EVAR
Surgery vs. EVAR
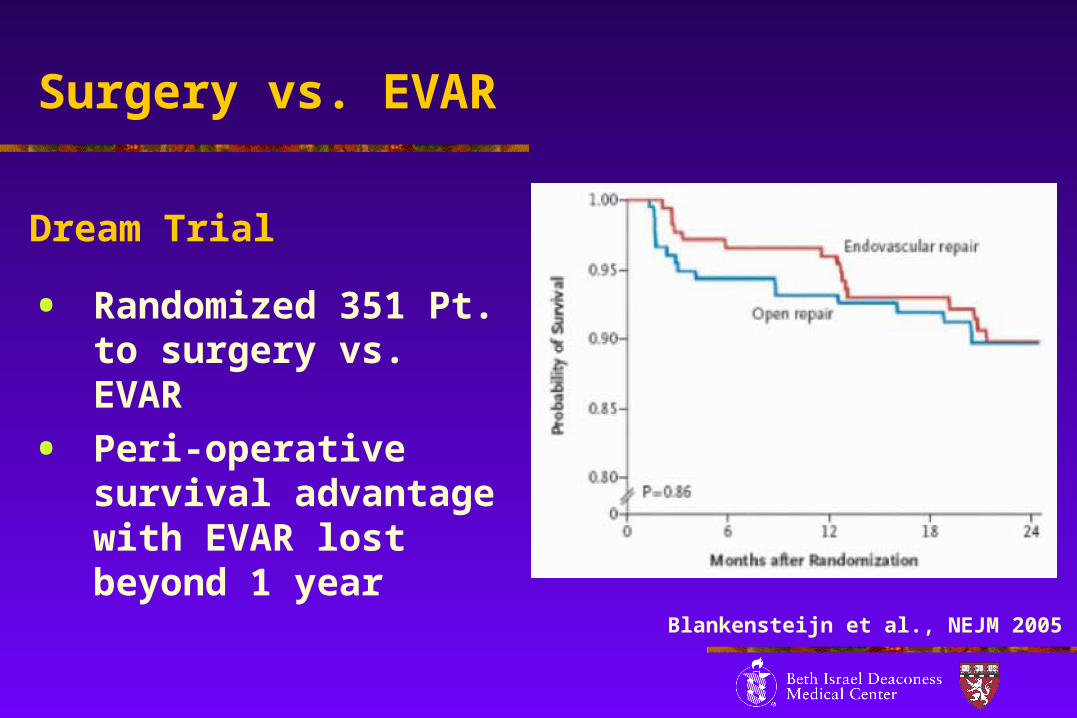
Dream Trial
• Randomized 351 Pt. to surgery vs. EVAR
• Peri-operative survival advantage with EVAR lost beyond 1 year
Blankensteijn et al., NEJM 2005
Related Documents











