Paul E de Jong, nephrologist University Medical Center Groningen The Netherlands Screening for Chronic Kidney Disease Where does Europe go?

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Paul E de Jong, nephrologist
University Medical Center GroningenThe Netherlands
Screening for Chronic Kidney Disease
Where does Europe go?

Lysaght, JASN, 2002
1990 2000 2010
426,000
1,490,000
2,500,000
Patients in chronic dialysis world-widedialysis costs ~ € 50.000/year

De Zeeuw et al. Kidney Int 2005;98:S25-29
PREVENDThe stages 1-5 of Chronic Kidney Disease

n= 85421 n= 85421
age 28age 28--75 yrs75 yrs
n= 40856n= 40856
-- morning urine samplemorning urine sample-- short questionnaireshort questionnaire
n= 8592n= 8592
oversamplingoversamplingelevated UAEelevated UAE
PREVEND: PREVEND: PPrevention of revention of RRenal enal and and VVascular ascular EEnd stage nd stage DDiseaseisease
www.prevend.orgpermanent follow up of this cohort
1997

CKD as predictor of renal events,
GFR or albuminuria?
PREVEND

Iseki et al; Am J Kidney Dis 2004;44:806-14
eGFR as predictor of end stage renal disease
n=95.252, follow-up: 7 years
0.01
0.1
1.0
10
100
1000
eGFR (mL/min)0 30 60 90 120
proteinuria negativeInci
denc
e of
ESR
D p
er 1
000
15
5 4 3 CKD stages

Iseki et al; Am J Kidney Dis 2004;44:806-814
eGFR and dipstick proteinuria as predictorof end stage renal disease
n=95.252, follow-up: 7 years
0.01
0.1
1.0
10
100
1000
proteinuria positive
eGFR (mL/min)0 30 60 90 120
proteinuria negativeInci
denc
e of
ESR
D p
er 1
000
15
5 4 3 2 1 CKD stages

PREVEND
Albuminuria predicts rate of renal function decline in the general population
-2
-1,8
-1,6
-1,4
-1,2
-1
-0,8
-0,6
-0,4
-0,2
00-15 15-30 30-150 150-300 >300
Slop
e of
rena
l fun
ctio
n de
clin
e (m
l/min
/yea
r)
Crude
Adjusted for age and sex
Adjusted for age, sex, BP,BPLD, lipids, LLD, glucoseand CV history
= UAE class
Van der Velde et al; JASN 2009; 20: 852-62 N=6.894
P<0.05
P<0.01
P<0.01
P<0.01
microalbuminuria macro

Total Medicare
Diabetes
Heart Failure
Dialysis/Tx
CKD
41.3% 48.1%
19%
7.8%
Alan Collins, USRDS database
Costs for kidney failure overlap with costs for diabetes and heart failure in age >60

CKD as predictor of CV events:
GFR or albuminuria?
PREVEND

Go et al, New Eng J Med 2004;351:1296-1305 Kayser-Permanente Study; n=1.120.295
0
1
2
3
4
5
6
7
>60
45-60
30-45
15-30 <1
5
>60
45-60
30-45
15-30 <1
5
Adj
uste
d H
azar
d R
atio
All cause mortality
CV events
GFR(mL/min/1.73m2)
eGFR as predictor of all cause mortality and cardiovascular events

Albuminuria as predictor of cardiovascular mortalityPREVEND
albumin concentration (mg/L)
1
2
3
4
5
2 10 100 1000
CV
mor
talit
y(a
ge a
nd s
ex a
djus
terd
rela
tive
risk)
Hillege et al; Circulation 2002;106:1777-82 N = 40.856
normo- micro- macro-

Brantsma et al, NDT 2008;23:3851-8
PREVEND
0 2 4 6 8
0,90
0,92
0,94
0,96
0,98
1,00
No CKD
Stage 1*
Stage 2*
Stage 3 and MA–
Stage 3 and MA+*
Follow-up in years
Prop
ortio
n fr
ee o
f car
diov
ascu
lar e
vent
CV outcome according to CKD class- age and sex adjusted -
*p <0.001 vs no CKD

Is it just identification of a subject with increased risk
or, ...
can we offer him a treatment?
PREVEND
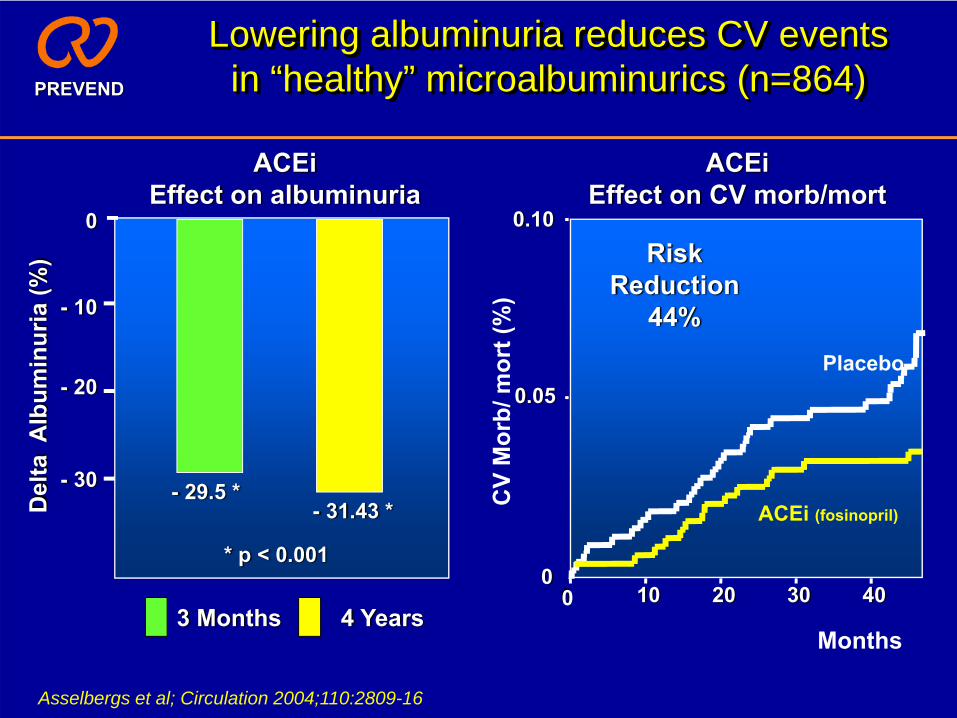
Asselbergs et al; Circulation 2004;110:2809-16
Lowering albuminuria reduces CV events in “healthy” microalbuminurics (n=864)
0 10 20 30 40
0.10
0.05
0
Placebo
ACEi (fosinopril)C
V M
orb/
mor
t (%
)
Months
RiskReduction
44%
Del
ta A
lbum
inur
ia (%
)
0
- 10
- 20
- 30
3 Months 4 Years
ACEiEffect on albuminuria
- 29.5 *- 31.43 *
* p < 0.001
ACEiEffect on CV morb/mort
PREVEND

eGFR
0
10
Follow-up (years)
Late intervention
Early intervention
GFR slope calculation affords early intervention
Need for dialysis
90
60
30
No albuminuria normal ageing
With albuminuria
PREVEND
Gansevoort et al. JASN 2009, 20: 465-8

Cost-effectiveness plane
0
400
800
1200
1600
2000
0 10 20 30
∆ Effect (in LYGs)
∆ C
ost
(100
0 x
in €
’s)
Low CostsLow Effects
High CostsHigh Effects
Low CostsHigh Effects
High CostsLow Effects

Cost vs effects: PREVEND
0
400
800
1200
1600
2000
0 10 20 30
∆ Effect (in LYGs)
∆ C
ost
(100
0 x
in €
’s)
€80,000 per LYG
€50,000 per LYG
€20,000 per LYG
UAE ≥ 300 mg/dUAE ≥ 30 mg/dUAE ≥ 15 mg/d
Boersma C et al. Clin Therapeutics 2010, in press
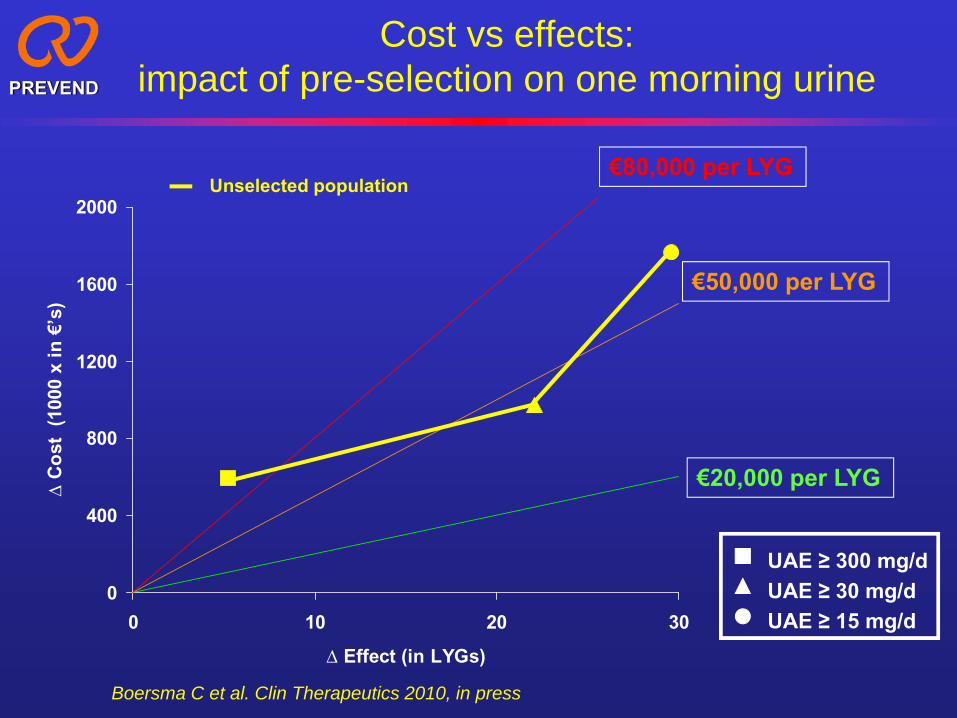
Cost vs effects: impact of pre-selection on one morning urinePREVEND
0
400
800
1200
1600
2000
0 10 20 30
∆ Effect (in LYGs)
∆ C
ost
(100
0 x
in €
’s)
€80,000 per LYG
€50,000 per LYG
€20,000 per LYG
UAE ≥ 300 mg/dUAE ≥ 30 mg/dUAE ≥ 15 mg/d
Unselected population
Boersma C et al. Clin Therapeutics 2010, in press

Cost vs effects: impact of pre-selection on one morning urinePREVEND
0
400
800
1200
1600
2000
0 10 20 30
∆ Effect (in LYGs)
∆ C
ost
(100
0 x
in €
’s)
€80,000 per LYG
€50,000 per LYG
€20,000 per LYG
UAE ≥ 300 mg/dUAE ≥ 30 mg/dUAE ≥ 15 mg/d
Unselected populationPre-selection on UAC ≥10 mg/L
Boersma C et al. Clin Therapeutics 2010, in press

Cost versus Effects:impact of age-limitationPREVEND
0
400
800
1200
1600
2000
0 20 40 60 80 100
∆ Effect (in LYGs)
∆ C
ost
(100
0 x
in €
’s)
€80,000 per LYG €50,000 per LYG €20,000 per LYG
€10,000 per LYG
All subjects
UAE ≥ 300 mg/dUAE ≥ 30 mg/dUAE ≥ 15 mg/d
Boersma C et al. Clin Therapeutics 2010, in press

Cost versus Effects:impact of age-limitationPREVEND
0
400
800
1200
1600
2000
0 20 40 60 80 100
∆ Effect (in LYGs)
∆ C
ost
(100
0 x
in €
’s)
€80,000 per LYG €50,000 per LYG €20,000 per LYG
€10,000 per LYG
All subjectsAge >50 years UAE ≥ 300 mg/d
UAE ≥ 30 mg/dUAE ≥ 15 mg/d
Boersma C et al. Clin Therapeutics 2010, in press

APPROACH-USA
Overall population
Percentage visiting GP
Measurements
Action
Target population
30-50%
History on renal and cardiovascular end organ damage
Measure renal and cardiovascular risk factors
Measure eGFR and albuminuria
When suspicion of primary renal disease: additional investigations + specific treatment
In case of CKD without suspicion of primary renal disease: treat CV risk factors
APPROACH-UK APPROACH-Netherlands
If known with DM, HT, CV-history, or age>50 yr
SCREENING
De Jong et al. CJASN 2008;3:616-23

APPROACH-USA
Overall population
Percentage visiting GP
Target population
30-50%
Disadvantage: - the patients diagnosed mostly are on treatment yet
Advantage: - being aware of CKD requires more aggressive treatment goals
APPROACH-UK APPROACH-Netherlands
If known with DM, HT, CV-history, or age>50 yr
SCREENING
De Jong et al. CJASN 2008;3:616-23

APPROACH-USA
Overall population
Percentage visiting GP
Measurements
Action
Target population If known with eGFR <60:
Confirm impaired eGFR; If positive
30-50% 2-3%
History on renal and cardiovascular end organ damage
Measure renal and cardiovascular risk factors
Measure eGFR and albuminuria
When suspicion of primary renal disease: additional investigations + specific treatment
In case of CKD without suspicion of primary renal disease: treat CV risk factors
3-4%
APPROACH-UK APPROACH-Netherlands
If known with DM, HT, CV-history, or age>50 yr
SCREENING
De Jong et al. CJASN 2008;3:616-23

APPROACH-USA
Overall population
Percentage visiting GP
Target population If known with eGFR <60:
Confirm impaired eGFR; If positive
30-50% 2-3%
Disadvantage: - there is just detection of stage 3 or more CKD
- focus might be incorrect as it detects only patients with a reason to do serum creatinine measurements
Advantage: - it does not require prior selection
3-4%
APPROACH-UK APPROACH-Netherlands
If known with DM, HT, CV-history, or age>50 yr
SCREENING
De Jong et al. CJASN 2008;3:616-23

APPROACH-USA
Overall population
Percentage visiting GP
Measurements
Action
Target population If known with eGFR <60:
Confirm impaired eGFR; If positive
30-50% 2-3% 7-8%
History on renal and cardiovascular end organ damage
Measure renal and cardiovascular risk factors
Measure eGFR and albuminuria
When suspicion of primary renal disease: additional investigations + specific treatment
In case of CKD without suspicion of primary renal disease: treat CV risk factors
15-20%
3-4%
APPROACH-UK APPROACH-Netherlands
Confirm microalbuminuria: If positive
Preselection on dipstick or albuminuria; If positive:
If known with DM, HT, CV-history, or age>50 yr
SCREENING
De Jong et al. CJASN 2008;3:616-23

age < 65 age > 65
Dutch GP-nephrologist CKD cooperation
green = GP follows DM and CVD guideliness whenever appropriateyellow = CKD guideliness followed by GP, unless x1; orange = consultation between GP and nephrologistred = nephrologist
x1 = rapid eGFR decline, underlying kidney disease, or metabolic complications
figures in cells refer to the number of subjects per 1000 population
Normoalbuminuria
Microalbuminuria
Macroalbuminuria
GFR > 90 254 15 -
GFR 60-90 678 27 2
GFR 45-60 20 2 1
GFR 30-45 - - -
GFR < 30 - - -
Normoalbuminuria
Microalbuminuria
Macroalbuminuria
GFR > 90 66 10 -
GFR 60-90 687 72 8
GFR 45-60 119 21 6
GFR 30-45 5 3 1
GFR < 30 1 - -

ConclusionsPREVEND
• CKD is found in about 10% of the population• The level of albuminuria is of more impact than
the level of GFR to predict both renal and CV prognosis
• Lowering albuminuria prevents CV events• Screening for albuminuria is cost-effective to
prevent CV events• Screening for albuminuria affords early
intervention• It can be implemented in GP practice
Related Documents











