Alloplasc Skin Substute (SUPRATHEL®) dressings in treatment of donor sites in children with burns... An opon for difficult-to decide cases... Bromelain based debridement agent introducon to our daily pracse, modificaons to the standard protocol and post-debridement wound dressing... Comparave Evaluaon of effecveness of alloplasc Skin Substute “SUPRATHEL®” and histoequivalent bioplasc material... Early surgical treatment of burns using wound coverings... Results from Applicaon to an Absorbable Synthec Membrane to Superficial and Deep Second Degree Wounds… The treatment of epidermal and deep dermal wounds with polylacd based membrane... The Use of SUPRATHEL® Skin Substute for Paral Thickness Burns in a UK Regional Burns Centre… Treatment of second degree burns... Use of alloplasc temporary skin substute* in the treatment burn wounds of II degree... Use of SUPRATHEL® in surgical, non-surgical, non-surgical and enzymacally debrided burns... Use of SUPRATHEL® as a complete epidermal substute in a boy with extensive toxic epidermal necrolysis... Applicaon of SUPRATHEL® in diverse indicaons Scienfic Update 10/2017 THE TEMPORARY SECOND SKIN

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Alloplastic Skin Substitute (SUPRATHEL®) dressings in treatment of donor sites in children with burns... An option for difficult-to decide cases... Bromelain based debridement agent introduction to our daily practise, modifications to the standard protocol and post-debridement wound dressing... Comparative Evaluation of effectiveness of alloplastic Skin Substitute “SUPRATHEL®” and histoequivalent bioplastic material... Early surgical treatment of burns using wound coverings... Results from Application to an Absorbable Synthetic Membrane to Superficial and Deep Second Degree Wounds… The treatment of epidermal and deep dermal wounds with polylactid based membrane... The Use of SUPRATHEL® Skin Substitute for Partial Thickness Burns in a UK Regional Burns Centre… Treatment of second degree burns... Use of alloplastic temporary skin substitute* in the treatment burn wounds of II degree... Use of SUPRATHEL® in surgical, non-surgical, non-surgical and enzymatically debrided burns... Use of SUPRATHEL® as a complete epidermal substitute in a boy with extensive toxic epidermal necrolysis...
Application of SUPRATHEL® in diverse indications
Scientific Update 10/2017
THE TEMPORARY SECOND SKIN

SUPRATHEL® received significant attention at both the EBA in Barcelona and the GBMC in Dubai this month with 3 oral and over 12 poster presentations. The presentations showed data on the
Over 1000 patients successfully treated with SUPRATHEL® at the UKB in Berlin where SUPRATHEL® has become the standard of care for all partial thickness burns (Dr. Sander, GBMC 2017), Potentially higher quality of skin after treatment with SUPRATHEL® (compared to AquacelAg or auto-grafting) (Dr. Demircan, EBA 2017),
SUPRATHEL®’s value in the treatment of children in Pakistan – including the ability to treat deep dermal burns and significant reduction in pain (Dr. Iqbal, EBA 2017).
The 12 posters on SUPRATHEL® presented at the EBA 2017 can be found online as well.
We thank all presenters for their contributions to better understanding when and how SUPRATHEL® can
be used in the clinical practice as well as the over 30 participants at our SUPRATHEL® User Workshop at the EBA.
If you have any questions about SUPRATHEL®, please feel free to contact me or our team. We will do whatever we can to make sure your patients will receive the best treatment. Thank you! Christian Planck Chief Operating Officer
Welcome

Copyright © 2017 O. Demidova, S. Manushin. [email protected]
O. Demidova, S. Manushin
Central City Clinical Hospital, Ulyanovsk, Russia
Aim of research:
The aim of this study was to investigate the
efficiency of alloplastic skin substitute dressings on pain
syndrome and epitheliazation of donor sites in burned
children.
Materials and Methods:
Twenty-four patients with 2-3 degree burns up
3% to 15% of body surface were studied. Patients were
treated in Burn Center from 1 January to 31 December
2016. Split grafts were isolated with disc dermatome.
Thickness of grafts was 0.3-0.4 mm. SUPRATHEL® was
placed on donor wounds in 11 patients. In control group
(13 patients) one-level gauze ointment dressings were
used. Patients age in SUPRATELR and control group did
not differ (11.9±3.36 and 14.2±4.94 months, Z=-1.2,
p=0.23).
Results:
In SUPRATHEL® group the dressings were not removed
until complete epitheliazation of donor wounds and
changing of SUPRATHEL® dressings was not necessary.
In control group changing of dressings was needed in 4
patients.
The Study has proved that in case of use of
alloplastic skin substitute SUPRATHEL®, median
epitheliazation time was 5.7±1.01 days, in control group -
time was 8.7±1.49 days (Z=-3.8, p=0.0002). According to
Verbal Descriptor Scale expression of pain syndrome was
less in SUPRATHEL® group than in control group
(1.5±1.04 and 5.2±0.9 respectively, Z=-4.1, P<0.001).
Conclusion:
Our study shown that use of alloplastic skin
substitute SUPRATHEL® is effective in treatment of
donor wounds in pediatric burns. Time of epithelization is
shortened and pain syndrome is reduced.
Alloplastic skin substitute (SUPRATHEL®) dressings in
treatment of donor sites in children with burns

Copyright © 2013 Corresponding Autor : Mehmet HABERAL,MD,FACS,FICS e-mail adress: [email protected]
Ayse Ebru ABALI, Gokhan MORAY, Mehmet HABERAL; Burn and Fire Disasters Institude, Baskent University, Ankara, Turkey
Delayed use of polylactide-based copolymer (Suprathel®) for pediatric partial-thickness burns:
An option for ‘difficult-to decide’ cases
Many partial-thickness burns in children lead to confusion whether they are superficial or deep. Polylactide-based copolymer (Suprathel®) is a synthehtic temporary skin substitude . it is promptly used for superficial dermal-burns. But, surgical-debridement is required before using Suprathel® for deeper dermal burn wounds.
This study aimed to document the outcomes of delayed outpatient use of Suprathel® (following outpatient wound-care with non-surgical debritement methods) in those cases whose wound-depths are ‘difficult-to-decide’.
The subjects: Pediatric burn-victims (n=47) who were treated with Suprathel® following outpatient wound-care with non-surgical debridement methods (2013-2016) Non-surgical debritment (every alternate day) • Debritement of thin necrotic material:Triticum Vulgare (fito krem, Abdi İbrahim, İstanbul-Turkey) •Debritement of thick necrotic material: Modified starch polymer gel (Askina gel, Braun, Sligo-Ireland) •After elimination of necrotic material, outpatient application of Suprathel®(Figure1) Collected Data: •Age, sex, burn-cause, extent of burns, depth of burn-wounds, body-sites affected; •Time-intervals between occurrence of injury and admission; •Time-intervals between admission and Suprathel®application;, •Time-intervals between occurrence of injury and completion of epithelization •Numbers of Suprathel® applications, •Surgical-debridements,split-thickness-skin-graftings/full-thickness-skin-graftings(STSG/FTSG) •Requirements of physiotherapy/splints, ,reconstructive surgeries (mean±SEM). •Followup: 3months-2years (Figure 2)
Results: Burn cause Age, and sex distribution
(M/F)
TBSA/TBSA partial thickness
(%)
Scalds (n=34,72,3%) 4,96±15 and 0,46/1 3,38±0,9/ 3.27±0,9
Contact burn (n=9,19,1%) 2,28±0,9 and 1/2 1,5±0,24/1,5±0,25
Flash Burns (n=2, 4,3%) 15.5±0,5 and 2/0 8.5±0,24/8,5±1,5
Flame burns (n=2, 4,3%) 16± 1 and 1/1 3,5±0,5/ 3.±1.
Total (n=47, 100%) 5,14±0,8 and 0,68/1 3,18±0,4/ 3.02±0,39
Time interval between injury and admission
Time interval between admission and suprathel
Time interval between injury and epithelisation
1,6±0,36 days
6,53±0,64 days 17,4±1,07 days
Suprathel application: Once
Suprathel application: Twice
No Suprathel application:
66% (n=31) 34,04% (n=16) burn wounds at head and neck iin 12 cases
Outpatient wound-care with non-surgical debridements followed by Suprathel® application is a functional option for ‘difficult-to-decide’ partial-thickness burns in childhood. This method seems to reduce need
for sedoanelgesia and to prevent exaggerated surgical approaches which may lead to painful and uncomfortable overtreatment courses.
Post-burn 2 days
Non-sugical debritements 6th day Removal of suprathel post-burn16 days
8 months after treatment
Treatment modalities
Acute/long-term follow up:
requried Not required
Surgical debritement 17,4% (n=8) 82,6% (n=39)
STSG/FTSG 6,5% (n=3) 93,5% (n=44)
Physiotherapy 32,6% (n=15) 67,4% (n=32)
Splinting 11,4% (n=5) 88,6% (n=42)
Reconstructive surgery 4,3% (n=2) 95,7% (n=45)
Patients and Methods:
Affected Body sites: Patients
Hands 38,9% (n=18) Feet 31,9% (n=15) Upper extremities 38,9% (n=18) Lower extremities 14,9% (n=7) Trunk 14,9% (n=7) genitals 4,3 % (n=2) Head and neck 29,8% (n=14)
Figure 1 Figure 2
DISCUSSION & CONCLUSIONS:

Foto ap
lication.
Modified protocol of BBD application and immediate post-debridement wound dressing .
The standard protocol of BBD application is based on the application of a sterile adhesive barrier (vaseline) on the non-injured skin outside of the burned area. Our modified protocol was based on the use of fatty gauzes applied on the burned area and on the non-injured skin after the standard BBD application onto the wound. A sterile occlusive film dressing was then applied to cover the wound (Fig. 1). After standard BBD removal, we used a short soaking with antibacterial solution (20 minutes) and then we applied a collagenase ointment (iruxol) for 12 to 24 hours.
RESULTS
• 62 patients were treated with BBD
- 37 male and 25 female, aged 18-79 . • The mean TBSA treated was 7.1 % (range 3-20%).
• 19 patients were autografted
• 43 patients were treated conservatively (Fig.2)
Caractheristics of patients treated conservatively
• 14 patients were treated with UrgoClean®
• 11 patients were treated with Suprathel®
• 17 patients were treated with fatty gauze
The patient and burn characteristics were shown in Table1.
Data regarding wound treatment characteristics were shown in Table 2.
Table 1 – Patient and burn characteristics
Urgoclean n =14
Suprathel n = 11
Fatty gauze n = 17
Gender (m/f), % 59.0/41.0 53.2/46.8 55.0/45.0
Mean age (years) 39.3 41.5 48.7
Mean % TBSA treated 7.9 7.2 8.3
Anatomic areas, % head/neck upper extremities torso lower extremities
2
39 27 32
5
49 18 28
2
20 48 30
CONCLUSIONS
In our experience, BBD proved to be an effective, fast and selective therapeutic tool fo.r burn wound management.
Our modifications to the standard protocol made BBD application easier and more practical and allowed a more effective eschar removal.
Our data regarding the use of Urgoclean, Suprathel and fatty gauze in the post-enzymatic debridement wound dressing suggest that all three dressings were
effective managing partial-thickness and deep partial-thickness burn wounds. Time to wound healing was similar among the three treatment groups. However,
the treatment profiles differed partially with a limited number of wound dressing changes and lower pain scores for the Urgoclean and Suprathel groups
compared with the fatty gauze group.
Table 2 – Wound treatment characteristics
Urgoclean n =14
Suprathel n = 11
Fatty gauze n = 17
Average healing time (days) 15 17 19l
Avarage pain scores 1.8 2.2 6.9
Number of wound dressing changes
1.9 2.3 8.1
Fig. 1 - Modified protocol of BBD application
a b c
Fig. 2 - (a) Mixed dorsal hand burn after BBD application; (b) Urgoclean
dressing; (c) spontaneous healing at day 13.
Bromelain based debridement agent: introduction to our daily practise, modifications to the standard protocol and post-debridement wound dressing
I. Mataro, S. Ruiz, E. Pagnozzi, A .Coppola, C. Gagliardo, R. d’Alessio Plastic and Reconstructive Surgery Department and Burn Unit. Hospital A. Cardarelli, Naples (Italy).
INTRODUCTION
In modern burn therapy an optimal debridement must be effective, fast and safe. At present, surgical excision followed by autografting is the standard of care
(SOC) for deep burns. However, invasive surgery often results in loss of viable tissue, blood and heat. We present an early single center experience with a new
Bromelain Based Debridement agent (BBD).
METHODS
• From May 2015 to May 2017
• 62 patients with deep partial and full thickness thermal burns
• Aged between 18-79 years
• TBSA no more than 20%
BBD application was performed at the patient’s bedside under IV analgesia while BBD removal was performed in the operating theatre under analgo-sedation.
After eschar removal, full thickness burns were autografted, while viable dermis and mixed wounds were treated with UrgoClean®, Suprathel® or fatty gauze.
A retrospective analysis of patients treated with conservative dressings was conducted to evaluate time to wound healing, pain scores, and number of dressing
changes. The pain scores were obtained during dressing changes using the visual analog pain scale 1–10; 0 being no pain, 5 being moderate pain, and 10, the
severe pain.

.
COMPARATIVE EVALUATION OF EFFECTIVENESS OF ALLOPLASTIC SKIN SUBSTITUTE “SUPRATHEL” AND HISTOEQUIVALENT-BIOPLASTIC MATERIAL
FOR TREATMENT OF BURN WOUNDS
Objectives: To investigate effectiveness of alloplastic skin substitute "Suprathel" for treating burn wounds.
Methods: "Suprathel" is a microporous membrane, consisting of copolymer of polylactide and other polymers. In conditions of wound
healing, this synthetic material performs substitute function of damaged skin and stimulates regeneration.
Before using materials, II-III degree burn wounds underwent dermabrasion by synthetic brush, electric dermatome, or hydrosurgical
system "Versajet". Patients from group of comparison were treated using histoequivalent-bioplastic material G-DERM (membrane
based on hyaluronic acid and collagen).
The results are shown in the tables below.
Discussion/Conclusion: Application of alloplastic skin substitute "Suprathel" provides effective treatment for border and mosaic II-III
degree burn wounds.
A.A.Alekseev, N.B.Malutina, Y.I.Turnikov, A.E.Mitichkin, S.V.Popov. Russian Medical Academy of continuous Postgraduate Education, Moscow, Russia.
Parameters Alloplastic skin substitute "Suprathel"
Histoequivalent-bioplastic material G-DERM
Number of patients 20 20
Time of epithelization (days after injury) 14,8±1,6 15,6±1,1
Wounds required auto skin grafting (%) 10 20
Pain during dressing change (score) 2,4± 0,5 5,1± 0,9
Day 3 after trauma II-III degree burn before dermabrasion
Day 3 after trauma Skin substitute on the wound after dermabrasion
Day 13 after trauma. Skin substitute is fixed on the wound
Day 19 after trauma. Epitelization
1 year after trauma. Normotrofic scars
Supr
athe
l
G-D
ERM

Bogdanov S.B., Babichev R.G.
«Research Institute - Regional Clinical Hospital №1 named after Professor S.V. Ochapovsky".
Krasnodar. Russian Federation.
Aim. To develop methods of early surgical treatment of deep dermal burns with wound dressings.
Methods. Annually in the center 1,300 treated patients with burns (including 700 children). Running up to 2000 operations. In
500 patients with deep dermal burns are performed annually in the early necrectomy 2-5 days after injury to the closure of
wound dressing wounds. Since 2015 applies «Suprathel». In order to create optimal conditions for the epithelialization of deep
dermal burns after necrectomy the wound impose «Suprathel».
Results. After necrectomy to the lower layers of the dermis perform napkins with epinephrine hemostasis for 5-7 minutes. Then
superimposed sterile wound covering «Suprathel», which is fixed with a bandage. Subsequently, only cosmetic dressings
performed starting from the third day after surgery. Wound coatings are not removed until complete epithelialization of
wounds. Epithelialization occurs depending on the depth of burns 8-12 days after surgery. When staged surgical treatment of
painful dressings with ointments, without «Suprathel», made every other day for 15-21 days.
Conclusion. In combustiology clinical picture of wound healing is diverse and depends on the stage of wound healing and burn
depth. In the traditional, staged surgical treatment of deep dermal burns tend to deepen with the formation of granulation tissue
and the need to follow autoplasty. A more preferred method of treatment of deep burns is a method of early surgical treatment,
in which the crust is removed in the early stages after the burn, and the wound is closed wound coverings. Research result has
been an advantage once the surgical treatment of wounds using «Suprathel» to the local conservative treatment with long-
lasting dressings.
EARLY SURGICAL TREATMENT OF BURNS USING WOUND COVERINGS
3 day after injury, formation of dermal burn necrosis
Tangential necromectomy with dermatome The bottom of the wound afte excision of necrosis, the lower layers of the dermis
Wound closed supratel 3 day after surgery 7 day after surgery, beginning of epithelialization
8 day afte surgery, active epithelialization
9 day after surgery, result of treatment
© 2017 Lehigh Valley Health Network
• Understand different treatment options for second degree burns• Compare outcomes after different treatments for second degree burns• Discuss outcome measures for second degree burns• Evaluate cost of different treatment options for second degree burns
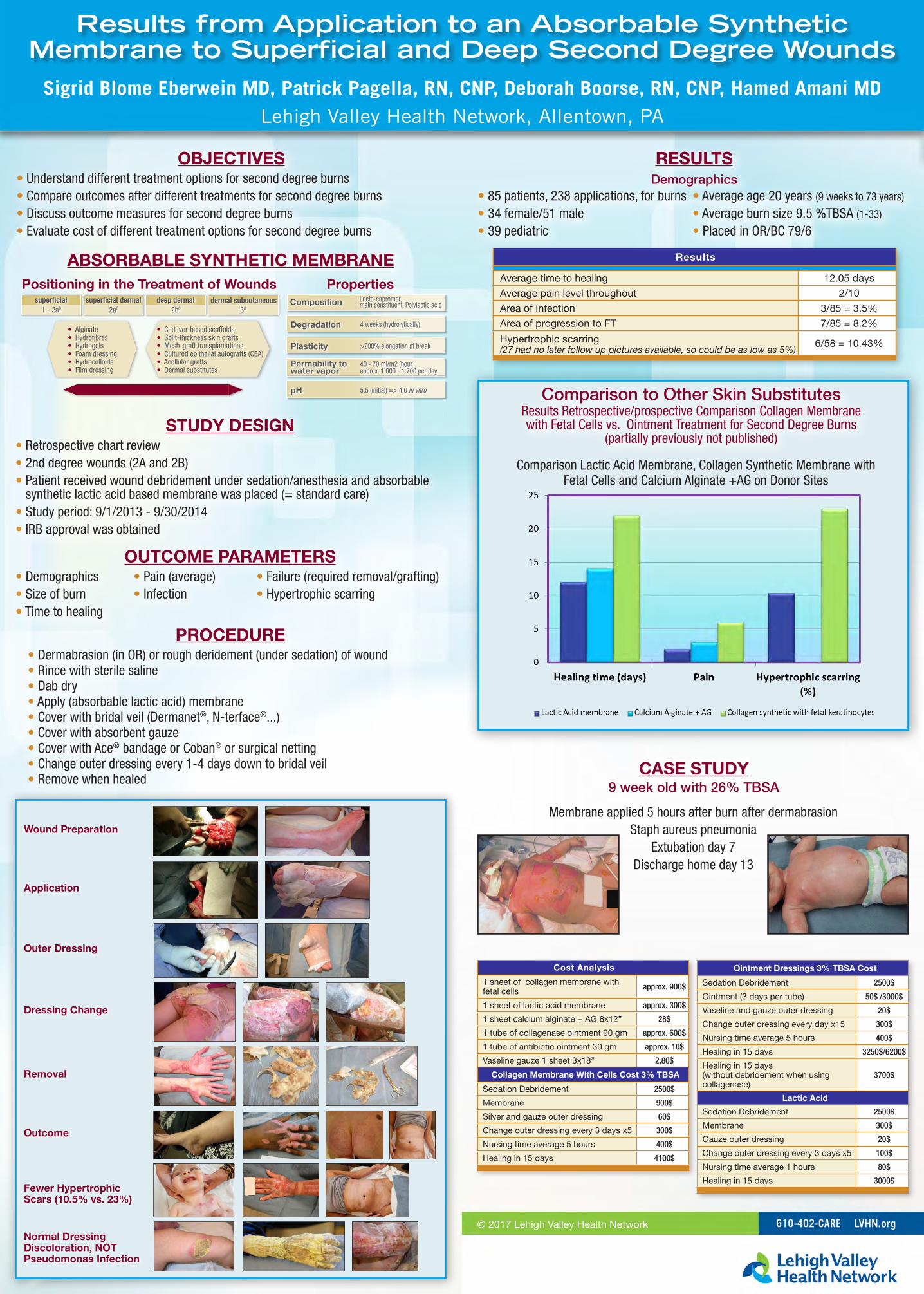
Results
Average time to healing 12.05 days
Average pain level throughout 2/10
Area of Infection 3/85 = 3.5%
Area of progression to FT 7/85 = 8.2%
Hypertrophic scarring(27 had no later follow up pictures available, so could be as low as 5%)
6/58 = 10.43%
Lehigh Valley Health Network, Allentown, PA
Results from Application to an Absorbable Synthetic Membrane to Superficial and Deep Second Degree Wounds
Sigrid Blome Eberwein MD, Patrick Pagella, RN, CNP, Deborah Boorse, RN, CNP, Hamed Amani MD
Comparison Lactic Acid Membrane, Collagen Synthetic Membrane with Fetal Cells and Calcium Alginate +AG on Donor Sites
PropertiesComposition Lacto-capromer,
main constituent: Polylactic acid
Degradation 4 weeks (hydrolytically)
Permability to water vapor
40 - 70 ml/m2 (hourapprox. 1.000 - 1.700 per day
pH 5.5 (initial) => 4.0 in vitro
Plasticity >200% elongation at break
Comparison to Other Skin SubstitutesResults Retrospective/prospective Comparison Collagen Membrane with Fetal Cells vs. Ointment Treatment for Second Degree Burns
(partially previously not published)
OBJECTIVES
ABSORBABLE SYNTHETIC MEMBRANEPositioning in the Treatment of Wounds
1 - 2a0
superficial2a0
superficial dermal2b0
deep dermal30
dermal subcutaneous
• Alginate• Hydrofibres• Hydrogels• Foam dressing• Hydrocolloids• Film dressing
• Cadaver-based scaffolds• Split-thickness skin grafts• Mesh-graft transplantations• Cultured epithelial autografts (CEA)• Acellular grafts• Dermal substitutes
• Retrospective chart review• 2nd degree wounds (2A and 2B)• Patient received wound debridement under sedation/anesthesia and absorbable
synthetic lactic acid based membrane was placed (= standard care)• Study period: 9/1/2013 - 9/30/2014• IRB approval was obtained
STUDY DESIGN
Cost Analysis
1 sheet of collagen membrane with fetal cells approx. 900$
1 sheet of lactic acid membrane approx. 300$
1 sheet calcium alginate + AG 8x12” 28$
1 tube of collagenase ointment 90 gm approx. 600$
1 tube of antibiotic ointment 30 gm approx. 10$
Vaseline gauze 1 sheet 3x18” 2,80$
Collagen Membrane With Cells Cost 3% TBSA
Sedation Debridement 2500$
Membrane 900$
Silver and gauze outer dressing 60$
Change outer dressing every 3 days x5 300$
Nursing time average 5 hours 400$
Healing in 15 days 4100$
• Demographics• Size of burn• Time to healing
OUTCOME PARAMETERS• Pain (average)• Infection
• Failure (required removal/grafting)• Hypertrophic scarring
Wound Preparation
Application
Outer Dressing
Dressing Change
Removal
Outcome
Fewer Hypertrophic Scars (10.5% vs. 23%)
Normal Dressing Discoloration, NOT Pseudomonas Infection
• Dermabrasion (in OR) or rough deridement (under sedation) of wound• Rince with sterile saline• Dab dry• Apply (absorbable lactic acid) membrane• Cover with bridal veil (Dermanet®, N-terface®...)• Cover with absorbent gauze• Cover with Ace® bandage or Coban® or surgical netting• Change outer dressing every 1-4 days down to bridal veil• Remove when healed
PROCEDURE
• 85 patients, 238 applications, for burns• 34 female/51 male• 39 pediatric
RESULTS
• Average age 20 years (9 weeks to 73 years)
• Average burn size 9.5 %TBSA (1-33)
• Placed in OR/BC 79/6
Demographics
Ointment Dressings 3% TBSA Cost
Sedation Debridement 2500$
Ointment (3 days per tube) 50$ /3000$
Vaseline and gauze outer dressing 20$
Change outer dressing every day x15 300$
Nursing time average 5 hours 400$
Healing in 15 days 3250$/6200$
Healing in 15 days(without debridement when using collagenase)
3700$
Lactic Acid
Sedation Debridement 2500$
Membrane 300$
Gauze outer dressing 20$
Change outer dressing every 3 days x5 100$
Nursing time average 1 hours 80$
Healing in 15 days 3000$
Membrane applied 5 hours after burn after dermabrasionStaph aureus pneumonia
Extubation day 7Discharge home day 13
CASE STUDY9 week old with 26% TBSA
Gladden 2008 „Current trends in lactate metabolism: introduction” Med. Sci. Sports Exerc. 40:475-476 Lu et al. 2002 „Hypoxia-inducible factor 1 activation by aerobic glycolysis implicates the Warburg effect in carciogenesis” J. Biol.
Chem. 277:23111-5 Lu et al. 2005 „Reversible inactivation of HIF-1 prolyl hydroxylases allows cell metabolism to control basal HIF-1” J. Biol. Chem.
280:41928-39 Constant et al. 2000 „Lactate elicits vascular endothelial growth factor from macrophages: a possible alternative to hypoxia. “
Wound. Repair Regen. 8:353-360 Beckert et al. 2006 „Lactate stimulates endothelial cell migration.“ Wound. Repair Regen. 14: 321-324
Nareike et al. 2005 „Sodium lactate increases LPS-stimulated MMP and cytokine expression in U937 histiocytes by enhancing AP-1 and NF-kappa transcriptional activities” Am. J. Physiol. Endocrinol. Metab. 289:E534-42 Milovanova et al. 2008 „Lactate
stimulates vasculogenic stem cell via the thioredoxin system and engages an autocrine activation loop involving hypoxia-inducible factor 1” Mol. Cell Biol. 28: 6248-61
Aslam et al. 2005 „High lactate in wounds may initiate vasculogeneis via stem cell homing“ J. Am. Coll. Surg. (3S):S58 Zieker et al. 2008 „Lactate modulates gene expression in human mesenchymal stem cells.” Langenbecks Arch. Surg. Wagner et al. 2004 „Stimulation of fibroblast by lactate-mediated oxidants” Wound. Repair Regen. 12:368-73 Green and Goldberg 1964
„Collagen and cell protein synthesis by an established mammalian fibroblast cell line” Nature 204: 347-9
.
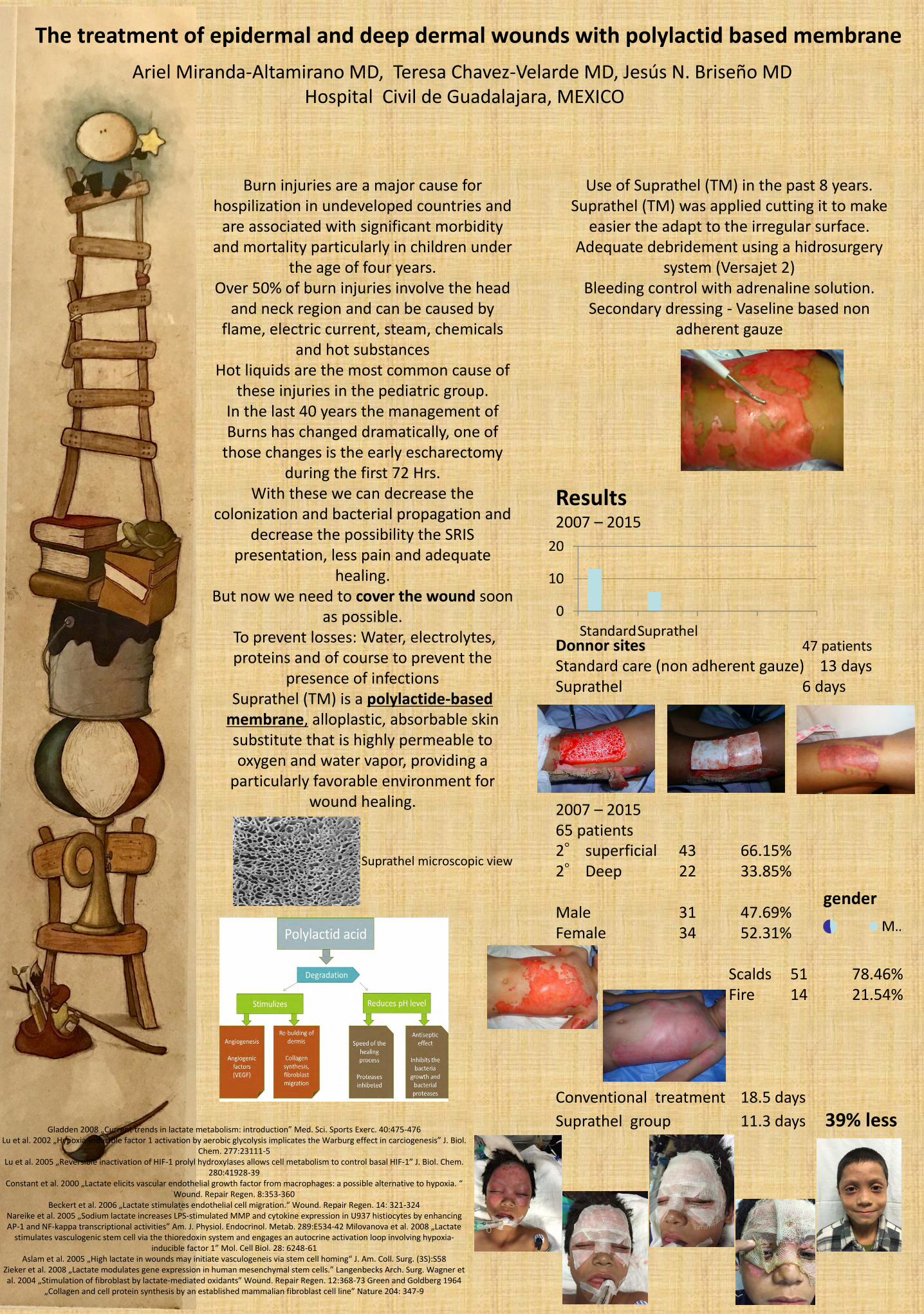
Ariel Miranda-Altamirano MD, Teresa Chavez-Velarde MD, Jesús N. Briseño MDHospital Civil de Guadalajara, MEXICO
The treatment of epidermal and deep dermal wounds with polylactid based membrane
Burn injuries are a major cause for hospilization in undeveloped countries and
are associated with significant morbidity and mortality particularly in children under
the age of four years. Over 50% of burn injuries involve the head
and neck region and can be caused by flame, electric current, steam, chemicals
and hot substancesHot liquids are the most common cause of
these injuries in the pediatric group. In the last 40 years the management of Burns has changed dramatically, one of
those changes is the early escharectomy during the first 72 Hrs.
With these we can decrease the colonization and bacterial propagation and
decrease the possibility the SRIS presentation, less pain and adequate
healing. But now we need to cover the wound soon
as possible.To prevent losses: Water, electrolytes, proteins and of course to prevent the
presence of infectionsSuprathel (TM) is a polylactide-based
membrane, alloplastic, absorbable skin substitute that is highly permeable to oxygen and water vapor, providing a
particularly favorable environment for wound healing.
Suprathel microscopic view
Use of Suprathel (TM) in the past 8 years. Suprathel (TM) was applied cutting it to make
easier the adapt to the irregular surface.Adequate debridement using a hidrosurgery
system (Versajet 2) Bleeding control with adrenaline solution. Secondary dressing - Vaseline based non
adherent gauze
Results2007 – 2015
Donnor sites 47 patients
Standard care (non adherent gauze) 13 daysSuprathel 6 days
2007 – 201565 patients 2° superficial 43 66.15%2° Deep 22 33.85%
Male 31 47.69%Female 34 52.31%
Scalds 51 78.46%Fire 14 21.54%
Conventional treatment 18.5 days
Suprathel group 11.3 days 39% less

The Use of Suprathel ® Skin Substitute for Partial Thickness Burns in a UK Regional Burns Centre
IntroductionInnovative new dressings such as Suprathel ® allow for effective skin replacement in the treatment of partial thickness and mid depth burn wounds. We aim to present our experience with the use and effectiveness of Suprathel®, a synthetic skin substitute, in a range of uses in burn practice for partial thickness burns in children and adults.
MethodsRetrospective analysis of medical case notes of St Andrews patients who had Suprathel® application from Jan 2014 to Feb 2017. Data was collected from case notes, the study evaluated re-epithelialization time, grafting, wound colonization, infection, length of hospital stay (LOS), wound over-granulation and hypertrophic scar formation. Suprathel® was applied after debridement, followed by Vaseline gauze or Silicone dressings, betadine gauze and bandages. Outer dressings were changed every 2 days unless Infection dictated otherwise.
ResultsEighteen patients were identified (mean age 12.15 years, range 1–54) with a mean total body surface area (TBSA) of 9.7% (range of burn size 2.5 – 21%) were included. 7 cases were superficial partial thickness, 11 cases were mixed depth with mid-deep dermal components. Median LOS was 9 days (range 2 - 26). Median re-epithelialization time was 15 days (range 9–48). 7 patients took over 21 days to heal. One patient developed hypertrophic scarring. 4 patients developed wound over-granulation. Suprathel® was applied to donor site in one case and directly to burn wound in 17 cases. 8 cases underwent Versajetdebridement prior to application. Suprathel® failed to adhere in one case. Three patients needed further split skin grafting to areas initially managed with Suprathel®. Out of the 18 patient we looked at 16 wounds were colonized during treatment, with 4 developing wound infection clinically.
ConclusionsSuprathel® is a versatile dressing solution for adult and paediatric patients suffering from burns. The different potential uses have learning curves for the multidisciplinary team. Suprathel® has the advantage that it may also be used to treat mid to deep dermal burns. In patients with extensive burns, Suprathel® can be used to cover the deep dermal burn wounds to prioritise skin grafts and their donor sites for full thickness burned areas. Further experiences with Suprathel® will help to determine its use to maximise its healing potential to improve aesthetic outcomes for scarring.
M.Nizamoglu, N Fox, K Cranmer, H Gerrish, N Martin, D Barnes, N El-Muttardi, P Dziewulski.St Andrew’s Centre for Plastic Surgery & Burns, Chelmsford, United Kingdom

© 2017 Lehigh Valley Health Network
Burn Recovery Center, Lehigh Valley Health Network, Allentown, PA
Treatment of Second Degree Burns with Lactic Acid Skin Substitute in the Outpatient Setting:
Pain and Patient ComfortDeborah Boorse, CRNP and Sigrid Blome-Eberwein, MD
Our burn center experience with lactic acid skin substitute spans 3 years treating over 400 patients with partial thickness thermal burns, ages ranging 8 weeks to 95 years old.
Under moderate sedation, wounds are initially debrided and lactic acid skin substitute and petroleum based gauze is applied. Outer dressings and burn net are then applied.
The patient is discharged with outer layer dressing changes planned every 2-3 days. Over the next 6-14 days, loose edges of the skin substitute are trimmed as they separate from epithelialized wound margins until all has separated in the outpatient setting.
METHODS
A burn wound coverage has long been sought that, among other requirements, reduces pain, protects the fragile wound bed, and minimizes the risk of infection during the healing phase of second degree burns.
OBJECTIVEOverall, there has been positive response from patients and families. Most patients and their families welcome the prospect of a “no-touch” wound care system as well as the decreased need for opiate pain control and dressing materials.
Benefits include: • Dressing changes, with virtually no pain, are easily taught to
family members. • The need for IV pain control for dressing changes is reduced,
resulting in decreased hospital length of stay. • The lactic acid skin substitute is generally well tolerated at
home.
Occasional reports of disadvantages include the following: • Itch beneath dressing (toward
the end of the healing phase); • Inability to shower; • Unusual (but inconsequential)
color changes in bilayer as healing progresses; and
• Uncomfortable warmth of dressing (rare).
RESULTS
The lactic acid skin substitute currently utilized in our burn center appears to meet the needs of pain control, wound bed protection, and infection risk minimization. The lactic acid skin substitute provides a relevant option in the treatment of partial thickness burns.
CONCLUSION

USE OF ALLOPLASTIC TEMPORARY SKIN SUBSTITUTE* IN THE TREATMENT BURN WOUNDS OF II DEGREE
V.S. Borisov, M.Y. Kaplunova, S.V. SmirnovBurn Center of the Sklifosovsky Institute for Emergency Medicine, Moscow, Russia
Objective: to evaluate the efficiency of alloplastic temporary skin substitute * in the treatment of patients with burn wounds of II degree
after debridement.
Material and method: the study included 7 patients with II degree burns on the area from 3 to 5% TBSA (an average of 4.2%), aged
from 28 to 55 years. All patients on 3-4 day from receipt of debridement was performed under anesthesia within the living dermis.
During the operation, performed a careful hemostasis. Further postoperative wounds were closed alloplastic temporary skin substitute*
and a single layer sheet of fatty gauze dressing, which fixed with a bandage. All patients received antibacterial therapy. The effectiveness
of alloplastic temporary skin substitute* in the topical treatment of postoperative burn wounds evaluated on terms of its healing, the
incidence of purulent complications, number of dressings, according to the degree of severity of pain.
Results: the 6 patients had favorable course of early postoperative period (the absence of suppuration, discharge from the wound, the
temperature of the reaction, pain). Therefore, the first ligation was made by 7 days after debridement. Were removed only the surface
layers of secondary casts over the alloplastic temporary skin substitute *. The second ligation was performed on 13-15 day, when it was
against the backdrop of biodegradable coatings complete healing has taken place. All wore bandaging painless nature and did not
require anesthesia.
In the one patient was noted accession secondary infection, necessitating daily dressings with antiseptics, antibacterial therapy has been
strengthened. Complete wound healing came only on the 23 day. Pain in this patient during dressing changes were more pronounced
pain in group II was more pronounced.
Conclusion: application of innovative alloplastic temporary skin substitute* in the treatment of patients with burns of II degree
efficiently and economically feasible.
Suprathel®*

22
43
NoComplica.onsSTSGInfec.on+STSG
USE OF SUPRATHEL IN SURGICAL, NON-SURGICAL AND ENZIMATICALLY DEBRIDED BURNS
Elena García-Vilariño, Enrique Salmerón González, Eloy Condiño Brito, Alberto Ruiz Cases, M. Dolores Pérez del Caz Unidad de Quemados. Hospital Universitari i Politècnic La Fe
CONCLUSION
Suprathel has provedtobeausefuldressingin certain burn cases.Due to the reduc=onin cure frequency andwoundmanipula=onareduc=on of pain,seda=on procedures,fas=ng periods andanesthe=c medica=onareachieved.
1. C.Uhlig,M.Rapp,B.Hartmann.Suprathel—Aninnova.ve,resorbableskinsubs.tuteforthetreatmentofburnvic.ms.Burns33(2007)221-2292. M.Keck,H.Selig,D.Lumenta.TheuseofSuprathelindeepdermalburns:Firstresultsofaprospec.vestudy.Burns3882012)388-3953. G.Hundeshagen,V.Collins,P.Wurzer.Aprospec.ve,randomized,controlledtrialcomparingtheoutpa.enttreatmentofpediatricandadultpar.al-thicknessburnswithSupratheloMepilexAg.JBurnCareRes.(May2017)
OBJECTIVEWeevaluatedtheuseofSuprathel®,a synthe.c copolymer membranefrom polylac.ds that provides atemporarywoundcoverageinburnpa.ents
METHODSFrom April 2013 toMay 2017, 29pa.ents withmid-dermal or deep-dermal burns a were treated withSuprathel® and evaluatedretrospec.vely.Suprathel®wasapplied:• AaerNexobrid®• Aaer hydro-debridement with
Versajet®• Ondonorsites• On mid-dermal non surgical
burns.The outer dressings were changedevery 2-3 days and the evolu.onwascloselyevaluated.
RESULTS
53year-oldfemale.A.1stDayofburn,showingdeepdermalburnaaerscald.B.WoundcoveragewithSuprathel®atemergencycare.C.Completereepitheliza.onaaerafollowingperiodof30days
A
CB
48year-oldmale.A.1stDayaaerfireburn.B.3rdDayofburnaaerNexobrid®.C.3rddaySuprathel®placement.D.40daysaaerdeep-dermalburn
A B C D

Chantaphakul, H., Sanon, T., Klaewsongkram, J.: Clinical characteristics and treatment outcome of Stevens-Johnson syndrome and toxic epidermal necrolysis. Experimental and Therapeutic Medicine (2015)Downey, A., Jackson, C., Harun, N., Cooper, A.: Toxic epidermal necrolysis: Review of pathogenesis and management. Journal of the American Academy of Dermatology 66, 995-1003 (2012).
Copyright © 2017 Renkert-Baudis M, [email protected]
1Renkert-Baudis M, 2Schöler M, 3Demirakca S, 3Jung T, 4Mockenhaupt M, 1Lange B
1Department of Pediatric Surgery, Pediatric Burn Center, University Medical Center, 68167 Mannheim, Germany2Department of Anaesthesiology and Surgical Intensive Care, University Medical Center, 68167 Mannheim, Germany3Department of Neonatology and Pediatric Intensive Care, University Medical Center, 68167 Mannheim, Germany4Department of Dermatology, University Freiburg – Medical Center, 79104 Freiburg, Germany
Use of Suprathel® as a complete epidermal substitute in a boy with extensive toxic epidermal necrolysis
ObjectivesToxic epidermal necrolysis (TEN) is a rare, potentially life-threatening condition characterized by extensive loss of skin and mucosa of more than 30%
total body surface area (TBSA). It is linked to certain drugs as well as viral or bacterial infections, resulting in a dysregulated immune reaction against
epithelial cells. Treatment, as in thermal injuries, should include an early referral to a burn unit. This case report demonstrates a life-saving
management of TEN with an epidermal substitute (Suprathel®) in a pediatric patient with epidermal damage of 100% TBSA.
MethodsA ten-year-old boy was admitted to our pediatric burn center complaining of foreign body sensation and photosensitivity of the eyes, headaches,
pyrexia and presenting with extensive epidermolysis involving 100% TBSA. A skin biopsy confirmed the diagnosis of TEN with a complete loss of the
epidermal layer as well as extensive mucosal involvement. The patient required fluid resuscitation and admission to the pediatric intensive care unit.
Wound care consisted of gentle debridement of the blistered areas followed by extensive Suprathel® application.
ResultsRepeated Suprathel® application maintained the skin barrier function over time and resulted in almost complete reepithelialization. The mucosa of the
urogenital tract and eyes showed an almost complete restitution, as well. After a six-week inpatient stay the patient could be discharged to our
outpatient care.
Two years after treatment the patient is satisfied with the results and the skin is virtually free of scars with a normal appearance and elasticity.
ConclusionIn children, TEN with extensive epidermal loss is a rare, life-threatening condition that requires admission to a specialized pediatric burn unit.
Suprathel® proves beneficial in the management of these cases by providing a skin barrier until natural reepithelialization occurs.
Clinical presentation on admission (after flu-like prodromal
stadium): severe conjunctivitis, mucosal erosions,
macules
Epidermal necrolysis, 100% TBSA Skin biopsy with complete detachment of the
epidermal layer
Suprathel® application after debridement,
nonintubated spontaneously breathing patient
Dressing change under sedation Two years after trauma: no scarring, some areas of hypopigmentation, full
range of motion, unimpaired vision

Polymedics Innovations Inc. 80 Pine Street, Floor 24New York, NY 10005 I USA
Phone +1 646 6042771Fax +1 646 3503129E-mail [email protected]
PolyMedics Innovations GmbH Heerweg 15 D73770 Denkendorf I Germany
Phone +49 (0)711 719 500-0Fax +49 (0)711 719 500-10E-mail [email protected]
Significant pain relief - by up to 60%1
Significantly less IV narcotic management required Minimally manipulative dressing changes without anesthesia
Low rate of infections and inflammatory response, no biologic risk Synthetic, biocompatible, absorbable No reported allergic reactions, only few cases with infections and inflammation
Fast wound healing2
Improved early epithelization Early mobilization can begin 2-5 days following application
Lower treatment costs3 - by up to 69% One-time wound dressing, no change of SUPRATHEL® needed Less care and aftercare needed, shortened need for hospitalization Less administration of pain medication needed
Good cosmetic and functional outcomes and scar quality4
KEY BENEFITS
Effective. Efficient. Reliable.
Imprint: PolyMedics Innovations GmbHHeerweg 15 D I 70773 Denkendorfwww.polymedics.de
Design PolyMedics Innovations CEO Prof. Dr. Heinrich Planck
Responsible of the redaction Christian Planck
Literature
1 Uhlig et al., Burns 33/2007; Schwarze at al., Am. Plast. Surgey 60/2009; Markl et al., Am Plast. Surg. 65/2010; Highton et al., Burns 39/2013 2 Uhlig et al., Burns Nov. 33/2007; Schwarze at al., Burns Nov. 33/2007 3 Keck et al., Burns 2012; Uhlig et al., Burns Nov. 33/2007; Highton et al., Burns 39/20134 Schwarze et al., Burns Nov. 33/2007; Everett at al., J. Wound Care 24/2015
MA-O-New
slette
r-201
7-10
/2-FIN
Related Documents











