UNCORRECTED PROOF 1 Microsystems technologies for drug delivery to the inner ear 2 Erin E. Leary Q1 Pararas a , David A. Borkholder b , Jeffrey T. Borenstein a, ⁎ 3 a Charles Stark Draper Laboratory, 555 Technology Square, Cambridge, MA 02139, USA 4 b Rochester Institute of Technology, Department of Electrical and Microelectronic Engineering, 79 Lomb Memorial Drive, Rochester, NY 14623, USA 5 6 abstract article info 7 Article history: 8 Received 31 August 2011 9 Accepted 15 February 2012 10 Available online xxxx 11 12 13 14 Keywords: 15 Cochlea 16 Intracochlear 17 Intratympanic 18 Hearing 19 Local drug delivery 20 Device 21 Micropump 22 Implantable 23 The inner ear represents one of the most technologically challenging targets for local drug delivery, but its 24 clinical significance is rapidly increasing. The prevalence of sensorineural hearing loss and other auditory dis- 25 eases, along with balance disorders and tinnitus, has spurred broad efforts to develop therapeutic compounds 26 and regenerative approaches to treat these conditions, necessitating advances in systems capable of targeted 27 and sustained drug delivery. The delicate nature of hearing structures combined with the relative inaccessi- 28 bility of the cochlea by means of conventional delivery routes together necessitate significant advancements 29 in both the precision and miniaturization of delivery systems, and the nature of the molecular and cellular 30 targets for these therapies suggests that multiple compounds may need to be delivered in a time- 31 sequenced fashion over an extended duration. Here we address the various approaches being developed 32 for inner ear drug delivery, including micropump-based devices, reciprocating systems, and cochlear 33 prosthesis-mediated delivery, concluding with an analysis of emerging challenges and opportunities for 34 the first generation of technologies suitable for human clinical use. These developments represent exciting 35 advances that have the potential to repair and regenerate hearing structures in millions of patients for 36 whom no currently available medical treatments exist, a situation that requires them to function with elec- 37 tronic hearing augmentation devices or to live with severely impaired auditory function. These advances also 38 have the potential for broader clinical applications that share similar requirements and challenges with the 39 inner ear, such as drug delivery to the central nervous system. 40 © 2012 Published by Elsevier B.V. 41 42 43 44 45 46 Contents 47 1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 48 2. Diseases of the inner ear . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 49 3. Inner ear physiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 50 4. Catheter and micropump-based delivery systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 51 5. Reciprocating microfluidic delivery system . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 52 6. Directed cochlear perfusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 53 7. Cochlear prosthesis-mediated delivery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 54 8. Emerging challenges . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 55 9. Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 56 Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 57 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 58 59 1. Introduction 60 The inner ear represents one of the most challenging target organs 61 for drug delivery, yet the potential clinical benefit to patients and the 62 size of the patient population are immense [1]. Conventional routes 63 such as oral delivery and injections are largely ineffective for several 64 reasons, principally because of the blood–cochlear barrier that blocks 65 most compounds from entering the inner ear from the bloodstream. 66 Further, drugs that are introduced systemically are likely to reach unin- 67 tended targets and may be toxic, and therefore progress toward develop- 68 ment of compounds capable of treating inner ear diseases including 69 hearing and balance disorders and tinnitus has been very limited. Most Advanced Drug Delivery Reviews xxx (2012) xxx–xxx ⁎ Corresponding author. E-mail address: [email protected] (J.T. Borenstein). ADR-12259; No of Pages 11 0169-409X/$ – see front matter © 2012 Published by Elsevier B.V. doi:10.1016/j.addr.2012.02.004 Contents lists available at SciVerse ScienceDirect Advanced Drug Delivery Reviews journal homepage: www.elsevier.com/locate/addr Please cite this article as: E.E.L. Pararas, et al., Microsystems technologies for drug delivery to the inner ear, Adv. Drug Deliv. Rev. (2012), doi:10.1016/j.addr.2012.02.004

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
2Q1
34
5
678910111213141516171819202122
43
44
4546
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
Advanced Drug Delivery Reviews xxx (2012) xxx–xxx
ADR-12259; No of Pages 11
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
F
Microsystems technologies for drug delivery to the inner ear
Erin E. Leary Pararas a, David A. Borkholder b, Jeffrey T. Borenstein a,⁎a Charles Stark Draper Laboratory, 555 Technology Square, Cambridge, MA 02139, USAb Rochester Institute of Technology, Department of Electrical and Microelectronic Engineering, 79 Lomb Memorial Drive, Rochester, NY 14623, USA
⁎ Corresponding author.E-mail address: [email protected] (J.T. Borens
0169-409X/$ – see front matter © 2012 Published by Eldoi:10.1016/j.addr.2012.02.004
Please cite this article as: E.E.L. Pararas, etdoi:10.1016/j.addr.2012.02.004
O
a b s t r a c t
a r t i c l e i n f o23
24
25
26
27
28
29
30
31
32
33
34
35
Article history:Received 31 August 2011Accepted 15 February 2012Available online xxxx
Keywords:CochleaIntracochlearIntratympanicHearingLocal drug deliveryDeviceMicropumpImplantable
36
37
38
39
40
CTED PROThe inner ear represents one of the most technologically challenging targets for local drug delivery, but its
clinical significance is rapidly increasing. The prevalence of sensorineural hearing loss and other auditory dis-eases, along with balance disorders and tinnitus, has spurred broad efforts to develop therapeutic compoundsand regenerative approaches to treat these conditions, necessitating advances in systems capable of targetedand sustained drug delivery. The delicate nature of hearing structures combined with the relative inaccessi-bility of the cochlea by means of conventional delivery routes together necessitate significant advancementsin both the precision and miniaturization of delivery systems, and the nature of the molecular and cellulartargets for these therapies suggests that multiple compounds may need to be delivered in a time-sequenced fashion over an extended duration. Here we address the various approaches being developedfor inner ear drug delivery, including micropump-based devices, reciprocating systems, and cochlearprosthesis-mediated delivery, concluding with an analysis of emerging challenges and opportunities forthe first generation of technologies suitable for human clinical use. These developments represent excitingadvances that have the potential to repair and regenerate hearing structures in millions of patients forwhom no currently available medical treatments exist, a situation that requires them to function with elec-tronic hearing augmentation devices or to live with severely impaired auditory function. These advances alsohave the potential for broader clinical applications that share similar requirements and challenges with theinner ear, such as drug delivery to the central nervous system.
© 2012 Published by Elsevier B.V.
4142
EContents
UNCO
RR
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 02. Diseases of the inner ear . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 03. Inner ear physiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 04. Catheter and micropump-based delivery systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 05. Reciprocating microfluidic delivery system . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 06. Directed cochlear perfusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 07. Cochlear prosthesis-mediated delivery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 08. Emerging challenges . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 09. Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0
62
63
64
65
1. Introduction
The inner ear represents one of the most challenging target organsfor drug delivery, yet the potential clinical benefit to patients and the
66
67
68
69tein).
sevier B.V.
al., Microsystems technologi
size of the patient population are immense [1]. Conventional routessuch as oral delivery and injections are largely ineffective for severalreasons, principally because of the blood–cochlear barrier that blocksmost compounds from entering the inner ear from the bloodstream.Further, drugs that are introduced systemically are likely to reach unin-tended targets andmay be toxic, and therefore progress toward develop-ment of compounds capable of treating inner ear diseases includinghearing and balance disorders and tinnitus has been very limited. Most
es for drug delivery to the inner ear, Adv. Drug Deliv. Rev. (2012),

T
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
200
2 E.E.L. Pararas et al. / Advanced Drug Delivery Reviews xxx (2012) xxx–xxx
UNCO
RREC
existing delivery approaches utilize direct injection of compounds intothe middle ear space, with a reliance on transport through the roundwindowmembrane (RWM) into the cochlea, a process that is inefficientbecause of enormous variability in drug diffusion rates due to anatomicdifferences between patients and limits on the achievable intracochleardrug concentration. The small size and relative inaccessibility of the co-chlea in humans present additional challenges regarding delivery mech-anisms; it is surrounded by the hardest bone in the body, and the coiledtubes within it are roughly 2 mm in diameter at their entrance and nar-row rapidly as they ascend toward the apex. Further, the hearing struc-tures within the cochlea are extremely delicate; in particular the haircells that line the basilar membrane within the organ of Corti (OC) arehighly sensitive to shear stresses and mechanical or chemical damagefrom a variety of sources. In addition to its sensitivity to fluid shear, thecochlea comprises afluid volumeof only 80 μl in humans and is thereforesusceptible to very small changes in total fluid volume. It is these consid-erations regarding the relative inaccessibility, small size and sensitivity ofthe inner ear that render it an ideal target for microsystems-based im-plantable drug delivery systems [2]. Many of these requirements associ-ated with miniaturization and precision are even more challengingconsiderations for the development of delivery platforms for pre-clinical studies in animals, where the total device volume and perilym-phatic fluid volume may be more than an order of magnitude smallerfor guinea pigs or mice relative to humans.
Recent advances in molecular biology related to regeneration ofsensory and neural cells within the inner ear point the way towardeventual treatments for hearing loss and other diseases [3]. The com-plex nature of regeneration and repair processes and the range of mo-lecular and cellular targets for regeneration highlight the need forprecisely controlled systems capable of delivering a broad range ofcompounds over extended periods of time. These compounds may in-clude apoptosis inhibitors, cytokines, neurotrophin ligands, antioxi-dants and gene therapy agents, and stem cell therapies, potentiallyintroduced in a complex timed-sequenced manner, with precise con-trol over delivery kinetics, transport mechanisms and binding reac-tions. These considerations heighten the requirements for nextgeneration delivery systems well beyond currently available implantsthat typically comprise drug-loaded polymer matrices that introducesingle compounds passively over limited periods of time [4]. Progresstoward safe and efficacious inner ear delivery systems will benefitfrom microsystems-based approaches, where multiple therapeuticcompounds can be introduced in a highly controlled and time-sequenced manner over periods of months to years, enabling precisecontrol over the drug concentration, kinetics andmolecular and cellu-lar targeting of therapies for hearing restoration.
Microsystems-based drug delivery systems are emerging for a rangeof clinical applications, and these capabilities have been leveraged towardthe inner ear [5–9]. As noted in these investigations, there are several as-pects of inner ear delivery that present specific technological challenges.These include the small space available for the delivery system, the ex-tended duration of treatment required for many diseases of the innerear, and the precise and gentlemanner inwhich drugsmay be introducedinto the delicate structures of the cochlea. These and other considerationslimit the applicability of many existing microsystems-based devices forinner ear delivery, and have spurred the development of novel technolo-gies and surgical approaches aimed at providing precisely controlled, ex-tended and safe delivery of compounds to the cochlea.
Here we will begin with an overview of clinical targets for therapyfor diseases of the inner ear, broadly classified as auditory and vestibulardisorders and tinnitus, followed by a review of inner ear physiology andrelevant considerations for delivery systems. We will then review fourbasic approaches for microfluidic inner ear delivery, includingmicropump-based systems, reciprocating approaches, directed perfu-sion and finally cochlear prosthesis-mediated delivery. Finally we willaddress emerging challenges and opportunities as these technologiesare advanced toward clinical practice.
Please cite this article as: E.E.L. Pararas, et al., Microsystems technologidoi:10.1016/j.addr.2012.02.004
ED P
RO
OF
2. Diseases of the inner ear
Diseases of the inner ear that represent targets of opportunity fordrug delivery approaches include a host of auditory diseases, vestibu-lar disorders, and tinnitus. Of these, by far the largest target patientpopulation suffers from SensoriNeural Hearing Loss (SNHL), whichoccurs because of damage to, or death of hair cells resulting fromaging, disease, noise exposure, or drug ototoxicity. Roughly 278 mil-lion individuals worldwide suffer from SNHL and over 1% of all chil-dren worldwide suffer from SNHL [3]. Hearing aids and cochlearprostheses represent the only currently available treatments forSNHL, but the total amplification possible with hearing aids is limitedand there are several other barriers to their use. Cochlear implanttechnology has advanced rapidly over the past several years, andtheir use for profound hearing loss has expanded dramatically. How-ever, there is growing interest and effort focused on the developmentof regenerative approaches for SNHL, with significant recent advancesin the understanding of cellular and molecular targets for regenera-tion. These advances are spurring efforts to develop delivery systemscapable of safely and efficaciously enabling a class of emerging thera-peutic compounds to reach these targets in the inner ear.
Noise-induced hearing loss (NIHL) and ototoxicity associated withvarious systemic drug therapies represent two additional majorcauses of hearing loss. The prevalence of NIHL is increasing rapidly,caused by either acute or chronic exposure to loud sounds, andsounds at or above 85 dB is associated with hearing loss when pa-tients are exposed to these levels over long periods of time [10]. Ex-posure to chronic loud noise leading to NIHL and tinnitus is one ofthe most prevalent injuries experienced by Armed Forces personnel[11]. Damage to both the hair cells and the auditory nerve occurs asa result of NIHL, largely associated with the formation of free radicalsin the inner ear. Rescue therapies delivered systemically are being in-vestigated as a means to treat NIHL, but direct delivery to the innerear is also being pursued using nanoparticle-based techniques and re-lated approaches [12]. Ototoxicity is frequently associatedwith chemo-therapy and radiation therapy in cancer patients, and is a particularlysevere concern with pediatric patients. Cisplatin-based chemotherapyresults in destruction of auditory sensory cells in large numbers(20–40%) of patients and is generally irreversible [13,14]. Platinumbinders and antioxidants have been explored as systemic approachesto limit otoxocity, but their use may result in a reduction in the efficacyof the cancer treatment. Therefore drug- and radiation-induced ototox-icity [15] represent important targets for local inner ear drug deliverythat would protect hearing without adversely affect the efficacy of theprimary treatment of the neoplasm.
Less common but very severe auditory diseases include conditionssuch as sudden sensorineural hearing loss (SSNHL) [16] and autoim-mune inner ear disease (AIED) [17–19]. High-dose systemic steroidtreatments are the principal route of therapy for both of these dis-eases, but are often associated with severe side effects that maycause the patient to terminate the medication and move to a cochlearimplant. Currently, intratympanic delivery and catheter-based ap-proaches to deliver drugs to the middle ear are used on some patientswith limited success. Direct delivery of steroids or other compoundsto the inner ear may represent a safer and more efficacious way totreat AIED and SSNHL.
Vestibular diseases represent a somewhat smaller patient populationbut comprise a set of potentially disabling conditions such as Meniere'sdisease, labyrinthitis and bilateral loss of labyrinthine function. Meniere'sdisease, or endolymphatic hydrops, represents a swelling offluid and con-comitant increase influid pressurewithin the cochlea that results in hear-ing loss, severe vertigo and pain, pressure and fullness of the affected ear[20–22]. Causes of this disease include trauma to the head, infections andallergy, and autoimmune disorders. Existing surgical and medical ap-proachesmay cause permanent loss of vestibular function [23], and there-fore interest is rising in therapeutic approaches involving the inner ear.
es for drug delivery to the inner ear, Adv. Drug Deliv. Rev. (2012),

TED P
RO
OF
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
257
258
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283
284
285
286
287
288
289
290
Fig. 1. (a.) A mid-modiolar section from a human temporal bone indicates the coiledstructure of the cochlea as itwinds around a centralmodiolius. Each segment (b.) contains3 fluid filled structures, the scala tympani (ST) scala media (SM) and scala vestibuli (SV).The organ of Corti (OC) is shown at the base of the SM.Used with permission from Elsevier [47].
3E.E.L. Pararas et al. / Advanced Drug Delivery Reviews xxx (2012) xxx–xxx
UNCO
RREC
Tinnitus, or ringing in the ears, affects 10% of the population andmay be debilitating in severe cases. Tinnitus is the most commoncomplaint reported by Armed Services personnel returning fromduty, and often results from exposure to loud noise or trauma andmay be accompanied by hearing loss. It is a particularly challengingtarget for therapy due to the complex nature of the condition andthe difficulty in quantifying tinnitus and the efficacy of therapeuticapproaches. Transtympanic injections with dexamethasone [24] andsteroids have achieved some success in reducing tinnitus while pre-serving hearing, but a direct intracochlear approach might ultimatelybe more effective in treatment of severe cases of tinnitus using one ofthe emerging therapeutic compounds currently being investigatedwith pump-based delivery systems.
3. Inner ear physiology
The inner ear is comprised of the cochlea, the auditory end organ,and the vestibular system for balance. It is housed deep in the petrousbone, the hardest bone in the body, near the brainstem. Its small sizecoupled with its inaccessibility presents unique challenges for drugdelivery. In addition, the sensitive and complex inner ear structuresare important considerations for drug delivery systems development.
The cochlea is a bony spiral filled with three fluid spaces that con-tinue longitudinally along the length of the spiral from apex to base. Itmeasures 31–33 mm long in humans [25], varies in diameter along itslength, and is bounded at the base by the round window and the ovalwindow. The RWM is highly compliant and bulges into the middle earspace when pressure is applied or fluid volume increases. It separatesthe fluid-filled space of the cochlea from the middle ear. The ovalwindow is connected to the stapes, a middle ear bone, and transmitsacoustic vibrations to the inner ear. The cochlea is a closed fluid sys-tem in humans, as the cochlear aqueduct connecting the scala tympa-ni (ST), one of the three coiled tubes in the cochlea, to cerebrospinalfluid (CSF) is generally not patent. However, in guinea pigs and inmice, two species often used in inner ear research, the cochlear aque-duct is open. This anatomic distinction between the species compli-cates analysis of drug delivery results and transfer of knowledgefrom animal testing to the clinical setting.
Stretching across themiddle of the cochlea is the OC, a basilar mem-brane holding the hair cells which are themechano-sensory cells of theinner ear. The hair cells are covered with stereocilia on their apical sur-face. The membrane moves in response to sound waves and is orga-nized tonotopically so that high frequency sounds cause the greatestmovement at the basal region where they are detected. Low frequencysounds, by contrast, cause greatermovement at the apex [26]. Hair cellsare arranged in rows that run the entire length of the cochlea. Threerows of outer hair cells amplify the motion of the basilar membrane tomore effectively stimulate the inner hair cells. One row of inner haircells releases a neurotransmitter in response to sound that excites affer-ent auditory neurons.
The three fluid spaces of the cochlea coil along with the OC frombase to apex. Viewed in cross-section, the upper and lower compart-ments are the scala vestibuli (SV) and the ST. They are filled peri-lymph, a fluid that is quite similar to CSF, and are in communicationwith each other at the apex through a structure known as the helico-trema. The round window is located at the base of the ST while the SVterminates at the oval window. The middle compartment, the scalamedia (SM), is filled with endolymph. The SM is bordered by theOC, with the apical surfaces of the cells lining the organ, includinghair cells, projecting into the SM. The structures of the inner ear areillustrated in Fig. 1.
Perilymph is the most abundant fluid in the cochlea, filling the STand SV. It bathes most of the cochlear cells, including hair cells in thebasal region and the neurons. The fluid is in diffusional continuitywith CSF. Relative to CSF, its composition is high in sodium ions andlow in potassium ions. However, protein concentration is significantly
Please cite this article as: E.E.L. Pararas, et al., Microsystems technologidoi:10.1016/j.addr.2012.02.004
higher (3 to 20 times) in the perilymph than in CSF [27–31]. This elevatedprotein concentration may be responsible for drug binding interactionsthat attenuate drug penetration during the delivery process [32]. Morethan one third of the proteins in perilymph comprise protease inhibitors,with serpins predominant. Additionally, apolipoproteins and enzymeseach constitute approximately 15% of the total protein content. The singlemost abundant protein is albumin at 14% [33]. In the human cochlea, thevolume of perilymph is about 70 μl, with 40 μl of that volume in the ST[34].
Endolymph fills the SM with a volume of approximately 8 μl inhuman. The ionic composition of endolymph is similar to the intracel-lular environment, high in potassium and low in sodium. The cellsthat line the SM form tight junctions, and this forms a unique envi-ronment for the apical surface of the hair cells. The compartment pro-vides an electrochemical environment with about 100 mV of positiveelectrical potential to support the hair cells' ability to transduce me-chanical motion into electrical potentials. The potential is maintainedby the stria vascularis, a structure running along the outside of theSM.
The coil of fluid compartments and OC wind around a centralstructure called the modiolus. The cell bodies of the auditory neurons,spiral ganglion neurons, are packed into the modiolus. The neuronssend dendrites to the inner hair cells and axons to the brain.
In the auditory process, a sound wave passes through the externalear and displaces the tympanic membrane, causing motion of the os-sicles, the three tiny middle ear bones. The stapes, the last bone in the
es for drug delivery to the inner ear, Adv. Drug Deliv. Rev. (2012),

T
291
292
293
294
295
296
297
298
299
300
301
302
303
304
305
306
307
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
336
337
338
339
340
341
342
343
344
345
346
347
348
349
350
351
352
353
354
355
356
357
358
359
360
361
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
385
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409
410
411
412
413
414
415
416
417
418
419
420
4 E.E.L. Pararas et al. / Advanced Drug Delivery Reviews xxx (2012) xxx–xxx
UNCO
RREC
series, transfers the motion to the fluid-filled space of the inner earbehind the oval window. The middle ear matches the acoustic imped-ance of the airborne sound to the fluid of the inner ear. Perilymphmotion causes the basilar membrane to move which in turn producesmotion of the stereocilia on the apical portion of the hair cells. Me-chanically sensitive ion channels on the stereocilia open and close,causing the hair cells to depolarize and repolarize. The inner haircells respond by releasing neurotransmitter from their base, whichactivates the auditory nerve fibers.
A number of electrophysiological parameters can be measured forcochlear function monitoring. Those used most often include distor-tion product otoacoustic emissions (DPOAEs) and auditory brainstemresponses (ABRs); both are non-invasive and are often used clinically.The DPOAEs serve as a monitor of outer hair cells. The mechanical re-sponse of the outer hair cell results in an acoustic signal propagatedback out through the auditory canal. These acoustic signals correspondto discrete frequencies and can be measured to non-invasively assesscochlear function. Using external electrodes, ABRsmonitor the synchro-nous activity of a group of nerve fibers in response to a click or tone pip.By varying the frequency of the tone pips, specific regions along thelength of the cochlea can be studied. Measurement of a related param-eter, the compound action potential, (CAP) requires an electrode to beplaced near the RWM.
4. Catheter and micropump-based delivery systems
Various systems have been developed to facilitate local delivery tothe inner ear. Early generations of devices were the Silverstein Micro-Wick™ and the Round Window Microcatheter™ (μCath) which havebeen used clinically to deliver agents to the intratympanic space,while the Alzet osmotic pump has been used in animal studies forboth intratympanic and intracochlear delivery to study a number ofapplications. The intratympanic delivery systems rely on diffusionthrough the RWM. Variability in thickness and composition of themembrane, along with potential loss of drug through the Eustachiantube, limit dosing control of drug reaching the inner ear. Intracochleardelivery requires a more invasive surgical technique. Cannulationthrough the round window or bony wall of the cochlea is mostoften used to gain direct access to the inner ear. An advantage ofthis approach is a greater degree of control over dosing relative tointratympanic approaches.
The MicroWick consists of an absorbent polyvinyl acetate wickthat is passed through a vent hole in the tympanic membrane andinserted to contact the round window. The wick absorbs medicationthat is administered in the external ear and transports it to theRWM for diffusion into the inner ear [35]. It can be placed underlocal anesthesia and allows patients to self-administer their treat-ment. The wick is removed at the conclusion of treatment.
Studies have shown the utility of the MicroWick in the treatmentof Meniere's disease, immune-mediated hearing loss, and suddenhearing loss. Patients suffering from vertigo due to Meniere's weredosed with gentamicin for 2 weeks in a study by Suryanarayanan. Re-sults showed good control of vertigo symptoms, but approximately aquarter of patients experienced some degree of hearing loss [36]. Inanother follow-up study, the authors concluded that long-term con-trol of vertigo symptoms can be achieved by gentamicin applicationusing the MicroWick, but they acknowledged that the optimum treat-ment paradigm has not yet been determined [37].
The MicroWick has been used for local delivery of steroids in thetreatment of AIED and in sudden deafness. Dexamethasone dropswere administered three times daily for 2 weeks, and about a thirdof patients with sudden deafness experienced improvement in hear-ing. Results were inconclusive for AIED patients due to the small sam-ple size [38]. Another study of methylprednisolone administeredthrough the MicroWick twice a day for 3 weeks also showed hearingimprovement in patients suffering from sudden hearing loss [39]. Van
Please cite this article as: E.E.L. Pararas, et al., Microsystems technologidoi:10.1016/j.addr.2012.02.004
ED P
RO
OF
Wijk reported on application of infliximab, a tumor necrosis factor αblocker, for the treatment of AIED. The pilot study resulted in im-proved hearing and reduced relapse [40].
The Round Window Microcatheter™ has been used clinically in anumber of applications. The catheter has two lumens, one for infusionand one for withdrawal, and has a rounded tip intended to be com-pressed into the bony niche next to the RWM. During anesthesia,the catheter is guided through the tympanic membrane and securedin place. The other end of the catheter exits the outer ear and canbe connected to various pumping systems for infusion of drug.
Several studies have reported on the use of the μCath for the treat-ment of Meniere's disease. One report on the infusion of low-dosegentamicin used a minipump from Disetronics attached to the cathe-ter to deliver for 10 days. The catheter was removed at the end oftreatment. Most patients experienced an elimination of vertigo andreduction in tinnitus associated with Meniere's, and hearingremained stable in all but one patient [41]. Similar improvement invertigo symptoms were seen in a long-term follow-up study [42].Two other studies reported significant improvement in vertigo butvariable and unacceptable levels of hearing loss. Authors discuss theneed to better control the dosage of gentamicin and better under-stand the disease and therapeutic mechanisms [43,44].
Plontke and colleagues have published research on the use of theμCath to locally deliver dexamethasone to patients suffering fromSSNHL. In these studies, a Panomat pump continuously deliveredthe glucocorticoid for 2–4 weeks, and the catheter was removed atthe conclusion. Typical infusion rates were on the order of 5 μl/h forperiods of up to 4 weeks. Results were mixed with one showing sta-tistically significant hearing improvement [45]. However, the othershowed minimal improvement over placebo. The authors did expresstheir belief that the results supported further investigation of thetechnique [46]. The location of the μCath implant in the round win-dow niche, shown in Fig. 2 of Ref. [46], necessitates reliance on addi-tional transport mechanisms through tissue to reach intracochleartargets.
Pre-clinical osmotic pumps have been used extensively both formiddle and inner ear delivery studies in animals. The small volumepump is subcutaneously implanted usually in rodents, and a cannulais routed to the round window niche or directly into the cochlea. Var-ious models allow for reservoir volumes of 0.1 to 2 ml and flow ratesfrom 0.1 to 10 μl/h, and the pumps provide continuous infusion for1 day to 6 weeks. The quantity of drug delivered over this periodcan greatly exceed the amount of perilymph in the cochlea, but theslow infusion rate allows for clearance mechanisms to equilibratetotal fluid volume. The pump operates by osmotic pressure in theouter section of the pump forcing drug in an inner, impermeablechamber out through the cannula. Delivery cannot be started orstopped nor can the flow rate be changed in situ. These devices areonly approved for laboratory studies and have not been used in clin-ical studies.
Osmotic pumps have been used to test therapies for a number ofinner ear disorders including NIHL, ototoxicity, vertigo, and others,and have been reviewed elsewhere [47]. Recent developments in-clude a study of betamethasone to treat a vestibular disorder in aguinea pig model, resulting in a shorter recovery time than the con-trol [48]. Another recent report of osmotic delivery involved sub-stance P, a neuropeptide in the class of tachykinins that has beenfound in abundant amounts in the vestibular system. Substance Pwas investigated for its influence on the system and its usefulnessin functional recovery in peripheral vestibular disorder. Resultsshowed that substance P caused excitatory actions in the vestibularsystem and therefore may hold the potential to be used as a treat-ment for patients suffering from vestibular dysfunction [49].
Emerging therapies to understand and treat hearing loss are beingtesting in guinea pigs using osmotic pumps. Gene therapy is a prom-ising approach for the treatment of hearing disorders, and a great deal
es for drug delivery to the inner ear, Adv. Drug Deliv. Rev. (2012),

TED P
RO
OF
421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454
455
456
457
458
459
460
461
462
463
464
465
466
467
468
469
470
471
472
473
474
475
476
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
496
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
Fig. 2. a. A schematic drawing of the reciprocating delivery system showing the flexiblemembrane and actuator. b. Photograph of wearable device for guinea pig studies. Thedevice measures 5.5×4.0×3.8 cm.Used with permission from Karger AG Basel and Springer [52,57].
5E.E.L. Pararas et al. / Advanced Drug Delivery Reviews xxx (2012) xxx–xxx
UNCO
RREC
of research is focused on non-viral methods of delivery. Linear poly-ethylenimine (PEI) has relatively low transfection efficiency, but sus-tained release from the osmotic pump improved efficiency andindicated the PEI presents an alternative for nonviral cochlear genetherapy [50].
The anti-apoptotic agent, z-VAD-FMK, is a caspase inhibitor. Thetherapeutic efficacy of this agent was tested in guinea pigs after noise-induced trauma by continuous infusion from an osmotic pump for14 days. Threshold shifts were less in the treated ear compared to theuntreated ear 2 days after exposure, and hair cell losses were signifi-cantly lower in the treated ear. Results suggest that the caspase path-way is involved in NIHL [51]. The versatility and ease of use of osmoticpumps in rodents will likely ensure their continued use in the study ofnovel therapies to treat inner ear disorders.
5. Reciprocating microfluidic delivery system
A team from Draper Laboratory and theMassachusetts Eye and Earis developing a reciprocating delivery system for direct intracochleardelivery [52]. The core of the delivery device is a reciprocating flowsystem for perfusion of drugs into the cochlear perilymph through asingle hole in the basal turn of the ST. The single cannula is directlyimplanted in the ST and acts as both inlet and outlet. Using the endog-enous perilymph as the carrier fluid for highly concentrated drug, thesystem repeatedly injects a small volume (0.2 to a few μl) of fluid intothe cochlea over a short (1–10 s) time, and then withdraws the lowerconcentrated perilymph into the device over a period of several mi-nutes. The critical elements of this device consist of an overall size con-sistent with surgical placement in a cavity formed within the mastoidspace behind the ear, a pumping element capable of infusing the druginto the cochlea, a valve-controlled drug reservoir, and integrationwith sensors for control of flow rate [53]. Studies have been conductedusing three-dimensional virtual reconstructions of human temporalbones to determine the appropriate overall size of the implant. A devicemeasuring 8.5 cm3 would accommodate 90% of patients [54].
The system operates by an actuator that applies cyclic pulses to amembrane covering the drug reservoir for delivery into the cochlea;relaxation of the actuator and the membrane permits return of thefluid to the system. The solenoid actuator impinges on the pumpingchamber's membrane to decrease its chamber volume and dispensesfluid from the reservoir into the cochlea. Releasing the membrane re-fills the system with cochlear fluid. The infusion and withdrawal cy-cles are timed such that substantial mixing of drug and perilymphoccurs in the cochlea. The refill step draws diluted fluid back intothe reservoir [55]. A diagram of the system and an example of a wear-able embodiment of the device for guinea pig studies are shown inFig. 2.
The reciprocating system is capable of safely accommodating thepulse volumes from the pump, restricting the flow into and out ofthe ear, and producing no net flow into the cochlea. Drug delivery oc-curs through diffusion and mixing of the high concentration fluidinjected into the inner ear, while lower concentration fluid isreturned to the device. Over time, no net volume change in the co-chlea occurs while the drug concentration in the cochlea increases.The intent of this method is to create a net increase in drug concen-tration while protecting the sensitive hair cells from changes in peri-lymph volume and pressure.
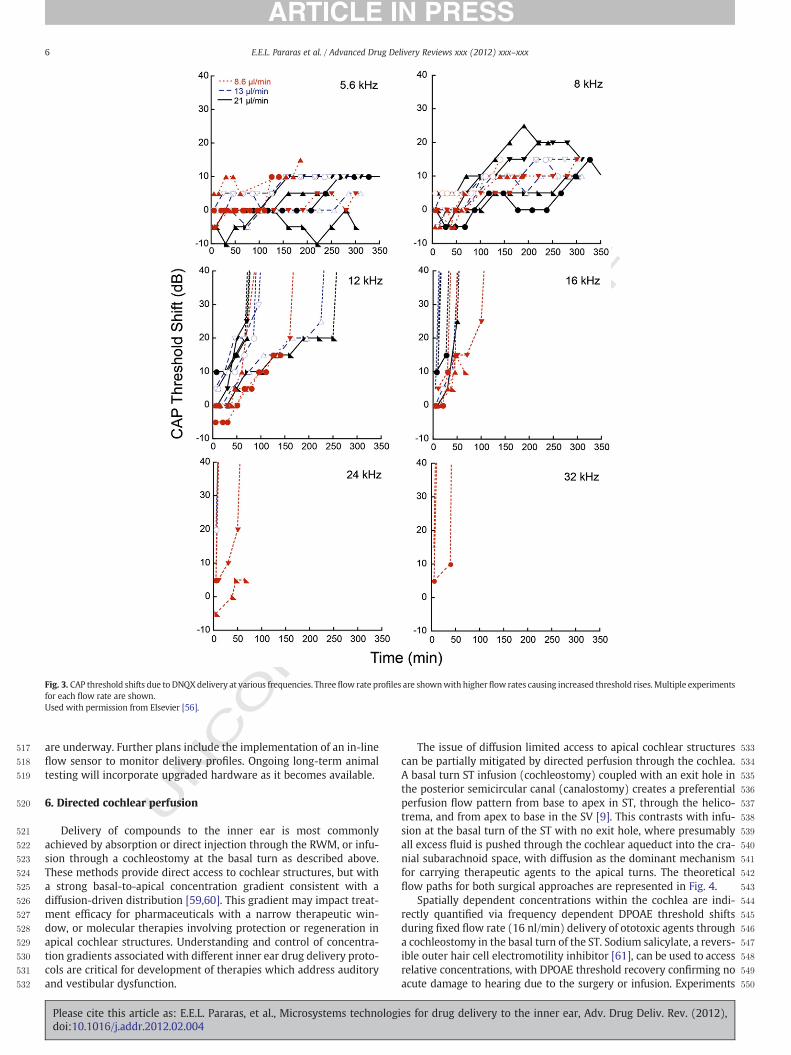
The system has been constructed and tested with acute delivery ofDNQX, a glutamate receptor blocker, in the guinea pig. Perfusion withthe control artificial perilymph showed no effect, while delivery ofDNQX showed a reversible, dose-dependent CAP threshold increase.The effect was also dependent on location along the length of the co-chlea with larger shifts at higher frequencies near the infusion loca-tion and decreasing shifts at lower frequencies in more apicalregions. DPOAEs, a measure of outer hair cell function, were not chan-ged which served as an internal control [53]. More recent studies
Please cite this article as: E.E.L. Pararas, et al., Microsystems technologidoi:10.1016/j.addr.2012.02.004
showed a threshold shift dependence on infusion flow rate with higherflow rates causing increased threshold rises [56], as shown in Fig. 3.
Initial modeling efforts of reciprocating drug distribution in thecochlea have been conducted using the data from these studies. Anal-ysis showed a strong dependence on diffusion, especially in regionsapical to the delivery site. Near the delivery site, flow rate effectswere seen. However, the study also showed what may be interpretedas a strong dependence on drug binding [56]. As discussed above inthe physiology section, many types of proteins that are known tobind drugs in plasma were identified in perilymph, including albuminand apolipoproteins [33]. Current efforts are underway to construct anumerical model to incorporate diffusion, reaction, convention, andother mechanisms important in understanding drug distribution.
To enable long-term wearable testing, a self-contained, program-mable system was built. It was designed to weigh less than 50 g andsized at approximately 80 cm3 to facilitate mounting on the skull ofadult guinea pigs. The system runs in an uninterrupted fashion fortwo weeks and allows extended testing of the device functionalityand drug distribution [57]. In order tomeet the size andweight require-ments, the delivery device was further miniaturized and fabricated fromlaminated layers of polyimide sheets thatweremachined using standardXYmilling tables [58]. The laminated portions comprise a flexible mem-brane covering the displacement chamber, valves, and channels. Themembrane is depressed using a commercially-available mini-actuator[55]. The electronic control system was custom-designed and built in-house and powered by lithium polymer batteries. It enables wirelessprogrammability with a standard infrared remote control.
Future directions are focused on continued miniaturization andincreased functionality. A reservoir capable of storing highly concen-trated drug and controlling dosing is being fabricated using identicallaminate fabrication techniques and tested. Additionally, designs forcustom micro-actuators in order to actuate the reciprocating system
es for drug delivery to the inner ear, Adv. Drug Deliv. Rev. (2012),
ORRECTED P
RO
OF
517
518
519
520
521
522
523
524
525
526
527
528
529
530
531
532
533
534
535
536
537
538
539
540
541
542
543
544
545
546
547
548
549
550
Fig. 3. CAP threshold shifts due to DNQXdelivery at various frequencies. Threeflow rate profiles are shownwith higherflow rates causing increased threshold rises.Multiple experimentsfor each flow rate are shown.Used with permission from Elsevier [56].
6 E.E.L. Pararas et al. / Advanced Drug Delivery Reviews xxx (2012) xxx–xxx
UNCare underway. Further plans include the implementation of an in-line
flow sensor to monitor delivery profiles. Ongoing long-term animaltesting will incorporate upgraded hardware as it becomes available.
6. Directed cochlear perfusion
Delivery of compounds to the inner ear is most commonlyachieved by absorption or direct injection through the RWM, or infu-sion through a cochleostomy at the basal turn as described above.These methods provide direct access to cochlear structures, but witha strong basal-to-apical concentration gradient consistent with adiffusion-driven distribution [59,60]. This gradient may impact treat-ment efficacy for pharmaceuticals with a narrow therapeutic win-dow, or molecular therapies involving protection or regeneration inapical cochlear structures. Understanding and control of concentra-tion gradients associated with different inner ear drug delivery proto-cols are critical for development of therapies which address auditoryand vestibular dysfunction.
Please cite this article as: E.E.L. Pararas, et al., Microsystems technologidoi:10.1016/j.addr.2012.02.004
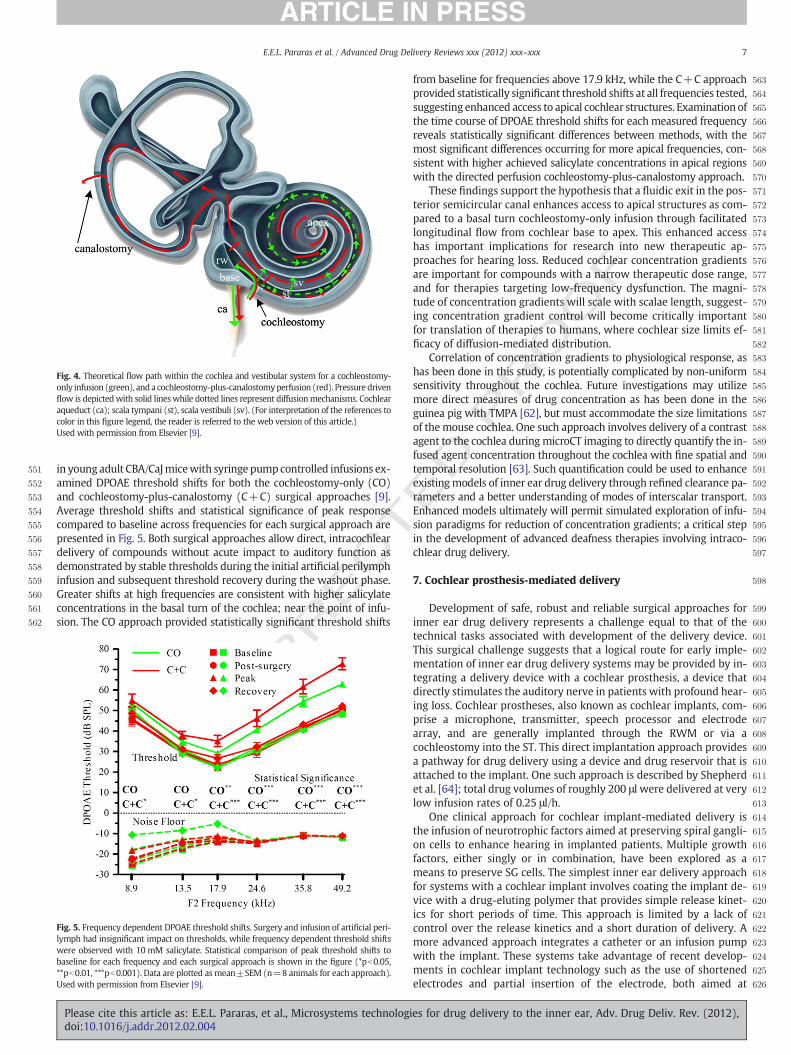
The issue of diffusion limited access to apical cochlear structurescan be partially mitigated by directed perfusion through the cochlea.A basal turn ST infusion (cochleostomy) coupled with an exit hole inthe posterior semicircular canal (canalostomy) creates a preferentialperfusion flow pattern from base to apex in ST, through the helico-trema, and from apex to base in the SV [9]. This contrasts with infu-sion at the basal turn of the ST with no exit hole, where presumablyall excess fluid is pushed through the cochlear aqueduct into the cra-nial subarachnoid space, with diffusion as the dominant mechanismfor carrying therapeutic agents to the apical turns. The theoreticalflow paths for both surgical approaches are represented in Fig. 4.
Spatially dependent concentrations within the cochlea are indi-rectly quantified via frequency dependent DPOAE threshold shiftsduring fixed flow rate (16 nl/min) delivery of ototoxic agents througha cochleostomy in the basal turn of the ST. Sodium salicylate, a revers-ible outer hair cell electromotility inhibitor [61], can be used to accessrelative concentrations, with DPOAE threshold recovery confirming noacute damage to hearing due to the surgery or infusion. Experiments
es for drug delivery to the inner ear, Adv. Drug Deliv. Rev. (2012),
T
551
552
553
554
555
556
557
558
559
560
561
562
563
564
565
566
567
568
569
570
571
572
573
574
575
576
577
578
579
580
581
582
583
584
585
586
587
588
589
590
591
592
593
594
595
596
597
598
599
600
Fig. 4. Theoretical flow path within the cochlea and vestibular system for a cochleostomy-only infusion (green), and a cochleostomy-plus-canalostomyperfusion (red). Pressure drivenflow is depicted with solid lineswhile dotted lines represent diffusionmechanisms. Cochlearaqueduct (ca); scala tympani (st), scala vestibuli (sv). (For interpretation of the references tocolor in this figure legend, the reader is referred to the web version of this article.)Used with permission from Elsevier [9].
7E.E.L. Pararas et al. / Advanced Drug Delivery Reviews xxx (2012) xxx–xxx
EC
in young adult CBA/CaJmicewith syringe pumpcontrolled infusions ex-amined DPOAE threshold shifts for both the cochleostomy-only (CO)and cochleostomy-plus-canalostomy (C+C) surgical approaches [9].Average threshold shifts and statistical significance of peak responsecompared to baseline across frequencies for each surgical approach arepresented in Fig. 5. Both surgical approaches allow direct, intracochleardelivery of compounds without acute impact to auditory function asdemonstrated by stable thresholds during the initial artificial perilymphinfusion and subsequent threshold recovery during the washout phase.Greater shifts at high frequencies are consistent with higher salicylateconcentrations in the basal turn of the cochlea; near the point of infu-sion. The CO approach provided statistically significant threshold shifts
UNCO
RR 601
602
603
604
605
606
607
608
609
610
611
612
613
614
615
616
617
618
619
620
621
622
623
624
625
626
Fig. 5. Frequency dependent DPOAE threshold shifts. Surgery and infusion of artificial peri-lymph had insignificant impact on thresholds, while frequency dependent threshold shiftswere observed with 10 mM salicylate. Statistical comparison of peak threshold shifts tobaseline for each frequency and each surgical approach is shown in the figure (*pb0.05,**pb0.01, ***pb0.001). Data are plotted as mean±SEM (n=8 animals for each approach).Used with permission from Elsevier [9].
Please cite this article as: E.E.L. Pararas, et al., Microsystems technologidoi:10.1016/j.addr.2012.02.004
ED P
RO
OF
from baseline for frequencies above 17.9 kHz, while the C+C approachprovided statistically significant threshold shifts at all frequencies tested,suggesting enhanced access to apical cochlear structures. Examination ofthe time course of DPOAE threshold shifts for each measured frequencyreveals statistically significant differences between methods, with themost significant differences occurring for more apical frequencies, con-sistent with higher achieved salicylate concentrations in apical regionswith the directed perfusion cochleostomy-plus-canalostomy approach.
These findings support the hypothesis that a fluidic exit in the pos-terior semicircular canal enhances access to apical structures as com-pared to a basal turn cochleostomy-only infusion through facilitatedlongitudinal flow from cochlear base to apex. This enhanced accesshas important implications for research into new therapeutic ap-proaches for hearing loss. Reduced cochlear concentration gradientsare important for compounds with a narrow therapeutic dose range,and for therapies targeting low-frequency dysfunction. The magni-tude of concentration gradients will scale with scalae length, suggest-ing concentration gradient control will become critically importantfor translation of therapies to humans, where cochlear size limits ef-ficacy of diffusion-mediated distribution.
Correlation of concentration gradients to physiological response, ashas been done in this study, is potentially complicated by non-uniformsensitivity throughout the cochlea. Future investigations may utilizemore direct measures of drug concentration as has been done in theguinea pig with TMPA [62], but must accommodate the size limitationsof themouse cochlea. One such approach involves delivery of a contrastagent to the cochlea during microCT imaging to directly quantify the in-fused agent concentration throughout the cochlea with fine spatial andtemporal resolution [63]. Such quantification could be used to enhanceexistingmodels of inner ear drug delivery through refined clearance pa-rameters and a better understanding of modes of interscalar transport.Enhanced models ultimately will permit simulated exploration of infu-sion paradigms for reduction of concentration gradients; a critical stepin the development of advanced deafness therapies involving intraco-chlear drug delivery.
7. Cochlear prosthesis-mediated delivery
Development of safe, robust and reliable surgical approaches forinner ear drug delivery represents a challenge equal to that of thetechnical tasks associated with development of the delivery device.This surgical challenge suggests that a logical route for early imple-mentation of inner ear drug delivery systems may be provided by in-tegrating a delivery device with a cochlear prosthesis, a device thatdirectly stimulates the auditory nerve in patients with profound hear-ing loss. Cochlear prostheses, also known as cochlear implants, com-prise a microphone, transmitter, speech processor and electrodearray, and are generally implanted through the RWM or via acochleostomy into the ST. This direct implantation approach providesa pathway for drug delivery using a device and drug reservoir that isattached to the implant. One such approach is described by Shepherdet al. [64]; total drug volumes of roughly 200 μl were delivered at verylow infusion rates of 0.25 μl/h.
One clinical approach for cochlear implant-mediated delivery isthe infusion of neurotrophic factors aimed at preserving spiral gangli-on cells to enhance hearing in implanted patients. Multiple growthfactors, either singly or in combination, have been explored as ameans to preserve SG cells. The simplest inner ear delivery approachfor systems with a cochlear implant involves coating the implant de-vice with a drug-eluting polymer that provides simple release kinet-ics for short periods of time. This approach is limited by a lack ofcontrol over the release kinetics and a short duration of delivery. Amore advanced approach integrates a catheter or an infusion pumpwith the implant. These systems take advantage of recent develop-ments in cochlear implant technology such as the use of shortenedelectrodes and partial insertion of the electrode, both aimed at
es for drug delivery to the inner ear, Adv. Drug Deliv. Rev. (2012),

T
627
628
629
630
631
632
633
634
635
636
637
638
639
640
641
642
643
644
645
646
647
648
649
650
651
652
653
654
655
656
657
658
659
660
661
662
663
664
665
666
667
668
669
670
671
672
673
674
675
676
677
678
679
680
681
682
683
684
685
686
687
688
689
690
691
692
693
694
695
696
697
698
699
700
701
702
703
704
705
706
707
708
709
710
711
712
713
714
715
716
8 E.E.L. Pararas et al. / Advanced Drug Delivery Reviews xxx (2012) xxx–xxx
RREC
avoiding structural damage during insertion of the implant. Biore-sorbable coatings applied to the surface of the cannula appear to re-duce insertion forces, and the infusion of steroids at the time ofimplantation may minimize surgical trauma. A single-use catheterwith syringe delivery represents the simplest implementation ofthis approach, but infusion pumps have also been explored forlonger-term delivery. One interesting approach to achieve longer-term delivery is laser machining of the cannula to generate multipledelivery ports that will improve apical distribution of the drug. Holediameters as small as 50 μm have been machined into the cannulato enhance drug distribution profiles, as shown in Fig. 6 [65].
8. Emerging challenges
Drug delivery to the inner ear without damaging hearing remainsa significant challenge. Microsystems technologies continue to play akey role in addressing these challenges and will ultimately yield solu-tions that overcome the limitations of currently available prostheses.Delivery of agents to the cochlea in animal models presents signifi-cant size constraints which are spurring innovations that aid therapydevelopment, and may enable new opportunities in human transla-tional results.
Drug delivery to the inner ear in animal models presents specificchallenges associated with size, fluid volumes, the cochlear interface,and chronic delivery. Generally a small capillary tube, either polyi-mide or polyimide coated fused silica, is used to connect the pumpsystem to the cochlea. The diameter of the target scalae at the pointof infusion determines maximal allowable insertion depth into thecochleostomy, which for the mouse can be smaller than 200 μm.This is generally controlled either by use of a micromanipulator andmicroscope visualization by the surgeon, or by creation of an inser-tion stop on the cannula. The latter requires precise placement ofthe insertion stop to control insertion depth; precision which is diffi-cult to achieve using manual production methods. A micromachinedmold approach which provides precise control of insertion depthwith a silastic insertion stop has been demonstrated [66]. A siliconmold was created using standard micromachining fabrication pro-cesses, involving a combination of anisotropic KOH etching and abackside aligned circular deep reactive ion etch which allows the can-nula tubing to be inserted through the mold. The molding process andresulting cannula with molded insertion stop are shown in Fig. 7. Themold fabrication process and molding techniques permit insertiondepth control within 5 μm with a controllable interface area to pro-mote robust sealing to the tympanic bulla at the cochleostomy site.
The low fluid volumes (b10 μl) and flow rates (b50 nl/min) asso-ciated with small rodent inner ear drug delivery dictate precise
UNCO 717
718
719
720
721
722
723
724
725
726
727
728
729
730
731
732
733
734
735
736
Fig. 6. Illustration of drug delivery enabled by laser-drilled holes of 50 μm diameter toenable enhanced drug distribution in the cochlea.Used with permission from Elsevier [64].
Please cite this article as: E.E.L. Pararas, et al., Microsystems technologidoi:10.1016/j.addr.2012.02.004
ED P
RO
OF
control of fluidic interfaces and entrapped air in the fluidic system.While entrapped air can be used to separate fluids for diffusion isola-tion within the capillary tubing [9] the volumes must remain small(a few nl) to avoid errors in infused volumes. Larger volumes(>0.5 μl) of air result in compression during pumping and delayedflow to the cannula outlet. Leaks in the system at fluidic interfacesor defects in the cannula tubing can drastically impact actual flowrates. Thus, each experiment requires careful verification thatintended flow rates are achieved, using microscope-based observa-tion as well as measurement of interface movement distances overtime.
Chronic infusions require departure from syringe pump systems ifthe complications of tethering are to be avoided. Backpack systemsallow inclusion of power, the micropump, control electronics, and areservoir of the drug to be delivered. As drug infusion systems shrinkin size, implantation becomes another possible alternative for chronicinfusions.
Inner ear drug delivery with implantable microsystems presentssignificant challenges and unique requirements, including accuratedosing at low flow rates, low voltage operation, a fluid flow pathwith controlled characteristics, and the ability to interface to infusiontubing. Emerging technologies are beginning to address these chal-lenges in a platform targeted for implantation in the mouse, butwith scalability to larger animals and potentially humans [67].
Accurate dosing requires control of flow rates, ideally with sensingfeedback for confirmation of achieved flow. In the laminar, low flowrate regime, sensing is most easily accomplished through the use ofa thermal anemometer. A resistive element generates heat that istransferred to the fluid, with the rate of heat transfer correlated tothe fluid flow rate. The bridge structure within the resistor consistsof a boron-doped polysilicon heater encapsulated by silicon oxideand silicon nitride, with the dimensions optimized to balance sensi-tivity, efficiency and mechanical robustness.
The fluid flow path within an implantable micropump must benon-reactive, non-water absorbing and biocompatible. A process forthe creation of deformable diaphragms over pump chambers andchannels with simultaneous coating of channel surfaces has been de-veloped, enabling integration of a biocompatible fluid flow path. Theprocess utilizes an oxide mask patterned with line/space pairs to de-fine fluidic channels and pump chambers, which are then isotropicallyetched in the silicon substrate through the mask. Subsequent deposi-tion of Parylene-C (chlorinated poly-para-xylylene), a biocompatiblepolymer with a long mean free path in the vapor phase, provides acoating for the interior surfaces of the fluidic channels. Continued de-position encapsulates the oxide hard mask, sealing the cavities andcreating deformable membranes over the pump chambers.
Capillary tubing is generally used to connect the micropump sys-tem to the cochlea for inner ear drug delivery. Coupling to the micro-fluidic system can add unacceptable volume for implant applicationsif additional coupling structures or out-of-plane approaches are uti-lized. Adhesives, epoxies and elastomers for coupling can result inblocked capillaries and/or gap formation and dead volumes. Recentadvances in in-plane interconnects for small diameter capillary tub-ing has significantly reduced overall fluidic interconnect volumewhile minimizing gap formation and eliminating blocked capillaries[68]. This robust interconnect technology requires only a singlemask level, and leverages deposition of parylene-C onto room tem-perature surfaces to capture small diameter capillary tubing.Parylene-C provides the requisite controlled deposition of a biocom-patible sealing material into the small spaces between the capillaryand the microfluidic channel. The characteristics of Parylene-C depo-sition into channels were invoked in conjunction with equations de-scribing molecular flow and diffusion to spatially model monomerconcentration and to estimate the polymer deposition within taperedchannels. Modeling of the deposition process permitted optimizationof channel geometries for full gap filling without voids at the tubing/
es for drug delivery to the inner ear, Adv. Drug Deliv. Rev. (2012),

T
OO
F
737
738
739
740
741
742
743
744
745
746
747
748
749
750
751
752
753
754
755
756
757
758
759
760
761
762
763
764
765
766
767
768
769
770
771
772
773
774
775
776
777
778
779
780
Fig. 7. Micromolded cannula insertion stops. (Left) Polyimide micro-tubing is inserted through a micromachined silicon mold, with a precise volume of Silastic delivered and thetubing cut to length following Silastic cure. (Right) Scanning electron micrograph of the cannula with integrated insertion stop. Inset is tubing tip (magnification 320×). Insertiondepth is A, the contact area for bonding is defined by dimensions B and C, and post-cut roundness is defined by D and E.Used with permission from IEEE [65].
9E.E.L. Pararas et al. / Advanced Drug Delivery Reviews xxx (2012) xxx–xxx
RREC
channel interface. Devices based on this process modeling have beenfabricated and characterized for voids along the length of the inter-connect, burst/leakage pressure, and pull strength. The interconnectsoccupied a total volume of 0.018 mm3 (18 nl), had zero dead volume,held 120 psi pressure, and exhibited a pull strength of 2.9 N with aninsertion depth of only 500 μm. An image of a microcapillary exitingthe side of the microfluidic chip is shown in Fig. 8.
Pumps for implantable applications may require the developmentof low voltage actuation systems which can be integrated over de-formable pump membranes as an alternative to high voltage piezo-electrics. Thermo-pneumatic actuation is one approach recentlyinvestigated for inner ear drug delivery systems. Using direct writedispensing technologies, multilayer structures were written over afour chamber peristaltic micropump consisting of pump chambers,channels and interconnects [69]. This hybrid MEMS approach allowsutilization of aspects of both traditional MEMS and emerging directwrite MEMS fabrication capabilities, and may potentially expand thepool of available actuation technologies that can be easily integratedwith microsystems-based pump systems.
One of the principal challenges in intracochlear drug delivery isthe avoidance of biofouling of implanted devices during extended de-livery. This challenge necessitates the use of highly biocompatiblematerials for all components in contact with biological fluids such
UNCO 781
782
783
784
785
786
787
788
789
790
791792793794795Q2796797798799
Fig. 8. SEM of the side of the microfluidic chip with small diameter (140-μmOD) tubingexiting in-plane.Used with permission from IEEE [67].
Please cite this article as: E.E.L. Pararas, et al., Microsystems technologidoi:10.1016/j.addr.2012.02.004
ED P
Ras perilymph, and robust encapsulation of device elements that maybe prone to fouling or trigger inflammatory responses such as electroniccomponents, power sources and flow sensors. Foulingmechanisms andgeneral biocompatibility may be associated with chemical interactionswith thematerial surfaces themselves, but may also involvemechanicalfactors such as the relative stiffness or compliance of tubing, wiring anddevice structures that may impart stresses to the surrounding tissue.Another critical aspect of biofouling is the danger of partial or total oc-clusion of the delivery cannula itself, due to crystallization of the drug,protein coating of the surface of the inner lumen, or other related phe-nomena. The slow infusion rates used in most systems may exacerbatethis process because they do not provide sufficient pumping forces toclear blockages as they form in the delivery tubing.
9. Summary
The inner ear is a complex organ requiring special considerationsfor drug delivery. Challenges including small size, inaccessibility,and delicate pressure-sensitive structures necessitate capabilities be-yond those of most common microsystems-based approaches for thisapplication. These challenges present opportunities for novel micro-systems uniquely designed for delivery to the inner ear. Researchersare developing methods including micropumps, reciprocating sys-tems, directed cochlear perfusion, and cochlear prosthesis-based sys-tems that hold great promise in treating the unmet needs of manypatients suffering from inner ear diseases and for whom currenttreatments are limited.
Acknowledgments
This publication was made possible by grant numbers 5 R01 DC006848-02 and 5 K25-DC008291 from the NIH, and its contents aresolely the responsibility of the authors and do not necessarily representthe official views of the NIH or the U.S. government.
References
[1] E.E. Swan, M.J. Mescher, W.F. Sewell, S.L. Tao, J.T. Borenstein, Inner ear drug deliveryfor auditory applications, Adv. Drug Deliv. Rev. 60 (2008) 1583–1599.
[2] A.A. McCall, E.E. Swan, J.T. Borenstein, W.F. Sewell, S.G. Kujawa, M.J. McKenna,Drug delivery for treatment of inner ear disease: current state of knowledge, EarHear. 31 156–165.
[3] M.C. Holley, The auditory system, hearing loss and potential targets for drugdevelopment, Drug Discov. Today 10 (2005) 1269–1282.
[4] W.M. Saltzman, Drug Delivery: Engineering Principles for Drug Therapy, OxfordUniversity Press, New York, 2001.
es for drug delivery to the inner ear, Adv. Drug Deliv. Rev. (2012),

T
800801802803804805806807808809810811812813814815816817818819820821822823824825826827828829830831832833834835836837838839840841842843844845846847848849850851852853854855856857858859860861862863864865866867868869870871872873874875876877878879880881882883884885
886887888889890891892893894895896897898899900901902903904905906907908909910911912913914915916917918919920921922923924925926927928929930931932933934935936937938939940941942943944945946947948949950951952953954955956957958959960961962963964965966967968969970971
10 E.E.L. Pararas et al. / Advanced Drug Delivery Reviews xxx (2012) xxx–xxx
UNCO
RREC
[5] Z. Chen, S.G. Kujawa, M.J. McKenna, J.O. Fiering, M.J. Mescher, J.T. Borenstein, E.E.Swan, W.F. Sewell, Inner ear drug delivery via a reciprocating perfusion system inthe guinea pig, J. Control. Release 110 (2005) 1–19.
[6] J. Fiering, M.J. Mescher, E.E. Leary Swan, M.E. Holmboe, B.A. Murphy, Z. Chen, M.Peppi, W.F. Sewell, M.J. McKenna, S.G. Kujawa, J.T. Borenstein, Local drug deliverywith a self-contained, programmable, microfluidic system, Biomed. Microdevices11 (2009) 571–578.
[7] M.J. Mescher, E.E. Swan, J. Fiering, M.E. Holmboe, W.F. Sewell, S.G. Kujawa, M.J.McKenna, J.T. Borenstein, Fabrication methods and performance of low-permeability microfluidic components for a miniaturized wearable drug deliverysystem, J. Microelectromech. Syst. 18 (2009) 501–510.
[8] D.A. Borkholder, State-of-the-art mechanisms of intracochlear drug delivery,Curr. Opin. Otolaryngol. Head Neck Surg. 16 (2008) 472–477.
[9] D.A. Borkholder, X. Zhu, B.T. Hyatt, A.S. Archilla, W.J. Livingston 3rd, R.D. Frisina,Murine intracochlear drug delivery: reducing concentration gradients withinthe cochlea, Hear. Res. 268 (2010) 2–11.
[10] E.D. Lynch, J. Kil, Compounds for the prevention and treatment of noise-inducedhearing loss, Drug Discov. Today 10 (2005) 1291–1298.
[11] R.G. DePalma, D.G. Burris, H.R. Champion, M.J. Hodgson, Blast injuries, N. Engl. J.Med. 352 (2005) 1335–1342.
[12] I. Sendowski, L. Abaamrane, F. Raffin, A. Cros, D. Clarencon, Therapeutic efficacy ofintra-cochlear administration of methylprednisolone after acoustic traumacaused by gunshot noise in guinea pigs, Hear. Res. 221 (2006) 119–127.
[13] L. Rybak, Mechanisms of cisplatin ototoxicity and progress in otoprotection, Curr.Opin. Otolaryngol. Head Neck Surg. 15 (2007) 364–369.
[14] L.P. Rybak, C.A. Whitworth, Ototoxicity: therapeutic opportunities, Drug Discov.Today 10 (2005) 1313–1321.
[15] N. Bhandare, P.J. Antonelli, C. Morris, R.S. Malayapa, W.M. Mendenhall, Ototoxicityafter radiotherapy for head and neck tumors, Int. J. Radiat. Oncol. Biol. Phys. 67(2007) 469–479.
[16] I. Mosnier, D. Bouccara, O. Sterkers, Management of idiopathic sudden sensorineuralhearing loss, Oto Rhino Laryngol. Nova 9 (1999) 217–223.
[17] A.F. Ryan, J.P. Harris, E.M. Keithley, Immune-mediated hearing loss: basicmechanismsand options for therapy, Acta Otolaryngol. 548 (2002) 38–43 Suppl.
[18] G.S. Yang, H.T. Song, E.M. Keithley, J.P. Harris, Intratympanic immunosuppressivesfor prevention of immune-mediated sensorineural hearing loss, Am. J. Otol. 21(2000) 499–504.
[19] E.L. Matteson, D.A. Fabry, S.E. Strome, C.L. Driscoll, C.W. Beatty, T.J. McDonald,Autoimmune inner ear disease: diagnostic and therapeutic approaches in a multi-disciplinary setting, J. Am. Acad. Audiol. 14 (2003) 225–230.
[20] S.G. Harner, C.L. Driscoll, G.W. Facer, C.W. Beatty, T.J. McDonald, Long-termfollow-up of transtympanic gentamicin for Meniere's syndrome, Otol. Neurotol.22 (2001) 210–214.
[21] S.G. Harner, J.L. Kasperbauer, G.W. Facer, C.W. Beatty, Transtympanic gentamicinfor Meniere's syndrome, Laryngoscope 108 (1998) 1446–1449.
[22] S.H. Chia, A.C. Gamst, J.P. Anderson, J.P. Harris, Intratympanic gentamicin therapyfor Meniere's disease: a meta-analysis, Otol. Neurotol. 25 (2004) 544–552.
[23] M.E. Hoffer, K. Allen, R. Kopke, P.Weisskopf, K.R. Gottshall, D.Wester, Transtympanicversus sustained-release administration of gentamicin: kinetics; morphology; andfunction, Laryngoscope 111 (2001) 1343–1357.
[24] M.E. Hoffer, D. Wester, R.D. Kopke, P. Weisskopf, K. Gottshall, Transtympanicmanagement of tinnitus, Otolaryngol. Clin. N. Am. 36 (2003) 353–358.
[25] H. Schuknecht, Pathology of the Ear, Lea and Febiger, Malvern, PA, 1993.[26] J. Tsuji, M.C. Liberman, Intracellular labeling of auditory nerve fibers in guinea
pig: central and peripheral projections, J. Comp. Neurol. 381 (1997) 188–202.[27] R. Thalmann, T. Comegys, I. Thalmann, Amino acid profiles in inner ear fluids and
cerebrospinal fluid, Laryngoscope 92 (1982) 321–328.[28] I. Thalmann, R. Kohut, J. Ryu, R. Thalmann, High resolution two-dimensional electro-
phoresis: technique and potential applicability to the study of inner ear disease, Am.J. Otol. 16 (1995) 153–157.
[29] I. Thalmann, R. Kohut, J. Ryu, T. Comegys, M. Senarita, R. Thalmann, Protein profileof human perilymph: in search of markers for the diagnosis of perilymph fistulaand other inner ear disease, Otolaryngol. Head Neck Surg. 111 (1994) 273–280.
[30] F. Scheibe, H. Haupt, Biochemical differences between perilymph, cerebrospinalfluid and blood plasma in the guinea pig, Hear. Res. 17 (1985) 61–66.
[31] J. Medina, D. Drescher, The amino-acid content of perilymph and cerebrospinalfluid from guinea-pigs and the effect of noise on the amino-acid composition ofperilymph, Neuroscience 6 (1981) 505–509.
[32] E.E. Swan, M. Peppi, Z. Chen, K.M. Green, J.E. Evans, M.J. McKenna, M.J. Mescher,S.G. Kujawa, W.F. Sewell, Proteomics analysis of perilymph and cerebrospinalfluid in mouse, Laryngoscope 119 (2009) 953–958.
[33] E.E.L. Swan, M. Peppi, Z. Chen, K.M. Green, J.E. Evans, M.J. McKenna, M.J. Mescher,S.G. Kujawa, W.F. Sewell, Proteomics analysis of perilymph and cerebrospinalfluid in mouse, Laryngoscope 119 (2009) 953–958.
[34] M. Igarashi, K. Ohashi, M. Ishii, Morphometric comparison of endolymphatic and peri-lymphatic spaces in human temporal bones, Acta Otolaryngol. 101 (1986) 161–164.
[35] H. Silverstein, Use of a new device, the MicroWick, to deliver medication to theinner ear, Ear Nose Throat J. 78 (1999) 595–600.
[36] R. Suryanarayanan, V.R. Srinivasan, G. O'Sullivan, Transtympanic gentamicintreatment using Silverstein MicroWick in Meniere's disease patients: long termoutcome, J. Laryngol. Otol. 123 (2009) 45–49.
[37] S.L. Hill, N.B. Digges, H. Silverstein, Long-term follow-up after gentamicin applicationvia the SilversteinMicroWick in the treatment ofMeniere's disease, Ear Nose ThroatJ. 85 (2006) 494–498.
[38] H. Silverstein, L.E. Jackson, S.I. Rosenberg, Silverstein MicroWick for treatment ofinner ear disease, Oper. Tech. Otolaryngol. 12 (2001) 144–147.
Please cite this article as: E.E.L. Pararas, et al., Microsystems technologidoi:10.1016/j.addr.2012.02.004
ED P
RO
OF
[39] F.v. Wijck, H. Staecker, P.P. Lefebvre, et al., Topical steriod therapy using the SilversteinMicroWick in sudden sensorineural hearing loss after failure of conventional treatment,Acta Otolaryngol. 127 (2007) 1012–1017.
[40] F.v.Wijk, H. Staecker, E. Keithley, P.P. Lefebvre, Local perfusion of the tumor necrosisfactor alpha blocker infliximad to the inner ear improves autoimmune neurosensoryhearing loss, Audiol. Neurootol. 11 (2006) 357–365.
[41] M.J. DeCicco, M.E. Hoffer, R.D. Kopke, D. Wester, K.A. Allen, K. Gottshall, M.J.O'Leary, Roundwindowmicrocatheter-administeredmicrodose gentamicin: resultsfrom treatment of tinnitus associatedwithMeniere's disease, Int. Tinnitus J. 4 (1998)141–143.
[42] R. Suryanarayanan, Long-term results of gentamicin inner ear perfusion inMeniere's disease, J. Laryngol. Otol. 118 (2004) 489–495.
[43] J. Thomsen, S. Charabi, M. Tos, Preliminary results of the new delivery system for gen-tamicin to the inner ear in patientswithMeniere's disease, Eur. Arch. Otorhinolaryngol.257 (2000) 362–365.
[44] P. Weisskopf, M.E. Hoffer, R.D. Kopke, K. Gottshall, K. Allen, D. Wester, Microdosegentamicin delivered via the round window microcatheter: a therapeutic optionin Meniere's disease, Oper. Tech. Otolaryngol. 12 (2001) 154–156.
[45] S.K. Plontke, H. Lowenheim, S. Preyer, P. Leins, K. Dietz, A. Koitschev, R.Zimmermann, H.-P. Zenner, Outcomes research analysis of continuous intratympanicglucocorticoid delivery in patients with acute severe to profound hearing loss: basisfor planning randomized controlled trials, Acta Otolaryngol. 125 (2005) 830–839.
[46] S.K. Plontke, H. Lowenheim, J. Mertens, C. Engel, C. Meisner, A. Weidner, R.Zimmermann, S. Preyer, A. Koitschev, H.-P. Zenner, Randomized, double blind,placebo controlled trial on the safety and efficacy of continuous intratympanicdexamethasonedelivered via a roundwindowcatheter for severe to profound suddenidiopathic sensorineural hearing loss after failure of systemic therapy, Laryngoscope119 (2009) 359–369.
[47] E.E.L. Swan,M.J. Mescher, W.F. Sewell, S.L. Tao, J.T. Borenstein, Inner ear drug deliveryfor auditory applications, Adv. Drug Deliv. Rev. 60 (2008) 1583–1599.
[48] H. Shimogori, H. Yamashita, Efficacy of intracochlear administration of betamethasoneon peripheral vestibular disorder in the guinea pig, Neurosci. Lett. 294 (2000) 21–24.
[49] H. Orita, H. Shimogori, H. Yamashita, Unilateral intra-perilymphatic infusion ofsubstance P enhances ipsilateral vestibulo-ocular reflex gains in the sinusoidal rotationtest, Neurosci. Lett. 449 (2009) 207–210.
[50] B.T.G. Tam, K.H. Foong, M.M.G. Lee, R. Ruan, Polyethylenimine-mediated cochleargene transfer in guinea pigs, Arch. Otolaryngol. 134 (2008) 884–891.
[51] L. Abaamrane, F. Raffin, S. Schmerber, I. Sendowski, Intracochlear perfusion of leupeptinand z-VAD-FMK: influence of antapoptotic agents on gunshot-induced hearing loss,Eur. Arch. Otorhinolaryngol. 268 (2011) 987–993.
[52] W.F. Sewell, J.T. Borenstein, Z. Chen, J. Fiering, O. Handzel, M. Holmboe, E.S. Kim,S.G. Kujawa, M.J. McKenna, M.M. Mescher, B. Murphy, E.E. Swan, M. Peppi, S. Tao,Development of a microfluidics-based intracochlear drug delivery device, Audiol.Neurootol. 14 (2009) 411–422.
[53] Z. Chen, S.G. Kujawa, M.J. McKenna, J.O. Fiering, M.J. Mescher, J.T. Borenstein, E.E.L.Swan, W.F. Sewell, Inner ear drug delivery via a reciprocating perfusion system inthe guinea pig, J. Control. Release 110 (2005) 1–19.
[54] O. Handzel, H. Wang, J. Fiering, J.T. Borenstein, M.J. Mescher, E.E.L. Swan, B.A.Murphy, Z. Chen, M. Peppi, W.F. Sewell, S.G. Kujawa, M.J. McKenna, Mastoid cavitydimensions and shape: method of measurement and virtual fitting of implantabledevices, Audiol. Neurootol. 14 (2009) 308–314.
[55] W.F. Sewell, J.T. Borenstein, Z. Chen, J. Fiering, O. Handzel, M. Holmboe, E. Kim,S.G. Kujawa, M.J. McKenna, M.J. Mescher, B.A. Murphy, E.E.L. Swan, M. Peppi,S.L. Tao, Development of a microfluidics-based intracochlear drug delivery device,Audiol. Neurootol. 14 (2009) 411–422.
[56] E.E.L. Pararas, Z. Chen, J. Fiering, M.J. Mescher, E.S. Kim, M.J. McKenna, S.G.Kujawa, J.T. Borenstein, W.F. Sewell, Kinetics of reciprocating drug delivery tothe inner ear, J. Control. Release 152 (2011) 270–277.
[57] J. Fiering, M.J. Mescher, E.E.L. Swan, M.E. Holmboe, B.A. Murphy, Z. Chen, M. Peppi,W.F. Sewell, M.J. McKenna, S.G. Kujawa, J.T. Borenstein, Local drug delivery with aself-contained, programmable, microfluidic system, Biomed. Microdevices 11(2009) 571–578.
[58] M.J. Mescher, E.E.L. Swan, J. Fiering, M. Holmboe, W.F. Sewell, S.G. Kujawa, M.J.McKenna, J.T. Borenstein, Fabrication methods and performance of low-permeability microfluidic components for a miniaturized wearable drug deliverysystem, IEEE J. MEMS 18 (2009) 501–510.
[59] S.K. Plontke, T. Biegner, B. Kammerer, U. Delabar, A.N. Salt, Dexamethasone concentra-tion gradients along scala tympani after application to the roundwindowmembrane,Otol. Neurotol. 29 (2008) 401–406.
[60] Z. Chen, A.A. Mikulec, M.J. McKenna, W.F. Sewell, S.G. Kujawa, A method forintracochlear drug delivery in the mouse, J. Neurosci. Methods 150 (2006) 67–73.
[61] D. Oliver, D. He, N. Klocker, J. Ludwig, U. Schulte, S. Waldegger, J. Ruppersberg, P.Dallos, B. Fakler, Intracellular anions as the voltage sensor of prestin, the outerhair cell motor protein, Science 292 (2001) 2340–2343.
[62] A.N. Salt, K. Ohyama, R. Thalmann, Radial communication between the perilymphaticscalae of the cochlea. II Estimation by bolus injection of tracer into the sealed cochlea,Hear. Res. 56 (1991) 37–43.
[63] M. Gladstone, X. Zhu, A. Luebke, R. Frisina, D.A. Borkholder, Using micro-computedtomography to asses transport parameters through fluid spaces of the cochlea, Bio-medical Engineering Society National Conference, University of Texas at Austin,2010.
[64] R. Shepherd, J. Xu, A multichannel scala tympani electrode array incorporating adrug delivery system for chronic intracochlear infusion, Hear. Res. 172 (2002)92–98.
[65] H. Staecker, C. Jolly, C. Garnham, Cochlear implantation: an opportunity for drugdevelopment, Drug Discov. Today 15 (2010) 314–321.
es for drug delivery to the inner ear, Adv. Drug Deliv. Rev. (2012),

972973974975976977
978979980981982983
985
11E.E.L. Pararas et al. / Advanced Drug Delivery Reviews xxx (2012) xxx–xxx
[66] D.G. Johnson, X.X. Zhu, R.D. Frisina, D.A. Borkholder, Micro-molded cannulae forintracochlear infusions in small rodents, Conf. Proc. IEEE Eng. Med. Biol. Soc.2007 (2007) 6617–6620.
[67] D.G. Johnson, M.J. Waldron, R.D. Frisina, D.A. Borkholder, Implantable micropumptechnologies for murine intracochlear infusions, Conf. Proc. IEEE Eng. Med. Biol.Soc. 1 (2010) 6441–6444.
UNCO
RRECT
984
Please cite this article as: E.E.L. Pararas, et al., Microsystems technologidoi:10.1016/j.addr.2012.02.004
[68] D. Johnson, R. Frisina, D. Borkholder, In-plane biocompatiblemicrofluidic interconnectsfor implantable microsystems, IEEE Trans. Biomed. Eng. 58 (2011) 943–948.
[69] D. Johnson, J. Getpreecharsawas, S. Balasubramanian, A. Datar, D. Cormier, D.A.Borkholder, Hybrid MEMS: extending micro manufacturing with direct write pro-cesses, Technical Digest of Transducers Research Foundation Technologies for FutureMicro-nano Manufacturing Workshop, 2011.
ED P
RO
OF
es for drug delivery to the inner ear, Adv. Drug Deliv. Rev. (2012),
Related Documents











