School COVID-19 Toolkit For Health Offices Version 2 Revised April 13,2021

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
School COVID-19 Toolkit
For Health Offices
Version 2 Revised April 13,2021
Table of Contents
https://www.mchenrycountyil.gov/Home/ShowDocument?id=100104
Introduction 1
Definitions of Commonly Used COVID-19 Terms 3
Narrative Flowchart suspected COVID-19 Student 4
Narrative Flowchart suspected COVID-19 Staff 5
School Nurse Flowsheet for Suspicious, Possible, and/or Positive Student/Staff 6
Worksheet A-COVID-19 Assessment- Student (revised) 7
Worksheet A-COVID-19 Assessment- Staff (revised) 9
Isolation and Quarantine Graphic (Definition and Release) Updated 10.23.20 11
Isolation and Quarantine Calendar Tool 12
Worksheet B -School Investigation Report (revised) 13
Worksheet C- Student Contact Form for Positive COVID-19 (revised) 15
Worksheet C - Staff Contact Form for Positive COVID-19 (revised) 16
COVID Investigation/Communication Notes 17
Symptom Comparison – School Health Nurse 18
FAQ from the School Nurse. 19
Isolation Room Guidelines (9/21/20) 21
Mask Exemption Request Form (9/23/20) 22
Staff PPE Guidelines (9/23/20) 23
Sample LDH Isolation/Quarantine Letter (10/28/20) 24
Sample Return Authorization Letter (3/2021) 25
Sample Vaccine Clinic Information (2/2021) 26
Sample Vaccine Schedule (2/2021) 29
Post Vaccine Management (2/2021) 30
Figure 2

Introduction:
The McHenry County Department of Health (MCDH) recognizes the challenges facing schools throughout McHenry County with the COVID-19 pandemic. MCDH shares in the goal of each McHenry County school to provide a safe environment for staff and students. MCDH from the start of the pandemic has been hosting weekly school calls to provide updates and answer questions. With the June 23, 2020 release of “Starting the 2020-21 School Year” from the Illinois State Board of Education a School Task Force was created. This task force is made up of McHenry County school health officials and public health officials to address health protocols for schools.
With the COVID-19 response in our community being very fluid, this toolkit will have ongoing updates as new recommendations and tools are developed. Recommendations and tools are all subject to change as new guidance is received from the Centers of Disease Control and Prevention (CDC), Illinois Department of Public Health (IDPH), Illinois State Board of Education (ISBE), and the McHenry County Department of Health (MCDH).
1
COVID-19 School Health Task Force The McHenry County Department of Health would like to extend our gratitude to the following
members of the School Task Force Team for volunteering their time and talents to help keep McHenry County Schools safe during this critical time.
School District Representatives Amy Belrichard, MSN, RN, PEL-NCSN Crystal Lake, District 47 Suzanne Blohm, MS, RN, PEL-CSN Cary, District 26 Connie Happ MSN, MAT, SN-PEL Woodstock High School, District 200 Amanda Keegan, RN West Elementary, District 47 Donna J. Kunz, MSN, RN, PEL-NCSN Huntley High School, District 158 Martha Manno MSN, RN, PEL-CSN Cary Grove High School District 155 Katie Palek, MSN, RN, PEL-CSN Marengo Community High School District 154 Dawn Ruffatti, RN, PEL-NCSN Conley Elementary School, District 158 Bria Spiniolas, BSN, RN, PEL-CSN Alden-Hebron School, District 19 Susan Sweinberg, RN Deer Path School, District 26 Lisa Tate, MAEL, BSN, RN, PEL-CSN Director of Nursing and Health Services Woodstock CUSD #200 Tara Weidner, BSN RN PEL-CSN Marengo Union Consolidated School District #165 District Nurse
Amy Wuerger, RN, MAEL, PEL-CSN, NCSN McHenry School District 15 Health Department Representatives Danielle Burck, BSN, RN Communicable Disease Coordinator McHenry County Department of Health Susan Karras, MBA, BSN, RN Director, Public Health Nursing McHenry County Department of Health Amanda Kurka, BSN, RN Communicable Disease Investigator McHenry County Department of Health Faith Schoen, BSN, RN Communicable Disease Investigator McHenry County Department of Health

Definitions of Commonly Used COVID-19 Terms
Antibody test -blood test that identifies antibodies to the virus. Some antibodies (IgG) begin to develop when you are sick and can be identified after you recover. Not recognized as valid at this time.
Case -someone who has COVID-19. Could infect others. Positive PCR.
Suspect Case -someone exposed to a case who develops symptoms, even if they have not been tested yet.
Confirmed/Positive Case -Must be isolated for a minimum of 10 days after symptom onset date (or specimen collection date if onset unclear or if asymptomatic) and can be released after afebrile and feeling well without fever reducing medical for at least 24 hours.
Contact -defined as being within 6 feet of an infected person for at least 15 minutes starting from 2 days before the onset of illness
Close Contact -an individual who was in contact (see above). Must be quarantined for 14 days after the last/most recent contact with the case when the case was infectious. If a close contact develops symptoms, they will follow isolation rules.
Household Contacts with separate living quarters between case and contacts -Quarantine for 14 days after the last exposure to case.
Household Contacts that share a room/living quarters (ongoing contact) -Quarantine during contact and for 14 days after the case is released from isolation.
Incubation Period - time from when someone is infected until symptoms develop. Ranges from 2-14 days. 50% of people will become ill by 5 days after being infected. 5% by 2 days. 95% by14 days.
Isolation -Separates sick people with a contagious disease from people who are not sick.
Polymerase Chain Reactions (PCR) -detects RNA in virus. Also called molecular test.
Quarantine -Separates and restricts the movement of people who were exposed to a contagious disease to see if they become sick.
Contact Tracing -common public health tool used to limit contact between infectious people and others, limiting the transmission of the disease.
3
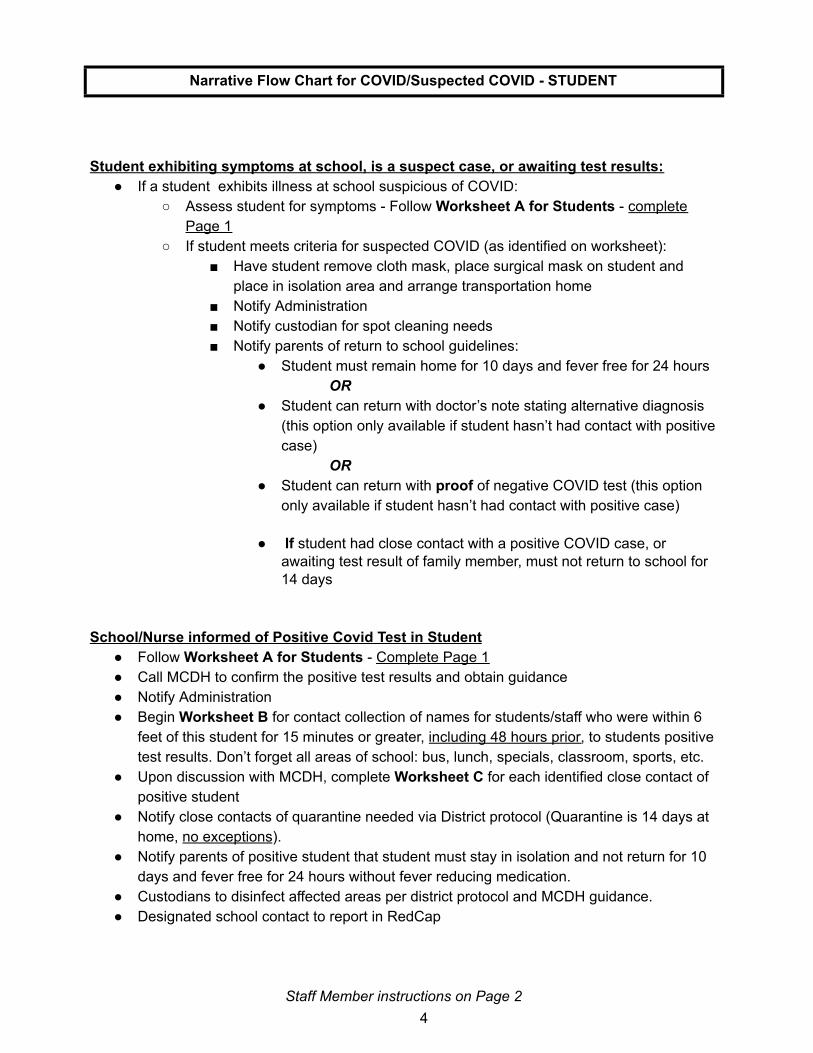
Narrative Flow Chart for COVID/Suspected COVID - STUDENT
Student exhibiting symptoms at school, is a suspect case, or awaiting test results: ● If a student exhibits illness at school suspicious of COVID:
○ Assess student for symptoms - Follow Worksheet A for Students - completePage 1
○ If student meets criteria for suspected COVID (as identified on worksheet):■ Have student remove cloth mask, place surgical mask on student and
place in isolation area and arrange transportation home■ Notify Administration■ Notify custodian for spot cleaning needs■ Notify parents of return to school guidelines:
● Student must remain home for 10 days and fever free for 24 hoursOR
● Student can return with doctor’s note stating alternative diagnosis(this option only available if student hasn’t had contact with positivecase)
OR ● Student can return with proof of negative COVID test (this option
only available if student hasn’t had contact with positive case)
● If student had close contact with a positive COVID case, orawaiting test result of family member, must not return to school for14 days
School/Nurse informed of Positive Covid Test in Student ● Follow Worksheet A for Students - Complete Page 1● Call MCDH to confirm the positive test results and obtain guidance● Notify Administration● Begin Worksheet B for contact collection of names for students/staff who were within 6
feet of this student for 15 minutes or greater, including 48 hours prior , to students positivetest results. Don’t forget all areas of school: bus, lunch, specials, classroom, sports, etc.
● Upon discussion with MCDH, complete Worksheet C for each identified close contact ofpositive student
● Notify close contacts of quarantine needed via District protocol (Quarantine is 14 days athome, no exceptions ).
● Notify parents of positive student that student must stay in isolation and not return for 10days and fever free for 24 hours without fever reducing medication.
● Custodians to disinfect affected areas per district protocol and MCDH guidance.● Designated school contact to report in RedCap
Staff Member instructions on Page 2 4

Narrative Flow Chart for COVID/Suspected COVID - STAFF MEMBER
Staff member exhibiting symptoms at school, is a suspect case, or awaiting test results: ● If a staff member should exhibit illness at school suspicious of COVID:
○ Assess staff for symptoms -Follow Worksheet A for Staff○ If staff meets criteria for suspected COVID (as identified on worksheet):
■ Notify Administration■ Have staff remove cloth mask and place surgical mask on staff and place
is isolation area awaiting personal belongings to be brought to him/her inorder to go home
■ Notify custodian for spot cleaning needs■ Notify staff member of return to school guidelines:
● Staff must remain home for 10 days and fever free for 24 hoursOR
● Staff can return with doctor’s note stating alternative diagnosisOR
● Staff can return with proof of negative COVID test
● If staff member had close contact with a positive COVID case, orawaiting test result of family member, must not return to school for14 days
School/Nurse informed of Positive Covid Test in Staff Member ● Follow Worksheet A for Staff- Complete Page 1● Call MCDH to confirm the positive test results and ask for guidance● Notify Administration● Begin Worksheet B for contact collection of names for students/staff who were within 6
feet of this student for 15 minutes or greater, including 48 hours prior , to the staffmember’s positive test results. Don’t forget all areas of school: Classroom, lunchroom,coaching, IEP meetings, staff meetings, collaboration meetings, supervision, etc.
● Upon discussion with MCDH, complete Worksheet C for each identified close contact ofpositive student
● Notify close contacts of quarantine needed via District protocol (Quarantine is 14 days athome, no exceptions ).
● Custodians to disinfect affected areas per district protocol and MCDH guidance.● Designated school contact to report in RedCap
5
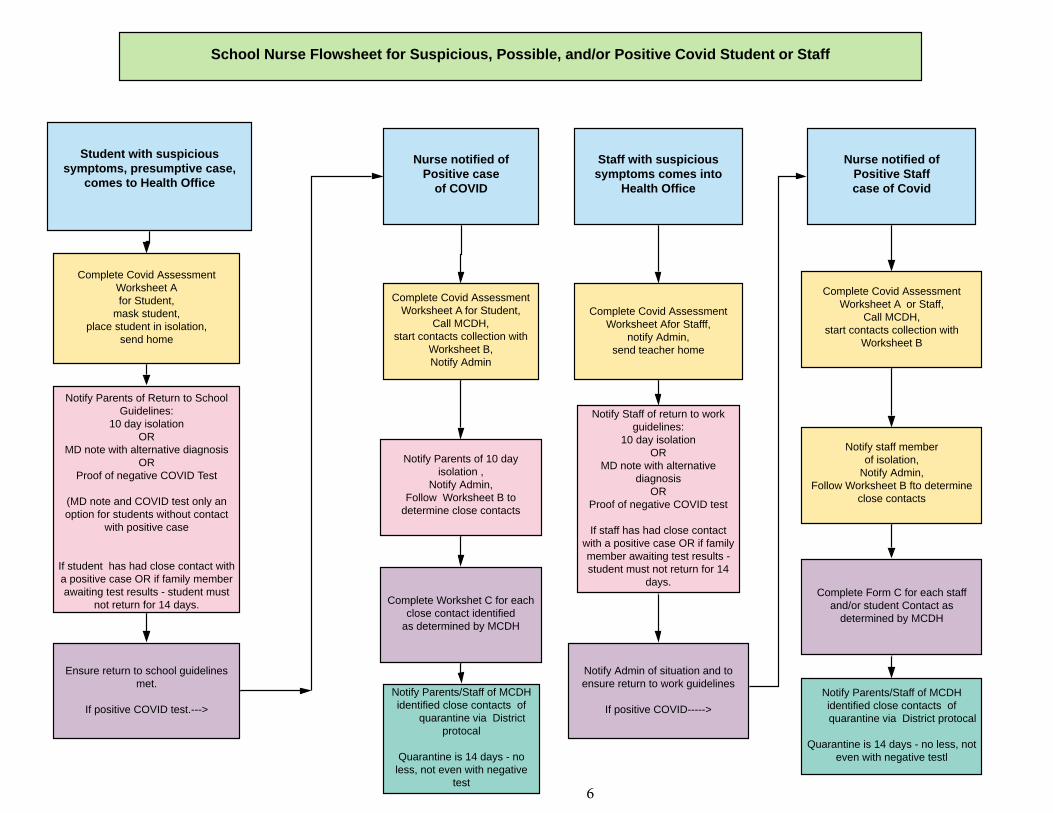
Student with suspicious symptoms, presumptive case,
comes to Health Office
Nurse notified of Positive case
of COVID
Complete Covid Assessment Worksheet Afor Student,
mask student,place student in isolation,
send home
Complete Covid AssessmentWorksheet A for Student,
Call MCDH, start contacts collection with
Worksheet B,Notify Admin
Staff with suspicious symptoms comes into
Health Office
Complete Covid AssessmentWorksheet Afor Stafff,
notify Admin, send teacher home
Nurse notified of Positive Staff case of Covid
Complete Covid Assessment Worksheet A or Staff,
Call MCDH, start contacts collection with
Worksheet B
Notify Parents of Return to School Guidelines:
10 day isolationOR
MD note with alternative diagnosisOR
Proof of negative COVID Test
(MD note and COVID test only an option for students without contact
with positive case
If student has had close contact with a positive case OR if family member awaiting test results - student must
not return for 14 days.
Notify Parents of 10 day isolation ,
Notify Admin,Follow Worksheet B to
determine close contacts
Notify Staff of return to work guidelines:
10 day isolationOR
MD note with alternative diagnosis
ORProof of negative COVID test
If staff has had close contact with a positive case OR if family member awaiting test results - student must not return for 14
days.
School Nurse Flowsheet for Suspicious, Possible, and/or Positive Covid Student or Staff
Complete Workshet C for each close contact identified
as determined by MCDH
Notify Admin of situation and to ensure return to work guidelines
If positive COVID----->
Notify staff member of isolation,
Notify Admin,Follow Worksheet B fto determine
close contacts
Complete Form C for each staff and/or student Contact as
determined by MCDH
Notify Parents/Staff of MCDH identified close contacts of
quarantine via District protocal
Quarantine is 14 days - no less, not even with negative
test
Notify Parents/Staff of MCDH identified close contacts of quarantine via District protocal
Quarantine is 14 days - no less, not even with negative testl
Ensure return to school guidelines met.
If positive COVID test.--->
6
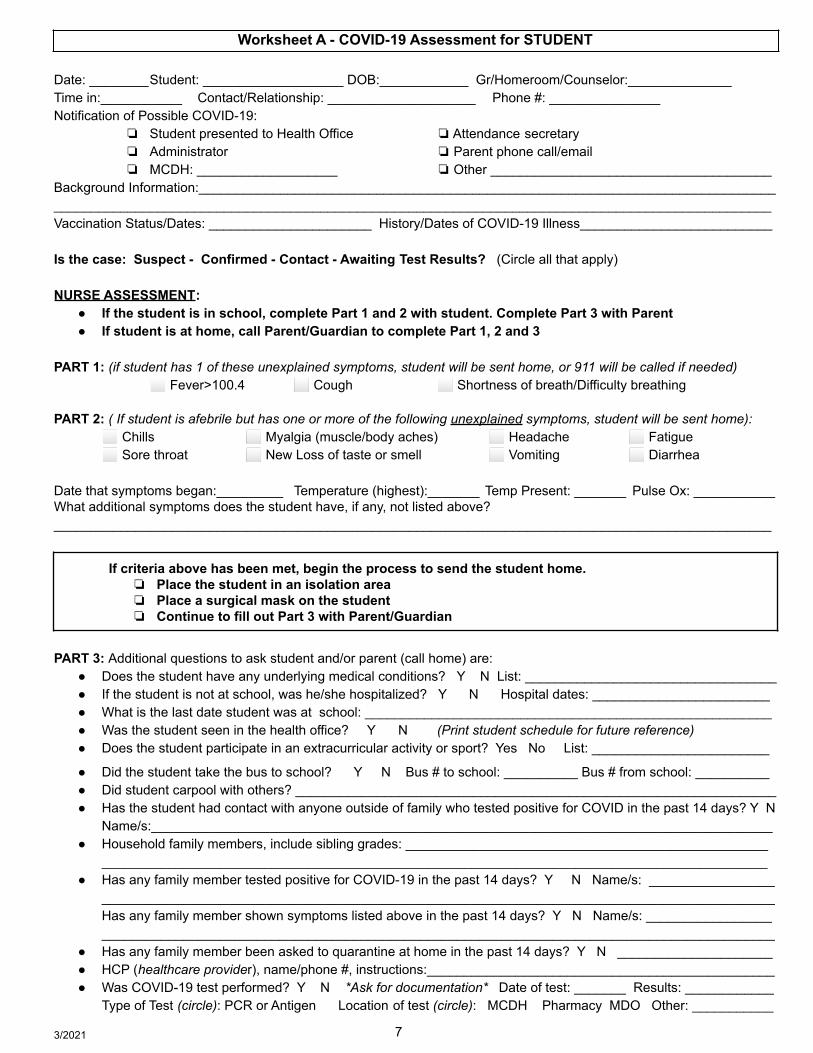
Worksheet A - COVID-19 Assessment for STUDENT
Date: ________Student: ___________________ DOB:____________ Gr/Homeroom/Counselor:______________Time in:___________ Contact/Relationship: ____________________ Phone #: _______________Notification of Possible COVID-19:
❏ Student presented to Health Office ❏Attendance secretary❏ Administrator ❏ Parent phone call/email❏ MCDH: ___________________ ❏ Other ______________________________________
Background Information:_______________________________________________________________________________________________________________________________________________________________________________Vaccination Status/Dates: ______________________ History/Dates of COVID-19 Illness__________________________
Is the case: Suspect - Confirmed - Contact - Awaiting Test Results? (Circle all that apply)
NURSE ASSESSMENT:● If the student is in school, complete Part 1 and 2 with student. Complete Part 3 with Parent● If student is at home, call Parent/Guardian to complete Part 1, 2 and 3
PART 1: (if student has 1 of these unexplained symptoms, student will be sent home, or 911 will be called if needed)⬜ Fever>100.4 ⬜ Cough ⬜ Shortness of breath/Difficulty breathing
PART 2: ( If student is afebrile but has one or more of the following unexplained symptoms, student will be sent home):⬜ Chills ⬜ Myalgia (muscle/body aches) ⬜ Headache ⬜ Fatigue⬜ Sore throat ⬜ New Loss of taste or smell ⬜ Vomiting ⬜ Diarrhea
Date that symptoms began:_________ Temperature (highest):_______ Temp Present: _______ Pulse Ox: ___________What additional symptoms does the student have, if any, not listed above?_________________________________________________________________________________________________
If criteria above has been met, begin the process to send the student home.❏ Place the student in an isolation area❏ Place a surgical mask on the student❏ Continue to fill out Part 3 with Parent/Guardian
PART 3: Additional questions to ask student and/or parent (call home) are:● Does the student have any underlying medical conditions? Y N List: __________________________________● If the student is not at school, was he/she hospitalized? Y N Hospital dates: ________________________● What is the last date student was at school: _______________________________________________________● Was the student seen in the health office? Y N (Print student schedule for future reference)● Does the student participate in an extracurricular activity or sport? Yes No List: ________________________
● Did the student take the bus to school? Y N Bus # to school: __________ Bus # from school: __________● Did student carpool with others? _________________________________________________________________● Has the student had contact with anyone outside of family who tested positive for COVID in the past 14 days? Y N
Name/s:____________________________________________________________________________________● Household family members, include sibling grades: _________________________________________________
__________________________________________________________________________________________● Has any family member tested positive for COVID-19 in the past 14 days? Y N Name/s: _________________
___________________________________________________________________________________________Has any family member shown symptoms listed above in the past 14 days? Y N Name/s: ____________________________________________________________________________________________________________
● Has any family member been asked to quarantine at home in the past 14 days? Y N _____________________● HCP (healthcare provider), name/phone #, instructions:_______________________________________________● Was COVID-19 test performed? Y N *Ask for documentation* Date of test: _______ Results: ____________
Type of Test (circle): PCR or Antigen Location of test (circle): MCDH Pharmacy MDO Other: ___________
3/2021 7
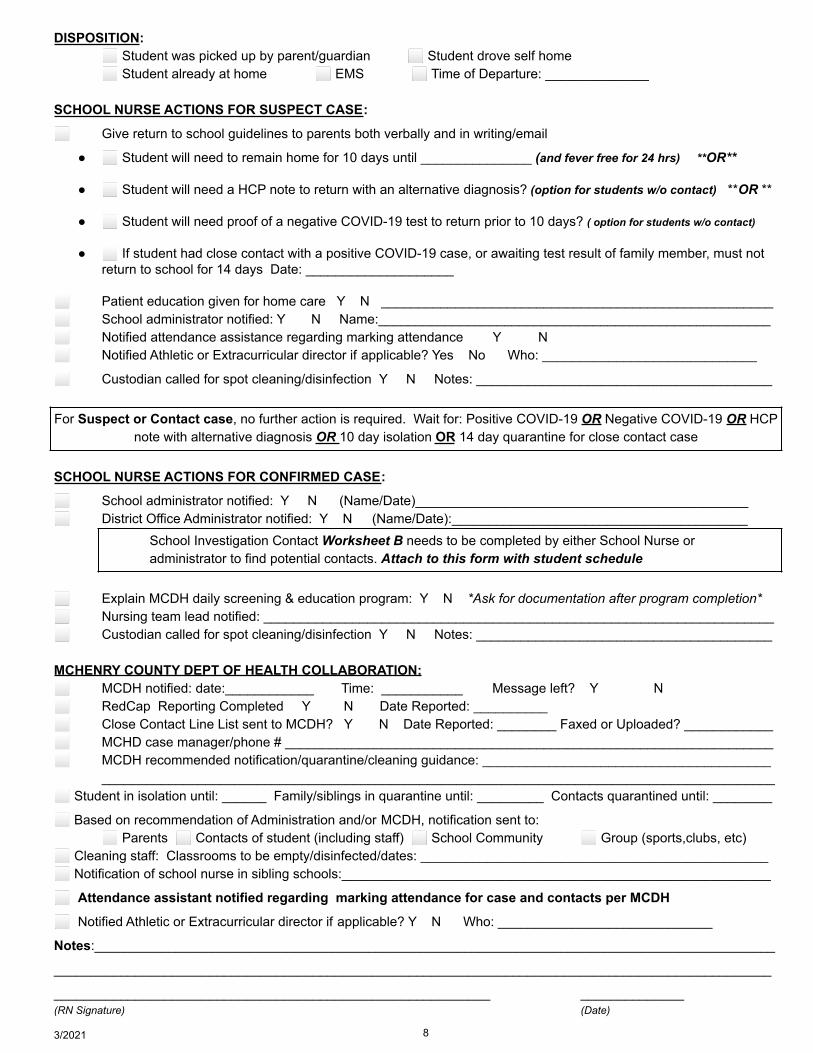
DISPOSITION:⬜ Student was picked up by parent/guardian ⬜ Student drove self home⬜ Student already at home ⬜ EMS ⬜ Time of Departure: ______________
SCHOOL NURSE ACTIONS FOR SUSPECT CASE:
⬜ Give return to school guidelines to parents both verbally and in writing/email
● ⬜ Student will need to remain home for 10 days until _______________ (and fever free for 24 hrs) **OR**
● ⬜ Student will need a HCP note to return with an alternative diagnosis? (option for students w/o contact) **OR **
● ⬜ Student will need proof of a negative COVID-19 test to return prior to 10 days? ( option for students w/o contact)
● ⬜ If student had close contact with a positive COVID-19 case, or awaiting test result of family member, must notreturn to school for 14 days Date: ____________________
⬜ Patient education given for home care Y N _____________________________________________________⬜ School administrator notified: Y N Name:_____________________________________________________⬜ Notified attendance assistance regarding marking attendance Y N⬜ Notified Athletic or Extracurricular director if applicable? Yes No Who: _____________________________
⬜ Custodian called for spot cleaning/disinfection Y N Notes: ________________________________________
For Suspect or Contact case, no further action is required. Wait for: Positive COVID-19 OR Negative COVID-19 OR HCPnote with alternative diagnosis OR 10 day isolation OR 14 day quarantine for close contact case
SCHOOL NURSE ACTIONS FOR CONFIRMED CASE:
⬜ School administrator notified: Y N (Name/Date)_____________________________________________⬜ District Office Administrator notified: Y N (Name/Date):________________________________________
School Investigation Contact Worksheet B needs to be completed by either School Nurse oradministrator to find potential contacts. Attach to this form with student schedule
⬜ Explain MCDH daily screening & education program: Y N *Ask for documentation after program completion*⬜ Nursing team lead notified: _____________________________________________________________________⬜ Custodian called for spot cleaning/disinfection Y N Notes: ________________________________________
MCHENRY COUNTY DEPT OF HEALTH COLLABORATION:⬜ MCDH notified: date:____________ Time: ___________ Message left? Y N⬜ RedCap Reporting Completed Y N Date Reported: __________⬜ Close Contact Line List sent to MCDH? Y N Date Reported: ________ Faxed or Uploaded? ____________⬜ MCHD case manager/phone # __________________________________________________________________⬜ MCDH recommended notification/quarantine/cleaning guidance: _______________________________________
___________________________________________________________________________________________⬜ Student in isolation until: ______ Family/siblings in quarantine until: _________ Contacts quarantined until: ________
⬜ Based on recommendation of Administration and/or MCDH, notification sent to:⬜ Parents ⬜ Contacts of student (including staff) ⬜ School Community ⬜ Group (sports,clubs, etc)
⬜ Cleaning staff: Classrooms to be empty/disinfected/dates: _______________________________________________⬜ Notification of school nurse in sibling schools:__________________________________________________________
⬜ Attendance assistant notified regarding marking attendance for case and contacts per MCDH
⬜ Notified Athletic or Extracurricular director if applicable? Y N Who: _____________________________
Notes:____________________________________________________________________________________________
_________________________________________________________________________________________________
___________________________________________________________ ______________(RN Signature) (Date)
3/2021 8
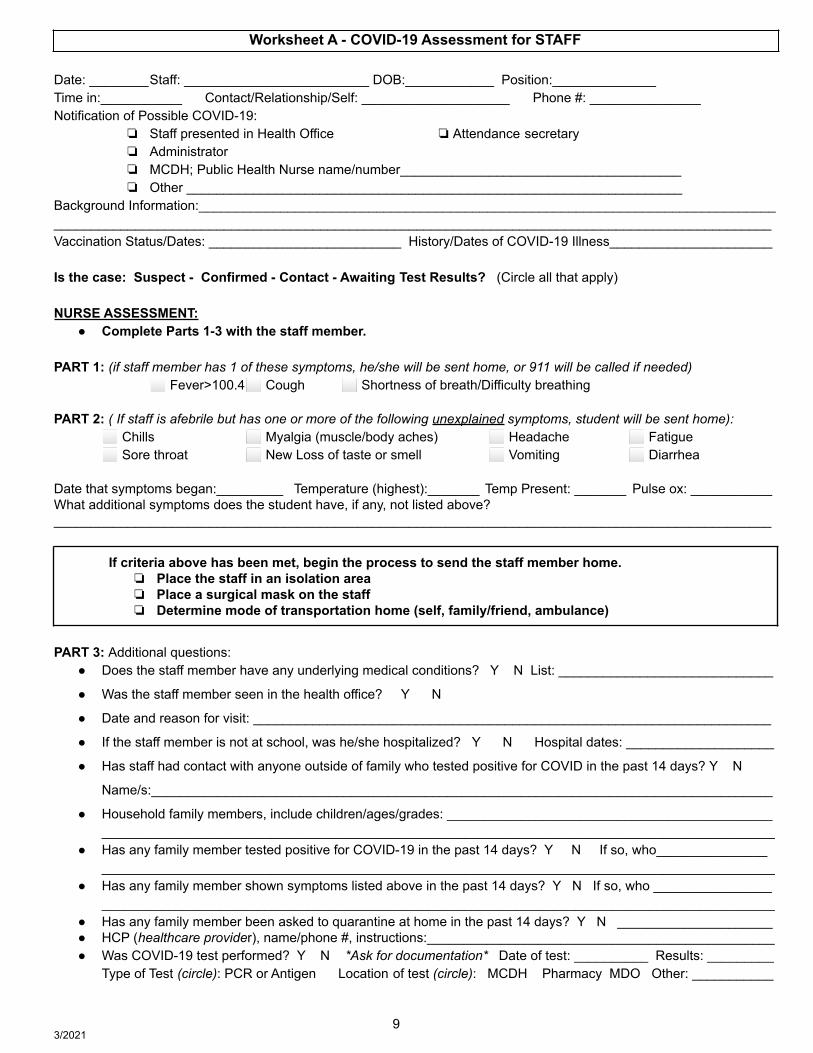
Worksheet A - COVID-19 Assessment for STAFF
Date: ________Staff: _________________________ DOB:____________ Position:______________Time in:___________ Contact/Relationship/Self: ____________________ Phone #: _______________Notification of Possible COVID-19:
❏ Staff presented in Health Office ❏Attendance secretary❏ Administrator❏ MCDH; Public Health Nurse name/number______________________________________❏ Other ___________________________________________________________________
Background Information:_______________________________________________________________________________________________________________________________________________________________________________Vaccination Status/Dates: __________________________ History/Dates of COVID-19 Illness______________________
Is the case: Suspect - Confirmed - Contact - Awaiting Test Results? (Circle all that apply)
NURSE ASSESSMENT:● Complete Parts 1-3 with the staff member.
PART 1: (if staff member has 1 of these symptoms, he/she will be sent home, or 911 will be called if needed)⬜ Fever>100.4⬜ Cough ⬜ Shortness of breath/Difficulty breathing
PART 2: ( If staff is afebrile but has one or more of the following unexplained symptoms, student will be sent home):⬜ Chills ⬜ Myalgia (muscle/body aches) ⬜ Headache ⬜ Fatigue⬜ Sore throat ⬜ New Loss of taste or smell ⬜ Vomiting ⬜ Diarrhea
Date that symptoms began:_________ Temperature (highest):_______ Temp Present: _______ Pulse ox: ___________What additional symptoms does the student have, if any, not listed above?_________________________________________________________________________________________________
If criteria above has been met, begin the process to send the staff member home.❏ Place the staff in an isolation area❏ Place a surgical mask on the staff❏ Determine mode of transportation home (self, family/friend, ambulance)
PART 3: Additional questions:● Does the staff member have any underlying medical conditions? Y N List: _____________________________
● Was the staff member seen in the health office? Y N
● Date and reason for visit: ______________________________________________________________________
● If the staff member is not at school, was he/she hospitalized? Y N Hospital dates: ____________________
● Has staff had contact with anyone outside of family who tested positive for COVID in the past 14 days? Y N
Name/s:____________________________________________________________________________________
● Household family members, include children/ages/grades: _______________________________________________________________________________________________________________________________________
● Has any family member tested positive for COVID-19 in the past 14 days? Y N If so, who__________________________________________________________________________________________________________
● Has any family member shown symptoms listed above in the past 14 days? Y N If so, who ___________________________________________________________________________________________________________
● Has any family member been asked to quarantine at home in the past 14 days? Y N _____________________● HCP (healthcare provider), name/phone #, instructions:_______________________________________________● Was COVID-19 test performed? Y N *Ask for documentation* Date of test: __________ Results: _________
Type of Test (circle): PCR or Antigen Location of test (circle): MCDH Pharmacy MDO Other: ___________
3/20219
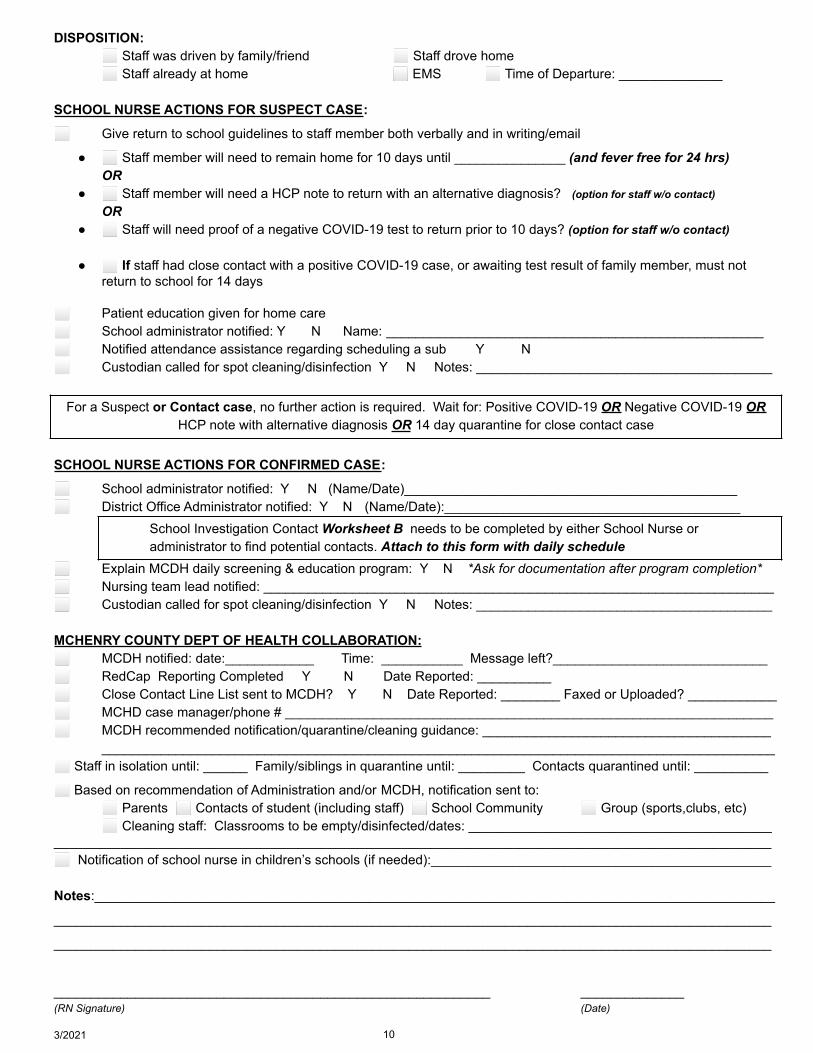
DISPOSITION:⬜ Staff was driven by family/friend ⬜ Staff drove home⬜ Staff already at home ⬜ EMS ⬜ Time of Departure: ______________
SCHOOL NURSE ACTIONS FOR SUSPECT CASE:
⬜ Give return to school guidelines to staff member both verbally and in writing/email
● ⬜ Staff member will need to remain home for 10 days until _______________ (and fever free for 24 hrs)OR
● ⬜ Staff member will need a HCP note to return with an alternative diagnosis? (option for staff w/o contact)OR
● ⬜ Staff will need proof of a negative COVID-19 test to return prior to 10 days? (option for staff w/o contact)
● ⬜ If staff had close contact with a positive COVID-19 case, or awaiting test result of family member, must notreturn to school for 14 days
⬜ Patient education given for home care⬜ School administrator notified: Y N Name: ___________________________________________________⬜ Notified attendance assistance regarding scheduling a sub Y N⬜ Custodian called for spot cleaning/disinfection Y N Notes: ________________________________________
For a Suspect or Contact case, no further action is required. Wait for: Positive COVID-19 OR Negative COVID-19 ORHCP note with alternative diagnosis OR 14 day quarantine for close contact case
SCHOOL NURSE ACTIONS FOR CONFIRMED CASE:
⬜ School administrator notified: Y N (Name/Date)_____________________________________________⬜ District Office Administrator notified: Y N (Name/Date):________________________________________
School Investigation Contact Worksheet B needs to be completed by either School Nurse oradministrator to find potential contacts. Attach to this form with daily schedule
⬜ Explain MCDH daily screening & education program: Y N *Ask for documentation after program completion*⬜ Nursing team lead notified: _____________________________________________________________________⬜ Custodian called for spot cleaning/disinfection Y N Notes: ________________________________________
MCHENRY COUNTY DEPT OF HEALTH COLLABORATION:⬜ MCDH notified: date:____________ Time: ___________ Message left?_____________________________⬜ RedCap Reporting Completed Y N Date Reported: __________⬜ Close Contact Line List sent to MCDH? Y N Date Reported: ________ Faxed or Uploaded? ____________⬜ MCHD case manager/phone # __________________________________________________________________⬜ MCDH recommended notification/quarantine/cleaning guidance: _______________________________________
___________________________________________________________________________________________⬜ Staff in isolation until: ______ Family/siblings in quarantine until: _________ Contacts quarantined until: __________
⬜ Based on recommendation of Administration and/or MCDH, notification sent to:⬜ Parents ⬜ Contacts of student (including staff) ⬜ School Community ⬜ Group (sports,clubs, etc)⬜ Cleaning staff: Classrooms to be empty/disinfected/dates: _________________________________________
_________________________________________________________________________________________________⬜ Notification of school nurse in children’s schools (if needed):______________________________________________
Notes:____________________________________________________________________________________________
_________________________________________________________________________________________________
_________________________________________________________________________________________________
___________________________________________________________ ______________(RN Signature) (Date)
3/2021 10
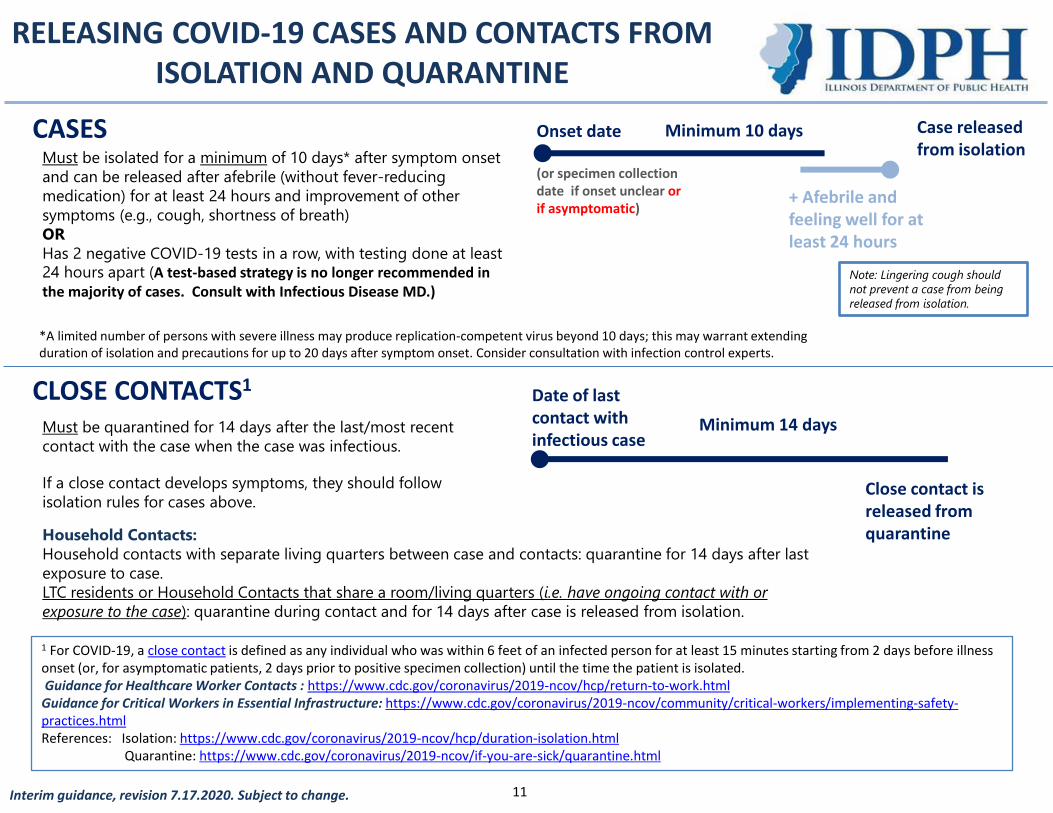
RELEASING COVID-19 CASES AND CONTACTS FROM ISOLATION AND QUARANTINE
CASES
CLOSE CONTACTS1
Must be isolated for a minimum of 10 days* after symptom onset
and can be released after afebrile (without fever-reducing
medication) for at least 24 hours and improvement of other
symptoms (e.g., cough, shortness of breath)
OR
Has 2 negative COVID-19 tests in a row, with testing done at least 24 hours apart (A test-based strategy is no longer recommended in the majority of cases. Consult with Infectious Disease MD.)
Must be quarantined for 14 days after the last/most recent
contact with the case when the case was infectious.
If a close contact develops symptoms, they should follow
isolation rules for cases above.
*A limited number of persons with severe illness may produce replication-competent virus beyond 10 days; this may warrant extendingduration of isolation and precautions for up to 20 days after symptom onset. Consider consultation with infection control experts.
Interim guidance, revision 7.17.2020. Subject to change.
Minimum 10 days
+ Afebrile andfeeling well for atleast 24 hours
Onset date
(or specimen collection date if onset unclear or if asymptomatic)
Case released from isolation
Close contact is released from quarantine
Date of last contact with infectious case
Minimum 14 days
1 For COVID-19, a close contact is defined as any individual who was within 6 feet of an infected person for at least 15 minutes starting from 2 days before illness onset (or, for asymptomatic patients, 2 days prior to positive specimen collection) until the time the patient is isolated.Guidance for Healthcare Worker Contacts : https://www.cdc.gov/coronavirus/2019-ncov/hcp/return-to-work.html
Guidance for Critical Workers in Essential Infrastructure: https://www.cdc.gov/coronavirus/2019-ncov/community/critical-workers/implementing-safety-practices.htmlReferences: Isolation: https://www.cdc.gov/coronavirus/2019-ncov/hcp/duration-isolation.html
Quarantine: https://www.cdc.gov/coronavirus/2019-ncov/if-you-are-sick/quarantine.html
Household Contacts:
Household contacts with separate living quarters between case and contacts: quarantine for 14 days after last
exposure to case.
LTC residents or Household Contacts that share a room/living quarters (i.e. have ongoing contact with or
exposure to the case): quarantine during contact and for 14 days after case is released from isolation.
Note: Lingering cough should
not prevent a case from being
released from isolation.
11
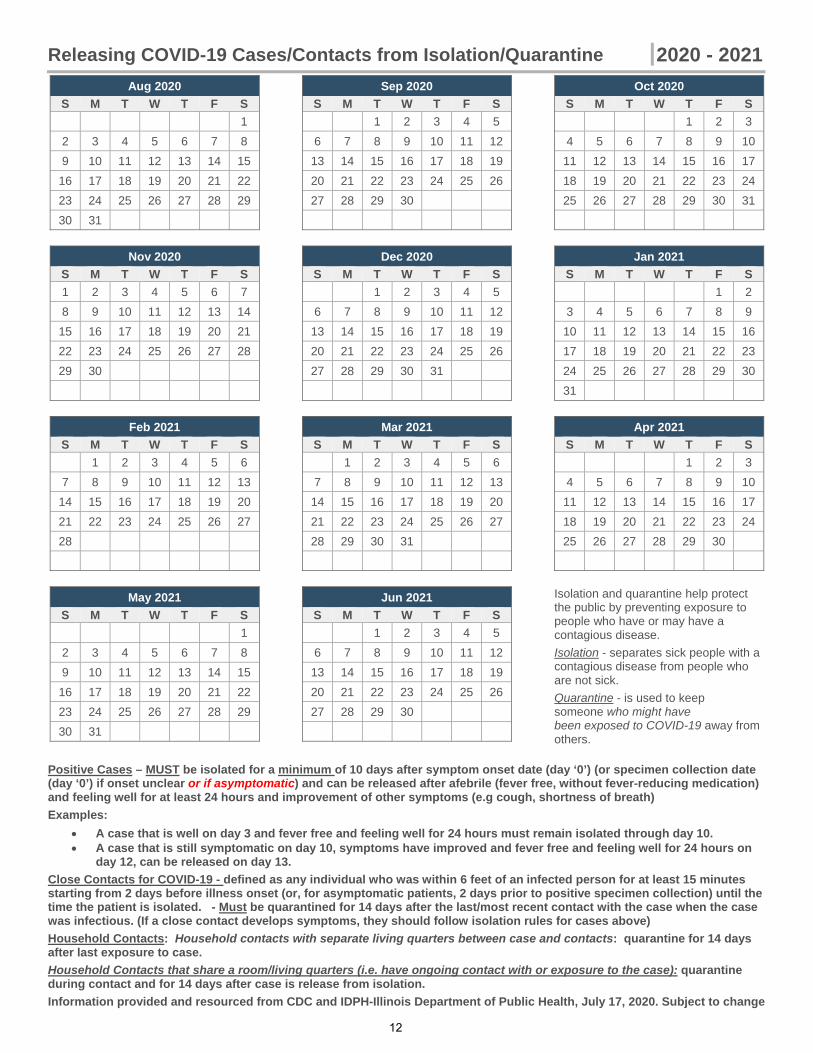
Releasing COVID-19 Cases/Contacts from Isolation/Quarantine 2020 - 2021
Aug 2020
S M T W T F S
1
2 3 4 5 6 7 8
9 10 11 12 13 14 15
16 17 18 19 20 21 22
23 24 25 26 27 28 29
30 31
Sep 2020
S M T W T F S
1 2 3 4 5
6 7 8 9 10 11 12
13 14 15 16 17 18 19
20 21 22 23 24 25 26
27 28 29 30
Oct 2020
S M T W T F S
1 2 3
4 5 6 7 8 9 10
11 12 13 14 15 16 17
18 19 20 21 22 23 24
25 26 27 28 29 30 31
Nov 2020
S M T W T F S
1 2 3 4 5 6 7
8 9 10 11 12 13 14
15 16 17 18 19 20 21
22 23 24 25 26 27 28
29 30
Dec 2020
S M T W T F S
1 2 3 4 5
6 7 8 9 10 11 12
13 14 15 16 17 18 19
20 21 22 23 24 25 26
27 28 29 30 31
Jan 2021
S M T W T F S
1 2
3 4 5 6 7 8 9
10 11 12 13 14 15 16
17 18 19 20 21 22 23
24 25 26 27 28 29 30
31
Feb 2021
S M T W T F S
1 2 3 4 5 6
7 8 9 10 11 12 13
14 15 16 17 18 19 20
21 22 23 24 25 26 27
28
Mar 2021
S M T W T F S
1 2 3 4 5 6
7 8 9 10 11 12 13
14 15 16 17 18 19 20
21 22 23 24 25 26 27
28 29 30 31
Apr 2021
S M T W T F S
1 2 3
4 5 6 7 8 9 10
11 12 13 14 15 16 17
18 19 20 21 22 23 24
25 26 27 28 29 30
May 2021
S M T W T F S
1
2 3 4 5 6 7 8
9 10 11 12 13 14 15
16 17 18 19 20 21 22
23 24 25 26 27 28 29
30 31
Jun 2021
S M T W T F S
1 2 3 4 5
6 7 8 9 10 11 12
13 14 15 16 17 18 19
20 21 22 23 24 25 26
27 28 29 30
Isolation and quarantine help protect the public by preventing exposure to people who have or may have a contagious disease.
Isolation - separates sick people with a contagious disease from people who are not sick.
Quarantine - is used to keep someone who might have been exposed to COVID-19 away from others.
Positive Cases – MUST be isolated for a minimum of 10 days after symptom onset date (day ‘0’) (or specimen collection date (day ‘0’) if onset unclear or if asymptomatic) and can be released after afebrile (fever free, without fever-reducing medication) and feeling well for at least 24 hours and improvement of other symptoms (e.g cough, shortness of breath)
Examples:
A case that is well on day 3 and fever free and feeling well for 24 hours must remain isolated through day 10. A case that is still symptomatic on day 10, symptoms have improved and fever free and feeling well for 24 hours on
day 12, can be released on day 13.
Close Contacts for COVID-19 - defined as any individual who was within 6 feet of an infected person for at least 15 minutes starting from 2 days before illness onset (or, for asymptomatic patients, 2 days prior to positive specimen collection) until the time the patient is isolated. - Must be quarantined for 14 days after the last/most recent contact with the case when the case was infectious. (If a close contact develops symptoms, they should follow isolation rules for cases above)
Household Contacts: Household contacts with separate living quarters between case and contacts: quarantine for 14 days after last exposure to case.
Household Contacts that share a room/living quarters (i.e. have ongoing contact with or exposure to the case): quarantine during contact and for 14 days after case is release from isolation.
Information provided and resourced from CDC and IDPH-Illinois Department of Public Health, July 17, 2020. Subject to change
12
Worksheet B - School Contact Investigation Report for SARS-CoV-19 (COVID-19)
***CONFIDENTIAL***** SHOULD BE COMPLETED BY SCHOOL NURSE OR ADMINISTRATOR****
Date: ________
Student or Staff w/ Positive Results: ____________________ Gr: ____ Homeroom/Counselor: ______________
Date of Start of Symptoms _______________ Date Last at School _____________________
Date of Positive Test: ___________________________
List of students or staff (close contacts) with possible exposure to positive student/staff during their infectiousperiod, meaning, within 6 feet of student, with or without masks, for at least 15 minutes (cumulative) during the 48hour timeframe prior to the start of symptoms (or date of positive test if asymptomatic). Print off student schedule toassist investigation.
The following areas/groups must be investigated to ensure all potential contacts were explored:
⬜ Classmates ⬜ Teachers ⬜ Aides ⬜ Specials ⬜ RTI/PBIS ⬜ Support Staff ⬜ Nurse⬜ Bus Driver ⬜ Coaches ⬜ Cafeteria ⬜ Admin ⬜ Volunteers ⬜ Sports ⬜ IEP Meetings⬜ Bus Peers ⬜ Substitutes ⬜ Clubs ⬜ Library ⬜ Custodian ⬜ Lunch Contacts ⬜ Class Group Work⬜ Transportation (car) Peers ⬜ Before/After school care ⬜ Secretarial Staff ⬜ Recess Contacts⬜ Counselor/SW/Psych ⬜ Siblings/Family Members ⬜ Therapists(SLP/PT/OT) ⬜ Extracurricular activity peers⬜ Peer Social Interactions ⬜ Traveling Teachers ⬜ IT Staff ⬜ Other ___________________
Name Gr/Position (if Staff) Describe Details of Contact (IncludeDates/Length of Contact)
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
3/2021 13
Worksheet B - School Contact Investigation Report for SARS-CoV-19 (COVID-19)Page 2
Name Gr/Position (if Staff) Describe Details of Contact (IncludeDates/Length of Contact)
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
___________________ ______________ _________________________________________________
Investigation Completed By: ____________________________________Date: _____________________
3/2021 14
Worksheet C STUDENT Contact Form for Positive COVID-19(this form to be attached to worksheet A)
Date: __________________
Student: _______________________ Gr: __________ Homeroom:________________
DOB: ___________________
Parent/Guardian Name: _________________________________________________________
Parent/Guardian Phone Number: ___________________________ ⬜ Cell ⬜ Home ⬜ Work
Home Address: _________________________________________________________________________
Per MCDH (or resident county) guidelines, was the student suggested to quarantine? Y N
Was Parent/Guardian notified of quarantine restrictions? Y N
Who notified the Parent/Guardian of restrictions? ______________________________________
Date quarantine started? ___________________________________________________________
Is the student ill with fever and/or respiratory illness? Y N
If so, what is the date of onset of symptoms? ____________________________________________Were any additional symptoms present? _______________________________________________
Referral to HCP? Y N
Date student can return to school ? (Must stay home 14 days after last date of last contact)_____________
Administration Actions:
⬜ Notify teacher about remote learning needs and length of remote instruction _________________⬜ Notify attendance assistant regarding marking attendance ________________________________
Notes:
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
3/2021 15
Worksheet C-STAFF Contact Form for Positive COVID-19(this form to be attached to worksheet A)
Date: __________________
Staff Member_______________________ School: ________________ Additional Schools? __________
DOB: ___________________
Position at School: _________________________________________________________
Home Address: _________________________________________________________________________
Phone Number: _________________________ ⬜ Cell ___________________ ⬜ Home
Per MCDH (or resident county) guidelines, was the staff member suggested to quarantine? Y N
Was Staff Member notified of quarantine restrictions? Y N
Who notified the staff member of restrictions? _________________________________
Date isolation started? __________________________________________________
Is the staff member ill with fever and/or respiratory illness? Y N
If so, what is the date of onset of symptoms? ____________________________________________Were any additional symptoms present? _______________________________________________
Referral to HCP? Y N
Date staff member can return to school: _____________________________________________________
Administration Actions:
⬜ Administrator to provide substitute for in school? _________________________________________⬜ Administrator to notify HR ___________________________________________________________
Notes: ________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
3/2021 16
COVID INVESTIGATION/COMMUNICATION NURSING NOTES
Student/Staff Name____________________ Grade/Position: ________________
Date Comments:
17
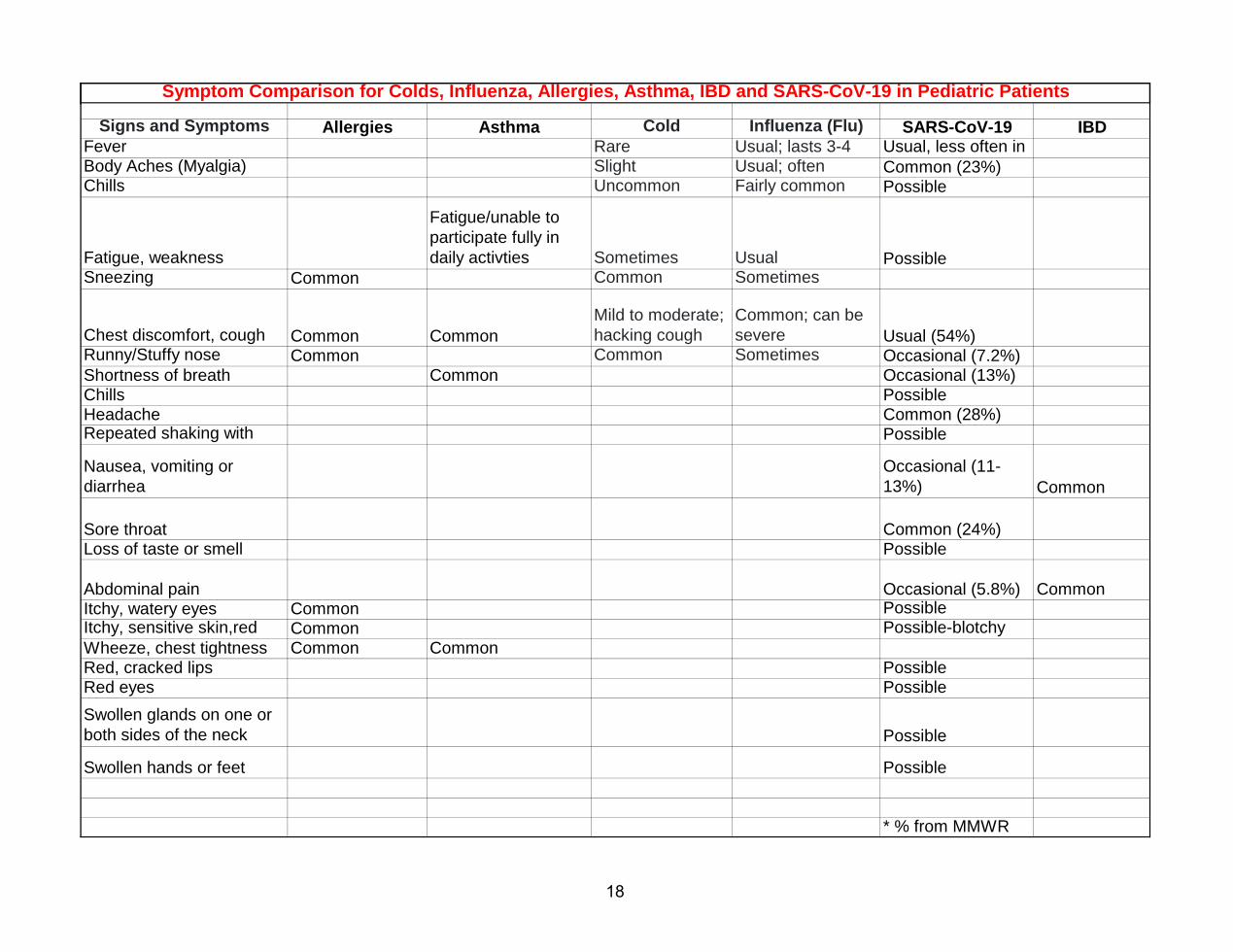
Signs and Symptoms Allergies Asthma Cold Influenza (Flu) SARS-CoV-19 IBDFever Rare Usual; lasts 3-4 Usual, less often in Body Aches (Myalgia) Slight Usual; often Common (23%)Chills Uncommon Fairly common Possible
Fatigue, weakness
Fatigue/unable to participate fully in daily activties Sometimes Usual Possible
Sneezing Common Common Sometimes
Chest discomfort, cough Common CommonMild to moderate; hacking cough
Common; can be severe Usual (54%)
Runny/Stuffy nose Common Common Sometimes Occasional (7.2%)Shortness of breath Common Occasional (13%)Chills PossibleHeadache Common (28%)Repeated shaking with Possible
Nausea, vomiting or diarrhea
Occasional (11-13%) Common
Sore throat Common (24%)Loss of taste or smell Possible
Abdominal pain Occasional (5.8%) CommonItchy, watery eyes Common Possible Itchy, sensitive skin,red Common Possible-blotchy Wheeze, chest tightness Common CommonRed, cracked lips PossibleRed eyes Possible
Swollen glands on one or both sides of the neck Possible
Swollen hands or feet Possible
* % from MMWR
Symptom Comparison for Colds, Influenza, Allergies, Asthma, IBD and SARS-CoV-19 in Pediatric Patients
18
COVID-19 FAQ’s From your School Nurse 2020/2021 As we all transition to what this upcoming school year will look like, here are some important FAQ’s that you may find helpful while in the building of your school. If you have further questions, please feel free to reach out to your school’s health office and/or administration. All the information below can be found on ISBE with further clarification if you have further questions.
FACE COVERINGS - Will my student (s) be required to wear a face covering? Yes. As required by IDPH, except while eating and during band, face coverings must be worn at all times in school buildings, even when social distance is maintained. All individuals in a school building must wear a face covering unless they have a medical contraindication, are under 2 years of age, have trouble breathing, or are unconscious, incapacitated, or unable to remove the face covering without assistance. Face coverings are not required outside if physical distance is maintained (if individuals remain 6 feet apart from each other). Face shields are not effective protection against coronavirus and should only be used in situations when other methods of protection are not available.
PHYSICAL DISTANCING - Are all individuals in a school building required to maintain physical distance (remain 6 feet apart) at all times? Physical distancing must be observed as much as possible. It is recommended that excess furniture be removed from classrooms to allow for as much space as possible in between desks.
How will the school handle students coming into the buildings, hallway passing and lockers? Based on individual school buildings, and to adhere to physical distancing requirements and IDPH limitations on gathering sizes, when possible the following are potential situations for your student(s):
● Limit the number of persons within hallways at any given time to the greatest extent possible● Limit required movement of students between classes.● Provide hallway supervision using hall and bathroom monitors to ensure a limited number of
persons enter bathrooms at one time.● Suspend the use of lockers, if possible. Sharing lockers should be prohibited. If lockers must be
used, consider staggering locker assignments and creating schedules to stagger locker access toallow for 6-foot distancing between students.
Is physical distance required to be maintained on school busses? No. No more than 50 individuals may be on a bus at one time. All individuals on a bus must wear a face covering. It is recommended that students from the same household sit together on a bus.
SYMPTOM SCREENINGS/TEMPERATURE CHECKS - How should symptom screenings be administered? Based on individual Districts, temperature and symptom screenings or self-certification and verification for all staff, students, and visitors entering school buildings will be required. Individuals who exhibit symptoms, should not come to school and should be referred to a medical provider for evaluation, treatment and be given information about when they can return to school. Refer to your individual district for more information.
20
Can students under the age of 18 self-certify? No. For students who are not legally emancipated, parents/guardians or the individual who enrolled the student will certify on behalf of the student.
CAPACITY LIMITS - What does ‘one space’ mean? Examples of one space may include one school bus, one classroom, or areas of a hallway. Capacity restrictions do not apply to an entire school building What does ‘one space’ mean when outside? Each group of 50 or fewer individuals must remain 30 feet apart. If individuals are 6 feet apart at all times, face coverings do not need to be worn.
POTENTIAL COVID-19 CASE IN MY STUDENT(S) CLASS - What to do if my student or another student is sent home with COVID-19 or COVID-19 like symptoms? Each school district will follow the below guidelines based from ISBE/IDPH along with the procedure developed for the individual health offices. Individuals who have tested positive for COVID-19 or who are suspected of having COVID-19 infection should seek medical attention, self-isolate. Individuals who have had close contact with an individual who has tested positive for COVID-19 or is suspected of having COVID-19 infection should be quarantined at home and monitored for symptoms for 14 days. Individuals who did not have close contact can return to school immediately after disinfection. *Close contact means the individual was within 6 feet of the individual who tested positive for COVID-19 or is suspected of having COVID-19 infection for more than 15 minutes. Schools should provide a supervised isolation space for students/staff who are experiencing COVID-19-like symptoms and may be awaiting evaluation and/or pickup. Judgment of nursing professionals or the administrator/designee (in the absence of a nurse) must determine who is placed in the isolation space and the level of supervision (e.g., supervised by nurse or unlicensed personnel) required for persons within the quarantine space.
*Close contact - is defined as any individual who was within 6 feet of an infected person for at least 15minutes, with or without masks, starting from 2 days before illness onset (or, for asymptomatic persons, 2days prior to positive specimen collection) until the time the person is isolated.
*Isolation - separates sick people with a contagious disease from people who are not sick.
*Quarantine - separates and restricts the movement of people who were exposed to a contagious diseaseto see if they become sick.
NOTE: Requirements are subject to change pursuant to updated public health guidance and changing public health conditions. Above information has been resourced from CDC and ISBE, last updated July 17, 2020
21
Isolation Room guidelines for school nursesIsolate student or staff if Part 1 or Part 2 symptoms are present:
PART 1: (if student has 1 of these unexplained symptoms, student will be sent home, or 911 will be called if needed)⬜ Fever>100.4⬜ Cough ⬜ Shortness of breath/Difficulty breathing
PART 2: ( If student is afebrile but has one or more of the following unexplained symptoms, student will be sent home):⬜ Congestion/runny nose ⬜ Fatigue ⬜ Myalgia (muscle/body aches)⬜ Headache ⬜ Sore throat ⬜ New Loss of taste or smell⬜ Nausea/Vomiting ⬜ Diarrhea ⬜ Abdominal Pain
Isolation room physical location will be decided for each building with Principal:1. If possible a door to separate completely for population and a phone.2. Hand sanitizer or sink required for hand hygiene.3. Cots or chairs should be 6 feet apart and separated by a floor to ceiling divider.4. Dividers should be cleanable - ideally plastic/vinyl.5. If available - open windows and use a fan to blow out of the window.6. Room used only for possible/suspected COVID cases and aerosol generating procedures.7. PPE includes - N95 mask for Nurse, face shield or goggles, gloves, and gown.8. Adult supervision required for the student in the isolation room.
Isolation Room Use:Use your nursing judgement and assessment skills to determine if a student is presenting withCOVID-19 like symptoms.
1. Teacher calls nurse for suspected illness2. Nurse gets coverage for the health office.3. Nurse will escort to the student to the isolation room.4. Student/staff enters the room and without touching anything and sits on a cot or chair.5. Staff should wash hands and don PPE, if not already performed.6. Change the mask from cloth to surgical. Place the cloth mask in a bag to be sent home for
cleaning.7. Assess student. Use worksheet A if suspected COVID.8. Call parent to pick up the child. Follow school procedure for other notifications and contact
tracing needs.9. After the student leaves the isolation room, notify the Principal, who will notify custodial staff.
a. Wait a minimum of 2 hours prior to cleaning, ideally wait 24 hours prior to cleaning.b. Post the time the area may be cleaned (2 hours post discharge).
10. Disposable items need to be discarded into a plastic trash bag in the room and tied/sealed.Custodial staff will remove the bagged items during cleaning.
9/21/2022
Mask/Face Shield Medical Exemption Form
Please complete all required fields below. Incomplete forms will not be accepted.
1.Parent/Guardian Section:
Student Information:Last Name: First Name: Middle Name (optional):Gender: □ Female □ Male Date of Birth:Address:City: State: Zip Code:Email Address: County:Phone Number: □ Home □ CellSchool Name: Grade:Does the Student Have an IEP or 504 plan? □ Y □N
Parent/Guardian Completing This Form:Last Name: First Name: Middle Name (optional):Relationship to student: □ Mother □ Father □ GuardianAddress:City: State: Zip Code:Email Address: County:Phone Number: □ Home □ Cell
2. Physician Section:Please list each pre-existingmedical condition that wouldpreclude the child from wearinga face mask while at school.
Please detail the medical contraindication(s) for eachmedical condition listed
For the physician/clinician. Please check all that apply and sign.___I certify that the physical condition of the above-named student is such that wearing a mask willendanger his/her life or health or is medically contraindicated due to other medical conditions.
___I certify that the physical condition of the above-named student is such that wearing a mask will NOTendanger his/her life or health or is NOT medically contraindicated due to other medical conditions.
___I certify that the physical condition of the above-named student is such that wearing a face shield willendanger his/her life or health or is medically contraindicated due to other medical conditions.
___I certify that the physical condition of the above -named student is such that wearing a face shield willNOT endanger his/her life or health or is NOT medically contraindicated due to other medical conditions.
Signature:__________________________________________________Office Phone:_________________Physician (MD, DO), Advanced Practice Nurse (APN), or delegated Physician Assistant (PA)
Updated 9/23/20
23
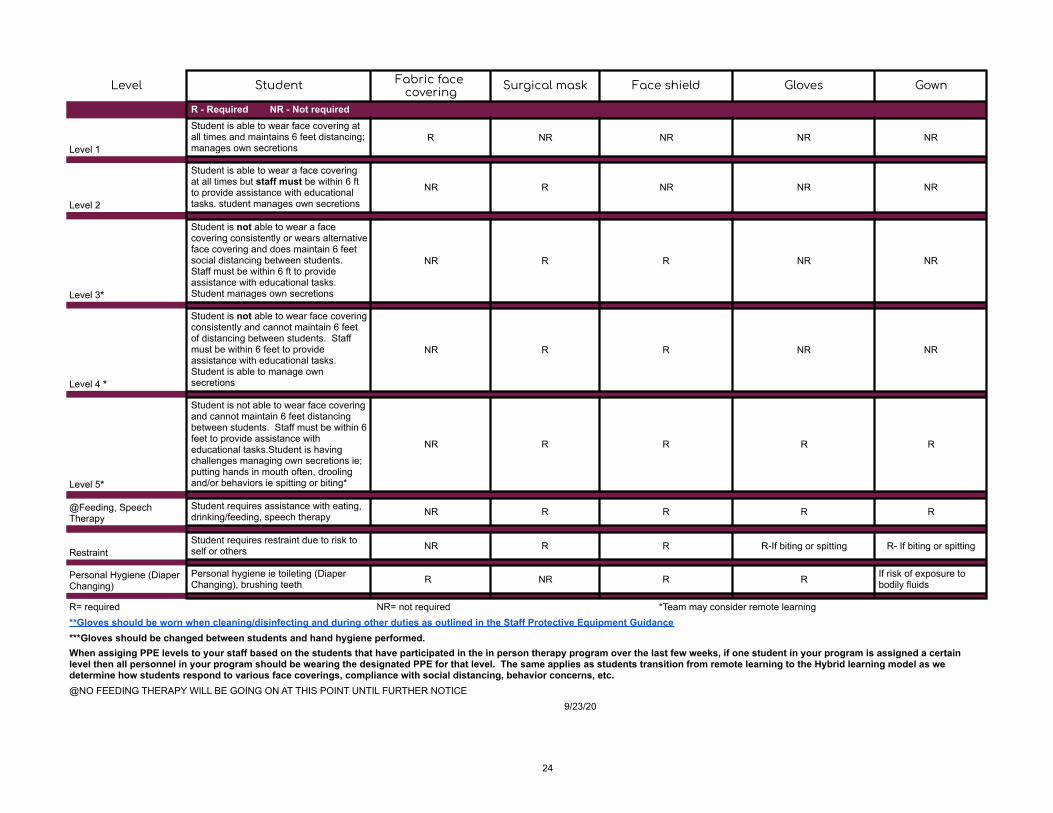
Level Student Fabric face covering Surgical mask Face shield Gloves Gown
R - Required NR - Not required
Level 1
Student is able to wear face covering at all times and maintains 6 feet distancing; manages own secretions
R NR NR NR NR
Level 2
Student is able to wear a face covering at all times but staff must be within 6 ft to provide assistance with educational tasks. student manages own secretions
NR R NR NR NR
Level 3*
Student is not able to wear a face covering consistently or wears alternative face covering and does maintain 6 feet social distancing between students. Staff must be within 6 ft to provide assistance with educational tasks. Student manages own secretions
NR R R NR NR
Level 4 *
Student is not able to wear face covering consistently and cannot maintain 6 feet of distancing between students. Staff must be within 6 feet to provide assistance with educational tasks. Student is able to manage own secretions
NR R R NR NR
Level 5*
Student is not able to wear face covering and cannot maintain 6 feet distancing between students. Staff must be within 6 feet to provide assistance with educational tasks.Student is having challenges managing own secretions ie; putting hands in mouth often, drooling and/or behaviors ie spitting or biting*
NR R R R R
@Feeding, Speech Therapy
Student requires assistance with eating, drinking/feeding, speech therapy NR R R R R
RestraintStudent requires restraint due to risk to self or others NR R R R-If biting or spitting R- If biting or spitting
Personal Hygiene (Diaper Changing)
Personal hygiene ie toileting (Diaper Changing), brushing teeth R NR R R If risk of exposure to
bodily fluids
R= required NR= not required *Team may consider remote learning**Gloves should be worn when cleaning/disinfecting and during other duties as outlined in the Staff Protective Equipment Guidance***Gloves should be changed between students and hand hygiene performed.When assiging PPE levels to your staff based on the students that have participated in the in person therapy program over the last few weeks, if one student in your program is assigned a certain level then all personnel in your program should be wearing the designated PPE for that level. The same applies as students transition from remote learning to the Hybrid learning model as we determine how students respond to various face coverings, compliance with social distancing, behavior concerns, etc.@NO FEEDING THERAPY WILL BE GOING ON AT THIS POINT UNTIL FURTHER NOTICE
9/23/20
24
Date_________________
Hello,
_____________________________________ is under (circle one: ISOLATION or QUARANTINE).
As per the guidance from the Illinois Department of Public Health (IDPH), the following guidance must be
followed to return to school if you are under isolation or quarantine:
Isolation: (separates people who test positive for COVID-19 and/or have COVID like
symptoms to limit contact with others)
● Stay at home for at least 10 days from the onset of symptoms AND
● Be fever free for 24 hours without the use of fever-reducing medication AND
● Improvement of symptoms
*If your symptoms worsen or do not improve, your isolation period may be extended, per
guidance from the McHenry County Department of Health*
Quarantine: (separates people who were a close contact to a positive COVID individual
to see if symptoms develop)
● Stay home for 14 days after the last exposure date to the COVID-19 case
● If COVID-19 illness develops, use the 10-day isolation period guidance for a COVID-19
case from the date of onset of symptoms. Testing is recommended.
You will receive a call from the McHenry County Department of Health (MCDH) regarding your status
soon. The number that will appear on your phone is 312-777-1999 and/or COVID Contact. Please take
their call and be ready to provide information regarding close contacts and locations visited. A close
contact is anyone who was within 6 feet of an infected individual for at least 15 minutes. It is imperative
that you share all close contacts with MCDH because any individual we are not made aware of will not
receive a release letter.
Health Assessments
Additionally, MCDH will enroll you/your student in a Health Assessment Program, which will require you
to submit your symptoms daily, for the duration of your isolation or quarantine period. You will have the
option to receive these Health Assessment surveys as an email or text, and they are sent out daily
around 7:00 AM.
At the end of the Health Assessment Program, IDPH and MCDH will generate a release from isolation or
quarantine letter, which will be required for you to return to school.
The release from isolation or quarantine letter will only be generated if you complete the satisfaction
survey after your last Health Assessment. This survey is sent out the day after your
isolation/quarantine period ends. If you do not complete the survey, or if you exit the browser, the
system will not email you the letter. Completion of the daily Health Assessment Surveys will ensure
you/your student is able to return to school as soon as possible.
If you have any questions, please contact (school nurse name, email, phone number)
10/28/2020
25

Return to School Certification
___________________________________may return to school on _____________________(date).
As per the guidance from the Illinois Department of Public Health (IDPH) and McHenry CountyDepartment of Health (MCDH), ______ District requires the following to return to school if you areunder isolation or quarantine:
The student/staff member has:
◻ Completed 10 day Isolation (requires Self-Certification or Health Department release*)
◻ Completed 14 day Quarantine (requires Self-Certification or Health Department release*)
◻ A negative COVID test (PCR or Rapid determined by RN) (requires results andSelf-Certification)
◻ An alternate diagnosis (requires physician documentation and Self-Certification)
The student/staff member is providing the following documentation with this form: (check all that apply)
◻ A release letter from the Health Department*
◻ A Self-Certification letter with Health Department release letter pending
◻ A Self-Certification letter with school nurse follow-up performed
◻ A copy of the negative COVID results (or verification of copy pending) and Self-Certification
◻ A note from the doctor (Must state an alternate diagnosis) and Self-Certification
Self-Certification
I certify that the Isolation or Quarantine period has been completed, I have a negative COVID test, or Ihave an alternate diagnosis and the information has been verified by the Health Department or the schoolnurse. I have not had a fever for 24 hours and I have not taken fever reducing medicine in the last 24hours and I am symptom free.
Symptoms include: fever (100.4 or higher), headache, shortness of breath, cough, sore throat, vomiting, diarrhea, loss of smell or taste,nausea, fatigue, body aches
_________________________________________ ____________________________________
Staff/Parent/Guardian Signature School Nurse Verification
* IDPH and MCDH may contact you and will generate a release from isolation or quarantine letter after completing the daily HealthAssessments. The number that will appear on your phone is 312-777-1999 and/or COVID Contact. The letter will only be generated ifyou complete the satisfaction survey after your last Health Assessment. If you do not complete the survey, or if you exit the browser, thesystem will not email you the letter. Completion of the daily Health Assessment Surveys will ensure you/your student is able to return toschool as soon as possible.
3/2021 Information may change based upon most recent CDC/IDPH/MCDH guidelines
26
Hello Everyone!Thank you so much for volunteering for the educator Covid Vaccine Clinic to be held in theField House (left side of the building near the football field) at High School, located at_____.Please note our start times for each clinic moved 15 minutes earlier to allow for enough time fortraining.
You will enter at Door 10. You will need to check in at the Volunteer Check in table where youwill sign in, confirm you have no symptoms of Covid, and get a temperature check. You will thenbe directed to the volunteer training area in the field house.
There is a lot of information in this email and I have attached the schedules for the clinics.(Please note I am sending all of Thursday schedules in one email and all of Friday schedules inanother).
I am attaching the consent form that needs to be completed by all MRC volunteers. If youhaven’t yet filled it out, please complete and email it back to me as soon as you are able.
I am also attaching information about the Moderna vaccine. Please read prior to the clinic. Wewill have a nurse from the health department at each of our clinics who will be able to answerany specific questions you may have.
The computer system we will be using is called ABS. We will be accessing those onchromebooks with a mouse (for easier navigating). I have attached screenshots of the screenswe will use so you can at least “see” the system prior to your training on the day you arescheduled.
Information for your day: I’m asking if all nurses could wear a white lab coat (or white shirt orsweater if you do not have a labcoat). I am trying to get us also a vest to wear, but in case thatfalls through, I’d like the nurses to be easily identified. Please know that you can bring water toyour table, but please make sure it has a cap/lid/top. Wear comfy shoes! Everyone must havea surgical mask and nurses doing injections must wear a face shield or eye glasses. Wewill have shields available and we do ask that you take it home, disinfect it, and re-use it if youare coming more than once.
This is going to be a fast paced, high energy, and fun clinic. For those of you who have workedthe MCDH clinics can attest, the average number of injections a nurse gives an hour isapproximately 20. We are aiming for that same goal...20 per nurse per hour (which is about 4-5every fifteen minutes). The clinic is set up for 45 appointments every 15 minutes. I am blessed
2/2021 127
to have 12 nurses (thank you again!) every shift which will give us a little buffer, as well as,help nurses get breaks throughout the day. Many of us will see teachers we know that wehaven’t seen in a long time and it will be very difficult not to be able to chat with them...but timeis of great importance here to keep the line moving well.
As you know, we are vaccinating educators who are thrilled (yet, some nervous) about thisvaccine. It should be a happy rewarding experience for everyone. There may be some peoplewho want to take selfies while getting the shot.the health department does allow this at theirclinics as long as you are not in the picture. Clients, or ourselves, cannot take pictures or videosof the clinic with other people in it (obviously due to HIPAA). We have asked them to comealone to the clinic (not bring their kids, etc) and have informed them that congregating isdiscouraged.
Volunteer Training: The start of your shift will include approximately 10 minutes of “Just inTime” training which is required by the MCDH to go over safety issues. Then, the nurses willbreak off into their own group for approximately 20-25 minutes of vaccine/computer training.
Vaccinators:Moderna Vaccine EAU for Healthcare Providers Administering
Moderna Vaccine EAU for Recipients and Caregivers
i. No diluent needed
ii. 10 dose vial (sometimes 11)
iii. Clear to white Liquid
iv. 0.5 ml dose
v. 2nd dose due in 28 days
Overview of the procedure for a Client Injection: Prior to the client getting to your table, they willhave already had a temperature check, symptom check, they will have verified their ID and theiremployment, and be given a vaccine card with the Moderna lot # on it, and also the date inwhich they can get their 2nd injection (28 days later for Moderna).
1. The client will approach your table.2. Ask the client’s name and find them on your chromebook in the ABS system3. We will re-ask the medical questions to verify the questions they have already
answered:a. Have you had an anaphylactic reaction to any vaccine or injectable mediation
in the past? (If yes they can not receive the vaccine at our clinic)
i. Oral medication anaphylaxis does not exclude them
2/2021 2
28
ii. If they say they carry an epi pen for any reason they need to wait in the
observation area for 30 minutes instead of 15
b. Have you had a vaccine in the past 14 days or plan to in the next 14 days? (Ifthey have received any vaccine in the last 14 day they can not receive the
vaccine at this clinic)
i. TB tests do not count
c. Have you ever had a Covid vaccine? (The February 11 / 12 clinic is for dose 1)
i. In March the question we will then ask them which vaccine they
received just make sure it is Moderna. We will also be checking their
vaccine card.
d. Have you had convalescent plasma or antibody treatment for Covid 19?
i. If yes they can not receive the vaccinee. Verify their date of birth Moderna is for 18 years and older (contact team lead if
a DOB is incorrect)4. We will then ask the client which arm they would like it in and have them sit and bare
their arm. At this point I like to enter the arm and my name in the computer system so Idon’t “forget” the clients name..
5. Give the injection6. Direct(or have your runner direct) the client to the Vaccine Check out Area7. Document there were “no adverse reactions” in the computer system8. HIT SUBMIT…...this is the part that is easy to forget but they cannot check out unless
they are submitted.
Runners: The nurses will have access to runners (hopefully one per table). You can use theserunners however works best for you. Some nurses like to have them wipe off the chairs betweenclients with disinfectant wipes for them, they can open bandaids for you, some like to have them“set up” their vaccine trays for the next dose, they can direct the clients to the Vaccine CheckOut station when you are done...the options are endless! :) They will be responsible for grabbingyou more gloves, wipes, bandaids, etc. Whatever you need! Don’t be afraid to ask them foranything...they are there to serve you :)
Vaccine Drawers: This is an important role...these nurses will be drawing up vaccines for eachtwo nurses they are assigned to. You will get training on the vaccine that day. Drawers may beasked to fill in injecting at times to help give injectors a break.
We will go over all of this information again before your shift but I just wanted to give you someinformation prior to Thursday and Friday.
From the bottom of my heart, and all the educators who will be getting their vaccine fromyou….thank you, thank you, THANK YOU!
2/2021 3
29
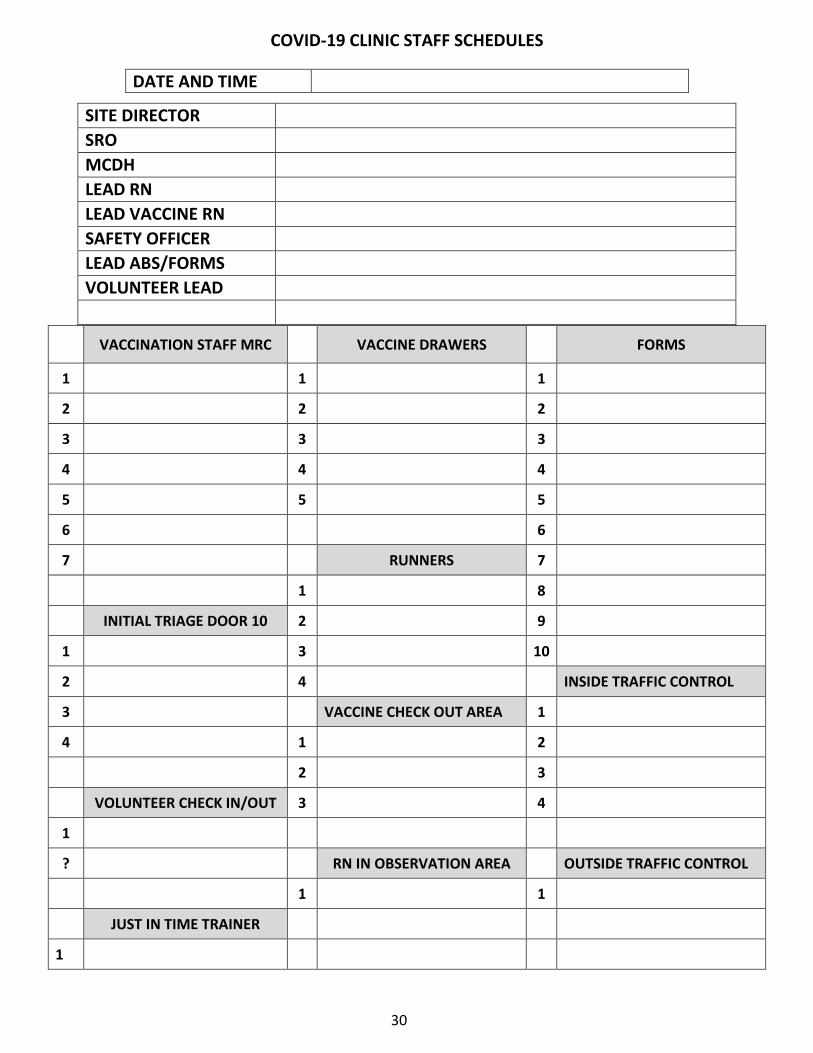
COVID-19 CLINIC STAFF SCHEDULES
DATE AND TIME
VACCINATION STAFF MRC VACCINE DRAWERS FORMS
1 1 1
2 2 2
3 3 3
4 4 4
5 5 5
6 6
7 RUNNERS 7
1 8
INITIAL TRIAGE DOOR 10 2 9
1 3 10
2 4 INSIDE TRAFFIC CONTROL
3 VACCINE CHECK OUT AREA 1
4 1 2
2 3
VOLUNTEER CHECK IN/OUT 3 4
1
? RN IN OBSERVATION AREA OUTSIDE TRAFFIC CONTROL
1 1
JUST IN TIME TRAINER
1
SITE DIRECTOR SRO MCDH LEAD RN LEAD VACCINE RN SAFETY OFFICER LEAD ABS/FORMS VOLUNTEER LEAD
30
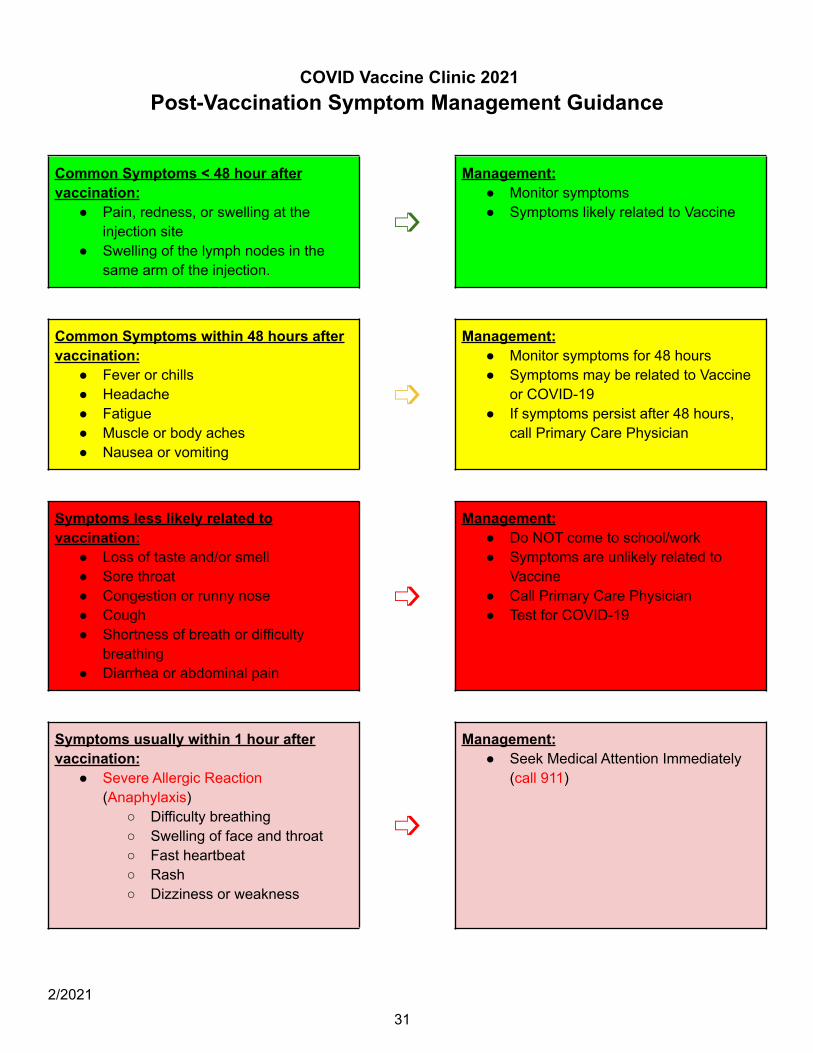
COVID Vaccine Clinic 2021Post-Vaccination Symptom Management Guidance
Common Symptoms < 48 hour aftervaccination:
● Pain, redness, or swelling at theinjection site
● Swelling of the lymph nodes in thesame arm of the injection.
➩
Management:● Monitor symptoms● Symptoms likely related to Vaccine
Common Symptoms within 48 hours aftervaccination:
● Fever or chills● Headache● Fatigue● Muscle or body aches● Nausea or vomiting
➩
Management:● Monitor symptoms for 48 hours● Symptoms may be related to Vaccine
or COVID-19● If symptoms persist after 48 hours,
call Primary Care Physician
Symptoms less likely related tovaccination:
● Loss of taste and/or smell● Sore throat● Congestion or runny nose● Cough● Shortness of breath or difficulty
breathing● Diarrhea or abdominal pain
➩
Management:● Do NOT come to school/work● Symptoms are unlikely related to
Vaccine● Call Primary Care Physician● Test for COVID-19
Symptoms usually within 1 hour aftervaccination:
● Severe Allergic Reaction(Anaphylaxis)
○ Difficulty breathing○ Swelling of face and throat○ Fast heartbeat○ Rash○ Dizziness or weakness
➩
Management:● Seek Medical Attention Immediately
(call 911)
2/2021
31
Related Documents