Presentation topic Schizophrenia spectrum disorder Presented by : Mangal Kardile

Schizophrenia spectrum disorder
Jul 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Presentation topic
Schizophrenia spectrum disorder
Presented by : Mangal Kardile
Spectrum?indicate an apparent qualitative distinction arising from a
quantitative continuum
Schizophrenia spectrum
• A spectrum as it applies to mental disorder is a range of linked conditions, sometimes also extending to include singular symptoms and traits
1) schizotypal personality disorder
2) schizoid personality disorder
3) delusional disorder
4) schizoaffective disorder
5) schizophreniform disorder
History of Schizo-spectrum
• Paul Eugen Bleuler (1857-1939) Swiss psychiatrist
• notable for understanding of mental illness and for coining the terms "schizophrenia
• replaced Kraepelin's term dementia praecox
• especially interested in Sigmund Freud's work in "introspective" & “unconscious” variant
• “Textbook of Psychiatry” (1916)- claimed Nobel prize
What is schizophrenia?
• is a mental disorder characterized by• breakdown of thought processes and by poor
emotional responsiveness• features auditory hallucinations, paranoid or bizarre
delusions, or disorganized speech and thinking• accompanied by significant social or occupational
dysfunction• onset of symptoms occurs in young adulthood, with a
global lifetime prevalence of about 0.3–0.7% • Diagnosis is based on observed behavior and the
patient's reported experiences.
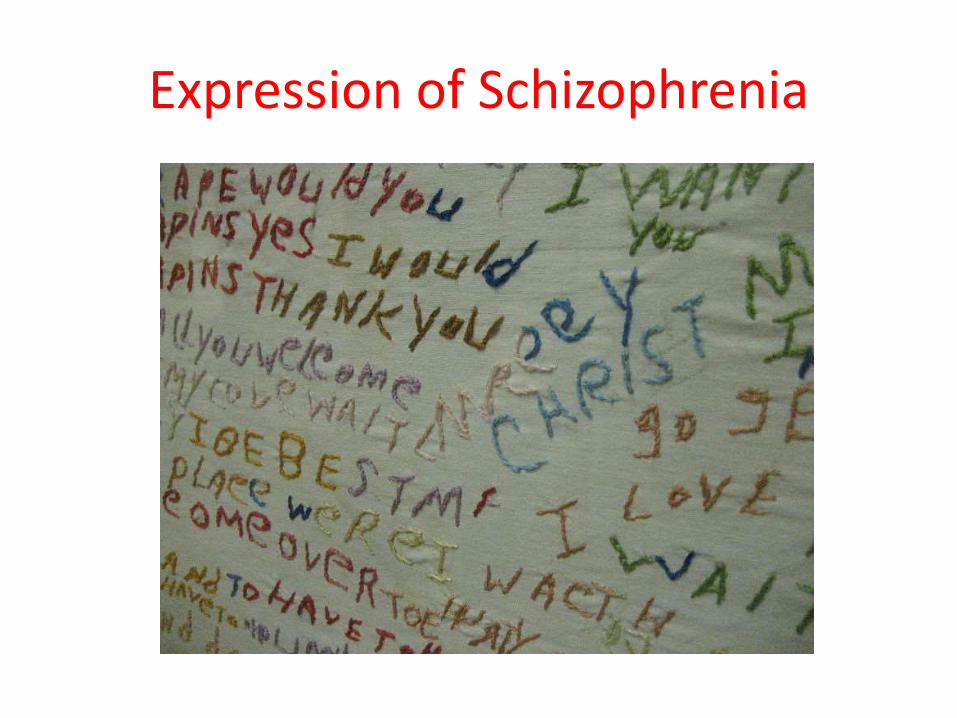
Expression of Schizophrenia
How is it diagnosed?
• American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders, DSM-IV-TR
• World Health Organization's International Statistical Classification of Diseases and Related Health Problems, the ICD-10
• These criteria use the self-reported experiences of the person and reported abnormalities in behavior
• clinical assessment by a mental health professional• Symptoms associated with schizophrenia occur along a
continuum in the population and must reach a certain severity before a diagnosis is made
• As of 2009 there is no objective test
Symptoms
• Characteristic symptoms: Two or more of the following, each present for much of the time during a one-month period (or less, if symptoms remitted with treatment).
• Delusions• Hallucinations• Disorganized speech, which is a manifestation of formal
thought disorder• Grossly disorganized behavior (e.g. dressing
inappropriately, crying frequently) or catatonic behavior• Negative symptoms: Blunted affect (lack or decline in
emotional response), alogia (lack or decline in speech), or avolition (lack or decline in motivation)
Symptoms
• onset is in childhood or adolescence-failure to achieve expected level of interpersonal, academic, or occupational
• Continuous signs of the disturbance persist for at least 6 months- include periods of prodromal or residual symptoms (may be only negative symptoms-apathy)
• Schizoaffective Disorder and Depressive or Bipolar Disorder With Psychotic Features have been ruled out because -
• either (1) no Major Depressive, Manic, or Mixed Episodes have occurred concurrently with the active-phase symptoms;
• (2) if mood episodes have occurred during active-phase, their total duration has been less than half of the total duration of the active periods.
Symptoms
• Acc. To DSM- The disturbance is not due to the direct physiological effects of a substance (e.g., an abused drug, a medication) or a general medical condition
• If there is a history of Autistic Disorder or another Pervasive Developmental Disorder or other communication disorder of childhood onset
- additional diagnosis of Schizophrenia is made only if prominent delusions or hallucinations are also present for at least 1 month (or less if successfully treated).
Schizophrenia subtypes
• Paranoid type: Delusions or auditory hallucinations, but thought disorder, disorganized behavior, or affective flattening are not present
- Delusions are persecutory and/or grandiose, but in addition to these, other themes such as jealousy, religiosity, or somatization may also be present
• Disorganized type: Named hebephrenic schizophrenia in the ICD
- thought disorder and flat affect are present together
• Catatonic type: almost immobile or exhibit agitated, purposeless movement. Symptoms can include catatonic stupor and waxy flexibility
• Undifferentiated type: Psychotic symptoms are present
- criteria for paranoid, disorganized, or catatonic types have not been met
• Residual type: positive symptoms are present at a low intensity only, but continual disturbance of(odd beliefs, unusual perceptual experiences)
1) Schizotypal personality disorder• is a personality disorder characterized by a need for social isolation• anxiety in social situations, odd behavior and thinking, and often unconventional
beliefs. • feel extreme discomfort with maintaining close relationships with people• They frequently misinterpret situations as being strange or having unusual meaning for
them • paranormal and superstitious beliefs are common• seek medical attention for things such as anxiety, depression, or other symptoms• Unusual perceptual experiences, including bodily illusions• Suspiciousness or paranoid ideation• Inappropriate or constricted affect, Ideas of reference (excluding delusions of ref)• Behavior or appearance is odd, eccentric or peculiar- common in individuals related to people with schizophrenia and is believed to be part of
the genetic "spectrum" of schizophrenia• DSM-IV-TR- beginning by early adulthood- DSM-IV designation of schizotypal as a
personality disorder is controversial• In ICD-10- Schizotypal disorder is classified as a clinical disorder associated with
schizophrenia
2) Schizoid personality disorder
• often aloof, cold, and indifferent, which causes interpersonal difficulty• trouble establishing personal relationships or expressing their feelings in a
meaningful way, and may remain passive in the face of unfavorable situations.
• unable to develop accurate reflections of themselves with respect to how well they are getting along with others
• If personal space is violated, they feel suffocated• "feel lost" without the people they are normally around because they
require a sense of security and stability• it is possible for schizoid individuals to form relationshipslong as these modes of relating do not require or force the need for
emotional intimacy---if invaded by others-------they prefer isolation - beginning by early adulthood (age eighteen or older)-It is a requirement of DSM-IV that a diagnosis of any specific personality
disorder also satisfies a set of general personality disorder criteria
3) Delusional disorder
• A delusion is a belief held with strong conviction despite superior evidence to the contrary
• uncommon psychiatric condition in which patients present with circumscribed symptoms of non-bizarre delusions
• absence of prominent hallucinations, thought disorder, mood disorder, or significant flattening of affect
• olfactory or tactile hallucinations related to the content of the delusion may be present
• the delusion or delusions cannot be due to the effects of a drug, medication, or general medical condition
• cannot be diagnosed in an individual previously diagnosed with schizophrenia.
• A person may be high functioning in daily life as this disorder bears no relation to one's IQ
• may not exhibit odd or bizarre behavior aside from these delusions
• Delusional disorders are present in 1.3% of all newly admitted patients to psychiatric hospitals, otherwise uncommon in psychiatric practice
• Peters Delusion Inventory (PDI) which focuses on identifying and understanding delusional thinking
Delusional disorder
• DSM defines six subtypes-• erotomanic -believes that someone is in love with him/her, • grandiose - believes that he/she is the greatest, strongest, fastest, richest,
and/or most intelligent person ever• jealous - believes that the love partner is cheating on him/her • persecutory -believes that someone is following him/her to do some harm
in some way • somatic - believes that he/she has a disease or medical condition and
mixed• The illness is chronic and frequently lifelong• delusions are logically constructed and internally consistent• Despite his/her profound conviction, there is often a quality of
secretiveness or suspicion when the patient is questioned about it• Delusions also occur as symptoms of many other mental disorders,
especially the other psychotic disorders
4) SCHIZOAFFECTIVE DISORDER• A. uninterrupted period of illness during which- Criterion A symptoms of
Schizophrenia are present, also either a Major Depressive Episode or a Manic Episode.
Note: The Major Depressive Episode must include Criterion A1: depressed mood.• B. During the lifetime duration of the illness, delusions and/or hallucinations are
present at least for 2 weeks in the absence of a major mood episode (depressive or manic)
• C. A major mood episode is present for the majority (≥ 50%) of the total duration of the time after Criterion A has been met
• D. Disturbance is not due to direct physiological effects of a substance (e.g., a drug of abuse, medication) or a general medical condition
• Specify Type:• Bipolar Type: If the disturbance includes a Manic or a Mixed Episode (or a Manic
or a Mixed Episode and Major Depressive Episodes)• Depressive Type: If the disturbance only includes Major Depressive Episodes
• Acc. To DSM- there must be a period of at least two weeks of psychosis without mood disorder, and these symptoms cannot be due to medication(s), substance use or another medical condition.
5) Schizophreniform disorder
• Delusions, hallucinations, disorganized speech, grossly abnormal psychomotor behavior, including catatonia, negative symptoms(diminished emotional expression)
• No schizoaffective, Major Depressive, Manic, or Mixed Episodes have occurred concurrently with the active-phase symptoms;
• if mood episodes occurred during active-phase symptoms, their total duration very less
• not due to the direct physiological effects of a substance, medication or a general medical condition
• episode of the disorder lasts at least 1 month but less than 6 months, required to diagnose as schizophrenia
• absence of blunted or flat affect• diagnosis must be made without waiting for recovery, it should be
qualified as “Provisional” ( with/without good prognostic features)e.g. confusion or perplexity at the height of the psychotic episode• good premorbid social and occupational functioning
causes of spectrum???
• Genetic- heritability vary because of the difficulty in separating the effects of genetics and the environment, greatest risk for first-degree relative (6.5%); more than 40% of monozygotic twins
• Environment- factors associated the living environment, prenatal stressors, parenting style
• Substance misuse- more than 50% use cannabis, cocaine, predominantly alcohol abuse
• Socioeconomic, cultural factors- demands frequent medication, rehabilitation, hospital care
• Developmental factors- hypoxia and infection, or stress and malnutrition in the mother during fetal development, born in winter or spring (cold regions and hot regions)
Etiology of spectrum???
• Biochemical factors- too much dopamine activity
• Serotonin- increment in negativity (Clozapine-drug)
• Norepinephrine - impaired emotional gratification,
• GABA- loss of GABAergic neurons in hippocampus
• Glutamate – induce attack (phencyclidine-drug)
• Nicotine – regulates neurotransmitters involved in cognition (good for short term memory)
Etiology of Neuropathology
- Potential Neuropathological basis-
- gray matter loss that occurs as schizophrenia develops neurochemicalabnormalities in cerebral cortex, basal ganglia, limbic system
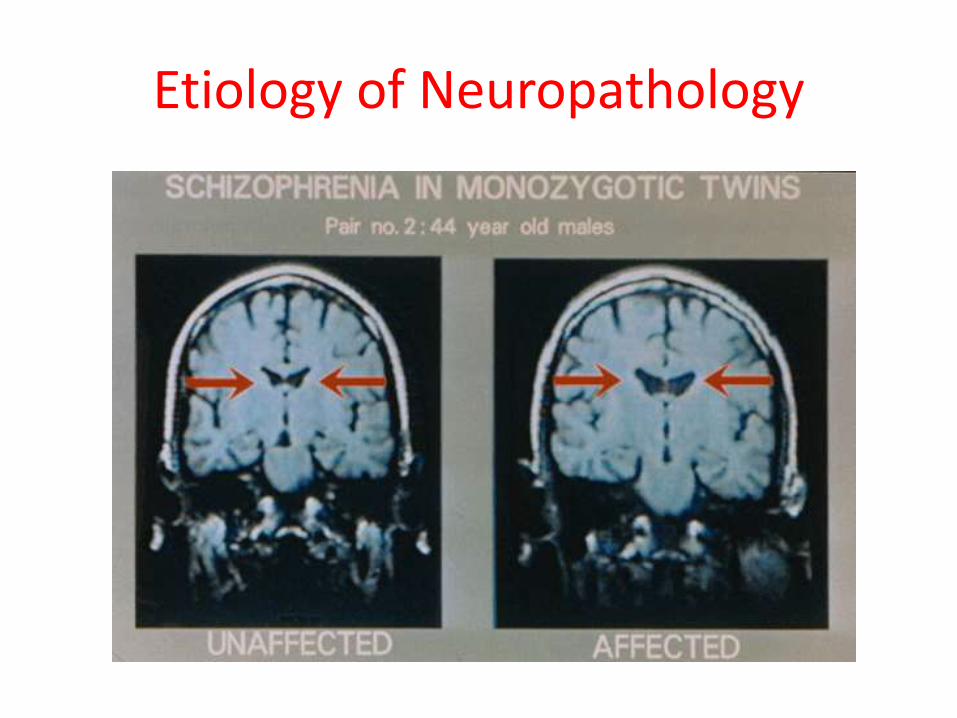
- Loss of brain volume, reduced density of axons, dendrites and synapses- Enlarged ventricles- (lateral and third- computer tomography)- Reduced symmetry in brain areas- Anatomical abnormalities and functional deficits in Prefrontal cortex
- Disorder of brain neural circuits (early developmental lesion of the dopaminergictracts to prefrontal cortex- connection of basal ganglia and cerebellum)- causing negative, positive and cognitive impairments
- Brain metabolism- magnetic resonance spectroscopy (study of specific molecules found – lower level of phosphomonoester, inorganic phosphate, higher level of phosphodiester
Etiology of Neuropathology
Management
• Treated with antipsychotic medications, often in combination with psychological and social supports
• Family Support - individuals diagnosed with schizophrenia are emotionally responsive, particularly to stressful or negative stimuli
• Psychiatric Medicines -atypical antipsychotic medication (e.g.Risperidone, Clozapine)
• Hospitalization may occur for severe episodes either voluntarily or involuntarily
• (Serious side effect of medication -neuroleptic malignant syndrome)• Functional magnetic resonance imaging (fMRI) and other brain
imaging technologies allow for the study of differences in brain activity in people diagnosed with schizophrenia.
• Psychological- Cognitive biases have been identified, insensitivity to problem may cause vulnerability to symptoms or to the disorder
Prognosis
• Consumes great human and economic costs• decreased life expectancy of 12–15 years, primarily
because of its association with obesity, sedentary lifestyles, and smoking, with an increased rate of suicide(occurring in the period following onset or first hospital admission)
• 16.7 million people globally are deemed to have moderate or severe disability from the condition
• Outcomes for schizophrenia appear better in the developing than the developed world
• Schizophrenia and smoking have shown a strong association(80% to 90% as compared with normal 20%)
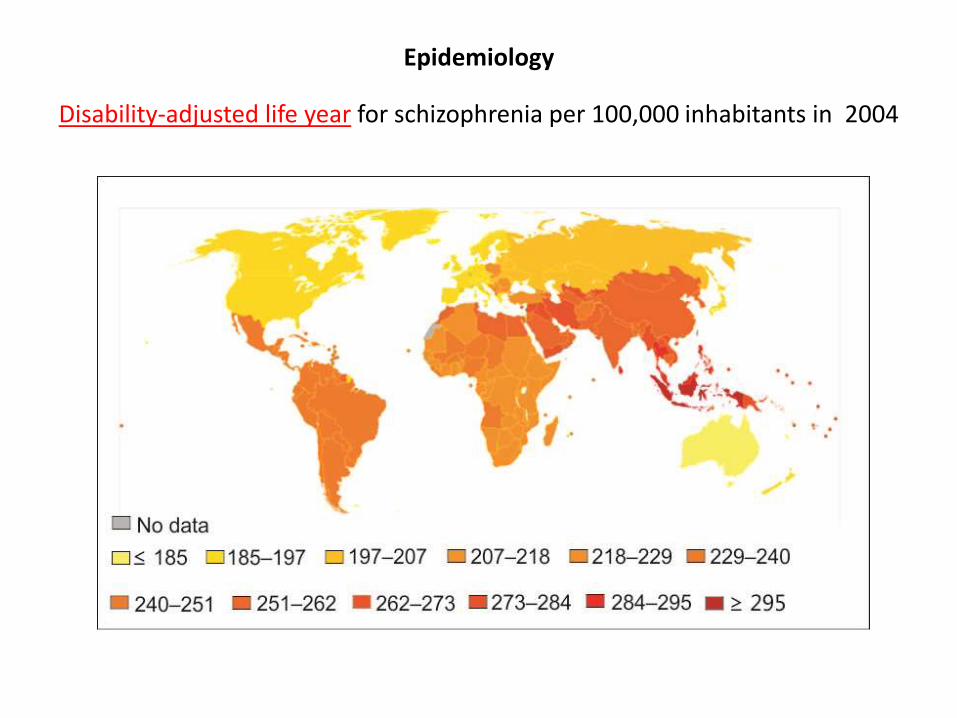
Epidemiology
Disability-adjusted life year for schizophrenia per 100,000 inhabitants in 2004
Epidemiology
• Schizophrenia affects around 0.3–0.7% of people at some point in their life, or 24 million people worldwide as of 2011
• It occurs 1.4 times more frequently in males than females and typically appears earlier in men
• the peak ages of onset are 20–28 years for males and 26–32 years for females
• Onset in childhood is much rarer, as is onset in middle-or old age.
• Some forensic psychiatric studies support serious crimes by schizophrenics – mainly murder of a near/dear one—then surrendering on the spot
• Ongoing research required……….....
Thank you
Related Documents