FEATURE ARTICLE Schizophrenia, neurodevelopment and corpus callosum GM Innocenti 1,2 , F Ansermet 2 and J Parnas 3,4 1 Division of Neuroanatomy and Brain Development, Department of Neuroscience, Karolinska Institutet, Stockholm, Sweden; 2 SUPEA, Unite ´ de Pedopsychiatrie de liaison, Ho ˆ pital Nestle ´ , Lausanne-CHUV, Switzerland; 3 Cognitive Research Unit, Copenhagen University Department of Psychiatry, Hvidovre Hospital, Brøndby, Denmark; 4 The National Research Foundation: Center for Subjectivity Research, University of Copenhagen, Copenhagen, Denmark The Zeitgeist favors an interpretation of schizophrenia as a condition of abnormal connectivity of cortical neurons, particularly in the prefrontal and temporal cortex. The available evidence points to reduced connectivity, a possible consequence of excessive synaptic pruning in development. A decreased thalamic input to the cerebral cortex appears likely, and developmental studies predict that this decrease should entail a secondary loss of both long- and short-range cortico-cortical connections, including connections between the hemi- spheres. Indeed, morphological, electrophysiological and neuropsychological studies over the last two decades suggest that the callosal connections are altered in schizophrenics. However, the alterations are subtle and sometimes inconsistent across studies, and need to be investigated further with new methodologies. Molecular Psychiatry (2003) 8, 261–274. doi:10.1038/sj.mp.4001205 Keywords: neuromorphology; EEG; neuropsychology; hemispheric interactions; cerebral cortex; neural connections; hypoconnectivity; hyperconnectivity; misconnectivity Schizophrenia (S) is a devastating and fascinating condition. At the core of the disease, there is an abnormal processing of internal and external events. The patients experience altered perceptual, cognitive, volitional and emotional states, delusion and hallu- cinations, particularly in the auditory but also in other sensory domains. They often fail to identify the boundaries between self and non-self and those between present, past and future. Cognitive and perceptual information is often associated with inappropriate emotional tags. Not surprisingly per- haps, schizophrenic experience and existence are in a peculiar way altered in relation to the shared intersubjective world, a feature that since Bleuler is sometimes referred to as autism. 1 Indeed, they live in a reality that is, in more or less subtle ways, profoundly different from our own. Connectivism and schizophrenia The task of understanding the pathophysiology of S provides a crucial test to the adequacy of modern Neurosciences in relating brain and mind (see Andreasen 2 ). Current theories stress the involve- ment of multiple neuronal systems, distributed among different brain structures in higher brain functions, 3–5 albeit with regional specialization. Accordingly, the Zeitgeist favors an interpretation of S as a condition of abnormal connectivity of cortical neurons, particularly in the prefrontal and temporal cortex. This hypothesis is not particularly novel and the supporting evidence has been reviewed; 6–11 there- fore, only some of the crucial elements of the hypothesis will be recalled here. Two opposite pathogenetic mechanisms, leading to abnormal connectivity, have been proposed. Synapses may fail to be eliminated in development, specifically during adolescenceFthe hyperconnectivity hypothe- sis 12 For, alternatively, too many synapses are elim- inatedFthe hypoconnectivity hypothesis. 13,14 Both hypotheses seem to be directly testable by neuro- pathological investigations. Nevertheless, they grossly oversimplify the structural–functional rela- tions that characterize cortical connections. The geometry of cortical axonal arbors is responsible for the spatial distribution, amplification and timing of the messages exchanged among neurons. 15,16 There- fore, neuronal interactions could be profoundly altered even by subtle morphological abnormalities in the spatial distribution of synaptic boutons, size of synaptic clusters, length or caliber of axons and axonal branches. Finally, the regulation of synaptic strength in the connections between cortical neurons is extremely complex (eg Markram, 17 Zilberter et al 18 and Zilberter 19 ) and could also be altered in S. The misconnectivity hypothesis of S, 20,21 albeit more difficult to test directly than the hyper- and hypo- connectivity hypotheses, should therefore also be considered at this stage. All the hypotheses mentioned can be grounded in well-characterized developmental processes, and are Received 31 January 2002; revised 27 May 2002; accepted 28 May 2002 Correspondence: Prof GM Innocenti, Division of Neuroanatomy and Brain Development, Department of Neuroscience, Retzius va ¨g 8, Karolinska Institutet, Stockholm S-17177, Sweden. E-mail: [email protected] Molecular Psychiatry (2003) 8, 261–274 & 2003 Nature Publishing Group All rights reserved 1359-4184/03 $25.00 www.nature.com/mp

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
FEATURE ARTICLE
Schizophrenia, neurodevelopment and corpus callosumGM Innocenti1,2, F Ansermet2 and J Parnas3,4
1Division of Neuroanatomy and Brain Development, Department of Neuroscience, Karolinska Institutet, Stockholm, Sweden;2SUPEA, Unite de Pedopsychiatrie de liaison, Hopital Nestle, Lausanne-CHUV, Switzerland; 3Cognitive Research Unit,Copenhagen University Department of Psychiatry, Hvidovre Hospital, Brøndby, Denmark; 4The National Research Foundation:Center for Subjectivity Research, University of Copenhagen, Copenhagen, Denmark
The Zeitgeist favors an interpretation of schizophrenia as a condition of abnormal connectivityof cortical neurons, particularly in the prefrontal and temporal cortex. The available evidencepoints to reduced connectivity, a possible consequence of excessive synaptic pruning indevelopment. A decreased thalamic input to the cerebral cortex appears likely, anddevelopmental studies predict that this decrease should entail a secondary loss of both long-and short-range cortico-cortical connections, including connections between the hemi-spheres. Indeed, morphological, electrophysiological and neuropsychological studies overthe last two decades suggest that the callosal connections are altered in schizophrenics.However, the alterations are subtle and sometimes inconsistent across studies, and need to beinvestigated further with new methodologies.Molecular Psychiatry (2003) 8, 261–274. doi:10.1038/sj.mp.4001205
Keywords: neuromorphology; EEG; neuropsychology; hemispheric interactions; cerebral cortex;neural connections; hypoconnectivity; hyperconnectivity; misconnectivity
Schizophrenia (S) is a devastating and fascinatingcondition. At the core of the disease, there is anabnormal processing of internal and external events.The patients experience altered perceptual, cognitive,volitional and emotional states, delusion and hallu-cinations, particularly in the auditory but also inother sensory domains. They often fail to identify theboundaries between self and non-self and thosebetween present, past and future. Cognitive andperceptual information is often associated withinappropriate emotional tags. Not surprisingly per-haps, schizophrenic experience and existence are in apeculiar way altered in relation to the sharedintersubjective world, a feature that since Bleuler issometimes referred to as autism.1 Indeed, they live ina reality that is, in more or less subtle ways,profoundly different from our own.
Connectivism and schizophrenia
The task of understanding the pathophysiology ofS provides a crucial test to the adequacy of modernNeurosciences in relating brain and mind (seeAndreasen2). Current theories stress the involve-ment of multiple neuronal systems, distributedamong different brain structures in higher brainfunctions,3–5 albeit with regional specialization.
Accordingly, the Zeitgeist favors an interpretation ofS as a condition of abnormal connectivity of corticalneurons, particularly in the prefrontal and temporalcortex. This hypothesis is not particularly novel andthe supporting evidence has been reviewed;6–11 there-fore, only some of the crucial elements of thehypothesis will be recalled here.
Two opposite pathogenetic mechanisms, leading toabnormal connectivity, have been proposed. Synapsesmay fail to be eliminated in development, specificallyduring adolescenceFthe hyperconnectivity hypothe-sis12For, alternatively, too many synapses are elim-inatedFthe hypoconnectivity hypothesis.13,14 Bothhypotheses seem to be directly testable by neuro-pathological investigations. Nevertheless, theygrossly oversimplify the structural–functional rela-tions that characterize cortical connections. Thegeometry of cortical axonal arbors is responsible forthe spatial distribution, amplification and timing ofthe messages exchanged among neurons.15,16 There-fore, neuronal interactions could be profoundlyaltered even by subtle morphological abnormalitiesin the spatial distribution of synaptic boutons, size ofsynaptic clusters, length or caliber of axons andaxonal branches. Finally, the regulation of synapticstrength in the connections between cortical neuronsis extremely complex (eg Markram,17 Zilberter et al18
and Zilberter19) and could also be altered in S. Themisconnectivity hypothesis of S,20,21 albeit moredifficult to test directly than the hyper- and hypo-connectivity hypotheses, should therefore also beconsidered at this stage.
All the hypotheses mentioned can be grounded inwell-characterized developmental processes, and are
Received 31 January 2002; revised 27 May 2002; accepted 28 May2002
Correspondence: Prof GM Innocenti, Division of Neuroanatomyand Brain Development, Department of Neuroscience, Retzius vag8, Karolinska Institutet, Stockholm S-17177, Sweden.E-mail: [email protected]
Molecular Psychiatry (2003) 8, 261–274& 2003 Nature Publishing Group All rights reserved 1359-4184/03 $25.00
www.nature.com/mp

therefore compatible with the attractive proposal thatS might be a consequence of abnormal brain devel-opment.22,23 Animal studies have shown that corticalconnections develop through phases of exuberantgrowth, followed by partial regression. Initially bothlong- and local axonal branches are formed in excessand, subsequently, massive elimination of axonalbranches takes place24–33 (see also Innocenti34 for areview). This regressive phase is concomitant withsynaptogenesis, which eventually leads to the over-production of synapses that are subsequently de-leted.35–38 The elimination of synaptic varicosities inlight-microscopically studied cortico-cortical axonalsystems reaches about 70% as shown in the visual33,39
and the prefrontal cortex.40 In S, a faulty regulation ineither the production or the elimination of axonalbranches and synapses might lead to abnormalconnectivity among cortical neurons, ie, to hyper-,hypo- or misconnectivity. The relatively late onset ofthe psychotic phase, in the second decade of life,suggests that the regressive events, most specificallythe synaptic pruning, could contribute to triggeringthe symptoms, but does not exclude a faulty growthand/or myelination of cortical axons. In fact, theidentification of prodromic symptoms in childrenat risk for S (reviewed in Marenco and Weinberger23
and Parnas and Carter41) suggests that S mightactually relate to earlier developmental events, inparticular to the elimination of axonal branches or tosynaptogenesis.
No anatomical evidence seems to support thehyperconnectivity hypothesis. However, hypercon-nectivity has been hypothesized on evidence ofincreased EEG coherence in schizophrenics (below).
Direct support for the hypoconnectivity hypothesisis also lacking since the cortical connections cannotbe directly visualized and even less quantified inman, a situation that might be coming to an end.42
Nevertheless, strong inferential support to the hy-pothesis comes from the evidence of increasedneuronal density in the cerebral cortex, particularlymarked in the dorsolateral prefrontal cortex,11,43 butalso significant in the temporal cortex43 and inthe visual area 17.44 This finding led to the ‘reducedneuropil hypothesis’.6 The reduction of the neuropilstrongly implies a decrease in the number or thesize of one of its components, essentially axonal anddendritic branches, spines, synaptic boutons (andglial processes), and hence of the connectivity. In linewith this is the finding of reduced spines onthe pyramidal neurons, in both the prefrontaland temporal cortex,45,46 since the spines generallycorrespond to synaptic sites. Evidence of abnormalsynaptic profiles (for recent data on temporalcortex and references, see Ong and Garey47) anddecreased concentration of synaptic proteins,48–50 inthe absence of RNA or mRNA decrease,51 similarlysuggest loss of synaptic boutons. However, dysregula-tion of several presynaptic proteins, including synap-sin II, might also occur independent of synapticelimination.52
The findings quoted above evoke the followingpossible pathogenic scenario. Dysregulation of pre-synaptic proteins might reduce neurotransmitterrelease, which in turn could prevent the activity-dependent stabilization of synaptic boutons and/oraxons. Indeed, decreased synaptic release can create acondition similar to input deprivation, a well-knowncause of the stunted development of cortico-corticalconnections (see below).
The hypoconnectivity hypothesis is compatiblewith several other aspects of S, including the well-established ventricular enlargement (reviewed inHarrison7 and Shenton et al53), the impaired fronto-temporal interactions14,54,55 and the reduced glutama-tergic transmission in S (see, eg, Tsai et al56 andMelone et al57). The decreased glutathione concentra-tion in schizophrenics58 might also be relevant sinceglutathione appears to have a protective role incortical connectivity.
Interestingly, pathologies of the white matter,which decrease cortical connections, in particularmetachromatic leucodystrophy,59 have been foundto be associated with schizophrenic-like symptoms.The hypoconnectivity hypothesis has also been testedin provocative simulation experiments usingneural networks. Progressive pruning of connectionsin neural networks can create parasitic foci of activa-tion, with some resemblance to ‘hallucinatory’percepts.10,60,61
Callosal connections and schizophrenia
Although several lines of work support the hypocon-nectivity hypothesis, the crucial question ofwhich kind of cortical connections might be affectedin S, and to which area(s), is unanswered. The largestfraction of cortical connections originates fromthe thalamus and from the cortex itself. A decreasein the thalamic input to the prefrontal cortex isprobable, since the number of thalamic neurons in theMD nucleus is decreased.62,63 Consistent with adecreased thalamic input is the loss of spines onpresumptive thalamo-recipient basal dendrites of thepyramidal neurons,45,46 and possibly the diminishedexpression of GABA-ergic markers (discussed inLewis8). Interestingly, in monkeys X-irradiated atE33-43, the total number of neurons is reduced by41% in the MD nucleus.11 The monkeys show anincreased density of cortical neurons in the cortex,similar to that observed in the schizophrenic brain.They also show cognitive deficits that becomeapparent only in adolescence.
However, in the schizophrenics and in the irra-diated monkey, the neuropil is not only decreased inthe thalamo-recipient layers 3 and 4 but in otherlayers as well, which suggests that other corticalconnections are also affected. A strong predictionbased on animal work is that the decreased thalamicinput in development would cause an abortivedifferentiation and loss of both long-range and localcortico-cortical connections in the prefrontal cortex.
Schizophrenia, neurodevelopment and corpus callosumGM Innocenti et al
262
Molecular Psychiatry

Indeed, this is precisely what input deprivationcauses, at least in sensory areas.64–67
The decreased size of pyramidal neurons in layer 3of the prefrontal cortex68,69 provides some support tothe hypothesis that cortico-cortical connections aredefective in schizophrenics since these neurons arean important source, as well as target, of cortico-cortical connections. However, the hypothesis can bemore directly tested by studies of callosal connec-tions. The advantage of these connections is thatunlike the other cortico-cortical connections, they canbe investigated morphologically, physiologically andneuropsychologically. They are also the only corticalconnections for which rather complete developmen-tal data exist, including the quantitative estimates ofaxonal elimination in normal development in cat,16,28
monkey,30 and by inference in man.70 The differentia-tion of the terminal arbor of callosal axons has alsobeen studied in detail and a number of developmentalstages have been identified.33,39
Obviously, a deficit of callosal connections cannotby itself explain the pathophysiology of S. Rather,abnormalities in callosal connections are likely to bean indicator of a more diffuse impairment of cortico-cortical networks since the developmental rules thatapply to callosal connections seem to apply to othercortico-cortical connections as well.67,71 Indeed, intra-areal excitatory connections in the prefrontal cortexmight also be altered in S.72
One decisive advantage of studying callosal connec-tions as a way of testing the hypothesis of defectivecortical connections in S is the existence of a largerelevant literature covering morphological, electrophy-siological and neuropsychological issues in normalindividuals, callosally split patients and schizophre-nics. Much of the latter literature was reviewedpreviously.21,73–75 Therefore, the present paper willconcentrate mainly on work over the last decade.
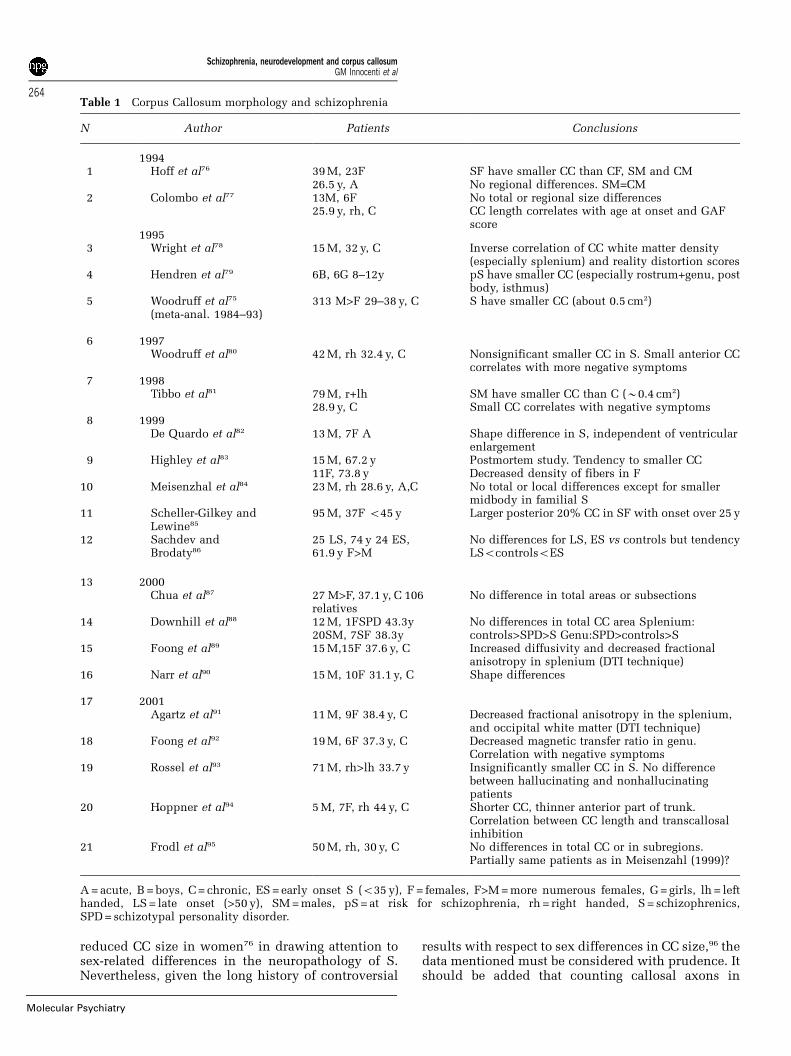
Morphological studiesTable 1 summarizes 21 morphological studies of thecorpus callosum (CC) since 1994. A meta-analysis byWoodruff et al75 on 313 cases reported in the literaturein the years 1984–93 demonstrated a decrease in CCsize of about 0.5 cm2. A subsequent study by Hoff etal76 in first-episode schizophrenics found a similardecrease, but only in women. A study by Hendren etal79 on 12 children with schizotypal personality and/or early onset S also found a smaller CC (about 1 cm)in the patients. These findings were not consistentwith the study by Colombo et al77, who howeverfound a shorter CC in the schizophrenics, a findinglater corroborated by Hoppner et al.94 A subsequentstudy by Woodruff et al80 on 42 right-handed male,chronic schizophrenics could find only a trendtowards a smaller CC in the patients. Similar resultswere obtained in a study by the same team on 71 malepatients, which however aimed at testing differencesin CC size between hallucinating and nonhallucinat-ing cases.93 Tibbo et al81 confirmed a reduction of theCC (of 0.4 cm2) in 79 male schizophrenics and found
an association between small CC and negativesymptoms. Subsequently, Highley et al,83 Meisenzhalet al,84 Sachdev and Brodaly,86 and Downhill et al88
found tendencies towards a total or local decreasedCC size, although statistical significance was reachedonly in a few of them.
Finally, Chua et al87 found no difference in total CCsize or in the size of CC sectors in familial schizo-phrenics, compared to their relatives or to controls.Interestingly, they suggested that the decreased CCmight be a trait of nongenetic factors influencing S.
One study85 found a 20% larger posterior CC inschizophrenic females with onset below 25 years thanin later-onset females or males.
The conclusion from the studies mentioned aboveseems to be that the differences in the size of the CCare subtle; therefore, they might be obscured byvariability in sampling, population heterogeneity,and sample sizes highly conductive to Type II error.Rossell et al93 estimated that in order to obtainstatistical significance with a reduction of CC area of0.20 cm2 in the patients, a sample of 308 individualsshould be analyzed. The findings can also beconfounded by a number of other methodologicalproblems, including the precision and reproducibilityof the midsagittal sectioning, the possible influence ofsex and handedness, the age of onset, duration andsymptomatological profile of the disease. Further-more, CC size should probably be corrected for totalbrain size, but although several methods exist, none isfully satisfactory.96 Also, if the decreased CC is due toloss of callosal axons (below) and this significantlycontributes to decreasing brain size (for example, byreducing the volume of the neuropil, that of the whitematter, or of the cortical neurons), the correctionwould, in fact, tend to obscure the finding. Finally,the studies exploring regional differences in CC sizeare particularly difficult to interpret since methods ofCC partitioning vary across studies (reviewed inBishop and Wahlstein96), including in S research,and the size of the CC partitions can be influenced byCC shape.70
On the whole, the majority of the studies found areduction of the CC in the schizophrenics, as alsonoticed in a review97of 27 imaging studies publishedbetween 1986 and 2000. At first glance, theseconclusions seem to support the hypoconnectivityhypothesis. Indeed, the smaller CC might be dueeither to a loss of interhemispheric axons or to adecrease in the thickness of the axons. In principle, itshould be possible to distinguish between these twoalternatives by counting callosal axons postmortem.In the best and most recent study of this kind,83 adecreased density of axons (suggesting a decreasednumber of axons) has indeed been reported forschizophrenic women, but not for men. The decreasewas distributed over the whole CC with prevalence inthe genu and rostral part of the body. Interestingly,these are the regions where axons interconnecting theprefrontal cortex cross the midline98 (Figure 1). Thestudy mentioned83 concurs with the report of a
Schizophrenia, neurodevelopment and corpus callosumGM Innocenti et al
263
Molecular Psychiatry
reduced CC size in women76 in drawing attention tosex-related differences in the neuropathology of S.Nevertheless, given the long history of controversial
results with respect to sex differences in CC size,96 thedata mentioned must be considered with prudence. Itshould be added that counting callosal axons in
Table 1 Corpus Callosum morphology and schizophrenia
N Author Patients Conclusions
19941 Hoff et al76 39 M, 23F SF have smaller CC than CF, SM and CM
26.5 y, A No regional differences. SM=CM2 Colombo et al77 13M, 6F No total or regional size differences
25.9 y, rh, C CC length correlates with age at onset and GAFscore
19953 Wright et al78 15 M, 32 y, C Inverse correlation of CC white matter density
(especially splenium) and reality distortion scores4 Hendren et al79 6B, 6G 8–12y pS have smaller CC (especially rostrum+genu, post
body, isthmus)5 Woodruff et al75
(meta-anal. 1984–93)313 M>F 29–38 y, C S have smaller CC (about 0.5 cm2)
6 1997Woodruff et al80 42 M, rh 32.4 y, C Nonsignificant smaller CC in S. Small anterior CC
correlates with more negative symptoms7 1998
Tibbo et al81 79 M, r+lh SM have smaller CC than C (B0.4 cm2)28.9 y, C Small CC correlates with negative symptoms
8 1999De Quardo et al82 13 M, 7F A Shape difference in S, independent of ventricular
enlargement9 Highley et al83 15 M, 67.2 y Postmortem study. Tendency to smaller CC
11F, 73.8 y Decreased density of fibers in F10 Meisenzhal et al84 23 M, rh 28.6 y, A,C No total or local differences except for smaller
midbody in familial S11 Scheller-Gilkey and
Lewine85
95 M, 37F o45 y Larger posterior 20% CC in SF with onset over 25 y
12 Sachdev andBrodaty86
25 LS, 74 y 24 ES,61.9 y F>M
No differences for LS, ES vs controls but tendencyLSocontrolsoES
13 2000Chua et al87 27 M>F, 37.1 y, C 106
relativesNo difference in total areas or subsections
14 Downhill et al88 12 M, 1FSPD 43.3y20SM, 7SF 38.3y
No differences in total CC area Splenium:controls>SPD>S Genu:SPD>controls>S
15 Foong et al89 15 M,15F 37.6 y, C Increased diffusivity and decreased fractionalanisotropy in splenium (DTI technique)
16 Narr et al90 15 M, 10F 31.1 y, C Shape differences
17 2001Agartz et al91 11 M, 9F 38.4 y, C Decreased fractional anisotropy in the splenium,
and occipital white matter (DTI technique)18 Foong et al92 19 M, 6F 37.3 y, C Decreased magnetic transfer ratio in genu.
Correlation with negative symptoms19 Rossel et al93 71 M, rh>lh 33.7 y Insignificantly smaller CC in S. No difference
between hallucinating and nonhallucinatingpatients
20 Hoppner et al94 5 M, 7F, rh 44 y, C Shorter CC, thinner anterior part of trunk.Correlation between CC length and transcallosalinhibition
21 Frodl et al95 50 M, rh, 30 y, C No differences in total CC or in subregions.Partially same patients as in Meisenzahl (1999)?
A = acute, B = boys, C = chronic, ES = early onset S (o35 y), F = females, F>M = more numerous females, G = girls, lh = lefthanded, LS = late onset (>50 y), SM = males, pS = at risk for schizophrenia, rh = right handed, S = schizophrenics,SPD = schizotypal personality disorder.
Schizophrenia, neurodevelopment and corpus callosumGM Innocenti et al
264
Molecular Psychiatry

humans can probably only be done with opticalmicroscopy, since the tissue is exceedingly difficult topreserve for high quality electron microscopy. There-fore, the counts can be accurate, at best, for axonswhose diameter exceeds the resolution of the lightmicroscope (about 0.2 mm), and the proportion ofaxons missed in the counts can be very large. Forexample, four times more axons were countedelectron microscopically than light microscopicallyin the cat.100 Therefore, a decrease in the size ofcallosal axons in S could be mistakenly interpreted asa loss of axons. Furthermore, it is unclear if the countsshould be corrected for brain size, because there areno robust reasons to expect that the number ofcallosal axons increases with brain size.
Another possible cause for the reduced CC size in Sis a reduction in the diameter of the callosal axonsand/or of their myelin sheaths, which appear to be themain determinant of CC size in development. Indeed,in children, as in animals, CC size increases progres-sively, in parallel with increased axonal caliber andmyelination.70
Four imaging studies suggest that myelination ofCC axons might be abnormal in S. A decrease in thedensity of the inferior part of the CC was reported,and was found to correlate with the reality distortionscore.78 Also, decreased fractional anisotropy wasfound in the splenium of the CC using tensordiffusion imaging (TDI),89,91 possibly involving axonsthat interconnect temporal and/or occipital areas.98
A decreased magnetic transfer ratio was found in thegenu,92 possibly betraying abnormal connections
between the prefrontal areas.98 Relevant to the sameissue is the preliminary finding of increased inter-hemispheric conduction time as estimated by thelatency of the transcallosal inhibition of motorresponse of the first dorsal interossus muscle in 10 Spatients.100 Patients were found to have an interhemi-spheric conduction time of 15.3 vs 12.4 ms incontrols. The duration of inhibition was also in-creased. This study recalls the finding of an increasedconduction time in schizophrenics (10 vs 4 ms) basedon a behavioral protocol.101 However, electrophysio-logical findings suggesting decreased conductiontime in S have also been reported (Gulmaum et al102
and below). Furthermore, the increased latency ofinhibition could not be confirmed by Hoppner et al94
in a study on 12 patients; the increased duration ofinhibition was confirmed, but its relation to CCconduction properties is obscure.
The studies mentioned as well as the reports ofshape differences in the CC82,90 indicate new avenuesfor CC investigations that might become prominent inthe coming years.
Electrophysiological studiesAt least since the studies of Livanov (quoted byLuria103), electrophysiological techniques have pro-vided another way of assaying callosal connectivity inS. Two methods have been used: the difference in thelatency of responses to ipsilateral and contralateralsensory stimuli and the study of interhemisphericEEG coherence (ICoh). The rationale for using thesemethods for assaying callosal connections is wellgrounded in animal studies and in some humanstudies, the review of which goes beyond the goals ofthis paper. Suffice it to say that the response of thesomatosensory cortex to stimuli in the ipsilateralperiphery is in part due to transmission across theCC.104–106 Inactivation of the CC eliminates the earlycomponent of the ipsilateral response without mod-ifying the contralateral response;104 therefore, thelatency difference between the responses to ipsilat-eral and contralateral stimulation provides an esti-mate of the transcallosal conduction time.107
EEG coherence, on the other hand, measures thestability of frequency relations between cortical oscil-lators, and therefore can identify spatially distributedsynchronous neuronal assemblies. From the animalwork, it appears that the integrity of callosal connec-tions is a prerequisite to the formation of synchronousneuronal assemblies in the two hemispheres, oscillat-ing in the gamma frequency band.108–111 Similarfindings and interpretations were extended to hu-mans.112 The role of callosal connections in establish-ing coherence in other frequency bands is less clear.
Several studies in the 1980s74 reported a decrease inthe difference in the latency of evoked potentials toipsilateral vs contralateral somesthesic stimulation inS, a finding that is difficult to reconcile with thehypothesis of callosal hypoconnectivity (but seebelow). An early study also provided evidence ofincreased ICoh in S, when care was taken to avoid the
Figure 1 Distribution in the CC, of axons interconnectingprefrontal and temporal cortex according to De Lacosteet al.98
Schizophrenia, neurodevelopment and corpus callosumGM Innocenti et al
265
Molecular Psychiatry

confounding effect of common referencing of thesignals and of medication.113 The increase wasrestricted to the theta band.
Table 2 shows the result of 12 interhemisphericand/or intrahemispheric EEG coherence studies overthe last decade. Of the 10 studies dealing withinterhemispheric coherence, seven reported coher-ence increase, two coherence decrease, and one nodifferences between controls and S. Intrahemisphericcoherence showed coherence decrease in four ofseven studies and increase in three studies.
Table 3 shows that these studies differ in manymethodological aspects, ie, the patient condition withrespect to medication and sex ratio, the type ofderivation, with most studies using the linked earsreference, three using bipolar derivation and oneusing vertex referenced recordings. They also differ inthe frequency band analyzed, with no studies addres-sing specifically the gamma band, now a candidatecarrier of perceptual processes (below). Finally, theydiffer in the conditions of EEG recording, with somestudies performed during tasks, others at rest.
The relation between ICoh coherence and CCintegrity is stressed by a single case study of a 28-year-old schizophrenic, with lipoma of the spleniumof the CC.120 ICoh was decreased over the centralcortex for alpha and beta frequencies and over central,parietal, occipital and temporal regions for the deltaand theta frequencies.
Some of the difficulties with the EEG studies in Sare illustrated by the results of Morrison-Stewart etal.116 The EEG responses were task-dependent, withmental calculus increasing, and a visuospatial taskdecreasing ICoh over the frontal and central electro-des. They were also related to medication, with
medicated patients responding as controls, with theexception of a lack of ICoh increase at the frontalmostelectrodes F1–F2, in the calculus task, and an increasein ICoh over the temporal electrodes T5–T6, duringthe visuospatial task. The unmedicated patientsshowed virtually no ICoh changes in either task.
Other difficulties are illustrated by the differentresults of the two studies that examined interhemi-spheric coherence between the posterior temporalregions T5–T6 under similar conditions of rest witheyes closed. One study115 found increased ICoh and theother124 decreased ICoh in the delta band. Theseconflicting findings might be related to the differentwidth of the delta band considered, or to the use ofdifferent reference electrodes in the two studies. Thefact that one group studied mainly drug-free, acuteschizophrenics.115 and the other medicated, chroniccases124 might contribute to the different findings.However, the latter interpretation is weakened by thefact that ICoh was also decreased in the asymptomaticsiblings of S patients.124 This finding seems to weakenthe possibility of viewing lowered EEG coherence as acorrelate of hypoconnectivity and/or that hypoconnec-tivity might be a cause of psychotic symptoms. It maybe interpreted as a correlate of endophenotypic vulner-ability to S, rather than of psychotic symptoms per se.
Neuropsychological studiesNeuropsychological studies of interhemispheric trans-fer in schizophrenics have provided evidence ofimpaired interhemispheric communication. Follow-ing the initial observations of Beaumont andDimond,125 patients have often been reported to beimpaired in matching stimuli presented separately tothe right and the left hemisphere. This suggests that
Table 2 EEG coherence abnormalities in schizophrenics
N Year Authors EEG coherence Location; condition
Intrah Interh
1 1989 Merrin et al113 + + Fronto-temporo-parietal; eyes open and tasks2 1991 Michelogiannis et al114 � +? Postcentral left; rest vs motor task3 1992 Nagase et al115 + O1–O2, T5–T6; rest eyes closed4 1996 Morrison-Stewart et al116
Treated =/+ Prefrontal tasks/visuospatial taskUntreated �/+* Prefrontal task/visuospatial task
5 1996 Merrin et al117 � �** C3–C4; eyes open or closed6 1997 Mann et al118 + ns+ Frontal; rest, eyes closed or open7 1997 Norman et al119 � Fronto-temporal decrease relates to reality distortion;
tasks as in 48 1997 Pinkofski et al120 � Temporal, parietal, occipital,
CC lipoma Case report9 1998 Tauscher et al121 � = Local frontal; fixation
10 1998 Wada et al122 + = at rest, increased reactivity F3, F4, T5, T6; flashes11 1998 Wada et al123 + Higher at rest, decreased reactivity Left, C3–O1, flashes12 2001 Winterer et al124 � T5–T6; rest eyes closed
+, � and = denote changes relative to the controls; ? ICoh not directly evaluated but less differences between hemispheres inS; * no ICoh changes during the tasks; ** coherence decrease with increasing negative symptoms; ns+, non-significantincrease.
Schizophrenia, neurodevelopment and corpus callosumGM Innocenti et al
266
Molecular Psychiatry

the communication between the hemispheres, via theCC and possibly the anterior commissure, is impaired.
David concluded his 1989 review73 by stating that‘Experiments requiring integration of stimuli pre-sented across the visual field, which presumablyrelies on an efficient CC, show impairment inschizophrenics, and this is especially so for non-verbal stimuli’. Similarly, Coger and Serafetinidesconcluded their 1990 review74 by stating: ‘The datafrom behavioral studies appear to support the notionof a problem associated with the transfer of informa-tion between the two cerebral hemispheres for somegroups of schizophrenic patients. Some inconsisten-cies in the data from different studies are indicative ofuncontrolled sources of variation’.
Along the same lines, recently Mohr et al126 studied12 male S subjects and reported that, as withcallosally split patients, they failed to show anyadvantage in the identification of words presented toboth hemispheres, compared to lateralized presenta-tion. Spivak et al127 studied 60 right-handed malepatients and found that S subjects failed to extinguishbilaterally presented somatosensory stimuli. Finally,12 S patients were found to fail in a bimanualcoordination task, although this impairment mayrelate to attentional deficits, not necessarily tointerhemispheric integration.128
The results mentioned are compatible with thenotion of callosal hypoconnectivity. However, they
have the shortcoming of not testing specifically thecallosal connections between the prefrontal areas, forwhich the evidence of decreased connectivity ispresently the strongest.
David and collaborators have provided evidence ofinterhemispheric interference in a lateralized Strooptest.129–131 The Stroop test more specifically relates toprefrontal cortex activation (see Audenaert et al132 fora recent confirmation). In the interhemispheric variantused by David, a color strip was projected to onevisual hemifield and the color word to the otherhemifield. In normal individuals or in nonschizo-phrenic patients, with stimuli presented in the samehemifield or across the hemifields, the responselatency to the stimulus is longer when the color andthe color word are incongruous than when they arecongruous (the Stroop effect). However, the differencedecreases when the stimuli are separated in the twohemifields. Instead, in S patients the divided pre-sentation increased the Stroop effect. This is due toan increased facilitation of the response when thestimuli are congruous, and to a decreased interferencewhen the stimuli are incongruous.133 The Stroop effectwas decreased in an acallosal subject, suggestingthat the CC, ‘by acting as a partial barrier, mediatesthe interhemispheric Stroop effect’.129 Therefore, thefinding in S patients was interpreted as evidence ofincreased callosal connectivity. This appears to beincompatible with the hypoconnectivity hypothesis
Table 3 EEG coherence abnormalities in schizophrenics
N Patients Controls EEG Task
N Age/sex Med N Age/sex Sy Ref Band
1 10C 43.4/M n 13 41.5/M Bipol y 3.5–7 Hz2 18C 34.5/M=F y 30 29/M=F 10/20 RLe a Finger movement, left hand3 9A, 2C 28.1/M=F n 15 25.4/M=F 10/20 RLe d 2–4 Hz b
13–30 HzRest eye closed
4 30C 32.1/M>F 20 y, 10 n 30 30.3/M>F 10/20 RLe a Mental calculus,visuospatial task
5 17C 38.8/M n F F 10/20 Cz a Eyes open or closed6 26A,
11C27.8/M>F n Bipol F3C3 0.5–30 Hz Rest eyes open, rest eyes closed
n F3T3 No band diff. Effects in siblings30 26.6 M>F F4T4
19sb 25.7/ M>F F4C4
7 73 32.3/M>F y 10/20 RLe a Mental calculus andvisuospatialas in 4
9 16C 27.6/M=F n 16 27.3 10/20 RLe a,W also b1,d Fixation10 18A 24.3/M=F n 30 22.3/M=F 10/20 RLe 14.1–15.1 Hz Flash at 15/s F3,F4, T5,T6
11 18A 24.3/M=F n 30 22.3/M=F Bipol d 2–3.5 Hz Flash at 5 and 15/s C3–O1
12 56C 35.2/M>F y 32 32.1/M>F d 0.5-5.5 Hz Rest eyes closed76sb 35.8/M>F n
10/20 Cz59C 36.4/M>F y 26 33.4/MoF Effects in siblings90sb 36.8/M>F n
A = acute, C = chronic, sb = siblings, RLe = linked ears, M = F: about the same number of males and females; y = yes, n = no,treatment at the time of the study.
Schizophrenia, neurodevelopment and corpus callosumGM Innocenti et al
267
Molecular Psychiatry

(but see below). However, an attempt to relate theStroop scores to the CC size has provided statisticallysignificant correlations between the Stroop scores andthe posterior CC, in a pooled sample of patients andcontrols.80 This complicates the interpretation of thelateralized Stroop effect as a function dependent onthe interaction between prefrontal areas.
Callosal markers and symptomatologyThe fundamental question of the relation betweenanatomical, electrophysiological or neuropsychologi-cal markers of callosal abnormality and S can betackled in at least two different ways. David131,134 hasreviewed the association between complete or partialCC agenesis and psychosis. Out of 17 cases of callosalabnormalities seven had S, four had other kinds ofpsychosis, three had mood disorders and two hadnon-psychiatric diagnoses. Therefore, although theCC may be abnormal in S, abnormal CC does notnecessarily cause S, although the frequency of S inthis group is clearly much higher than in the normalpopulation.
In other studies, the association between anatomi-cal, electrophysiological or neuropsychological callo-sal parameters, and symptoms has been analyzed.Results collected over the last decade are shown inTable 4. The important study of Gunther et al135
showed a decreased CC in 15 patients with negativesymptoms, compared with 14 patients with positivesymptoms. Although the differences with the care-fully selected control subjects were statisticallyinsignificant, not surprisingly due to the smallsample, CC size in the control group fell betweenthe two S groups. A positive correlation between CCsize and cerebral blood flow was also found.135
Negative correlation between CC size and negativesymptoms was found by Tibbo et al.81 The alterationsin S patients with negative symptoms might relate tothe anterior part of the CC, whose size appears to bereduced80 and where abnormalities were localizedwith MTR.92 In two separate studies117,137 examining atotal of 31 male, unmedicated patients, Merrin andcollaborators reported a negative correlation betweenICoh in the a band of the EEG and negativesymptoms.117,137
Other associations between CC markers and S havealso been reported (Table 4), but await confirmation.
Schizophrenia and ‘binding’ processes
There exists a large set of EEG data in S, most ofwhich cannot be interpreted in terms of corticalconnectivity and are therefore not clearly relevant tothe goals of this paper. An exception is a handful ofrecent studies on the gamma frequency band, whoseinterest is two-fold. First, evidence has accumulatedthat the activity in the gamma band might be involvedin integrating the activity of separate neuronal groups,representing different features of a perceived object,into a perceptually coherent whole, a process referredto as ‘binding’.137–140 Second, cortico-cortical connec-
tions, in particular callosal connections, appear to beinvolved in the synchronization of spatially separateneuronal populations, in the gamma band.108–112
Therefore, a deficit in the gamma band in S mightrefer both to the dissociations observed within andbetween thinking, perceiving and feeling, which is ahallmark of S,141–143 and to the altered cortico-corticalconnectivity, in particular the callosal connectivity.
A deficit in the gamma band in S patients wasshown by the inability of the patients to followauditory stimulus frequencies in the 40 Hz fre-quency.144 In a backward masking paradigm, Spatients were also found to lack a gamma frequencyoscillation.145 Finally, Haig et al146 reported a de-creased gamma band response in an oddball auditoryparadigm using ERPs. A subsequent study from thesame group reported a reduced gamma amplituderelated to novelty processing, in the right hemisphere,and a delayed latency of gamma activity related tonovelty and routinization, in the left hemisphere.147
These findings were interpreted as ‘a disruptedbalance between the two hemispheres in patientswith S’. Whether such an imbalance might implyabnormal functioning of callosal connection is un-clear, but plausible.
A direct test of the hypothesis that S patients mightbe impaired in visual binding processes,20 albeit notnecessarily due to CC abnormalities, was attempted ina group of 10 chronic patients, nine first admissionpatients, and 10 patients with prodromal schizotypaldisorders.148 Based on the number of correct re-sponses in figure detection tasks and in Muller–Lyervisual illusion, it was concluded that the chronicschizophrenics showed deteriorated performance,while, surprisingly, the prodromal disorder groupshowed improved performance in visual binding.
Developmental-pathogenic scenarios
On the whole, callosal studies support the notion thatcortico-cortical connections are abnormal in S pa-tients. Most of the findings, in particular the anato-mical evidence of a reduced CC and the neuro-psychological evidence of impaired interhemisphericintegration, fit the hypoconnectivity hypothesis, bet-ter than the hyperconnectivity hypothesis. However,the S patients are obviously not split-brains. Probably,the reduced callosal connectivity is paralleled bysome reorganization and abnormality in the remain-ing axons along the lines of the misconnectivityhypothesis. For example, the partial loss of callosalaxons in S, could induce the remaining axons toincrease their number of boutons and/or sprout intovacated territories. The consequence would be anenhanced rather than decreased coupling betweenthe hemispheres because each callosally projectingneuron in one hemisphere could more powerfullycontrol the excitability of neurons in the otherhemisphere, and in a broader than normal territory.This might explain the apparently paradoxical find-ing, in S patients, of an increased ICoh, an enhanced
Schizophrenia, neurodevelopment and corpus callosumGM Innocenti et al
268
Molecular Psychiatry

Stroop effect and decreased interhemispheric transfertime, as judged by the difference in response latencyto ipsilateral and contralateral stimulations.
Unfortunately, uncertainties on how precisely callo-sal connections are modified in S hinder the possibi-lity of postulating a single, detailed, developmentalpathogenic scenario for the likely callosal abnormal-ities. At least three scenarios can be considered.
The first is that callosal connections might be theunique and specific target of S. This seems unlikely.As has been repeatedly stressed in this paper andelsewhere (eg Zufferey et al67 and Kennedy et al71 andreferences therein), callosal connections are function-ally and developmentally similar to other cortico-cortical connections and, aside from the instance ofcommissural agenesis, they are not reported to be thetarget of specific pathologies. Furthermore, it isimplausible that even a severe loss of callosalconnections alone could, be responsible for theneuropil reduction reported in the S cortex. Twoother possible scenarios remain.
The reported morphological, electrophysio-logical and neuropsychological callosal abnormalitiesmight all be secondary to abnormalities of onehemisphere. Concurring genetic and epigeneticfactors might alter specifically one hemisphere,because they target specific functional domains thatare lateralized in the human brain.152–155 This wouldbe reflected in the altered callosal connectivity to andfrom the affected hemisphere. The possibility that theleft hemisphere may be anatomically and electrophy-siologically more affected than the right hemispherefits with a number of anatomical findings, in
particular, the greater enlargement of the left thanthe right lateral ventricles.7,53,149 It also fits with theview of a more negative-emotion-prone right hemi-sphere and with the possible role of the left hemi-sphere as the ‘interpreter’.150 Indeed, some of therecognized key symptoms of S, in particular socialwithdrawal, anhedonia and ‘cognitive slippage’,143 fitwhat one would expect from left hemisphere dis-turbance and consequent imbalance between rightand left hemisphere functions. Clearly, the issue ofright–left hemisphere differences in S requires furtherattention, and indeed a substantial although some-what controversial literature exists in this domain.151
Interestingly, some of the key anatomical findingssupporting the notion of hypoconnectivity in S derivefrom studies of the left hemisphere.44,63,68,69 A specificlinkage between left hemisphere and S is also explicitin proposals relating the phylogenetic origins oflanguage and S.152–154 Unfortunately, the genes re-sponsible for lateralization are undefined, and theirnumber and modalities of phenotypic expression arematters of debate.156 Thus, the genetic hypotheses onS, although relevant and stimulating, are insuffi-ciently specified in neurobiological terms to accountfor the structural changes that might underlie thepsychosis, its pathophysiology and symptomatology.
The third scenario is that the disturbance of callosalconnections might reflect a more widespread failurein cortico-cortical connectivity, although with differ-ences across areas.11 This view is based on thesimilarities in the processes that govern the develop-ment of callosal and of other cortico-cortical connec-tions. As mentioned earlier in this paper, both sets of
Table 4 Correlation between callosal markers, symptoms and/or other variables
Gunther et al (1991):135 Smaller CC in negative symptom patients than in positive symptom patients. Positive correlationbetween CC size and cerebral blood flow.
Merrin and Floyd (1992):117 Negative correlation between EEG a (ICoh) in the frontal region and negative symptoms.
Colombo et al (1994):77 Positive correlation between CC length and global adjustment factor (GAF) score and age at onset.
Phillips et al (1996):133 No correlation between Stroop effects, illness stage and subtype.
Merrin and Floyd (1996):137 Negative correlation between EEG a (ICoh) in the frontal region and negative symptoms.
Woodruff et al (1997):80 Positive correlation between facilitation at Stroop and posterior CC areas; negative correlationbetween interference at Stroop and posterior CC areas; negative correlation between anterior CC areas and negativesymptoms (avolition, anhedonia, affective flattening).
Tibbo et al (1998):81 Negative correlation between CC size and negative symptoms.
Downhill et al (2000):88 Negative correlation between CC size and severity of positive symptoms. No correlation withnegative symptoms.
Rossell et al (2001):93 No differences in CC total or regional size between hallucinating and nonhallucinating patients.
Foong et al (2001):92 MTR reduction in genu, correlates with negative, not with positive symptoms.
Hoppner et al (2001):94 Positive correlation between CC length (not CC thickness) and duration of transcallosal mediatedinhibition.
Frodl et al (2001):95 Positive correlation between size of posterior CC body and amplitude of late components of P300.
Schizophrenia, neurodevelopment and corpus callosumGM Innocenti et al
269
Molecular Psychiatry

connections develop through a combination of target-aimed growth, exuberance and pruning at differentstages, in particular in the formation of long and shortbranches and of synaptic boutons.16,33 These devel-opmental processes are partially under the control ofepigenetic factors. Indeed, they can be altered bysensory deprivation, fetal alcohol, thyroid-hormonedeficiency, epilepsy, cytoarchitectonic abnormalities,early lesions and perinatal ischemia (for data andreferences, see Innocenti,16,34,64 Parnas et al,20 McCas-land et al,66 Zufferey et al67 and Kennedy et al 71). Thislist is not exhaustive and some of the same factorshave also been implicated in S. Some of the factorsaffecting the development of callosal connectionsappear to operate through ‘instructions’ reaching thecerebral cortex from the thalamus. Therefore, in linewith our previous proposal,20 if a reduced thalamo-prefrontal connectivity were to be the earliest occur-ring anatomical disturbance in S, the followingcascade of events could be envisaged. Fewer axonalbranches and synapses would be formed and/ormaintained by cortico-cortical neurons in the devel-oping prefrontal cortex. This would lead to abnormalspatio-temporal patterns of activity which, on the onehand, would lead to prepsychotic or psychoticsymptoms and, on the other, if occurring early in life,during the critical period for this kind of connections,could aggravate abnormalities in connectivity. Ad-mittedly, intrahemispheric and intra-areal connec-tions have been studied less in detail than the callosalconnections, and in both cases the available informa-tion is mainly about projections originating in layer 3of the primary visual areas. In these areas, not all thecortico-cortical axons appear to be equally sensitive tovisual deprivation.67 In particular, axons from thedeep layers are less sensitive than those originating inthe upper layers.64 This highlights another facet of themisconnectivity hypothesis. The alteration of connec-tions originating from supragranular layers mightgenerate a functional imbalance between layers,whose consequences remain to be investigated.Finally, it is tempting to assume that connections inthe association areas, in particular the prefrontal,temporal and cingulate areas, might follow similardevelopmental rules as in the primary visual areas;however only a handful of studies exist to indicatethat this might indeed be the case.32,40,72
Lessons from the past and future directions
The considerations above stress the need for advan-cing, at the cellular, molecular and system level, thecurrent knowledge of the processes responsible for theformation of cortical networks. In addition, the resultsof the numerous, often excellent studies of callosalconnections in S teach a number of important lessonsthat should be kept in mind in future studies of thiskind, and more generally in studies aimed at clarifyingthe neuroanatomical, neurophysiological, neuropsy-chological and developmental substrates of S.
First, the findings are, and will probably continue tobe relatively subtle and close attention should be paidto a number of methodological issues, several of whichhave been discussed earlier.73,74 One issue is that thechoice of patients can introduce undesirable varia-bility within and across studies. The variability has atleast three dimensionsFearly vs late schizophrenics,first episode vs chronic patients, positive vs negativesymptomsFnot to mention other variables that mightalso affect CC morphology and function such asgender, handedness or even experience. Also, Spatients tend to have general impairment in perfor-mance and this may be worsened by the medication.Finally, in light of what was said above, the choice ofan appropriate control group is not trivial.
Second, a number of methodological refinementsare desirable in the morphological, physiological andneuropsychological studies of the CC in S. Measure-ments of the total CC size have provided conflictingresults, not only in the field of S but also concerningthe long controversial association between CC, genderand functional lateralization.96 What is worse, thegross measurements of the CC are ambiguous withrespect to the underlying anatomical differences.These could be related to the number of axons, thediameter of axons and/or their myelin sheath, andalso to number or size of nonaxonal components inthe CC, including glial (and probably neuronal) cellbodies, or blood vessels. The main factors determin-ing callosal size in development appear to be theincrease in-axon diameter and myelination.28,70 Evena considerable loss of callosal axons could be maskedby an increase in the diameter of the remaining ones,which is what one would expect if the remainingaxons, as suggested above, sprout into vacatedterritories. The same cautions must be applied to theinterpretation of regional differences in CC size.These measurements have the advantage of poten-tially capturing abnormalities in axonal systemsconnecting specific cortical areas but have thedisadvantage of being difficult to apply rigorously,given the large individual variability in CC shape.This variability creates serious obstacles whenequivalent CC regions must be compared acrossindividuals. Unfortunately, the difficulty of partition-ing the CC objectively and reproducibly in ways thatcould allow across-studies comparisons is not alwaysrecognized. Consequently, regional callosal measure-ments are often difficult to compare and interpret.
Hopefully, a more generalized usage of tensordiffusion imaging or of magnetic transfer ratio willprovide information on callosal structure at a level of‘quasi-histological’ resolution circumventing some ofthe difficulties mentioned above.
Electrophysiological investigations of interhemi-spheric interactions should be extended to the gammaband. ICoh of signals in the gamma band of the EEGshould be analyzed in epoch-related and in ERPstudies, possibly during tasks designed to engageselectively different callosal channels, ie, the connec-tions between specific functional areas. The use of
Schizophrenia, neurodevelopment and corpus callosumGM Innocenti et al
270
Molecular Psychiatry

high-resolution EEG or EMG, combined with techni-ques of signal deblurring, could greatly improve thespatial resolution of signal sampling. Transcallosalresponses to magnetic stimulation could provideadditional data on the functionality of callosal axons.
Neuropsychological tests assaying specifically thevarious callosal channels are desirable. The design ofthese tests can be guided by the large body of studiesin patients with complete or incomplete CC transec-tion and/or by functional imaging studies of bilateralvs unilateral cortical activation.
The third consideration deriving from the literatureon CC and S is the need for an interdisciplinaryapproach correlating, in the same patients, structural,neuropsychological and electrophysiological results.As reported above, studies of this kind are beginningto appear. A possible strategy would be to firstidentify structural abnormalities in a specific callosalsector. Then, based on the known topographicalrelation between CC sectors and cortical origin ofthe axons, the neuropsychological and electrophysio-logical tests appropriate to probe the potentiallyabnormal callosal channels could be applied.
The fourth desirable condition in studies of CC and Sis the longitudinal follow-up approach, in children andadolescents at risk for S, and/or schizotypal relatives ofschizophrenic probands using the combined meth-odologies mentioned above. These approaches havethe merit of providing data uncontaminated bychronicity and long medication. Furthermore, theycan provide information as to which developmentalprocesses are the most probable cause of the initialsymptoms. Comparison of schizophrenic patients withtheir biological relatives is helpful to disentangle traitand state phenomena. These goals being attained,therapeutic interventions aimed at changing the courseof the disease might become possible.
In the end, it should not be forgotten that Ssymptoms wax and wane. Consequently, the structur-al-deficit-based hypothesis such as hyperconnectivity,hypoconnectivity and misconnectivity will be insuffi-cient to account for the pathophysiology of the disease.Changes in the regulation of neurotransmitter functionin the structures concerned may also be important.Equally important might be to elucidate the elusiveand complex relations between cortical structure andcortical functions, taking a nonlinear dynamic ap-proach157 to cortical activity as a starting point.
Acknowledgements
This work was supported by Swedish Medical Re-search Council grant no. 12954. We are grateful to CarlHolmgren for providing useful advice on this text.
Notes added in proofSince this paper was accepted for publication:
Keshavan et al. ( J Neurol Neurosurg Psychiatry 2002; 72: 757–760)reported smaller CC, anterior genu, anterior body, isthmus and anteriorsplenium in a group of 31 first episode, untreated schizophrenics.
Frumin et al. (Am J Psychiatry 2002; 159: 866–868) reported nosignificant difference in size but differences in shape of the CC in 14first episode schizophrenics.
Fitzgerald et al. (Schizophr Res 2002; 56: 199–209) reported a decreasein the duration of transcallosal inhibition, evoked by transcranialstimulation, independent of medication dose, in 25 schizophrenics.
Florio et al. (Cognitive Neuropsychiatry 2002; 7: 97–111) failed tomeasure transcallosal transfer using the reaction-time paradigm ofPoffenberger and suggested a slowing down of visuomotor responsessubserved by the left hemisphere.
A review on synchronous gamma activity and schizophrenia byK-H Lee et al. (Brain Res Rev, in press) complements some aspects ofthe present paper.
References
1 Parnas J, Bovet P. Autism in schizophrenia revisited. ComprPsychiatry 1991; 32: 7–21.
2 Andreasen NC. Linking mind and brain in the study of mentalillnesses: a project for a scientific psychopathology. Science 1997;275: 1586–1593.
3 Mountcastle V. An organizing principle for cerebral function: theunit module and the distributed system. In: Edelman GE,Mountcastle V (eds). The Mindful Brain. MIT Press: Cambridge,MA, 1978; pp 7–50.
4 Edelman G. Neural Darwinism. The Theory of Neuronal GroupSelection. Basic Books Inc: New York, 1987; p 331.
5 Engel AK, Roelfsema PR, Fries P, Brecht M, Singer W. Role of thetemporal domain for response selection and perceptual binding.Cereb Cortex 1997; 7: 571–582.
6 Selemon LD, Goldman-Rakic P. The reduced neuropil hypothesis:a circuit based model of schizophrenia. Biol Psychiatry 1999; 45:17–25.
7 Harrison PJ. The neuropathology of schizophrenia; a criticalreview of the data and their interpretation. Brain 1999; 122: 593–624.
8 Lewis DA. Is there a neuropathology of schizophrenia? Recentfindings converge on altered thalamic–prefrontal cortical con-nectivity. The Neuroscientist 2000; 6: 208–218.
9 Lewis DA, Lieberman JA. Catching up on schizophrenia: naturalhistory and neurobiology. Neuron 2000; 28: 325–334.
10 McGlashan TH, Hoffman RE. Schizophrenia as a disorder ofdevelopmentally reduced synaptic connectivity. Arch Gen Psy-chiatry 2000; 57: 637–648.
11 Selemon LD. Regionally diverse cortical pathology in schizo-phrenia: clues to the etiology of the disease. Schizophrenia Bull2001; 27: 349–377.
12 Feinberg I. Schizophrenia: caused by a fault in programmedsynaptic elimination during adolescence? J Psychiatry Res 1982;17: 319–334.
13 Beaumont JC, Dimond S. Brain disconnection and schizophrenia.Br J Psychiatry 1973; 123: 661–662.
14 Friston KJ, Frith CD. Schizophrenia: a disconnection syndrome?Clin Neurosci 1995; 3: 89–97.
15 Innocenti GM, Lehmann P, Houzel JC. Computational structure ofvisual callosal axons. Eur J Neurosci 1994; 6: 918–935.
16 Innocenti GM. Exuberant development of connections, and itspossible permissive role in cortical evolution. Trends Neurosci1995; 18: 371–426.
17 Markram H. A network of tufted layer 5 pyramidal neurons.Cereb Cortex 1997; 7: 523–533.
18 Zilberter Y, Kaiser KM, Sakmann B. Dendritic GABA releasedepresses excitatory transmission between layer 2/3 pyramidaland bitufted neurons in rat neocortex. Neuron 1999; 24: 979–988.
19 Zilberter Y. Dendritic release of glutamate suppresses synapticinhibition of pyramidal neurons in rat neocortex. J Physiol 2000;528: 489–496.
20 Parnas J, Bovet P, Innocenti GM. Schizophrenic trait features,binding, and cortico-cortical connectivity: a neurodevelopmentalpathogenetic hypothesis. Neurol Psychiatry Brain Res 1996; 4:185–196.
Schizophrenia, neurodevelopment and corpus callosumGM Innocenti et al
271
Molecular Psychiatry

21 Crow TJ. Schizophrenia as a transcallosal misconnection syn-drome. Schizophrenia Res 1998; 30: 111–114.
22 Weinberger DR. Implications of normal brain development for thepathogenesis of schizophrenia. Arch Gen Psychiatry 1987; 44:660–669.
23 Marenco S, Weinberger DR. The developmental hypothesis ofschizophrenia: following a trail of evidence from cradle to grave.Dev Psychopat 2000; 12: 501–527.
24 Innocenti GM, Fiore L, Caminiti R. Exuberant projection into thecorpus callosum from the visual cortex of newborn cats. NeurosciLett 1977; 4: 237–242.
25 Innocenti GM. Growth and reshaping of axons in the establish-
ment of visual callosal connections. Science 1981; 212: 824–827.26 Ivy GO, Killackey HP. The ontogeny of the distribution of callosal
projection neurons in the rat parietal cortex. J Comp Neurol 1981;195: 367–389.
27 Stanfield BB, O’Leary DDM, Fricks C. Selective collateralelimination in early postnatal development restricts corticaldistribution of rat pyramidal tract neurones. Nature 1982; 298:
371–373.28 Berbel P, Innocenti GM. The development of the corpus callosum
in cats: a light- and electron-microscopic study. J Comp Neurol1988; 276: 132–156.
29 Kennedy H, Bullier J, Dehay C. Transient projection from thesuperior temporal sulcus to area 17 in the newborn macaquemonkey. Proc Natl Acad Sci USA 1989; 86: 8093–8097.
30 LaMantia A-S, Rakic P. Axon overproduction and elimination inthe corpus callosum of the developing rhesus monkey. J Neurosci1990; 10: 2156–2175.
31 Callaway EM, Katz LC. Emergence and refinement of clusteredhorizontal connections in cat striate cortex. J Neurosci 1990; 10:1134–1153.
32 Webster MJ, Ungerleider LG, Bachevalier J. Connections of
inferior temporal areas TE and TEO with medial temporal-lobestructures in infant and adult monkeys. J Neurosci 1991; 11:1095–1116.
33 Bressoud R, Innocenti GM. Typology, early differentiation andexuberant growth of a set of cortical axons. J Comp Neurol 1999;406: 87–108.
34 Innocenti GM. The development of projections from cerebral
cortex. Prog Sens Physiol 1991; 12: 65–114.35 Cragg BG. The development of synapses in the visual system of
the cat. J Comp Neurol 1975; 160: 147–166.36 Huttenlocher PR. Synaptic density in human frontal cortexF
developmental changes and effects of aging. Brain Res 1979; 163:195–205.
37 Huttenlocher PR, De Courten C, Garey LJ, Van der Loos H.
Synaptogenesis in human visual cortexFevidence for synapseelimination during normal development. Neurosci Lett 1982; 33:247–252.
38 Bourgeois J-P, Rakic P. Changes of synaptic density in the primaryvisual cortex of the macaque monkey from fetal to adult stage.J Neurosci 1993; 13: 2801–2820.
39 Aggoun-Zouaoui D, Kiper D, Innocenti GM. Growth of callosalterminal arbors in primary visual areas of the cat. Eur J Neurosci1996; 8: 1132–1148.
40 Woo T-U, Pucak ML, Kye CH, Matus CV, Lewis DA. Peribuberalrefinement of the intrinsic and associational circuitry in themonkey prefrontal cortex. Neuroscience 1997; 80: 1149–1158.
41 Parnas J, Carter JW. High-risk studies and developmentalhypothesis. In: Hafner H, Resch F (eds). Risk and ProtectiveFactors in Schizophrenia: Towards a Conceptual Disease Model.Springer-Verlag: Berlin, 2001.
42 Galuske RAW, Schlote W, Singer W. Interhemispheric asymme-tries of the modular structure in human temporal cortex. Science2000; 289: 1946–1949.
43 Pakkenberg B. Total nerve cell number in neocortex in chronicschizophrenics and controls estimated using optical disectors.Biol Psychiatry 1993; 34: 768–772.
44 Selemon LD, Rajkowska G, Goldman-Rakic PS. Abnormally highneuronal density in the schizophrenic cortex: a morphometricanalysis of prefrontal areas 9 and occipital area 17. Arch GenPsychiatry 1995; 52: 805–818.
45 Garey LJ, Ong WY, Patel TS, Kanani M, Davis A, Mortimer AM etal. Reduced dendritic spine density on cerebral cortical pyrami-dal neurons in schizophrenia. J Neurol Neurosurg Ps 1998; 65:446–453.
46 Glantz LA, Lewis DA. Decreased dendritic spine density onprefrontal cortical pyramidal neurons in schizophrenia. ArchGen Psychiatry 2000; 57: 65–73.
47 Ong WY, Garey LJ. Ultrastructural features of biopsed tempor-opolar cortex (area 38) in a case of schizophrenia. SchizophreniaRes 1993; 10: 15–27.
48 Glantz LA, Lewis DA. Reduction of synaptophysin immunor-eactivity in the prefrontal cortex of subjects with schizophrenia:regional and diagnostic specificity. Arch Gen Psychiatry 1997; 54:943–952.
49 Karson CN, Mrak RE, Schluterman KO, Sturner WO Sheng JG,Griffin WST. Alterations in synaptic protein and their encodingmRNAs in prefrontal cortex in schizophrenia: a possibleneurochemical basis for ‘hypofrontality’. Mol Psychiatry 1999;4: 39–45.
50 Honer WG, Falkai P, Chen C, Arango V, Mann JJ, Dwork AJ.Synaptic and plasticity-associated proteins in anterior frontalcortex in severe mental illness. Neuroscience 1999; 91: 1247–1255.
51 Glantz LA, Austin MC, Lewis DA. Normal cellular levels ofsynaptophysin mRNA expression in the prefrontal cortex ofsubjects with schizophrenia. Biol Psychiatry 2000; 48: 389–397.
52 Miormics K, Middleton FA, Marquez A, Lewis DA, Levitt P.Molecular characterization of schizophrenia viewed by micro-array analysis of gene expression in prefrontal cortex. Neuron2000; 28: 53–67.
53 Shenton ME, Dickey CC, Frumin M, McCarley RW. A review ofMRI findings in schizophrenia. Schizophrenia Res 2001; 49: 1–52.
54 Weinberger DR, Berman KF, Suddath R, Torrey EF. Evidence ofdysfunction of a prefrontal–limbic network in schizophrenia: amagnetic resonance imaging and regional blood flow study ofdiscordant monozygotic twins. Am J Psychiatry 1992; 149: 890–897.
55 Andreasen NC, O’Leary DS, Flaum M, Nopoulos P, Watkins GL,Boles Ponto LL et al. Hypofrontality in schizophrenia: distributeddysfunctional circuits in neuroleptic naıve patients. Lancet 1997;349: 1730–1734.
56 Tsai G, Passani La, Slusher BS, Carter R, Baer L, Kleinman JE etal. Abnormal excitatory neurotransmitter metabolism in schizo-phrenic brains. Arch Gen Psychiatry 1995; 52: 829–836.
57 Melone M, Vitellaro-Zuccarello L, Vallejo-Illarramendi A, Perez-Samartin A, Matute C, Cozzi A, Pellegrini-Giampietro DE et al.The expression of glutamate transporter GLT-1 in the rat cerebralcortex is down-regulated by the antipsychotic drug clozapine.Mol Psychiatry 2001; 6: 380–386.
58 Do KQ, Trabesinger AH, Kirsten-Kruger M, Lauer CJ, Dydak U,Hell D et al. Schizophrenia: glutathione deficit in cerebrospinalfluid and prefrontal cortex in vivo. Eur J Neurosci 2000; 12:3721–3728.
59 Hyde TM, Ziegler JC, Weinberger DR. Psychiatric disturbance inmetachromatic leukodystrophy: insight into the neuronbiology ofpsychosis. Arch Neurol 1992; 49: 401–406.
60 Friston KJ. Theoretical neurobiology and schizophrenia. BrMedical Bull 1996; 52: 644–655.
61 Hoffman RE. Neural network simulations, cortical connectivity,and schizophrenic psychosis. MD Computing 1997; 14: 200–208.
62 Pakkenberg B. Pronounced reduction of nerve cell numberin mediodorsal thalamic nucleus and nucleus accumbens inschizophrenics. Arch Gen Psychiatry 1990; 47: 1023–1028.
63 Popken GJ, Bunney WE, Potkin SG, Jones EG. Subnucleus-specific loss of neurons in medial thalamus of schizophrenics.Proc Natl Acad Sci USA 2000; 97: 9276–9280.
64 Innocenti GM, Frost DO, Illes J. Maturation of visual callosalconnections in visually deprived kittens: a challenging criticalperiod. J Neurosci 1985; 5: 255–267.
65 Olavarria J. The effect of visual deprivation on the number ofcallosal cells in the cat is less pronounced in extrastriate cortexthan in the 17/18 border region. Neurosci Lett 1995; 195:147–150.
Schizophrenia, neurodevelopment and corpus callosumGM Innocenti et al
272
Molecular Psychiatry

66 McCasland JS, Bernardo KL, Probst KL, Woolsey TA. Corticallocal circuit axons do not mature after early deafferentation. ProcNatl Acad Sci USA 1992; 89: 1832–1836.
67 Zufferey PD, Jin F, Nakamura H, Tettoni L, Innocenti GM. Therole of pattern vision in the development of cortico-corticalconnections. Eur J Neurosci 1999; 11: 2669–2688.
68 Rajkowska G, Selemon LD, Goldman-Rakic PS. Neuronal andglial somal size in the prefrontal cortex. A postmortem morpho-metric study of schizophrenia and Huntington disease. Arch GenPsychiatry 1998; 55: 215–224.
69 Pierri JN, Volk CLE, Sunyaung Auh MS, Sampson A, Lewis DA.Decreased somal size of deep layer 3 pyramidal neurons in theprefrontal cortex of subjects with schizophrenia. Arch GenPsychiatry 2000; 158: 466–473.
70 Clarke S, Kraftsik R, Van der Loos H, Innocenti GM. Formsand measures of adult and developing human corpus callosum: isthere sexual dimorphism? J Comp Neurol 1989; 280: 213–230.
71 Kennedy H, Meissirel C, Dehay C. Callosal pathways and theircompliancy to general rules governing the organization ofcorticocortical connectivity. In: Dreher B, Robinson S (eds).Vision and Visual Dysfunction, Vol 3: Neuroanatomy of theVisual Pathways and their Development. Macmillan: London,1991, pp 324–359.
72 Lewis DA, Gonzales-Burgos G. Intrinsic excitatory connections inthe prefrontal cortex and the pathophysiology of schizophrenia.Brain Res Bull 2000; 52: 309–317.
73 David AS. Divided visual field studies in schizophrenia. In:Crawford J, Parker D (eds). Developments in Clinical andExperimental Neuropsychology. Plenum Press: New York, 1989,pp 113–126.
74 Coger RW, Serafetinides EA. Schizophrenia, corpus callosum,and interhemispheric communication: a review. Psychiatry Res1990; 34: 163–184.
75 Woodruff PWR, McManus IC, David AS. Meta-analysis of corpuscallosum size in schizophrenia. J Neurol Neurosur Ps 1995; 58:457–461.
76 Hoff AL, Neal C, Kushner M, DeLisi LE. Gender differences incorpus callosum size in first-episode schizophrenics. BiolPsychiatry 1994; 35: 913–919.
77 Colombo C, Bonfanti A, Scarone S. Anatomical characteristics ofthe corpus callosum and clinical corelates in schizophrenia. EurArch Psychiatry Clin N 1994; 243: 244–248.
78 Wright IC, McGuire PK, Poline J-B, Trevere JM, Murray RM, FrithCD et al. A voxel-based method for the statistical analysis of grayand white matter density applied to schizophrenia. Neuroimage1995; 2: 244–252.
79 Hendren RL, Hodde-Vargas J, Yeo RA, Vargas LA, Brooks WM,Ford C. Neuropsychophysiological study of children at risk forschizophrenia: a preliminary report. J Am Acad Child Psychiatry1995; 34: 1284–1291.
80 Woodruff PWR, Phillips ML, Rushe T, Wright IC, Murray RM,David AS. Corpus callosum size and inter-hemispheric functionin schizophrenia. Schizophr Res 1997; 23: 189–196.
81 Tibbo P, Nopoulos P, Arndt S, Andreasen NC. Corpus callosumshape and size in male patients with schizophrenia. BiolPsychiatry 1998; 44: 405–412.
82 DeQuardo JR, Keshavan MS, Bookstein FL, Bagwell WW, GreenWDK, Sweeney JA et al. Landmark-based morphometric analysisof first-episode schizophrenia. Biol Psychiatry 1999; 45:1321–1328.
83 Highley JR, Esiri MM, McDonald B, Cortina-Borja M, Herron BM,Crow TJ. The size and fibre composition of the corpus callosumwith respect to gender and schizophrenia: a post-mortem study.Brain 1999; 122: 99–110.
84 Meisenzahl EM, Frodl T, Greiner J, Leinsinger G, Maag K-P, HeissD et al. Corpus callosum size in schizophreniaFa magneticresonance imaging analysis. Eur Arch Psychiatry Clin N 1999;249: 305–312.
85 Scheller-Gilkey G, Lewine RRJ. Age at onset and sex differencesin corpus callosum area in schizophrenia. Schizophr Res 1999;40: 229–235.
86 Sachdev PS, Brodaty H. Mid-sagittal anatomy in late-onsetschizophrenia. Psychol Med 1999; 29: 963–970.
87 Chua SE, Sharma T, Takei N, Murray RM, Woodruff PWR. Amagnetic resonance imaging study of corpus callosum size infamilial schizophrenic subjects, their relatives, and normalcontrols. Schizophr Res 2000; 41: 397–403.
88 Downhill JE, Buchsbaum MS, Wei T, Spiegel-Cohen J, Hazlett EA,Haznedar MM et al. Shape and size of the corpus callosum inschizophrenia and schizotypal personality disorder. SchizophrRes 2000; 42: 193–208.
89 Foong J, Maier M, Clark CA, Barker GJ, Miller DH, Ron MA.
Neuropathological abnormalities of the corpus callosum inschizophrenia: a diffusion tensor imaging study. J NeurolNeurosur Ps 2000; 68: 242–244.
90 Narr KL, Thompson PM, Sharma T, Moussai J, Cannestra AF,Toga AW. Mapping morphology of the corpus callosum inschizophrenia. Cereb Cortex 2000; 10: 40–49.
91 Agartz I, Andersson JLR, Skasre S. Abnormal brain white matterin schizophrenia: a diffusor tensor imaging study. Neuroreport2001; 12: 2251–2254.
92 Foong J, Symms MR, Barker GJ, Maier M, Woermann FG, MillerDH, Ron MA. Neuropathological abnormalities in schizoprenia:evidence from magnetization transfer imaging. Brain 2001; 124:882–892.
93 Rossell SL, Shapleske J, Fukuda R, Woodruff PWR, Simmons A,David AS. Corpus callosum area and functioning in schizophre-nic patients with auditory–verbal hallucinations. Schizophr Res2001; 50: 9–17.
94 Hoppner J, Kunesch E, Grossmann A, Tolzin C-J, Schultz M,Schlafke D et al. Dysfunction of transcallosally mediated motorinhibition and callosal morphology in patients with schizophre-nia. Acta Psychiat Scand 2001; 104: 227–235.
95 Frodl T, Meisenzhal EM, Muller D, Greiner J, Juckel G, LeisingerG et al. Corpus callosum and P300 in schizophrenia. SchizophrRes 2001; 49: 107–120.
96 Bishop KM, Wahlsten D. Sex differences in the human corpuscallosum: myth or reality? Neurosci Biobehav Rev 1997; 21:581–601.
97 Schenton ME, Dickey CC, Frumin M, McCarley RW. A review ofMRI findings in schizophrenia. Schizophr Res 2001; 49: 1–52.
98 De Lacoste MC, Kirkpatrick JB, Ross ED. Topography of thehuman corpus callosum. J Neuropat Exp Neur 1985; 44: 578–591.
99 Koppel H, Innocenti GM. Is there genuine exuberancy of callosalprojections in development? A quantitative electro-microscopicstudy. Neurosci Lett 1983; 41: 33–40.
100 Boroojerdi D, Topper R, Foltys H, Meincke U. Transcallosalinhibition and motor conduction studies in patients withschizophrenia using transcranial magnetic stimulation. Br JPsychiatry 1999; 175: 375–379.
101 Schwartz BD, Winstead DK, Walker WG. A corpus callosumdeficit in sequential analysis by schizophrenics. Biol Psychiatry1984; 19: 1667–1676.
102 Gulmann NC, Widshiodtz G, Orbaek K. Alterations of interhemi-spheric conduction through the corpus callosum in chronicschizophrenia. Biol Psychiatry 1982; 17: 585–594.
103 Luria AR. The Working Brain. Basic Books, Inc.: New York, 1973;p 398.
104 Innocenti GM, Manzoni T, Spidalieri G. Relevance of the callosaltransfer in defining the peripheral reactivity of somesthesiccortical neurons. Arch Ital Biol 1973; 3: 187–221.
105 Picard N, Lepore F, Ptito M, Guillemot JP. Bilateral interaction inthe second somatosensory area (SII) of the cat and contribution ofthe corpus callosum. Brain Res 1990; 17(536): 97–104.
106 Fabri M, Polonara G, Quattrini A, Salvolini U, Del Pesce M,Manzoni T. Role of the corpus callosum in the somatosensoryactivation of the ipsilateral cerebral cortex: an fMRI study ofcallosotomized patients. Eur J Neurosci 1999; 11: 3983–3994.
107 Salamy A. Commissural transmission: maturational changes inhumans. Science 1978; 200: 1409–1411.
108 Engel AK, Konig P, Kreiter AK, Singer W. Interhemisphericsynchronization of oscillatory neuronal responses in cat visualcortex. Science 1991; 252: 1177–1179.
109 Nowak LG, Munk MHJ, Nelson JI, James AC, Bullier J. Structuralbasis of cortical synchronization. I. Three types of interhemi-spheric coupling. J Neurophysiol 1995; 74: 2379–2400.
Schizophrenia, neurodevelopment and corpus callosumGM Innocenti et al
273
Molecular Psychiatry
110 Munk MHJ, Nowak LG, Nelson JI, Bullier J. Structural basis ofcortical synchronization. II. Effects of cortical lesions. J Neuro-physiol 1995; 74: 2401–2414.
111 Kiper DC, Knyazeva MG, Tettoni L, Innocenti GM. Visualstimulus dependent changes in inter-hemispheric EEG coher-ence. J Neurophysiol 1999; 82: 3082–3094.
112 Knyazeva MG, Kiper DC, Vildavski VY, Desplands PA, Maeder-Ingvar M, Innocenti GM. Visual-stimulus-dependent changes ininterhemispheric EEG coherence in humans. J Neurophysiol1999; 82: 3095–3107.
113 Merrin EL, Floyd TC, Fein G. EEG coherence in unmedicatedschizophrenic patients. Biol Psychiatry 1989; 25: 60–66.
114 Michelogiannis S, Paritsis N, Trikas P. EEG coherence duringhemispheric activation in schizophrenics. Eur Arch Psy Clin N1991; 241: 31–34.
115 Nagase Y, Okubo Y, Matsuura M, Kojima T, Toru M. EEGcoherence in unmedicated schizophrenic patients: topographicalstudy of predominantly never medicated cases. Biol Psychiatry1992; 32: 1028–1034.
116 Morrison-Stewart SL, Velikonja D, Corning WC, Williamson P.Aberrant interhemispheric alpha coherence on electroencepha-lography in schizophrenic patients during activation tasks.Psychol Med 1996; 26: 605–612.
117 Merrin EL, Floyd T. Negative symptoms and EEG alpha inschizophrenia: a replication. Schizophr Res 1996; 19: 151–161.
118 Mann K, Maier W, Franke P, Roschke J, Gansicke M. Intra- andinterhemispheric electroencephalogram coherence in siblingsdiscordant for schizophrenia and healthy volunteers. BiolPsychiatry 1997; 42: 655–663.
119 Norman RMG, Malla AK, Williamson PC, Morrison-Stewart SL,Helmes E, Cortese L. EEG coherence and syndromes in schizo-phrenia. Br J Psychiatry 1997; 170: 411–415.
120 Pinkofsky HB, Struve FA, Meyer MA, Patrick G, Reeves RR.Decreased multi-band posterior interhemispheric coherence witha lipoma on the corpus callosum: a case report of a possibleassociation. Clin Electroencephal 1997; 28: 155–159.
121 Tauscher J, Fischer P, Neumeister A, Rappelsberger P, Kasper S.Low frontal electroencephalographic coherence in neuroleptic-free schizophrenic patients. Biol Psychiat 1998; 44: 438–447.
122 Wada Y, Nanbu Y, Jiang Z, Koshino Y, Hashimoto T. Interhemi-spheric EEG coherence in never-medicated patients with para-noid schizophrenia: analysis at rest and during photicstimulation. Clin Electroencephal 1998; 29: 170–176.
123 Wada Y, Nanbu Y, Kikuchi M, Koshino Y, Hashimoto T. Aberrantfunctional organization in schizophrenia: analysis of EEGcoherence during rest and photic stimulation in drug-naivepatients. Neuropsychobiol 1998; 38: 63–69.
124 Winterer G, Egan MF, Radler T, Hyde T, Coppola R, WeinbergerDR. An association between reduced interhemispheric EEGcoherence in the temporal lobe and genetic risk for schizophre-nia. Schizophr Res 2001; 49: 129–143.
125 Beaumont JG, Dimond S. Brain disconnection and schizophrenia.Br J Psychiatry 1973; 123: 661–662.
126 Mohr B, Pulvermuller F, Cohen R, Rockstroh B. Interhemisphericcooperation during word processing: evidence for callosaltransfer dysfunction in schizophrenic patients. Schizophr Res2000; 46: 231–239.
127 Spivak B, Elimelech D, Ocring R, Mester R, Kotler M, WeizmanA. Hemispheric function in disorganized type schizophrenia:performance on the quality extinction test. Eur Psychiatry 2000;15: 402–406.
128 Bellgrove MA, Bradshaw JL, Velakoulis D, Johnson KA, RogersMA, Smith D et al. Bimanual coordination in chronic schizo-phrenia. Brain Cognition 2001; 45: 325–341.
129 David AS. Stroop effects within and between the cerebralhemispheres: studies in normals and acallosals. Neuropsycholo-gia 1992; 30: 161–175.
130 David AS. Callosal transfer in schizophrenia: too much or toolittle? J Abnorm Psychol 1993; 102: 573–579.
131 David AS. Severe psychiatric disturbance and abnormalities ofthe corpus callosum: review and case series. J Neurol NeurosurgPs 1993; 56: 85–93.
132 Audenaert K, Lahorte P, Brans B, van Laere K, Goethals I, vanHeeringen K et al. The classical stroop interference task as a
prefrontal activation probe:a validation study using 99Tcm-ECDbrain SPECT. Nucl Med Commun 2001; 22: 135–143.
133 Phillips ML, Woodruff PWR, David AS. Stroop interference andfacilitation in the cerebral hemispheres in schizophrenia.Schizophr Res 1996; 20: 57–68.
134 David AS. Schizophrenia and the corpus callosum: develop-mental. Structural and functional relationships. Behav Brain Res1994; 64: 203–211.
135 Gunther W, Petschs R, Steinberg R, Moser E, Streck P, Heller H etal. Brain disfunction during motor activation and corpuscallosum alteration in schizophrenia measured by cerebral bloodflow and magnetic resonance imaging. Biol Psychiatry 1991; 29:535–555.
136 Merrin EL, Floyd TC. Negative symptoms and EEG alpha activityin schizophrenic patients. Schizophr Res 1992; 8: 11–20.
137 Eckhorn R, Bauer R, Jordan W, Brosch M, Kruse W, Munk M et al.Coherent oscillations: a mechanism of feature linking in thevisual cortex? Multiple electrode and correlation analyses in thecat. Biol Cybern 1988; 60: 121–130.
138 Gray CM, Konig P, Engel AK, Singer W. Oscillatory responses incat visual cortex exhibit inter-columnar synchronization whichreflects global stimulus properties. Nature 1989; 338: 334–337.
139 Joliot M, Ribary U, Llinas R. Human oscillatory brain activitynear 40 Hz coexists with cognitive temporal binding. Proc NatlAcad Sci USA 1994; 91: 11 748–11 751.
140 Singer W, Gray CM. Visual feature integration and the temporalcorrelation hypothesis. Annu Rev Neurosci 1995; 18: 555–586.
141 Stransky E. Zur Auffassung gewisser Symptome der Dementiapraecox. Neurolog Centralbl 1904; 23: 1074–1143.
142 Bleuler E. Dementia Preacox oder Gruppe der Schizophrenien.Frantz Deuticke: Leipzig und Wien, 1911, p 420.
143 Meehl PE. Schizotaxia, schizotypy, schizophrenia. Am Psychol1962; 17: 827–838.
144 Kwoon JS, O’Donnell BF, Wallenstein GV, Greene RW, HirayasuY, Nestor PG et al. Gamma frequency-range abnormalities toauditory stimulation in schizophrenia. Arch Gen Psychiatry1999; 56: 1001–1005.
145 Green MF, Neuchterlein KH. Cortical oscillations and schizo-phrenia. Timing is of the essence. Arch Gen Psychiatry 1999; 56:1007–1008.
146 Haig AR, Gordon E, De Pascalis V, Meares RA, Bahramali H,Harris A. Gamma activity in schizophrenia: evidence of impairednetwork binding? Clin Neurophysiol 2000; 111: 1461–1468.
147 Lee K-H, Williams LM, Haig A, Goldberg E, Gordon E. Anintegration of 40 Hz Gamma and phasic arousal: novelty androutinization processing in schizophrenia. Clin Neurophysiol2001; 112: 1499–1507.
148 Parnas J, Vianin P, Saebye D, Jansson L, Volmer Larsen A, Bovet P.Visual binding abilities in the initial and advanced stages ofschizophrenia. Acta Psychiat Scand 2001; 103: 1–10.
149 Wright, IC, Rabe-Hesketh S, Woodruff P, David AS, Murray RM,Bullmore ET. Meta-analysis of regional brain volumes inschizophrenia. Am J Psychiatry 2000; 157: 16–25.
150 Gazzaniga S, Ivry RB, Mangoun GR. Cognitive Neuroscience.Norton and Company: New York, 1998.
151 Petty RG. Structural asymmetries of the human brain and theirdisturbance in schizophrenia. Schizophr Bull 2000; 25: 121–139.
152 Crow TJ, Commentary on Annett, Yeo et al., Klar, Saugstadt andOrr: cerebral asymmetry language and psychosisFthe case for aHomo sapiens-specific sex-linked gene for brain growth. Schi-zophr Res 1999; 39: 219–231.
153 Crow TJ. Schizophrenia as the price that homo sapiens pays forlanguage: a resolution of the central paradox in the origin of thespecies. Brain Res Rev 2000; 31: 118–129.
154 Annett M. The theory of an agnostic right shift gene inschizophrenia and autism. Schizophr Res 1999; 39: 177–182.
155 Yeo RA, Gangestadt SW, Edgar C, Thoma R. The evolutionarygenetic underpinning of schizophrenia: the developmentalinstability model. Schizophr Res 1999; 39: 197–206.
156 Lee Y-J, Zhu Y-S, Shen M-F, Tong S-B, Thakor NV. The nonlineardynamical analysis of the EEG in schizophrenia with temporaland spatial embedding dimension. J Med Eng Technol 2001; 25:79–83.
Schizophrenia, neurodevelopment and corpus callosumGM Innocenti et al
274
Molecular Psychiatry
Related Documents











