Schizophrenia Schizophrenia and and Related Psychotic Related Psychotic Disorders Disorders Diana O. Perkins, MD, MPH Associate Professor of Psychiatry Director, Schizophrenia Treatment and Evaluation Program

Schizophrenia and Related Psychotic Disorders Diana O. Perkins, MD, MPH Associate Professor of Psychiatry Director, Schizophrenia Treatment and Evaluation.
Dec 19, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Schizophrenia Schizophrenia and and
Related Psychotic DisordersRelated Psychotic Disorders
Diana O. Perkins, MD, MPH
Associate Professor of Psychiatry
Director, Schizophrenia Treatment and Evaluation Program

Schizophrenia and Related Psychotic Schizophrenia and Related Psychotic DisordersDisorders
Clinical characteristics Epidemiology Etiology

Psychotic DisordersPsychotic Disorders
Clinical Characteristics

Schizophrenia is Schizophrenia is Heterogeneous...Heterogeneous...
A syndrome defined by a constellation of clinical symptoms
With multiple causes, that are similarly expressed

Show video tapeShow video tape

Schizophrenia: Clinical FeaturesSchizophrenia: Clinical Features
Positive Symptoms
a distortion or excess of normal function Negative Symptoms
a decrease or loss in normal function Disorganization
of thoughts and behavior Cognitive Impairments Mood Symptoms

Features of SchizophreniaFeatures of SchizophreniaPositive symptoms
Cognitive deficits
Functional ImpairmentsWork
Interpersonal relationshipsSelf-care
Negative symptoms
Mood symptoms
Disorganization

Positive Symptoms (Psychosis)Positive Symptoms (Psychosis)
Disturbance of Perception (Hallucinations)
Disturbance of Thought Content (Delusions)

Positive SymptomsPositive Symptoms
Disturbance of Perceptionmay effect any sensory modality

Positive Symptoms: HallucinationsPositive Symptoms: Hallucinations
Auditory Hallucinations• involve voices or sounds
• single or multiple
• familiar or unfamiliar
• may make insulting remarks or be pleasant
• may comment on behavior
• may command person to perform acts
Positive Symptoms: HallucinationsPositive Symptoms: Hallucinations
Other Sensory Modalities• Tactile: may involve electrical, tingling, or
burning sensations
• Visual
• Gustatory
• Olfactory

Positive Symptoms: DelusionsPositive Symptoms: Delusions
Delusions• fixed false beliefs
• examples:- persecutory delusions- delusions of reference- delusions of being controlled- thought broadcasting/insertion/withdrawal- grandiose- religious- nihilistic - somatic

Features of SchizophreniaFeatures of Schizophrenia
Positive symptoms- Hallucinations- Delusions
Cognitive deficits
Functional ImpairmentsWork
Interpersonal relationshipsSelf-care
Negative symptoms
Mood symptoms
Disorganization

Negative SymptomsNegative Symptoms
Negative symptoms include:decreased expression of feelingsdiminished emotional rangepoverty of speechdecreased interestsdiminished sense of purposediminished social drive

Differential Diagnosis of Negative SymptomsDifferential Diagnosis of Negative Symptoms
Negative Symptoms primary to schizophrenia:The “Deficit Syndrome”: primary and enduring negative
symptoms in individuals with schizophrenia
• The Deficit Syndrome occurs in about 20% of treated patients

Differential Diagnosis of Negative SymptomsDifferential Diagnosis of Negative Symptoms
Negative Symptoms may be secondary to:antipsychotic EPS side effects
- decreased emotional expression and apathy may be due to Parkinsonian side effects
- lack of initiation of activity may be due to bradykinesia
psychosisdepression or anxietydemoralization

Features of SchizophreniaFeatures of Schizophrenia
Positive symptoms- Delusions- Hallucinations- Disorganization
Cognitive deficits
Functional ImpairmentsWork
Interpersonal relationshipsSelf-care
Negative symptoms- emotional range- expression of emotion- motivation/drive- interests- social drive - poverty of speech
Mood symptoms
Disorganization

Positive Symptoms: DisorganizationPositive Symptoms: Disorganization
• Disorganization of Speech– tangential or circumstantial speech– looseness of associations
• Disorganization of Behavior– odd mannerisms– catatonic stupor

Video TapeVideo Tape
Positive symptoms:• Hallucinations• Delusions
Disorganization• Speech• Behavior
Negative symptoms:

Features of SchizophreniaFeatures of Schizophrenia
Positive symptoms- Delusions- Hallucinations- Disorganization
Cognitive deficits
Functional ImpairmentsWork
Interpersonal relationshipsSelf-care
Negative symptoms- emotional range- expression of emotion- motivation/drive- interests- social drive - poverty of speech
Mood symptomsDisorganization- speech- behavior

Cognitive Domains: Cognitive Domains:
Severe Impairment in SchizophreniaSevere Impairment in Schizophrenia
Severe Impairments– Serial learning– Executive functioning– Vigilance– Motor speed– Verbal Fluency
Moderate Impairment– Delayed recall– Distractibility– Immediate memory span– Visuomotor skills– Working memory

Working MemoryWorking Memory– Aspects of Working Memory
• Temporary storage and manipulation of information
• “workspace” for holding items of information in mind as recalled, manipulated, and associated with other ideas and information
– Tests• patients with schizophrenia tend to perform 1-2
standard deviations below the mean
• Tests: visual, spatial, auditory working memory


12



Executive FunctionExecutive Function
– Aspects of Executive Function• Focus attention• Distinguish the important aspect of a task or a
situation from unimportant• Prioritize• Perform mental or physical activities proper sequence• Modulate behavior based on social cues
– Tests: • Patients perform 2-3 standard deviations below mean
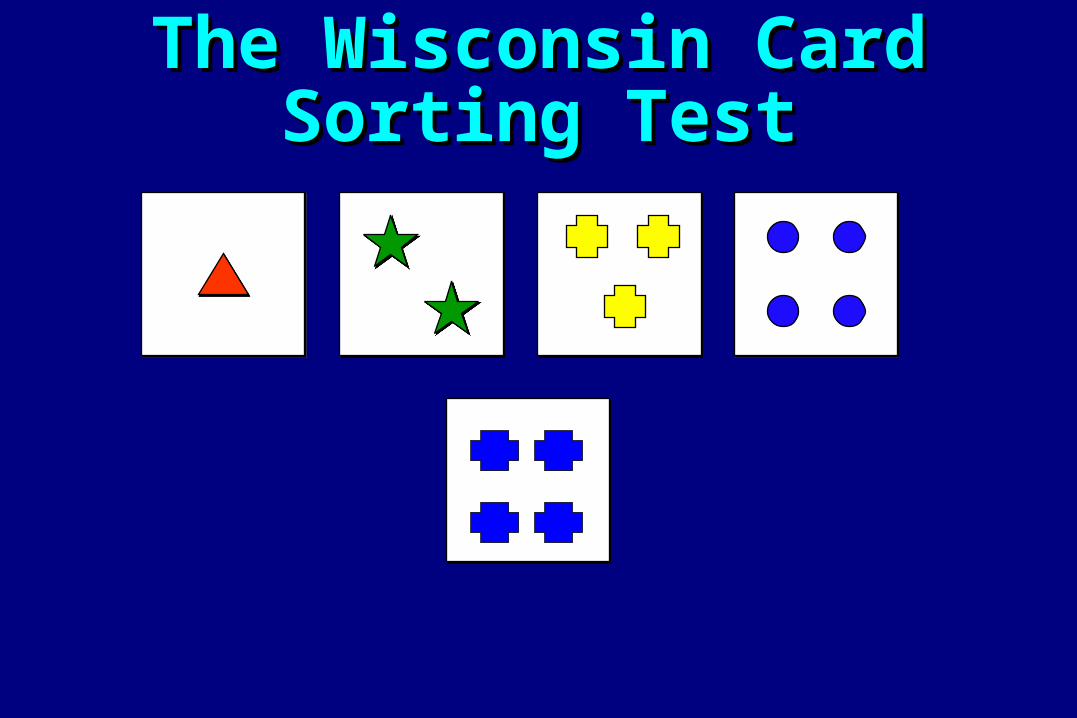
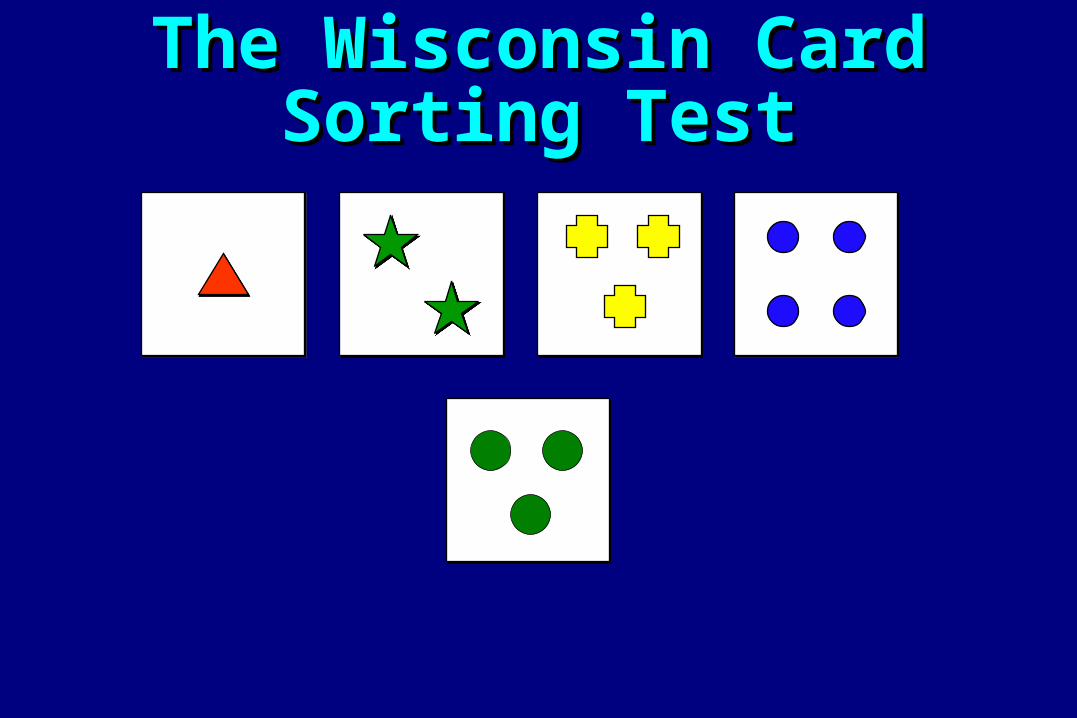
• Examples: Trail Making Tests, Wisconsin Card Sort, Tower of London

The Wisconsin Card Sorting TestThe Wisconsin Card Sorting Test

The Wisconsin Card Sorting TestThe Wisconsin Card Sorting Test

The Wisconsin Card Sorting TestThe Wisconsin Card Sorting Test

The Wisconsin Card Sorting TestThe Wisconsin Card Sorting Test

The Wisconsin Card Sorting TestThe Wisconsin Card Sorting Test
The Wisconsin Card Sorting TestThe Wisconsin Card Sorting Test

The Wisconsin Card Sorting TestThe Wisconsin Card Sorting Test

The Wisconsin Card Sorting TestThe Wisconsin Card Sorting Test

The Wisconsin Card Sorting TestThe Wisconsin Card Sorting Test
The Wisconsin Card Sorting TestThe Wisconsin Card Sorting Test

The Wisconsin Card Sorting TestThe Wisconsin Card Sorting Test

VigilanceVigilance– Ability to monitor target stimuli over an
extended duration of time• inability to attend to relevant stimuli and ignore
irrelevant stimuli• inability to concentrate• increased susceptibility to distractions• inability to sustain effort and attention
– Tests of Vigilance: • patients perform 2-3 standard deviations below the
mean• example: CPT

Cognitive Functions: Cognitive Functions:
Mild or No Impairment in SchizophreniaMild or No Impairment in Schizophrenia
Mild Impairment• Perceptual Skills• Delayed recognition
memory• Confrontation naming
No Impairment• Word recognition• Long-term factual memory

Features of SchizophreniaFeatures of Schizophrenia
Positive symptoms- Delusions- Hallucinations- Disorganization
Cognitive deficits- Attention- Memory- Verbal fluency- Motor function- Executive function
Functional ImpairmentsWork
Interpersonal relationshipsSelf-care
Negative symptoms- Decreased experience and expression of emotions- Decreased motivation/drive- Decreased initiative- Social withdrawal
Mood symptomsDisorganization- speech- behavior

Mood SymptomsMood Symptoms
– Dsyphoric•anger, hostility, fear, irritability, depression, anxiety
•high risk of suicide
– Euphoric• sense of power, control, exhilaration

Mood SymptomsMood Symptoms
– Primary to schizophrenia– “Reactive”
•psychosis is frightening
• reality of illness is demoralizing
– Co-morbid disorder•major depressive episode

Features of SchizophreniaFeatures of SchizophreniaPositive symptomsDelusionsHallucinationsDisorganized speech
Cognitive deficitsAttentionMemoryVerbal fluencyExecutive function (eg, abstraction)
Functional ImpairmentsWork
Interpersonal relationshipsSelf-care
Negative symptomsAnhedoniaAffective flatteningAvolitionSocial withdrawalAlogia
Mood symptomsDepression/AnxietyAggression/HostilitySuicidality
Disorganization- speech
- behavior

Diagnosis of SchizophreniaDiagnosis of Schizophrenia
Symptoms
Severity/Impairment/Distress
Duration

Differential Diagnosis of SchizophreniaDifferential Diagnosis of Schizophrenia
Significant psychotic symptoms for at least one week
Continuous signs of the disturbance for at least six months
Markedly impaired ability to function
Without known etiology

Differential Diagnosis of Differential Diagnosis of SchizophreniaSchizophrenia
Differential Diagnosis: related disordersSchizophreniform DisorderBrief Psychotic DisorderDelusional DisorderSchizoaffective DisorderSchizoid PersonalitySchizotypal Personality DisorderParanoid Personality Disorder

Differential Diagnosis of Differential Diagnosis of SchizophreniaSchizophrenia
Differential Diagnosis: Mood Disorders with Psychotic Features
Major Depression
Bipolar Disorder

Organic Mental Disorders
substance induced (e.g. PCP, amphetamine, cocaine, hallucinogens, cannabis, alcohol, a variety of prescribed medications
most diseases affecting the central nervous system
Differential Diagnosis of Differential Diagnosis of SchizophreniaSchizophrenia

casecase
Vignette 1: Michael
OVERVIEWDemographics:Michael is a 23 year old single male. He lives with his father. He completed some college and currently works at the shipping dock of a department store. Occupational History:Michael has worked for nearly a year at the shipping dock. He has had several other jobs that he quit when he felt “frustrated”. He has also been unemployed for several long periods. He calls in sick to work several times a month and is currently on probation at work. Status of Current Treatment:He is currently an outpatient in the psychiatric clinic. He was hospitalized for 4 days approximately two months ago. Chief Complaint and Description of Problem:Michael reports that he has trouble fitting in and believes that all his co-workers are “weird”. He reports feeling “a little confused” at work, but admits he usually goes to work “high” on
marijuana or crack.

Vignette 1: Michael
History:Michael had been in his usual state of good health until approximately three years ago. At the time he was smoking crack cocaine and marijuana several times a week and reports several episodes where he thought that the police were following him and bugging his phone. All of the episode occurred after a heavy episode of drug use, and resolved after one or two days. He eventually went to the psychiatric clinic for help with the episodes of paranoia, but denied any substance use to the clinic staff. He was prescribed haloperidol, which he took for two days, and then stopped because the medication made him feel “weird”. Prior to three years ago, the patient had no history of mental illness. However, over the past 3 years he has frequently used crack and marijuana and during periods of heavy use he has consistently felt “more paranoid” and “cut-off from everyone”. There are no other major life changes and there have been no deaths of close friends or relatives. However, his relationship with this father is quite strained. His mother died over 10 years ago. About 2 months ago Michael was admitted to the hospital after becoming very aggressive towards his father. He accused his father of sabotaging his car, trying to kill him, and said he would “get dad before dad got me”. In the emergency room Michael was agitated, and was fearful that sirens were the police coming to arrest him. He also reported hearing “voices” telling him “bad stuff” while in the emergency room. Urine toxicology screen was positive for marijuana, PCP, and cocaine. His agitation and paranoid ideation, as well as the “voices” resolved by the third hospital day, without any medication treatment.

Vignette 1: Michael
Treatment History:Michael has had one prior substance abuse inpatient stay lasting 6 days, where, off substances and without medication, his psychotic symptoms resolved. Other Current Problems:He reports that he always feels “weird and anxious”. He smokes marijuana or crack 1-3 times a day and drinks “several beers” daily.
Current Social Function:Michael has no close friends although he will socialize with co-workers occasionally while at work. He is estranged from his father who feels that he does not try hard enough to get better. Outside of work, he watches TV and listens to music.

Vignette 1: Michael
For the past several months, Michael has said he feels anxious and depressed most of the time, because he feels he has no life and no future. He says he never feels interested in anything, and he wishes that he were “more motivated”. His appetite is fine and he has had no change in weight. He reports that his sleep is “pretty good” and he is sleeping 6-8 hours a night. He denies motor changes (either periods of agitation or motor slowing), and his movements and rate of speech are normal during the SCID interview. He states his energy is “fine”. He feels hopeless about the future, specifically that he will never get a “good job” or have a “decent place to live” but denies feeling worthless or guilt. He blames his father for his current living and work situation. He states that his concentration is “fine”, and there is no evidence of impaired concentration during the interview. He denies recurrent thoughts of death or suicidal ideation. He denies any other periods of depression or loss of interest/motivation in the past five years. Michael denies any periods of time when he has felt euphoric or irritable. He denies thoughts that others take special notice of him. He acknowledges “feeling paranoid” at times when he smokes crack and marijuana. At these times he believes that the police are bugging his phone, and following him and trying to “get him”. He denies any other unusual beliefs. After smoking crack and marijuana he admits that he also occasionally hears muffled voices coming up from the floor, but the voices are indistinct. He admits to hearing the sirens in the emergency room, but he says “I think I was really hearing that”. He denies any other perceptual abnormalities. He states that the paranoid ideas or the “voices” have always resolved when he has stopped the drugs for a week or more, as is true during this hospitalization. On examination, he is reasonably well dressed and well groomed. His motor behavior is normal and well organized. He exhibits a full range and normal display of affect. His speech is normal in rate and rhythm, and his thought form is generally well-organized. He exhibits poor eye contact .watches TV and listens to music.

Schizophrenia: EpidemiologySchizophrenia: Epidemiology
Common disease:One in every 100 people develops schizophrenia
Each year, 100,000 people are newly diagnosed with schizophrenia in the U.S.
On any given day, 600,000 people are in active treatment for schizophrenia in the U.S.


Etiology Risk Factors for SchizophreniaEtiology Risk Factors for Schizophrenia Genetic Vulnerability Factors Environmental Risk Factors
• Obstetrical Trauma• In-utero events
• Infectious Pathogens• Nutritional Factors
• Substance Abuse • Stressful life events
• College• Boot Camp

What does What does youryour baby’s future hold? baby’s future hold?
Courtesy of Canadian Schizophrenia Society
Schizophreniais a geneticneurodevelopmentaldisorder
Schizophrenia
occurs in
all races
all cultures
all social classes
and both sexes
Schizophrenia
can be treated
but not cured
…yet!
ScSchhizizopophrhreeniania


Genetic Loci Linked to Schizophrenia

Schizophrenia: CourseSchizophrenia: Course
Age of onsetmay begin at any agetypically begins in late adolescents and early adulthood
late onset formmales often have earlier age on onset than females

Coursevaries from recovery to severe disability
in treatment settings commonly see more severe, chronic course
SchizophreniaSchizophrenia

Gestation/Birth 10 20 30 40 50
Premorbid Prodromal Onset/Deterioration
Residual/Stable
Stages Of Illness
HealthyWorseningSeverity OfSigns AndSymptoms
Natural History Of SchizophreniaNatural History Of Schizophrenia
Years

Natural History of SchizophreniaNatural History of Schizophrenia
Gestation/Birth 10 20 30 40 50
premorbid prodromal onset/deterioration
residual/stable
Stages of Illness
Healthy Worsening Severity of Signs and Symptoms

SchizophreniaSchizophrenia
Course: VariableComplete recovery (~ 5-10%)Complete, or almost complete remission of symptoms, but with periodic exacerbations of illness symptoms
Chronic symptoms, serious impact in function

Schizophrenia Schizophrenia Factors affecting prognosis:
age of onsetsexpremorbid functionabrupt versus insidious onsetfamily history of mood disorderprecipitating eventsduration of untreated illnesssubstance abuse

Prospective Study of First Episode Prospective Study of First Episode SchizophreniaSchizophrenia
Weeks of TreatmentWeeks of Treatment
8080
2020
0011 44 1919 2828 3434 4343 5252
Per
cen
t o
f P
atie
nts
Rem
itti
ng
Per
cen
t o
f P
atie
nts
Rem
itti
ng
Remission Rate 87%Remission Rate 87%Median Time to Remission 11 wksMedian Time to Remission 11 wks
Robinson et al. 1999Robinson et al. 1999
4040
6060
100100Time to RemissionTime to Remission
77 1010 1313 1616 2222 2525 3131 3737 4040 4646 4949

First-Episode: Predictors ofFirst-Episode: Predictors ofTreatment ResponseTreatment Response
Duration of untreated illness :Mean Median
Active psychosis:52 wks 11 wksProdrome: 151 wks
The longer the duration of pre-treatment symptoms, the poorer the clinical outcome (r=.4, p=.0001)
The longer the duration of pretreatment symptoms, the longer the time to respond to antipsychotic medication treatment (p=.03)
Loebel et al. Am J Psychiatry 1992;149:1183-1188

Cumulative relapse rates by episode of Cumulative relapse rates by episode of
illnessillness
0
10
20
30
40
50
60
70
80
90
Year 1 Year 2 Year 3 Year 4 Year 5
1st Relapse(104 patients at risk)
2nd Relapse (63 patients at risk)
3rd Relapse (20 patients at risk)
* Refers to year(s) after recovery from the previous episodeRobinson et al 1999

Mean Time to ResponseMean Time to ResponseSuccessive EpisodesSuccessive Episodes
0 20 40 60 80 100 120Days to Therapeutic Response
1
2
Episode (N=40)
1
2
Episode (N=12)
3
Lieberman JA. J Clin Psychiatry. 1996;57(suppl):68-71


Alternative Pathways to the Alternative Pathways to the Development of Residual Positive Development of Residual Positive
Symptoms in Schizophrenia:Symptoms in Schizophrenia:
A Treatment Resistant Clinical Sub-type: Patients who have persistent positive symptoms despite treatment with antipsychotics early in the course of illness.
Neuroprogressive Pathology: Symptoms that are initially treatment responsive and become unresponsive after subsequent episodes of illness.

Related Documents











