SPECTRUM DISORDERS and other PSYCHOTIC DISORDERS

Schizophrenia
Dec 13, 2015
psychotic disorders
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
SPECTRUM DISORDERS and other PSYCHOTIC DISORDERS

Contents Introduction History Recent statistics Etiological Factors Clinical Features

IntroductionSchizophrenia is a
clinical syndrome of variable, but profoundly disruptive, psychopathology that involves cognition, emotion, perception, and other aspects of behavior.

The expression of these manifestations varies across patients and over time, but the effect of the illness is always severe and is usually long lasting. The disorder usually begins before age 25, persists throughout life, and affects persons of all social classes.

Both patients and their families often suffer from poor care and social ostracism because of widespread ignorance about the disorder. Although schizophrenia is discussed as if it is a single disease, it probably comprises a
group of disorders

with heterogeneous etiologies, and it includes patients whose clinical presentations, treatment response, and courses of illness vary.
Clinicians should appreciate that the diagnosis of schizophrenia is based entirely on the psychiatric history and mental status examination. There is no laboratory test for schizophrenia.

Sto
ries o
f S
ch
izop
hre
nia

Emil Kraepelin translated Morel's démence précoce into dementia precox, a term that emphasized the change in cognition (dementia) and early onset (precox) of the disorder.

Patients with dementia precox were described as having a long-term deteriorating course and the clinical symptoms of hallucinations and delusions.

Eugene BleulerBleuler coined the term
schizophrenia, which replaced dementia precox in the literature. He chose the term to express the presence of schisms between thought, emotion, and behavior in patients with the disorder.

Bleuler stressed that, unlike Kraepelin's concept of dementia precox, schizophrenia need not have a deteriorating course. This term is often misconstrued, especially by lay people, to mean split personality. Split personality, called dissociative identity disorder

The Four As
associational disturbances of thought, especially looseness,
affective disturbances, autism, and Ambivalence Bleuler also identified accessory
(secondary) symptoms, which included those symptoms that Kraepelin saw as major indicators of dementia precox: hallucinations and delusions.

Kurt Schneider Schneider contributed a
description of first-rank symptoms, which, he stressed, were not specific for schizophrenia and were not to be rigidly applied but were useful for making diagnoses. He emphasized that in patients who showed no first-rank symptoms, the disorder could be diagnosed exclusively on the basis of second-rank symptoms and an otherwise typical clinical appearance.
Clinicians frequently ignore his warnings and sometimes see the absence of first-rank symptoms during a single interview as evidence that a person does not have schizophrenia.

Kurt Schneider Criteria for Schizophrenia
1.First-rank symptoms 1.Audible thoughts 2.Voices arguing or discussing or both 3.Voices commenting 4.Somatic passivity experiences 5.Thought withdrawal and other
experiences of influenced thought 6.Thought broadcasting 7.Delusional perceptions 8.All other experiences involving
volition made affects, and made impulses
1.Second-rank symptoms 1.Other disorders of perception 2.Sudden delusional ideas 3.Perplexity 4.Depressive and euphoric mood
changes 5.Feelings of emotional
impoverishment 6.“…and several others as
well†�
Schneider first rank symptoms of schizophrenia
Individual symptoms that are highly specific for schizophrenia
Occur in about 80% of schizo pts, 40% in bipolar mood disorder ( only mania)& 20% in severe major depression

Schizophrenia

Gender and AgeSchizophrenia is equally prevalent
in men and women. Onset is earlier in men than in women.
Approximately 3 to 10 percent of women with schizophrenia present with disease onset after age 40. About 90 percent of patients in treatment for schizophrenia are between 15 and 55 years old.
Onset of schizophrenia before age 10 or after age 60 is extremely rare.

Some studies have indicated that men are more likely to be impaired by negative symptoms than are women and that women are more likely to have better social functioning than are men prior to disease onset. In general, the outcome for female schizophrenia patients is better than that for male schizophrenia patients. When onset occurs after age 45, the disorder is characterized as late-onset schizophrenia.

In Malaysia
• Lifetime prevalence 1-1.5%• There is 7351 cases had been reported from 2003-2005
• The incidence was noted higher in males, urban and migrant population
Incidence and prevalence(In Malaysia)
• 60% of the schizophrenia cases are man
Sex ratio
• Prevalence > low socioeconomic groups
Socioeconomic status
• Common between 15 and 35, rare before 10 and after 40 years old. Earlier onset for ♂
Age of onset

Epidemiology: Sex
Philippines
Local figures are unavailable but Philippine Health Statistics said authorities are alarmed at the increasing suicide rate in the country.
In 2000 alone, there were 1.8 deaths from suicide per 100,000 population.
Suicide is common in people with schizophrenia.

According to the World Health Organization, schizophrenia is one of the top 10 causes of disabilities in developed countries.

A disability survey made by the National Statistics Office (NSO) showed it is among the third most common form of disabilities with a prevalence rate of 88 cases per 100,000 population.

“The region with the highest prevalence rate is Southern Tagalog at 132.9 cases per 100,000 population, followed by NCR at 130.8 per 100,000 population and Central Luzon at 88.2 per 100,000 population,” the NSO revealed.





A Philippine study conducted in three primary health centers in urban slum in Manila in 1993-1994 showed that 17 % of adults and 16 % of children had mental disorders. Prevalence of mental health disorders was at 35%. A study conducted by the University of the Philippines’ Department of Psychiatry in the rural areas in 1989 yielded similar findings, where 34% of those with mental disorders had social problems.

The three most frequent diagnoses among the adults were: psychosis (4.3%), anxiety (14.3%) and panic (5.6%). For children and adolescents, the top five most prevalent psychiatric conditions were: enuresis (9.3%), speech and language disorder (3.9%), mental sub-normality(3.7%), adaptation reaction (2.4%) and neurotic disorder (1.1%)

A study performed in the 1970s even showed that 12 out of 1000 Filipinos have severe mental disorder, quite an alarming rate if compared with the internationally recognized rate of 1/1000.

In the past three decades, Filipinos have been exported as work force abroad in the light of economic justifications to support their families. Of the 7.76 million Filipinos overseas in 197 countries, 2.86 million immigrants or permanent residents, 3.38 million documented OFWs, and 1.5 million irregularly documented overseas workers. 75% of these workers are women, majority of which work as domestic helpers in countries such as Saudi Arabia, Taiwan, UAE, Hong Kong and Kuwait.

Seafarers, mostly male workers, find it most difficult during long periods of isolation out at sea specially those who work in cargo ships and tankers, in contrast to those who work on cruise liners whose ships dock more often, allowing them to interact with other people almost everyday.
Filipinas working as domestic helpers abroad are exposed to situations that render them vulnerable to physical, sexual and psychological abuses.

In 2007, reported by Philippine Star Cases of mental illness in the country are on
the rise with the increase in population, reporting that the most common disease is schizophrenia which affects one percent of the total population.Dr. Noel Reyes, a psychiatrist at the National Center for Mental Health in Mandaluyong City, said one of the most common brain diseases among Filipinos is schizophrenia, which afflicts one percent of the total population.

Increase in the incidence of mental illness was also due to the widespread use of prohibited drugs.
He said the Dangerous Drugs Board recently released data, which shows that eight million Filipinos are drug users.
Most common in seafarers.

At the GMA News’ online hub, (2008) there is was an article entitled "1 in 5 adult Pinoys have psychiatric disorders.” It further says that more people are developing mental disorders due to “extreme life experiences.”
between 17 to 20 percent of the country’s adult population have psychiatric disorders.
About 10 to 15 percent of children aged 5 to 15 are believed to have mental problems.

Etiology

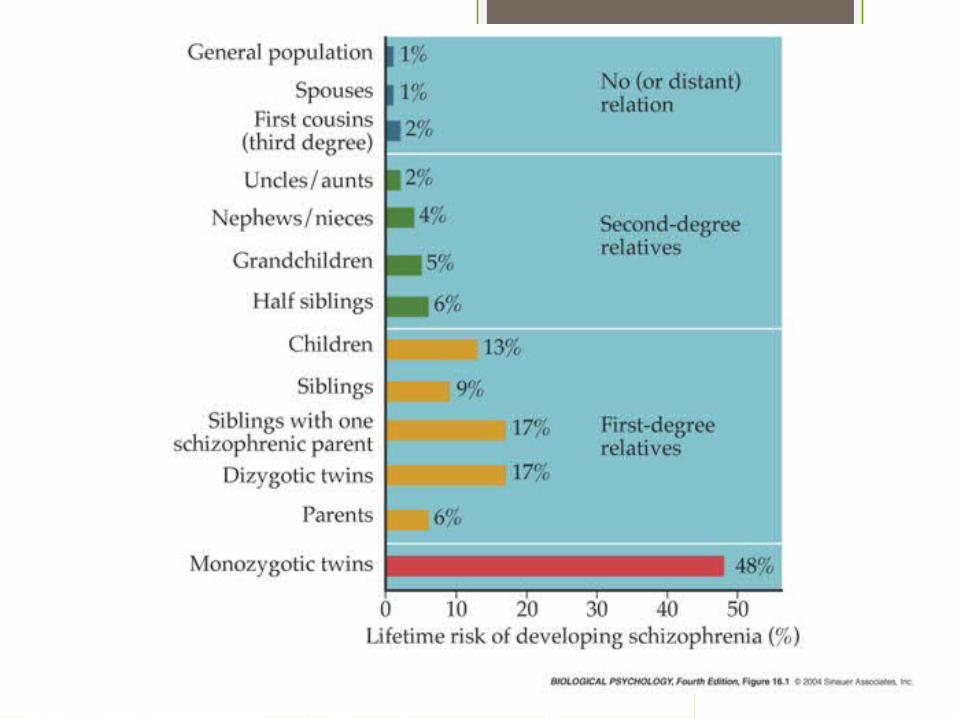
Genetic TheoriesSchizophrenia occur at an
increased rate among the biological relatives of patients with schizophrenia. The likelihood of a person having schizophrenia is correlated with the closeness of the relationship to an affected relative (e.g., first- or second-degree relative). 3-7%

Genetics – Twin Studies
Gottesman 1991 suggests that schizophrenia is inherited through genes. Studied 40 twins - the concordance rate for MZ twins is about 48% and only about 17% for DZ twins.
Also Cardno 2002 – showed concordance rate of 26.5 MZ and 0% for DZ.

Genetics – Family Studies
Gottesman also studied families – he concluded that if both your parents suffer from Schizophrenia, then you have a 46% chance of developing it yourself (compared to a 1% chance of someone selected at random will suffer)
The more genetically similar relatives are, the more concordance is found.

Polygenic Transmissions
Reports on chromosome 5 are associated with some pattern of familial transmission.
Eye Movement Dysfunction- Various studies have reported abnormal eye movements in 50 to 85 percent of patients with schizophrenia, compared with about 25 percent in psychiatric patients without schizophrenia and less than 10 percent in nonpsychiatrically ill control subjects.

In studies of schizophrenic patients with no history of illness in either the maternal or paternal line, it was found that those born from fathers older than the age of 60 were vulnerable to developing the disorder. Presumably, spermatogenesis in older men is subject to greater epigenetic damage than in younger men.

Developmental TheoriesBirth Season- Persons who
develop schizophrenia are more likely to have been born in the winter and early spring and less likely to have been born in late spring and summer.

In the Northern Hemisphere, including the United States, persons with schizophrenia are more often born in the months from January to April. In the Southern Hemisphere, persons with schizophrenia are more often born in the months from July to September. Season-specific risk factors, such as a virus or a seasonal change in diet, may be operative.

Another hypothesis is that persons with a genetic predisposition for schizophrenia have a decreased biological advantage to survive season-specific insults.

PrenatalGestational and birth complications,
exposure to influenza epidemics, or maternal starvation during pregnancy, Rhesus factor incompatibility, and an excess of winter births is implicated. The nature of these factors suggests a neurodevelopmental pathological process in schizophrenia, but the exact pathophysiological mechanism associated with these risk factors is not known.

Evidence that prenatal malnutrition may play a role in schizophrenia was derived from the studies of the Dutch Hunger Winter of 1944 to 1945. Severe caloric restriction in the western Netherlands was associated with substantially decreased fertility, increased mortality, and diminished birth weight.

Biological ExplanationsGeneticsBio chemicals
Brain Structure

DOPAMINE HYPOTHESIS

Biochemical Factors – The Dopamine Hypothesis
This theory claims that excessive amounts of dopamine or an oversensitivity of the brain to dopamine is the cause of schizophrenia
There is strong empirical support which suggests that dopamine plays an important role in schizophrenia – e.g drugs which block dopamine (Phenothaiazines) also seem to reduce the symptoms of schizophrenia.

Normal Level of Dopamine In The
Human Brain
Elevated Level of Dopamine In The Brain of a Schizophrenic Patient
(specifically the D2 receptor)
Neurons that use the transmitter ‘dopamine’ fire too often and transmit too many messages or too often.
Certain D2 receptors are known to play a key role in guiding attention.
Lowering DA activity helps remove the symptoms of schizophrenia

DOPAMINE HYPOTHESIS
The Dopamine hypothesis states that the brain of schizophrenic patients produces more dopamine than normal brains.
–Evidence comes from –studies with drugs –post mortems –pet scans

Falkai et al 1988Autopsies have found that people
with schizophrenia have a larger than usual number of dopamine receptors.
Increase of DA in brain structures and receptor density (left amygdala and caudate nucleus putamen)
Concluded that DA production is abnormal for schizophrenia
POST MORTEM

Parkinson’s disease
Parkinson’s sufferers have low levels of dopamine
L-dopa raises DA activity People with Parkinson's develop
schizophrenic symptoms if they take too much L-dopa
–Chlorphromazine (given to schizophrenics) reduces the symptoms by blocking D2 receptors

Lindstroem et al (1999)Radioactively labelled a chemical L-
Dopa administered to 10 patients with schizophrenia and 10 with no diagnosis
L-Dopa taken up quicker with schizophrenic patients
Suggests they were producing more DA than the control group.
PET SCANS

Other neurotransmitter abnormalities implicated in schizophrenia:elevated serotonin.elevated
norepinephrine.decreased gamma-
aminobutyric acid (GABA).

Anatomical abnormalities
Enlargement of lateral ventricles
Smaller than normal total brain volume
Cortical atrophyWidening of third ventricleSmaller hippocampus

Brain Structure
People with schizophrenia have abnormally large ventricles in the brain. Ventricles are fluid filled cavities. This means that the brains of schizophrenics are lighter than normal.

Brain Structure EvidenceAndreasen et 1990 –
conducted a very well controlled CAT scan study and found significant enlargement of the ventricles in schizophrenics compared to controls.
However this was only the case for men and not for women. Therefore cant generalise to everyone.

Further Evaluation
The main problem with such studies is that it is not found in all schizophrenics. This has lead to further research done by Crow 1985.
He suggested two types of schizophrenia with two biological causes.

Two Syndrome Hypothesis - Crow 1985
Type one - genetically inherited associated with dopamine – characterised by positive symptoms.
Type Two – Neurodevelopmenal disorder – to do with Brain structure – characterised by negative symptoms.

Psychological TheoriesPsychological Testing shows:Lack of creativityAttention DeficitsLoss of Executive Functions

Psychoanalytic TheoriesSigmund Freud postulated that
schizophrenia resulted from developmental fixations that occurred earlier than those culminating in the development of neuroses. These fixations produce defects in ego development. Because the ego affects the interpretation of reality and the control of inner drives, such as sex and aggression, these ego functions are impaired. Thus, intrapsychic conflict arising from the early fixations and the ego defect, which may have resulted from poor early object relations, fuel the psychotic symptoms.

Psychoanalytic theory also postulates that the various symptoms of schizophrenia have symbolic meaning for individual patients. For example, fantasies of the world coming to an end may indicate a perception that a person's internal world has broken down.

Feelings of inferiority are replaced by delusions of grandeur and omnipotence. Hallucinations may be substitutes for a patient's inability to deal with objective reality and may represent inner wishes or fears. Delusions, like hallucinations, are regressive, restitutive attempts to create a new reality or to express hidden fears or impulses.

Margaret MahlerThere are distortions in the
reciprocal relationship between the infant and the mother. The child is unable to separate from, and progress beyond, the closeness and complete dependence that characterize the mother-child relationship in the oral phase of development. As a result, the person's identity never becomes secure.

In a study of British 4-year-old children, those who had a poor mother-child relationship had a sixfold increase in the risk of developing schizophrenia, and offspring from schizophrenic mothers who were adopted away at birth were more likely to develop the illness if they were reared in adverse circumstances compared to those raised in loving homes by stable adoptive parents.

Harry Stack Sullivan viewed schizophrenia as a disturbance in interpersonal relatedness. The patient's massive anxiety creates a sense of unrelatedness that is transformed into parataxic distortions, which are usually, but not always, persecutory. To Sullivan, schizophrenia is an adaptive method used to avoid panic, terror, and disintegration of the sense of self. The source of pathological anxiety results from cumulative experiential traumas during development.

Double-Bind Communication
The double-bind concept was formulated by Gregory Bateson and Donald Jackson to describe a hypothetical family in which children receive conflicting parental messages about their behavior, attitudes, and feelings.

In Bateson's hypothesis, children withdraw into a psychotic state to escape the unsolvable confusion of the double bind. Unfortunately, the family studies that were conducted to validate the theory were seriously flawed methodologically. An example of a double bind is the parent who tells the child to provide cookies for his or her friends and then chastises the child for giving away too many cookies to playmates.
No longer accepted.

Expressed Emotion. Parents or other caregivers may behave with overt criticism, hostility, and overinvolvement toward a person with schizophrenia. Many studies have indicated that in families with high levels of expressed emotion, the relapse rate for schizophrenia is high. The assessment of expressed emotion involves analyzing both what is said and the manner in which it is said.

Learning Theoriesschizophrenia learn irrational
reactions and ways of thinking by imitating parents who have their own significant emotional problems.
poor interpersonal relationships of persons with schizophrenia develop because of poor models for learning during childhood.

ROLE OF DRUGS
–Amphetamines (agonists) lead to increase in DA levels
–Large quantities lead to delusions and hallucinations

Substance abuse The lifetime prevalence of any
drug abuse (other than tobacco) is often greater than 50 percent.
There has been particular interest in the association between cannabis and schizophrenia. Those reporting high levels of cannabis use (more than 50 occasions) were at sixfold increased risk of schizophrenia compared to nonusers.

The use of amphetamines, cocaine, and similar drugs should raise particular concern because of their marked ability to increase psychotic symptoms.
In one population-based study, the lifetime prevalence of alcohol within schizophrenia was 40 percent.

Cultural and Socioeconomic Factors
People in developing countries are less likely to develop schizophrenia.

Clinical features

PSYCHOSIS
Mood disorders
Schizophrenia “spectrum” disorders
“organic” mental disorders
Substanceinduced
DeliriumDementiaAmnestic d/o
“Functional”disorders

Key Features
Acute syndrome (positive symptoms)
• Hallucinations• Delusion• Disorganised
speech/thinking/ behaviour
• Catatonic behaviours• Delusion of reference
Chronic syndrome (negative symptoms)
• Affective Flattening• Alogia• Avolition• Anhedonia• Attention(poor)

Positive symtomsThose that appear to reflect an excess or
distortion of normal functions. Positive symptoms are those that have a positive reaction from some treatment. In other words, positive symptoms respond to treatment.
Delusions. Those where the patient thinks he is being followed or watched are common; also the belief that people on TV, radio are directing special messages to him/her.

Hallucinations. Distortions or exaggerations of perception in any of the senses.
Often they hear voices within their own thoughts followed by visual hallucinations.

Disorganized thinking/speech.
AKA loose associations; speech is tangential, loosely associated or incoherent enough to impair communication.

Grossly disorganized behavior.
Difficulty in goal directed behavior (ADLs), unpredictable agitation or silliness, social disinhibition, or bizarre behavior.
There is a purposelessness to behavior.

Inappropriate response to stimuli
Unusual motor behavior (pacing, rocking)
DepersonalizationDerealizationSomatic preoccupations

Catatonic behavior.
Marked decrease in reaction to immediate environment, sometimes just unaware of surroundings, rigid or bizarre postures, aimless motor activity.

Disorganized SymptomsThis one is
somewhat new and may not be considered valid.
It is thought disorder, confusion, disorientation and memory problems.

Negative Symptoms
Those that appear to reflect a diminution or loss of normal functions.
May be difficult to evaluate because they are not as grossly abnormal as positive symptoms.
Currently there is no treatment that has a consistent impact on negative symptoms

Affective flattening.
Reduction in the range and intensity of emotional expression, including facial expression, voice tone, eye contact and body language.
Alogia (poverty of speech)
Lessening of speech fluency and productivity, thought to reflect slowing or blocked thoughts; often manifested as short, empty replies to questions.

Avolition
The reduction, difficulty or inability to initiate and persist in goal-directed behavior. Often mistaken for apparent disinterest.

No longer interested in going out with friends
No longer interested in activities that the person used to show enthusiasm
No longer interested in anythingSitting in the house for hours or
days doing nothing
Cognitive SymptomsDifficulties in concentration
and memory:Disorganized thinkingSlow thinkingDifficulty understandingPoor concentrationPoor memoryDifficulty expressing
thoughtsDifficulty integrating
thoughts, feelings, behaviors

Psychotic Disorders
Schizo-phrenia
Usually insidious
Many Chronic >6 months
Delusional disorder
Varies (usually insidious)
Delusions only
Chronic >1 mo.
Brief psychotic disorder
Sudden Varies Limited <1 mo.
Onset Symptoms Course Duration

Kurt Schneider (German psychiatrist) ’s symptoms of first rank
1. Auditory hallucinations: audible thought or thought echo ; referring third person; running commentary.
2. Alienation of thought: thought insertion or withdrawal
3. Diffusion of thought (thought broadcasting)
4. Sensation of feelings, impulses or acts being controlled by external forces
5. Somatic passivity < external agency (e.g. X-rays, hypnosis)
6. Delusional perception

MANAGEMENTS

Course• Complete recovery 20%
• Recurrent acute illness20%
• Chronic disease starting acutely20%
• Chronic disease starting insidiously20%
• Suicide10-15%

Prognosis Recover completely/long
term minimal symptoms- 30%(The percentage on the rise)
Recurrent illness -poorer prognosis
Young patient -high risk of suicide

Predictors for poor outcome
Features of the illness
Insidious onset
Long 1st episode
Previous psychiatric history
Negative symptoms
Younger age at onset
Features of the patient
Male
Single, separated, widowed or divorced
Poor psychosexual adjustment
Poor employment
Social isolation
Poor compliance
Assessment
No confirmatory laboratory studies.
Diagnosis made based on psychotic symptoms and functional deterioration.
Diagnostic evaluation: aim Establish the presense of
psychosis Eliminate other differential
diagnosis

Evaluation of of psychosis

105
Need rapid tranquilisati
on
Urgent
No
Yes Combination of parenteral treatment
Yes
Yes
No
Identify Phases of Illness
No
Adequate dose &
duration
Oral medication is preferred When parenteral needed, use a single agent
•Provide comprehensive plan (pharmacological, psychosocial & service level interventions)•Offer conventional APs (300-1000mg CPZ equivalent) or AMS or OLZ•Monitor clinical response, side effects & treatment adherence
Poor response
Optimise APs usage
•Exclude substance abuse, treatment non-adherence & concurrent other general medical conditions•Optimise psychosocial interventions•Refer to psychiatrist for trial of clozapine
Yes
No
•Plan for recovery (ACT, family intervention, psychoeducation, social skills training & supported employment)•APs usage to continue with single oral agent from acute phase; use depot when non-adherent•Monitor for clinical response, side effects & treatment adherence
Acute phase
Relapse prevention
ALGORITHM FOR MANAGEMENT OF SCHIZOPHRENIA
Diagnosis of Schizophrenia
Stable phase
· Follow-up at primary care· Follow manual on Garispanduan
Perkhidmatan Rawatan Susulan Pesakit Mental di Klinik Kesihatan
Prevention & management of side effects of APs at all phases·aonitor EPS/akathisia/weight gain/diabetes/heart disease/sexual dysfunction·Follow schedule of physical care as per follow-up manual

THREE PHASES OF SCHIZOPHRENIA
Prodromal
• Decline in functioning that precedes 1st psychotic episode
• Socially withdrawn, irritable
• Physical complaints
• Newfound interest in religion / the occult
Psychotic (acute
phase)• Positive
symptoms• Perceptual
disturbances (e.g. auditory hallucinations)
• Delusions (usually secondary, delusion of reference common)
• Disordered thought process / content
Residual (chronic
phase)• Occurs between
episodes of psychosis
• Marked by negative symptoms (flat affect, social withdrawal)
• odd thinking and behaviour


Click icon to add picture
Related Documents











