Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
/ /
262 THE INDIAN MEDICAL GAZETTE [May, 1941
SCARS AND OPACITIES OF THE CORNEA AND THEIR TREATMENT
By G. S. GUHA
Honorary Ophthalmic Surgeon, Government Hospital, Shillong
In our country, corneal soars and opacities are common. This is especially so in the crowded streets of big cities. The large majority of the partially blinded and a considerable pro- portion of the totally blinded are suffering from this ocular affection. The important causes of this group of ocular affections in our country are ophthalmia-neonatorum, neglected con-
junctivitis and corneal ulcers, smallpox, irritant drugs, trachoma, and keratomalacia. These scars and opacities may be due either
to the primary affection of the cornea itself
{e.g., primary ulcer of the cornea, perforating or penetrating injury, or injury to the cornea
by a foreign body or irritant drugs) or to its
secondary affection from the spread of an infec- tive or inflammatory process {e.g., neglected acute or chronic conjunctivitis, trachoma, glaucoma, scleritis, episcleritis, cyclitis, and
iridocyclitis), a growth from the other parts of the eye {e.g., pterygium), or the result of a
specific infective process of the system {e.g.,
syphilis, tuberculosis, leprosy, smallpox, chicken pox, cholera, and rarely influenza, cerebro-
spinal meningitis, malaria, and kala-azar), defi- ciency diseases {e.g., keratomalacia), senile and other degenerative conditions {e.g., arcus senilis, axial degeneration of the cornea, band-shaped opacity of the cornea, etc.), neurotrophic dis- orders {e.g., various forms of herpetic keratitis and lesion of the 5th nerve), or of the spread of certain skin conditions {e.g., rosacea, acne).
Again, such rare conditions as metabolic {e.g., keratitis in gout, sclerosing keratitis in diabetes, central indolent ulcer of the cornea in cachectic conditions in children) and endocrine {e.g., corneal grey spots in myxcedema) disorders, desiccation, exposure, and irritation {e.g., kera- titis sicca, keratitis lagophthalmos, in trichiasis, and ectropion of the lids, etc.), pigmentations of the cornea {e.g., metallic pigmentations of the cornea, melanosis of the cornea, and blood staining of the cornea), and congenital condi- tions {e.g., in congenital leucomata, congenital staphyloma, keratoconus and embryatoxis) may be the cause of corneal scars and opacities. Before going into the discussion of the treat-
ment of scars and opacities of the cornea,
some important facts about the structure and function of the cornea and its pathological variations should be borne in mind.
1. It is an avascular structure and its
nourishment depends mainly on dialysis from the periphery. Hence its metabolic process is
sluggish and its affection tends to be chronic. 2. Its function depends mainly on its trans-
parency and any slight injury to its tissue may affect this transparency.
3. The extreme sensibility of its epithelium and the imperviousness of its superficial cells to all toxins, except to the gonococcus and
diphtheria bacillus, and probably to the pneumo- coccus are its natural protections.
4. Its ̂ epithelium has wonderful powers of
regeneration. Therefore any damage of the
corneal tissue up to the limit of the epithelium is not of much consequence.
5. Its epithelium is continuous with the
epithelium of the conjunctiva; hence it is not difficult to see how the affection of the conjunc- tiva may also affect the cornea.
6. Its endothelium, like the external con-
tinuity of its epithelium with the conjunctiva, has also continuity with the uveal tract; there- fore an affection of the uveal tract may affect the cornea secondarily through its endothelium.
7. The sclerotic and the cornea are struc-
turally continuous with each other, both form- ing the external tunic of the eye; hence any
affection of the sclerotic may also spread to
the cornea.
8. The Bowman's membrane has little power of resistance and is easily affected. When once
destroyed, it never regenerates; therefore some
degree of permanent opacity is sure to result after it has been affected.
May, 1941] SCARS AND OPACITIES OF THE CORNEA: GUHA 263
9- The corneal lamella) in the substantia Propria when destroyed is not reformed, unless the defect is superficial, in which case the loss ?* tissue is replaced by epithelial growth.
10- Descemet's membrane, unlike Bowman's
jttembrane and the substantia propria, is a
ughly resistant structure. Therefore it is a great check to external infective processes Peering the eye.
11. In superficial injuries of the cornea, the detect is recovered by growth of the epithelium and no opacity of the cornea results.
12. When the injury of the cornea is deeper, ^generation of the epithelium together with the urination of new blood vessels from the peri- phery result in the growth' of connective tissue
_lch gives rise to corneal opacities or scars. 13. If the loss of corneal tissue is extensive
and scar tissue formation deficient, the thin cornea is likely to bulge out owing to the pres- ence of the intra-ocular pressure, resulting in an stasia of the cornea.
14. When the whole thickness of the cornea, ?Xcept Descemet's membrane is destroyed the atter, being very resistant, may still persist but u^ge forward as a result of intra-ocular pres-
Slll'e and thus form a keratocele. 15. In perforating wounds or in perforating
J?er of the cornea, if there is loss of aqueous, le iris may come in contact with the cornea
and slowly get attached to it by fibrinous exudate and thus form an anterior synechia
adherent leucoma. 16. In a perforating injury through the
centre c>f the cornea with the escape of aqueous and injury of the lens capsule, the lens capsule may form a synechia with the cornea.
I?- If any corneal scar is extensive, incar-
nated with the iris and ectasia, anterior aPhyloma is produced, which may be partial
?n. total, depending on the extent of the prolapsed ris tissue; when a part of the iris tissue gets ^tangled in the corneal perforation, a newly ?nned growth of the iris tissue may form in the
^ar tissue resulting in the pigment formation the adherent leucoma. 18. The entangled iris tissue in the perforated
i ea'. 0r the torn capsule of the lens in perforat- n? injuries may keep the opening partially
, ,Pen, so that the aqueous may slowly escape rough forming a fistula which looks like a ack dot on the cornea and which area is
1
ained by fluorescein. - 19- If the iris is carried not only into the ound but protrudes through it, the condition is ahed prolapse of the iris. 20. jn advanced cases of injuries to the
o?rnea, penetrating or otherwise, where the lens r
especially the vitreous may escape forming a ? opacity of the whole cornea, the condition
called phthisis bulbi anterior. Owing to
^ sudden lowering of tension in some other
^'ases, there may be choroidal haemorrhage, and _n.e vitreous, retina and choroid may come out
h the shrinkage of the whole eyeball, a con-
dition called the phthisis bulbi. Phthisis bulbi may also form as a result of cyclitis. Left to themselves, scars or opacities of the
cornea tend to clear up, especially in younger individuals and when the lesion is superficial, as already explained. Hence age is a great factor in regard to prognosis of vision after corneal affections. Besides having a tendency to clear up, such scars may give rise to pig- mentary or other degenerative changes. In extensive scar formation, glaucoma may result with associated degenerative changes in the
ciliary body, choroid, retina, and vitreous.
Treatment
1. Prophylactic or preventive (?) Mechanical protection of the eye by
goggles against accidental injuries of the cornea. (?) Vaccination against smallpox. (c) Introduction of vitamins in diet to pre-
vent keratomalacia.
(d) Prophylactic or preventive treatment for non-perforating wounds or ulcers against per- foration where the prognosis in regard to vision may be grave.
2. Medicinal
Medicinal treatment may be resorted to in more-or-less recent and superficial opacities of the cornea and where there is not much involve- ment of the neighbouring structures. Drugs used for the absorption of the corneal
Scars are mostly those which improve the local circulation. Such drugs are hydrargyri oxidum flavum, dionin, calomel, noviform, jequirity, quinine bisulphate, benzyl-cinnamic-ester, etc., instillation of oily drops, e.g., paroleine may be useful in keratitis sicca.
In addition to the local use of drugs non- specific protein therapy in the shape of milk
injections may give good results. Besides, specific therapy in syphilitic and
leprotic cases, as well as tuberculin in tuber- culous cases when not too late, may surprisingly clear up corneal opacities. Also local and in- ternal administration of vitamin A is useful in cases of keratomalacia and superficial punctate keratitis.
3. Physical Physical methods of treatment are used
with the idea of producing locally more lymph and peripherally more blood circulation; these
are finger massage, electric vibro massage,
ultra-violet ray, etc. The results of such methods of treatment are
very seldom satisfactory.
4. Operative treatment
Satisfactory results are mostly found by operative treatment.
(A) Optical iridectomy. In central and deep scars, where there is sufficient clear cornea left
at the periphery, optical iridectomy should be done.
264 THE INDIAN MEDICAL GAZETTE [May, 1941
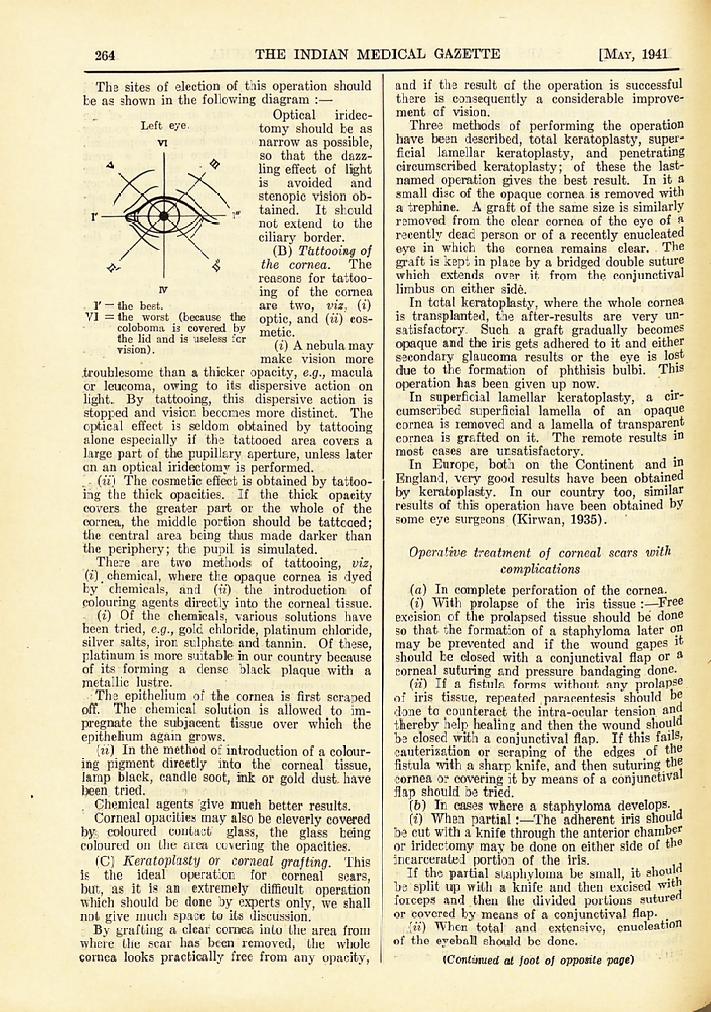
The sites of election of this operation should be as shown in the following diagram :?
Optical iridec-
tomy should be as narrow as possible, so that the dazz-
ling effect of light is avoided and
stenopic vision ob- tained. It should not extend to the
ciliary border. (B) Thttooing of
the cornea. The reasons for tattoo-
ing of the cornea are two, viz, (i) optic, and (ii) cos- metic.
(i) A nebula may make vision more
.troublesome than a thicker opacity, e.g., macula or leucoma, owing to its dispersive action on
light. By tattooing, this dispersive action is
stopped and vision becomes more distinct. The
optical effect is seldom obtained by tattooing alone especially if the tattooed area covers a
large part of the pupillary aperture, unless later on an optical iridectomy is performed.
r (u) The cosmetic effect is obtained by tattoo- ing the thick opacities. If the thick opacity covers the greater part or the whole of the
cornea, the middle portion should be tattooed; the central area being thus made darker than the periphery; the pupil is simulated.
There are two methods of tattooing, viz, (i) # chemical, where the opaque cornea is dyed by chemicals, and (u) the introduction of
colouring agents directly into the corneal tissue. (i) Of the chemicals, various solutions have
been tried, e.g., gold chloride, platinum chloride, silver salts, iron sulphate and tannin. Of these, platinum is more suitable in our country because of its forming a dense black plaque with a
metallic lustre. The epithelium of the cornea is first scraped
off. The chemical solution is allowed to im-
pregnate the subjacent tissue over which the
epithelium again grows. (it) In the method of introduction of a colour-
ing pigment directly into the corneal tissue, lamp black, candle soot, ink or gold dust, have been tried.
Chemical agents give much better results. Corneal opacities may also be cleverly covered
by, coloured contact glass, the glass being coloured on the area covering the opacities.
(C) Keratoplasty or corneal grafting. This is the ideal operation for corneal scars, but, as it is an extremely difficult operation which should be done by experts only, we shall not give much space to its discussion. By grafting a clear cornea into the area from
where the scar has been removed, the whole cornea looks practically free from any opacity,
and if the result of the operation is successful there is consequently a considerable improve- ment of vision. Three methods of performing the operation
have been described, total keratoplasty, super- ficial lamellar keratoplasty, and penetrating circumscribed keratoplasty; of these the last- named operation gives the best result. In it a
small disc of the opaque cornea is removed with a trephine. A graft of the same size is similarly removed from the clear cornea of the eye of a
recently dead person or of a recently enucleated eye in which the cornea remains clear. The
graft is kept in place by a bridged double suture which extends over it from the conjunctival limbus on either side. In total keratoplasty, where the whole cornea
is transplanted, the after-results are very un-
satisfactory. Such a graft gradually becomes opaque and the iris gets adhered to it and either secondary glaucoma results or the eye is lost due to the formation of phthisis bulbi. This
operation has been given up now. In superficial lamellar keratoplasty, a cir-
cumscribed superficial lamella of an opaque cornea is removed and a lamella of transparent cornea is grafted on it. The remote results in
most cases are unsatisfactory. In Europe, both on the Continent and in
England, very good results have been obtained by keratoplasty. In our country too, similar results of this operation have been obtained by some eye surgeons (Kirwan, 1935).
Operative treatment of corneal scars with
complications
(a) In complete perforation of the cornea. (i) With prolapse of the iris tissue :?Free
excision of the prolapsed tissue should be done so that the formation of a staphyloma later on
may be prevented and if the wound gapes it
should be closed with a conjunctival flap or a
corneal suturing and pressure bandaging done. (ii) If a fistula forms without any prolapse
of iris tissue, repeated paracentesis should be
done to counteract the intra-ocular tension and
thereby help healing and then the wound should be closed with a conjunctival flap. If this fails? cauterization or scraping of the edges of the
fistula with a sharp knife, and then suturing the cornea or covering it by means of a conjunctival flap should be tried.
(b) In cases where a staphyloma develops. (i) When partial :?The adherent iris should
be cut with a knife through the anterior chamber or iridectomy may be done on either side of the incarcerated portion of the iris. ,
If the partial staphyloma be small, it should be split up with a knife and then excised witn forceps and then the divided portions sutured or covered by means of a conjunctival flap. #
(ii) When total and extensive, enucleation of the eyeball should be done.
(Continued at foot of opposite page)
IV
I' = the best. VI the worst (because the
coloboma is covered by the lid and is useless for vision).
Left eye.
I' = the best. VI = the worst (because the
coloboma is covered by the lid and is useless for vision).
(Continued from -previous -page)
SELECT BIBLIOGRAPHY
Axenfeld, T. (1935) .. Lehrbuch und Atlas der
Augenheilkunde. Gustav
n Fischer, Jena, p. 368.
JuKe-Elder, W.S.(1930). Brit. J. Ophthalmol., 14, 61, 185.
Idem (1938). Textbook of Ophthalmology. C. V. Mosby and Co., St. Louis, Vol. II, pp. 1282, 1283, 1826, 1828, 1950, 1952, IQfjQ 9fifl4 9035
{JmwAN, E. O'G. (1935). Indian Med. Gaz., 70, 61. Arsons, J. H. (1930) .. Diseases of the Eye.
Macmillan and Co., New York, pp. 234, 246.
Related Documents