Program Location The Westin Riverwalk Hotel 420 West Market Street, San Antonio, Texas 78205 Saturday, July 7 th 7:00 am - 8:00 am Registration, Continental Breakfast, & Visit Exhibits Lectures presented by Alan Kabat, OD 8:00 am - 9:45 am OSD is NOT a 4 Letter Word COPE ID# 58280-AS CEE Available 2 D/T Hours 9:45 am - 10:15 am Break & Visit Exhibits 10:15 am - 12:00 pm Dermatology 101 - Lessons for Eye Care Practitioners COPE ID# 58281-SD CEE Available 2 D/T Hours 12:00 pm - 1:00 pm Lunch & Visit Exhibits Lectures presented by Michael Chaglasian, OD 1:00 pm - 2:45 pm Glaucoma Update New Tools and Treatment Options COPE ID# 56782-GL CEE Available 2 D/T Hours 2:45 pm - 3:15 pm Break & Visit Exhibits 3:15 pm - 5:00 pm Ocular Emergencies for the Primary Care Optometrist COPE ID# 58307-AS CEE Available 2 D/T Hours

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Program Location
The Westin Riverwalk Hotel 420 West Market Street, San Antonio, Texas 78205
Saturday, July 7th 7:00 am - 8:00 am Registration, Continental Breakfast, & Visit Exhibits
Lectures presented by Alan Kabat, OD
8:00 am - 9:45 am OSD is NOT a 4 Letter Word COPE ID# 58280-AS
CEE Available 2 D/T Hours
9:45 am - 10:15 am Break & Visit Exhibits
10:15 am - 12:00 pm Dermatology 101 - Lessons for Eye Care Practitioners COPE ID# 58281-SD
CEE Available 2 D/T Hours
12:00 pm - 1:00 pm Lunch & Visit Exhibits Lectures presented by Michael Chaglasian, OD
1:00 pm - 2:45 pm Glaucoma Update New Tools and Treatment Options COPE ID# 56782-GL
CEE Available 2 D/T Hours
2:45 pm - 3:15 pm Break & Visit Exhibits
3:15 pm - 5:00 pm Ocular Emergencies for the Primary Care Optometrist COPE ID# 58307-AS
CEE Available 2 D/T Hours

1
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, FAAO
Memphis, Tennessee
Promotional Speaker: OCuSOFT
Shire
Clinical Researcher: Bio-Tissue
Shire
Vmax Vision
Editorial Boards: Optometric Office (FVMG)
Optometric Physician (Jobson)
Review of Optometry (Jobson)
Advisory Boards: Avellino Labs
Bruder
EyeGate Pharma
OCuSOFT
Shire
Sun Ophthalmics
TearScience
Vmax Vision
Clinical Consultant: Bio-Tissue
Lacrivera
Vmax Vision
Per COPE stipulations, all disclosed financial relationships are current to within 12 months of this speaking engagement… July 7, 2018.
Complex disorder with numerous etiological factors
Confusing terminology
Numerous diagnostic strategies but no single confirmatory test
Numerous treatment options with variable / partial success
- Difficult to predict WHICH patients will be successful with WHICH therapy
Confusion leads to indecision… Indecision leads to fear…
OCULAR SURFACE DISEASE

2
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
STEP #1
LISTEN!!
Patients will give you clues to the diagnosis if you listen
closely and identify key complaints…
SYMPTOMS OF DED
Common complaints include:
• Burning
• Stinging
• Dryness
• Itching
• Grittiness
• Sandy
• Crusty
• Sore
• Tired
But also, listen for things like:
• Redness
• Blurry vision
• Fluctuating vision
• Difficulty with prolonged:
Reading
Computer work
Driving
Watching television
QUESTIONNAIRES
Permit quantification of symptoms in terms of severity and frequency
Many options
Validated by TFOS**
- Ocular Surface Disease Index (OSDI)
- Dry Eye Questionnaire (DEQ-5)
- Impact of Dry Eye on Everyday Living (IDEEL)
- National Eye Institute’s Visual Function
Questionnaire (NEI VFQ-25)
- Dry Eye-related Quality-of-Life Score (DEQS)
- Computer-vision Symptom Scale (CVSS-17)

3
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
TFOS DEWS IITHE OCULAR SURFACE (2017)
STEP #2
CONDUCT AN APPROPRIATE WORKUP
TFOS DEWS IITHE OCULAR SURFACE (2017)

4
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
THOUGHTS ON DIAGNOSTIC TESTING
TEARLAB
Measures tear osmolarity (osmolality)
- Normal: 280-295 mOsml/L
- >308 mOsm/L is considered hyperosmolar
- Inter-eye difference = hallmark of DED ( >8 mOsms/L between eyes)
Highly regarded by researchers; variable acceptance amongst clinicians
- Biggest issue is variability
CPT 83861-QW
INFLAMMADRY
Detects elevated MMP-9 in tears
- NON-SPECIFIC inflammatory biomarker
- QUALITATIVE, not quantitiative
May help to identify, classifying and monitor DED
May help determine best candidates for anti-inflammatory medications
CPT 83516-QW (Immunoassay for Analyte)
5
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
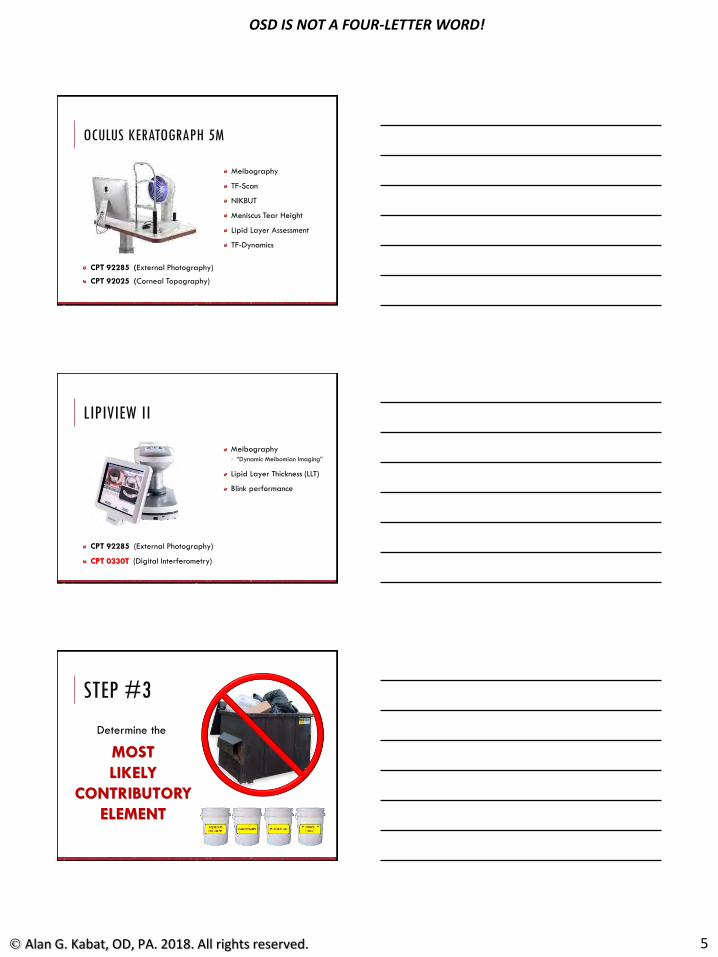
OCULUS KERATOGRAPH 5M
CPT 92285 (External Photography)
CPT 92025 (Corneal Topography)
Meibography
TF-Scan
NIKBUT
Meniscus Tear Height
Lipid Layer Assessment
TF-Dynamics
LIPIVIEW II
CPT 92285 (External Photography)
CPT 0330T (Digital Interferometry)
Meibography
- “Dynamic Meibomian Imaging”
Lipid Layer Thickness (LLT)
Blink performance
STEP #3
Determine the
MOST
LIKELY
CONTRIBUTORY
ELEMENT

6
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
OSD “BUCKETS”
Aqueous deficiency (Dry eye syndrome - H04.123)
Keratoconjunctivitis sicca (non-Sjögren’s - H16.223)
Sicca syndrome with keratoconjunctivitis(Sjögren’s syndrome - M35.01)
Filamentary keratitis (H16.123)
OSD “BUCKETS”
Anterior blepharitis (Unspecified blepharitis - H01.00-)
Meibomian gland dysfunction (Unspecified blepharitis - H01.00-)
Lagophthalmos (Unspecified lagophthalmos - H02.20-)
DON’T FORGET DEMODEX!!
ICD10 = B88.0
Demodex is an exoparasite of the skin, particularly common on the face
- Causes a form of blepharitis that can be challenging to differentiate from dry eye based on symptoms alone
- Potentially impacts the pilosebaceous glands (D. folliculorum) and Meibomian glands (D. brevis)
Requires not only basic lid hygiene but also acaricidal therapy

7
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
OSD “BUCKETS”
Anterior basement membrane disease (Other hereditary corneal dystrophies - H18.59)
Conjunctivochalasis (H11.823)
Pinguecula (H11.153)
Pterygium(Unspecified pterygium - H11.053)
OSD “BUCKETS”
Allergic conjunctivitis (Other chronic allergic conjunctivitis - H10.45)
Recurrent erosion of cornea (H18.83-)
Dermatochalasis (H02.83-)
Epiphora due to insufficient drainage (H04.223)
Stenosis of lacrimal punctum(H04.563)
STEP #4
IMPLEMENT APPROPRIATE THERAPY
FOR MLCE

8
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
Dry Eye Disease Diagnosis & Classification
TFOS DEWS II
TFOS DEWS II
STEP THERAPIES
Patient education
Environmental modification (humidifiers, etc.)
Dietary modifications (including EFA supplements)
Identification/elimination of contributory medications
Lid hygiene and warm compresses (home therapy)
Ocular lubricants

9
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
LID HYGIENE:MECHANICAL BLEPHAROEXFOLIATION
Induction therapy for blepharitis; removes margin debris & deposits
- Scurf & collarettes
- CD (Demodex)
- Meibomian gland caps
- Biofilm (?)
Performed q3-6 months for patients with chronic blepharitis
BlephEx
LidPro (Mibo Medical Group)
OCULAR LUBRICANTS
Proactive artificial tear recommendations based on prevailing etiology and individual need
- As noted in the report… “if MGD is present, then consider lipid-containing supplements”
- Other considerations should include:
Viscosity and/or gel-forming capability
Ophthalmic ointments
Osmolarity
Preservatives
WHEN SHOULD I USE A
PRESERVATIVE-FREE PRODUCT?
Even mild or transient preservatives can have a negative impact on the ocular surface when used excessively and/or long-term.
Patients using drops more than four times a day EVERY day should likely be on a PF formulation.
Also consider for:
- Patients with atopic disease
- Patients using concurrent chronic care drops (e.g. glaucoma)
- Patients with persistent epithelial disruption (i.e. staining)

10
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
WHEN SHOULD I USE A
GEL-DROP OR GEL PRODUCT?
Increasing viscosity helps to extend the residence time of a solution on the ocular surface.
Patients who report improved symptoms but limited duration of action with typical ATs may benefit from a gel or gel-drop.
The limiting factor of increased viscosity is diminished acuity, or increased BLUR.
ALWAYS sample a gel or gel-drop in-office to assess vision if it is to be used during waking hours.
Some also prefer to use a gel or gel-drop QHS.
- Questionable efficacy, as these will not last 6-8 hours.
WHEN SHOULD I USE A
LIPID-EMULSION PRODUCT?
Since the normal tear film contains a lipid component, it is rarely “wrong” to use a lipid-emulsion product.
Lipid-emulsions are specifically INDICATED for patients with evaporative dry eye due to MGD.
- Help to restore lipid component of tears.
- Increase lubricity of ocular surface; reduce “drag” of lid.
- May help to partially dissolve coalesced oils at MG orifices.
As with gels, the limiting factor when using a lipid-emulsion product is diminished acuity, or increased BLUR.
WHEN SHOULD I USE AN
OPHTHALMIC OINTMENT?
Ointments are most commonly used for patients with nocturnal lagophthalmos, QHS.
- Far greater retention time than gels.
- Far greater tendency for blur / reduced acuity.
Ointments may be necessary for patients with severe ocular surface disease (e.g. keratoconjunctivitis sicca) who have exhausted all other options for increased viscosity ATs.
Personal observation without a shred of scientific evidence… Older patients tend to tolerate ointments and gels

11
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
STEP THERAPIES
If above options are inadequate consider
Non-preserved ocular lubricants
Tea tree oil for Demodex
Tear conservation
- Punctal occlusion
- Moisture chamber goggles
Overnight treatments (ointments, etc.)
In-office, physical heating and expression of the meibomian glands
• Prescription drugs to manage DED
• Topical antibiotic or AB/steroid
• Topical corticosteroid (short-term)
• Topical secretagogues
• Topical cyclosporine
• Topical lifitegrast
• Oral macrolide or tetracycline ABs
TEA TREE OIL FOR DEMODEXIN-OFFICE TREATMENT
“One can prepare a mixture of 50% tea tree oil by diluting the tea tree oil in either macadamia or walnut oil…”
IN-OFFICE TEA TREE OIL TREATMENT
Oust Demodex Swabstix
- 50% Tea Tree Oil / 40% Sea Buckthorn Oil / 10% Caprylic Acid

12
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
TEA TREE OIL FOR DEMODEXCLIRADEX WITH T4O
T40 represents one of the 13 essential oils in TTO
- Found to be the most demodicidalof components
- MORE effective than TTO at equivalent percentages
No other commercially available source of T4O in the United States
Tighe S, Ying-Ying G, Tseng CG. Terpinen-4-ol is the most active ingredient of tea tree oil to kill Demodex mites. TranslVis SciTechnol. 2013 Nov;2(7):1-8.
ORAL IVERMECTIN FOR DEMODEX
STROMECTOL (Merck & Company)
- Antihelminthic agent; typically prescribed for parasitic disorders such as strongyloidiasis or onchocerciasis
- Demodex therapy = two 200-mcg/kg doses given 7 days apart
e.g. for a 165-pound adult, five 3-mg tablets at the time of diagnosis, and an identical dose to one week later.
- Most common side-effects include: nausea, diarrhea, dizziness and pruritus (all <3%)
Holzchuh FG, Hida RY, Moscovici BK, et al. Clinical treatment of ocular Demodex folliculorum by systemic ivermectin. Am J Ophthalmol. 2011
Jun;151(6):1030-1034.e1.

13
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
PUNCTAL OCCLUSION
Earliest “plugs” were developed in the 1970’s
Peak utilization through the late 1990’s- Declining 3rd party reimbursement in 2000’s saw a drop-off
- Original Delphi Panel (2006) and original DEWS report (2007) suggested that punctal occlusion was most appropriate for moderate-severe dry eye (Level 3)
TFOS DEWS II suggests EARLIER use of punctal occlusion (Step 2)
Newer materials may offer better, safer options
PUNCTAL OCCLUSION
Jehangir N, Bever G, Mahmood SM, Moshirfar M. Comprehensive Review of the Literature on Existing Punctal Plugs for the Management of Dry Eye
Disease. J Ophthalmol. 2016;2016:9312340.
PUNCTAL OCCLUSIONWHEN TO CONSIDER…
Dry eye associated with a rapid tear break-up time
Aqueous-deficient dry eye secondary to systemic disease (e.g. Sjögren syndrome)
Systemic medications that reduce tear production (e.g. antihistamines, antidepressants)
Symptomatic contact lens wear
Dry eye related to refractive surgery
Lid closure abnormalities
Corneal irregularities or scarring that affects tear stability
Toxic epitheliopathy
Superior limbic keratoconjunctivitis
Jones L, Downie LE, Korb D, et al. TFOS DEWS II Management and Therapy Report. Ocul Surf. 2017 Jul;15(3):575-628.

14
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
PRESCRIPTION DRUGSConsider in those patients who:- Fall primarily into the “aqueous deficient bucket”
- No longer have adequate control of symptoms with artificial tears alone
- Have positive evidence of inflammation (e.g. InflammaDry)
Demonstrate persistent ocular surface damage (NaFl or LG staining)
- Have concurrent systemic disorders that may be contributory (e.g. RA, SS)
Cyclosporin A 0.05% emulsion (Restasis & Restasis Multidose)- FDA-approved in 2003
- Indicated “to increase tear production in patients whose tear production is presumed to be suppressed due to ocular inflammation associated with keratoconjunctivitis sicca”
Lifitegrast 5% (Xiidra)- FDA-approved in 2016
- Indicated “for the treatment of the signs and symptoms of dry eye disease”
RESTASIS
Cyclosporine 0.05% emulsion
Allergan (Irvine, CA)
Approved for BID dosing
“… did not increase tear production in patients using anti-inflammatory eye drops or tear duct plugs.”
10-28-2016: FDA approval for RESTASIS® Multi-Dose Preservative-Free (MDPF).
CYCLOSPORINE A - MOA
Calcineurin inhibitor
Blocks transcription of cytokine genes in activated T-cells
Ultimately blocks production of IL-2
- Diminishes subsequent T-cell proliferation and activation
“… its precise mechanism of action in dry eye is unknown.”

15
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
CYCLOSPORINE A - MOA
Actions in OSD:
Reduction of activated T-lymphocytes
Reduced markers of conjunctival apoptosis (CD40, CD40L and Fas)
Reduction of pro-inflammatory cytokines (IL-6)
Beneficial effect on conjunctival epithelium
- Normalization of conjunctival squamous metaplasia
- Increase in goblet cell density (191%)
Increased tear production (Schirmer)
* 0.005% ophthalmic emulsion
* In HUMAN (in vivo) clinical trials
* After 6 months of treatment
• Donnenfeld E, Pflugfelder SC. Topical ophthalmic cyclosporine: pharmacology and clinical uses. Surv Ophthalmol. 2009;54(3):321-38.
• Kunert KS, Tisdale AS, Gipson IK. Goblet cell numbers and epithelial proliferation in the conjunctiva of patients with dry eye syndrome treated with cyclosporine. Arch Ophthalmol. 2002;120(3):330-7.
• Brignole F, Pisella PJ, De Saint Jean M, et al. Flow cytometric analysis of inflammatory markers in KCS: 6-month treatment with topical cyclosporin A. Invest OphthalmolVis Sci. 2001;42(1):90-5.
• Sall K, Stevenson OD, Mundorf TK, et al. CsA Phase 3 Study Group. Two multicenter, randomized studies of the efficacy and safety of cyclosporine ophthalmic emulsion in moderate to severe dry eye disease. Ophthalmology. 2000;107(4):631-9.
XIIDRA
Lifitegrast 5% solution
Shire (Waltham, MA)
Approved for BID dosing
LIFITEGRAST - MOAActivation and migration of free lymphocytes to the ocular surface are key steps in the inflammatory process associated with dry eye disease
This process is initiated and influenced by the binding of the T-cell integrin lymphocyte function antigen-1 (LFA-1) to intercellular adhesion molecule-1 (ICAM-1).
Lifitegrast acts as an ICAM-1 decoy; it prevents the binding of LFA-1 with ICAM-1 on the inflamed epithelial cell surface.
Activation and homing of T-cells is prevented.
The cycle of T-cell mediated inflammation on the ocular surface is broken.
1. Expression2. Recruitment
3. Activation4. Release

16
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
LIFITEGRAST CLINICAL TRIALS
Four 12-week clinical trials
- Total of 2,133 patients
12-month safety study
- 331 patients
Co-primary endpoints
- Eye dryness score (symptom)
- Inferior NaFl corneal staining (sign)
CLINICAL RESULTS – SYMPTOMS & SIGNS
O
P
U
S
-
1
O
P
U
S
-
2
O
P
U
S
-
3
SAFETY / ADVERSE EVENTSRESTASIS
• One of the safest chronic-use ophthalmic drugs available
• Notable AEs
• Stinging upon instillation: 17% (10%)
• Delayed onset of action
XIIDRA
• Good safety in Phase 2 & Phase 3 clinical studies (OPUS / SONATA)
• Notable AEs (5-25%):• Instillation site irritation (burning)
• Blurred vision (on instillation)
• Dysgeusia (taste alteration)

17
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
OTX-101 A/K/A SECIERA (SUN PHARMA)
Described as a “nanomicellar cyclosporine solution for topical ophthalmic administration”
- Nanomicelles - self-assembling, nano-sized (particle size ≤500 nm) colloidal dispersions with a hydrophobic core and hydrophilic shell... used as carriers for solubilizing hydrophobic drugs.
- Helps to improve tissue penetration of drugs, enhance and sustain drug levels, and reduce systemic side effects
Completed Phase 3 clinical trials; filed NDA in late 2017
STEP THERAPIES
If above options are inadequate consider
Oral secretagogues
Autologous/allogenic serum eye drops
Therapeutic contact lens options- Soft bandage lenses
- Rigid scleral lenses
ORAL SECRETAGOGUES
Options:- Pilocarpine (Salagen)
- Cevimeline (Evoxac)
Action: - Cholinergic parasympatheticomimetic agonists
- Bind to muscarinic (M1 and/or M3) receptors causing pharmacological stimulation of exocrine glands
- Primarily affect the salivary and lacrimal glands; also causes smooth muscle contraction
Specifically indicated for the treatment of xerostomia (dry mouth) in patients with Sjögren syndrome- Technically off-label for dry eye
- Ideally used only under a rheumatologist or internist’s supervision

18
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
ORAL SECRETAGOGUES
Common side-effects include:
- Excessive sweating
- GI irritation, nausea, vomiting, diarrhea
- Rhinitis
- Excessive salivation, salivary gland enlargement
- Miosis, headache
- Bradycardia, tremor
Severe reactions can include:
- Arrhythmias, AV block
- Severe hypotension
- Bronchospasm
INCREASED TEAR SECRETION VIA ELECTRICAL IMPULSE
TrueTear (Allergan)
- Formerly Oculeve
- Described as a “non-surgical, non-pharmaceutical, externally applied device” that employs “neurostimulation of the trigeminal nerve” to increase tear volume
- Rechargeable, hand-held unit
- Disposable hydrogel tip
FDA-cleared in April 2017
Good candidates are “at least 22 years old and have dry eye from inadequate tear production”.
Robinson M, Lewis RA, Sierra P. Intranasal lacrimal neurostimulation versus two control applications for acute tear production inmoderate to severe dry eye. American Academy of Optometry 2016. Anaheim, CA.

19
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
Robinson M, Lewis RA, Sierra P. Intranasal lacrimal neurostimulation versus two control applications for acute tear production inmoderate to severe dry eye. American Academy of Optometry 2016. Anaheim, CA.
Robinson M, Lewis RA, Sierra P. Intranasal lacrimal neurostimulation versus two control applications for acute tear production inmoderate to severe dry eye. American Academy of Optometry 2016. Anaheim, CA.
Robinson M, Lewis RA, Sierra P. Intranasal lacrimal neurostimulation versus two control applications for acute tear production inmoderate to severe dry eye. American Academy of Optometry 2016. Anaheim, CA.

20
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
Prospective, 6-month, open-label, single-arm, non-randomized study
40 subjects with mild-severe DED
4 subjects were concurrently using topical cyclosporine (Restasis) BID
Provided intranasal stimulation device to be used at home QID (or more as needed)
Follow-up assessments at Days 7, 14, 30, 60, 90 and 180.
Outcome measures – EFFICACY:
1° - mean Schirmer score (under topical anesthesia), unstimulated vs. stimulated (with CTA)
2° - ocular surface staining, TBUT, and subject-assessment of DED symptoms and severity
Outcome measures – SAFETY:
1° - AEs
2° - CDVA, IOP, SLE, DFE
Friedman NJ, Butron K, Robledo N, Loudin J, Baba SN, Chayet A. A nonrandomized, open-label study to evaluate the effect of nasal stimulation on tear
production in subjects with dry eye disease. Clin Ophthalmol. 2016 May 4;10:795-804.
Friedman NJ, Butron K, Robledo N, Loudin J, Baba SN, Chayet A. A nonrandomized, open-label study to evaluate the effect of nasal stimulation on tear
production in subjects with dry eye disease. Clin Ophthalmol. 2016 May 4;10:795-804.
Friedman NJ, Butron K, Robledo N, Loudin J, Baba SN, Chayet A. A nonrandomized, open-label study to evaluate the effect of nasal stimulation on tear
production in subjects with dry eye disease. Clin Ophthalmol. 2016 May 4;10:795-804.

21
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
Friedman NJ, Butron K, Robledo N, Loudin J, Baba SN, Chayet A. A nonrandomized, open-label study to evaluate the effect of nasal stimulation on tear
production in subjects with dry eye disease. Clin Ophthalmol. 2016 May 4;10:795-804.
Friedman NJ, Butron K, Robledo N, Loudin J, Baba SN, Chayet A. A nonrandomized, open-label study to evaluate the effect of nasal stimulation on tear
production in subjects with dry eye disease. Clin Ophthalmol. 2016 May 4;10:795-804.
AUTOLOGOUS SERUM EYE DROPS
Autologous: - (cells or tissues) obtained from the host
individual
Serum:- protein-rich liquid that remains when
cellular blood components are removed
Features:- patient-specific
- hypoallergenic
- non-preserved
- 20% - 50% concentration
- frozen / ~1 wk after opening
- typically dosed q2hKabat AG. Customized Solutions for the Dry Eye Patient.
Review of Optometry. 2015 Oct. 152(10):100-8.

22
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
AUTOLOGOUS SERUM EYE DROPS
Mangan R, Lehman S. How (and Why) to Make Autologous Serum. Review of Optometry. 2012 Mar. 40(3):42-54.

23
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
ALLOGENIC SERUM EYE DROPS
Elate-Ocular™
Cambium Medical Technologies; Atlanta, GA- “… a pro-regenerative allogeneic (not autologous) human platelet-derived
topical ophthalmic product intended for use in treating the symptoms of chronic dry eye…”
- “… formulated from the novel processing of base human platelets sourced from healthy and generally younger eligible donors (versus patients) from U.S. blood collection centers.”
IND (investigational new drug application) filed in August 2017
Currently proceeding with Phase 1 / Phase 2 clinical trial
STEP THERAPIES
If above options are inadequate consider
Topical corticosteroid for longer duration
Amniotic membrane grafts
Surgical punctal occlusion
Other surgical approaches (e.g. tarsorrhaphy, salivary gland transplantation)

24
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
AMNIOTIC MEMBRANE THERAPY
May be indicated for corneal complications associated with severe dry eye disease, i.e.- Filamentary keratitis
- Persistent epithelial defects
Mechanism(s) of action:- Biological bandage
- Carrier for ex vivo expansion of corneal epithelial cells
- Substrate (basement membrane) transplant
- Promoter of epithelialization
- Suppressor of inflammation*
- Inhibitor of scarring*
- Inhibitor of angiogenesis*
- Anti-microbial agent*
Dua HS, Gomes JA, King AJ, Maharajan VS. The amniotic membrane in ophthalmology. Surv Ophthalmol. 2004 Jan-Feb;49(1):51-77.
AMNIOTIC MEMBRANE THERAPY
CORNEA• Persistent epithelial defects
and perforations
• Neurotrophic keratitis
• Limbal stem cell deficiency
• Pseudophakic bullous keratopathy
• Infectious keratitis
• Chemical burns
CONJUNCTIVA• Pterygium surgery
• Conjunctivochalasis surgery
• Tumor excision and reconstruction
• Symblepharon prevention
• Chemical burns
• Stevens-Johnson syndrome
• Glaucoma filtering surgery

25
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
AMNIOTIC MEMBRANE THERAPY
Cryopreserved:- PROKERA® (BioTissue)
PROKERA® Slim, PROKERA® PLUS, PROKERA® CLEAR
Dried / dehydrated: - AmbioDisk (Katena/IOP Ophthalmics) –
9, 12, 15 mm
- AmnioTek-C (ISP Surgical) –
12 mm
- aril (Blythe Medical) –
5, 8, 10.5, 15 mm
- BioDOptix® (BioD) –
9, 12, 15 mm
- Eclipse (Ophthalogix) –
10, 12, 14, 16 mm
- ReNovo Oculus (RegenMed Group) –
12 mm
- VisiDisc (Skye Biologics) –
10, 12, 15 mm
- Others… ?
AMT: CLINICAL SCIENCE
AMT: CRYOPRESERVED OR DEHYDRATEDIs one really BETTER than the other?
Other considerations:
- Ease of use
- Patient comfort
Courtesy: YouTube & Dr. Derek Cunningham, Austin, TX Courtesy: YouTube & Dr. Peter J. Cass, Beaumont, TX

26
OSD IS NOT A FOUR-LETTER WORD!
Alan G. Kabat, OD, PA. 2018. All rights reserved.
AMT: SOONER OR LATER?
~1.5M on Rx
Past or Present
Mild
Dry EyeSevere
Dry Eye
Moderate
Dry EyeCurrent AMT UseIdeal AMT Use
• Complete diffuse staining
• Severe inflammation
• Severe symptoms or is neurotrophic
• Severe fluctuating vision
• Every other therapy has failed
• “Trainwreck”
• Some staining (25%)
• Some inflammation
• Some fluctuating vision
• May have pain & symptoms
• 1-2 top-line therapies have failed
• Is already on Restasis/Xiidra
Questions? Email me at: [email protected]

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
1 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Memphis, Tennessee
Promotional Speaker: OCuSOFT
Shire
Clinical Researcher: Bio-Tissue
Shire
Vmax Vision
Editorial Boards: Optometric Office (FVMG)
Optometric Physician (Jobson)
Review of Optometry (Jobson)
Advisory Boards: Avellino Labs
Bruder
EyeGate Pharma
OCuSOFT
Shire
Sun Ophthalmics
TearScience
Vmax Vision
Clinical Consultant: Bio-Tissue
Lacrivera
Vmax Vision
Per COPE stipulations, all disclosed financial relationships are current to within 12 months of this speaking engagement… July 7, 2018.

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
2 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Allergic
Infectious viral
bacterial
parasitic
Inflammatory
Papulosquamous
DERMATOLOGY:
CATEGORIES & ETIOLOGIES
Hyperplastic
Neoplastic benign
pre-malignant
malignant
A = Asymmetry
B = Bordersb = bleeding
C = Colorc = circulation
D = Diameter
E = Evolving…

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
3 Alan G. Kabat, OD, PA. 2017. All rights reserved.
AKA: acrochordon, “skin tag” or skin polyp
A small, benign, usually pedunculated (stalked) tissue growth, varying in size from ~2-5 mm may be skin colored or hyperpigmented
round to oval; may be multilobular
non-infectious (unlike viral papillomas)
More commonly noted in obese individuals; may be associated with pregnancy, diabetes
Most frequently noted in skin folds – neck, axillae, eyelid canthi or adnexa
Usually asymptomatic; painful only if inflamed or irritated

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
4 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Lesions are treated only if they display bleeding or irritation, pose a significant cosmetic concern or interfere with function (e.g. lid ptosis)
Treatment options include: Cryotherapy with liquid nitrogen
Surgical removal: may be removed via ◦ Surgical scissors or shavebox
◦ Electrodessication and curettage
Chemical cautery (trichloroacetic acid)

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
5 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Most common benign tumor of the elderly
Proliferation of epidermal cells
Frequently occur in sunlight-exposed areas
Presentation: Well-circumscribed, rough-surfaced round or oval
lesions with uneven pigmentation
Flat or slightly elevated in early stages
Later becomes dome shaped and more wart-like with a “stuck-on” quality
◦ “barnacles of aging”
Ocular: typically affect the upper lids & adnexa

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
6 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Medical therapy: Superficial lesions can be treated with
trichloracetic acid
Cryotherapy carries risk of pigmentary changes & scarring
Surgical removal is the treatment of choice; options include: Shave biopsy (smaller lesions)
Light curettage, electrodesiccation, or a combination of the two (larger lesions)
Laser & dermabrasion surgery have also be used with some success
AKA: solar keratosis
Most common sun-related growth
Usually occur in fair-skinned individuals (who burn easily and tan poorly) with occupations or hobbies that expose them to excessive UV exposure
May be a precursor of squamous cell carcinoma
Presentation:
chiefly found on the sun-exposed areas of the face, ears, forearms, hands, back, chest, or shoulders
multiple discrete, slightly elevated, scaly reddish-brown lesions; may present with central ulceration
usually 3-10 mm in diameter and gradually enlarge

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
7 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Patient education regarding sun exposure
Medical therapy (FDA approved):
Fluorouracil 5% (Efudex®)
Imiquimod 5% (Aldara®)
Diclofenac 1% gel (Voltaren®)
PDT with δ-aminolevulinic acid(Levulan®)
Other options include chemical peels or dermabrasion
Residual lesions treated surgically
BEFORE DAY 14 DAY 30
• Facial lesions: BID for 3-4 weeks
• For other body sites: BID for 6-8 weeks

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
8 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Most common malignant skin tumor
Predominant in elderly, fair-skinned individuals
Chronic sun exposure = significant risk factor
Slowly progressive & rarely metastatic
Presentation:
translucent, raised nodule with "pearly" margins; over time, telangiectatic vessels may develop
ulceration may occur at the lesion's center
Morpheaform variety lies under surface – very difficult to assess
Photo courtesy of Dr. Mike Dufek (Miami, FL)

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
9 Alan G. Kabat, OD, PA. 2017. All rights reserved.
PREVALENCE OF ANATOMIC LOCATION:
OCULAR BCC
Accounts for <10% of all basal cell carcinomas
Presents as a firm, pale, waxy yellow plaque with indistinct borders
More aggressive and invasive despite being less obvious
More likely to show recurrence

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
10 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Biopsy is CRITICAL!
Treatment of choice is surgical:
Wide margin excision with frozen border section
◦ 3 mm for clearly defined lesions (Nemet et al, AJO 8/06)
Mohs micrographic surgery
Exenteration only in extreme cases
Cryotherapy, radiation, or chemotherapy for those unable or unwilling to undergo surgery
much lower rates of success
Aldara (imiquimod) has shown promise with smaller, non-aggressive BCC
Less common than basal cell carcinoma (5-10%)
Predominant in elderly, fair-skinned, sun-exposed individuals
May convert from benign lesions (e.g., actinic keratosis)
Slightly more aggressive than BCC
low rate of metastasis
Characteristic appearance:
a roughened, scaly patch, mildly elevated and red
may have crusted and/or bloody margins
patients describe the lesion as “a scab that won’t heal”

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
11 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Management for squamous cell carcinoma is identical to that for BCC. Excisional biopsy
Mohs surgical technique
Realize that SCC is somewhat more aggressive than BCC, with greater propensity for: Perineural invasion
Metastasis
Recurrence

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
12 Alan G. Kabat, OD, PA. 2017. All rights reserved.
7th most common cancer in the U.S.
Significant tendency toward growth & metastasis… Melanoma is responsible for 75% of skin cancer deaths in
the United States.
Primary risk factors:
1. Changing nevus
2. Increased age (> 60 years)
3. Large numbers of moles (common acquired and atypical) or history of multiple, atypical moles
4. Fair complexion
5. Family history of melanoma
6. Geographic location in sunny climates

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
13 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Any suspected melanomas should be IMMEDIATELY referred for biopsy… Exceedingly high incidence of metastasis and rapid
rate of growth
Most potentially life-threatening of all skin cancers
Management for melanoma is identical to that for BCC. Excisional biopsy
Mohs surgical technique
papulo- :
Papule – a small solid elevation of skin, generally < 5 mm in diameter
-squamous : Denoting a tendency to scale or exfoliate; a
condition that results in “flaking”

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
14 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Idiopathic disorder of the sebaceous glands affects forehead, cheeks, chin, nose, and eyelids
more common in older patients, women, those with fair skin (i.e. Northern European descent)
Presentation: General: erythema (“skin flushing”),
telangiectasia, coarseness of skin (may result in rhinophyma or “WC Fields nose”), and inflammatory papulopustular eruptions resembling acne
Ocular: chronic, unrelenting blepharitis, thickened lid margins and meibomian stasis; may see secondary conjunctivitis, hordeola/chalazia, canalicultis
1. ERYTHEMATOTELANGIECTATIC
2. PAPULOPUSTULAR ROSACEA
3. PHYMATOUS (RHINOPHYMA)
4. OCULAR ROSACEA
.

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
15 Alan G. Kabat, OD, PA. 2017. All rights reserved.

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
16 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Recognize and avoid triggers!
Dietary:
Hot drinks (coffee, tea, soup)
Alcohol
Spicy foods
Environmental:
Excessive UV or heat
Smoking
Stress
Medical therapy: Tetracycline (250-500 mg daily-tid), doxycycline (50-100
mg daily-bid) or minocycline (100 mg daily) X 2-4 mos. ◦ Remember drug interactions and side-effects
Topical metronidazole as adjuvant to systemic therapy Topical and systemic corticosteroids are contraindicated Courses of isotretinoin (Accutane™) 0.5-1 mg/kg/d for 4
months may be helpful for recalcitrant disease
Soolantra
Mirvaso
Rhofade
Surgical Care: permanent telangiectasias and rhinophyma may be treated by electrosurgery, laser, or dermabrasion

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
17 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Lid hygiene – ??
CONSIDER DEMODEX!!
Copious lubrication (lipid-restorative products)
Topical medications: Corticosteroids – ??
Restasis® (cyclosporine 0.05%) – ??
Remember – topical therapy is palliative; systemic treatment is warranted

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
18 Alan G. Kabat, OD, PA. 2017. All rights reserved.
A papulosquamous disorder of the sebum-rich areas of the scalp, face, and trunk may be linked to Pityrosporum ovale (a yeast)
induced/aggravated by humidity, trauma, seasonal changes, emotional stress
Intermittent, active phases with burning, scaling & itching, alternating with inactive periods increased activity in winter and early spring
Manifestations range from mild dandruff to exfoliative erythroderma; occurs as “cradle cap” in infants
seborrheic dermatitis

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
19 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Dandruff often responds to frequent shampooing Keratolytics - salicylic acid, tar, selenium sulfide & zinc
Antifungals - ketoconazole (helps reduce P. ovale reservoirs)
Medicated shampoos may be used on scalp, body lesions and in beards, but not other facial skin or eyelids
Medical therapy: Topical antifungals - 2% ketoconazole cream
Topical steroids are discouraged except for short-term use, as they may hasten recurrences & foster dependence
Topical immunosuppressants - tacrolimus or pimecrolimus(OFF-LABEL) in recalcitrant cases
Systemic, low-dose isotretinoin in the most severe cases
◦ 10 mg po qod◦ de Souza Leão Kamamoto et al. Low-dose oral isotretinoin for moderate to severe seborrhea and seborrheic
dermatitis: a randomized comparative trial. Int J Dermatol. 2017 Jan;56(1):80-85.
Lid hygiene is paramount!
Lid scrubs are appropriate
Warm compresses and lubrication therapy may help further alleviate symptoms
Other agents:
Dandruff shampoos, etc. for scalp and body should NOT be used in the eyes, but should be advised for concurrent areas of seborrhea
Ketoconazole for blepharitis is controversial…

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
20 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Hyperproliferation of epidermal keratinocytes
Unknown etiology; activated T-cells identified
Exacerbations triggered by trauma, stress, alcohol, medications, and infection
Presentation:
Scaly, “silvery” plaques with underlying erythema
Obvious on scalp, joints (elbows, wrists), extremities
Psoriatic arthritis: stiffness & pain in the distal joints
Ocular findings can include blepharitis, conjunctivitis, nodular episcleritis and even uveitis
Symptoms: itching, generalized discomfort; painful ulcerations can result from scratching

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
21 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Non-invasive therapy includes daily sun exposure, sea bathing, topical moisturizers, and relaxation.
Medical therapy: Topical coal tar or salicylic acid compounds Topical anthralin (Anthralin®, Psoriatec®)
Topical calcipotriene (Dovonex®, a vitamin D analog)
Topical corticosteroids (e.g. Aristocort®, Diprolene®)
◦ Systemic corticosteroids are generally ineffective and may exacerbate the disease
Ultraviolet light treatment (PUVA) In severe cases retinoids (e.g. Tazorac®), methotrexate,
cyclosporine, and hydroxyurea may be used
IV/IM biologics: Infliximab (Remicade)
◦ physician administered (infusion)
Adalimumab (Humira)
Etanercept (Enbrel)
Ustekinumab (Stelara)
Secukinumab (Cosentyx)
Ixekizumab (Taltz)
Oral medications:
Apremilast (Otezla)

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
22 Alan G. Kabat, OD, PA. 2017. All rights reserved.
AKA: “wart”
Benign proliferations of skin and mucosa caused by human papilloma virus (HPV) transmitted by direct or indirect contact
can affect any area on the skin and mucous membranes; often seen on hands, feet
may be variably pigmented or flesh-colored with keratinized surface; “black dots” are pathognomonic
Presentation: two main types Verruca plana – round, flat-topped and slightly elevated with
a granular surface appearance
Verruca digitata – “cauliflower” surface appearance on stalk of varying length; may have numerous finger-like projections

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
23 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Treatment is difficult, though verruca often resolve spontaneously (~65% over 2 years)
Options include: Benign neglect
Topical salicylic acid preparations (Compound-W®)
Vesicants (cantharidin*, podophyllin)
Other agents include imiquimod (Aldara®), cidofovir, tretinoin, and 5-fluorouracil.
Surgical removal:
◦ Chemocautery with trichloroacetic acid
◦ Cryoablation (liquid nitrogen) or photoablation
◦ Electrodesiccation and curettage
◦ Surgical paring / excision
* Moed L, Shwayder TA, Chang MW. Cantharidin revisited: a blistering defense of an ancient medicine. Arch Dermatol 2001;137(10):1357-60.

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
24 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Associated with a large DNA poxvirus
More commonly seen in children
In adults, disease may be sexually transmitted
Presentation:
multiple raised papules or pustules with umbilicated centers; filled with a cheese-like material
typically affects the trunk, hands, face, & lid margins
when sexually transmitted, affects genitalia, thighs, buttocks and peri-anal regions
Usually asymptomatic; may cause itching or tenderness in some individuals
follicular response seen in extreme cases

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
25 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Self-limited, typically resolving spontaneously over 3-12 months; however, to prevent autoinoculation or transmission to close contacts, therapy may be beneficial.
Medical therapy (all are off-label): Topical vesicants (e.g. cantharidin, podophyllin)
Topical retinoids (e.g. tretinoin [Retin-A])
Topical imiquimod
Surgical management: Chemical cautery via trichloracetic acid, tincture of iodine, or
silver nitrate
Cryotherapy with liquid nitrogen
Laser photoablation

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
26 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Definition: a hereditary predisposition to allergy or hypersensitivity
Affects ~3-12% of the population
Manifestations:
dermatitis, urticaria
asthma, rhinoconjunctivitis, etc.
Caused by inappropriate cellular immune response; Type I (a.k.a. IMMEDIATE) hypersensitivity reaction
AKA: atopic eczema
Focal manifestation of a systemic condition
Presentation: Erythema, scaling, lichenification, pigmentary changes
Typically affects the “skin crease areas” – antecubital & popliteal areas, corners of the mouth, neck, behind the ears, outer canthi, or eyelids
Ocular: blepharitis, atopic keratoconjunctivitis (AKC), papillary conjunctival reaction, Trantas dots (limbal deposits of eosinophils), atopic cataracts, and keratoconus.
Symptoms: pruritis (itching) & discomfort AKC often presents with ocular pain and lacrimation
DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
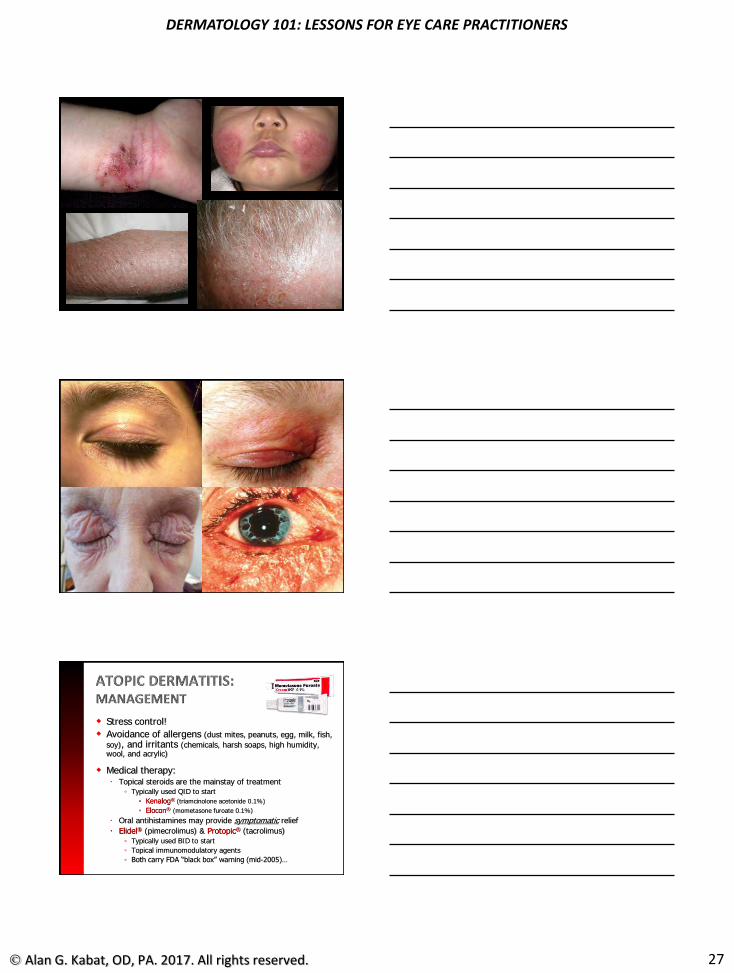
27 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Stress control!
Avoidance of allergens (dust mites, peanuts, egg, milk, fish,
soy), and irritants (chemicals, harsh soaps, high humidity, wool, and acrylic)
Medical therapy: Topical steroids are the mainstay of treatment
◦ Typically used QID to start
◦ Kenalog® (triamcinolone acetonide 0.1%)
◦ Elocon® (mometasone furoate 0.1%)
Oral antihistamines may provide symptomatic relief
Elidel® (pimecrolimus) & Protopic® (tacrolimus)
◦ Typically used BID to start
◦ Topical immunomodulatory agents
◦ Both carry FDA “black box” warning (mid-2005)…

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
28 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Results from direct skin exposure to allergens or other irritants, e.g.
acids, alkalis, resins, or other chemicals; dyes, plants, preservatives, cosmetics, metals; excessive moisture
Type IV (a.k.a. DELAYED) hypersensitivity
Presentation:
Erythema, edema, exudative vesicles; may result in crusting, eczema, or lichenification if not treated
Ocular: eyelid edema & induration, conjunctival edema & hyperemia, papillary response
Symptoms: profound itching, lacrimation

DERMATOLOGY 101: LESSONS FOR EYE CARE PRACTITIONERS
29 Alan G. Kabat, OD, PA. 2017. All rights reserved.
Remove the offending agent!
Avoid harsh soaps and detergents, irritating fabrics and chronic scratching
Medical treatment:
conservative use of topical steroids
wet saline compresses to exudative lesions
oral antihistamines for control of itching
oral steroids only if control of symptoms with topical treatment is not sufficient

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 1
Michael Chaglasian, OD, FAAOChief of Staff, Illinois Eye Institute
Associate Professor, Illinois College of Optometry
Consultant: Reichert, Carl Zeiss Meditec,
Advisory Boards:Aerie, Allergan, Alcon/Novartis, Bausch+Lomb
Research Grants:Topcon
New IOP Monitoring and Measuring:Senimed TriggerFishiCare HomeOcular Response AnalayzerCorneal Hysteresis
New Medications:VyzultaRhopressaRoclatan
Drug Delivery:Bitmatoprost Ring
Travoprost
Progression AnalysisPerimetry
OCT

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 2
2 minutes from 6 IOP measures in one yr
Out of 525,600 min in one year
IOVS 2003
Arsani S, Zeimer R, Wilensky J, et al. Large diurnal fluctuations in intraocular pressure are an independent risk factor in patients with glaucoma. J Glaucoma. 2000;9:134‐142.
1
5.76
0
1
2
3
4
5
6
7
Diurnal IOP Range 3.11 mm Hg Diurnal IOP Range 5.4 mm HG
Relative Risk of Disease
Progression
5-6x GreaterRisk

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 3
“Glaucoma is a 24‐h disease and the absence of individual patient data on circadian IOP dynamics constitutes a gaping deficit in our knowledge.Recent studies have demonstrated the feasibility of A‐IOP‐M. It can be expected that it will become part of the routine diagnostic evaluation of glaucoma patients by 2020.”
Curr Opin Ophthalmol 2015, 26:214–220
A new measurement principle – Ocular Volume Change
IOP exerts force on the eye shell, leading to ocular volume changes. Sensing through the ocular shell is influenced by ocular biomechanics; Tissue elasticity an individual variable.
pressure
strain gauge
contact lens
tissue biomechanics
The first ever FDA approved Contact Lens Sensor system, March 2016
Automated recording of Ocular Volume Changes (OVC) over 24 hours
Proven safe system
Repeatable 24 hour profiles
Individual signature‐like profiles
Highly sensitive
Patient‐ & practitioner‐independent
Promising clinical benefits
SENSIMED Triggerfish®

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 4
Potential Roles: (need further investigation)
OVC as a new biomarker to PREDICT the course of the disease vs. just monitoring the progression
OVC as a CLASSIFIER for Glaucoma patients having normal pressure (NTG)
OVC as a new and additional endpoint to assess the EFFECTIVENESS OF INTERVENTION
HOWEVER, THERE ARE LIMITED DIRECT COMPARISONS BETWEEN VOLUME CHANGE AND IOP
Predicting those who are at highest risk for progression is important
Being able to predict the risk of progression in advance of that progression having occurred (above a particular threshold) for each patient would help us move away from the current “wait and see routines”
Being able to predict in advance future progression rate would help drive earlier and more objective decisions around performing surgical intervention on higher risk patients.
De Moraes et al., 2016
Parameters associated with faster MD change at P < 0.25 were the:• number of large peaks while awake, • mean peak ratio while asleep, • mean peak ratio while awake, • wake‐to‐sleep slope and,• variability from the mean while awake.

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 5
Interpretation of CLS results remains a challenge. At present, the main value of CLS measurements seems to be in documenting relative changes of IOP‐related events and their timing.
Medication effects on IOP may not be as observable due to less effect on the 24 hour rhythm
Currently Sensimed is still investigating and exploring the appropriate business model and clinical utilization for the US
FDA Approved , but not currently available
Mansouri, Weinreb. Curr Opin Ophthalmol 2015, 26:214–220
Potential Roles:
Early Detection
Individualized Therapy
Alternative Interventions
Improved Adherence
Mansouri, Weinreb. Swiss Med Wkly. 2012;142:w13545
http://icare‐usa.com/
March 2017

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 6
The Icare® HOME tonometer is a handheld, battery operated device that measures intraocular pressure (IOP) without the need for topical anesthetic.
The device is intended as an adjunct for monitoring IOP of adult patients (self‐use). The HOME tonometer is designed for use at home or on the go.
IOP, date, time, eye recognition (right/left) and measurement quality are all stored in the internal memory.
Patient cannot view IOP readings
Data is transferred to a PC for further analysis by the prescribing physician.
New features: positioning light, automatic eye recognition system, series or single measurements, new user interface panel.

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 7
1. Asrani S, Chaterjee A, Wallace DK, et al. Evaluation of the ICare rebound tonometer as a home intraocular pressure monitoring device. J Glaucoma. 2011
2. Halkiadakis I, Stratos A, Stergiopoulos G, et al. Evaluation of iCare‐ONE rebound tonometer as a self‐measuring intraocular pressure device in normal subjects. Graefes Arch Clin ExpOphthalmol. 2012
3. Rosentreter A, Jablonski KS, Mellein AC, et al. A new rebound tonometer for home monitoring of intraocular pressure. Graefes Arch Clin Exp Ophthalmol. 2011
4. Sakamoto M, Kanamori A, Fujihara M, et al. Assessment of iCare ONE rebound tonometer for self‐measuring intraocular pressure. Acta Ophthalmol. 2014
Potential Areas of Error:1. Rebound tonometry may be less accurate in the higher
IOP range (>23mm Hg)
2. Overestimation with increasing CCT
Munkwitz S, Elkarmouty A, Hoffman EM, et al. Comparison of the ICare rebound tonometer and the Goldmann applanationtonometer over a wide IOP range. Graefes Arch Clin ExpOphthalmol. 2008Rosentreter A, Jablonski KS, Mellein AC, et al. A new rebound tonometer for home monitoring of intraocular pressure. Graefes Arch Clin Exp Ophthalmol. 2011
No significant safety issues reported for the Icare® TA01i or ic100 tonometers with a large number sold worldwide (40,000+) and in the United States (11,000+)
In use by health care personnel with varying degrees of tonometer experience and some of which have little or no ophthalmic training.
No significant safety issues reported for the Icare® HOME tonometer or its predecessor, Icare ONE; over 2,000 tonometers in use worldwide
Majority in Europe after Icare ONE received CE mark in late 2009 and was introduced in 2010.
171 patients 10 (6%) stopped b/c of difficulty in using the device27 (16%) unable to achieve certification
HOME and GAT were within 5 mmHg
116 of 127 patients (92%)MD of ‐0.33 mmHg (SD 3 mmHg)
No corneal abrasions or adverse events
Ophthalmology 2016;123:1675‐1684

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 8
Glaucoma suspects and ocular hypertensives prior to initiating treatmentGlaucoma patients disease progression and in office IOP that is at or near target IOP goalsStable glaucoma patients with high risk factors for progressionPatients with poor compliance where additional IOP information may demonstrate critical need for laser or surgical procedurePatients who would benefit from having additional IOP information
iCare Home is available for purchase nowThere is no CPT code (not reimbursable)
Fee is charged to patient for use of device over a three to five (5) day period
Practitioner and Staff are trained and “Certified”
Patient is selected and is trained in office.Approximately 10‐20 minutes
Patient uses device at home for 3 Days5‐6 readings per day
Patient returns device to office. Linkage to software to download the data.
Reviewed with patient.
Adjustment to treatment plan if warranted.

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 9
Data Interpretation:Highest Peak IOP out of office?Higher Mean IOP?Highest Fluctuation of IOP?
Are there good clinical indicators for this test?What about “environmental” factors?Will it improve medication compliance?
Taking Glaucoma risk assessment to the next level:
THE ROLE OF CORNEAL HYSTERESIS
Ocular Response Analyzer
(Reichert)
Michael Chaglasian, ODIllinois Eye Institute Illinois College of [email protected]
1. Glass DH et al. Invest Ophthalmol Vis Sci. 2008;49:3919‐3926.2. Wells AP et al. Invest Ophthalmol Vis Sci. 2008;49:3262‐32683. Taylor DA et al. Corneal Biomechanics. In: Copeland RA Jr., Afshari NA, eds.: Copeland and Afshari’s Principles and Practice of
Cornea. Two Volume Cornea Textbook. Jaypee Brothers. 2012:148‐157.
Section 1: Introduction to Corneal HysteresisBioengineering of the Eye: Emerging Concepts
Viscoelastic tissue with complex, interconnected microstructure1
Geometrical attributes are not a surrogate for biomechanical properties1
• eg: CCT does not describe viscoelasticity
The eye appears to be a mechanical structural continuum2
• Tissue properties may provide additional diagnostic information3
27
©2002 Park et al. Invest Ophthalmol Vis Sci.

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 10
1. Vincent J. Basic elasticity and viscoelasticity. In: Vincent J, ed. Structural Biomaterials. 3rd ed. Princeton, NJ: Princeton University Press; 2012:1‐28.
2. PubMed Search for “hysteresis” on October 3, 2014 returned 7696 results. 3. Hjortdal JO1. On the biomechanical properties of the cornea with particular reference to refractive surgery. Acta Ophthalmol Scand Suppl.
1998;(225):1‐23.
Section 1: Introduction to Corneal HysteresisHysteresis: Not a New Concept
A measurement that characterizes response to application and removal of force (load/unload)1
• Found in materials or systems that do not instantly follow forces applied to them but react slowly, or
dissipate a portion of the applied energy 1
More than 7500 papers published on hysteresis in a variety of medical fields2
• Various tissues and structures (tendon, lung, arteries, etc)
• The importance of Corneal visco‐elasticity had been discussed and explored (EX‐VIVO)prior to the ORA3
28
Classic “Hysteresis Loop”Sir James Alfred Ewing Identified the phenomenonof hysteresis and coined theterm in 1890
Hysteresis Property:“More like a Shock Absorberand NOT just a Coil Spring”
1. Luce DA. J Cataract Refract Surg. 2005;31:156‐162.2. Dupps WJ Jr. J Cataract Refract Surg. 2007;33:1499‐1501.3. Glass DH et al. Invest Ophthalmol Vis Sci. 2008;49:3919‐3926.
Section 1: Introduction to Corneal Hysteresis What is Corneal Hysteresis (CH)
The only in‐vivo measurement of corneal/ocular biomechanics• CH specifically refers to the output
of the measurement process performed by the Ocular Response Analyzer (ORA)1,2
Corneal Hysteresis reflects the ability of the corneal tissue to dissipate energy 1
• Function of viscoelastic damping2
• Not a characterization of stiffness3
Provides insight into ocular properties that were not previously understood or conceived of
29
Ocular Response Analyzer measurement signal
David Luce, PhDInvented the concept of Corneal Hysteresis
Section 1: Introduction to Corneal Hysteresis CH: Average Values in Normal Subjects
1. Fontes BM J Refract Surg. 2008 Nov;24(9):941-5. 2. Carbonaro. The Heritability of Corneal Hysteresis and Ocular Pulse Amplitude A Twin Study doi:10.1016/j.ophtha.2008.02.0113. Lam A. Et Al. Optom Vis Sci. 2007 Sep;84(9):909-144. Kamiya Et Al. J Refract Surg. 2009 Oct;25(10):888-935. Ortiz Et Al. J Cataract Refract Surg. 2007 Aug;33(8):1371-56. John Et. Al. 2007 Spring;39(1):9-14
CH Values in Normals around the worldN CH*
Brazil1105 10.1 ± 1.8
UK2272 pairs 10.2 ± 1.2
China3125 10.9 ± 1.5
Japan4204 10.2 ± 1.3
Spain588 10.8 ± 1.5
USA6 44 10.5 ± 1.2
*CH units are mmHg

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 11
CH: Risk Factor for Glaucoma
Low CH (<9 mmHg) = Higher Risk
High CH (>12 mmHg) = Lower Risk
Less significant RF contribution:
• CH 9‐12 mmHg
As with any RF, CH alone cannot be considered a definitive indicator of glaucoma, though it may be an indicator for further evaluation particularly in presence of other glaucoma risk factors
Other Related Findings
Corneal hysteresis has been shown to be lower in various types of glaucomatous eyes in comparison to normal eyes; these include POAG, PACG, NTG, and pseudoexfoliative glaucoma.
Low Hysteresis Associated with OAG and Visual Field Asymmetry
• More sensitive than CCT or IOP
Low‐baseline corneal hysteresis is associated with a greatermagnitude of IOP reduction following various glaucoma therapies including topical prostaglandin therapy and SLT.
Prakavan M. J Ophthalmic Vis Res 2014Anand A, et al. Invest Ophthalmol Vis Sci 2010Heirnisis C. Graefes Arch Clin Exp Ophthalmol 2013
Corneal Hysteresis Studies:
CH is repeatable, typically with good correlation R / L
No diurnal variation in normal eyes
Small decrease with age (as with CCT)
• Appears to be valuable to repeat procedure
CH is low with high (>30) IOP
• And may rise after hypotensive therapy
CH is low following LASIK (use IOP cc measure)
CH is low in corneal pathology (Keratconus)
• Neither of these suggest increased risk of glaucoma

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 12
Why is CH relevant in Glaucoma?
34
(Low) CH has been consistently shown to be independently and strongly associated with or
predictive of glaucoma progression
Corneal Hysteresis as a Risk Factor forGlaucoma Progression:
Conclusions:
The CH measurements were significantly associated with risk of glaucoma progression. Eyes with lower CH had faster rates of visual field loss than those with higher CH.
The prospective longitudinal design of this study supports the role of CH as an important factor to be considered in the assessment of the risk of progression in patients with glaucoma.
Ophthalmology 2013;120:1533‐1540
Corneal Hysteresis and Progressive Retinal Nerve Fiber Layer Loss in Glaucoma
CONCLUSIONS:
Lower CH was significantly associated with faster rates of RNFL loss over time.
The prospective longitudinal design of this study provides further evidence that CH is an important factor to be considered in the assessment of the risk of progression in patients with glaucoma.
Am J Ophthalmol 2016

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 13
CH Predicts the Development of Glaucoma
200 Glaucoma Suspects followed for 4 years
2002: Clinical research with ORA commences
2005: The 1st generation ORA was made commercially available
2012: Generation II ORA was launched
3rd Generation “ORA G3” introduced September 2015
Measures:
• Corneal Hysteresis (CH)
• Goldmann‐correlated IOP (IOPg)
• Corneal compensated IOP (IOPCC)
Ocular Response Analyzer Technology
• Becomes a second tonometer for the office.
• Can be used on all patients.
Corneal Compensated IOP: An IOP measurement that is less influenced by corneal properties than Goldmann or other tonometers. This value is closer to the “true pressure” and has been shown to be a better indicator of glaucoma than Goldmann. Matches GAT on average, so numerical “Scale” is the same
Corneal Hysteresis: An indication of corneal biomechanical properties that has been show to be independently predictive of future glaucoma progression. Reimbursable under CPT 92145.Typical average value is 10.5. Typical Range is 8‐14. Low is bad
IOPg: A Goldmann‐correlated IOP measurement for reference purposes so that clinicians can appreciate what a Goldmann would read simultaneously with the IOPcc value above.
Waveform Score: A signal analysis algorithm that rates the “quality” of the measurement signal on a scale of 0‐10. The higher the value, the more reliable the IOP and CH values are. 6‐10 is excellent. 4‐5 is not so good. 3 or below is poor.
Section 4: Ocular Response Analyzer TechnologyInterpretation of measurement values

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 14
IOPcc = Corneal Compensated IOP
40
An IOP measurement that is less influenced by corneal properties than Goldmann or other tonometers.
This value is closer to the “true pressure” and has been shown to be a better indicator of glaucoma than Goldmann.
Matches GAT on average, so numerical “Scale” is the same
In post‐LASIK/refractive surgery and in Corneal Pathology (KC, Fuchs’)
CH is NOT a reliable indicator of glaucoma risk due to modified biomechanics• In these situations there is increased importance of IOPcc
There a need to educate ORA users for correct interpretation of CH values:
Children have significantly higher CH values than adults, which should be taken into consideration when determining glaucoma risk
CH values are artificially low with very high IOP (30+)
41
Special considerations:
Implementing ORA in Clinical Practice:
ORA will NOT replace Goldmann tonometry• Advantageous to have different tonometric devices
Evidenced based guidelines needed for low/medium/high CH values
QUESTIONS:
How often to repeat?
How does the ORA best fit into practice workflow?• Screening room (eg, like an auto‐refractor)
• Or only on select patients?
Where does ORA fit into the measurement process?• Prior to the patient getting into the chair
• Prior to anesthesia (before measurement of CCT)

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 15
How am I using ORA and Corneal Hysteresis?
Obtaining CH on new glaucoma and glaucoma suspects
Using IOPcc on LASIK patients
Obtaining on progressing patients and other potentially high risk patients
Adjusting therapy and management for patients with low CH
Last “new” class of medication to be FDA approved
Timoptic
Betagan
Trusopt (1995)
Alphagan 0.2%
Pilocarpine
Argon Laser
No OCT
Fundus CamerasPolaroid or 35mm slide
Encouraged “drawing” ONH
Humphrey PerimeterSTATPAC but No True Progression Analysis
No Randomized Clinical Trial data had been published
OHTS, EMGT, AGIS, CNTGSG

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 16
Cosopt
Lumigan 0.03%; 0.01%
Travatan; Travatan Z
Alphagan P 0.1%
Azopt
Combigan
Simbrinza
Zioptan(preservative free PGA)
Cosopt PF
No new mechanism of action (MOA)*
*Rescula (unoprostone) 2000 and 2012. Likely activity on BK channels in TM
VyzultaTM
Latanoprostene bunod
FDA Approved, Available NOW
RhopressaTM
Netarusdil
Approved, available now
RoclatanTM
Netarusdil + latanoprostPossibly in 2019
Latanoprostene bunod is a dual mechanism, dual pathway molecule, consisting of latanoprost acid, linked to an Nitric Oxide‐donating moiety, which enhances trabecular meshwork/Schlemm’s canal (conventional) outflow by inducing cytoskeletal relaxation.
Latanoprost plus nitric oxide (NO)
Kaufman, P. EXPERT OPINION ON PHARMACOTHERAPY, 2017

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 17
Latanoprostenelatanoprost
Increases uveoscleraloutflow
Bunod donates Nitric Oxide (NO)Exerts its effect in trabecular smooth muscle
Resulting in trabecular relaxationand increased conventional outflow
Cavet ME, et al. Invest Ophthalmol Vis Sci. 2014;55(8):5005-5015. Ellis DZ, et al. Invest Ophthalmol Vis Sci. 2009;50(4):1808-1813.
Nitric Oxide may have other therapeutic roles in the eye and optic nerve
Latanoprostene = latanoprostIncreases uveoscleral outflow
Bunod donates Nitric Oxide (NO)Exerts its effect in trabecular smooth muscle
Resulting in trabecular relaxation and increased conventional outflow
NO may have other therapeutic roles in the eye and optic nerve
Cavet ME, et al. Invest Ophthalmol Vis Sci. 2014;55(8):5005-5015. Ellis DZ, et al. Invest Ophthalmol Vis Sci. 2009;50(4):1808-1813.
Kang JH, et al. JAMA Ophthalmol. 2016;134(3):294-303.
Diet
Nitrate (NO3- ) Nitric oxide (NO )Nitrite (NO2- )
Bacterial enzymesin mouth
Enzymatic and nonenzymatic reactions in our blood and tissues
Study Design: Assess the relation between dietary nitrate and new glaucoma cases (63,893 females and 41,094 males)
Lowest quintile of nitrate intake (~80 mg/d) compared with the highest quintile (~240 mg/d)
Result:Participants consuming the highest amounts of nitrates from green leafy vegetables had a 44% reduced relative risk of POAG with early paracentral vision loss and a 21% lower relative risk of all POAG

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 18
Study designRandomized (2:1 [LBN:timolol]) phase 3, multicenter, double‐masked, parallel‐group studies
2 treatment groupsLBN, 0.024%, qhs for 3 months
Timolol, 0.5%, bid for 3 months
Weinreb RN, et al. Ophthalmology. 2016;123(5):965-973.
APOLLO LUNAR
Number of subjects* 420 387
Mean baseline IOPLBN Timolol
26.7 mm Hg26.5 mm Hg
26.6 mm Hg26.4 mm Hg
Weinreb RN, et al. Br J Ophthalmol. 2015;99(6):738-745.

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 19
Nocturnal IOP with latanoprostenebunod treatment was 2.5 mmHg lower than baseline
Liu J et al Am J Ophthalmol 2016;
Liu J et al Am J Ophthalmol 2016;
LBN had higher OPP
Not included on FDA labeling
Latanoprost with New MOA with Nitric Oxide of improving TM outflow
More effective (~1.23 mmHg) than latanoprost
7.5‐9.1 mmHg lower IOP
Side EffectsConj. Hyperemia= 6%

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 20
First Line TherapyAlternate/Replacement for latanoprost/PGA
Good for all? Better for those with more advanced disease? Better for those with lower IOP?
Switch/Adjunctive TherapyWhen small additional IOP is needed, advantage of maintaining single bottle therapy
PGA w/ adjunctive med and not @ targetSwitch to LBN w/ adjunctive
No data on adjunctive therapy role
Rhopressa.com

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 21
Netarsudil ‐ MOA:1. ROCK causes alteration of cellular components of
the trabecular meshwork and Schlemm’s canal;rho kinase inhibitors decrease resistance in the trabecular meshwork outflow pathway and promote reduction of IOP.
2. ROCK inhibition lowers EVP
3. NET inhibition lowers AH production
Lin, et al Discovery and Preclinical Development of Netarsudil, a Novel Ocular Hypotensive Agent for the Treatment of Glaucoma. J Ocul Pharmacol Ther. 2017
Ciliary Processes
CORNEA
Uveoscleral Outflow
NET
RKI
Trabecular Meshwork
Episcleral Veins
Schlemm’s Canal
NET
RKI
Rhopressa (Netarsudil): An Investigational Drug Candidate for Glaucoma
THREE IOP LOWERING MECHANISMS:
1. ROCK inhibition relaxes TM1, increases outflow1,2
2. ROCK inhibition lowers Episcleral Venous Pressure (EVP)3
3. NET inhibition reduces AH production2
1. Wang SK, Chang RT. Clin Ophthal 2014;8:883-890.2. Wang RF, Williamson JE, Kopczynski C, Serle JB. J Glaucoma 2015. 24(1):51-54. 3. Kiel JW, Kopczynski C. J Ocul Pharmacol Ther 2015; 31:146–151.
Rhopressa™ QD met the criteria for non‐inferiority to timolol BID for the primary efficacy analysis(forbaselineIOP<25, <27 and<28mmHg
Mean IOP Reduction ~ 3.9 ‐ 4.1 mmHg

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 22
The three studies demonstrated up to 5 mmHg reductions in IOP for subjects treated with RHOPRESSA 0.02% once daily in the evening.
For patients with baseline IOP < 25 mmHg, the IOP reductions with RHOPRESSA 0.02% dosed once daily were similar to those with timolol 0.5% dosed twice daily.
For patients with baseline IOP equal to or above 25 mmHg, however, RHOPRESSA 0.02% resulted in smaller mean IOP reductions at the morning time points than timolol 0.5% for study visits on Days 43 and 90;
the difference in mean IOP reduction between the two treatment groups was as high as 3 mmHg, favoring timolol.
Conjunctival Hemorrhagesporadic sub‐conjunctival petechiae
Cornea Verticillataasymptomatic non‐toxic lipid deposits
only visible via biomicroscopy evaluation
Instillation Site Painsame incidence as timolol
transient
Corneal Verticillatafrom amiodarone

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 23
Potential drug of choice as adjunctive therapy to PGAswhen additional IOP lowering is desiredAdjunctive studies have NOT been completed
Rhopressa™ Advantages
Efficacy vs. other adjunctive therapies
QD PM dose
Lack of serious and systemic drug‐related AE’s
• Long duration of medication delivery• 3 to 6 months or more
• Obviously compliance benefits
• Good safety profiles thus far
• Good efficacy compared to drop therapy
• Retention for some devices may be a challenge
• Injection delivery for other devices is a hurdle

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 24
Large silicon ring that sits in the fornix
Visible @ medial canthus
Helps identify ring
Sustained drug delivery for 6 months
20% IOP reduction at all time points in clinical trials
Slightly less than timololBID
PGA continuous dose effect
High Retention Rate93% @ 3 months
88% @ 6 monthsMinimal Discomfort
Side Effects:Ring:
Increased mucous in AM
Medication:Hyperemia, etc.
Phase 3 Trials continue
Unclear how it will be marketed, Rx’d
http://www.sec.gov/Archives/edgar/data/850693/000119312514254394/d750005dex992.htm
• No Topical SEs• 7‐9 mmHg IOP
reduction• Phase 3 Trials now

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 25
Visual Field Testing
Remains an essential exam component.In fact, indications for more frequent testing on patients.
Recent papers have suggested that the 24‐2 test pattern has limited ability to detect central field defects
50% of retinal ganglion cells are found within 4.5mm of fovea
Macula region comprises only 10% of overall visual field area though it is responsible for 60% of area of visual cortex
Damage to central 100 associated with diminished contrast sensitivity, reduced reading ability
24‐2 Pattern on Retinal SurfaceVF testing under samples the macula. Possibility of small defects going undetected

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 26
12 testLocations6 deg sep
64 testLocations2 deg sep
24‐2 10‐2

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 27
Good Test Takers, Younger patients
Minimal to no defects on 24‐2
OCT Macula/Ganglion Cell scan is abnormal
High Risk Patients
Perhaps good idea as part of baseline for many suspects and ocular hypertensives
Alternate with 24‐2More frequent VFs when possible

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 28
Is disease present ?
How bad is it ?
Is it getting worse?
Case example of “early”,normal‐tension glaucoma.
The optic nerve photograph shows thinning of the inferior optic nerve neuroretinal rim (A) with a superior paracentral visual field defect (B).
SD‐OCT imaging confirms corresponding inferior RNFL thinning seen both on the thickness map and quadrant thickness (C) and inferotemporal macular thinning of the ganglion cell and inner plexiform layers (D).RNFL
RNFLGCA
Is my patient getting worse?
How can I tell for certain?Variability in perimetric testing
Challenges of structural assessment
Newer Question:What is the rate of progression?
Can we quantify this?

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 29
Baseline exams.Establishes initial visual field status.
VFI Rate of Progression Analysis.
• Trend Analysis of patients
overall visual field history
Today’s Visual Field. • Complete report of
current visual field exam
including PD, VFI,
progression analysis and
GPA Alert.
Detecting progression remains one of the most difficult tasks in glaucoma Mx
One Example:It can be hard to distinguish disease progression from exam variability and/or aging changes
There is no consensus on the best technique or criteria to detect progression, or what amount would be clinically significant.
Research and Literature does not easily translate into daily clinical care.
Progression may be measured by:
Functional change in visual field; structural change in the optic disc or retinal nerve fiber layer; or combined functional and structural change.
Accomplished through clinical examination, ophthalmoscopy, threshold perimetry, and imaging.

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 30
Most patients with glaucoma do progress if monitored for a long enough time
Even with IOP in the “normal range”59% of treated patients in EMGT (Leske et al 2007)
Treatment regimens should parallel the rate of patient’s progression
Slow progressors (majority) may need minimal intervention to maintain a high QoL
Rapid progressors (minority, ~20%) often require substantially more aggressive IOP reduction
Caprioli J. AJO 2008
Avg. rate = ‐1.0 dB/yr~30 yrs to perimetric blindness
HighTG = ‐1.31 dB/yr
NormalTG = ‐0.36
ExfoliativeG = ‐3.13~10 yrs to p. blindness
Heijl Ophthalmology 2009;116:2271–2276

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 31
MD = ‐4 dB MD = ‐13 dB MD = ‐29 dB
Mean Deviation
HAP Staging Scale: 0 to ‐6 dB = Early‐6 to ‐12dB = Moderate
> ‐12 = Severe
‐1 dB ‐5 dB ‐25 dB5 Years IOP = 44 mmHg
~ ‐5 dB/yr
Some rates of progression put patient at risk of visual disability
Most do not follow this path
Estimated ~ 17% of patient (even under care)
Fast Rates of Progression =
‐> 0.5 ‐ 1.0 dB per year or higher (varies w/age)However, slower rates in younger patients are still at risk due to longer life with disease
Luke J. Saunders, Felipe A. Medeiros, Robert N. Weinreb & Linda M. Zangwill (2016) What rates of glaucoma progression are clinically significant?, Expert Review of Ophthalmology, 11:3, 227-234, DOI: 10.1080/17469899.2016.1180246

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 32
Average 50 yo pt. @ ‐0.6 dB/year
20 years to ‐12dBdefined as severe VF
17 more yrs to ‐22dBdefined as “statutory blindness”
70 yrs
87 yrs*assumes a linear rate of progression
60 yo @ ‐1dB/yrStarting at ‐10dB
At 80 yrs =
90 yo @ ‐1 dB/yrStarting @ ‐2 dB
At 100 yrs+

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 33
Ophthalmology 2013;120:512–519
Ophthalmology 2013;120:512–519
Detecting Visual Field Progression in Glaucoma
Factors Impacting Progression Measure• Long Term Fluctuation• Reliability• Confirmatory Testing
• Ability to Efficiently Review the Data

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 34
Baseline Exams
Visual Field Index
Most Recent Test
The VFI Bar• historical and
projected VFI loss
Loss to date
Projected future loss100%
Arch Ophthalmol. 2009;127(12):1610‐1615
Event analysis‐ compares baseline to most recent data; change as dictated by criteria has occurred or not.
Trend analysis‐ looks at the significance of rate of change over time.
Identifies progression by looking at patient behavior over time. Uses all data points and a linear regression formula
Weakness‐ progression is not necessarily linear
Event analysis and trend analysis are complementary.Without event analysis, we have no early detection of glaucoma or early detection of progression in patients having glaucoma diagnoses. Without rate analysis, we have no ability to decide if detected changes are clinically significant.

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 35
Trend Analysis“Measures the rate of change”
A regression line is drawn to determine rate of change for all the data that has been collected over time.
Using VFImeasures a % rate of change
Most valuable when multiple VF tests have been completed
Good for identifying fast progressors
Baseline
Most Recent Exam
‐1.1%
EventAnalysis
What Rate of Loss is Significant?Greater than: ~1‐1.5%/yr (vary w/age, loss at Dx, etc.)
‐0.1% ‐1.4%

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 36
Stable cases = <0.3 dB/year
Progressive cases= >0.9 dB/year (“catastrophic”)
Consider doing 3 fields in first year and one every 6 months the next year
At a total of 5 in 2 years, good identification of the catastrophically worsening patient
Then scale back to 1 per year
Many already known to be generally stable don’t need this intensity
Important: Change Baseline Exams

Glaucoma Update: New Tools 2018
Michael Chaglasian, OD 37
Event AnalysisAsks “Has this changed”, compared to baseline an appearance on consectutive tests
Point by Point basis
Mostly used in early follow up time period
But also helpful in middle and late stages
Good for slow progressors
Look for shaded triangles indicating a single point that is worsening over consecutive tests
Point By Point Progression Analysis• Shows which point have progressed from baseline
Event Progression Analysis
GPA Summary Report:
Trend Line looks okay,Event Analysisis NOT!
‐1.0%


Ocular Emergencies
M. Chaglasian, OD 1
Ocular Emergencies for the Primary Care Optometrist
Michael Chaglasian, OD, FAAOAssociate ProfessorIllinois Eye Institute
Illinois College of [email protected]
Disclosure
No relevent disclosures for this presentation.
What is a “True” Emergency?
Pain (vs. discomfort)
Current or potential for:
Vision loss
Structural damage
Needs immediate (same day) attention

Ocular Emergencies
M. Chaglasian, OD 2
“True” Emergency
History is key to differentiating emergency versus urgency Phone or in person
Proper triage is essential
After hours protocol
Your office and your specialists
Medico-legal implications
History
Vision
One or both eyes?
Visual field
Sudden or gradual
Blurred or lost?
Diplopia?
Mono or Bino
Pain
Redness
Onset
Trauma
Contact lenses
Recent ocular disease or surgery
Other diseases
cardiac, vascular, or autoimmune
viruses
Medications or recent changes to medications
Nausea/vomiting
Emergency Exam
Acuity
Visual fields
Pupils
Ocular Motility
External examination
SLE
IOP
Fundus exam

Ocular Emergencies
M. Chaglasian, OD 3
Emergency Kit
Eye shield
Pressure patch
Sterile eye wash
Alger brush
Forceps
Golf spud
pH paper
Bandage CL’s
Diamox
Topical drops
Antibiotics
NSAID’s
Steroids
Cycloplegics
“True” Emergency
Chemical Burns
Alkaline
Central Retinal Artery Occlusion
Both have extremely high risk of severe and permanent vision loss which can be prevented via immediate intervention and treatment
Chemical Trauma
Acid exposure Only penetrate through epithelium car battery, vinegar, and
some refrigerants
Alkaline exposure Penetrates tissues more easily and
have a prolonged effect lime, (plaster, cement) lye,
ammonia found in household cleaners, fertilizers, and pesticides
Have patient bring agent if possible

Ocular Emergencies
M. Chaglasian, OD 4
Chemical Burns Copious irrigation
anesthetic
speculum
sterile saline v tap water
Contacts can be removed after irrigation
Sweep fornices – repeatedly
Examination after irrigation and neutralization of pH
Debride necrotic tissue
Want neutral pH of 7.0 –check q15min with pH paper
Chemical Burns
Determine area of involvement
Assessed by extent of FL staining
Assess depth of conjunctival penetration
Vascular ischemia, necrosis of limbal and bulbar conjunctiva
Loss of limbal vascular plexus is key indicator to severity of permanent vision loss
Check IOP
Tonopen
IOP meds
Roper Hall Classification of Ocular Burns
Grade Prognosis Limbal Ischemia Corneal Damage
1 Good None Epithelial Damage
2 Good Less than 1/3 Haze but iris detail visible
3 Guarded 1/3‐1/2 Total haze that obscures iris
4 Poor >1/2 Opaque cornea

Ocular Emergencies
M. Chaglasian, OD 5
Alkali Chemical Burn
50 yo CM bricklayer
Mortar splashed in eyes 1 day prior
Went to ER, eyes rinsed, given drops and Augmentin
c/o FBS, OD; OS feels fine
VA: OD HM; OS 20/20-2
pH: 10 OD, 7.4 OS
Alkali Chemical Burn
Needs more irrigation and debridement
Emergency amniotic membrane transplant (AMT)
Chemical Burn Management
Cycloplegic
AB or AB/steroid combo ung
Pain control Cyclo, steroids, NSAIDs
Artificial tears
Pressure patch BCL not tolerated
Oral narcotics/NSAID
Topical sodium ascorbate 10% and Citrate Oral
Doxycycline
Diamox
Tarsorraphy
Glue/permanent
AMT
Limbal stem cell transplant
Uninjured eye - autograft
Close relative – allograft
Corneal transplant
Artificial corneas

Ocular Emergencies
M. Chaglasian, OD 6
Chemical Burn - Ocular Sequelae
Advanced glaucoma
Eyelid destruction
Symblepharon
Cicatricial Entropion - months
Trichiasis
Ectropion
Ankyloblepharon
Descemet membrane detachment
Retinal detachments
Chronic Dry Eye
Persistent epithelial defects/ RCE
Infectious keratitis
Stromalysis
Perforation
Irreversible intraocular damage
Phthisis bulbi
Hypopyon
Amniotic Membrane Transplant (not Bandage)
Used as a surgical graft, where the tissue is integrated into the host. Amniotic membrane provides the scaffold for re-epithelialization.
Amniotic membrane is the innermost layer of the placenta, with 3 layers: Epithelium
thick basement membrane: supports epi call migration and inhibits apoptosis
Avascular stromal matrix: rich in growth factors & protease inhibitors
16. Sippel KC, et al. Amniotic membrane surgery. Curr Opin Ophthalmol 2001;12:269-281
AM applied with epithelial-basement side facing UP, stroma DOWNActs as basement membrane for corneal epithelium to grow over
AMT
When used as a graft, AM is typically glued or sutured in place, and epithelium is expected to grow over it.
AMT has an low immune response, so few rejections
Shown to: 1. epithelialization
2. fibrosis, inflammation, scarring
3. provides an anti-inflammatory and anti-scarring effect that minimizes the buildup of scar tissue
Other uses: Stevens-Johnson syndrome
Bullous /band keratopathy, pterygia
Prevent post-op adhesion of conj/sclera in trabeculectomy

Ocular Emergencies
M. Chaglasian, OD 7
CRAO
Sudden, painless, unilateral loss of vision
(+) APD
Swollen, pale posterior pole
“Cherry red” spot
• Vascular attenuation &/or boxcarring of flow in arteries & veins
• May see an embolus in vessel on optic nerve
CRAO
47yoCF with 3 day h/o blur, OS, with severe loss yesterday
Had been seen twice in previous week
1 MD, 1 OD
Dx: Dry eyes
Tx: Artificial tears
Spoke to tech yesterday
Casual about coming in
OD OS
20/20 Distance Acuity CF 1’
(+) APD
12 TA 12
BP 128/79
WNL SLE WNL
Patient findings

Ocular Emergencies
M. Chaglasian, OD 8
CRAO
In office AC paracentesis & digital massage
ASA
To Cardiologist
Echocardiogram
To ER
Blood work
ESR: rule out Temporal Arteritis
To PCP
Hematology workup
To Retina
Brimonidine Vision Never Improved
CRAO
Echocardiogram
Dilated aortic root
associated with connective tissue dx
Blood work:
ESR: minimally elevated
Elevated homocysteine level
amino acid in blood derived from the digestion of protein-rich foods
Elevated PTT (Partial thromboplastin test)
Other hypercoagulability factors negative
Negative CT, MRI, MRA
CRAO Causes
Emboli
74% cholesterol
10.5% calcific
15.5% platelet-fibrin
Thrombosis
Vasculitis
GCA
Post-trauma
In patients of 70 years of age and older, giant cell arteritis is more likely to be the cause than in younger patients.

Ocular Emergencies
M. Chaglasian, OD 9
CRAO
Incidence
3.5/10,000 in general population
92% of patients have </= CF acuity
Only ~ 8% will experience VA improvement
Two thirds of patients experience 20/400 vision while only one in six will experience 20/40 vision or better.
Risk Factors
Age >40
Systemic conditions
HTN, DM, CV dx, prior MI, stroke, hypercholesterol, hypercoagulable state
Social/Medication history
Smoking
CRAO Testing
ESR & CRP
r/o GCA
CBC/lipid profile
Cardiology referral
risk of MI
Carotid Doppler –r/o emboli from carotid
Auto-immune
Inflammatory
Hematology workup
Coagulopathies
Younger pts
CRAO
Retina suffers no detectable damage up to 97 minutes
BUT sustains massive, irreversible damage after 4 hours
Hayreh SS, Zimmerman MB, Kimura A, et al. Central retinal artery occlusion. Retinal survival time. Exp Eye Res 2004;78:723‐36.

Ocular Emergencies
M. Chaglasian, OD 10
CRAO & Mortality
Patients with emboli have a 56% mortality rate over 9 years, compared to 27% for an age-matched population without emboli
Life expectancy of patients with CRAO is 5.5 years compared to 15.4 years for an age-matched population without CRAO
CRAO – Acute treatment
• Lower IOP• Anterior chamber paracentesis
• remove 0.1 to 0.4 ml of aqueous fluid within the first 24 hours.
• Digital ocular massage• Some use 3‐Mirror Lens
• IOP lowering agents
CRAO – Acute treatment
Move occlusion
Carbon/carbogen inhalation
CO2 dilates arterioles & increases O2 delivery to ischemic tissues
Paper bag – dilate retinal vessel Remove embolus
Local intraarterial fibrinolysis (LIF) was associated with similar visual outcomes but increased rate of adverse reactions when compared to observation in the EAGLE study.
The study did not recommend LIF for acute CRAO.

Ocular Emergencies
M. Chaglasian, OD 11
CRAO
Risk of neovascularization NVD, NVI, NVG
Reports from 2.5-35%
18.2% @ an average of 8.5 weeks post CRAO
Ocular neovascularization following central retinal artery occlusion: prevalence and timing of onset. Eur J Ophthalmol. 2010 Nov‐Dec;20(6):1042‐6.
Urgencies
Giant Cell Arteritis
Endophthalmitis
CRVO
Papilledema
Optic neuritis
Corneal abrasion
Iritis
Corneal ulcer
Penetrating injury
Ruptured globe
Lacerations
Corneal foreign body
Retinal detachment
Orbital cellulitis
Giant Cell Arteritis / Temporal Arteritis

Ocular Emergencies
M. Chaglasian, OD 12
Background on GCA
Giant cell arteritis (GCA) is the most common primary vasculitis in adults.
Histopathologically, GCA is marked by generalized granulomatous inflammation of medium- to large-sized vessels that occurs in the elderly.
Patients commonly note associated symptoms such as headache, jaw claudication, diplopia, myalgias, and constitutional symptoms.
The most commonly feared sequela of GCA is permanent visual loss secondary to arteritic anterior ischemic optic neuropathy (AAION).
Since the vision loss from AAION can progress rapidly, and can involve the fellow eye within a matter of days, GCA is considered an ophthalmologic emergency.
Giant Cell Arteritis / Temporal Arteritis
Inflammation of medium & large sized arteries of the body, restricting blood flow & causing pain
VA loss usually unilateral, but risk of loss in other eye if not treated within 1 week
Elderly (>60), white, female
Scalp tenderness, jaw claudication, HA, loss of appetite, weight loss, fatigue
Need stat ESR & temporal artery biopsy Normal Sed Rate: F= (age+10)/2 M= age/2
GCA Exam Findings
CRAO
AION
Flame hemes, cotton wool spots
Pale, swollen disc
6th nerve palsy

Ocular Emergencies
M. Chaglasian, OD 13
Treatment
High dose systemic steroids
60-100mg qd
IV methylprednisone
250 mg q6h x 3 days
Aspirin
Referrals: Neurology, Rheumatology, Ophthalmology
Temporal Artery Biospy
Color duplex ultrasonography
Ocular Urgencies
Trauma
Penetrating/non-penetrating
Hyphema
Blowout fractures
Ruptured Globe
Lacerations
Corneal Abrasions
Foreign Bodies
Retinal detachment
Orbital Cellulitis
Iritis
Corneal ulcer
Optic neuritis
Acute exophthalmus
Trauma
2,500,000 traumatic eye injuries /yr in US
40,000-60,000 lead to visual loss
40% of all new cases of monocular blindness
80% occur in men
75% are work related
Average age 30
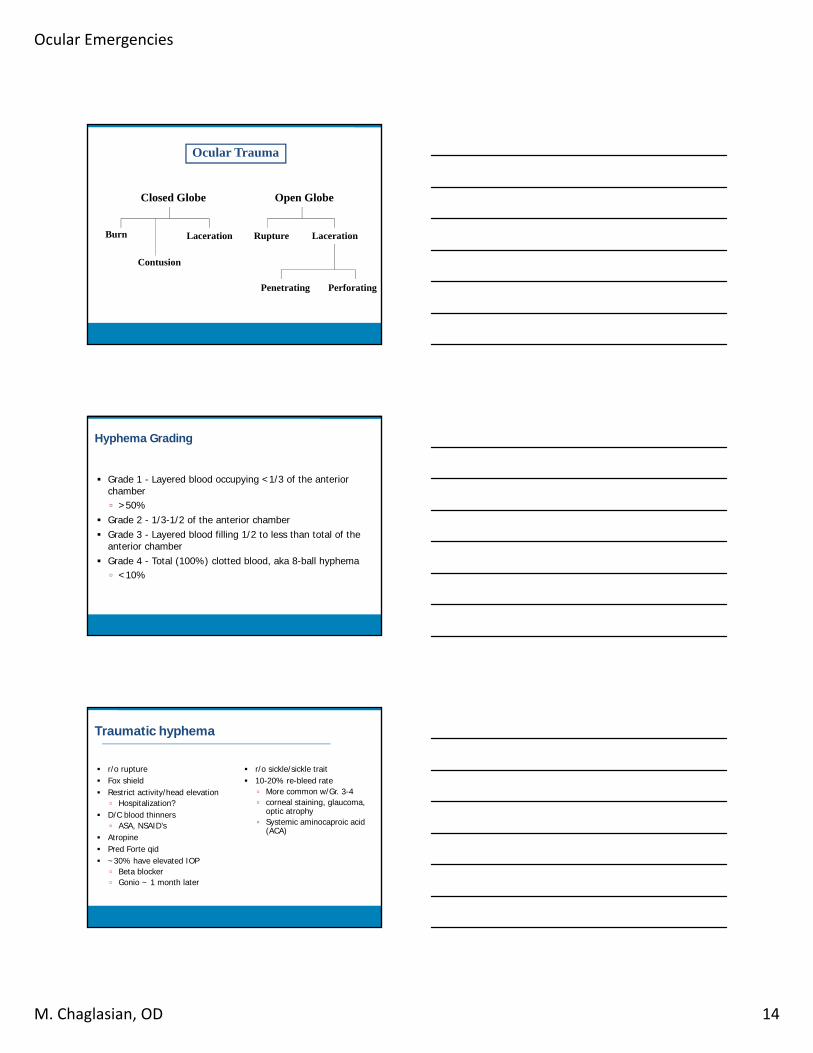
Ocular Emergencies
M. Chaglasian, OD 14
Ocular Trauma
Closed Globe Open Globe
Burn
Contusion
Laceration Laceration
Penetrating Perforating
Rupture
Hyphema Grading
Grade 1 - Layered blood occupying <1/3 of the anterior chamber
>50%
Grade 2 - 1/3-1/2 of the anterior chamber
Grade 3 - Layered blood filling 1/2 to less than total of the anterior chamber
Grade 4 - Total (100%) clotted blood, aka 8-ball hyphema
<10%
Traumatic hyphema
r/o rupture
Fox shield
Restrict activity/head elevation
Hospitalization?
D/C blood thinners
ASA, NSAID’s
Atropine
Pred Forte qid
~30% have elevated IOP
Beta blocker
Gonio ~ 1 month later
r/o sickle/sickle trait
10-20% re-bleed rate
More common w/Gr. 3-4
corneal staining, glaucoma, optic atrophy
Systemic aminocaproic acid (ACA)

Ocular Emergencies
M. Chaglasian, OD 15
Angle Recession
Blunt trauma which causes a hyphema is more likely to also cause an angle recession
Between 2 and 20% of patients with angle recession will go on to develop glaucoma
Traumatic Glaucoma
patients with damage to greater than two-thirds of angle are also more likely to develop glaucoma
glaucoma associated with angle recession may develop months to years following the injury
Glaucoma is related to magnitude of hyphema,
Only 13% get when hyphema is less than half of AC
Bed rest (head elevated) or very limited activity along with patching are usually recommended.
Management
Early Phase Glaucoma and Acute Trauma
Acute Inflammation / Iritis
Hyphema
red blood cells in the anterior chamber
results from a tear in the angle that breaks a blood vessel
rebleeds occur up to 7 days after trauma

Ocular Emergencies
M. Chaglasian, OD 16
Hyphema
Measure the percent of hyphema in AC
Measure the IOP
may have very high IOP
NO gonioscopy,
must wait 7 days to prevent causing a rebleed
Check sickle cell status
Those with SC may need AC wash out
Medications: Early Phase
For Inflammation:
Cycloplegia:
w/ atropine 1% BID, Homatropine 5%
Topical steriods:
prednisolone acetate 1% QID
NO aspirin products: rebleed
Elevated IOP from Hyphema
PGAs:
Not an option for early phase
Good option b/c uveoscleral outflow
Beta Blockers
Timoptic XE, Betagan, etc.
Alphagan
Topical or Oral CAI’s
Cosopt or Combigan= good option
The usual duration of an uncomplicated hyphema is 6 days
Anterior Chamber “Wash Out”

Ocular Emergencies
M. Chaglasian, OD 17
Trauma - Penetrating Injury
If rupture- STOP exam
Fox shield and to hospital for exam under anesthesia
CT if foreign body can’t be seen
Systemic antibiotics
Compromise protective outer layers, increasing the risk of infection
Risk of endophthalmitis
Intraocular contents may be outside the globe
Trauma - Laceration
Corneal
Conjunctival
Lid
Be alert with high velocity injuries for intraocular foreign bodies
Seidel’s sign: (+) full thickness laceration
Corneal Lacerations
Full thickness
protect w/ shield & immediate referral
Partial thickness
treat as abrasion

Ocular Emergencies
M. Chaglasian, OD 18
Corneal Laceration
41yoCM- construction foreman
Nail ricocheted off a wall and hit his OD 1 day prior – felt OK
Today, 5/10 pain, photophobia, FBS
h/o metallic FB 10 ya
Recent tetatnus shot
Corneal Laceration
Va OD: 20/20; OS: 20/25
(+) epi defect
(+) AC rxn
(-) Seidel’s sign
TA 9 mmHg, OU
Lid eversion negative
Fundus exam WNL
+ Ocuflox
+ Cyclogyl
Get CT to r/o intraocular foreign body
Corneal Laceration
1 day follow up, feels 50% better
Va 20/30
No epithelial defect
+ stromal haze
Decrease Ocuflox
Start Pred-Forte

Ocular Emergencies
M. Chaglasian, OD 19
Conjunctival Lacerations
SLE
Subconj heme
(+) Fl stain
DFE
Mild Majority are self-limiting Antibiotic, patch, follow up 1 day
Severe
Antibiotic, patch & refer
Blow Out Fracture
Direct trauma to the globe causes an increase in intra-orbital pressure & decompression via orbital floor fracture
Maxillary bone & posterior medial wall
Periorbital swelling, ecchymosis & restricted eye movement
Diplopia, hypesthesia of cheek & teeth, orbital pain
Most common sign is limited upward or downward gaze due to entrapment of IR or IO
Crepitus
palpate the bony rim of the orbit or lid
small bubbles of air "pop" when compressed.
Management
When should surgical repair of blowout fractures be considered? Fractures with persistent symptoms (typically double vision or pain) are
usually candidates for surgical repair. Timing of the repair varies, but most often is within two weeks of the injury. Initial repair may consist of any of the following:
• exploration of fracture site and repositioning of bone• release of trapped tissue from fracture site• covering of fracture site with synthetic material
What long-term problems may develop following blowout fractures? Most fractures heal without long-term effects. However, strabismus
surgery (eye muscle surgery) is sometimes necessary for persistent double vision. Occasionally, persistent double vision can be treated with non-surgical methods (prism glasses or botulinum toxin injections)

Ocular Emergencies
M. Chaglasian, OD 20
Blow Out Fracture
Ice packs 24-48 hours, no nose blowing
Recovery can be spontaneous - 2-3 days
Systemic antibiotics
Can trigger orbital cellulitis, angle recession glaucoma, & RD.
Prompt surgery if poor cosmesis, persistent diplopia, enophthalmus, pediatric patient with entrapment
Corneal Abrasion
Acute pain & photophobia
May need anesthetic to perform exam
Debride loose epi if necessary
Antibiotic/cycloplegic/NSAID
Pressure patch v. Bandage CL
RCE issues
Corneal Abrasion
44yoCM
CC: Pocked in OS with belt buckle 1 day prior
: S/P PRK OU
(+) FBS, photophobia, redness
Antibiotics Cycloplegic Treat any associated anterior
chamber reaction BCL? Debridement of loose tissue RCE issues Fingernail, paper, fingernail, pre‐existing EBMD

Ocular Emergencies
M. Chaglasian, OD 21
Corneal/Conjunctival Foreign Body
• History important
• ? object
• High speed?
• DFE
• SLE
• Lid eversion
1) Removal:irrigation, moistened cotton swab, spud, needle, forceps, Alger brush
2) Antibiotic/cyclo/patch/BCL
3) Steroids for scar modulation after defect healed
Rhegamatogenous Retinal Detachment
Symptoms: Flashes Vitreous separates from
the retinal pigment epithelium
Floaters Separation at retinal
vessel may leak blood into the vitreous
Decreased VA from macular involvement can lead to severe, permanent vision loss
Separation of neurosensory retina from the underlying RPE, by fluid from the vitreous cavity and into the sub-retinal space.
Time course of retinal break or defect to time of detachment is highly variable and unpredictable
Rhegamatogenous RD
Develop from Retinal Defect:
Hole or Break in sensory retina
Frequently from Posterior Vitreous Detachment (PVD)
Other Forms of Retinal Detachments:
Exudative
Tractional

Ocular Emergencies
M. Chaglasian, OD 22
Retinal Detachment
• 51yo AAM presents to Urgent Care @ IEI• CC: Sudden blurry vision superiorly OS
• x1 week, painless & progressive(-) trauma(-) flashes
• POH: Cataract extraction, OU • LEE: 2 years ago at IEI, no SRx
• PMH: HTN, NIDDM (controlled)
Entrance Examination
• VA sc: OD 20/60+1 PH: 20/60+2• OS 20/50-1 PH: 20/40+2
• Pupils: PERRL 1+APD(OS)
• EOMs: FROM OU
• CVF: FTFC OD• Constricted superiorly OS
Slit-Lamp Examination
OD OS
Adnexa/Lids: 1+ MGD 1+ MGD
Conjunctiva/Sclera: W&Q W&Q
Cornea: Unremarkable Unremarkable
Angles: 4+T/4+N 4+N/4+T
Anterior Chamber: D&Q D&Q
Iris: Unremarkable, (‐)NVI Unremarkable, (‐)NVI
Lens:PCIOL in place, intact,
clearPCIOL in place, intact,
clear
IOP (Goldmann): 14 12
Anterior Vitreous: Unremarkable (+)Shafer’s sign

Ocular Emergencies
M. Chaglasian, OD 23
Rhegmatogenous Retinal Detachment
Patient education:
risk of permanent vision, need for IMMEDIATE retinal referral.
Patient Treatment and Outcome:
RRD Statistics
Prevalence: RRD 10-15/100,000• 70%: Non-Traumatic
• 50% myopic• 1-3D: 4x risk, >3D: 10x risk
• 10% increased risk in fellow eye• 10%: Trauma• 20%: Post-Cataract Surgery
• S/P Cataract Extraction• 10 year risk: 6x risk
• S/P Refractive lens exchange • 2-8% RRD within 1 month
• 20 - 30% have lattice degeneration
SYMPTOMATOLOGY
Often asymptomatic and thus detected on routine examination
Inferior and temporal location from atrophic holes Patients less aware of these slowly progressive RDs as superior and nasal
fields of view are less sensitive
Flashes/Floaters. Yes or No? Not noticed while sleeping Unilateral symptoms often masked Not affecting central vision Slow progression/change Frequent “Red Herring” TIA, acephalgic migraine, PVD w/o detachment PVD Follow Up: 6-8 weeks of exam detection or with increased
symptoms

Ocular Emergencies
M. Chaglasian, OD 24
Key Findings for Referral
Finding a retinal break
Finding subretinal fluid
May not find break, but it’s likely there as that’s how the fluid got in
Other Signs:
Acute PVD
Pigment cells in vitreous or vitreal heme
Techniques to help:
Scleral depression and 3-Mirror retinal exam
OCT
OCT for RD
Use Wide-field Mode
Helpful in Differential diagnosis
Helpful in determining macular status
“on or off”
Treatment
Laser Slit lamp or Laser Indirect Ophthalmoscopy
LIO for more peripheral breaks
For subclinical holes and breaks with limited SRF and areas of contact between the retina and RPE remain
Laser is applied at the border of the attached and detached retina, the photocoagulation creates “seal” that prevent further progression of the break/detachment
Monitor Asymptomatic Breaks?
Low (~5%) risk for progression

Ocular Emergencies
M. Chaglasian, OD 25
Treatment
Pneumatic Retinopexy (62-78%) Oil/Gas bubble with laser
Pars Plana Vitrectomy: small incision Fluid-Air, air-gas exchange, silicone oil injection with
laser
Scleral Buckle: for larger RDs
Thin scleral band placed under conjunctiva to indent sclera towards retina followed by laser or cryotherapy
Decreased in utilization in favor of PPV due to numerous SEs
Clinical Pearls - Urgency
Macula Off Duration Mean Postoperative VA†
≤10 days 20/41
11 days to 6 weeks 20/121
>6 weeks 20/178
Macula On Status Timeframe
Progressive/large Immediate/next day
Stable/small/inferior <5 days
†Scleral buckle repairs
Endophthalmitis
Incidence 0.13%
( review of 215 articles from 1963-2003)
Symptoms:
Pain, decreased vision, photophobia, redness
Signs:
Corneal edema, hypopyon, vitritis,

Ocular Emergencies
M. Chaglasian, OD 26
Endophthalmitis Vitrectomy Study (1995)
420 patients < 6 weeks post CE or 2o IOL c s/s of endophthalmitis
Randomized to +/- systemic antibiotics
Randomized to ParsPlanaVitrectomy (PPV) v AC tap & vitreous injection with antibiotics
Results:
Patients with > LP: Tap and inject (no need for immediate PPV)
Patients with < LP: Immediate PPV, and inject
3 fold increase in the frequency of achieving 20/40 or better acuity
Acute Angle Closure Glaucoma
Classic Symptoms:
Unilateral, painful eye
Blurred vision, halos
Nausea, vomiting
Characteristics:
Older, white, hyperopic females age > 30 yrs
Peak age 55-70
First-degree relative with ACG
History - previous episodes, medications, surgeries, etc.
When can the angle close?

Ocular Emergencies
M. Chaglasian, OD 27
Acute Angle Closure Glaucoma
Symptoms: Pain, halos around lights, redness, nausea, vomiting
Signs: Corneal edema, fixed,oval mid-dilated pupil, ciliaryflush, AC inflammation, glaukomflecken
Extremely elevated IOP
Gonioscopy
Indentation
Both eyes
CLINICAL FEATURES:
Acute Angle Closure Attack:
diffuse conjunctival hyperemia
cloudy, edematous cornea
fixed, oval, mid‐dilated pupil
VA often significantly reduced
IOP ranges 40‐70+ mm Hg
inflammation / aqueous cell/flare
“CLASSIC” PATIENT SYMPTOMS:
These symptoms are associated with “Acute” Angle Closure deep, aching pain (high IOP)
redness, tearing, photophobia
blurred vision, halos (edema)
nausea, vomiting (pain)
Headache
Note:
Many patients do NOT have these symptoms

Ocular Emergencies
M. Chaglasian, OD 28
GONIOSCOPY
Look for PAS (peripheral anterior synechia) as evidence of angle closure
Gonioscopy of both eyes to confirm a narrow angle approach (symmetry)
Only Indentation gonioscopy shows this, not three mirror.
Gonioscopy Lenses Posner 4 mirror
» Handle
Sussman 4 mirror» No handle
» www.ocular-instruments.com
Indentation Gonioscopy
A. = Appositional angle closure
B. = Synechial angle closure

Ocular Emergencies
M. Chaglasian, OD 29
Gonioscopy on the Web!
www.gonioscopy.org
When can the angle close?
Management - Acute Angle Closure Glaucoma
Oral CAI’s (250 - 500 mg Diamox) Tablet form only, not Sequel form Sequel takes too long to act
Topical fixed combination: Combigan / Cosopt Iopidine (if available)
Topical steroids
When IOP < 45, add 1-2% pilocarpine
Definitive Treatment: Laser Peripheral Iridotomy (LPI) Eliminates pupillary block
Prophylactic LPI of fellow eye

Ocular Emergencies
M. Chaglasian, OD 30
Corneal Ulcer
Peripheral vs Central
Infection
Staph, strep, moraxella, pseudomonas
Pain, redness, photophobia
CL wear
Chronic eyelid disease
SLE: focal accummulation of inflammatory cells in excavation with overlying epi defect
Corneal Ulcer
15yoCF
Being treated elsewhere for Corneal ulcer, OS
> 1 week with fortified antibiotics, oral AB’s
SCL wearer
Fell asleep on a road trip
VA sc: OD 20/20, OS 20/400 PH NI
Differential Dx
Infiltrate
Ulcer
Pseudomonas
Fungal
Acanthamoeba

Ocular Emergencies
M. Chaglasian, OD 31
Corneal Ulcer Treatment
Discontinue CL wear
Antibiotic
BESIVANCE (besifloxacin) 0.6%
1 gtt q15minX 2 hrs, then hourly while awake
Cycloplegic
Culture if available, if central, if >3mm
Corneal Ulcer Treatment
Fortified agents?
subconjunctival loading dose injection of 0.3 cc gentamicin mixed with 0.3 cc lidocaine at the time of presentation
Steroids when defect is closed to modulate scarring The SCUT study (Steroids for Corneal Ulcers Trial), a large series
involving 500 patients that was published in the Archives of Ophthalmology, found no overall difference in three-month BSCVA and no safety concerns with adjunctive corticosteroid therapy for bacterial corneal ulcers
If NI, consider fungal or acanthamoeba….
Optic Neuritis
Unilateral, acute loss of vision Women, 20-45yo, AA Strong association with MS The patient’s history may reveal the following signs and symptoms of optic
neuritis: Preceding viral illness Rapidly developing impairment of vision in 1 eye or, less commonly, both
eyes: During an acute attack Dyschromatopsia in the affected eye: Occasionally may be more
prominent than the decreased vision [4]
Retro-orbital or ocular pain: In association with the vision changes and usually exacerbated by eye
movement; the pain may precede vision loss Uhthoff phenomenon, in which vision loss is exacerbated by heat or
exercise

Ocular Emergencies
M. Chaglasian, OD 32
Optic Neuritis: Signs and Symptoms
Varying degrees of vision reduction:
Ranging from a mild decrease in visual acuity to complete vision loss, which is often monocular but can be binocular
scotomas, ocular or orbital pain, worse on EOM’s
(+) APD, color vision & VF loss
Abnormal contrast sensitivity and color vision:
In almost all patients with adult optic neuritis who have decreased visual acuity
Optic Neuritis: Signs and Symptoms
Field defects: May include altitudinal, arcuate, nasal step, central
scotoma, cecocentral scotoma
Initially, the optic nerve head may appear normal.
Papillitis (swollen disc) may be seen in one third of patients with optic neuritis
Evaluation and Workup
Magnetic resonance imaging (MRI) is highly sensitive for and specific in the assessment of inflammatory changes in the optic nerves, and for central nervous system white matter lesions.
MRI also helps to rule out structural lesions.
Labs. Only if other forms of neuritis are possible
Erythrocyte sedimentation rate
Thyroid function tests
Antinuclear antibodies
Angiotensin-converting enzyme
Rapid plasma reagin
Mitochondrial deoxyribonucleic acid (DNA) mutation studies

Ocular Emergencies
M. Chaglasian, OD 33
Management
Visual function begins to improve 1 week to several weeks after onset, even without any treatment
Permanent residual deficits in color vision and contrast and brightness sensitivity are common
Pharmacologic therapy in optic neuritis (ON) is directed at ameliorating the acute symptoms of pain and decreased vision caused by demyelinating inflammation of the nerve; varying regimens of corticosteroids have been used for this purpose.
IV steroids do little to affect the ultimate visual acuity in patients with optic neuritis, but they do speed the rate of recovery;
Some clinicians advocate IV steroids in patients with either severe or bilateral vision loss
Optic Neuritis Treatment Trial
448 pts
Oral placebo, IV steroids with placebo orals, or oral steroids
The primary goal was to determine whether oral or IV steroids altered the visual outcome in patients with acute optic neuritis.
IV steroids accelerated recovery of VA initially, but provides no longterm benefit.
Oral steroids provided no visual benefit and was associated with a higher rate of recurrence.
Initial MRI result, if abnormal with white matter abnormalities, was the single most important predictor of the future risk of MS Routine blood tests of no value
If Possible MS
For patients with optic neuritis whose brain lesions on MRI indicate a high risk of developing clinically definite MS, treatment with immunomodulators:
interferon [INF] beta-1a,
INF beta-1b,
glatiramer acetate
(may be considered)

Ocular Emergencies
M. Chaglasian, OD 34
Papilledema
Bilateral optic nerve head edema, secondary to increased ICP
Decreased acuity may not be presenting symptom
Headache
Need imaging to rule out space occupying lesion
Lumbar tap/CSF studies
Pseudotumor Cerebri - Dx. of exclusion
Central Retinal Vein Occlusion
Non-ischemic v. Ischemic
Ischemic – less common, more severe with poorer prognosis
NVG/NVI
q1month x 6months, q2-3 months x 6 months, q4-6 months x 3 years
Men > 50
<40: Needs systemic workup
antiphospholipid antibody syndrome
Poor acuity, possible APD
Hemes, dilated vessels, CWS, retinal & macula edema
Lower IOP
Neovasculogenesis:
Chronic retinal hypoxia is theorized to initiate the production of an angiogenic substance / vasoproliferative substance which elicits new blood vessel growth.
Vascular Endothelial Growth Factor (VEGF)
Iris tissue is the primary site for developing neovascularization.
Progresses through several stages:

Ocular Emergencies
M. Chaglasian, OD 35
Angle Closure Stage
Time frame for development to this stage:
can be variable, from days to months
NVG is known as the:
"Ninety day glaucoma“, because of its rapid onset
Features:
pain, photophobia
decreased Va
increased IOP, high
conj. congestion
iritis
corneal edema
rubeosis iridis
ectropian uvea
synechial angle closure
First Step= Medical treatment.
Medical therapy is directed at lowering the IOP, reducing the anterior segment inflammation and making the patient more comfortable.
Note the similarities and differences to the management of primary acute angle closure
Rapid IOP Reduction:
Acetazolamide: 250 mg x 2
Beta blocker and Alphagan
Anti-inflammatory:
prednisolone acetate 1%
Atropine 1%
For pain and inflammation
Referral for Avastin and PRP

Ocular Emergencies
M. Chaglasian, OD 36
Central Retinal Vein Occlusion
Prompt referral to PCP
FBS, ESR, CBC, lipid profile, FTA-ABS
Strong association with HTN, DM, POAG
Check BP and IOP in office
Hyperlipidemia, hyperviscosity
Macula edema treatment:
Avastin
Ozurdex
Kenalog
PRP
Orbital Cellulitis
Usually results from spread of infection from paranasal sinuses
CT
ENT consult
Tx with IV antibiotics
Must distinguish from Preseptal
Both present with lid edema, pain, redness
FEVER
PROPTOSIS
PRECIPITATING EVENT
ANY AGE, SEX, RACE
Patient “Emergencies”
Ocular Migraine
Redness/itching/burning/discharge
Subconjunctival hemorrhage
Gradual change in visual acuity
Lid bumps (non- painful)
Refractive changes

Ocular Emergencies
M. Chaglasian, OD 37
Take Home Message
Be prepared
Have appropriate equipment/ referrals in place
Take the time to train your staff
You are ultimately responsible
Be methodical in your thinking & your examination
Know when it’s OK to treat, and when you must refer
Thank you!
Related Documents











