Copyright @ 2009 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited. ORIGINAL ARTICLE Sarcolemmal Neuronal Nitric Oxide Synthase Defect in Limb-Girdle Muscular Dystrophy: An Adverse Modulating Factor in the Disease Course? Marina Fanin, PhD, Elisabetta Tasca, PhD, Anna Chiara Nascimbeni, PhD, and Corrado Angelini, MD Abstract Reduction of neuronal nitric oxide synthase (nNOS) has been associated with the pathogenesis and clinical expression of inherited myopathies. To determine whether a defect in nNOS might be an adverse modulating factor in the course of limb-girdle muscular dystrophy, we investigated cytosolic and sarcolemmal nNOS expression in muscle biopsies from 32 patients with 7 forms of limb-girdle muscular dystrophy. Primary calpainopathy, dysferlin- opathy, and caveolinopathy biopsies showed normal levels of cytosolic nNOS and preserved sarcolemmal nNOS immunoreactiv- ity. By contrast, the cytosolic nNOS levels in sarcoglycanopathy muscles were variably reduced. Sarcolemmal nNOS immunoreac- tivity varied from absent to reduced, depending on the integrity of the sarcoglycan complex. In muscles with loss of the entire sarcoglycan complex, sarcolemmal nNOS was absent; it otherwise depended on the specific sarcoglycan gene and type of mutation. The integrity of the entire sarcoglycan complex is, therefore, essential for the stabilization of nNOS to the sarcolemma. Absence of sarcolemmal nNOS in sarcoglycanopathy muscle was always associated with severe muscular dystrophy and sometimes with dilated cardiomyopathy, supporting the hypothesis that nNOS defect might contribute to skeletal and cardiac muscle disease progression. These results emphasize the value of nNOS immunohistochemical analysis in limb-girdle muscular dystrophy and provide additional insights for future therapeutic interventions in these disorders. Key Words: Limb-girdle muscular dystrophy, Nitric oxide synth- ase, nNOS, Sarcoglycan. INTRODUCTION The dystrophin-glycoprotein complex (DGC) of stri- ated muscle fiber sarcolemma is composed of cytoskeletal proteins (dystrophin, syntrophins), the dystroglycan complex and the sarcoglycan (SG) complex (1). The DGC provides a mechanical linkage between laminin in the extracellular matrix and the intracellular F-actin cytoskeleton (2). The structural and functional integrity of this connection is crucial for stabilization of the sarcolemma during contractions. The SG complex is composed of 4 glycoproteins (i.e. >-, A-, F-, and C-SG); the mutant genes of these glycopro- teins cause a group of autosomal recessive limb-girdle muscular dystrophies (LGMDs) termed sarcoglycanopathies (LGMD2D, 2E, 2C, 2F, respectively) (3). When 1 gene is mutated, all of the other SG components are secondarily reduced (4), assembly of the SG complex is compromised, and the sarcolemma integrity and stability are lost. A similar pathogenetic mechanism leads to Duchenne muscular dys- trophy (DMD) caused by mutations in the dystrophin gene. By virtue of its interactions with other proteins including neuronal nitric oxide synthase (nNOS), the DGC also has signaling roles. The nNOS is anchored at the sarcolemma by the binding of a PDX protein motif localized at its N-terminus to a similar motif in >1-syntrophin that binds to dystrophin (5Y8). Nitric oxide (NO), which is formed by nNOS activity, is a messenger molecule that regulates development, contractility, and blood flow in muscle (9). Nitric oxide rapidly transduces signaling events in a calcium-dependent manner. In adult muscle, nNOS is usually localized at the sarcolemma and the neuromuscular and myotendinous junctions. Significant amounts of nNOS are associated with the muscle phosphofructokinase isoform in the soluble fraction, although the nature of this interaction is unclear. Regulation of nNOS activity depends on its interactions with various proteins; it may be inhibited by caveolin-3, a component of the DGC that might displace the activator calmodulin, and by the protein inhibitor of nNOS, an endogenous protein that destabilizes the nNOS dimer (10). Under normal physiological conditions, the production of NO by nNOS results in the inhibition of sympathetic vasoconstriction in muscle. It has been suggested, therefore, that secondary loss of nNOS in muscular dystrophies contributes to fiber degeneration because reduced nNOS reduces the normal protective action of NO against local ischemia during contraction (i.e. the vascular hypothesis); it would also increase the cellular susceptibility to superoxides (i.e. the oxidative stress hypothesis) (11Y14). Muscle samples from DMD patients, dystrophin- deficient mdx mice and >1-syntrophin knockout mice show 383 J Neuropathol Exp Neurol Volume 68, Number 4, April 2009 J Neuropathol Exp Neurol Copyright Ó 2009 by the American Association of Neuropathologists, Inc. Vol. 68, No. 4 April 2009 pp. 383Y390 From the Department of Neurosciences, University of Padua (MF, ET, ACN, CA); and Venetian Institute of Molecular Medicine (MF, ET, ACN, CA), Padua, Italy. Send correspondence and reprint requests to: Marina Fanin, PhD, Venetian Institute of Molecular Medicine, via Giuseppe Orus 2, 35129 Padova, Italy; E-mail: [email protected] The study was supported by Grant No. GTB07001 from the Telethon-Italy (to Corrado Angelini), by Grant No. 2007.0889/12925 from the Association Fran0aise contre le Myopathies (to Marina Fanin), and by Grant No. COFIN 2006/062912 from the Italian Ministry for University and Research (to Corrado Angelini).

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Copyright @ 2009 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited.
ORIGINAL ARTICLE
Sarcolemmal Neuronal Nitric Oxide Synthase Defect inLimb-Girdle Muscular Dystrophy: An Adverse Modulating
Factor in the Disease Course?
Marina Fanin, PhD, Elisabetta Tasca, PhD, Anna Chiara Nascimbeni, PhD, and Corrado Angelini, MD
AbstractReduction of neuronal nitric oxide synthase (nNOS) has been
associated with the pathogenesis and clinical expression of inheritedmyopathies. To determine whether a defect in nNOS might be anadverse modulating factor in the course of limb-girdle musculardystrophy, we investigated cytosolic and sarcolemmal nNOSexpression in muscle biopsies from 32 patients with 7 forms oflimb-girdle muscular dystrophy. Primary calpainopathy, dysferlin-opathy, and caveolinopathy biopsies showed normal levels ofcytosolic nNOS and preserved sarcolemmal nNOS immunoreactiv-ity. By contrast, the cytosolic nNOS levels in sarcoglycanopathymuscles were variably reduced. Sarcolemmal nNOS immunoreac-tivity varied from absent to reduced, depending on the integrity ofthe sarcoglycan complex. In muscles with loss of the entiresarcoglycan complex, sarcolemmal nNOS was absent; it otherwisedepended on the specific sarcoglycan gene and type of mutation.The integrity of the entire sarcoglycan complex is, therefore,essential for the stabilization of nNOS to the sarcolemma. Absenceof sarcolemmal nNOS in sarcoglycanopathy muscle was alwaysassociated with severe muscular dystrophy and sometimes withdilated cardiomyopathy, supporting the hypothesis that nNOS defectmight contribute to skeletal and cardiac muscle disease progression.These results emphasize the value of nNOS immunohistochemicalanalysis in limb-girdle muscular dystrophy and provide additionalinsights for future therapeutic interventions in these disorders.
Key Words: Limb-girdle muscular dystrophy, Nitric oxide synth-ase, nNOS, Sarcoglycan.
INTRODUCTIONThe dystrophin-glycoprotein complex (DGC) of stri-
ated muscle fiber sarcolemma is composed of cytoskeletalproteins (dystrophin, syntrophins), the dystroglycan complex
and the sarcoglycan (SG) complex (1). The DGC provides amechanical linkage between laminin in the extracellularmatrix and the intracellular F-actin cytoskeleton (2). Thestructural and functional integrity of this connection is crucialfor stabilization of the sarcolemma during contractions.
The SG complex is composed of 4 glycoproteins (i.e.>-, A-, F-, and C-SG); the mutant genes of these glycopro-teins cause a group of autosomal recessive limb-girdlemuscular dystrophies (LGMDs) termed sarcoglycanopathies(LGMD2D, 2E, 2C, 2F, respectively) (3). When 1 gene ismutated, all of the other SG components are secondarilyreduced (4), assembly of the SG complex is compromised,and the sarcolemma integrity and stability are lost. A similarpathogenetic mechanism leads to Duchenne muscular dys-trophy (DMD) caused by mutations in the dystrophin gene.
By virtue of its interactions with other proteinsincluding neuronal nitric oxide synthase (nNOS), the DGCalso has signaling roles. The nNOS is anchored at thesarcolemma by the binding of a PDX protein motif localizedat its N-terminus to a similar motif in >1-syntrophin thatbinds to dystrophin (5Y8). Nitric oxide (NO), which isformed by nNOS activity, is a messenger molecule thatregulates development, contractility, and blood flow inmuscle (9). Nitric oxide rapidly transduces signaling eventsin a calcium-dependent manner. In adult muscle, nNOS isusually localized at the sarcolemma and the neuromuscularand myotendinous junctions. Significant amounts of nNOSare associated with the muscle phosphofructokinase isoformin the soluble fraction, although the nature of this interactionis unclear. Regulation of nNOS activity depends on itsinteractions with various proteins; it may be inhibited bycaveolin-3, a component of the DGC that might displace theactivator calmodulin, and by the protein inhibitor of nNOS,an endogenous protein that destabilizes the nNOS dimer (10).
Under normal physiological conditions, the productionof NO by nNOS results in the inhibition of sympatheticvasoconstriction in muscle. It has been suggested, therefore,that secondary loss of nNOS in muscular dystrophiescontributes to fiber degeneration because reduced nNOSreduces the normal protective action of NO against localischemia during contraction (i.e. the vascular hypothesis); itwould also increase the cellular susceptibility to superoxides(i.e. the oxidative stress hypothesis) (11Y14).
Muscle samples from DMD patients, dystrophin-deficient mdx mice and >1-syntrophin knockout mice show
383J Neuropathol Exp Neurol � Volume 68, Number 4, April 2009
J Neuropathol Exp NeurolCopyright � 2009 by the American Association of Neuropathologists, Inc.
Vol. 68, No. 4April 2009
pp. 383Y390
From the Department of Neurosciences, University of Padua (MF, ET, ACN,CA); and Venetian Institute of Molecular Medicine (MF, ET, ACN, CA),Padua, Italy.
Send correspondence and reprint requests to: Marina Fanin, PhD, VenetianInstitute of Molecular Medicine, via Giuseppe Orus 2, 35129 Padova,Italy; E-mail: [email protected]
The study was supported by Grant No. GTB07001 from the Telethon-Italy (toCorrado Angelini), by Grant No. 2007.0889/12925 from the AssociationFran0aise contre leMyopathies (toMarina Fanin), and byGrant No. COFIN2006/062912 from the Italian Ministry for University and Research (toCorrado Angelini).

Copyright @ 2009 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited.
absent nNOS at the sarcolemma, although it remains in thecytosol (5, 15). Absent sarcolemmal nNOS has also been re-ported in Becker muscular dystrophy, with dystrophin genedeletions that remove the central rod domain (exons between10 and 53), a region that is crucial for the interaction ofnNOS and >1-syntrophin (16Y18). The observation of a lossof sarcolemmal nNOS in disorders different from dystrophi-nopathies but having similar pathogenetic mechanismssuggested that a similar pathogenetic mechanism might occurin LGMD muscle. In a previous study, sarcolemmal nNOSwas found to be normal in an >-sarcoglycanopathy (16), butin a more extensive investigation of sarcoglycanopathies, itwas found to be reduced (19). Among LGMD cases otherthan those caused by sarcoglycanopathies, only caveolinop-athy caused by caveolin-3 gene mutations has been inves-tigated for nNOS expression in muscle; it was found to beeither normal in patients with rippling muscle disease (20) orseverely reduced in patients with LGMD phenotype (21).
It remains controversial, therefore, whether the loss ofsarcolemmal nNOS compounded with the defect of anothermuscle protein such as dystrophin or a sarcoglycan couldmodulate the disease course. Previous studies in mdx micehave demonstrated that normal nNOS activity could reducedystrophic symptoms, and forced expression of nNOS re-duced muscle pathology (8, 22), that the nNOS transgene inthe myocardium prevented ventricular fibrosis and greatlyreduced myocarditis (23), and that sarcolemmal nNOS wasrestored by the use of a minidystrophin vector (24). More-over, the level of nNOS expression seemed to be inverselycorrelated with the severity of the disease in caveolinopathy(21) and in Becker muscular dystrophy muscle (16). Bycontrast, other results have suggested that a reduction of NOSactivity would not significantly contribute to the dystrophicpathology. For example, mdx mice crossed with NOS-nullmutant mice showed no difference in muscle pathologycompared with mdx mice (8, 25, 26), nNOS-null mice do notshow muscular dystrophy (16), and >1-syntrophin knockoutmice with a loss of sarcolemmal nNOS did not show muscledegeneration (15).
In this study, we analyzed the cytosolic nNOS expres-sion and its sarcolemmal localization in muscle biopsies from32 patients with 7 different forms of molecularly definedLGMD. An understanding of the role of nNOS in humanmuscle pathology and specifically in progression and mod-ulation of the disease phenotype would be of greatimportance for future therapeutic interventions in LGMD.
MATERIALS AND METHODS
Selection of Patients and Muscle BiopsiesThe Neuromuscular Center at the Neurosciences Depart-
ment of the University of Padua hosts the Neuromuscular TissueBank, which contains about 7,500muscle biopsy specimens frompatients with various neuromuscular disorders. For the purpose ofthis study, the database connected to the Tissue Bank wassurveyed for patients who had molecularly proven forms ofLGMD.On the basis of tissue availability, we selected themusclesamples from 32 patients diagnosed as follows: 8 calpainopathy(LGMD2A), 2 dysferlinopathy (LGMD2B), 2 F-sarcoglycan-
opathy (LGMD2C), 4 >-sarcoglycanopathy (LGMD2D), 7 A-sarcoglycanopathy (LGMD2E), 1 C-sarcoglycanopathy(LGMD2F), and 8 caveolinopathy (LGMD1C). The moleculardiagnosis of LGMD had been assessed using a preliminaryscreening of multiple protein defects followed by the identi-fication of causative gene mutations.
We also studied muscle biopsies from 5 DMD patientsand from 6 subjects who were free of any muscle disorder asdisease and normal controls, respectively. Patients had under-gone open diagnostic muscle biopsies (mostly of the quad-riceps femoris and seldom of the biceps/triceps brachii) afterwritten consent was obtained. All diagnostic procedures wereconducted according to the local Ethical Committee. Aftersurgery, muscle specimens were frozen in isopentane, chilledin liquid nitrogen, and then stored at Y80-C until processing.
Immunohistochemical AnalysisCryostat sections, 8-Km-thick, were placed on gelati-
nized slides and processed using a panel of monoclonalantibodies to the 4 SG complex components, >-SG (diluted1:20), A-SG (diluted 1:100), F-SG (diluted 1:100), and C-SG([diluted 1:100] all from Novocastra, Newcastle-upon-Tyne,United Kingdom); nNOS (against an epitope in the N-terminus[diluted 1:100]; Santa Cruz Biotechnology, Santa Cruz, CA);caveolin-3 ([diluted 1:100] Transduction Laboratories,Lexington, KY); and spectrin ([diluted 1:100] SPEC1,Novocastra). Monoclonal antibody against neonatal myosin([diluted 1:100] nMHC, Novocastra) was used to labelregenerating fibers in serial muscle sections.
Primary antibodies were incubated on the sectionsovernight in a humid chamber. The specific labeling wasdeveloped using anti-mouse cyanine-3 conjugated immuno-globulins (Serotec, Oxford, United Kingdom). Negativecontrols with omission of a primary antibody showed nostaining. Sections were examined by fluorescence micro-scopy. The intensity of reaction was determined by a singleobserver and graded by comparison to the controls as normal,moderate reduction, severe reduction, or absence of reaction.
Semiquantitative Immunoblot AnalysisImmunoblot analysis was conducted with minor modifi-
cations as previously described (27). Briefly, cryostat sections ofmuscle biopsies were dissolved in Laemmli loading buffer,boiled, and centrifuged. Proteins were resolved by sodiumdodecyl sulfateYpolyacrylamide gel electrophoresis and blottedto nitrocellulose membrane. Blots were air dried, blocked with5% nonfat milk in Tris-Tween-20 saline buffer, and incubatedovernight with monoclonal antibodies against dystrophin(DYS-2, diluted 1:1000), >-SG (diluted 1:500), calpain-3(Calp12A2, diluted 1:800), dysferlin ([diluted 1:2000] all fromNovocastra), and against an epitope of amino acids 1095-1289in the C-terminal domain of nNOS ([diluted 1:1000] Trans-duction Lab.). After thorough washing, the immunoreactivebands were visualized using anti-mouse biotinylated immuno-globulins and streptavidin-biotinylated-peroxidase complex(both diluted 1:1000 and incubated for 1 hour) and developedusing the chemiluminescent method.
The quantity of each protein in the samples wasdetermined by densitometry using ImageJ software v.1.34,
Fanin et al J Neuropathol Exp Neurol � Volume 68, Number 4, April 2009
� 2009 American Association of Neuropathologists, Inc.384

Copyright @ 2009 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited.
normalizing the corresponding protein band on blots to themyosin band in the post-transfer Coomassie blue-stained gelsand expressed as a percentage of the mean of controls.
RESULTS
Clinical and Molecular Patient DataThe clinical phenotypes, ages at biopsy, and the
expression of mutant proteins in muscle from the 32 LGMDpatients are reported in Tables 1 and 2. Seventeen LGMDpatients had progressive muscular dystrophy with early onsetof muscle weakness (before 12 years of age), 7 had anLGMD phenotype with onset of weakness in adolescence oradulthood, 4 had a distal myopathy phenotype with onset ofweakness in the distal leg muscles, 3 were asymptomatic withonly elevated creatine kinase level (hyperCKemia pheno-type), and 1 had rippling muscle disease.
The patients’ ages ranged from 1 to 59 years at the timeof the study. Most of the sarcoglycanopathy patients hada severe form of muscular dystrophy with early onset ofweakness and/or early loss of independent ambulation. Asevere dilated cardiomyopathy was documented in associa-tion with severe muscular dystrophy in 5 sarcoglycanopathypatients (Patients 9, 10, 12, 13, 14; Table 1).
nNOS ImmunohistochemistryMuscle from patients with sarcoglycanopathy showed
variable patterns of nNOS immunolabeling at the sarcolemmathat depended on the overall reaction for the SG complex; themuscle from 6 patients with >-sarcoglycanopathy or A-sarcoglycanopathy who had a complete defect of all SGcomplex components (Patients 5, 7, 8, 9, 10, 11) also hadabsent nNOS sarcolemmal immunolabeling (Table 1; Figs. 1and 2); the cases with a complete defect of only 1 SG proteinassociated with partial defect of the other SG subunits hadpositive sarcolemma nNOS reaction (Figs. 1 and 2), althoughit was sometimes of reduced intensity. Scattered musclefibers had absent sarcolemmal nNOS staining; these showedlabeling for neonatal myosin, indicating that they wereundergoing regeneration (Fig. 3).
Muscle from patients with calpainopathy, dysferlinop-athy, and caveolinopathy showed sarcolemmal nNOS immu-nopositivity, although the intensity of the reaction wassometimes reduced (Fig. 2). The DMD muscle, used as adisease control, invariably showed absent nNOS sarcolemmalstaining (Fig. 2).
nNOS ImmunoblottingWe performed nNOS immunoblot analysis only in
muscle biopsy samples in samples for which there was
TABLE 1. Clinical and Muscle Pathological Data of Sarcoglycanopathy and Duchenne Muscular Dystrophy Patients
Patient Disease*
Age atStudyyears Phenotype
CardiacDisease*
MutantProteinWesternBlot
Mutant ProteinImmunohistochemistry
nNOSWesternBlot, %
nNOSImmunohistochemistry
1 F-Sarcoglycanopathy 6 Early-onsetLGMD
ND >-SG:10%
F-SG: severe reduction 83 Severe reduction
2 F-Sarcoglycanopathy 35 Early-onsetLGMD
ND V F-SG: absent 50 Moderate reduction
3 >-Sarcoglycanopathy 43 Early-onsetLGMD
ND >-SG:absent
Other SGs: moderatereduction
87 Moderate reduction
4 >-Sarcoglycanopathy 7 HyperCKemia ND >-SG:20%
F-SG: normal reaction 85 Moderate reduction
5 >-Sarcoglycanopathy 6 Early-onsetLGMD
ND All SGs:absent
All SGs: absent 69 Absent
6 >-Sarcoglycanopathy 11 Early-onsetLGMD
ND >-SG:absent
Other SGs: severereduction
73 Severe reduction
7 A-Sarcoglycanopathy 1 Early-onsetLGMD
ND All SGs:absent
All SGs: absent 45 Absent
8 A-sarcoglycanopathy 10 Early-onsetLGMD
ND All SGs:absent
All SGs: absent V Absent
9 A-Sarcoglycanopathy 12 Early-onsetLGMD
DCM All SGs:absent
All SGs: absent V Absent
10 A-Sarcoglycanopathy 27 Early-onsetLGMD
DCM All SGs:absent
All SGs: absent V Absent
11 A-Sarcoglycanopathy 9 Early-onsetLGMD
ND All SGs:absent
All SGs: absent V Absent
12 A-Sarcoglycanopathy 24 Early-onsetLGMD
DCM >-SG:50%
Other SGs: moderatereduction
V Severe reduction
13 A-Sarcoglycanopathy 19 Early-onsetLGMD
DCM >-SG:10%
Other SGs: severereduction
40 Severe reduction
14 C-Sarcoglycanopathy 34 Early-onsetLGMD
DCM >-SG:10%
Other SGs: severereduction
52 Moderate reduction
DCM, dilated cardiomyopathy; LGMD, limb-girdle muscular dystrophy; ND, not determined; nNOS, neuronal nitric oxide synthase; SG, sarcoglycanopathy.
J Neuropathol Exp Neurol � Volume 68, Number 4, April 2009 nNOS Expression in LGMD
� 2009 American Association of Neuropathologists, Inc. 385

Copyright @ 2009 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited.
sufficient tissue available. The amount of nNOS wassignificantly reduced (40%Y55% of controls) in all patientswith A- and C-sarcoglycanopathies (Fig. 4; Table 1) and in 1patient each with calpainopathy, F-sarcoglycanopathy, andcaveolinopathy (Patients 15, 2, 31; Tables 1 and 2). Theaverage amount of nNOS was 65% of controls in thesarcoglycanopathy patients, whereas it was not significantlydifferent from control in the remaining LGMD cases(average, 102% of controls; Fig. 4; Table 2). In 5 DMDmuscle samples, the amount of nNOS was highly variable,ranging from normal to 17% of controls.
Correlation Between nNOS Expression andClinical Phenotype or Genotype
Absence of sarcolemmal nNOS expression wasobserved in 6 sarcoglycanopathy patients that had absenceof the entire SG complex (Table 1) and in DMD muscles.These sarcoglycanopathy patients had either A- or >-sarcoglycanopathy; all of these cases had a severe form ofearly-onset progressive muscular dystrophy. In particular, 2patients (Patients 9 and 10) who at the time of biopsy wereolder than 12 years had already lost independent ambulation.Four of 6 sarcoglycanopathy patients (Patients 5, 7, 8, and11) and both DMD patients were too young at the time of
this study to determine the eventual presence of cardiacinvolvement, but 2 of 6 (Patients 9 and 10) had severedilated cardiomyopathy at 12 and 27 years of age,respectively, as well as severe muscular dystrophy. Twoadditional A-sarcoglycanopathy (Patients 12 and 13) and 1 F-sarcoglycanopathy (Patient 14) patients, who had residual SGprotein and reduced nNOS sarcolemmal immunolabeling,had a slowly progressive LGMD phenotype associated withsevere dilated cardiomyopathy (Table 1). In Patient 13, ahomozygous mutation (c.22+10dupl) allowed the synthesisof very small amounts of all 4 SG complex components thatwere correctly localized to the sarcolemma and detected byimmunofluorescence (Fig. 1, right panels).
The absent sarcolemmal nNOS in LGMD patients wasindependent of which SG gene (A-SG or >-SG) was mutatedand the type of gene mutation; that is, in cases with 2 missensealleles and in cases with 2 null mutant alleles.
DISCUSSIONThe present results offer further support to the
hypothesis of a possible role of an nNOS sarcolemmal defectin skeletal and possibly also cardiac muscle disease pro-gression in sarcoglycanopathies.
TABLE 2. Clinical and Muscle Pathological Data of LGMD2A, LGMD2B, LGMD1C Patients
Patient Disease
Age atBiopsy,years Phenotype
Mutant ProteinWestern Blot
Mutant ProteinImmunohistochemistry
nNOS WesternBlot, %
nNOSImmunohistochemistry
15 Calpainopathy 49 LGMD Calpain-3: 100% V 52 Normal
16 Calpainopathy 19 Early-onsetLGMD
Calpain-3: absent V 106 Severe reduction
17 Calpainopathy 46 LGMD Calpain-3: absent V 99 Normal
18 Calpainopathy 55 Early-onsetLGMD
Calpain-3: 10% V 105 Severe reduction
19 Calpainopathy 30 HyperCKemia Calpain-3: 10% V 130 Normal
20 Calpainopathy 33 LGMD Calpain-3: 5% V 94 Severe reduction
21 Calpainopathy 38 LGMD Calpain-3: absent V 96 Moderate reduction
22 Calpainopathy 22 LGMD Calpain-3: absent V 80 Moderate reduction
23 Dysferlinopathy 59 Distalmyopathy
Dysferlin: absent V 176 Moderate reduction
24 Dysferlinopathy 34 Distalmyopathy
Dysferlin: absent V 116 Moderate reduction
25 Caveolinopathy 21 Early-onsetLGMD
V Caveolin-3: severereduction
125 Moderate reduction
26 Caveolinopathy 26 Distalmyopathy
V Caveolin-3: severereduction
106 Moderate reduction
27 Caveolinopathy 10 HyperCKemia V Caveolin-3: severereduction
122 Severe reduction
28 Caveolinopathy 58 Distalmyopathy
V Caveolin-3: severereduction
92 Moderate reduction
29 Caveolinopathy 40 LGMD V Caveolin-3: normalreaction
98 Moderate reduction
30 Caveolinopathy 13 Early-onsetLGMD
V Caveolin-3: severereduction
87 Moderate reduction
31 Caveolinopathy 32 LGMD V Caveolin-3: severereduction
55 Severe reduction
32 Caveolinopathy 14 Ripplingmuscle
V Caveolin-3: severereduction
105 Severe reduction
LGMD, limb-girdle muscular dystrophy; nNOS, neuronal nitric oxide synthase.
Fanin et al J Neuropathol Exp Neurol � Volume 68, Number 4, April 2009
� 2009 American Association of Neuropathologists, Inc.386

Copyright @ 2009 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited.
The nNOS was present at normal levels in the cytosoland was maintained at the sarcolemma in calpainopathy,dysferlinopathy, and caveolinopathy muscle biopsy samples,suggesting that the interactions between the mutant protein inthese conditions and nNOS are not crucial for the nNOSsignaling pathway, which seems to be linked to the DGC.The apparent discrepancy between reduced sarcolemmalnNOS reaction and normal cytosolic expression that weobserved in some nonsarcoglycanopathy LGMD patientsmight be explained by a partial dissociation of nNOS from
the sarcolemma because the interaction between nNOS andDGC is relatively weak. This dissociation might occur duringthe solubilization procedure, thereby contributing to itsrelative concentration in the cytosol (26),
We found that in sarcoglycanopathy muscle, thesarcolemmal nNOS reaction varied from absent to reduced,depending on the integrity of the DGC, and that the cytosolicnNOS levels were lower than in controls. Similar resultsin DMD muscle (5, 16, 12) suggest that the preservation ofdystrophin is crucial for stabilizing nNOS to the sarcolemma.
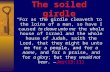
FIGURE 1. Muscle biopsies from 1 control and 2 A-sarcoglycanopathy patients immunolabeled with antibodies against >-, A-, F-, andC-sarcoglycan (SG), neuronal nitric oxide synthase (nNOS), and caveolin-3 (CAV). In A-sarcoglycanopathy Patient 7, the 4 SG complexcomponents and nNOS were completely absent at the sarcolemma; A-sarcoglycanopathy Patient 13 showed severely reduced butdetectable immunolabeling for all SG proteins and positive but reduced nNOS sarcolemmal expression. Caveolin-3 was present in allbiopsies (original magnification: 200�).
J Neuropathol Exp Neurol � Volume 68, Number 4, April 2009 nNOS Expression in LGMD
� 2009 American Association of Neuropathologists, Inc. 387

Copyright @ 2009 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited.
We demonstrated that the integrity of the SG complex is alsoessential for the sarcolemmal localization of nNOS, aspreviously suggested (19), and showed that sarcolemmalnNOS expression correlates with the residual level of SGcomplex. Thus, muscle from sarcoglycanopathy patients withcomplete loss of all the 4 SG complex components, most ofwhom are affected with A-sarcoglycanopathy, also had absentsarcolemmal nNOS, whereas sarcoglycanopathy muscle withresidual expression at least 1 SG subunit had positivesarcolemmal nNOS immunolabeling. The absence of sarco-lemmal nNOS was independent of which is the SG genemutated (i.e. it was frequently found in A-sarcoglycanopathypatients), but it was also observed in >-sarcoglycanopathymuscle, reflecting the frequency of the absence of the wholeSG complex in the different sarcoglycanopathies. Moreover,absence of sarcolemmal nNOS was not dependent on the typeof SG gene mutation. Further support for the notion that the
integrity of the whole DGC is essential for localization ofnNOS to the sarcolemma is the finding that immatureregenerating fibers lack sarcolemmal nNOS (Fig. 3), asoccurs with dystrophin and other sarcolemmal proteindeficiencies (28, 29).
Cytosolic nNOS expression in sarcoglycanopathymuscles was about 65% of that in controls, but it is unclearwhether this was the result of intracellular degradation,reduced production, or the dystrophic pathology. Pathoge-netic events underlying muscular dystrophy might includetranscriptional downregulation of nNOS expression. Forexample, nNOS messenger RNA levels were greatly reducedin mdx muscle, suggesting a defect in nNOS expression (12).Alternatively, nNOS may be less stable in the cytosol andmight be more rapidly degraded in dystrophic muscle. Otherstudies indicate that reduced NO levels in DMD can beexplained as removal of NO by superoxides rather than as
FIGURE 2. Membrane-associated neuronal nitric oxide synthase (nNOS) in muscle biopsies was decreased in proportion toresidual sarcoglycan complex, but the extent of immunolabeling did not correlate with any specific sarcoglycanopathy (SG).Immunolabeling for nNOS in Duchenne muscular dystrophy (DMD [A]), SG (BYF), and nonsarcoglycanopathy (GYL) patients.Sarcolemmal nNOS immunoreactivity was present, although sometimes reduced in intensity or patchy in F-sarcoglycanopathy(LGMD2C [B]), >-sarcoglycanopathy (LGMD2D [C]), calpainopathy (LGMD2A [G, H]), dysferlinopathy (LGMD2B [I, J]),caveolinopathy (LGMD1C [K, L]), C-sarcoglycanopathy (LGMD2F [F]), and in A-sarcoglycanopathy (LGMD2E) with partialsarcoglycan defect (E). It was completely absent in DMD (A) and in A-sarcoglycanopathy patients with a complete SG complexdefect (D) (original magnification: 200�).
Fanin et al J Neuropathol Exp Neurol � Volume 68, Number 4, April 2009
� 2009 American Association of Neuropathologists, Inc.388

Copyright @ 2009 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited.
downregulation of nNOS expression. Thus, the reductionmight be secondary to oxidative stress rather than fromreduced NOS expression (30).
Loss of sarcolemmal nNOS in DMD muscle may resultin aberrant regulation of adrenergic vasoconstriction and toa defective vasodilation (31, 11). Dystrophic muscle withoutmembrane-localized nNOS may be unable to maintain anormal vasoconstriction during exercise; without vasculardilation and subsequent blood flow, skeletal and cardiacmuscles may have ischemia and focal necrosis. The excessiveNO generated in necrotic myocytes from focally mislocalizedNOS may provide the signal for vasospasm in the nearbysmooth muscle cells. Vasospasm has been demonstratedin F- and C-SGYdeficient and in mdx mice (32, 33); using
transgene rescue in SG-null mice, SG expression wasrestored in cardiomyocytes that was sufficient to correctcardiac focal degeneration and eliminate coronary arteryvasospasm (33).
Absence or severe reduction of nNOS expression at thesarcolemma was associated with severe early-onset musculardystrophy in all cases and with the presence of dilatedcardiomyopathy in 2 of 3 sarcoglycanopathy patients whowere old enough to exhibit cardiomyopathy (34, 35). Further-more, experimental evidence in animal models of sarcogly-canopathies showed that transgenic mice with A-SG andC-SG deficiency had severe muscular dystrophy and cardio-myopathy, and that SG and DGC complexes were disruptedin skeletal, cardiac, and vascular smooth muscle, suggestingthat a perturbation of vascular smooth muscle might be anadditional mechanism that could contribute to the de-velopment of myopathy and cardiomyopathy (36Y38). TheNO was found to be increased in regions of cardiac tissuedamage and altered membrane permeability in SG mutantmice (39). The absence of SG complex in the vascularsmooth muscle might lead either to structural changes or toan impairment of metabolic and signaling pathways involvedin the microvascular dysfunction (36); that is, high Ca++
levels and disturbance of the NOS pathway increasevasculature contractility, making cardiomyocytes moresusceptible to intermittent ischemia. Indeed, the use ofvasodilator drugs has been shown to prevent the developmentof acute myocardial necrosis in animal models of A- andC-sarcoglycanopathy (36, 40).
The finding that absent sarcolemmal nNOS can befound not only in some Becker muscular dystrophy patients(18) but also in sarcoglycanopathies emphasizes the value ofnNOS immunohistochemical analysis in LGMD and providesfurther insights for future therapeutic interventions. Forexample, antioxidants that attenuate the superoxide attackand restore the bioactive NO level and exogenous NO donorsor dietary addition of a NOS substrate such as L-arginine maybe useful approaches for the treatment of these disorders.
FIGURE 4. Neuronal nitric oxide synthase (nNOS) immunoblotting of muscle biopsy homogenate from control and from patientswith different types of limb-girdle muscular dystrophy (LGMD). After normalization with myosin (MHC) content, as determined onpost-transfer Coomassie blue stained gels (lower panel), nNOS protein quantity in samples from 2 A-sarcoglycanopathy patients(Patients 7 and 13) and 1 C-sarcoglycanopathy patient (Patient 14) was reduced to approximately 50% of control (lower row); itwas variably expressed in the other disorders (upper row).
FIGURE 3. Two pairs ([A] and [B]; [C] and [D]) of muscleserial sections from a calpainopathy patient immunolabeledfor neuronal nitric oxide synthase (nNOS) (A, C) and neonatalmyosin (B, D) demonstrated nNOS-negative fibers under-going regeneration, as indicated by neonatal myosin immu-nopositivity (asterisks indicate the same fibers; originalmagnification: 200�).
J Neuropathol Exp Neurol � Volume 68, Number 4, April 2009 nNOS Expression in LGMD
� 2009 American Association of Neuropathologists, Inc. 389

Copyright @ 2009 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited.
REFERENCES1. Ervasti JM, Campbell KP. Membrane organization of the dystrophin<
glycoprotein complex. Cell 1991;66:1121Y312. Campbell KP. Three muscular dystrophies: Loss of cytoskeleton<
extracellular matrix linkage. Cell 1995;80:675Y793. Lim LE, Campbell KP. The sarcoglycan complex in limb-girdle
muscular dystrophy. Curr Opin Neurol 1998;11:443Y524. Duggan DJ, Gorospe JR, Fanin M, Hoffman EP, Angelini C. Mutations
in the sarcoglycan genes in patients with myopathy. N Engl J Med 1997;336:618Y24
5. Brenman JE, Chao DS, Xia H, et al. Nitric oxide synthase complexedwith dystrophin and absent from skeletal muscle sarcolemma inDuchenne muscular dystrophy. Cell 1995;82:743Y52
6. Grozdanovic Z. NO message from muscle. Microsc Res Tech 2001;55:148Y53
7. Grady RM, Grange RW, Lau KS, et al. Role for alpha-dystrobrevin inthe pathogenesis of dystrophin-dependent muscular dystrophies. NatCell Biol 1999;1:215Y20
8. Wehling M, Spencer MJ, Tidball JG. A nitric oxide synthase trans-gene ameliorates muscular dystrophy in mdx mice. J Cell Biol 2001;155:123Y31
9. Stamler JS, Meissner G. Physiology of nitric oxide in skeletal muscle.Physiol Rev 2001;81:209Y37
10. Jaffrey SR, Snyder SH. PIN: An associated protein inhibitor of neuronalnitric oxide synthase. Science 1996;274:774Y77
11. Sander M, Chavoshan B, Harris SA, et al. Functional muscle ischemiain neuronal nitric oxide synthase-deficient skeletal muscle of childrenwith Duchenne muscular dystrophy. Proc Natl Acad Sci U S A 2000;97:13818Y23
12. Chang W, Iannaccone ST, Lau KS, et al. Neuronal nitric oxide synthaseand dystrophin-deficient muscular dystrophy. Proc Natl Acad Sci U S A1996;93:9142Y47
13. Crosbie RH. NO vascular control in Duchenne muscular dystrophy. NatMed 2001;7:27Y29
14. Rando TA. Role of nitric oxide in the pathogenesis of musculardystrophies: A Btwo-hit[ hypothesis of the cause of muscle necrosis.Microsc Res Tech 2001;55:223Y35
15. Kameya S, Miyagoe Y, Nonaka I, et al. >1-syntrophin gene disruptionresults in the absence of neuronal-type nitric oxide synthase at thesarcolemma but does not induce muscle degeneration. J Biol Chem1999;274:2193Y200
16. Chao DS, Gorospe JR, Brenman JE, et al. Selective loss of sarcolemmalnitric oxide synthase in Becker muscular dystrophy. J Exp Med 1996;184:609Y18
17. Wells KE, Torelli S, Lu Q, et al. Relocalization of neuronal nitric oxidesynthase (nNOS) as a marker for complete restoration of the dystrophinassociated protein complex in skeletal muscle. Neuromuscul Disord2003;13:21Y31
18. Torelli S, Brown SC, Jimenez-Mallebrera C, et al. Absence of neuronalnitric oxide synthase (nNOS) as a pathological marker for the diagnosisof Becker muscular dystrophy with rod domain deletions. NeuropatholAppl Neurobiol 2004;30:540Y45
19. Crosbie RH, Barresi R, Campbell KP. Loss of sarcolemma nNOS insarcoglycan-deficient muscle. FASEB J 2002;16:1786Y91
20. Vorgerd M, Ricker K, Ziemssen F, et al. A sporadic case of ripplingmuscle disease caused by a de novo caveolin-3 mutation. Neurology2001;57:2273Y77
21. Herrmann R, Straub V, Blank M, et al. Dissociation of the dystroglycancomplex in caveolin-3 deficient limb girdle muscular dystrophy. HumMol Genet 2000;9:2335Y40
22. Archer JD, Vargas CC, Anderson JE. Persistent and improved functionalgain in mdx dystrophic mice after treatment with L-arginine anddeflazacort. FASEB J 2006;20:738Y40
23. Wehling-Henricks M, Jordan MC, Roos KP, Deng B, Tidball JG.Cardiomyopathy in dystrophin-deficient hearts is prevented by expres-sion of a neuronal nitric oxide synthase transgene in the myocardium.Hum Mol Genet 2005;14:1921Y33
24. Wang B, Li J, Qiao C, et al. A canine minidystrophin is functional andtherapeutic in mdx mice. Gene Ther 2008;15:1099Y106
25. Crosbie RH, Straub V, Yun HY, et al. Mdx muscle pathology isindependent of nNOS perturbation. Hum Mol Genet 1998;7:823Y29
26. Wehling M, Stull JT, McCabe TJ, Tidball JG. Sparing of mdxextraocular muscles from dystrophic pathology is not attributable tonormalized concentration or distribution of neuronal nitric oxidesynthase. Neuromuscul Dis 1998;8:22Y29
27. Anderson LVB, Davison K. A multiplex western blotting system for theanalysis of muscular dystrophy proteins. Am J Pathol 1999;154:1017Y22
28. Fanin M, Angelini C. Regeneration in sarcoglycanopathies: Expressionstudies of sarcoglycans and other muscle proteins. J Neurol Sci 1999;165:170Y77
29. Hoshino S, Ohkoshi N, Ishii A, Shoji S. The expression of nNOS anddystrophin in rat regenerating muscle. J Muscle Res Cell Motil 2002;23:139Y45
30. Punkt K, Schering S, Loffler S, et al. Nitric oxide synthase isup-regulated in muscle fibers in muscular dystrophy. Biochem BiophysRes Comm 2006;348:259Y64
31. Thomas GD, Sander M, Lau KS, Huang PL, Stull JT, Victor RG.Impaired metabolic modulation of alpha-adrenergic vasoconstriction indystrophin-deficient skeletal muscle. Proc Natl Acad Sci U S A 1998;95:15090Y95
32. Hainsey TA, Senapati S, Kuhn DE, Rafael JA. Cardiomyopathicfeatures associated with muscular dystrophy are independent ofdystrophin absence in cardiovasculature. Neuromuscul Dis 2003;13:294Y302
33. Wheeler MT, Allikian MJ, Heydemann A, et al. Smooth musclecellVextrinsic vascular spasm arises from cardiomyocyte degener-ation in sarcoglycan-deficient cardiomyopathy. J Clin Invest 2004;113:668Y75
34. Melacini P, Fanin M, Duggan DJ, et al. Heart involvement in musculardystrophies due to sarcoglycan gene mutations. Muscle Nerve 1999;22:473Y79
35. Fanin M, Melacini P, Boito C, Pegoraro E, Angelini C. LGMD2Epatients risk developing dilated cardiomyopathy. Neuromuscul Dis2003;13:303Y9
36. Coral-Vazquez R, Cohn RD, Moore SA, et al. Disruption of thesarcoglycan-sarcospan complex in vascular smooth muscle: A novelmechanism for cardiomyopathy and muscular dystrophy. Cell 1999;98:465Y74
37. Araishi K, Sasaoka T, Imamura M, et al. Loss of the sarcoglycancomplex and sarcospan leads to muscular dystrophy in beta-sarcoglycandeficient mice. Hum Mol Genet 1999;8:1589Y98
38. Durbeej M, Cohn RD, Hrstka RF, et al. Disruption of the A-sarcoglycangene reveals pathogenetic complexity of limb-girdle muscular dystrophytype 2E. Mol Cell 2000;5:141Y51
39. Heydemann A, Huber JM, Kakkar R, Wheeler MT, McNally EM.Functional nitric oxide synthase mislocalization in cardiomyopathy. JMol Cell Cardiol 2004;36:213Y23
40. Cohn RD, Durbeej M, Moore SA, et al. Prevention of cardiomyopathy inmouse models lacking the smooth muscle sarcoglycan-sarcospancomplex. J Clin Invest 2001;107:1Y7
Fanin et al J Neuropathol Exp Neurol � Volume 68, Number 4, April 2009
� 2009 American Association of Neuropathologists, Inc.390
Related Documents