Plasmapheresis in Sepsis Bilgin CÖMERT, MD. Dokuz Eylül University, School of Medicine Department of Medical Intensive Care Unit

Salon a 14 kasim 13.30 14.45 bi̇lgi̇n cömert
Jul 24, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Plasmapheresis in Sepsis
Bilgin CÖMERT, MD.
Dokuz Eylül University, School of Medicine
Department of Medical Intensive Care Unit

Terminology
• Therapeutic Plasma Exchangeseparates out plasma from other components of blood, the plasma is removed and replaced with a replacement solution such as colloid solution (e.g., albumin and/or plasma) or combination of crystalloid/colloid solution
• Plasmapheresisseparates out plasma from other components of blood and the plasma is removed (i.e. less than 15% of total plasma volume) without the use of replacement solution

Plasmapheresis/Plasma Exchange in Critical Illness
• Thrombotic Thrombocytopenic Purpura
• Atypical Hemolytic Uremic Syndrome
• Thrombotic Microangiopathy: Drug-Associated (ticlopidine and clopidogrel)
• Wilson’s disease in fulminant hepatic failure with hemolysis
• Guillain-Barre Syndrome
• Chronic Inflammatory Demyelinating Polyradiculoneuropathy
• Sydenham’s Chorea
• Multiple Sclerosis
• Myasthenia Gravis
• Goodpasture’s Syndrome
• Wegener’s Granulomatosis
Sepsis Treatment (Standart)
• Antimicrobial agents
• Control of the source of the infection
• Hemodynamic support• Fluids• Vasopressors
• Oxygenation and ventilatory support
• Avoidance of complications

Sepsis Treatment (innovative)
• Corticosteroids• Monoclonal antibodies to TNF• Antitrombin• Activated protein C• Extracorporeal Therapies• CRRT• Plasma Exchange• ECMO

Aims of the Extracorporeal Therapies• Provide immunohomeostasis of pro- and anti-inflammatory
cytokines and other sepsis mediators
• Decrease organ microthrombosis through removal of pro-coagulant factors
• Modulating the impaired septic coagulation response in sepsis
• Provide mechanical support of organ perfusion during the acute septic episode
Semin Pediatr Infect Dis 2006;17:72-9

Artif Organs 2003;27:792-801

Plasma Exchange
• Remove harmful and toxic mediators from circulation as non-selectively
• If fresh frozen plasma is used as the replacement solution, substance consumed during systemic inlammatory process would be replaced

Plsmapheresis
(n=54)
Control(n=52) P
AgeApache III
41±1556.4±18.8
48±1653.5±15.8
0.030.40
28-day survivalTotal study populationAbdominal groupOther groups
18 (33%)11/33 (33%)7/21 (33%)
28 (54%)11/16 (68%)17/36 (47%)
0.050.030.4
Intensive Care Med 2002;28:1434-9

22 Adults, 8 Children
• Filtration/PE group n=14
• Control group n=16
Continuous Plasmafiltration in sepsis syndrome
Crit Care Med 1999;27:2096-104
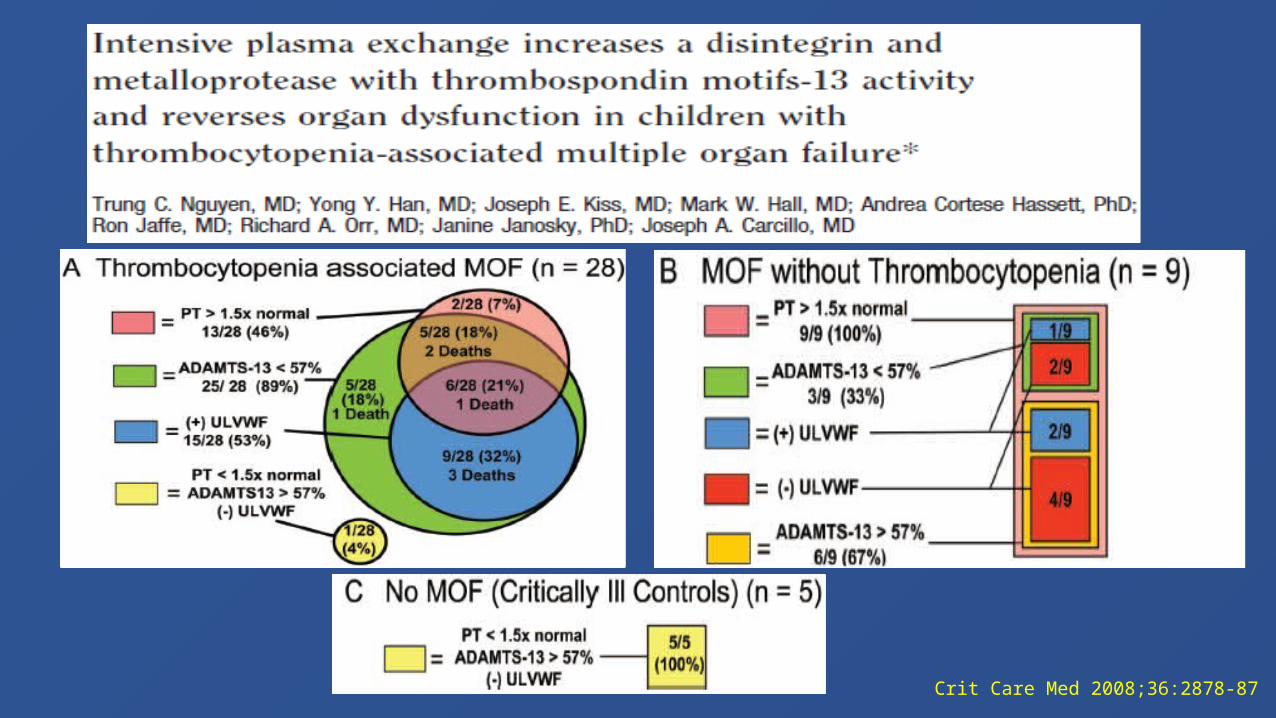
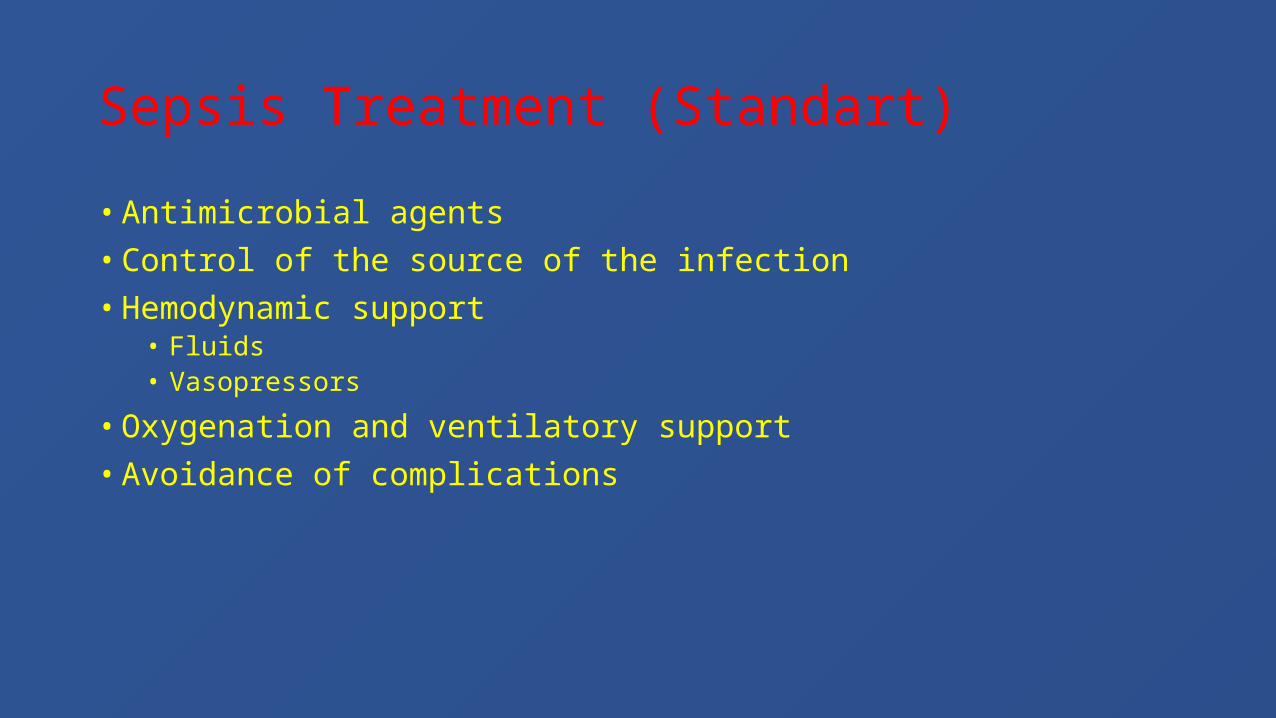
Crit Care Med 2008;36:2878-87
Survival (28-day)
Plasma Exchange (n=5) 5/5
Standard Therapy (n=5)1/5 Crit Care Med 2008;36:2878-87
*Semin Pediatr Infect Dis 2006;17:72-9
Survival 28-day 1-year
Plasma Exchange (n=60) 90%80%
Standard Therapy (n=16) 20%15%
(Unpublished data)*

Crit Care Med 2007;35:2375-82
p < 0.01 p < 0.001
P < 0.001

• Therapeutic Plasma Exchange in Sepsis with Multiorgan Failure
Recommendation : Grade 2B
J Clin Apheresis 2010;25:83-177
Surviving Sepsis Campaign-2012
Plasma therapies in children to correct sepsis-induced thrombotic purpura disorders• Progressive DIC• Secondary Thrombotic microangiopathy• TTP
• Recommendation: Grade 2C
• No recommendations for adultsCrit Care Med 2013;41:580-637

Related Documents