DOI 10.1378/chest.09-0821 2009;136;1029-1038; Prepublished online July 24, 2009; Chest Gustavo J. Rodrigo, José A. Castro-Rodriguez and Vicente Plaza Monotherapy for Stable COPD -Agonists β Corticosteroids vs Long-Acting -Agonists and Inhaled β Long-Acting Safety and Efficacy of Combined http://chestjournal.chestpubs.org/content/136/4/1029.full.html and services can be found online on the World Wide Web at: The online version of this article, along with updated information ISSN:0012-3692 ) http://chestjournal.chestpubs.org/site/misc/reprints.xhtml ( of the copyright holder. may be reproduced or distributed without the prior written permission Northbrook, IL 60062. All rights reserved. No part of this article or PDF by the American College of Chest Physicians, 3300 Dundee Road, 2009 Physicians. It has been published monthly since 1935. Copyright CHEST is the official journal of the American College of Chest © 2009 American College of Chest Physicians by Gustavo Medrano on November 1, 2009 chestjournal.chestpubs.org Downloaded from

Safetyandefficacy
Mar 19, 2016
http://www.alatorax.org/images/stories/demo/pdf/epoc/Publicacionesmiembros/2009/Safetyandefficacy.pdf
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

DOI 10.1378/chest.09-0821 2009;136;1029-1038; Prepublished online July 24, 2009;Chest
Gustavo J. Rodrigo, José A. Castro-Rodriguez and Vicente Plaza Monotherapy for Stable COPD
-AgonistsβCorticosteroids vs Long-Acting -Agonists and InhaledβLong-Acting
Safety and Efficacy of Combined
http://chestjournal.chestpubs.org/content/136/4/1029.full.htmland services can be found online on the World Wide Web at: The online version of this article, along with updated information
ISSN:0012-3692)http://chestjournal.chestpubs.org/site/misc/reprints.xhtml(
of the copyright holder.may be reproduced or distributed without the prior written permission Northbrook, IL 60062. All rights reserved. No part of this article or PDFby the American College of Chest Physicians, 3300 Dundee Road,
2009Physicians. It has been published monthly since 1935. Copyright CHEST is the official journal of the American College of Chest
© 2009 American College of Chest Physicians by Gustavo Medrano on November 1, 2009chestjournal.chestpubs.orgDownloaded from

Safety and Efficacy of CombinedLong-Acting �-Agonists and InhaledCorticosteroids vs Long-Acting�-Agonists Monotherapy for Stable COPDA Systematic Review
Gustavo J. Rodrigo, MD; Jose A. Castro-Rodriguez, MD, PhD;and Vicente Plaza, MD
Background: Current guidelines recommend the use of inhaled corticosteroids (ICSs) added tolong-acting �2-agonists (LABAs) for treatment of symptomatic patients with severe and verysevere COPD. However, the evidence has been inconclusive. The aim of this review was to assessthe safety and efficacy of LABAs/ICSs compared with LABA monotherapy for patients withmoderate-to-very severe COPD.Methods: Systematic searches were conducted on MEDLINE, EMBASE, the Cochrane Con-trolled Trials Register, and the trial registers of manufacturers, without language restriction.Primary outcomes were COPD exacerbations and mortality. Secondary outcomes included lungfunction, health-related quality of life, and adverse effects.Results: Eighteen randomized controlled trials (12,446 participants) were selected. Therapy withLABAs/ICSs did not decrease the number of severe exacerbations (relative risk [RR], 0.91; 95% CI,0.82 to 1.01; I2 � 1%), or all-cause mortality (RR, 0.90; 95% CI, 0.76 to 1.06; I2 � 0%), respiratorymortality (RR, 0.80; 95% CI, 0.61 to 1.05; I2 � 0%), and cardiovascular mortality (RR, 1.22; 95% CI,0.88 to 1.71; I2 � 0%). To the contrary, the number of moderate exacerbations (RR, 0.84; 95% CI,0.74 to 0.96; I2 � 50%) and the St. George respiratory questionnaire total score (weighted meandifference, �1.88; 95% CI, �2.44 to �1.33; I2 � 29%) were significantly reduced with LABA/ICStherapy. Although therapy with LABAs/ICSs increases FEV1 significantly (0.06 and 0.04 L, respec-tively), they were associated with an increased risk of pneumonia (RR, 1.63; 95% CI, 1.35 to 1.98;I2 � 20%).Conclusions: Compared with LABA monotherapy, the magnitude of the benefits of LABA/ICStherapy did not reach that of the criteria for predefined clinically important effects and wereassociated with serious adverse effects. (CHEST 2009; 136:1029–1038)
Abbreviations: ICS � inhaled corticosteroid; LABA � long-acting �2-agonist; MI � myocardial infarction; NNTB �number needed to treat for benefit; NNTH � number needed to treat for harm; RR � relative risk; SABA � short-acting�2-agonist; SGRQ � St. George respiratory questionnaire; WMD � weighted mean difference
COPD is a preventable and treatable disease thatis characterized by airflow limitation that is not
fully reversible.1,2 The main therapeutic goals are toprevent and control symptoms, reduce the frequencyand severity of exacerbations, and improve healthstatus and exercise tolerance. Current guidelines1,2
recommend a stepwise increase in treatment, de-pending on the severity of the disease. Short-actinginhaled bronchodilators (short-acting �2-agonists[SABAs] and anticholinergic agents) are recom-
mended for the relief of symptoms on an as-neededbasis, whereas long-acting inhaled bronchodilators(long-acting �2-agonists [LABAs] or tiotropium) ina regularly scheduled regimen are recommendedas first-line therapy in symptomatic patients withmoderate-to-very severe COPD.
Evidence3 shows that LABA monotherapy is asso-ciated with significant improvements regardingCOPD exacerbations, pulmonary function, qualityof life, and use of rescue medication, with a low
CHEST Original ResearchCOPD
www.chestjournal.org CHEST / 136 / 4 / OCTOBER, 2009 1029
© 2009 American College of Chest Physicians by Gustavo Medrano on November 1, 2009chestjournal.chestpubs.orgDownloaded from

incidence of adverse effects. However, in view of themulticomponent nature of COPD, the use of inhaledcorticosteroids (ICSs), particularly in combinationwith a LABA has obtained widespread acceptanceamong clinicians. In fact, the addition of ICSs inpatients with severe or very severe disease (stages IIIor IV) with repeated exacerbations is recommendedfor decreasing exacerbation rates, and improvinglung function and health status.1,2 Nevertheless, theevidence of the superiority of combination therapy(LABAs/ICSs) over LABA monotherapy has beeninconclusive. While a 2007 review4 failed to demon-strate the superiority of combination therapy overLABA monotherapy in reducing COPD exacerba-tions, others have reported5–7 some benefits of ther-apy with LABAs/ICSs in terms of COPD exacerba-tions, pulmonary function, and quality of life. Evenso, these conclusions might be questionable becausethey are based on a reduced number of selectedstudies and outcomes. Consequently, we performeda systematic review to assess the safety and efficacyof the use of LABAs/ICSs in COPD patients com-pared with LABA monotherapy. The following twospecific questions were identified: (1) what are therisks of adding an ICS to a LABA compared withLABAs monotherapy? and (2) does therapy withLABAs/ICSs provide significant clinical benefitscompared with LABA monotherapy?
Materials and Methods
Search Strategy and Selection Criteria
We identified studies from MEDLINE, EMBASE (January1980 to May 2009), and the Cochrane Controlled Trials Register(second quarter of 2009) databases by using the following MeSH,full text, and keywords terms: (long-acting �2 adrenoceptoragonist OR salmeterol OR formoterol OR inhaled corticoste-roids OR fluticasone OR budesonide OR beclomethasone)AND (COPD OR chronic bronchitis OR emphysema). Also,we performed a search of relevant files from AstraZeneca
(www.astrazenecaclinicaltrials.com) and GlaxoSmithKline (www.gsk-clinicalstudyregister.com) databases. Trials published solelyin abstract form were excluded because the methods and resultscould not be fully analyzed.
The specific inclusion criteria were as follows: (1) stable adultpatients aged � 40 years with COPD satisfying the diagnosticcriteria of the American Thoracic Society/European RespiratorySociety1 or the Global Initiative for Chronic Obstructive LungDisease2; (2) therapy with inhaled LABAs plus ICSs (deliveredvia metered-dose inhaler or dry powder inhaler) as the interven-tion arm compared with therapy with a LABA; (3) study dura-tions of � 1 month; (4) randomized controlled trials (parallel-group design) without language restriction; and (5) primaryoutcomes “severe COPD exacerbation” (requiring hospitalizationor withdrawals) and “moderate COPD exacerbations” (requiringsystemic corticosteroids or antibiotic use), all-cause mortality(deaths for any cause), respiratory deaths (deaths due to arespiratory event such as COPD exacerbation or pneumonia),and cardiovascular mortality (including sudden death) during thetreatment period. Secondary outcome measures were as follows:mean change in FEV1 (pre-bronchodilator therapy and post-bronchodilator therapy); mean change from baseline in the St.George respiratory questionnaire (SGRQ) total score8; end-of-treatment dyspnea score; withdrawals from the study during thetreatment period (overall, due to adverse effects, and due to lackof efficacy); and adverse effects (pneumonia, oropharyngealcandidiasis, viral respiratory infections, and myocardial infarc-tions [MIs]).
Data Abstraction and Validity Assessment
Titles, abstracts, and citations were independently analyzed byall reviewers. From full text, they independently assessed studiesfor inclusion based on the criteria for population, intervention,study design, and outcomes. Three reviewers (G.J.R., J.C.R., andV.P.) were independently involved in all stages of study selection,data extraction, and quality assessment. Any disagreement wasresolved by consensus. In case of multiple published or unpub-lished reports for a particular study, data from the most recentversion were extracted.
Statistical Analysis
Binary outcomes were pooled by using common relative risks(RRs) and 95% CIs. If pooled effect estimates were significantlydifferent between groups, we calculated the number needed totreat for benefit (NNTB) or the number needed to treat for harm(NNTH). For continuous outcomes, the standardized meandifference or weighted mean difference (WMD) and 95% CIswere calculated. Heterogeneity was further measured by usingthe I2 test.9 With low heterogeneity (I2 � 40%), data werecombined by mean of a fixed-effects model10; otherwise, arandom-effects model was used. Publication bias of primaryoutcomes was evaluated by means of the visual inspection offunnel plots.11 A predefined sensitivity analysis of the primaryoutcome of severe COPD exacerbations was conducted to ex-plore the influence of the following factors: concealment alloca-tion12 (adequate vs unclear); trial duration (long-term [� 52weeks] vs short-term [� 52 weeks]); reversibility to SABA (poorlyreversible patients or FEV1 � 15% from baseline vs reversiblepatients or FEV1 � 15% from baseline); choice of LABAs(salmeterol vs formoterol); and the use of ICSs before thepatients were enrolled (� 50% of patients vs � 50% of patients).Subgroups were compared by using the interaction test.13 Ap value of � 0.05 using a two-tailed test was considered toindicate significance. Metaanalyses were performed with using a
Manuscript received April 2, 2009; revision accepted July 2, 2009.Affiliations: From the Departamento de Emergencia (Dr. Ro-drigo), Hospital Central de las Fuerzas Armadas, Montevideo,Uruguay; the School of Medicine (Dr. Castro-Rodriguez), Pon-tificia Universidad Catolica de Chile, Santiago, Chile; and Serveide Pneumologia (Dr. Plaza), Hospital de la Santa Creu i SantPau, Universitat Autonoma de Barcelona, Barcelona, Spain.Funding/Support: The funding for this study came from salarysupport for Dr. Rodrigo. No sponsorship from institutions orpharmaceutical industry was provided to conduct this study.Correspondence to: Gustavo J. Rodrigo, MD, Departamentode Emergencia, Hospital Central de las Fuerzas Armadas, Av 8de Octubre 3020, Montevideo 11600, Uruguay; e-mail: [email protected]© 2009 American College of Chest Physicians. Reproductionof this article is prohibited without written permission from theAmerican College of Chest Physicians (www.chestjournal.org/site/misc/reprints.xhtml).DOI: 10.1378/chest.09-0821
1030 Original Research
© 2009 American College of Chest Physicians by Gustavo Medrano on November 1, 2009chestjournal.chestpubs.orgDownloaded from

statistical software package (Review Manager, version 5.0.20; theNordic Cochrane Centre, the Cochrane Collaboration; Copen-hagen, Denmark).
Results
Of 164 potential relevant citations, 18 randomized,controlled trials14–31 fulfilled the inclusion crit-eria (Fig 1). Five trials were unpublished.27–31 Dataanalysis was restricted to the LABAs/ICSs andLABAs arms of those trials (12,446 patients) [Table1]. Five studies used formoterol/budesonide combi-nation therapy,17,20,26,27 and 13 studies used salmet-erol/fluticasone combination therapy.14–16,18,19,21–31
Seven studies14–16,21,23,24,31 evaluated therapy withinhaled fluticasone in combination with salmeterolat a dosage of 500 �g twice daily, seven stud-ies18,19,22,25,28–30 assessed therapy with fluticasone ata dosage of 250 �g twice daily, and four stud-ies17,20,26,27 evaluated therapy with budesonide at adosage of 320 �g twice daily. All trials used singleinhalers containing both ICSs and LABAs to deliver thecombined therapy. Eleven trials15–21,23–26 reported thata mean of 31% of patients (range, 0 to 55% of patients)had received ICSs before they were enrolled in thestudy. There were 11 long-term trials (ie, � 52
weeks)16–18,20,21,23–25,27–29 and 7 short-term trials (ie,� 52 weeks).14,15,19,22,26,30,31 Studies enrolled mostlystable patients with COPD who met the Global Initia-tive for Chronic Obstructive Lung Disease criteria formoderate-to-very severe COPD exacerbations.2 Themean age of patients was 64 years (72% of patientswere male), with an average baseline FEV1 of 40% ofpredicted normal values. Allocation concealment wasadequate in only 5 studies,16,20,21,23,24 and was unclearin the remaining 13 studies.
Primary Outcomes
Compared with LABA monotherapy, combinationtherapy with LABAs/ICSs did not significantlydecrease the risk of severe COPD exacerbations(11.3% vs 12.5%, respectively) [Table 2]. The posthoc subgroup analysis did not show significant dif-ferences in COPD exacerbations regarding conceal-ment allocation, trial duration, reversibility to SABAuse, LABA choice, and use of ICSs before thepatients were enrolled in the study (Table 3). To thecontrary, the use of LABAs/ICSs was associated witha significantly reduced risk of moderate COPDexacerbations when compared with LABAs alone(17.5% vs 20.1%, respectively), with evidence ofstatistical heterogeneity among trials. The NNTBwas 31 (95% CI, 20 to 93).
Patients receiving therapy with LABAs/ICSs werenot associated with a significant decrease of overallmortality when compared with those receivingLABAs alone (4.5% vs 5.5%, respectively) [Fig 2]. Inthe same way, the metaanalysis did not showsignificant differences between groups regardingthe risk of respiratory deaths (1.8% in the LABAs/ICSs group vs 2.4% in the LABAs group) andcardiovascular mortality (1.6% vs 1.4%, respectively),without evidence of statistical heterogeneity (Fig 2).On visual inspection of the funnel plots (Fig 3),publication bias could be ruled out for all-cause,respiratory, and cardiovascular mortality. To thecontrary, for severe COPD exacerbations, the plotpresented an asymmetrical shape with an absence ofsmall studies showing a group benefit for therapywith LABAs.
Secondary Outcomes
Regarding pulmonary function, patients treatedwith LABAs/ICSs showed significantly greater in-creases in the mean change in FEV1 from baseline(pre-bronchodilator therapy and post-bronchodilatortherapy) compared with patients treated with LABAsalone (Table 4); however, both comparisons showedstatistical heterogeneity. Patients receiving therapywith LABAs/ICSs showed a significantly greaterreduction in the SGRQ total score. Finally, at the
Figure 1. Flowchart for identification of studies.
www.chestjournal.org CHEST / 136 / 4 / OCTOBER, 2009 1031
© 2009 American College of Chest Physicians by Gustavo Medrano on November 1, 2009chestjournal.chestpubs.orgDownloaded from

Table 1—Characteristics of Included Studies
StudiesStudy Location/
DurationPatients: No.
(% male)
MeanAge,
yrMean Baseline
FEV1
CurrentSmoker
BronchodilatorResponse, %
Intervention:Dose
AllocationConcealment
Cazzola et al14 Single-center/12 wk S: 20 (90) 65 1.15 L 45 pack-yr � 12 S: 50 �g twiceMDI
Unclear
SF: 40 (92) 64 1.16 L 44 pack-yr � 12 SF: 50/250 or50/500 �gtwice MDI
Mahler et al15 69 centers/24 wk S: 160 (64) 64 40% predicted 46% 21 S: 50 �g twiceDPI
Unclear
SF: 165 (62) 63 41% predicted 46% 21 SF: 50/500 �gtwice DPI
Calverley et al16 196 centers/52 wk S: 372 (70) 63 46% predicted 51% 3.7 S: 50 �g twiceDPI
Adequate
SF: 358 (75) 63 49% predicted 52% 4.0 SF: 50/500 �gtwice DPI
Calverley et al17 109 centers/52 wk F: 255 (75) 63 36% predicted 36% 6 F: 9 �g twiceDPI
Unclear
FB: 254 (78) 64 36% predicted 33% 6 FB: 9/320 �gtwice DPI
Dal Negroet al18
Single-center/52 wk S: 6 (100) 55–78 48% predicted 0% 3 S: 50 �g twiceDPI
Unclear
SF: 5 (83) 53–77 50% predicted 0% 3.5 SF: 50/ 250 �gtwice DPI
Hanania et al19 75 centers/24 wk S: 177 (58) 64 42% predicted 51% 20 S: 50 �g twiceDPI
Unclear
SF:178 (61) 63 41% predicted 43% 19 SF: 50/250 �gtwice DPI
Szafranski et al20 89 centers/52 wk F: 201 (76) 63 36% predicted 38% 6 F: 9 �g twiceDPI
Adequate
FB:208 (76) 64 36% predicted 30% 6 FB: 9/320 �gtwice DPI
Wouters et al21 39 centers/52 wk S: 184 (75) 64 1.41 L 35% 4 S: 50 �g twiceDPI
Adequate
SF: 189 (73) 63 1.41 L 39% 4 SF: 50/500 �gtwice DPI
O’Donnellet al22
21 centers/8 wk S: 59 (75) 65 40% predicted 34% 18 S: 50 �g twiceDPI
Unclear
SF: 62 (69) 63 42% predicted 42% 18 SF: 50/250 �gtwice DPI
Calverley et al23 444 centers/156 wk S: 1,521 (76) 65 44% predicted 43% 4 S: 50 �g twiceDPI
Adequate
SF: 1,533 (75) 65 44% predicted 43% 4 SF: 50/500 �gtwice DPI
Kardos et al24 95 centers/ 44 wk S: 487 (78) 64 40% predicted 37% 7 S: 50 �g twiceDPI
Adequate
SF: 507 (74) 64 40% predicted 37% 6 SF: 50/500 �gtwice DPI
Ferguson et al25 94 centers/52 wk S: 388 (52) 65 33% predicted 38% NA S: 50 �g twiceDPI
Unclear
SF: 394 (58) 65 33% predicted 40% NA SF: 50/250 �gDPI twice
Tashkin et al26 194 centers/26 wk F: 284 (66) 64 39% predicted 42% NA F: 9 �g twiceDPI
Unclear
FB: 845 (69) 63 39% predicted 44% NA FB: 9/160 �g or320/9 �gtwice MDI
D-5899C0000127
237 centers/52 wk F: 495 (65) 63 34% predicted 41% 16 F: 9 �g twiceDPI
Unclear
FB: 988 (63) 64 34% predicted 36% 16 FB: 9/320 �g or160/9 MDItwice
(Continued)
1032 Original Research
© 2009 American College of Chest Physicians by Gustavo Medrano on November 1, 2009chestjournal.chestpubs.orgDownloaded from
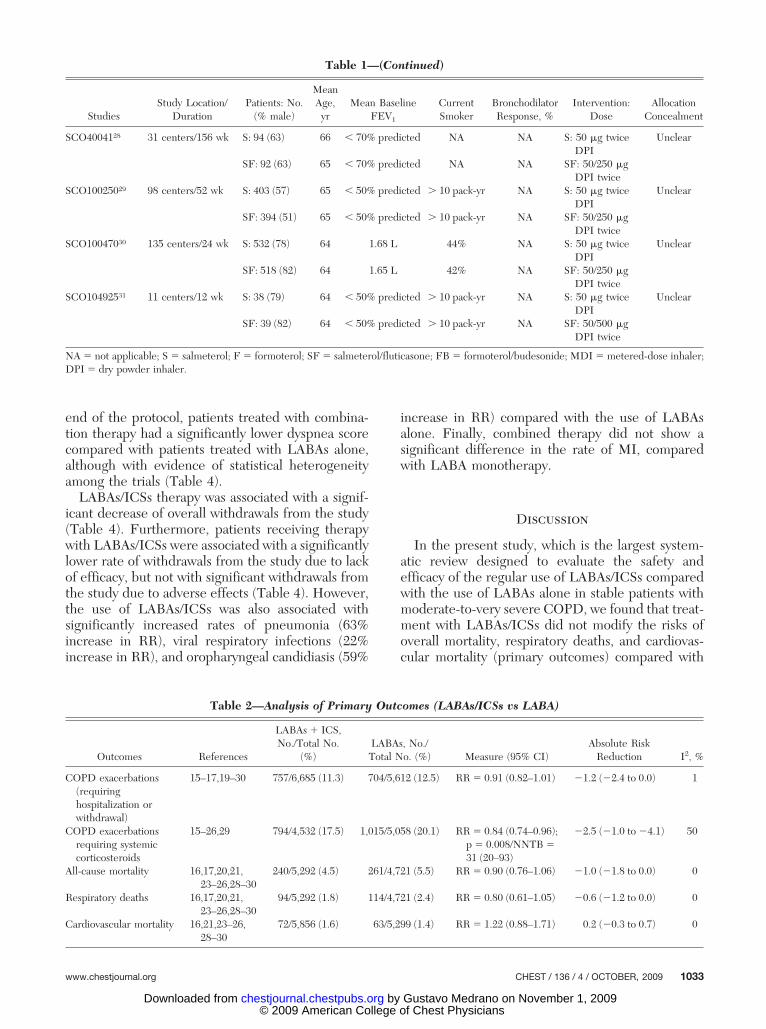
end of the protocol, patients treated with combina-tion therapy had a significantly lower dyspnea scorecompared with patients treated with LABAs alone,although with evidence of statistical heterogeneityamong the trials (Table 4).
LABAs/ICSs therapy was associated with a signif-icant decrease of overall withdrawals from the study(Table 4). Furthermore, patients receiving therapywith LABAs/ICSs were associated with a significantlylower rate of withdrawals from the study due to lackof efficacy, but not with significant withdrawals fromthe study due to adverse effects (Table 4). However,the use of LABAs/ICSs was also associated withsignificantly increased rates of pneumonia (63%increase in RR), viral respiratory infections (22%increase in RR), and oropharyngeal candidiasis (59%
increase in RR) compared with the use of LABAsalone. Finally, combined therapy did not show asignificant difference in the rate of MI, comparedwith LABA monotherapy.
Discussion
In the present study, which is the largest system-atic review designed to evaluate the safety andefficacy of the regular use of LABAs/ICSs comparedwith the use of LABAs alone in stable patients withmoderate-to-very severe COPD, we found that treat-ment with LABAs/ICSs did not modify the risks ofoverall mortality, respiratory deaths, and cardiovas-cular mortality (primary outcomes) compared with
Table 2—Analysis of Primary Outcomes (LABAs/ICSs vs LABA)
Outcomes References
LABAs � ICS,No./Total No.
(%)LABAs, No./Total No. (%) Measure (95% CI)
Absolute RiskReduction I2, %
COPD exacerbations(requiringhospitalization orwithdrawal)
15–17,19–30 757/6,685 (11.3) 704/5,612 (12.5) RR � 0.91 (0.82–1.01) �1.2 (�2.4 to 0.0) 1
COPD exacerbationsrequiring systemiccorticosteroids
15–26,29 794/4,532 (17.5) 1,015/5,058 (20.1) RR � 0.84 (0.74–0.96);p � 0.008/NNTB �31 (20–93)
�2.5 (�1.0 to �4.1) 50
All-cause mortality 16,17,20,21,23–26,28–30
240/5,292 (4.5) 261/4,721 (5.5) RR � 0.90 (0.76–1.06) �1.0 (�1.8 to 0.0) 0
Respiratory deaths 16,17,20,21,23–26,28–30
94/5,292 (1.8) 114/4,721 (2.4) RR � 0.80 (0.61–1.05) �0.6 (�1.2 to 0.0) 0
Cardiovascular mortality 16,21,23–26,28–30
72/5,856 (1.6) 63/5,299 (1.4) RR � 1.22 (0.88–1.71) 0.2 (�0.3 to 0.7) 0
Table 1—(Continued)
StudiesStudy Location/
DurationPatients: No.
(% male)
MeanAge,
yrMean Baseline
FEV1
CurrentSmoker
BronchodilatorResponse, %
Intervention:Dose
AllocationConcealment
SCO4004128 31 centers/156 wk S: 94 (63) 66 � 70% predicted NA NA S: 50 �g twiceDPI
Unclear
SF: 92 (63) 65 � 70% predicted NA NA SF: 50/250 �gDPI twice
SCO10025029 98 centers/52 wk S: 403 (57) 65 � 50% predicted � 10 pack-yr NA S: 50 �g twiceDPI
Unclear
SF: 394 (51) 65 � 50% predicted � 10 pack-yr NA SF: 50/250 �gDPI twice
SCO10047030 135 centers/24 wk S: 532 (78) 64 1.68 L 44% NA S: 50 �g twiceDPI
Unclear
SF: 518 (82) 64 1.65 L 42% NA SF: 50/250 �gDPI twice
SCO10492531 11 centers/12 wk S: 38 (79) 64 � 50% predicted � 10 pack-yr NA S: 50 �g twiceDPI
Unclear
SF: 39 (82) 64 � 50% predicted � 10 pack-yr NA SF: 50/500 �gDPI twice
NA � not applicable; S � salmeterol; F � formoterol; SF � salmeterol/fluticasone; FB � formoterol/budesonide; MDI � metered-dose inhaler;DPI � dry powder inhaler.
www.chestjournal.org CHEST / 136 / 4 / OCTOBER, 2009 1033
© 2009 American College of Chest Physicians by Gustavo Medrano on November 1, 2009chestjournal.chestpubs.orgDownloaded from

treatment with LABAs alone. On the contrary, theanalysis of secondary outcomes showed that therapywith LABAs/ICSs significantly increased the risk ofpneumonia, oropharyngeal candidiasis, and viral re-spiratory infections (question 1). However, it isinteresting to point out that these adverse effectswere not accompanied by a concomitant and propor-tional increase in respiratory-related mortality or over-all mortality. Concerning the benefits (question 2), wefound that therapy with LABAs/ICSs significantlydecreased the frequency of moderate COPD exac-erbations independently of concealment allocation,trial duration, reversibility to SABA therapy, LABAchoice, and previous use of ICSs.
In the same way, therapy with LABAs/ICSs wasassociated with significant increases in the meanchange in pre-bronchodilator therapy and post-bronchodilator therapy FEV1, the mean change inSGRQ total score, and with a significant decrease inthe end-of-treatment dyspnea score compared withtreatment with LABAs alone. However, given thatthe size of these benefits did not reach the suggestedclinically important minimal differences (FEV1, 0.10to 0.14 L; SGRQ score, 4-unit decrement),32 therelevance of these improvements seems uncertain.In the same way, the 16% decrease in the rate ofmoderate COPD exacerbations was smaller than thesuggested threshold value of 22% for clinical signif-icance.32 Conversely, treatment with LABAs/ICSsfailed to significantly reduce the risk of severeCOPD exacerbations. These facts suggest a limitedextra efficacy when ICSs were added to LABAs forCOPD treatment.
The relative benefits of therapy with LABAs/ICSsmust be weighed against the risks. Thus, the mostconcerning side effect was the increase in the risk ofpneumonia associated with the administration of
ICSs added to LABAs. The precise mechanism isuncertain, but it could be related to the fact thatICSs achieve locally high concentrations in the lung,increasing the risk of pneumonia due to their immu-nosuppressive effects.33 Thus, inhaled fluticasone atdosages of 1,000 �g/d exerts effects on serum corti-sol levels that are equivalent to 10 mg of prednisone,a dose that may double the risk of pneumonia inpatients with arthritis.34 Our analysis showed anincrease in the risk of pneumonia with both moder-ate dosages of fluticasone (500 �g/d; RR, 1.75; 95%CI, 1.16 to 2.64; I2 � 30%) and high dosages offluticasone (1,000 �g/d; RR � 1.64; 95% CI, 1.32 to2.06, I2 � 22%). To the contrary, therapy withLABAs/ICSs was associated with significant de-creases in overall withdrawals and withdrawals dueto lack of efficacy compared with LABA mono-therapy. This finding could be associated with thefact that therapy with LABAs/ICSs significantly re-duces dyspnea with a greater clinical effectivenessperception. Also, this fact could be associated withbetter control of the disease.
When we compared the results of the presentmetaanalysis with those of previous reviews (basedon a limited number of published trials), we foundsome similarities and few differences. For example, aCochrane review5 of 10 studies, reported a signifi-cant RR reduction of moderate COPD exacerbationsof 18% with the combined treatment with LABAs/ICSs compared with treatment with LABAs alone.Also, the combination therapy was more effectivethan that with LABAs alone in improving qualityof life as measured by the SGRQ (�1.64 points),and predose and postdose FEV1 (0.06 and 0.05 L,respectively). While there was no significant dif-ference in terms of overall mortality, pneumoniaoccurred more commonly in patients receiving
Table 3—Sensitivity Analysis. Comparisons Between RR in COPD Exacerbations Requiring Hospitalization orWithdrawal) Stratified by Concealment Allocation (Adequate vs Unclear), Trial Duration (Long-Term > 52 Weeksvs Short-Term < 52 Weeks), Reversibility to SABAs (Poorly Reversible Patients or FEV1 < 15% From Baseline vs
Reversible Patients or FEV1 > 15%), Baseline Severity (Moderate to Severe vs Severe to Very Severe), LABAschoice (Salmeterol vs Formoterol), and Use of ICSs Before the Patients Were Enrolled (< 50% of Patients vs < 50%
of Patients)
Subgroup Comparisons RR (95% CI) �I2Interactive Test17
RR (95% CI) p Value
Adequate16,20,21,23,24 vs unclearconcealment14,15,17–19,22,25–31
0.93 (0.82–1.05) �35% vs 0.90 (0.77–1.05) �0% 0.96 (0.79–1.18) 0.74
Long-term16,17,20,21,23,25,27–29 vsshort-term15,19,22,24,26,30
0.93 (0.84–1.03) �1% vs 0.80 (0.59–1.11) �0% 0.86 (0.61–1.19) 0.37
Poorly reversible16,17,20,21,23,24 vsreversible15,19,22,25–30
0.90 (0.80–1.01) �0% vs 0.94 (0.74–1.20) �0% 1.04 (0.79–1.36) 0.75
Salmeterol15,16,19,21–25,28–30 vsFormoterol17,20,26,27
0.94 (0.84–1.05) �0% vs 0.87 (0.73–1.04) �41% 0.92 (0.75–1.14) 0.46
Previous use of ICS (� 50%16, 24,26 vs� 50% of patients15,17–21,23–25)
0.84 (0.65–1.14) �28% vs 0.92 (0.88–1.04), �31% 1.06 (0.79–1.43) 0.65
1034 Original Research
© 2009 American College of Chest Physicians by Gustavo Medrano on November 1, 2009chestjournal.chestpubs.orgDownloaded from

combined therapy (58% increase in RR). How-ever, another metaanalysis4 that was limited to fiveEnglish-language trials failed to demonstrate thesuperiority of combination treatment over LABAmonotherapy in reducing COPD exacerbations andoverall mortality.
More recently, Sobieraj et al7 on the basis of sevenstudies reported that therapy with LABAs/ICSs de-creased the risk of moderate COPD exacerbations(relative reduction risk of 18%), decreased theSGRQ total score (�1.98 points), and increased therisk of pneumonia (32% increase in RR) compared
with therapy with LABAs alone. Additionally, com-bined therapy also showed a reduced risk in overallwithdrawals (17% increase in RR), and withoutdifference in the rate of overall mortality betweengroups. Another systematic review35 has found noevidence that therapy with LABAs alone is moreeffective than combined therapy with LABAs/ICSs.In the same study, a subgroup analysis showed that,when added to LABAs, ICSs significantly reducedthe number of exacerbations in patients with FEV1� 40% predicted. However, these conclusions areuncertain because the review was based on only
Figure 2. Pooled RR for overall mortality, respiratory deaths, and cardiovascular mortality (with 95%CIs) of eligible studies comparing inhaled LABAs/ICSs with LABAs.
www.chestjournal.org CHEST / 136 / 4 / OCTOBER, 2009 1035
© 2009 American College of Chest Physicians by Gustavo Medrano on November 1, 2009chestjournal.chestpubs.orgDownloaded from

seven studies15–17,19,20,23,24 (6,376 patients withCOPD). Finally, Singh et al36 showed a significantlyincreased risk of pneumonia with combined therapycompared with LABA monotherapy (32% increase inRR) without a significantly increased risk of death.Interestingly, the risk of pneumonia could be specif-ically attributed to the use of ICSs because the riskfor pneumonia associated with ICS use was similarwhen therapy with ICSs were compared with pla-cebo or when ICSs were added to therapy withLABAs and compared with LABA therapy alone. Inthe same way, a recent trial37 comparing therapywith inhaled tiotropium with therapy with salmet-erol/fluticasone in patients with COPD showed anincreased hazard ratio for time to reported pneumo-nia for combined therapy of � 2 years (94% increasein RR).
This review was performed according to the meth-odological criteria suggested for scientific reviews.38
The fact that there was low evidence of clinical andstatistical heterogeneity between studies increasedthe confidence of our findings. Furthermore, therewas no evidence of publication bias in the majority ofprimary outcomes. However, our metaanalysis had
several potential limitations that came from thequality of the reported data. Thus, the trials did notconsistently use similar definitions of COPD exacer-bations or pneumonia. In particular, we recognizedthat the severity of exacerbations is a complex con-cept constituted by several factors, and that this factcould modify our results. Also, most of the studieswere not specifically designed to monitor outcomesas all-cause, respiratory, or cardiovascular mortality.Additionally, the risk of bias was unclear in 13 trialsin the analysis. Also, the fact that 80% of thereviewed patients were men limits the applicabilityof the results since COPD is suspected to affect menand women equally.
This metaanalysis confirms and extends data fromprevious reviews. The main results of our review areas follows: LABAs/ICSs did not decrease the risk ofall-cause, respiratory, and cardiovascular mortality;however, therapy with LABAs/ICSs increases therisk of pneumonia, oropharyngeal candidiasis, andviral respiratory infections. The use of LABAs/ICSswas associated with a lower incidence of moderateCOPD exacerbations (but not of severe exacerba-tions), increased pulmonary function, improved dys-
Figure 3. Funnel plots of LABAs/ICSs vs LABAs comparing COPD severe exacerbations (A), all-cause mortality (B), respiratory deaths (C),and cardiovascular mortality (D).
1036 Original Research
© 2009 American College of Chest Physicians by Gustavo Medrano on November 1, 2009chestjournal.chestpubs.orgDownloaded from

pnea, and health-related quality-of-life total scores.However, the magnitude of these benefits did notreach the recent predefined criteria to be clinicalimportant.32
Current guidelines1,2 recommend the use ofICSs in combination with LABAs to reduce thefrequency of exacerbations in symptomatic pa-tients with severe and very severe COPD. Further-more, some authors39 have suggested that, in COPDpatients as in asthma patients, concomitant ICStherapy is preferable over LABA monotherapy. Nev-ertheless, this review suggests that combinationtherapy with LABAs/ICSs presents a borderlinestatistical and limited clinical significance comparedwith LABA monotherapy. Moreover, combinationtherapy offers no statistically significant additionalsurvival benefit and increased the risk of seriousadverse effects. Even so, this last issue requiresfurther prospective evaluation in large studies usingobjective definitions of pneumonia. It is likely thatmost patients with COPD with these levels of sever-ity should be treated only with LABA monotherapy.However, it is possible also that a future definition ofdifferent COPD phenotypes will allow us to knowwhich patients can benefit from ICSs, and whichshould only be treated with LABAs. Thus, patientswho benefit from combination therapy with LABAs/ICSs could be those patients with steroid-responsiveeosinophilic bronchitis.
Acknowledgments
Author contributions: Dr. Rodrigo (1) has made substantialcontributions to conception and design, acquisition of data, andanalysis and interpretation of data; (2) has drafted the submittedarticle and revised it critically for important intellectual content;and (3) has provided final approval of the version of the article tobe published. Dr. Castro-Rodriguez (1) has made substantialcontributions to conception and design, and interpretation ofdata; (2) has revised the article critically for important intellectualcontent; and (3) has provided final approval of the version to bepublished. Dr. Plaza (1) has made substantial contributions toconception and design, and interpretation of data; (2) has revisedthe article critically for important intellectual content; and (3) hasprovided final approval of the version to be published.Financial/nonfinancial disclosures: Dr. Rodrigo has partici-pated as a lecturer and speaker in scientific meetings and coursesunder the sponsorship of Boehringer Ingelheim, GlaxoSmithKline,AstraZeneca, Dr. Esteve SA, and Merck Sharp and Dome. Dr.Castro-Rodriguez has participated as a lecturer and speaker inscientific meetings and courses under the sponsorship of MerckSharp and Dohme, GlaxoSmithKline, and Grunenthal; and asmember of the advisory board for GlaxoSmithKline. Dr. Plaza hasparticipated as a lecturer and speaker in scientific meetings andcourses under the sponsorship of AstraZeneca, GlaxoSmithKline,Dr. Esteve SA, and Merck Sharp and Dohme.
References1 Celli BR, MacNee W, ATS/ERS Task Force. Standards for the
diagnosis and treatment of patients with COPD: a summary ofthe ATS/ERS position paper. Eur Respir J 2004; 23:932–946
2 Global Initiative for Chronic Obstructive Lung Disease. Globalstrategy for the diagnosis, management and prevention of
Table 4—Analysis of Secondary Outcomes (LABAs/ICSs vs LABAs)
Outcomes References
LABAs � ICSs,No./Total No.
(%)LABAs, No./Total No. (%) Measure (95% CI) �p Value
Absolute RiskReduction I2, %
Mean change inpre-bronchodilatortherapy FEV1, L
14–16,19,21–27,29–30
5,613 5,082 WMD � 0.06 (0.04–0.07)�0.0001
82
Mean change inpost-bronchodilatortherapy FEV1, L
14–16,19,22,23,26,27
3,455 2,501 WMD � 0.04 (0.02–0.05)�0.0001
64
Mean change inSGRQ
16,17,20,23–26,30
4,617 4,040 WMD � �1.88 (�2.44 to �1.33)�0.0001
29
End-of-treatmentdyspnea score
15,16,19,21,22,24–26,30
3,216 2,643 SMD � �0.20 (�0.25 to �0.15)�0.0001
82
Total withdrawals 14–17,19–31 1,731/5,919 (29.2) 1,731/5,919 (29.2) RR � 0.87 (0.82–0.92) �0.0001;NNTB � 25 (18–41)
�1.6 (�0.2 to �3.0) 0
Withdrawals due toadverse effects
15,16, 19–21,23–26,28–30
680/5,381 (12.6) 654/4,803 (13.6) RR � 0.93 (0.84–1.03) �0.26 �1.0 (�0.3 to 2.3) 0
Withdrawals due tolack of efficacy
15,16,23,25,29,30
63/3,362 (1.9) 117/3,376 (3.5) RR � 0.54 (0.40–0.72) �0.0001;NNTB � 73 (56–120)
�1.6 (�0.8 to �2.4) 0
Pneumonia 15,16,19,21,23–26,28–31
263/5,212 (5.0) 153/4,540 (3.4) RR � 1.63 (1.35–1.98) �0.0001;NNTH � 40 (26–72)
1.7 (0.9 to 2.5) 20
Oropharyngealcandidiasis
16,19,21,22,24,26,27,29
292/3,521 (8.4) 200/2,741 (7.2) RR � 1.59 (1.07–2.37) �0.002;NNTH � 22 (10–179)
1.2 (0.1 to 2.3) 65
Viral respiratoryinfections
15–17,19,22,23,25,27,29,30
441/4,844 (9.1) 342/4,362 (7.8) RR � 1.22 (1.07–1.39) �0.004;NNTH � 57 (33–179)
1.3 (0.1 to 2.4) 0
MI 16,23–25,28,29 34/3,278 (1.0) 33/3,265 (1.0) RR � 1.03 (0.64–1.64) �0.91 0 (�0.5 to 0.5) 13
SMD � standardized mean difference.
www.chestjournal.org CHEST / 136 / 4 / OCTOBER, 2009 1037
© 2009 American College of Chest Physicians by Gustavo Medrano on November 1, 2009chestjournal.chestpubs.orgDownloaded from

COPD. Available at: www.goldcopd.org. Accessed August 27,2009
3 Rodrigo GJ, Nannini LJ, Rodriguez-Roisín R. Safety oflong-acting �-agonists in stable COPD: a systematic review.Chest 2008; 133:1079–1087
4 Wilt TJ, Niewoehner D, MacDonald R, et al. Management ofstable chronic obstructive pulmonary disease: a systematicreview for a clinical practice guideline. Ann Intern Med 2007;147:639–653
5 Nannini LJ, Cates CJ, Lasserson TJ, et al. Combined corticoste-roid and long-acting �-agonist in one inhaler versus long-acting�-agonists for chronic obstructive pulmonary disease. CochraneDatabase Syst Rev (database online). Issue 4, 2007
6 Hanania NA. The impact of inhaled corticosteroid and long-acting �-agonist combination therapy on outcomes in COPD.Pulm Pharmacol Ther 2008; 21:540–550
7 Sobieraj DM, White M, Coleman CI. Benefits and risks ofadjunctive inhaled corticosteroids in chronic obstructive pulmo-nary disease: a meta-analysis. Clin Ther 2008; 30:1416–1425
8 Jones PW, Quirk FH, Baveystock CM. The St. George’srespiratory questionnaire. Respir Med 1991; 85:25–31
9 Higgins JPT, Thompson SG, Deecks JJ, et al. DG. Measuringinconsistency in meta-analyses. BMJ 2003; 327:557–560
10 Mantel N, Haenszel W. Statistical aspects of the analysis ofdata from retrospective studies of disease. J Natl Cancer Inst1959; 22:719–748
11 Egger M, Davey Smith G, Schneider M, et al. Bias inmeta-analysis detected by a simple, graphical test. BMJ 1997;315:629–634
12 Higgins JPT, Green S, eds. Cochrane handbook for system-atic reviews of interventions version 5.0.1 [updated Septem-ber 2008]. Available at: www.cochrane-handbook.org. Ac-cessed August 27, 2009
13 Altman DG, Bland JM. Interaction revisited: the differencebetween two estimates. BMJ 2003; 326:219
14 Cazzola M, Di Lorenzo G, Di Perna F, et al. Additive effectsof salmeterol and fluticasone or theophylline in COPD. Chest2000; 118:1576–1581
15 Mahler DA, Wire P, Horstman D, et al. Effectiveness offluticasone propionate and salmeterol combination deliveredvia the diskus device in the treatment of chronic obstructivepulmonary disease. Am J Respir Crit Care Med 2002; 166:1084–1091
16 Calverley P, Pauwels R, Vestbo J, et al. Combined salmeteroland fluticasone in the treatment of chronic obstructive pul-monary disease: a randomized controlled trial. Lancet 2003;361:449–456
17 Calverley PM, Boonsawat W, Cseke Z, et al. Maintenancetherapy with budesonide and formoterol in chronic obstruc-tive pulmonary disease. Eur Respir J 2003; 22:912–919
18 Dal Negro RW, Pomari C, Tognella S, et al. Salmeterol andfluticasone 50 microg/250 microg bid in combination providesa better long-term control than salmeterol 50 microg bidalone and placebo in COPD patients already treated withtheophylline. Pulm Pharmacol Ther 2003; 16:241–246
19 Hanania NA, Darken P, Horstman D, et al. The efficacy andsafety of fluticasone propionate (250 �g)/salmeterol (50 �g)combined in the discus inhaler for the treatment of COPD.Chest 2003; 124:834–843
20 Szafranski A, Cukier A, Ramirez A, et al. Efficacy and safetyof budesonide/formoterol in the management of chronicobstructive pulmonary disease. Eur Respir J 2003; 21:74–81
21 Wouters EFM, Postma DS, Fokkens B, et al. Withdrawal offluticasone propionate from combined salmeterol/fluticasone
treatment in patients with COPD causes immediate andsustained disease deterioration: a randomized controlled trial.Thorax 2005; 60:480–487
22 O’Donnell DE, Sciurba F, Celli B, et al. Effect of fluticasonepropionate/salmeterol on lung hyperinflation and exerciseendurance in COPD. Chest 2006; 130:647–656
23 Calverley PM, Anderson JA, Celli B, et al. Salmeterol andfluticasone propionate and survival in chronic obstructivepulmonary disease. N Engl J Med 2007; 356:775–789
24 Kardos P, Wencker M, Glaab T, et al. Impact of salmeterol/fluticasone propionate versus salmeterol on exacerbations insevere chronic obstructive pulmonary disease. Am J RespirCrit Care Med 2007; 175:144–149
25 Ferguson GT, Anzueto A, Fei R, et al. Effect of fluticasonepropionate/salmeterol (250/50 mg) or salmeterol (50 mg) onCOPD exacerbations. Respir Med 2008; 102:1099–1108
26 Tashkin DP, Rennard SI, Martin P, et al. Efficacy and safetyof budesonide and formoterol in one pressurized metered-dose inhaler in patients with moderate to very severe chronicobstructive pulmonary disease: results of a 6-month random-ized clinical trial. Drugs 2008; 68:1975–2000
27 AstraZeneca. Clinical trial register: D-5899C00001 trial. Avail-able at: http://www.astrazenecaclinicaltrials.com/clinicaltrials/. Ac-cessed August 27, 2009
28 GlaxoSmithKline. Clinical trial register: SCO40041 trial.Available at: http://www.gsk-clinicalstudyregister.com/. AccessedAugust 27, 2007
29 GlaxoSmithKline. Clinical trial register: SCO100250 trial. Avail-able at: http://www.gsk-clinicalstudyregister.com/. AccessedAugust 27, 2007
30 GlaxoSmithKline. Clinical trial register: SCO100470 trial. Avail-able at: http://www.gsk-clinicalstudyregister.com/. AccessedAugust 27, 2007
31 GlaxoSmithKline. Clinical trial register: SCO104925 trial.Available at: http://www.gsk-clinicalstudyregister.com/. Ac-cessed August 27, 2007
32 Cazzola M, MacNee W, Martinez FJ, et al. Outcomes forCOPD pharmacological trials: from lung function to biomar-kers. Eur Respir J 2008; 31:416–468
33 Suissa S, McGhan R, Niewoehner D, et al. Inhaled cortico-steroids in chronic obstructive pulmonary disease. Proc AmThorac Soc 2007; 4:535–542
34 Wolfe F, Caplan L, Michaud K. Treatment for rheumatoidarthritis and the risk of hospitalization for pneumonia: asso-ciations with prednisone, disease modifying antirheumaticdrugs, and anti-tumor necrosis factor therapy. ArthritisRheum 2006; 54:628–634
35 Puhan MA, Bachmann LM, Kleijnen J, et al. Inhaled drugsto reduce exacerbations in patients with chronic obstruc-tive pulmonary disease: a network meta-analysis. BMCMed 2009; 7:2
36 Singh S, Amin AV, Loke YK. Long-term use of inhaledcorticosteroids and the risk of pneumonia in chronic obstruc-tive pulmonary disease: a meta-analysis. Arch Intern Med2009; 169:219–229
37 Wedzicha JA, Calverley PMA, Seemungal TA, et al. Theprevention of chronic obstructive pulmonary disease exacer-bations by salmeterol/fluticasone propionate or tiotropiumbromide. Am J Respir Crit Care Med 2008; 177:19–26
38 Moher D, Cook DJ, Eastwood S, et al. Improving the qualityof reports of meta-analyses of randomized controlled trials:the QUOROM statement. Lancet 1999; 354:1896–1900
39 Sears M. Long-acting bronchodilators in COPD [editorial].Chest 2008; 133:1057–1058
1038 Original Research
© 2009 American College of Chest Physicians by Gustavo Medrano on November 1, 2009chestjournal.chestpubs.orgDownloaded from

DOI 10.1378/chest.09-0821; Prepublished online July 24, 2009; 2009;136; 1029-1038Chest
Gustavo J. Rodrigo, José A. Castro-Rodriguez and Vicente PlazaCOPD
-Agonists Monotherapy for StableβCorticosteroids vs Long-Acting -Agonists and InhaledβSafety and Efficacy of Combined Long-Acting
November 1, 2009This information is current as of
& ServicesUpdated Information
l.htmlhttp://chestjournal.chestpubs.org/content/136/4/1029.fulhigh-resolution figures, can be found at:Updated Information and services, including
References
9.full.html#ref-list-1http://chestjournal.chestpubs.org/content/136/4/102accessed free at:This article cites 31 articles, 20 of which can be
Open AccessoptionFreely available online through CHEST open access
Permissions & Licensing
http://www.chestjournal.org/site/misc/reprints.xhtml(figures, tables) or in its entirety can be found online at: Information about reproducing this article in parts
Reprints http://www.chestjournal.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
Email alerting service
online article.article. Sign up in the box at the top right corner of the Receive free email alerts when new articles cite this
formatImages in PowerPoint
format. See any online article figure for directions downloaded for teaching purposes in PowerPoint slide Figures that appear in CHEST articles can be
© 2009 American College of Chest Physicians by Gustavo Medrano on November 1, 2009chestjournal.chestpubs.orgDownloaded from