Safety of Ambulatory Safety of Ambulatory Bariatric Surgery Bariatric Surgery Senapati PS, Menon A, Al-Rashedy M, Senapati PS, Menon A, Al-Rashedy M, Thawdar P, Akhtar K, Ammori BJ Thawdar P, Akhtar K, Ammori BJ Department of Obesity and Metabolic Department of Obesity and Metabolic Surgery Surgery Salford Royal Hospital, UK Salford Royal Hospital, UK BIDA May 2012 BIDA May 2012

Safety of Ambulatory Bariatric Surgery Senapati PS, Menon A, Al-Rashedy M, Thawdar P, Akhtar K, Ammori BJ Department of Obesity and Metabolic Surgery Salford.
Dec 23, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Safety of Ambulatory Safety of Ambulatory Bariatric SurgeryBariatric Surgery
Senapati PS, Menon A, Al-Rashedy M, Thawdar Senapati PS, Menon A, Al-Rashedy M, Thawdar P, Akhtar K, Ammori BJP, Akhtar K, Ammori BJ
Department of Obesity and Metabolic SurgeryDepartment of Obesity and Metabolic SurgerySalford Royal Hospital, UKSalford Royal Hospital, UK
BIDA May 2012BIDA May 2012
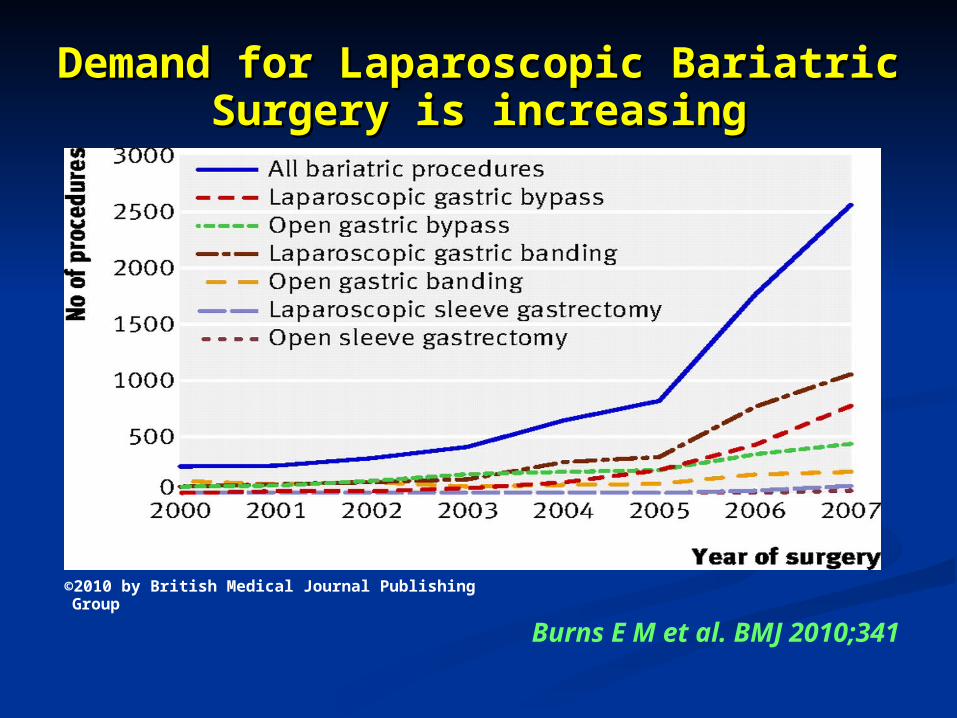
Demand for Laparoscopic Bariatric Surgery Demand for Laparoscopic Bariatric Surgery is increasingis increasing
Burns E M et al. BMJ 2010;341
©2010 by British Medical Journal Publishing Group


Co-morbidity ResolutionCo-morbidity ResolutionGastric Banding Gastric Bypass BPD or DS
EWL 47% 62% 70%
Resolution of DM 48% 84% 99%
Resolution of Hyperlipidaemia
59% 68% 83%
Resolution of HT 43% 68% 83%
Resolution of Sleep Apnoea
95% 80% 92%
Buchwald et al. JAMA.2004:292:1724-1737
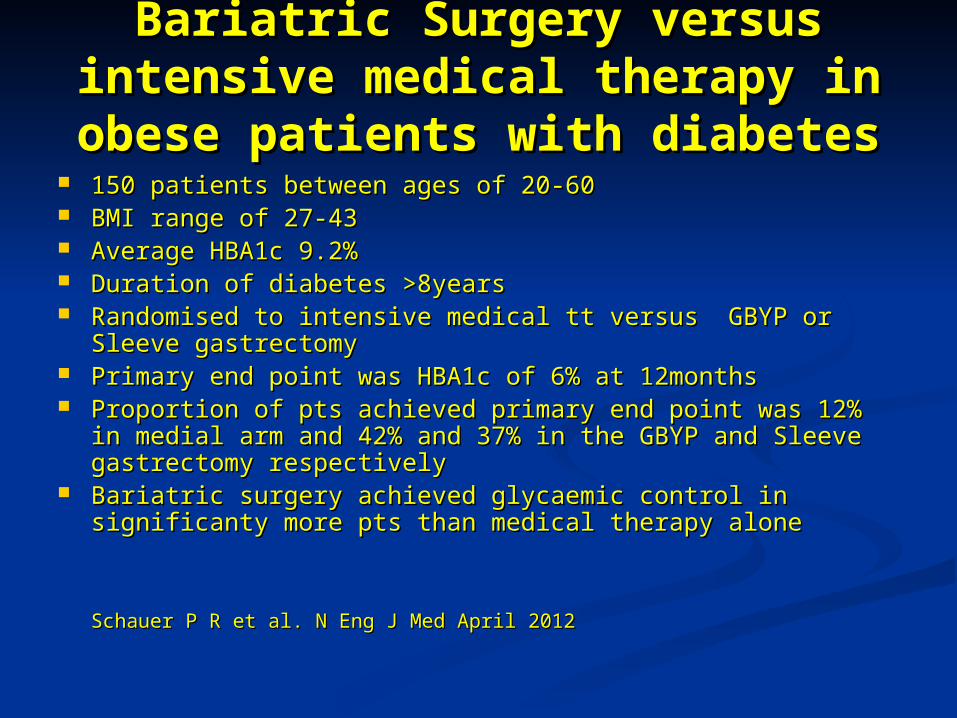
Bariatric Surgery versus intensive Bariatric Surgery versus intensive medical therapy in obese patients medical therapy in obese patients
with diabeteswith diabetes 150 patients between ages of 20-60150 patients between ages of 20-60 BMI range of 27-43BMI range of 27-43 Average HBA1c 9.2%Average HBA1c 9.2% Duration of diabetes >8yearsDuration of diabetes >8years Randomised to intensive medical tt versus GBYP or Sleeve Randomised to intensive medical tt versus GBYP or Sleeve
gastrectomygastrectomy Primary end point was HBA1c of 6% at 12monthsPrimary end point was HBA1c of 6% at 12months Proportion of pts achieved primary end point was 12% in Proportion of pts achieved primary end point was 12% in
medial arm and 42% and 37% in the GBYP and Sleeve medial arm and 42% and 37% in the GBYP and Sleeve gastrectomy respectivelygastrectomy respectively
Bariatric surgery achieved glycaemic control in significanty Bariatric surgery achieved glycaemic control in significanty more pts than medical therapy alonemore pts than medical therapy alone
Schauer P R et al. N Eng J Med April 2012Schauer P R et al. N Eng J Med April 2012
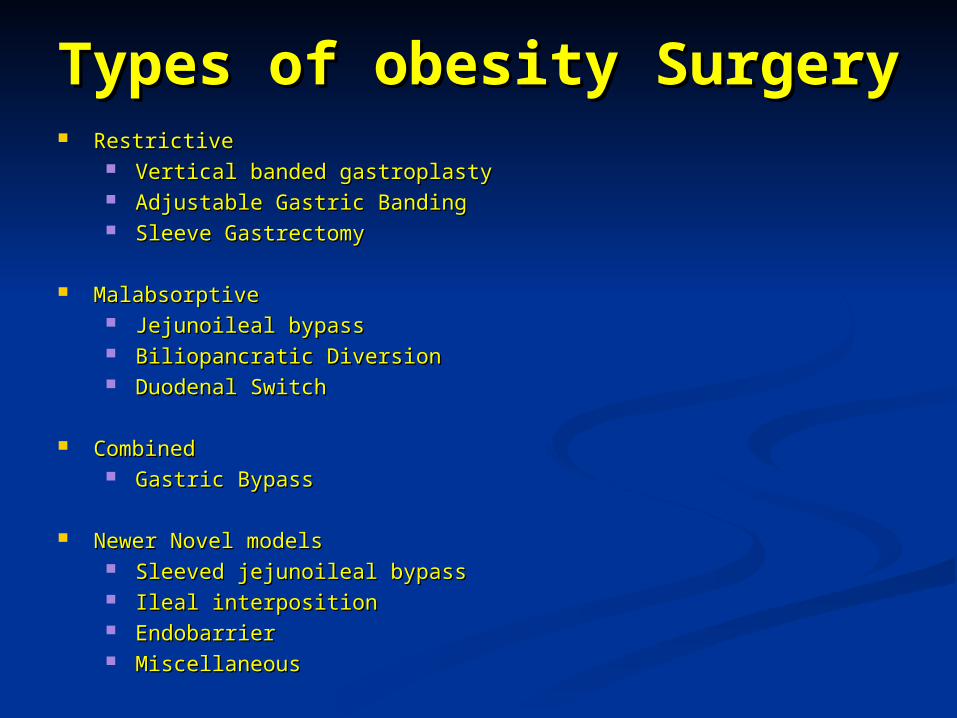
Types of obesity SurgeryTypes of obesity Surgery RestrictiveRestrictive
Vertical banded gastroplastyVertical banded gastroplasty Adjustable Gastric BandingAdjustable Gastric Banding Sleeve GastrectomySleeve Gastrectomy
MalabsorptiveMalabsorptive Jejunoileal bypassJejunoileal bypass Biliopancratic DiversionBiliopancratic Diversion Duodenal SwitchDuodenal Switch
CombinedCombined Gastric Bypass Gastric Bypass
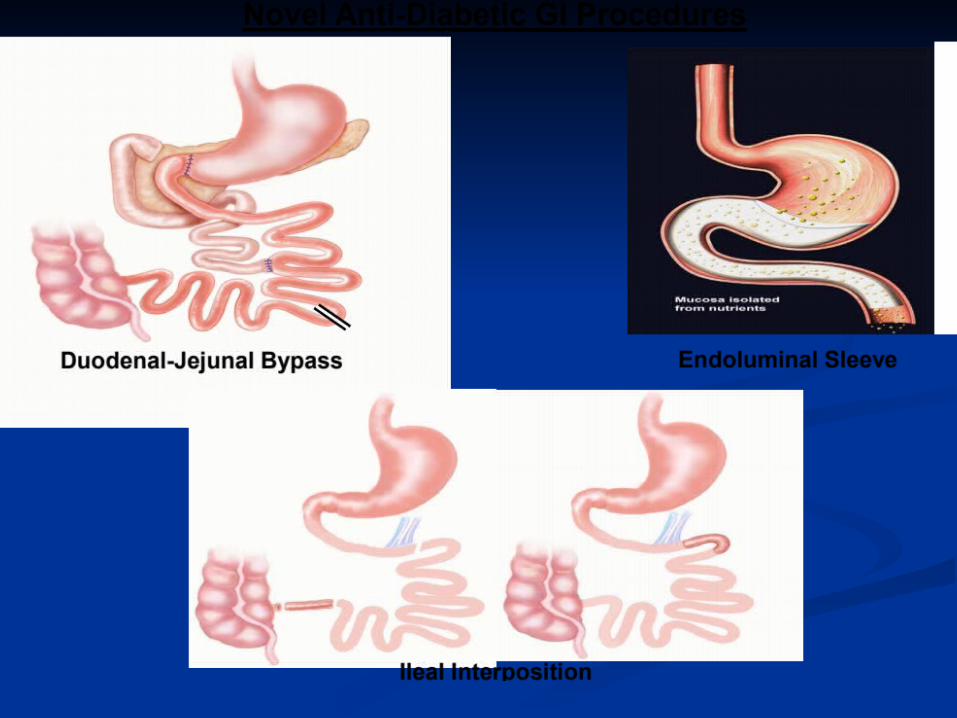
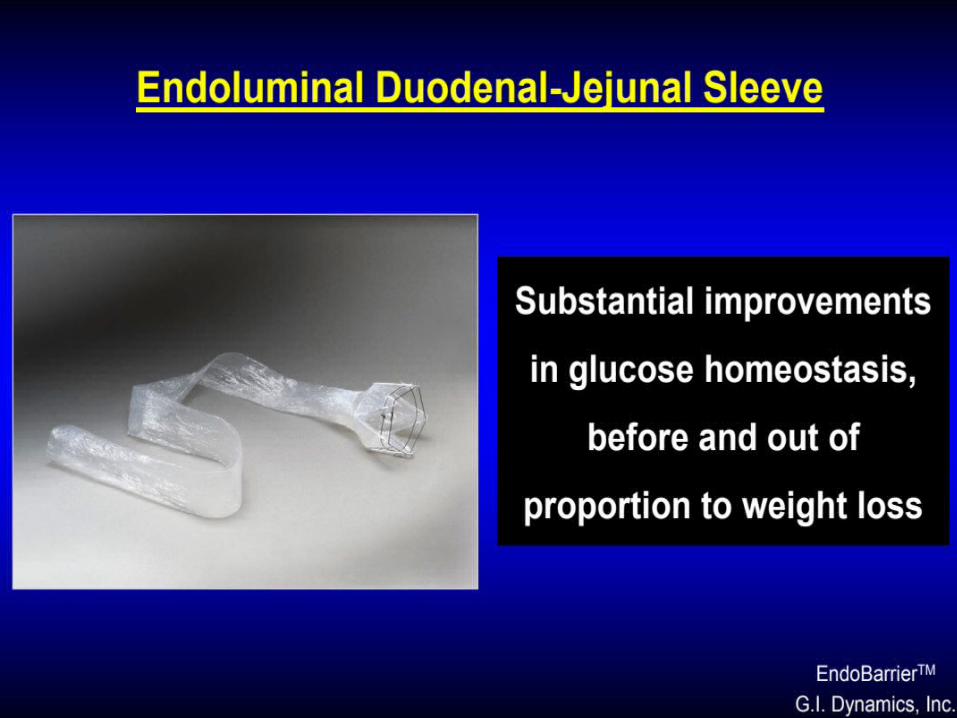
Newer Novel modelsNewer Novel models Sleeved jejunoileal bypassSleeved jejunoileal bypass Ileal interpositionIleal interposition EndobarrierEndobarrier MiscellaneousMiscellaneous

ADJUSTABLE GASTRIC ADJUSTABLE GASTRIC BANDINGBANDING


Gastric BypassGastric Bypass

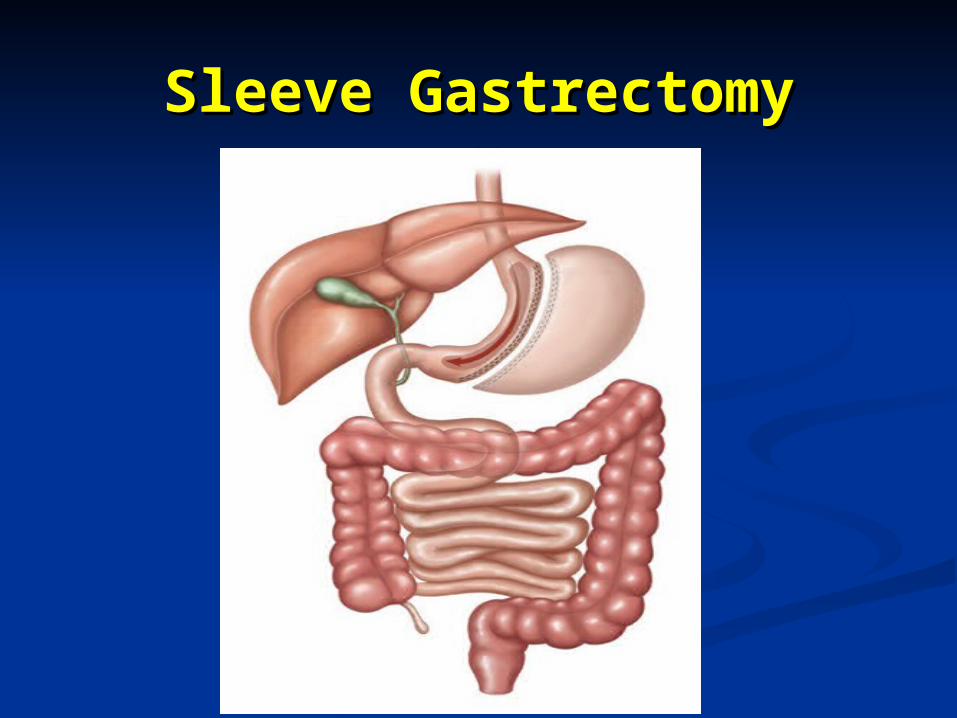
Sleeve GastrectomySleeve Gastrectomy
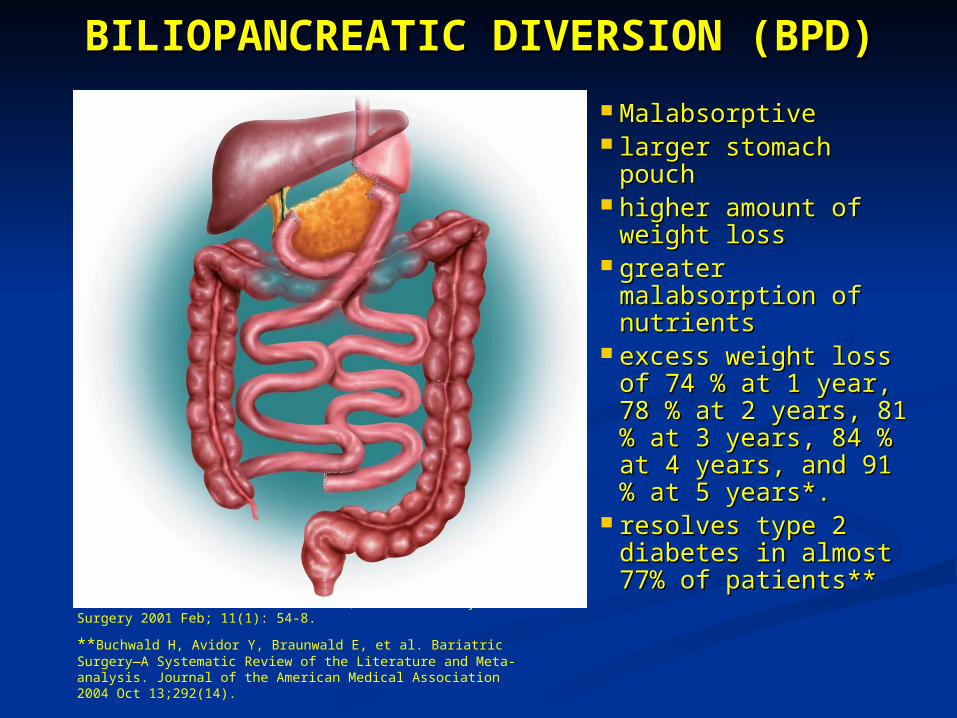
BILIOPANCREATIC DIVERSION BILIOPANCREATIC DIVERSION (BPD) (BPD)
MalabsorptiveMalabsorptive larger stomach larger stomach
pouchpouch higher amount of higher amount of
weight lossweight loss greater greater
malabsorption of malabsorption of nutrientsnutrients
excess weight loss excess weight loss of 74 % at 1 year, of 74 % at 1 year, 78 % at 2 years, 81 78 % at 2 years, 81 % at 3 years, 84 % % at 3 years, 84 % at 4 years, and 91 at 4 years, and 91 % at 5 years*. % at 5 years*.
resolves type 2 resolves type 2 diabetes in almost diabetes in almost 77% of patients**77% of patients**
*Duodenal Switch: An Effective Therapy for Morbid Obesity – Intermediate Results” Baltasar A, Bou R. Obesity Surgery 2001 Feb; 11(1): 54-8.
**Buchwald H, Avidor Y, Braunwald E, et al. Bariatric Surgery—A Systematic Review of the Literature and Meta-analysis. Journal of the American Medical Association 2004 Oct 13;292(14).

BILIOPANCREATIC DIVERSION (BPD) BILIOPANCREATIC DIVERSION (BPD) WITH DUODENAL SWITCH WITH DUODENAL SWITCH
MalabsorptiveMalabsorptive larger stomach larger stomach
pouchpouch higher amount of higher amount of
weight lossweight loss greater greater
malabsorption of malabsorption of nutrientsnutrients
excess weight loss excess weight loss of 74 % at 1 year, of 74 % at 1 year, 78 % at 2 years, 81 78 % at 2 years, 81 % at 3 years, 84 % % at 3 years, 84 % at 4 years, and 91 % at 4 years, and 91 % at 5 years*. at 5 years*.
resolves type 2 resolves type 2 diabetes in almost diabetes in almost 77% of patients**77% of patients**
*Duodenal Switch: An Effective Therapy for Morbid Obesity – Intermediate Results” Baltasar A, Bou R. Obesity Surgery 2001 Feb; 11(1): 54-8.
**Buchwald H, Avidor Y, Braunwald E, et al. Bariatric Surgery—A Systematic Review of the Literature and Meta-analysis. Journal of the American Medical Association 2004 Oct 13;292(14).



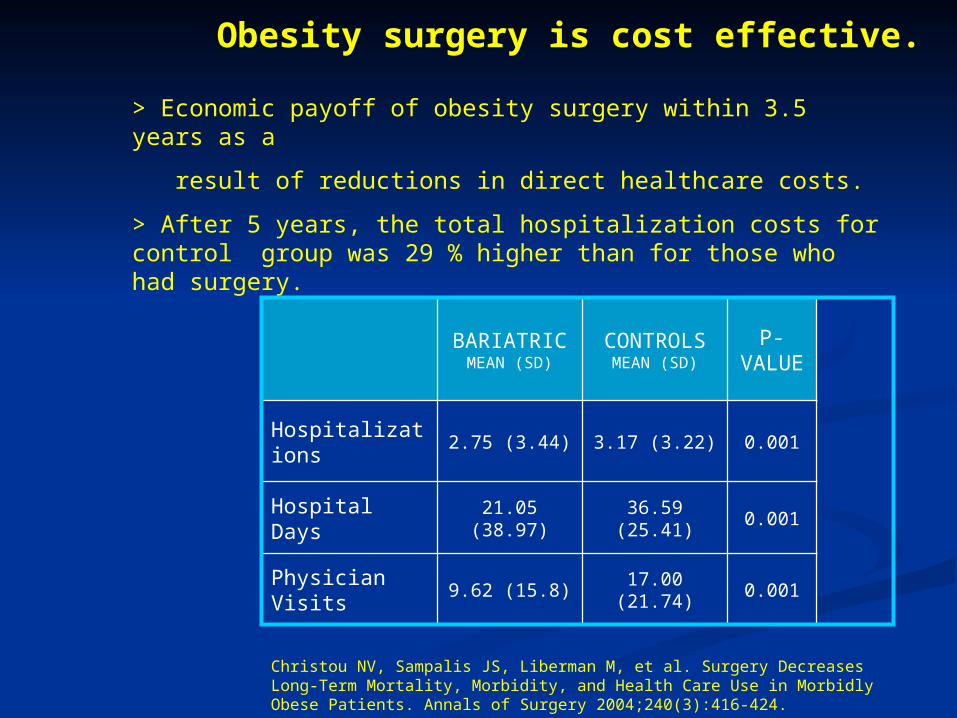
Five-Year Healthcare UtilizationFive-Year Healthcare Utilization
Christou NV, Sampalis JS, Liberman M, et al. Surgery Decreases Long-Term Mortality, Morbidity, and Health Care Use in Morbidly Obese Patients. Annals of Surgery 2004;240(3):416-424.
> Economic payoff of obesity surgery within 3.5 years as a
result of reductions in direct healthcare costs.
> After 5 years, the total hospitalization costs for control group was 29 % higher than for those who had surgery.
Obesity surgery is cost effective.
BARIATRICMEAN (SD)
CONTROLSMEAN (SD)
P-VALU
E
Hospitalizations 2.75 (3.44) 3.17 (3.22) 0.001
Hospital Days 21.05 (38.97) 36.59 (25.41) 0.001
Physician Visits 9.62 (15.8) 17.00 (21.74) 0.001

But this comes at a cost….But this comes at a cost….
Mean cost of laparoscopic bariatric surgery is Mean cost of laparoscopic bariatric surgery is $17000 a patient according to an economic analysis $17000 a patient according to an economic analysis of 3561 patientsof 3561 patients
Cremieux PY, Buchwald H et al. American Journal Cremieux PY, Buchwald H et al. American Journal Management Care. Management Care. 2008 Sep;14(9):589-96.2008 Sep;14(9):589-96.
Economic costs may be addressed with Economic costs may be addressed with ambulatory stay following surgeryambulatory stay following surgery
Meta-analysis of trials comparing ambulatory Meta-analysis of trials comparing ambulatory stay versus inpatient following laparoscopic stay versus inpatient following laparoscopic cholecystectomy demonstrated reduced cholecystectomy demonstrated reduced costs with higher patient satisfaction and costs with higher patient satisfaction and comparable 30-day readmission rates.comparable 30-day readmission rates.
Ahmed et al. Surg Endosc Ahmed et al. Surg Endosc 2008 Sep;22(9):1928-342008 Sep;22(9):1928-34..
Ambulatory stay following laparoscopic Ambulatory stay following laparoscopic gastric banding shown to reduce costs by gastric banding shown to reduce costs by 600 euros per patient600 euros per patient
Wasowicz-Kemps et al. Surg Endosc 2006; 20:1233-7.Wasowicz-Kemps et al. Surg Endosc 2006; 20:1233-7.
Evidence for Ambulatory Bariatric Evidence for Ambulatory Bariatric SurgerySurgery
Laparoscopic Gastric Band InsertionLaparoscopic Gastric Band Insertion Systematic review of 1 RCT and five cohort studies Systematic review of 1 RCT and five cohort studies
99.9% of 2549 patients were discharged within 23 hours99.9% of 2549 patients were discharged within 23 hours 0.55% 30-day readmission0.55% 30-day readmission
Thomas H et al. Thomas H et al. Obes Surg 2011 Jun;21(6):805-10.Obes Surg 2011 Jun;21(6):805-10.
RYGBRYGB Median stay in large study of 4631 patients is 2 days. Median stay in large study of 4631 patients is 2 days.
However Medicare guidelines recommend ambulatory stayHowever Medicare guidelines recommend ambulatory stayLancaster RT et al. Surg Endosc 22:2554-2563Lancaster RT et al. Surg Endosc 22:2554-2563
Milliman Care guidelines Ambulatory Care 14Milliman Care guidelines Ambulatory Care 14thth edition, Seattle edition, Seattle Systematic review of 4 cohort studies Systematic review of 4 cohort studies
84% of 2201 patients discharged within 23 hours84% of 2201 patients discharged within 23 hours 1.82% 30-day readmission1.82% 30-day readmission
Thomas H et al. Thomas H et al. J Laparoendosc Adv Surg Tech A. 2011 J Laparoendosc Adv Surg Tech A. 2011 Oct;21(8):677-81.Oct;21(8):677-81.

ObjectivesObjectives
To examine discharge within 23 hours of To examine discharge within 23 hours of laparoscopic bariatric surgery in terms of:laparoscopic bariatric surgery in terms of: FeasibilityFeasibility SafetySafety

MethodsMethods
Retrospective single-centre review of patients Retrospective single-centre review of patients undergoing laparoscopic bariatric surgery undergoing laparoscopic bariatric surgery between October 2008 and January 2012.between October 2008 and January 2012.
Decision to discharge made by senior member Decision to discharge made by senior member of clinical team, and after review by specialist of clinical team, and after review by specialist nurses, dietician, and diabetic team (when nurses, dietician, and diabetic team (when indicated)indicated)
Patient SelectionPatient Selection
Inclusions (Planned Inpatient Stay cases)Inclusions (Planned Inpatient Stay cases) Roux-en-Y Gastric Bypass (RYGB)Roux-en-Y Gastric Bypass (RYGB) Sleeve Gastrectomy (LSG)Sleeve Gastrectomy (LSG) Adjustable Gastric Banding (LAGB)Adjustable Gastric Banding (LAGB) Revisional bariatric surgeryRevisional bariatric surgery
Exclusions (short planned day cases)Exclusions (short planned day cases) Insertion of Intra-gastric BalloonInsertion of Intra-gastric Balloon LAGB port revisions/removalsLAGB port revisions/removals
Outcomes and AnalysisOutcomes and Analysis Outcome measuresOutcome measures
Demographic data including pre-operative Body Mass Index (BMI)Demographic data including pre-operative Body Mass Index (BMI) Successful discharge within 23 hours of surgerySuccessful discharge within 23 hours of surgery Readmission to hospital within 30 days of surgeryReadmission to hospital within 30 days of surgery All-cause mortality following surgeryAll-cause mortality following surgery
AnalysisAnalysis Comparisons made between success of 23 hour discharge between Comparisons made between success of 23 hour discharge between
different operative groups with One-Way ANOVA test.different operative groups with One-Way ANOVA test. Comparisons also made between patients <23 hour stay and Comparisons also made between patients <23 hour stay and
patients>23 hour stay with 2 tailed t-test and Chi-squared where patients>23 hour stay with 2 tailed t-test and Chi-squared where appropriateappropriate
Demographics (Age, Gender, BMI)Demographics (Age, Gender, BMI) Operating timeOperating time 30-day readmission30-day readmission
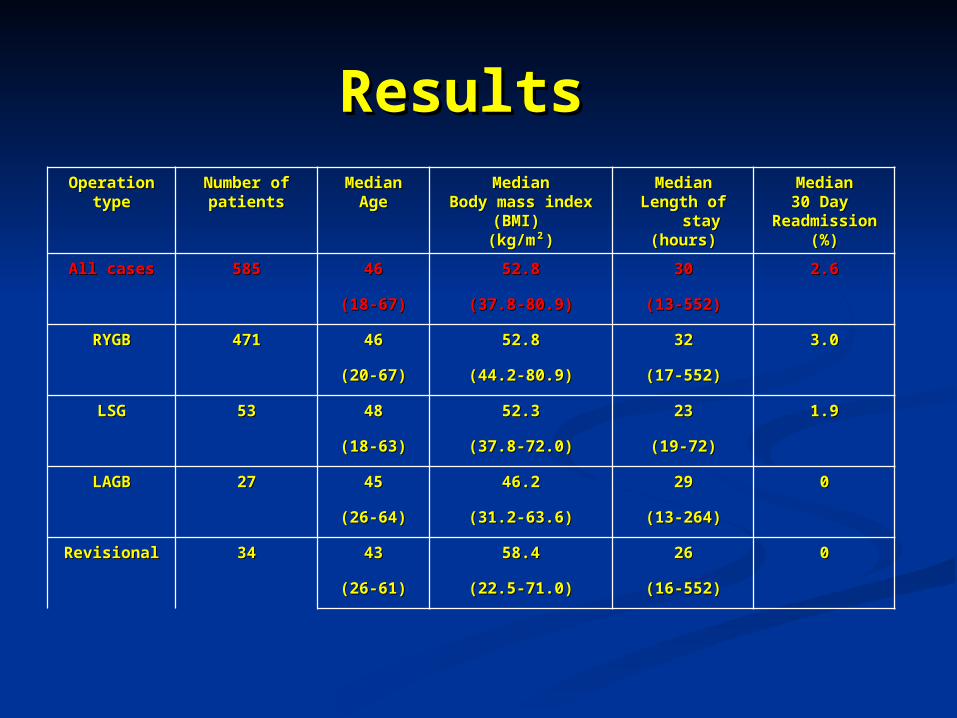
ResultsResults OperationOperation
typetypeNumber ofNumber ofpatientspatients
MedianMedianAgeAge
MedianMedianBody mass indexBody mass index
(BMI) (BMI) (kg/m²)(kg/m²)
MedianMedianLength of Length of
staystay(hours)(hours)
MedianMedian30 Day 30 Day
ReadmissionReadmission(%)(%)
All casesAll cases 585585 4646 52.852.8 3030 2.62.6
(18-67)(18-67) (37.8-80.9)(37.8-80.9) (13-552)(13-552)
RYGBRYGB 471471 4646 52.852.8 3232 3.03.0
(20-67)(20-67) (44.2-80.9)(44.2-80.9) (17-552)(17-552)
LSGLSG 5353 4848 52.352.3 2323 1.91.9
(18-63)(18-63) (37.8-72.0)(37.8-72.0) (19-72)(19-72)
LAGBLAGB 2727 4545 46.246.2 2929 00
(26-64)(26-64) (31.2-63.6)(31.2-63.6) (13-264)(13-264)
RevisionalRevisional 3434 4343 58.458.4 2626 00
(26-61)(26-61) (22.5-71.0)(22.5-71.0) (16-552)(16-552)

Successful Discharge within 23 Successful Discharge within 23 hours of surgeryhours of surgery
44.1
51.8
34
29.1
24.4
0
10
20
30
40
50
60
All cases RYGB LSG LAGB Revsional
Operation
% C
ases
dis
char
ged
<23
hour
s ho
urs
•RYGB patients significantly less likely to be discharged <23h compared to all other groups (p<0.01)
•LSG patients less likely to be discharged <23h compared to LAGB p<0.05)*
*
*
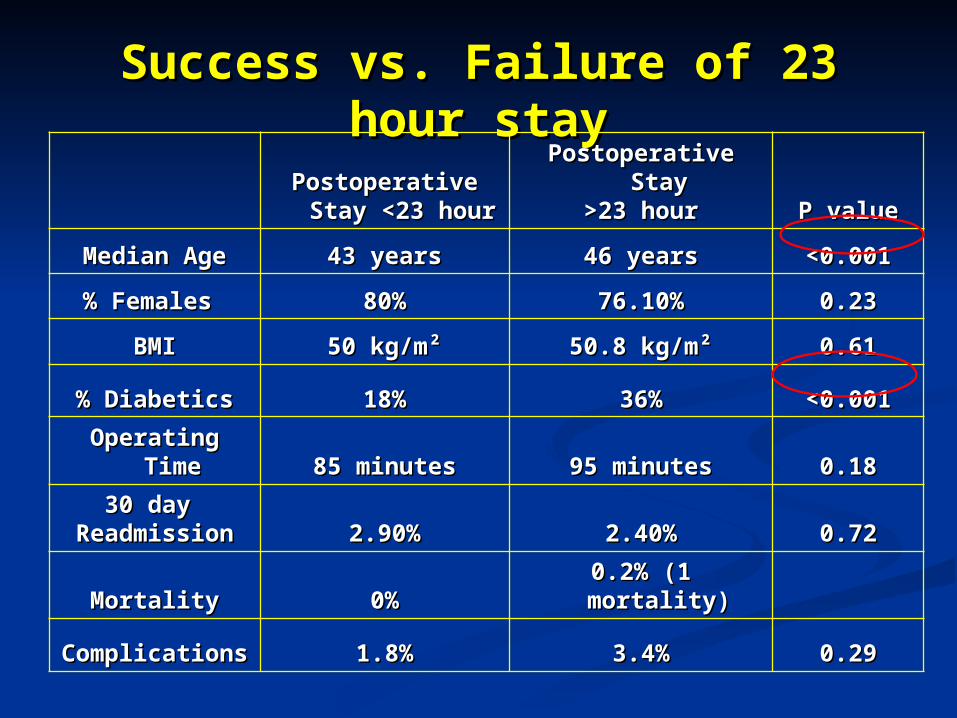
Success vs. Failure of 23 hour staySuccess vs. Failure of 23 hour stayPostoperative Stay Postoperative Stay
<23 hour<23 hourPostoperative StayPostoperative Stay
>23 hour>23 hour P valueP value
Median AgeMedian Age 43 years43 years 46 years46 years <0.001<0.001
% Females % Females 80%80% 76.10%76.10% 0.230.23
BMIBMI 50 kg/m²50 kg/m² 50.8 kg/m²50.8 kg/m² 0.610.61
% Diabetics% Diabetics 18%18% 36%36% <0.001<0.001
Operating TimeOperating Time 85 minutes85 minutes 95 minutes95 minutes 0.180.18
30 day 30 day ReadmissionReadmission 2.90%2.90% 2.40%2.40% 0.720.72
MortalityMortality 0%0% 0.2% (1 mortality)0.2% (1 mortality)
ComplicationsComplications 1.8%1.8% 3.4%3.4% 0.290.29
DiscussionDiscussion Ambulatory stay following laparoscopic bariatric surgery is feasible Ambulatory stay following laparoscopic bariatric surgery is feasible
after laparoscopic bariatric surgery, without compromising safetyafter laparoscopic bariatric surgery, without compromising safety
Age and Diabetic status may be significant factors to consider when Age and Diabetic status may be significant factors to consider when selecting patients for ambulatory stay. selecting patients for ambulatory stay.
The low rates of successful 23-hour discharge with RYGB and LSG The low rates of successful 23-hour discharge with RYGB and LSG may be explained by: may be explained by: The patients in this study were not initially planned for ambulatory stayThe patients in this study were not initially planned for ambulatory stay Patient co-morbidities and intra-operative factors which may or may not Patient co-morbidities and intra-operative factors which may or may not
be modifiablebe modifiable Higher proportion of diabetic patientsHigher proportion of diabetic patients Resource limitations preventing prompt dischargeResource limitations preventing prompt discharge
Further work needed to identify preoperative factors predicting Further work needed to identify preoperative factors predicting successful ambulatory stay to allow better patient selectionsuccessful ambulatory stay to allow better patient selection

Thank you for listeningThank you for listening

Related Documents











