SAFE EFFICACIOUS AUTOLOGOUS TREATMENT OF CLI, PAD, ANGINA, ISCHEMIC & DILATED CARDIOMYOPATHY FEBRUARY 10, 2020 © HEMOSTEMIX INC. ALL RIGHTS RESERVED. Tech Pioneer‘06

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

SAFE EFFICACIOUS AUTOLOGOUS TREATMENT OF CLI, PAD, ANGINA, ISCHEMIC & DILATED CARDIOMYOPATHY
FEBRUARY 10, 2020 © HEMOSTEMIX INC. ALL RIGHTS RESERVED.
Tech Pioneer‘06

This presentation contains forward looking statements that reflect management’s expectations regarding the future growth and results of operational
performance including but not limited to the scientific, financial, competitive and business prospects of Hemostemix Inc. (“Hemostemix” or the
“Company”). This Presentation contains “forward-looking statements” and “forward-looking information” within the meaning of applicable securities
legislation. Forward-looking information is generally, but not always identified by words such as “may”, “would”, “could”, “will”, “likely”, “expect”,
“anticipate”, “believe”, “intend”, “plan”, “forecast”, “project”, “estimate”, “potential”, “might”, “seek”, “budget”, “outlook”, and other similar expressions. In
addition, forward looking statements include, but are not limited to, the Company’s assessment of and targets for the stem-cell industry, including the
potential opportunities and challenges in the current stem cell industry; matters pertaining to Hemostemix, including its strategy and anticipated and
potential transactions and the characteristics thereof; future acquisition opportunities, partnerships, licensing opportunities and joint ventures and its pro
forma impact to capitalization following the completion of any of the Company's business opportunities; matters pertaining to the Company’s future
research and development initiatives including future clinical trials, management’s estimated timelines regarding the Company’s clinical trials,
regulatory approvals for ACP-01 and NCP-01, and many other projected timelines including regulatory approvals of the Company’s submission(s);
financial modeling matters, including metrics pertaining to anticipated financial and operational performance of operations; and, any matters pertaining
to the potential for commercialization of its technology, sources and extent of necessary funding, manufacturing scalability and future business
outcomes.
Actual results, performance and achievement(s) could differ materially from that expressed in, or implied by, any forward-looking information in this
Presentation and, accordingly, investors should not place undue reliance on any such forward-looking information. Forward-looking information should
not be read as guarantees of future performance or results. Forward-looking information and results could differ materially from general business,
economic, competitive and regulatory risks now and in the future, including that the Company's current phase II clinical trial will be completed within
the timelines and on the terms currently anticipated. As well, results may be inconsistent with general assumptions about the economic environment
and stem cell industry environment, the business operations of Hemostemix including that each business will continue to operate in a manner
consistent with past practice and pursuant to certain industry expectations and current market conditions.
Any forward-looking statements speak only as of the date on which such statement is made and the Company disclaims any intention or obligation to
update or revise any forward-looking information as a result of new information, future events or otherwise, unless required by applicable law. New
factors emerge from time to time and it is not possible for management to predict how such factors impact the Company’s business, or the extent to
which any factor or combination of factors may cause actual results to differ materially from those contained in any forward-looking statements.
Forward-looking information contained in this Presentation is based on the Company’s current estimates, expectations and projections, which the
Company believes are reasonable as of the current date. The Company can give no assurance that these estimates, expectations and projections will
prove to be correct. Historical statements should not be taken as a representation that such trends will be replicated in the future. No statement in this
Presentation is intended to be nor may be construed to be an investment recommendation or a profit forecast.
FORWARD-LOOKING INFORMATION

PAT E N T E D AU T O L O G O U S S T E M C E L L T H E R AP Y P L AT F O R M
Hemostemix Inc.
>300 Patients treated.
Abstract results show improvement in
83% of patients tested¹
91 patents cover five patent families
including automated production of
autologous peripheral blood-based
ACP-01 & NCP-01
Ongoing 20 Centre International Phase
II Clinical Trial for Critical Limb
Ischemia
ACP-01: Studied and clinically trialled for the treatment of ischemia-based conditions of:
Critical Limb Ischemia and
Peripheral Arterial Disease
Angina
Dilated Cardiomyopathy
Ischemic Cardiomyopathy
Future potential : Other
Cardiovascular Diseases
¹ Source: Abstract entitled: “Autologous Stem Cell Treatment for CLI Patients with No Revascularization Options: An Update of the Hemostemix ACP-01 Trial With 4.5 Year Followup”

HOW SCALABLE IS OUR PLATFORM? HEMISTEMIX – AT A GLANCE
Patented
• 91 Patents issued worldwide
• Automation of Production Patent
Expandable Platform
• ACP-01 – 5 indications
• NCP-01 - stroke model as an indication
• Machine engineered
Optimized Business Plan
• Lean structure
• Experienced management team
• World class Scientific Advisory Board
Key Partnerships
• License Negotiations Started
• By Indication by Country
Data Driven
• Historical Data >300 patients treated
• 12 Years of treatment History
• Multiple Trials (2) and Investigator led
studies (3) completed
Clinical Trials–Clinical Data
• 20 NA Sites : 56th patient enrollment
• Abstract results show 83% of patients (10 of
12) show improvement
• Futility Analysis to be completed when 42
patients achieve 26 weeks of follow-up.

THE IMPORTANCE OF CELL THERAPY
• Regenerative medicine is the leading
edge for biotech investment
• Unmet need for new less invasive,
less expensive non-surgical
treatments
• Right to try legislation approved in
the USA mirrors EU and SE Asia
autologous conventions of use
• There is a gradual shift away from
drugs toward personalized cell based
therapies
• Aging populations worldwide
• Good health and quality of life are key
concerns with aging
• Poor diet and lifestyle increase
prevalence of conditions of ischemia -
related diseases treatable with ACP-
01.
Disease Trends support need for
new therapies
Strong Government
and Public support
Population and
Lifestyle Factors
• CLI is a major global health
problem - incidence growing with
aging population
• CLI has limited treatment options–
significant amputations and high
cost to society
• Cardiovascular disease (“CVD”) is the
number one cause of deaths in North
America and worldwide causing
approximately 1 in 3 deaths
• Rising healthcare and economic costs-
CVD costs anticipated to double by 2035
in USA
• Type 2 diabetes is a global health
epidemic on the rise resulting in
increasing PAD and CLI diagnosis

ACP-01 DIFFERENTIATORS
Autologous. Proven safety and
efficacy
Blood draw: safer, less invasive
than fat or bone marrow
Global portfolio of 91 patents
Including automated production
Low Patient RisksSelf-donation, means no immune
rejection or disease transmission
High Cell ViabilityFresh cells in ready-to-use syringes,
no cryopreservation required
Simple ProtocolSafe and easy to perform in
outpatient clinic
No Ethical ConcernsStem cells derived
directly from patient
No Reported Safety IssuesNo mobilization drugs
needed to collect cells
ScalableSimple, cost-effective
production process
Non-surgical, enhanced cell therapy treatment for restoring circulation to blood starved tissues and organs

ACP-01 POTENTIAL MARKETSM U L T I P L E C U R R E N T A N D F U T U R E I N D I C AT I O N S P O T E N T I A L
Cardiovascular Disease
In the United States, total
costs of CVD in 2016 was $555B;
it is projected to be $1.1T by 2035
Critical Limb Ischemia
Peripheral Arterial Disease
Angina and CVD
Vascular Dementia
Ischemic Renal Disease
Ischemic Erectile Dysfunction Disease
CLI - Tip of the Iceberg
CLI - Estimated total costs up
to $248B¹ in US.
1Source: The Sage Group2Source: American Heart Association Report: Cardiovascular Disease: A costly Burden for America

WHY ACP-01 FOR CLI? IT SAVES LIMBS
Hope for CLI Patients Facing Amputation
Extract and enrich patient’s
own cell population from
peripheral blood
01Inject patient’s cell population
to form new blood vessels,
saving limb
02
Self-Donor
Uses patient’s own cells,
no immune rejection, no
observed safety issues
Simple
Cell harvest via blood draw
Quick
7 days from draw to
reinjection into patient’s limb

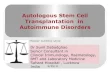
47 Days post ACP-01 Treatment
Befo
reA
fter
CLI WITH ACP-01 IMPROVEMENTS VISUALIZED

PHASE II TRIAL FOR CLI UPDATE
Phase II
Trial well
under wayCRO engagedMinimum 6 month and 12 month
follow-ups
20 sites on-boarded
FDA and Health Canada
approved
56th Patient treatment underway Multicenter in US and Canada
Randomized, placebo-controlled double blind
Phase II clinical trial to confirm the safety and efficacy of ACP-01
US FDA and Health Canada approved trial protocol

PHASE I I CLI TRIAL MILESTONES
A catalyst for future trialsProgression of the CLI Trial has opened the door for other ACP-01 clinical trials
Phase II CLI Trial
Study Completion⁴
Interim Data⁴
Patient Monitoring⁴
First Patient Treatment³
Site & Patient Recruiting⁴
US FDA Approval²
Health Canada Approval¹
CRO engaged
H2 2017 H1 2018 H2 2018 H1 2019 H2 2019 H1 2020 H2 2020
¹Health Canada Phase II Trial continuation approval received in December 2017. ²US FDA Phase II Clinical Trial continuation approval received April 2018.³First patient treatment under continued clinical trial announced May 3. 2018.⁴Anticipated timeline. See Forward-Looking Information.

ACP-01 STUDY AND TRIAL HISTORY
Type of Study Study Location Objective of StudyStudy
Design
Number of
SubjectsPatients Study Status
Pilot Safety/
FeasibilityThailand
To assess the feasibility and safety
of the implantationOpen label 6 Diagnosed CLI Completed
Phase 1b Safety
and EfficacyHungary
To assess safety or ex vivo expanded,
peripheral blood-derived, autologous
angiogenic cell precursors (ACPs)
in no option PAD patients
Open label 20 Diagnosed PAD
Completed
And
Published
Phase II Safety
and Efficacy
Canada and
United States
Time to major
amputation/mortality
Randomized
Double Blind
Placebo
Controlled
95 (Anticipate
Futility Analysis
to be
completed
when 42
patients
complete 26
weeks of
follow-up)
Diagnosed CLI In Progress
Clinical Trial
Safety/
Feasibility
ThailandTo assess the feasibility and safety of
intracoronary injectionOpen label
24 Planned (17
completed)Diagnosed Angina
Completed
And
Published
Safety and
EfficacyThailand
To determine the safety and efficacy of
intracoronary injection of ACPs in
relieving symptoms of angina pectoris
and congestive heart failure in chronic
ischemic heart disease subject with
maximal medical therapy and no option
for revascularization procedures
Open label 106
Diagnosis of severe
ischemic heart
disease with
continued angina
pain or heart failure
symptoms
Completed
Results Available
Safety and
Efficacy
Bangkok Heart
Hospital
INTRAMYOCARDIAL ANGIOGENIC
CELL PERCURSOR INJECTION FOR
CARDIOMYOPATHY, Asian
Cardiovascular & Thoracic Annals, 2008,
Vol. 16, No. 2, p 143 - 148,
Open label 41
Diagnosed Ischemic
Cardiomyopathy or
Dilated
Cardiomyopathy
Completed
And
Published

ACP-01 STUDY AND ABSTRACT RESULTS
ABSTRACT TTLE: AUTOLOGOUS STEM CELL TREATMENT FOR CLI PATIENTS WITH NO
REVASCULARIZATION OPTIONS: AN UPDATE OF THE HEMOSTEMIX ACP-01 TRIAL WITH 4.5 YEAR
FOLLOWUP Jonathan Misskey MD MHPE¹, Lynn Cunada, RN², Kyle Makofka³, Alan Jacobs MSEE. MD
PhD.³, Iris Zhong⁴, Thomas Lindsay MDCM⁴, York N. Hsiang, MB ChB., MHSc., FRCSCS¹ (¹Department of
Surgery, UBC, ²Vancouver Coastal Health, ³Hemostemix Inc, ⁴ Division of Vascular Surgery, Peter Munk
Cardiac Centre, University Health Network and Department of Surgery, University of Toronto)
Results: Twelve patients with CLI and no interventional options were enrolled (10 male, 2 female, mean age
76 years). Prior to treatment with ACP-01 or placebo, 3 patients had ischemic rest pain, 8 patients had
ulceration, and one patient had gangrene. Post treatment, one patient with unremitting rest pain and toe
gangrene required a below knee amputation, and one patient with gangrene of the first to third toes required a
forefoot amputation. Healing of ulcers and resolution of ischemic rest pain occurred in the other 10 (83%)
patients. There were no clinically significant safety issues. Outcomes have been maintained for up to 4.5
years (3.5 years for 2 patients, 3 years for 1 and 1 patient died after ulcer healing secondary to congestive
heart failure at 6 months).
Conclusions: Preliminary long-term results of ACP-01 autologous stem cell treatment in CLI patients with no
revascularization options are encouraging. Enrollment in the study is ongoing at medical centers in Canada
and the US. We recommend Vascular surgeons to discuss this study with their CLI patients who have no
further revascularization options available.
Source: AUTOLOGOUS STEM CELL TREATMENT FOR CLI PATIENTS WITH NO REVASCULARIZATION OPTIONS: AN
UPDATE OF THE HEMOSTEMIX ACP-01 TRIAL WITH 4.5 YEAR FOLLOWUP

ACP-01 STUDY AND ABSTRACT RESULTSSAFETY AND EFFICACY STUDY - Thailand:
Purpose: To assess the safety and efficacy of transcoronary injection of angiogenic cells precursors (ACPs) in
patientswith ischemic cardiomyopathy.
Methods: Between 2005 and 2008, 106 ischemic heart disease patients on maximal medical therapy and nooption for revascularization procedures who underwent transcoronary injection of ACPs at Chaophya hospital,Bangkok, Thailand were enrolled in the study. This study is a report of case series with non-randomized dataand without control cohort. Follow-up of patients were made mostly by patients' own cardiologists at 2, 4, 6 and12 months according to the protocol because majority of patients were from abroad.
Results: Baseline study:
• The mean age of 106 patients was 66 ± 10.6 years.
• Majority of patients had Canadian Cardiovascular Society (CCS) class and New York Heart Association
(NYHA) functional class III- IV. Most patients had poor left ventricular systolic function.
• At 1 year follow-up, there was significant improvement of CCS class from 2.63 ± 0.66 to 1.53 ± 0.76 (N = 39, p<
0.001) while NYHA functional class improved from 2.69± 0.56 to1.64 ± 0.83 (N=32,p< 0.001).
• Post treatment at 2-4 months, patients with poor left ventricular ejection fraction (LVEF ≤40%) at baseline, the LVEF
was increasedfrom34.4%± 16.4%to39.1%± 15.5%(N=39,p< 0.05).
• The quality of life by SF-36 version 2 Health Survey revealed that General Health and Physical functioning were
significantly improved. Procedural mortality rate was0%.
Conclusions: Transcoronary injection of ACPs improved cardiac function (increased LVEF), exercise capacity and
quality of life with high safety profile for ischemic cardiomyopathy patients with no-option revascularization.
Source: Transcoronary Injection of Angiogenic Cells Precursors an Autologous Stem Cell in Ischemic Cardiomyopathy: A Clinical study of 106 cases in Thailand. ASEAN HEART JOURNAL, Vol 17, No. 1, January 2009.

ACP-01 STUDY AND ABSTRACT RESULTSD I A G N O S E D A N G I N A C L I N I C A L T R I A L
Purpose:
To assess the safety and efficacy of intracoronary injection Angiogenic Cell Precursors (“ACP”s) based product for the treatment of
patients with chronic stable angina pectoris who were on maximal drug therapy.
Methods:
Twenty four patients were prospectively enrolled and treated with ACPs. The administration of the therapy was based upon identifying
ischemic but viable myocardium (SPECT-MIBI scan) in the distribution of occluded coronary arteries. ACPs were prepared from cells
separated from non-mobilized peripheral blood of each patient, cultured ex vivo and injected via a catheter with proximal balloon
occlusion of the coronary artery. The patients were assessed clinically pretreatment and at 1, 3 and 6 months after treatment using the
following parameters: Canadian Cardiovascular Society (“CCS”) Scale, six minute walk (“6MW”) test, exercise capacity as assessed by
metabolic equivalents (“MET”s) and SPECT-MIBI perfusion defect.
Preliminary Reported Results:
Twenty patients have completed 3 months follow up and 17 have completed 6 months follow up.
The clinical condition improved in all patients at 3 and 6 months vs. pretreatment:
• 6MW increasing from 333.65±26.56 to 414.95±28.54 meters at 3 months and to 413.25±33.17 meters at 6 months (both P<0.001);
• exercise capacity increasing from 5.62±0.52 to 6.73±0.64 METs at 3 months (P<0.004) and to 7.09±0.79 METs at 6 months (P<0.04);
• perfusion defect decreasing from 38.46±6.19% to 23.89±5.79% at 3 months (P<0.004) and to 21.05±5.16% at 6 months (P<0.005);
and
• mean CCS score decreasing from 2.1±0.19 to 1.05±0.05 at 3 months and to 1.18±0.13 at 6 months (both P<0.001).
• One patient died two weeks after the treatment due to acute myocardial infarction. Coronary angiography demonstrated occlusion in
an untreated artery and patency of the ACP-treated artery.
Conclusion:
ACP therapy for chronic stable angina seems to be safe and improves anginal symptoms at 3 and 6 months. Larger studies are being
initiated to evaluate the benefit of ACPs for the treatment of this and additional severe heart diseases.
Source: Circulation Journal Vol. 114 No. Suppl._18. Abstract 3682: Treatment of Patients with Severe Angina Pectoris Using Intracoronarily Injected Autologous Blood-Borne Angiogenic Cell Precursors. https://www.ahajournals.org/doi/10.1161/circ.114.suppl_18.II_786-c.

INDICATION PIPELINE
Candidate Indication
Development Phase
Status
Preclinical Clinical
ACP-01 • Critical limb ischemia • Phase II clinical trial
• Currently 20 sites and 56
patients enrolled.
• Trial ongoing
ACP-01
• PAD
• Angina Pectoris
• Ischemic & dilated
Cardiomyopathy
• Congestive Heart Disease
• Acute Myocardial Infraction
• Ischemic Renal Disease
• Vascular Dementia
• Erectile Dysfunction
• Preparing for Phase II Angina
Pectoris trial
• Seeking JV partners to fund
phase II trials in each
indication
• Safety trials completed
NCP-01
• Stroke
• Spinal Cord Injury
• Amyotrophic Lateral
Sclerosis (ALS)
• Preclinical
• Seeking JV Partners to fund
trials.
• In R&D
BCP-01
• Bone fractures
• Skeletal breaks
• Surgical procedures
• Preclinical
• Seeking JV Partners to fund
trials
• Preliminary R&D

M A N A G E M E N T A N D D I R E C T O R S
Thomas Smeenk, BA, President,
Interim CEO, Founder & Director
• Founder, President and VP
Business Development,
TheraVitae Inc., which went public
as Hemostemix Inc. QT.
• A finance and business
development executive with a
proven track record of bringing
new discoveries to market.
• A public company executive since
1996, serving most recently as
President & CEO of Broadway
Gold Mining Ltd, where he
completed a $30 million agreement
with Rio Tinto. Prior, VP Business
Development, Memex Inc.
(TSXV:MEM), a company he took
public; President & CEO of e-
Manufacturing Networks Inc.
(TSXV:OEE), a company he took
public; President and CEO of
Tyranex Gold Inc. and President
and CEO of IBI Corporation.
David L. Wood, Chairman of the
Board
• Founder and President of Zenith
Appraisal and Land Consulting Ltd.
and Double Check Consulting Inc.,
both private consulting entities
• Former Director and former CEO
and CFO OF DataMiners Capital
Corp., a NEX listed company.
• Former Director of Black Bull
Resources Inc., a mining company
formerly listed on the TSXV.
• Served on the Audit Committees
and as Board Chairman and
Director of various TSXV listed
companies from 1999-2013
• Professional appraiser and
obtained his designation from the
Appraisal Institute of Canada (AIC)
in 2001
Dr. Ronnie Hershman, M.D.,
F.C.C.S., Director
• Graduated Magna Cum Laude
from Sophie Davis Center for
Biomedical Research in 1980.
• Practicing Cardiologist since 1987
and Medical Director of NYU
Langone Long island Cardiac
Care.
• Pioneer in performing laser
assisted coronary angioplasty
• Entrepreneur and investor for more
than two decades
• Director and/or Officer of more
than nine life science companies
• Advisor to late stage life science
VC that has funded 24 companies
• Track record of investing in
companies that commercialize
technologies quickly and globally

S C I E N T I F I C A D V I S O R Y B O A R D
Dr. Alan Lumsden, M.D.
• Walter W. Fondren III Chair,
Medical Director of the Houston
Methodist DeBakey Heart and
Vascular Center and chair of the
Department of Cardiovascular
Surgery at Houston Methodist
Hospital since 2008
• Emory University in Atlanta -
completed his surgical residency
and vascular training leading to
position as Chief of the Division
of Vascular Surgery
• International reputation as a
leader in the field of
endovascular surgery. He
conducts FDA-mandated training
for surgeons nationwide and has
received millions of dollars for his
research from the National
Institutes of Health. He has
contributed more than 200
papers to medical literature.
Dr. Kumar L. Hari, PhD
• Chief Scientific Officer at cBio, a
private disease diagnostics and
tracking firm
• Expertise is in chromosome
biology, functional genomics, and
bioinformatics and oversaw the
development of the MRS and
PATRN platforms
• At cBio, Dr. Hari led the team in
engagements with the FDA,
various universities and other US
government organizations
• Former director of program
management efforts at the
California Institute of
Regenerative Medicine and at
the Myelin Repair Foundation
• PhD in Cell Biology from UC San
Diego
and a B.Sc. in Genetics from UC
Davis
Dr. Norman Wong, B.Sc (Hon),
M.Sc, M.D., FRCP(C)
• Co-Founder of Resverlogix Corp.
(TSX:RVX), and Chief Scientific
Officer since 2003
• Currently Professor of Medicine
and Biochemistry & Molecular
Biology and Director of the Libin
Gene/Cell Therapy Unit within
the Faculty of Medicine at the
University of Calgary
• Specializes in the areas of
Endocrinology,
Internal Medicine, Molecular
Biology,and Gene/Cell Therapy
• Author and co-author of over 275
articles and abstracts and has
been invited to sit on more than
40 national or international
panels and committees
• Consulted for leading
pharmaceutical companies,
including Eli Lilly, Merck Frost,
GlaxoSmithKline, Solvay
Pharmaceuticals and Abbott
Laboratories

SHARE CAPITAL OVERVIEW
Share capital structure as of December 31, 2019($CAD)
Number Ex. Price Expiry or Closing
Common Shares Issued and outstanding 300,898,610
Stock Options 20,783,736 $0.05-$0.10 Jan 2020-Mar 2024
Share Purchase Warrants¹ 3,934,851 $0.05-$0.65 Sep 2020-Dec 2020
Subtotal Fully Diluted 326,367,197
¹Share Purchase Warrants - details
Number Ex. Price Expiry
3,857,071 $0.05 Sept 15, 2020
77,780 $0.65 Dec 2, 2020

PERSONALIZED STEM CELL THERAPY TODAY
W O R L D E C O N O M I C F O R U M T E C H N O L O G Y P I O N E E R , 2 0 0 6
Shaping
The Future
of MedicineFor more Information please contact:
Suite 1150, 707-7th Avenue SW
Calgary, AB T2P 3H6
www.hemostemix.comThomas A. SmeenkPresident & Interim CEO
905-580-4170
Related Documents