
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript


Page 2 Sackler Journal of Medicine | Volume 6 | Issue 1 | 2021
MISSION STATEMENTWhat’s emerging in medicine today? The Sackler Journal of Medicine – a forum where trends in medicine including translational research, the economics and policy of healthcare, and clinical experiences are explored, analyzed and discussed. SJM is a peer-reviewed journal for medical students to discuss and learn about the latest medical breakthroughs and the fundamentals of medicine.
We encourage student and physician collaboration to bring you literature reviews, case reports, original research, reflective pieces, and short commentaries on published papers. Take the opportunity to contribute your work, experiences and voice to the conversation.
Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021

SUBMISSIONS INFORMATION
Submissions from students, faculty, and individuals are welcomed. For more information please visit the “Submissions” page on the Sackler Journal of
Medicine website at sacklerjom.org
CONTACT US
Email: [email protected]: www.sacklerjom.org

Page 4 Sackler Journal of Medicine | Volume 6 | Issue 1 | 2021
ISSN: 2472-0323
COVER IMAGE
Created by Anais Di Via Ioschpe
FUNDING
Sackler Journal of Medicine is funded by the Sackler School of Medicine at Tel Aviv University.
EDITORIAL BOARD
Bora Golijanin & Dania HalperinEditors-in-Chief
Samantha TopeDirector of Submissions
Adam SlavickDirectors of Manuscripts
Sean Ghiam & Ariel RafieDirector of Graphics & Design
PEER REVIEWERS
Yael FrankCaroline BraunerDavid RabinovitzTalia MandellShanee NavonJosh PankinAdi Levy
ASSOCIATE EDITORS
Yishai SchwartzAllison Siegel
MANUSCRIPT EDITORS
Hershel HorowitzCaroline KaufmanAvi Petroff
MEDICAL ILLUSTRATORS
Anais Di Via IoschpeHannah SragoviczeDahila FischerJonathan SokalNiko MorozovOrian Raviv
ADVISORY BOARD
Shuey Mirkin and Samantha TopeFormer Editors-in-Chief
Dr. Aaron Allen
FACULTY ADVISER
Dr. Aaron Allen
The Editoral Board would like to give a special thanks to Tami Lipkin-Zur and Adi Knaan for their support.
Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021
Page 5Sackler Journal of Medicine | Volume 6 | Issue 1 | 2021
Table of Contents
Letter From the Editors ........................................................................................................7
Letter from Dr. Allen ............................................................................................................8
Tractography Based Connectivity in Deep Brain Stimulation for Obsessive Compulsive Disorder? .............................................................................................................................9 Michael Chodakiewitz
COVID-19 Vaccines: Importance of Including Pregnant Individuals in Clinical Trials ..........18Yael Frank and Alisa Kachikis
Wnt Signaling in Corneal Diseases and Wound Healing .....................................................22Sean Ghiam, Ruchi Shah, Alexander Ljubimov
Individualized Approach for Counseling Patients Faces with the Decision of Transferring a Low-Level Mosaic Embryo ................................................................................................27Tohar Kochav Lev, Bei Sun, Ron Shemtov, Talia Ditkoff, Tomer Singer
The First Half of The Preclinical Education at Sackler School of Medicine .........................30Noah Igra and Yuval Raviv
Should there be strict age cutoff for intended parents through gestational surrogacy? A Case Report ........................................................................................................................33Bei Sun, Tohar Kochav Lev, Liron Barel, Tomer Singer
Can stress induced pathways regulate glycogen synthase kinase 3 beta (GSK3β)..............35Noa Mecica and Costin Antonescu
Sackler Art of Medicine Spring 2021 Contest Winners ......................................................42Tori Grant, Jillian Shapiro, Hannah Sragovicz
Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021

Page 6 Sackler Journal of Medicine | Volume 6 | Issue 1 | 2021 Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021

Page 7Sackler Journal of Medicine | Volume 6 | Issue 1 | 2021
Letter From the Editors
To the Reader:
Finding answers and meaning in our day to day, as we shape our lives, our world, our future, is no easy feat. For some, the past few years were wrought with addi-tional personal and professional challeng-es that burdened their search for meaning. For others, these new experiences sparked ideas, motivating them to work tirelessly towards clarity. These lessons influence who we are today, and where we are head-ed. Albert Einstein famously wrote, “The more I learn, the more I realize that I don’t know.” As medical students, we need to be curious, ask questions, and seek out knowledge fearlessly. It is exciting to think of what we have yet to discover and learn about. In whatever way we can, an integral part of our medical education is under-standing the language and techniques of medical research. As physicians, this abili-ty to distill and clarify information will be one of many that we must hone. One of the lessons we have learned as students in the last few years is that the fear of the uncertain never resolves. Un-certainty is the only certainty! We must be ready to embrace it and learn from it. With all this in mind, we bring you this latest edition of the Sackler Journal of Medicine. We are proud to be well into the 7th year at the Sackler Journal of Medicine and present to you the hard work of our medical student community. These scien-tists and soon to be physicians understand that science does not aim at an immediate result. They lay the foundation for those who are to come, and point the way.
In this special issue there is original re-search, reviews, opinion pieces, art works, as well as masterfully crafted essays on the Art of Medicine. It is an honor to contribute in some small way to building our research commu-nity at the Sackler Faculty of Medicine of Tel Aviv University , and we hope that all of us will achieve ever greater heights in our per-sonal and professional lives. Thank you to all who supported and contributed this year. Thank you to all the peer reviewers, manuscript and associate edi-tors, artists, and the directorial team who keep the wheels spinning so that this journal can be published year after year. We very much couldn’t have done it without all of you.
Wishing you best success,
Dania Halperin and Bora GolijaninCo-Editors in Chief
Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021

Page 8 Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021
Letter From Dr. AllenAaron Allen M.D.Faculty Advisor- SJM Deputy Director New York State ProgramSackler Faculty of MedicineTel Aviv University Israel
Dear Sackler Journal of Medicine Readers, There is a story told of a group of Jewish chil-dren who were learning about the death of Jacob in The Bible. There were visited in their classroom by the school principal and were asked to read out loud and explain to the class the verse in Genesis 47:28 . (And Jacob lived in the land of Egypt 17 years…). Each stu-dent in turn read and explained the verse as they were taught in class and in turn each student was told by the principal that his or her reading was incorrect. Finally, in exasperation the teacher of the class, who had seen no problem with the children’s reading, stepped in and asked the principal what was wrong. Seeing the con-fusion on the teacher’s and the students faces, the prin-cipal responded by reading the verse himself. He read “and Jacob LIVED in the land of Egypt 17 years…” al-most shouting the work lived. He then explained to the children that being alive is the greatest gift one can have and it should not only be recognized but empha-sized as to its importance. Similar to nearly half of the local population I recently was diagnosed and recovered from COVID- 19. Although I did not need to be hospitalized or treated thank G-d, I was sick with cough fever and shortness of breath. Lying in bed and feeling weak, I began to think of the multitudes of people across the globe who weren’t so lucky and succumbed to this terrible disease. It is at times like this that you realize what a big gift every day and every moment of life is – especially if you are healthy and able to contribute to the world. We in the Sackler community, have struggled through the Pandemic like many other institutions with zoom lectures and quizzes and in some cases a near complete change in the entire curriculum. De-
spite these challenges however, students were able to graduate on time and have achieved outstanding match results. However even more impressive, is the percentage of Sackler students who volunteered both in the U.S and in Israel to help in any way they can combating the Pandemic. Tens of volunteers for Magen David Adom, Vaccine drives and education, and many students who have done and published im-portant research related to COVID -19. This more than anything else, shows so clearly the strength and commitment of the Sackler community to preserving life and doing whatever is necessary to lend a helping hand even in the darkest of circumstances. The publication of the Journal is another such example of incredible student led dedication and per-severance. Despite the challenges of organizing the reviewers and editors the submissions and produc-tion of the Journal have progressed from year to year and it is fast becoming the primary outlet for student’s academic work at the school. I would like to congrat-ulate the Editors and Staff for another outstanding edition. Finally, I would like to remind us all of the gift of life that we have all received by surviving the Pan-demic and how critical our contribution to preserving that gift to all our patients and their families.
Wishing the entire Sackler community the best of health and success.
Dr. Aaron

Page 9Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 ORIG
INA
L RESEARCH
Tractography Based Connectivity in Deep Brain Stimulation for Obsessive Compulsive DisorderMichael (Meir) Chodakiewitz1,2,3
Abstract – Introduction: Deep brain stimulation (DBS) has been increasingly used in the treatment of obsessive-compulsive disorder (OCD). Diffusion tractography has been used to aid in precise DBS targeting and electrode placement for various neurological disorders. The goal of this paper is to review the available literature on the use of DTI tractography in DBS for OCD and to evaluate DBS connectivity patterns that are associated with improved clinical outcome.
Methods: A systematic review was performed in accordance with PRISMA guidelines using PubMed and Google Scholar. A total of 128 studies were identified in the preliminary PubMed search as well as 8 records from review of references. After the initial screening for relevance and applying our subsequent criteria for inclusion, 7 articles (6 from Pubmed and 1 Non-PubMed article) were determined to fit all inclusion criteria and were included in this review.
Results: Despite heterogeneous OCD symptomatology, positive outcomes are observed across studies with variations in targeting and connectivity of these targets. Notably, the identified unified tract highlights a putative pathological circuit in a complex disease with symptomatologic multiplicity and demonstrates significant similarity to the tractographically defined MFB, which may contribute to the pathological circuitry of OCD.
Conclusion: Significant variation in targeting and connectivity suggest that various targets may modulate a single distributed brain network associated with symptoms of OCD, with each unique target site modulating possible additional unshared tracts or networks. Further investigations are warranted for the potential utilization of symptom-specific DBS targeting for OCD, which may require subcategorization of OCD symptomatologic subtypes and associated connectivity patterns to optimize outcomes. However, it is important to note that the two concepts--that of a unified tract and symptom-specific targeting within this tract, need not be mutually exclusive.
1Sacker School of Medicine – Tel Aviv University—Ramat Aviv, Israel. 2University of California – Los Angeles (UCLA) —Department of Neurosurgery – Los Angeles, CA3Cedars Sinai – Kerlan Jobe Institute – Center for Sports Neurology and Pain Medicine--Los Angeles, CA
Learning Points » To understand the connectivity patterns in
patients with OCD who have undergone DBS surgery.
» To analyze DBS targeting and identified connectivity patterns may relate to clinical outcomes.
» To delineate the pathological circuitry in-volved in OCD symptomatology with the goal of optimizing DBS targeting and clinical outcomes.
Introduction
Deep brain stimulation (DBS) has been increasingly used in the treatment and symptom-atic management of various psychiatric disorders, including treatment-resistant obsessive-compulsive disorder (OCD).20, 21,22,23 In contrast to certain neu-rological disorders such as essential tremor, which expresses a relatively fixed symptomatology across
patients, OCD is a heterogeneous disease in which symptoms can be subcategorized by the varying behaviors or symptomatic dimensions.24 Patients with OCD may present with obsessions and com-pulsions of contamination, washing, doubts and checking, forbidden thoughts, symmetry and ordering, or repeating.25
DBS targets for OCD have focused on brain regions considered to be components of the reward and motivation system including, with some overlap, the nucleus accumbens (NAcc)26 the ventral capsule/ventral striatum (VC/VS)27, the limbic part of the subthalamic nucleus (STN)28, the anterior limb of the internal capsule (ALIC)29, inferior thalamic peduncle (ITP)30, bed nucleus of the stria terminalis (BNST)33, anteromedial globus pallidus interna (amGPi)34, superolateral branch of the medial forebrain bundle (slMFB, now more appropriately referred to as ventral tegmental area projection pathway or vtaPP)5, as well as the medi-al dorsal and ventral anterior nucleus of the thala-mus (MD/V ANT)35. Raviv and colleagues recently

Page 10 Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 O
RIG
INA
L RE
SEA
RCH
reviewed targets for DBS for OCD and highlight-ed that the most commonly targeted brain regions are the VC/VS, ALIC, NAcc and BNST, which all have a degree of structural overlap and thus may be best considered as a group of “striatal region” targets, distinct from STN, pallidum and ITP 45. A recent report by Haber and colleagues also highlights the similarity of these “striatal region” targets, particularly with respect to their overall connectivity patterns.44 Despite the symptomatic
Methods
A systematic review was performed in accor-dance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines and a flow diagram of advanced keyword search results and study selection is outlined below in Figure 1 37. An online search using PubMed (until August 2020) was performed to identify relevant articles for inclusion
heterogeneity, most current approaches to DBS for OCD lack individualization and do not con-sider symptom-specific targeting. Conventional surgical planning for DBS has been based on direct or indirect targeting of anatomical land-marks combined with intraoperative stimulation and clinical testing to aid in localizing specific functional foci of deep brain structures. Recent advances in imaging technologies include the use of diffusion tensor imaging (DTI) or dif-fusion MRI (dMRI), which have been utilized for surgical planning by providing estimates of white matter tracts (tractography) and their structural connections to surrounding tissues. Diffusion tractography has been used to aid in precise DBS targeting and electrode placement for various neurological disorders including Par-kinson disease, essential tremor, and dystonia 31,32 as well as for pain and psychiatric disorders36
with the goal of improving surgical outcome. The goal of this paper is to review the available literature on the use of DTI tractography in
DBS for OCD and to evaluate DBS connectivity patterns that are associated with improved clinical outcome.
into the review utilizing the following advanced key-word search : (((“tractography”[All Fields] OR “diffusion tensor imaging”[All Fields] OR “DTI”[All Fields] OR “Connectome”[All Fields]) AND (“deep brain stimu-lation”[All Fields] OR “DBS”[All Fields] OR “Neuro-modulation”[All Fields] OR “Stimulation”[All Fields]) AND (“obsessive compulsive disorder”[All Fields] OR “OCD”[All Fields] OR “obsessive-compulsive”[All Fields]))). Once the initial set of studies was selected, the reference list of each selected study was also reviewed to identify any other relevant manuscripts. Strict inclusion and exclusion criteria were determined prior to relevant article selection and full-text analysis to minimize article selection bias. Abstracts, reviews, editorials, conference presentations and single case reports were excluded from the selection, as well as manuscripts that did not meet the selection criteria. The selection criteria necessary for inclusion was the following: (i) studies including hu-man subjects who underwent DBS for treatment-resistant OCD, (ii) DTI/dMRI data was acquired pre-operatively, post-operatively or obtained from normative connectome data, (iii) the DTI data was utilized either for surgical planning or analyzed retrospectively, (iv) baseline status and post-operative patient outcome was reported for all patients. In addition to the method described above, the same advanced keyword search was performed in a second database, Google Scholar, to minimize risk of publication bias. After duplicate articles were screened and excluded, a single relevant article from this addition-al database fit the selection criteria and was included in systematic review. To ascertain the risk of bias and validity of the individual selected studies, each study was analyzed and categorized based on adequacy of randomization, blinding of patients and health care providers, and sample size as shown in Figure 1C. A total of 128 studies were identified in the pre-liminary PubMed search as well as 8 records from review of references. After the initial screening for relevance and applying our subsequent criteria for inclusion, 7 articles (6 from Pubmed and 1 Non-PubMed article) were deter-mined to fit all inclusion criteria and were included in this review. In all cases, post-DBS reduction of at least 35% was considered a responder, unless otherwise noted.Art by Anais Di Via Ioschpe

Page 11Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 ORIG
INA
L RESEARCH
Results: Overview of selected articles
Striatal region targets and associated connectivity profiles
In a trial conducted by Baldermann and col-leagues1, a cohort of 22 patients, (13 female; age = 41.7 ± 12.3 years), who were all diagnosed with severe treatment-refractory OCD underwent bilateral DBS of ALIC/NAC, with the tip of the electrodes located at the posterior border of the nucleus accumbens. A subgroup of 10 patients (8 female) received preoperative diffusion MRI (dMRI). The authors report that stimulation-de-pendent connectivity patterns were calculated separately
for each of the 10 patients with pre-operative dMRI as well as for the additional 12 patients in the study using normative connectivity data (utilizing data from the Human Connectome Project). The investigators identified fibers predictive of effective DBS across the whole sample using the volume of tissue activated (VTA) in each patient, finding a fiber tract within the ventral ALIC that passed by the ventral striatum, bordering the bed nucleus of the stria terminalis, and connecting the medial PFC (mPFC) with the thalamus. Pa-tients with VTAs reaching these white matter areas apical and posterior to the NAC had the highest mean symptomatic improvement. Conversely, they found that fibers associated with negative outcome encompassed streamlines to the medial forebrain bundle (MFB), the posterior limb of the anterior commissure, and fibers within the inferior lateral fascicle. Using the normative connectome data, a region-of-interest (ROI) analysis revealed significant correlations between clinical improvement and VTA connectivity with right middle frontal gyrus (rMFG, r = .602, p = .002). Additionally, clinical outcomes correlated with connectivity to the mPFC and bilat-eral dorsolateral PFC (dlPFC) (r = .630, p < .001) Hartmann et al., investigated and described a similar connectivity pattern that was associated with superior clinical outcome2. They assessed 24-month post-DBS outcomes based on reduction in the Yale-Brown Obsessive Compulsive Scale3 (YBOCS) in 6 patients undergoing ALIC-NA DBS for OCD2. Best responders (2 of the 6 patients), who experienced a 68-86% reduction in YBOCS scores, had unique connectivity profiles with stimulation activating a larger proportion of fibers projecting to the anterior part of the rMFG, with very few fibers projecting to the temporal lobe, superior frontal gyrus, amygdala, and the accumbens area. In a trial led by Liebrand and colleagues 4, clinical outcomes across 12 patients implanted with vALIC DBS for OCD were related to connectivity of the target with two specific fiber bundles: supe-rior outcomes were associated with the active DBS contact being nearer to the MFB and more distant from the anterior thalamic radiation (ATR). This finding was based on 12 month post-DBS YBOCS scores, with 7 responders (≥ 35% improvement) and 5 non-responders. Interestingly, the report of superior outcomes with MFB connectivity stands in contradiction to that of Balderman and colleagues, who found that MFB connectivity was associated with poorer outcomes.
Figure 1. PRISMA flow diagram for systematic literature review.
Figure 1C. Assessment of individual risk of bias in selected studies

Page 12 Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 O
RIG
INA
L RE
SEA
RCH
Tyagi and colleagues reported on a cohort of six patients with treatment refractory OCD who underwent bilateral VC/VS DBS, wherein respond-ers were defined as having a ≥35% reduction in Y-BOCS, consistent with prior reports 7,8,9,10. Five out of 6 patients were responders, with a particu-larly strong improvement in mood (as measured by the Montgomery–Åsberg Depression Rating Scale). Average streamlines generated from individual VTAs were connected to the medial orbitofrontal cortex (OFC), the mediodorsal thalamus, the amyg-dala (via the amygdalofugal pathway), the hypo-thalamus, and the habenula (via the habenulointer-peduncular tract). The medial OFC has been shown to be hyperactive during the early processing of threat-related stimuli in OCD 38. The amygdalofu-gal pathway is an output tract from the basolateral nucleus of the amygdala to the mediodorsal thala-mus and OFC. The habenulointerpeduncular tract has been implicated in the development of depres-sion via inhibition of brainstem serotonergic raphe nuclei 39 . However, the specificity of these tracts relating to therapeutic outcomes is unclear given the high responder rate in this study. Utilizing a novel individualized approach, Barcia and colleagues11 implanted bilateral DBS electrodes in a cohort of 7 treatment-refractory OCD patients (four female), with contacts span-ning the striatum (nucleus accumbens to caudate). Patients then underwent three-month stimulation periods for each contact (as well as sham) followed by clinical evaluation. At the end of the stimulation period, six out of the seven patients were respond-ers (≥35% with a Y-BOCS reduction of 47%. The team attempted to characterize each OCD patient by their individual predominant symptom content via preoperative symptom-provocation fMRI, and evaluated connectivity between prefrontal activa-tions during symptom provocation and the VTA of each of the four DBS contacts. In 6 of 7 patients, the most clinically effective striatal area (termed “best contact”) coincided with the probabilistic tractog-raphy projections from the activated prefrontal areas. While “best contact” connectivity patterns varied among patients, there was a notable overlap in connectivity in 5 of 6 responders, which was localized to a small area in the right frontal pole.
Direct targeting of the ventral tegmental area projec-tion pathway
Coenen and colleagues sought to directly utilize supero-lateral MFB (slMFB) as a DBS target
for treatment refractory OCD in two patients based on a tractographic rendition of the slMFB5. However, since the original report, it has become evident that the projection pathway described did not align with the anatomic definition of the slMFB, prompting the authors to rename this target as the ventral tegmental area projection pathway (vtaPP)12. The medial fore-brain bundle (MFB) as originally defined by Coenen and colleagues using tractography consists of fibers that are oriented medially to the STN, coursing from the VTA superiorly and anteriorly toward the lateral wall of the third ventricle and continuing rostrally toward the nucleus accumbens, septum, and adjacent structures. They further defined the slMFB as that part of the tract that leaves the main trunk of the MFB in the VTA, originating laterally, undercutting the thalamus, and ascending into the inferior portion of the ALIC and demonstrating connectivity the ventral striatum and nucleus accumbens46. Patient specific DBS targeting of the area (vtaPP) was associated with positive clinical outcome, with both patients show-ing significant symptomatic improvement (30%-50% reduction of Y-BOCS scores compared to pre-DBS baseline) at 12 month follow up. Of note, both patients in the study had similar contamination-based manifes-tations of OCD5.
Anteromedial Subthalamic Nucleus as a target and its associated connectivity profile
In the study reported by Tyagi and colleagues, the same cohort of six patients also underwent simul-taneous amSTN (anteromedial subthalamic nucleus), with the purpose of comparatively investigating the most efficacious site as well as each DBS site’s respec-tive effect on mood and cognitive flexibility6. Tyagi et al. results showed that DBS stimulation at each site significantly and equivalently reduced OCD symptoms with little additional gain following combined stimu-lation. The amSTN VTAs showed connectivity to the lateral OFC, dorsal anterior cingulate cortex (dACC), dlPFC, and MFB. DBS of the amSTN, but not the VC/VS, significantly improved cognitive flexibility (as measured by the Cambridge Neuropsychological Test Automated Battery Intra-Extra Dimensional Set-Shift (EDS)), but had a less profound effect on mood, as described earlier in the above section.
Target-independent approaches to identifying OCD related connectivity patterns
Li and colleagues12 sought to identify therapeu-

Page 13Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 ORIG
INA
L RESEARCH
tic connectivity patterns independent of DBS target used, retrospectively analyzing data from two co-horts of OCD patients that underwent DBS of ALIC (N=22, Cologne) or STN (N=14, Grenoble). Using normative connectomic data from the Human Con-nectome Project19, structural connectivity between VTAs and all other brain areas was calculated in both good and poor DBS responders. A fiber bun-dle that was positively discriminative of treatment response emerged independently in both cohorts. This common fiber bundle is connected to the STN and mediodorsal nucleus of the thalamus, traverses through ALIC and has a wide array of frontal con-nections including dACC and ventrolateral PFC (vlPFC). The tract defined exclusively in the STN cohort significantly predicted outcomes in the ALIC cohort, and vice-versa. Li and colleagues further val-idated these findings by successfully cross-predicting clinical improvement in two additional cohorts (Ma-drid: N=8, two electrodes in each patient targeting bilateral nucleus accumbens (NAcc); London: N=6, four electrodes in each patient targeting bilateral ALIC and STN)). They suggest a functional role of cortical input from the dACC and vlPFC to the STN that may be involved in pathological circuitry in OCD.
Summary of Connectivity Profiles Associated with DBS Outcomes:
These studies highlight the connectivity of DBS targets associated with efficacious stimulation for OCD(see figure 1A). Looking at the VC/VS, NA, ALIC target region, Baldermann et al.1 identified that connectivity to the medial and lateral PFC was associated with superior clinical outcomes in DBS to the ALIC/NAC and that effective DBS showed a positive correlation between connectivity to the dlPFC and the mPFC including the cingulate cortex, noting the pivotal role of connectivity to the right MFG for optimal DBS. Similarly, Hartmann et al.2 described that connectivity to the anterior part of the right MFG was associated with superior clinical outcome. Alternatively, Liebrand et al.,4 concluded that DBS outcome correlated with proximity and connectivity to the vtaPP. Notably, in Coenen et al.,5 patient specific DBS targeting of the vtaPP directly was associated with positive clinical outcome. In the investigation conducted by Tyagi and colleagues6, patients were implanted with bilateral electrodes targeting both VC/VS and amSTN. The VC/VS target showed connectivity to the medial OFC, the mediodorsal thalamus, the amygdala (via the amygdalofugal pathway), the hypothalamus, and the habenula (via the habenulointerpeduncular tract) and was associated with positive outcome as well as improvement mood symptoms. The amSTN target showed connectivity to the lateral orbitofron-tal cortex (OFC), dorsal anterior cingulate cortex (DACC), dorsolateral prefrontal cortex (DLPFC), and medial forebrain bundle (MFB) and was also

Page 14 Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 O
RIG
INA
L RE
SEA
RCH
associated with DBS outcome as well as improve-ments in cognitive flexibility. Li et al.12 identified a common fiber bundle associated with DBS outcome, independent of the specific DBS target, that connects the subthalamic nucleus and mediodorsal nucleus of the thalamus, traverses through the anterior limb of the internal capsule and has a wide array of frontal connections including dorsal anterior cingulate cortex and ven-trolateral prefrontal cortex. Barcia and colleagues identified a more symptom-specific approach and concluded that targeting and connectivity associated with optimal outcome varied across patients, but that pre-op-erative MRI index derived from fMRI symptom provocation combined with probabilistic tractog-raphy was able to predict optimal stimulation site. Additionally, 5 of 6 responders showed overlap in connectivity localized to a small area in the right frontal pole. Discussion
Orbitofrontal Cortex (OFC) Connectivity
A recent review by Haber et al. described the connectivity profiles of four OCD DBS sites (ALIC, VS, STN, and midbrain) and concluded that all four sites likely involve OFC/ACC connec-tions passing through, entering, or leaving the IC, however at different locations in the brain44. They also noted that specific cortical region or regions stimulated depend on the specific electrode loca-tion. The authors concluded that ALIC targets can engage all ascending and descending connections as well as connections in the adjacent VS, while the VS target involves VS connections, as well as other ascending and descending connections, including, but not limited to, ALIC and amygdala fibers. These finding illuminate the notion that both ALIC and VS targets engage similar fiber pathways, albeit to varying extents. Similarly, STN and the midbrain also target connections of the OFC/ACC along with their basal ganglia components. The authors noted that an important specification of STN and mid-brain sites is that they likely involve a wider range of diencephalic and brainstem connections through passing fibers. The midbrain site targets a combi-nation of the striato-midbrain, pallido-midbrain, cortico-midbrain, cortico-STN, cortico ZI, and a variety of brainstem targets44. The importance of OFC connectivity was also notably described by Tyagi and colleagues6, in both their VC/VS target as
well as the STN target, highlighting the importance of medial OFC and lateral OFC connectivity, respec-tively, which correlated to DBS outcome. These find-ings would suggest that OFC cortico-striato-thalam-ic circuitry is dysfunctional in OCD. It is understood that the medial and lateral aspects occupy distinct trajectories within the OFC cortico-striato-thalamic circuitry and are functionally distinct40. Abnormal functional connectivity between lateral OFC (Brod-mann areas 10, 11, 47) and caudate nucleus has been shown to be associated with errors in the Cambridge Neuropsychological Test Automated Battery In-tra-Extra Dimensional Set-Shift (EDS) relating to cognitive flexibility in OCD41. Additionally, amSTN DBS has been shown to improve glucose metabolism in OFC (Brodmann areas 10, 11) in association with better Y-BOCS scores42. These findings are com-patible with the observations of this study that the amSTN DBS site was associated with improved EDS performance and that tractography streamlines from activated contacts connected to the lateral OFC.
Right Middle Frontal Gyrus Connectivity
Baldermann et al. and Hartmann et al. each elucidated the importance of right MFG connectiv-ity with DBS outcome in OCD. MFG is within the dlPFC (Brodmann areas 9 and 46), which is associ-ated with executive functions, such as maintaining or shifting sets in response to changing task de-mands48. Previous studies have also highlighted the importance of these areas and associated connectiv-ity patterns as well as modulation of these specific tracts. Nuclear imaging techniques have shown that prefrontal and orbitofrontal cortical metabolism decreases during therapeutic OCD DBS in a similar fashion to the metabolic changes observed during pharmacotherapy or behavioral therapies49,50,51. Similarly, investigations by Figee and colleagues utilized resting-state fMRI scans and revealed that DBS reduced the connectivity between the NAc and the lateral prefrontal cortex (lPFC) and medial prefrontal cortex (mPFC) with stronger connectivity in OCD patients rather than in controls during DBS OFF, but not during DBS ON52. However, while Liebrand and colleagues uti-lized a similar target region (vALIC), the researchers illuminated a different tract/connectivity pattern (MFB) that was correlated to optimal DBS outcome Similarly, Coenen et al demonstrated the signifi-cance of MFB connectivity by targeting the vtaPP directly with positive clinical outcome. Contrasting-ly, Baldermann et al. found that MFB connectivity

Page 15Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 ORIG
INA
L RESEARCH
was negatively associated with clinical outcome. Symptom Specific Targeting
While Li and colleagues describe a unified connectivity profile, we should remain cognizant of the different symptoms that OCD patients can display and that studies suggest that distinct circuit-ry may mediate different patterns of symptomatic improvement. Tyagi and colleagues showed that the VC/VS and STN targets each had different connec-tivity profiles, Notably, while VC/VS target showed connectivity to medial OFC, and STN showed connectivity to lateral OFC, both targets showed equally positive clinical outcome. This finding may further support the involvement of OFC connec-tivity in OCD, which is supported by Haber et al. as discussed previously. They report, however, that the VC/VS target had significant improvement in mood symptoms, while the STN target had significant improvement in cognitive flexibility. This important finding sheds light on the complexity of OCD symp-tomatology, and likewise illuminates the complexity of possible symptom-specific connectivity patterns in this disease. Barcia and colleagues addressed this point in their study by utilizing a symptom-specific and patient-specific approach to mapping and lo-calizing targets. While optimal connectivity profiles varied across patients in their study, the investigators report that connectivity with fMRI-defined activa-tions related to symptom provocation is predictive of outcomes. These studies highlight that while many seek to define a common connectivity profile, further consideration of disease dimensions may be valuable for optimizing connectivity-based targeting.
Unified Tract for Therapeutic Outcomes
Interestingly, despite heterogeneity in symp-tomatology, it is noteworthy that positive outcomes are observed across studies, including significant variation in targeting and connectivity of these targets. This finding therefore could point to the possibility that all of the various proposed targets above may be modulating a single distributed brain network associated with symptoms of OCD, with the addition of each unique target site modulating possible additional unshared tracts or networks. Li and colleagues were able to successful-ly identify the same optimal tract across multiple cohorts in the study, which included both ALIC and STN target sites. Notably, the investigators were able to demonstrate the ability of this optimal tract to predict optimal Y-BOCS across multiple cohorts. The
tract, which traverses the ALIC and connects areas of PFC with STN and MD nucleus of the thalamus, may represent a hyperdirect path connecting frontal regions to the STN. Notably, previously reported OCD targets of amSTN and vtaPP demonstrated the highest connectivity with this unified tract and therefore most predictive of positive outcomes. The unified pathway delineated by Li and colleagues parallels a highly similar pathway within the ALIC, the MFB. This similarity is particularly significant as MFB was additionally highlighted as a pathway that correlated with clinical outcome by both Liebrand et al. and Tyagi et al. Despite important advances in our under-standing of connectivity of therapeutic DBS targets for OCD, we should acknowledge that our experi-ence with DBS for OCD remains limited and that it is important to continue to collect as much data as possible, particularly with respect to connectivi-ty of targets and symptom domains to advance the field. Additionally, the potential inconsistencies and mismatches in nomenclature used to describe differ-ent tracts/pathways may present conflicting results across studies that may theoretically be confirmato-ry if connectivity tract nomenclature and anatomical descriptions were standardized.
Conclusion
The unified tract reported by Li and col-leagues highlights a putative pathological circuit in a complex disease with symptomatologic multiplicity. Additionally, this unified tract demonstrates sig-nificant similarity to the tractographically defined MFB, which may be of particular importance in the newly identified unified tract and in the pathologi-cal circuitry of OCD. While there is likely common circuitry across targets, this does not negate the importance of symptom-specific targeting to select the most appropriate tract for an individual patient. Further investigations in this direction are warrant-ed for the potential utilization of symptom-specific DBS targeting for OCD, which may require sub-categorization of OCD symptomatologic subtypes and associated connectivity patterns to potentially optimize clinical outcome at an individualized level. Importantly, we must accept that the two concepts, that of a unified tract and symptom-specific target-ing within this tract, need not be mutually exclusive.

Page 16 Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 O
RIG
INA
L RE
SEA
RCH
References1. Baldermann JC, Melzer C, Zapf A, Kohl S, Timmermann L, Tittgemeyer M, Huys D, Visser-Vandewalle V, Kühn AA, Horn A, Kuhn J. Connectivity Profile Predictive of Effective Deep Brain Stimulation in Obsessive-Compulsive Disorder. Biol Psychiatry. 2019 May 1;85(9):735-743. doi: 10.1016/j.biopsych.2018.12.019. Epub 2019 Jan 9. PubMed PMID: 30777287.
2. Hartmann CJ, Lujan JL, Chaturvedi A, Goodman WK, Okun MS, McIntyre CC, Haq IU. Tractography Activation Patterns in Dorsolateral Prefrontal Cortex Suggest Better Clinical Responses in OCD DBS. Front Neurosci. 2015;9:519. doi: 10.3389/fnins.2015.00519. eCollection 2015. PubMed PMID: 26834544; PubMed Central PMCID: PMC4717315.
3. Goodman W. K., Price L. H., Rasmussen S. A., Mazure C., Fleischmann R. L., Hill C. L., et al. . (1989). The yale-brown obsessive compulsive scale. I. Development, use, and reliability. Arch. Gen. Psychiatry 46, 1006–1011. 10.1001/archpsyc.1989.01810110048007
4. Liebrand LC, Caan MWA, Schuurman PR, van den Munckhof P, Figee M, Denys D, van Wingen GA. Individual white matter bundle trajectories are associated with deep brain stimulation response in obsessive-compulsive disorder. Brain Stimul. 2019 Mar - Apr;12(2):353-360. doi: 10.1016/j.brs.2018.11.014. Epub 2018 Nov 27. PubMed PMID: 30522916.
5. Coenen VA, Schlaepfer TE, Goll P, Reinacher PC, Voderholzer U, Tebartz van Elst L, Urbach H, Freyer T. The medial forebrain bundle as a target for deep brain stimulation for obsessive-compulsive disorder. CNS Spectr. 2017 Jun;22(3):282-289. doi: 10.1017/S1092852916000286. Epub 2016 Jun 8. PubMed PMID: 27268576.
6. Tyagi H, Apergis-Schoute AM, Akram H, Foltynie T, Limousin P, Drummond LM, Fineberg NA, Matthews K, Jahanshahi M, Robbins TW, Sahakian BJ, Zrinzo L, Hariz M, Joyce EM. A Randomized Trial Directly Comparing Ventral Capsule and Anteromedial Subthalamic Nucleus Stimulation in Obsessive-Compulsive Disorder: Clinical and Imaging Evidence for Dissociable Effects. Biol Psychiatry. 2019 May 1;85(9):726-734. doi: 10.1016/j.biopsych.2019.01.017. Epub 2019 Jan 30. PMID: 30853111; PMCID: PMC6467837.
7. Abelson J.L., Curtis G.C., Sagher O., Albucher R.C., Harrigan M., Taylor S.F. Deep brain stimulation for refractory obsessive-compulsive disorder. Biol Psychiatry. 2005;57:510–516.
8. Goodman W.K., Foote K.D., Greenberg B.D., Ricciuti N., Bauer R., Ward H. Deep brain stimulation for intractable obsessive compulsive disorder: Pilot study using a blinded, staggered-onset design. Biol Psychiatry. 2010;67:535–542.
9. Denys D., Mantione M., Figee M., van den Munckhof P., Koerselman F., Westenberg H. Deep brain stimulation of the nucleus accumbens for treatment-refractory obsessive-compulsive disorder. Arch Gen Psychiatry. 2010;67:1061–1068.
10. Luyten L., Hendrickx S., Raymaekers S., Gabriels L., Nuttin B. Electrical stimulation in the bed nucleus of the stria terminalis alleviates severe obsessive-compulsive disorder. Mol Psychiatry. 2016;21:1272–1280.
11. Barcia JA, Avecillas-Chasín JM, Nombela C, Arza R, García-Albea J, Pineda-Pardo JA, Reneses B, Strange BA. Personalized striatal targets for deep brain stimulation in obsessive-compulsive disorder. Brain Stimul. 2019 May - Jun;12(3):724-734. doi: 10.1016/j.brs.2018.12.226 Epub 2018 Dec 20. PubMed PMID: 30670359.
12. Ningfei Li, Juan Carlos Baldermann, Astrid Kibleur, Svenja Treu, Harith Akram, Gavin J.B. Elias, Alexandre Boutet, Andres M. Lozano, Ludvic Zrinzo, Eileen Joyce, Stephan Chabardes, Veerle Visser-Vandewalle, Mircea Polosan, Jens Kuhn, Andrea A. Kühn, Andreas Horn. Toward a unified connectomic target for deep brain stimulation in obsessive-compulsive disorder. February 25, 2020 doi: https://doi.org/10.1101/608786 Pre-print, https://www.biorxiv.org/content/10.1101/608786v3.article-info Now Published (7-3-2020)
13.. Horn, A. et al. Connectivity Predicts deep brain stimulation outcome in Parkinson disease. Ann. Neurol. 82, 67–78 (2017).
14. Baldermann, J. C. et al. Connectivity profile predictive of effective deep brain stimulation in obsessive compulsive disorder. Biol. Psychiatry (2019) doi:10.1016/j.biopsych.2018.12.019.
15. Ewert, S. et al. Toward defining deep brain stimulation targets in MNI space: A subcortical atlas based on multimodal MRI, histology and structural connectivity. NeuroImage 170, 271–282 (2018).
16. Horn, A. et al. Probabilistic conversion of neurosurgical DBS electrode coordinates into MNI space. NeuroImage 150, 395–404 (2017).
17. Neumann, W.-J. et al. Functional segregation of basal ganglia pathways in Parkinson’s disease. Brain 141, 2655–2669 (2018).
18. Horn, A. et al. Lead-DBS v2: Towards a comprehensive pipeline for deep brain stimulation imaging. NeuroImage 184, 293–316 (2019)
19. Van Essen, D. C. et al. The WU-Minn Human Connectome Project: An overview. NeuroImage 80, 62–79 (2013).
20. P. Blomstedt, R.L. Sjöberg, M. Hansson, O. Bodlund, M.I. Hariz Deep brain stimulation in the treatment of obsessive-compulsive disorder World Neurosurg, 80 (2013), 10.1016/j.wneu.2012.10.006
21. D. Denys. Deep brain stimulation of the nucleus accumbens for treatment-refractory Obsessive-Compulsive Disord, 67 (2014), pp. 1061-1068
22. J. Pepper, M. Hariz, L. Zrinzo. Deep brain stimulation versus anterior capsulotomy for obsessive-compulsive disorder: a review of the literature. J Neurosurg, 122 (2015), pp. 1028-1037, 10.3171/2014.11.JNS132618
23. M. van Westen, E. Rietveld, M. Figee, D. Denys. Clinical outcome and mechanisms of deep brain stimulation for obsessive-compulsive disorder. Curr Behav Neurosci Rep, 2 (2015), pp. 41-48, 10.1007/s40473-015-0036-3
24. N. Lipsman, J.S. Neimat, A.M. Lozano. Deep brain stimulation for treatment-refractory obsessive-compulsive disorder: the search for a valid target. Neurosurgery, 61 (2007), pp. 1-11, 10.1227/01.neu.0000279719.75403.f7
25. M.H. Bloch, A. Landeros-Weisenberger, M.C. Rosario, C. Pittenger, J.F. Leckman.Meta-analysis of the symptom structure of obsessive-compulsive disorder. Am J Psychiatry, 165 (2008), pp. 1532-1542, 10.1176/appi.ajp.2008.08020320
26. V. Sturm, D. Lenartz, A. Koulousakis, H. Treuer, K. Herholz, J.C. Klein, et al.The nucleus accumbens: a target for deep brain stimulation in obsessive-compulsive- and anxiety-disorders. J Chem Neuroanat, 26 (2003), pp. 293-299, 10.1016/j.jchemneu.2003.09.003

Page 17Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 ORIG
INA
L RESEARCH
27. B.D. Greenberg, L a Gabriels, D a Malone, a R. Rezai, G.M. Friehs, M.S. Okun, et al. Deep brain stimulation of the ventral internal capsule/ventral striatum for obsessive-compulsive disorder: worldwide experience. Mol Psychiatr, 15 (2010), pp. 64-79, 10.1038/mp.2008.55
28. L. Mallet, M. Polosan, N. Jaafari, N. Baup, M.-L. Welter, D. Fontaine, et al. Subthalamic nucleus stimulation in severe obsessive-compulsive disorder N Engl J Med, 359 (2008), pp. 2121-2134, 10.1056/NEJMoa0708514
29. B. Nuttin, P. Cosyns, H. Demeulemeester, J. Gybels, B. Meyerson Electrical stimulation in anterior limbs of internal capsules in patients with obsessive-compulsive disorder. Lancet, 354 (1999), p. 1526, 10.1016/S0140-6736(99)02376-4
30. F. Jimenez-Ponce, F. Velasco-Campos, G. Castro-Farfan, H. Nicolini, A.L. Velasco, R. Salin-Pascual, et al. Preliminary study in patients with obsessive-compulsive disorder treated with electrical stimulation in the inferior thalamic peduncle. Neurosurgery, 65 (2009), pp. 203-209, 10.1227/01.NEU.0000345938.39199.90
31. Diffusion Tractography in Deep Brain Stimulation Surgery: A Review. Calabrese E. Front Neuroanat. 2016; 10():45.
32. Integrating diffusion tensor imaging-based tractography into deep brain stimulation surgery: a review of the literature. Torres CV, Manzanares R, Sola RG Stereotact Funct Neurosurg. 2014; 92(5):282-90.
33. Luyten, L., Hendrickx, S., Raymaekers, S., Gabriëls, L. & Nuttin, B. Electrical stimulation in the bed nucleus of the stria terminalis alleviates severe obsessive-compulsive disorder. Mol. Psychiatry 21, 1272–1280 (2016)
34.Nair, G., Evans, A., Bear, R. E., Velakoulis, D. & Bittar, R. G. The anteromedial GPi as a new target for deep brain stimulation in obsessive compulsive disorder. J. Clin. Neurosci. 1, 815–821 (2014).
35. Maarouf, M. et al. Deep Brain Stimulation of Medial Dorsal and Ventral Anterior Nucleus of the Thalamus in OCD: A Retrospective Case Series. PLOS ONE 11, e0160750 (2016)
36. See AAQ, King NKK. Improving Surgical Outcome Using Diffusion Tensor Imaging Techniques in Deep Brain Stimulation. Front Surg. 2017;4:54. doi: 10.3389/fsurg.2017.00054. eCollection 2017. Review. PubMed PMID: 29034243; PubMed Central PMCID: PMC5625016.
37. Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(7): e1000097. doi:10.1371/journal.pmed1000097
38. Apergis-Schoute A.M., Gillan C.M., Fineberg N.A., Fernandez-Egea E., Sahakian B.J., Robbins T.W. Neural basis of impaired safety signaling in obsessive compulsive disorder. Proc Natl Acad Sci U S A. 2017;114:3216–3221
39. Hikosaka O. The habenula: From stress evasion to value-based decision-making. Nat Rev Neurosci. 2010;11:503–513.
40. Fettes P., Schulze L., Downar J. Cortico-Striatal-thalamic loop circuits of the orbitofrontal cortex: Promising therapeutic targets in psychiatric illness. Front Syst Neurosci. 2017;11:25.
41. Vaghi M.M., Vertes P.E., Kitzbichler M.G., Apergis-Schoute A.M., van der Flier F.E., Fineberg N.A. Specific frontostriatal circuits for impaired cognitive flexibility and goal-directed planning in obsessive-compulsive disorder: Evidence from resting-state functional connectivity. Biol Psychiatry. 2017;81:708–717.
42. Le Jeune F., Verin M., N’Diaye K., Drapier D., Leray E., Du Montcel S.T. Decrease of prefrontal metabolism after subthalamic stimulation in obsessive-compulsive disorder: A positron emission tomography study. Biol Psychiatry. 2010;68:1016–1022.
43. Dougherty D.D., Baer L., Cosgrove G.R., Cassem E.H., Price B.H., Nierenberg A.A. Prospective long-term follow-up of 44 patients who received cingulotomy for treatment-refractory obsessive-compulsive disorder. Am J Psychiatry. 2002;159:269–275.
44. Haber, Suzanne N., Yendiki, Anastasia., Jbabdi, Saad. Four deep brain stimulation targets for obsessive-compulsive disorder: Are they different? Biological Psychiatry 0,0, 7 2020
45. Raviv N, Staudt MD, Rock AK, MacDonell J, Slyer J, Pilitsis JG. A Systematic Review of Deep Brain Stimulation Targets for Obsessive Compulsive Disorder. Neurosurgery. 2020 Jul 2;87(6):1098–110. doi: 10.1093/neuros/nyaa249. Epub ahead of print. PMID: 32615588; PMCID: PMC7666902.
46. Coenen VA, Panksepp J, Hurwitz TA, Urbach H, Mädler B. Human medial forebrain bundle (MFB) and anterior thalamic radiation (ATR): imaging of two major subcortical pathways and the dynamic balance of opposite affects in understanding depression. J Neuropsychiatry Clin Neurosci. 2012 Spring;24(2):223-36. doi: 10.1176/appi.neuropsych.11080180. PMID: 22772671.
47. Coenen, Volker A., et al. “Medial forebrain bundle stimulation as a pathophysiological mechanism for hypomania in subthalamic nucleus deep brain stimulation for Parkinson’s disease.” Neurosurgery 64.6 (2009): 1106-1115.
48.Bonelli, Raphael M., and Jeffrey L. Cummings. “Frontal-subcortical circuitry and behavior.” Dialogues in clinical neuroscience 9.2 (2007): 141.
49.Swedo, S. E., Pietrini, P., Leonard, H. L., Schapiro, M. B., Rettew, D. C., Goldberger, E. L., et al. (1992). Cerebral glucose metabolism in childhood-onset obsessive-compulsive disorder. Revisualization during pharmacotherapy. Arch. Gen. Psychiatry 49, 690–694. doi: 10.1001/archpsyc.1992.01820090018003
50. Nuttin, B. J., Gabriëls, L. A., Cosyns, P. R., Meyerson, B. A., Andréewitch, S., Sunaert, S. G., et al. (2003). Long-term electrical capsular stimulation in patients with obsessive-compulsive disorder. Neurosurgery 52, 1263–1272. discussion: 1272–1264. doi: 10.1227/01.neu.0000064565.49299.9a
51. Van Laere, K., Nuttin, B., Gabriels, L., Dupont, P., Rasmussen, S., Greenberg, B. D., et al. (2006). Metabolic imaging of anterior capsular stimulation in refractory obsessive-compulsive disorder: a key role for the subgenual anterior cingulate and ventral striatum. J. Nucl. Med. 47, 740–747.
52. Figee, M., Luigjes, J., Smolders, R. et al. Deep brain stimulation restores frontostriatal network activity in obsessive-compulsive disorder. Nat Neurosci 16, 386–387 (2013). https://doi.org/10.1038/nn.3344

Page 18 Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021CO
MM
ENTA
RY/R
EVIE
W
Abstract Research from the first year of the COVID-19 pandemic has demonstrated that pregnant individuals are at greater risk of severe illness from SARS-CoV-2 infections. However, despite early warnings from medical organizations, pregnant individuals were excluded in clinical trials, resulting in little data on the safety and efficacy of the COVID-19 vaccine in pregnancy in the early stage of the COVID-19 vaccine roll-out. The absence of pregnant individuals in clinical trial data creates a significant gap in data for the pregnant population regarding the COVID-19 vaccine and provides limited guidance for obstetrical healthcare providers in counseling their patients. As of October 2021, the CDC reports that an estimated mere 33.8 percent of the pregnant population in the US has been vaccinated. The example of the COVID-19 vaccine clinical trials and roll-out strongly argues for reevaluation of inclusion of pregnant individuals in early clinical trials to better inform this population and their health providers on the safety and benefits of specific vaccinations during pregnancy.
Introduction
As the new variants of the SARS-CoV-2 virus spread across the world creating another wave of COVID-19 infections, hospital admissions and the number of critically ill patients rise. Re-cent data from the University of Toronto suggests that the Delta variant of SARS-CoV-2 has shown a 235 percent increase in ICU admissions and a 133 percent rise in deaths when compared to prior variants1. With this new rise in COVID-19 cases and virulence of the Delta variant, the populations that are more vulnerable to severe illness from SARS-CoV-2 are once again at greater risk. Severe COVID-19 illness in pregnant persons is associat-ed with greater rates of infection, hospitalization, ICU admissions and case-fatality2,3,4. Studies have also found associations between COVID-19 in-fection and preterm deliveries, pre-eclampsia, and cesarean sections5,6. The adverse maternal and fetal outcomes associated with COVID-19 infections highlight the importance of vaccine access and vaccine acceptance for pregnant persons. Howev-er, pregnant people were excluded from the 2020 phase three SARS-CoV-2 vaccine clinical trials of Pfizer, Moderna, Janssen, Sinovac, and Astra-Zene-ca7.
Historical perspective on exclusion of pregnant indi-viduals from clinical trials
While the Food and Drug Administra-tion (FDA) was in part established in response to ‘tonics’ prescribed to women that contained addictive drugs (resulting in the Food and Drugs Act in 19068 and the Nuremburg trials in 1946, which emphasized the rights of human research subjects leading to the Universal Declaration of Human Rights9), it was actually in the 1960-70s when protectionist policies regarding participants of reproductive age and pregnant individuals in clinical research were formed. In 1961-1962, a new drug, Thalidomide, given to treat morning sickness was found to have severe teratogenic effects10. In addition, in 1971 and 1974, individuals who used diethylstilbestrol (DES) as a contraceptive device were found to have severe adverse health outcomes
COVID-19 Vaccines: Importance of Including Pregnant Individuals in Clinical Trials Yael Frank1, Alisa Kachikis2
1 Sackler School of Medicine, Tel Aviv University, Tel Aviv2Department of Obstetrics and Gynecology, University of Washington, Seattle
Art by Jonathan Sokal

Page 19Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 COM
MEN
TARY/REVIEW
in their female children11,12. In 1975, the US De-partment of Health and Human Services (DHHS) designated pregnant individuals as a “vulnerable population” with limitations in research involve-ment9,13. This was extended to early phases of clini-cal trials on pharmaceuticals in 1977 by the FDA8. Within a short period of time, pregnant individu-als were effectively excluded from participation in any early clinical trial14. More recently, discussions on involvement of pregnant individuals in research has shifted from a protectionist to an inclusionist view. An example of global inclusionist policy aimed at involving the pregnant population in research and vaccine initiatives includes the MenAfriVac mass immunization campaigns in 2010. The WHO’s Global Advisory Committee on Vaccine Safety concluded that MenAfriVac should be offered to anyone pregnant due to clear evidence of benefit from immunization, no alternative way to protect against meningococcal disease, risk for disease in the specific geographical area and lack of adverse safety15. Today, researchers and medical profession-als know much more about which drugs cross the placenta and which substances could potentially present risks to the fetus. However, protectionist views appear to prevail over inclusionist perspec-tives and pregnant persons are still excluded from most clinical trials. This was the case during the Ebola treatment trials in West Africa in 2013-201616,17,18 and now during the COVID-19 pan-demic, in which despite recommendations from public health authorities including the Centers for Disease Control and Prevention (CDC), the Amer-ican College of Obstetricians and Gynecologists (ACOG), and the American Academy of Pediatrics (AAP), pregnant individuals were not included in COVID-19 vaccine phase 2 or 3 clinical trials19,20. In the case of the vaccine for SARS-CoV-2, the Emergency Use Authorization (EUA) by the FDA of Pfizer’s and Moderna’s messenger RNA (mRNA) - based vaccines created a dramatic par-adigm shift. Despite the exclusion of the pregnant population from clinical trials, pregnant persons were deemed eligible to be vaccinated. As a re-sponse to the EUA, the Advisory Committee on Immunization Practices (ACIP) made an interim recommendation for use of the Pfizer-BioN-Tech BNT162b2 and the Moderna mRNA-1273 COVID-19 vaccine in persons ≥ 16 and 18 years, respectively21. The Society for Maternal-Fetal Med-
icine (SMFM) and ACOG strongly recommended that pregnant individuals be given the opportunity to re-ceive the COVID-19 vaccination, especially healthcare workers with increased exposure to the virus, given the rationale that COVID-19 infection in pregnancy is associated with increased risk of adverse events. Fur-thermore, there may be added benefit for fetuses from transplacental antibody transfer, and neonates and infants may benefit from antibodies in breast milk22,23. The broadly accepted “protection by exclusion” prac-tice in protectionist policies therefore placed a burden on health authorities, and pregnant individuals had to decide whether to receive the vaccine with virtually no clinical data on safety or efficacy. COVID-19 vaccines and pregnancy
Art by Jonathan Sokal
The safety information available prior to phase three clinical trials did not suggest any specific con-cerns for the SARS-CoV-2 mRNA vaccines in preg-nancy. The mRNA in the Pfizer-BioNTech BNT162b2 and Moderna mRNA-1273 vaccines encodes the spike protein, a part of the SARS-CoV-2 viral envelope. Once delivered to the host, vaccine mRNA enters host cells which use the mRNA to generate the spike protein and stimulate the immune system to form antibodies against this protein. The vaccine does not contain live virus and mRNA delivered in the vac-cine does not enter the nucleus of the cell and does not alter host DNA24. Furthermore, no adverse safety signals were found in developmental and reproduc-tive toxicity (DART) animal studies for Pfizer-BioN-Tech BNT162b2, Moderna mRNA-1273, and Janssen (Johnson and Johnson) viral vector vaccines24. A small number of people who participated in clinical trials for Pfizer, Moderna, Janssen and AstraZeneca became pregnant after enrolling in the studies. These individu-als had similar miscarriage rates compared to baseline

Page 20 Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021CO
MM
ENTA
RY/R
EVIE
W
data without safety concerns, however the small number of individuals limits interpretation of this data25. Since the FDA’s EUA for COVID-19 vac-cines, several studies have collected observational data on the outcomes in pregnant individuals who chose to get vaccinated. A study conducted in one of Israel’s largest Health Maintenance Organizations found similar vaccine efficacy in pregnant individ-uals compared to the general population26. Studies by the CDC have found vaccinated persons to have similar rates of adverse pregnancy outcomes and miscarriages compared to the general pregnant pop-ulation27,28. Overall, pregnant individuals were found to tolerate COVID-19 vaccines well29. More recently, due to the severity of COVID-19 infections in pregnancy with the Delta variant, the CDC, ACOG and SMFM have released statements recommending COVID-19 vaccines in pregnancy, and have also recently recommended that pregnant individuals receive a booster dose of a vaccine if six months have passed since the previous vaccination30,31. While more observational studies are currently ongoing, the delay in presenting data on the safety and efficacy of COVID-19 vaccines in pregnancy, as well as providing clear recommenda-tions for vaccination guidelines in pregnancy, has had a serious cost. Many pregnant persons chose to defer vaccination. A study on vaccination practices among reproductive-aged healthcare providers in the priority group for COVID-19 vaccination found that compared to non-pregnant individuals of re-productive age, individuals who were pregnant were six times more likely to delay receiving a COVID-19 vaccine and twice as likely to decline altogether32. As of October 2021, only 33.8 percent of pregnant persons in the US are estimated to have received a COVID-19 vaccine based on CDC surveillance33.
Conclusion
In summary, the inclusion of pregnant indi-viduals in clinical trials is of utmost importance and would greatly benefit the healthcare of this popu-lation in a future pandemic. In the example of the COVID-19 vaccine roll-out, pregnant individuals were given the option to be vaccinated given the risks associated with COVID-19 infection in preg-nancy. Yet, due to the exclusion of pregnant people in vaccine trials, there was a lack of data early on and lack of a clear recommendation for COVID-19 vaccination in the pregnant population which creat-ed increased hesitancy to receive the vaccine. Exclu-
sion of specific populations from clinical trials should be based on scientific evidence such as safety concerns from animal studies or phase 1 and 2 clinical trials. Experts in obstetrics and maternal-fetal medicine could provide insight on the broader effects of including or ex-cluding pregnant individuals in specific research stud-ies. The COVID-19 vaccine roll-out illustrates that the decision to include the pregnant population in future vaccine clinical trials could have potentially life-saving effects.
References1. Fisman DN, Tuite AR. Evaluation of the relative virulence of novel SARS-CoV-2 variants: a retrospective cohort study in Ontario, Canada. Canadian Medical Association Journal. 2021:cmaj.211248.
2. Zambrano LD, Ellington S, Strid P, Galang RR, Oduyebo T, Tong VT, et al. Update: Characteristics of Symptomatic Women of Reproductive Age with Laboratory-Confirmed SARS-CoV-2 Infection by Pregnancy Status - United States, January 22-October 3, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(44):1641-7.
3. Delahoy MJ, Whitaker M, O’Halloran A, Chai SJ, Kirley PD, Alden N, et al. Characteristics and Maternal and Birth Outcomes of Hospitalized Pregnant Women with Laboratory-Confirmed COVID-19 - COVID-NET, 13 States, March 1-August 22, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(38):1347-54.
4. Chinn J, Sedighim S, Kirby KA, Hohmann S, Hameed AB, Jolley J, et al. Characteristics and Outcomes of Women With COVID-19 Giving Birth at US Academic Centers During the COVID-19 Pandemic. JAMA Netw Open. 2021;4(8):e2120456.
5. Papageorghiou AT, Deruelle P, Gunier RB, Rauch S, García-May PK, Mhatre M, et al. Preeclampsia and COVID-19: results from the INTERCOVID prospective longitudinal study. Am J Obstet Gynecol. 2021.
6. Khoury R, Bernstein PS, Debolt C, Stone J, Sutton DM, Simpson LL, et al. Characteristics and Outcomes of 241 Births to Women With Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection at Five New York City Medical Centers. Obstet Gynecol. 2020;136(2):273-82.
7. Doshi P. Will covid-19 vaccines save lives? Current trials aren’t designed to tell us. BMJ. 2020;371:m4037.
8. U.S. Food and Drug Administration. 100 Years of Protecting and Promoting Women’s Health: U.S. Department of Health and Human Services; 2015 [Available from: https://www.fda.gov/ForConsumers/ByAudience/ForWomen/ucm118458.htm#1906:_Fight ing_Addictive__Medicines.
9. Stevens PE, Pletsch PK. Informed consent and the history of inclusion of women in clinical research. Health Care Women Int. 2002;23(8):809-19.
10. Administration USFaD. About the Office of Scientific Investigations: U.S. Department of Health and Human Services; 2014 [Available from: https://www.fda.gov/AboutFDA/CentersOffices/OfficeofMedicalProductsandTobacco/CDER/ucm091393.htm.
Page 21Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 COM
MEN
TARY/REVIEW
11. Centers for Disease Control and Prevention. DES History: CDC; 2011 [Available from: https://www.cdc.gov/des/consumers/about/history.html.
12. Elevated risk of pelvic inflammatory disease among women using the Dalkon Shield. MMWR Morbidity and mortality weekly report. 1983;32(17):221-2.
13. Johnson T, Fee E. Women’s Participation in Clinical Research: From Protectionism to Access. In: Mastroianni A, Faden R, Federman D, editors. Women and Health Research: Ethical and Legal Issues of Including Women in Clinical Studies, Volume 2 Workship and Commissioned Papers Washington (DC): National Academy Press (US); 1994.
14. McCarthy CR. Historical background of clinical trials involving women and minorities. Acad Med. 1994;69(9):695-8.
15. World Health Organization. Committee concludes that new meningitis vaccine is safe and should be offered to pregnant women: WHO; 2011 [Available from: http://www.who.int/immunization/newsroom/newsstory_meningitis_vaccine_safe_pregnancy_jan2011/en/.
16. Alirol E, Kuesel AC, Guraiib MM, dela Fuente-Núñez V, Saxena A, Gomes MF. Ethics review of studies during public health emergencies - the experience of the WHO ethics review committee during the Ebola virus disease epidemic. BMC Medical Ethics. 2017;18:43.
17. World Health Organization. Managing Ethical Issues in Infectious Disease Outbreaks. Geneva: WHO; 2016.
18. Gomes MF, de la Fuente-Nunez V, Saxena A, Kuesel AC. Protected to death: systematic exclusion of pregnant women from Ebola virus disease trials. Reproductive health. 2017;14(Suppl 3):172.
d Legal Issues of Including Women in Clinical Studies, Volume 2 Workship and Commissioned Papers Washington (DC): National Academy Press (US); 1994.
14. McCarthy CR. Historical background of clinical trials involving women and minorities. Acad Med. 1994;69(9):695-8.
15. World Health Organization. Committee concludes that new meningitis vaccine is safe and should be offered to pregnant women: WHO; 2011 [Available from: http://www.who.int/immunization/newsroom/newsstory_meningitis_vaccine_safe_pregnancy_jan2011/en/.
16. Alirol E, Kuesel AC, Guraiib MM, dela Fuente-Núñez V, Saxena A, Gomes MF. Ethics review of studies during public health emergencies - the experience of the WHO ethics review committee during the Ebola virus disease epidemic. BMC Medical Ethics. 2017;18:43.
17. World Health Organization. Managing Ethical Issues in Infectious Disease Outbreaks. Geneva: WHO; 2016.
18. Gomes MF, de la Fuente-Nunez V, Saxena A, Kuesel AC. Protected to death: systematic exclusion of pregnant women from Ebola virus disease trials. Reproductive health. 2017;14(Suppl 3):172.
19. Smith DD, Pippen JL, Adesomo AA, Rood KM, Landon MB, Costantine MM. Exclusion of Pregnant Women from Clinical Trials during the Coronavirus Disease 2019 Pandemic: A Review of International Registries. Am J Perinatol. 2020;37(8):792-9.
20. Steenhuysen J. Large U.S. COVID-19 vaccine trials will exclude pregnant women for now Online: Reuters; [updated 31 July 2020. Available from: https://www.reuters.com/article/us-health-coronavirus-vaccines-pregnancy/large-u-s-covid-19-vaccine-trials-will-exclude-pregnant-women-for-now-idUSKCN24W1NZ.
21. Oliver S, Gargano J, Marin M, al e. The Advisory Committee on Immunization Practices’ Interim Recommendation for Use of Moderna COVID-19 Vaccine — United States, December 2020. . MMWR Morb Mortal Wkly Rep 2021;69:1653-6.
22. Society for Maternal-Fetal Medicine. Society for Maternal-Fetal Medicine (SMFM) Statement: SARS-CoV-2 Vaccination in Pregnancy 2020 [updated 1 December 2020. Available from: https://s3.amazonaws.com/cdn.smfm.org/media/2591/SMFM_Vaccine_Statement_12- 1-20_(final).pdf
23. American College of Obstetricians and Gynecologists. Practice Advisory: COVID-19 Vaccination Considerations for Obstetric–Gynecologic Care 2020 [updated 30 July 2021. Available from: https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2020/12/covid-19-vaccination-considerations-for-obstetric-gynecologic-care.
24. Zhang C, Maruggi G, Shan H, Li J. Advances in mRNA Vaccines for Infectious Diseases. Frontiers in Immunology 2019;10:594. doi:10.3389/fimmu.2019.00594.
25. Male V. Are COVID-19 vaccines safe in pregnancy? Nat Rev Immunol. 2021;21(4):200-1.
26. Dagan, N, Barda, N, Biron-Shental, T, et al. Effectiveness of the BNT162b2 mRNA COVID-19 vaccine in pregnancy. Nat Med 2021;27:1693–1695. https://doi.org/10.1038/s41591-021-01490-8.
27. Shimabukuro TT, Kim SY, Myers TR, Moro PL, Oduyebo T, Panagiotakopoulos L, et al. Preliminary Findings of mRNA Covid-19 Vaccine Safety in Pregnant Persons. N Engl J Med. 2021.
28. Zauche L WB, Smoots AN, Olson CK, Oduyebo T, Kim SY, Peterson EE, Ju J, Beauregard J, Wilcox AJ, Rose CE, Meaney-Delman D, Ellington SR, . Receipt of mRNA COVID-19 vaccines preconception and during pregnancy and risk of self-reported spontaneous abortions, CDC v-safe COVID-19 Vaccine Pregnancy Registry 2020-21 2021 [Available from: https://assets.researchsquare.com/files/rs-798175/v1/3cacf992-b20b-4da3-810f-ef4f23046b8f.pdf?c=1628775201].
29. Kachikis A, Englund JA, Singleton M, Covelli I, Drake AL, Eckert LO. Short-term Reactions Among Pregnant and Lactating Individuals in the First Wave of the COVID-19 Vaccine Rollout. JAMA Netw Open. 2021;4(8):e2121310.
30. ACOG. COVID-19 Vaccines and Pregnancy: Conversation Guide 2021 [updated 2021. Available from: https://www.acog.org/covid-19/covid-19-vaccines-and-pregnancy-conversation-guide-for-clinicians].
31. SMFM. Provider Considerations for Engaging in COVID-19 Vaccine Counseling With Pregnant and Lactating Patients 2021 [updated 26 October 2021. Available from: https://s3.amazonaws.com/cdn.smfm.org/media/3201/Provider_Considerations_for_Engaging_in_COVID_Vaccination_Considerations_10-26-21_%28final%29.pdf].
32. Townsel C, Moniz MH, Wagner AL, et al. COVID-19 vaccine hesitancy among reproductive-aged female tier 1A healthcare workers in a United States Medical Center. J Perinatol. 2021;41(10):2549-2551. doi:10.1038/s41372-021-01173-9.

Page 22 Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 CO
MM
ENTA
RY/R
EVIE
W
Introduction
The cornea is the anterior most translucent part of the eye. It functions not only to protect, but also to focus light onto the retina and aid with visual acuity. The corneal epithelium is rehabili-tated and sustained by corneal epithelial stem cells (limbal stem cells) located at the limbus, the junc-tion between the conjunctiva and cornea.1 Limbal stem cells are maintained and differentiated into corneal epithelium by key molecular events aided by Wnt proteins: lipid-modified glycoproteins. Wnt proteins allow communication between corneal epi-thelial cells to help regulate cell growth, function, differentiation, and cell death.2 The Wnt signaling pathways have been char-acterized by three different pathways: the canon-ical, the noncanonical planar cell polarity (PCP), and the noncanonical Wnt/calcium. All pathways begin with the Wnt protein binding to a frizzled class receptor (FZD) and transducing a signal to a Disheveled protein (Dvl) within the cell. However, the canonical Wnt pathway leads to regulating gene transcription, while the noncanonical PCP and noncanonical Wnt/calcium pathway lead to regu-lating the cytoskeleton and calcium inside the cell, respectively.3 Mutations and alterations in the Wnt protein and signaling pathways may be responsible for diseases and pathological processes in the eye. This review will be focusing on Wnt signaling in the cornea.
Development
The molecular events of Wnt signaling begin as early as ocular surface ectoderm differenti-ation.4 Data from a two dimensional colony of hu-man induced pluripotent stem cells (hiPSC) model mimicking early human eye development demon-strated that Bone Morphogenetic Protein 4 (BMP4) and Wnt signaling play a role in the development of ocular surface ectoderm.4 In differentiating hiPSCs,
putative antagonists of Wnt signaling, secreted frizzled related protein-2 (SFRP2) and Dickkopf1(DKK1), are highly expressed in the neural ectoderm. Additionally, application of exogenous BMP4 to hiPSCs supports Wnt signaling inhibition which increases expression of both p63 and PAX6, which are known drivers to induce the differentiation of ocular surface ectoderm into corne-al epithelia. Thus, in the very earliest stages of human eye development, a fine balance of BMP4 exposure and WNT inhibition determines the specification of surface ectodermal lineage and its fate.4
Another study utilizing RNA-sequence anal-ysis on chick periocular neural crest (pNC) showed differential expression of Wnt signaling.5 The analysis demonstrated significant expression (p<0.05) in several ligands involved in the canonical pathway (i.e Wnt2B, Wnt4, Wnt5A, Wnt6, Wnt9A, and Wnt9B), PCP path-way (i.e DAMM2, MAPK10, ROCK2, PRICKLE2, RHOA, RAC1, CDC42), and Wnt/calcium pathway (i.e NFACTC1, PRKCA, CAMK2D, RYK, CAMK2B) in
Art by Anais Di Via Ioschpe
Wnt Signaling in Corneal Diseases and Wound HealingSean Ghiam1,2, Ruchi Shah Ph.D1, Alexander Ljubimov Ph.D1.1Cedars-Sinai Medical Center, Board of Governs Regenerative Medicine Institute, Eye Program, Los Angeles, CA 2Sackler School of Medicine, Tel Aviv University, Tel Aviv

Page 23Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 COM
MEN
TARY/REVIEW
pNC and neural crest-derived corneal cell develop-ment into highly specialized corneal endothelial cells and keratocytes. The expression of the genes were val-idated by in situ hybridization. Thus, these candidates may be involved in establishing the corneal endothe-lium and keratocyte identity by inducing cell migra-tion and polarity during development.5 This data may further help future analyses on molecular signaling involved in neural crest cell differentiation and offer insight into genes involved in corneal dysgenesis and diseases.
Keratoconus
Keratoconus is a progressive noninflamma-tory disease in which the cornea thins and bulges out-ward into a cone shape. This may result in irregular astigmatism, blurred vision, glare, and sensitivity to light.6 Keratoconus is the most common cause of cor-neal transplant in developing countries with a prev-alence of 1.38 per 1000 worldwide and 0.17 per 1000 in the United States.7 This disease can be described as multifactorial due to its influences by environmental and genetic factors.6 While it has been shown that the frequency of eye rubbing,8 atopy,9 excessive sunlight exposure, industrial toxins,10 and contact lens11 use are important environmental risk factors, there is evidence of the role of Wnt proteins and its signaling pathways in the pathogenesis of keratoconus, which highlight the effect of genetic factors.12-16
Genome-wide association studies (GWAS) identified single nucleotide polymorphisms (SNPs) in the RNAs of Wnt7B and Wnt10A in keratoconus affected humans.12,13 These studies have stated that variants in Wnt7B and Wnt10A in humans are asso-ciated with an increased risk of developing keratoco-nus. Wnt7B and Wnt10A play an important role in regulating the central corneal thickness.12,13 It may be hypothesized that the missense mutations in these proteins may have a lower affinity for their receptor, interfering with their effect of downstream signaling. More studies should be done to examine the exact pathological and biological mechanism these variants may exhibit. Additionally, transcriptomic and immu-nohistochemical analysis of keratoconus affected hu-man corneas found Wnt10A to be under expressed at the transcriptional and translational levels compared to healthy human corneas.14 The expression of Wn-t10A was found to be significantly (p<0.05) decreased in the Bowman’s layer. Wnt10A functions to upreg-ulate the expression of type I collagen (COL1A1), a major component of the corneal extracellular matrix, providing the epithelium tensile strength. Moreover,
most of the COL1A1 is localized to the Bowman’s layer. Thus, it has been hypothesized that when Wn-t10A levels are low, it can reduce the production of COL1A1 and compromise the biomedical strength of the cornea.14 The molecular pathway Wnt10A exhibits to upregulate COL1A1 remains unclear and more studies should be done to elucidate the mech-anism. A RNA sequence based study has shown dysregulation in Wnt signaling in keratoconus affected corneal epithelium by the downregula-tion of angiopoietin-like 7 (ANGPTL7), trans-forming growth factor beta receptor 3 (TFGBR3), and secreted frizzled-related protein 1 (SFRP1).15 ANGPTL7, a target gene of Wnt proteins, plays a role in maintaining corneal avascularity and provid-ing transparency. In healthy corneas, ANGPTL7 is highly expressed in keratocytes. However, there is uncertainty in the role of downregulation that this anti-angiogenic gene plays in the progression in keratoconus affected corneas. SFRP1 expression is reported to be reduced in the tears from keratoco-nus patients, while increased in keratoconus-affect-ed corneal epithelium. The SRP family proteins are reported to have tumor suppressive functions such as aiding in DNA repair, induction of apoptosis, detoxification, and transcriptional regulation. More-over, SFRP1 prevents the binding of the Wnt pro-tein to their transmembrane receptors (FZD), thus inhibiting signal transduction in the cell. TGFBR3 is reported to suppress Wnt signaling by binding to Wnt3A, which is responsible in regulating endothe-lial cell proliferation in the cornea.15
Another study reported DNA methylation changes encoding for the Wnt3 and Wnt5A proteins in keratoconus corneas.16 It was observed that both genes were hypermethylated. Although Wnt5A was transcriptionally downregulated, Wnt3 was remark-ably upregulated. This irregularity was explained by the fact that DNA methylation can affect alternative splicing and gene expression indirectly by the use different mechanisms.16
Aniridia-Related Keratopathy
Aniridia-Related Keratopathy (ARK) is thought to be a cause of insufficient number of corneal epithelial stem cells in the limbus. This deficiency hinders the ability to maintain the cor-nea clear and recover from irritation and injury. Therefore, this predisposes the cornea to become thickened, opaque, and excessively vascularized

Page 24 Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 CO
MM
ENTA
RY/R
EVIE
W
after childhood.17-19 This rare disorder is caused by mutations in PAX6, an essential gene in eye develop-ment.20
An in vitro ARK model of CRISPR/Cas9 engineered human keratocytes analysis revealed altered gene and protein expression of the Wnt pathway.21 It was shown that gene expression of the WNT5 protein was decreased with no difference in protein levels between healthy and PAX6 mutant keratocytes. Similarly, there were no differences in gene expression of β-catenin, a key nuclear effector of canonical Wnt signaling in the nucleus, between healthy keratocytes and PAX6 mutant keratocytes, but its proteins levels were decreased.21 In another study by the same researchers,20 naïve ARK cor-neas (corneal buttons from patients with advanced ARK submitted to penetrating keratoplasty for the first time) and transplanted corneas (from patients who were re-transplanted due to failure of a former transplant from a healthy donor) were utilized to analyze gene and protein expression involved in the Wnt pathway. In this study, the naïve and transplant-ed ARK patients, β-catenin was observed in epi-thelial cells, blood vessels, and in the subepithelial pannus. In contrast to the in vitro ARK model ker-atocytes21, the naïve and transplant ARK patients had increased amounts of Wnt5.20 Sloniecka et al. (2021) report that the differences may be attributed to environmental stimuli of chronic inflammation in ARK corneas, that were absent in the in vitro model. It was also stated that the absence of a proper basement membrane between the layers in the ARK corneas may influence the corneal epithelium stro-ma and Wnt pathway.20
In a similar study, PAX6 was overexpressed in a mouse cornea (Pax6 Tg) to alter corneal epithe-lial cells and observe changes in expression of Wnt signaling components compared to wild type cornea mice (WT).22 It was observed that the promoter of the Wnt inhibitory factor 1 (Wifi1) was upregulated sevenfold in Pax6 Tg versus WT. It was postulated that this change in expression may contribute to the observed abnormal phenotype in the Pax6 Tg corneas. Davis et al. (2011) suggested that Pax6 may play a role in suppressing the Wnt pathway via tran-scriptional upregulation of the Wif1 gene. To sup-port this notion, a microarray analysis of the Pax6 Tg corneas was conducted. Results from the analysis showed an increase in Wif1 mRNA levels, as well as those of a second Wnt inhibitor— SFRP2.22 Although PAX6 and Wnt7A show low expression in the corneal endothelium, they are known to be expressed significantly more in the corneal epithelium.23 A study created an in vi-
tro-cell-free limbal epithelium cell expansion and three dimensional corneal differentiation protocol to investigate the molecular events in maintenance and differentiation of limbal stem cells (LSC) into corneal epithelium.24 It was found that Wnt7a facilitates corneal epithelium differen-tiation with support of PAX6. In the absence of Wnt7a or PAX6, the LSC were differentiated into a skin-like epithe-lium, which is linked to other human corneal diseases like ARK. In this study, Ouyang et al. (2014) were unsuccessful inconverting transduced PAX6 skin epithelium stem cells into LSCs in vitro. However, when the transduced skin epithelial stem cells were transplanted into rabbit eyes with corneal injuries, the cells were able to differentiate into corneal epithelial cells and aid in healing the dam-aged corneal surface.24 This discovery suggested a critical interaction between Wnt7a and PAX6 in the maintenance and differentiation of corneal epithelial cell fate, that may aid future interventions and strategies in treating corneal diseases like ARK.
Wound Healting
Repair of a wounded cornea involves the remain-ing epithelial cells to provide prompt coverage and closure of the injured area.25 These epithelial cells exhibit prolifer-ation and migration in the process of wound healing with the aid of Wnt family proteins.26,27 A study using human corneal epithelial cells (CEC) demonstrated the impor-tance of Wnt7A in CEC proliferation, through its effects on Metalloproteinase 12 (MMP-12).27 During the process of wound healing, Wnt7A induces -catenin accumulation and activates Rac GTPase. Sequentially, Rac and -catenin work synergistically to induce the transcription of MMP-12. Lyu et al. (2005) also showed that the inhibition of MMP-12 delayed the process of wound healing induced by Wnt7A. Since Wnt7A and MMP-12 appear to contrib-ute to the corneal wound healing process, these proteins may be potential targets for therapy where there is diffi-culty in repairing the cornea. An additional study using human CEC demon-strated the importance of Wnt5A in CEC migration, another critical role in wound healing.28 In this study, Wnt5A was induced by brief stimulation of IL-1 through NF-B in human CECs, which led to cell migration. Sub-sequently, Wnt5A’s binding to FZD5 and Ro2 resulted in activation of Dvl and later binding between DAAM1 and Cdc42. Activated Cdc42 inhibited RhoA to allow parallel dephosphorylation and activation of slingshot 1, a protein phosphatase. This ultimately led to dephosphorylation and activation of cofilin, which resulted in enhanced cel-lular migration.28 Thus, the evidence of noncanonical

Page 25Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 COM
MEN
TARY/REVIEW
Wnt signaling enhanced cell migration may also provide an alternative therapeutic target where there are challeng-es in corneal healing. Previous studies have shown that transforming growth factor-alpha (TGF-α) plays a role in the corneal wound healing process.29,30 However, when TGF-α is over-expressed in human CEC, it may lead to endothelial ab-normality and disruption in ocular surface homeostasis.31 In a study using double-transgenic mice overexpressing TGF-α, peripheral anterior synechiae was associated with canonical Wnt signaling suppression and noncanonical Wnt signaling upregulation. It was noted that increased myosin light chain phosphorylation may activate nonca-nonical Wnt signaling.31 Thus, overexpression of TGF-α may be pathogenic due to alterations in Wnt signaling, preventing proper homeostasis and healing of CECs.
Conclusion
Research in Wnt signaling has appreciably advanced our knowledge about the many facets of Wnt pathways and roles they play in corneal diseases and wound healing. However, there are still questions that need to be addressed. One such question is the molecular mechanism Wnt proteins exhibit to upregulate other proteins and the molecular factors and switches for canonical vs. non-canonical Wnt signaling pathways. Distinguishing the different types of Wnt signaling in the cornea and obtaining the knowledge on the sequential molecular mechanisms of Wnt cascades in corneal diseases may provide new diagnostic and prognostic markers and therapeutic targets for developing novel strategies in disease treatment. A possible rational drug strategy could entail the use of miRNAs to target aberrant Wnt signaling, or utilizing stem cells to proliferate and self-renew proteins involved in the Wnt signaling cascade. With the aid of more studies, a hopeful future for patients with corneal diseases may lie ahead.
References1. Sridhar MS. Anatomy of cornea and ocular surface. Indian J Ophthal-mol. 2018;66(2):190-194. doi:10.4103/ijo.IJO_646_17
2. Nakatsu MN, Ding Z, Ng MY, Truong TT, Yu F, Deng SX. Wnt/β-caten-in signaling regulates proliferation of human cornea epithelial stem/pro-genitor cells. Invest Ophthalmol Vis Sci. 2011;52(7):4734-4741. Published 2011 Jul 1. doi:10.1167/iovs.10-6486
3. Komiya Y, Habas R. Wnt signal transduction pathways. Organogenesis. 2008;4(2):68-75. doi:10.4161/org.4.2.5851
4. Kobayashi Y, Hayashi R, Shibata S, Quantock AJ, Nishida K. Ocular surface ectoderm instigated by WNT inhibition and BMP4. Stem Cell Res. 2020 Jul;46:101868. doi: 10.1016/j.scr.2020.101868. Epub 2020 Jun 1. PMID: 32603880; PMCID: PMC7347012
5. Bi L, Lwigale P. Transcriptomic analysis of differential gene expression during chick periocular neural crest differentia-tion into corneal cells. Dev Dyn. 2019 Jul;248(7):583-602. doi: 10.1002/dvdy.43. Epub 2019 May 2. PMID: 31004457; PMCID: PMC6746171.
6. Asimellis G, Kaufman EJ. Keratoconus. [Updated 2021 Aug 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publish-ing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470435/
7. Hashemi, Hassan MD*; Heydarian, Samira PhD†; Hoosh-mand, Elham MSc‡; Saatchi, Mohammad PhD§; Yekta, Abbasali PhD¶; Aghamirsalim, Mohamadreza MD‖; Valadkhan, Mehr-naz M.Sc*; Mortazavi, Mehdi MD**; Hashemi, Alireza MD††; Khabazkhoob, Mehdi PhD‡‡ The Prevalence and Risk Factors for Keratoconus: A Systematic Review and Meta-Analysis, Cornea: February 2020 - Volume 39 - Issue 2 - p 263-270 doi: 10.1097/ICO.0000000000002150
8. McMonnies CW. Abnormal rubbing and keratecta8. sia. Eye Contact Lens. 2007;33:265–271.
9. Sharma N, Rao K, Maharana PK, et al. Ocular allergy and kera-toconus. Indian J Ophthalmol. 2013;61:407–409.
10. Gordon-Shaag A, Millodot M, Shneor E, et al. The genet-ic and environmental factors for keratoconus. Biomed Res Int. 2015;2015:795738.
11. Macsai MS, Varley GA, Krachmer JH. Development of keratoconus after contact lens wear. Patient characteristics. Arch Ophthalmol. 1990;108:534–538
12. Gao X, Nannini DR, Corrao K, Torres M, Chen YI, Fan BJ, Wiggs JL; International Glaucoma Genetics Consortium, Taylor KD, Gauderman WJ, Rotter JI, Varma R. Genome-wide associa-tion study identifies WNT7B as a novel locus for central corneal thickness in Latinos. Hum Mol Genet. 2016 Nov 15;25(22):5035-5045. doi: 10.1093/hmg/ddw319. PMID: 28171582; PMCID: PMC6078592.
13. Cuellar-Partida G, Springelkamp H, Lucas SE, Yazar S, Hewitt AW, Iglesias AI, Montgomery GW, Martin NG, Pennell CE, van Leeuwen EM, Verhoeven VJ, Hofman A, Uitterlinden AG, Ramdas WD, Wolfs RC, Vingerling JR, Brown MA, Mills RA, Craig JE, Klaver CC, van Duijn CM, Burdon KP, MacGregor S, Mackey DA. WNT10A exonic variant increases the risk of keratoconus by decreasing corneal thickness. Hum Mol Genet. 2015 Sep 1;24(17):5060-8. doi: 10.1093/hmg/ddv211. Epub 2015 Jun 5. PMID: 26049155.
14. Foster JW, Parikh RN, Wang J, Bower KS, Matthaei M, Chakra-varti S, Jun AS, Eberhart CG, Soiberman US. Transcriptomic and Immunohistochemical Analysis of Progressive Keratoconus Reveal Altered WNT10A in Epithelium and Bowman’s Layer. Invest Oph-thalmol Vis Sci. 2021 May 3;62(6):16. doi: 10.1167/iovs.62.6.16. PMID: 33988693; PMCID: PMC8132000.
15. Khaled ML, Bykhovskaya Y, Yablonski SER, et al. Differ-ential Expression of Coding and Long Noncoding RNAs in Keratoconus-Affected Corneas. Invest Ophthalmol Vis Sci. 2018;59(7):2717-2728. doi:10.1167/iovs.18-24267
16. Kabza M, Karolak JA, Rydzanicz M, Udziela M, Gasperowicz P, Ploski R, Szaflik JP, Gajecka M. Multiple Differentially Methyl-ated Regions Specific to Keratoconus Explain Known Keratoconus Linkage Loci. Invest Ophthalmol Vis Sci. 2019 Apr 1;60(5):1501-1509. doi: 10.1167/iovs.18-25916. PMID: 30994860.

Page 26 Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 CO
MM
ENTA
RY/R
EVIE
W
17. Ihnatko R, Eden U, Fagerholm P, Lagali N. Congenital An-iridia and the Ocular Surface. Ocul Surf. 2016 Apr;14(2):196-206. doi: 10.1016/j.jtos.2015.10.003. Epub 2015 Dec 29. PMID: 26738798.
18. Bausili MM, Alvarez de Toledo J, Barraquer RI, Michael R, Tresserra F, de la Paz MF. Histopathology Findings of Corne-al Buttons in Congenital Aniridia Patients. Ophthalmic Res. 2016;56(4):202-206. doi: 10.1159/000444930. Epub 2016 Apr 29. PMID: 27160090.
19. Auw-Haedrich C, Agrawal M, Gabbert HE, Meyer P, Arnold N, Reinhard T. Immunohistochemical expression of epithelial cell markers in corneas with congenital aniridia and ocular cic-atrizing pemphigoid. Acta Ophthalmol. 2011 Feb;89(1):47-53. doi: 10.1111/j.1755-3768.2009.01603.x. PMID: 19558573.
20. Vicente A, Byström B, Lindström M, Stenevi U, Pedrosa Domellöf F. Aniridia-related keratopathy: Structural chang-es in naïve and transplanted corneal buttons. PLoS One. 2018;13(6):e0198822. Published 2018 Jun 11. doi:10.1371/jour-nal.pone.0198822
21. Sloniecka, M., Vicente, A., Byström, B., & Domellöf, F.P. (2021). Cell signaling pathways in human mutant PAX6 corneal cells: An in vitro model for aniridia-related keratopathy. bioRxiv 2021.03.19.436143; doi: 10.1101/2021.03.19.436143
22. Davis J, Piatigorsky J. Overexpression of Pax6 in mouse cor-nea directly alters corneal epithelial cells: changes in immune function, vascularization, and differentiation. Invest Ophthal-mol Vis Sci. 2011;52(7):4158-4168. Published 2011 Jun 13. doi:10.1167/iovs.10-6726
23. Tokuda, Y., Okumura, N., Komori, Y. et al. Transcriptome dataset of human corneal endothelium based on ribosomal RNA-depleted RNA-Seq data. Sci Data 7, 407 (2020). https://doi.org/10.1038/s41597-020-00754-1
24. Ouyang, H., Xue, Y., Lin, Y. et al. WNT7A and PAX6 define corneal epithelium homeostasis and pathogenesis. Nature 511, 358–361 (2014). https://doi.org/10.1038/nature13465
25. Ljubimov AV, Saghizadeh M. Progress in corneal wound healing. Prog Retin Eye Res. 2015;49:17-45. doi:10.1016/j.pret-eyeres.2015.07.002
26. Lyu J, Joo CK. Expression of Wnt and MMP in epithelial cells during corneal wound healing. Cornea. 2006 Dec;25(10 Suppl 1):S24-8. doi: 10.1097/01.ico.0000247209.01262.4e. PMID: 17001188.
27. Lyu J, Joo CK. Wnt-7a up-regulates matrix metalloprotein-ase-12 expression and promotes cell proliferation in corneal epithelial cells during wound healing. J Biol Chem. 2005 Jun 3;280(22):21653-60. doi: 10.1074/jbc.M500374200. Epub 2005 Mar 31. PMID: 15802269.
28. Lee JG, Heur M. Interleukin-1β-induced Wnt5a enhances human corneal endothelial cell migration through regulation of Cdc42 and RhoA. Mol Cell Biol. 2014;34(18):3535-3545. doi:10.1128/MCB.01572-13
29. Schultz G, Chegini N, Grant M, Khaw P, MacKay S. Effects of growth factors on corneal wound healing. Acta Ophthal-mol Suppl. 1992;(202):60-6. doi: 10.1111/j.1755-3768.1992.tb02170.x. PMID: 1322013.
30. McClintock JL, Ceresa BP. Transforming growth factor-{al-
pha} enhances corneal epithelial cell migration by promoting EGFR recycling. Invest Ophthalmol Vis Sci. 2010;51(7):3455-3461. doi:10.1167/iovs.09-4386
31. Yuan Y, Yeh LK, Liu H, Yamanaka O, Hardie WD, Kao WW, Liu CY. Targeted overexpression of TGF-α in the cor-neal epithelium of adult transgenic mice induces changes in anterior segment morphology and activates noncanonical Wnt signaling. Invest Ophthalmol Vis Sci. 2013 Mar 11;54(3):1829-37. doi: 10.1167/iovs.12-11477. PMID: 23412089; PMCID: PMC3626521.CO
MM
ENTA
RY/R
EVIE
W

Page 27Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 COM
MEN
TARY/REVIEW
Individualized Approach for Counseling Patients Faces with the Decision of Transferring a Low-Level Mosaic EmbryoTohar Kochav Lev1, Bei Sun1, Ron Shemtov 1, Talia Ditkoff 1, Tomer Singer, M.D. 2
1 Sackler School of Medicine, Tel Aviv University, Tel Aviv2 Associate Professor Zucker School of Medicine, Hempstead, New York
Introduction and Background
Preimplantation genetic testing for aneuploidy (PGT-A) is used to screen IVF embryos for chromosomal abnormalities prior to transferring the embryo. It involves taking a biopsy of approximately 5 cells from the blastocyst.
PGT-A results include euploid (all normal cells), aneuploid (all abnormal cells), or (should this be and instead of or?) mosaic (a mix of normal and abnormal cells) cells. A mosaic embryo is defined as having two or more genetically different cells.1 Mosa-ic embryos can be further subdivided into high-level or low-level mosaicism.
There is variability in protocols regarding classification and transferring of mosaic embryos. Different clinics’ genetic laboratories across the United States have various (just because you already used different in the sentence) thresholds for determining a fetus as aneuploid, euploid, or mosaic, ranging from 15-30%. The most common threshold used is euploidy being <20% abnormal cells (36.3%) and aneuploidy being >80% abnormal cells (46.2%).2 Mosaic embryos are defined as being between these two thresholds, with low-level mosaicism generally defined as 20-40% and high-level mosaicism defined as 40-80%. Many clinics (42.9%) have transferred, and most clinics (62.6%) would be willing to transfer a mosaic embryo.2 To further highlight the uncertainty in practices of mosaic embryos, it was found that nearly 40% of clinics were unsure of the thresholds they apply for mosaic embryos and 25% of clinics did not have a threshold at all.2 The classification/threshold percentages in this paragraph are great, I’m just wondering if it would be even better if you showed these percentages as a figure (i.e. a pie chart, bar graph, or table). There are a lot of numbers, and a figure could paint a picture of the data in the reader’s head.
In the process of PGT-A, the biopsied cells are taken from the trophectoderm, the outer layer of the blastocyst. The trophectoderm evolves into the placenta and membranes, whereas the inner cell mass becomes the actual embryo. Given the source of the cells tested by PGT-A, the results may indicate evolving confined placental mosaicism (CPM), mosaicism in both the placenta and the fetus, mosaicism in the placenta with a fully aneuploid fetus, or aneuploid cell elimination as the embryo further develops.
The possible outcomes for a child born from a mosaic embryo are (a) a child with an apparently normal karyotype without birth defects or developmental delays, (b) a child with an apparently normal karyotype with birth defects or developmental delays, or (c) a child with mosaic or full aneuploidy on karyotype. Notably, the degree of mosaicism in the future child cannot be estimated solely by PGT-A results.

Page 28 Sackler Journal of Medicine | Volume 5 | Issue 2 | 2021 CO
MM
ENTA
RY/R
EVIE
W
The range of outcome possibilities raises several ethical dilemmas regarding the transferring of a mosaic embryo. Through this review, a series of cases will be presented to introduce the complexity of such decisions and weigh the risks and benefits of transferring a low-mosaic embryo.
Case #1:
The patient is a 41-year-old woman who first presented to Shady Grove Fertility in 2019. She had previously completed IVF with ICSI (Intracytoplasmic sperm injection) and PGT-A. The patient has a total of eight frozen embryos, six of which were found to be aneuploid, one was found to be a high-level mosaic, and one was found to be a low-level mosaic. The patient now requests to move forward with the transfer of the low-level mosaic embryo due to financial constraints of undergoing an additional IVF cycle.
Case #2:
The patient is a 45-year-old woman who initially presented to Shady Grove Fertility in 2015 for egg freezing. At that time, the patient was single and her AMH (Anti-Müllerian hormone) was 3.3 ng/ml. A few years following the ovum pickup, she met her partner. At the age of 41, the patient returned to the clinic with her partner to thaw her oocytes and perform ICSI. However, due to personal ethical preferences, the patient and her partner elected to thaw only some of the oocytes. Of the thawed embryos, all of them were determined to be abnormal. Following this result, the remaining oocytes were thawed. All of the remaining embryos were also determined to be abnormal with the exception of one embryo that is a low-level mosaic. At this time, the patient has a low ovarian reserve with undetectable AMH levels. The patient was counseled and educated regarding the high risk of non-implantation and miscarriage rates, and would like to move forward with the transfer of the low-level mosaic embryo.
Discussion and Conclusion
The decision of transferring a low-level mosaic embryo involves three parties: the physi-cian, the patient/couple, and the embryo. Risks and benefits to each of these parties must be considered. Patient autonomy is weighed against the procedural risks, the emotional trauma of suf-fering a miscarriage or non-implantation, and the outcome of the future child. The outcome of the future child may have implications on the patient/couple, as well as on the child itself.
While the American Society for Repro-ductive Medicine (ASRM) does not endorse or recommend PGT-A for all IVF cases, it does acknowledge its vital role in detecting mosaicism. Therefore, the ASRM sets clear standards for cli-nicians to follow in regards to pretest and posttest counseling. The ASRM even provides key points to follow when having these challenging discus-sions with patients.3 The American College of Obstetricians and Gynecologists (ACOG) is more straightforward in their endorsement and recom-mendation of traditional diagnostic testing and screening for aneuploidy after PGT-A. They do, however, acknowledge the frequency of false-posi-tive and false-negative results, especially in regards to mosaicism, due to the nature of the tests.4 The ACOG recognizes that further research is neces-sary to better understand the clinical significance of mosaicism.
Since the detection of mosaic embryos is a relatively new phenomenon, data is limited regarding the outcomes of these embryos. Howev-er, it is believed that there are increased risks for failed implantation, miscarriage, and adverse out-comes. Mosaic embryo transfer is associated with a lower live birth rate, as compared to euploid embryo transfer.5 Studies have suggested a 37% ongoing implantation rate and 25% miscarriage rate after transfer of a mosaic embryo compared to a 77% ongoing implantation rate and 7% mis-carriage rate after transfer of a euploid embryo.6 Furthermore, a meta-analysis found that mosaic embryo transfers had significantly lower preg-nancy rates than euploid embryos (40.1% versus 59.0%), a lower live birth rate than euploid embry-os (27.1% versus 47.0%), and higher miscarriage rate than euploid embryos (33.3% versus 20.5%).7

Page 29Sackler Journal of Medicine | Volume 5 | Issue 2 | 2021 COM
MEN
TARY/REVIEW
lower degree of mosaicism (20–40% compared to 40-80%) was associated with higher ongoing implantation rates (50% and 27%).6
Following the transfer of a mosaic em-bryo, multiple cases of live births with normal chromosomes have been reported.8 In such cases, amniocentesis results have suggested that mosa-icism may be self-corrected during development.8 This could be due to an inaccuracy of the initial embryo biopsy.(I am a little confused here - is the mosaicism self-correcting, or was the initial biopsy incorrectly performed and the embryo was never actually mosaic) While there have been reports of apparently healthy babies born with normal karyotypes on peripheral blood after the transfer of a mosaic embryo, long-term follow-up data for these cases are lacking. There has been one published case of a healthy child born with true fetal mosaicism with peripheral blood show-ing 2% mosaic monosomy, the same chromosomal abnormality as was found on PGT-A.9
In the PGT-A procedure, a relatively small number of cells are biopsied, thus it remains possible for some cases of mosaicism to be eluded. Therefore, potentially mosaic embryos that are classified as euploid may be unknowingly trans-ferred and undergo the same risk as transferring a mosaic embryo. Only about 60-70% of apparently euploid embryos implant.10 This may suggest that some embryos classified as normal actually fail to implant due to abnormal cells that were not captured by PGT-A, or embryos harboring unde-tected mosaicism.
A valid alternative is to offer patients/cou-ples in this situation the option to pursue an ad-ditional cycle of IVF with ICSI and PGT-A in an attempt to obtain a euploid embryo. If this addi-tional cycle is not successful in obtaining a euploid embryo, the option of transferring the mosaic embryo would still remain a possibility. However, as seen in the cases presented, this option is not always viable due to financial constraints or low ovarian reserve.
The cases suggest that an individualized approach should be taken for each patient faced with the decision of transferring a low-mosaic embryo. Each patient should be evaluated not only for personal preferences, social factors, and emotional out-
comes, but also viability of alternative options. It is proposed that all parties involved should weigh the risks and benefits with the outcome of the future child in mind.
References1. Malan V, Vekemans M, Turleau C. Chimera and other fertilization errors. Clin Genet. 2006 Nov;70(5):363-73. doi: 10.1111/j.1399-0004.2006.00689.x. PMID: 17026615.
2. Kim TG, Neblett MF, Shandley LM, Omurtag K, Hipp HS, Kawwass JF. National mosaic embryo transfer practices: a survey. Am J Obstet Gynecol. 2018 Dec;219(6):602.e1-602.e7. doi: 10.1016/j.ajog.2018.09.030. Epub 2018 Sep 29. PMID: 30278174.
3. Practice Committee and Genetic Counseling Professional Group (GCPG) of the American Society for Reproductive Medicine. Electronic address: [email protected]. Clinical man-agement of mosaic results from preimplantation genetic testing for aneuploidy (PGT-A) of blastocysts: a committee opinion. Fertil Steril. 2020 Aug;114(2):246-254. doi: 10.1016/j.fertn-stert.2020.05.014. PMID: 32741460.
4. Preimplantation Genetic Testing: ACOG Committee Opin-ion, Number 799. Obstet Gynecol. 2020 Mar;135(3):e133-e137. doi: 10.1097/AOG.0000000000003714. PMID: 32080053.
5. Zhang L, Wei D, Zhu Y, Gao Y, Yan J, Chen ZJ. Rates of live birth after mosaic embryo transfer compared with euploid embryo transfer. J Assist Reprod Genet. 2019 Jan;36(1):165-172. doi: 10.1007/s10815-018-1322-2. Epub 2018 Sep 24. PMID: 30246223; PMCID: PMC6338591.
6. Abhari S, Kawwass JF. Pregnancy and Neonatal Outcomes after Transfer of Mosaic Embryos: A Review. J Clin Med. 2021 Mar 27;10(7):1369. doi: 10.3390/jcm10071369. PMID: 33801687; PMCID: PMC8037456.
7. Zhang YX, Chen JJ, Nabu S, Yeung QSY, Li Y, Tan JH, Suksal-ak W, Chanchamroen S, Quangkananurug W, Wong PS, Chung JPW, Choy KW. The Pregnancy Outcome of Mosaic Embryo Transfer: A Prospective Multicenter Study and Meta-Anal-ysis. Genes (Basel). 2020 Aug 21;11(9):973. doi: 10.3390/genes11090973. PMID: 32825792; PMCID: PMC7565393.
8. Liu YL, Yu TN, Chen CH, Wang PH, Chen CH, Tzeng CR. Healthy live births after mosaic blastocyst transfers with the use of next-generation sequencing. Taiwan J Obstet Gynecol. 2019 Nov;58(6):872-876. doi: 10.1016/j.tjog.2019.07.032. PMID: 31759546.
9. Kahraman S, Cetinkaya M, Yuksel B, Yesil M, Cetinkaya CP. The birth of a baby with mosaicism resulting from a known mosaic embryo transfer: a case report. Human Reproduction. 2020 Mar;35(3):727-733. doi: 10.1093/humrep/dez309.
10. Lee E, Illingworth P, Wilton L, Chambers GM. The clinical effectiveness of preimplantation genetic diagnosis for aneuploi-dy in all 24 chromosomes (PGD-A): systematic review. Human Reproduction. 2015 Feb;30(2):473-48. doi: 10.1093/humrep/deu303.

Page 30 Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021
The First Half of The Preclinical Education at Sackler School of MedicineBy Noah Igra and Yuval Raviv
Introduction
This upcoming spring marks the first time the U.S. Medical Licensing Examination (USMLE) Step 1 exam will be pass/fail. Performance on the Step 1 exam was a metric whose objectivity was necessary for international medical graduates (IMGs) in their application for residency. Its exclusion would ultimately result in a shift of priority towards other aspects of their medical education such as Step 2 Clinical Skills performance, research, clerkship evaluations, etc1. While this change is praised for addressing the exam’s negative impact on student mental health, the implication for IMGs remains unclear2. As students at Sackler School of Medicine (SSOM), our first year of medical school was very similar to that experienced by the upperclassmen, suggesting that we will be given a similar preclinical education despite the upcoming differences in our own residency applications.
To reflect on our medical education, we collected data concerning scheduled class time during our first year at SSOM (M1). Hours were recorded from Tel Aviv University’s course management website, Moodle, as well as the Google Calendar managed by the SSOM administration. Of the five M1 study blocks (i.e. Block 1, Block 2, etc.), the first two were collected from the current M1 schedule (Class of 2025). Case-based learning (CBL) usually includes a lecture, a small-group application activity, and a reflection on that activity as a class. When available, we used the Moodle activity time limit to derive the CBL length proper. Unfortunately, the data for Systems Histology (Block 3) was not collected.
Lectures in Medical School
During the first year of medical school, M1 students spent a total of 554.45 hours in class. Out of all classwork hours, 69% were spent in lecture, 14% in CBL, 12% in lab, and 5% in Art and Science of Medicine (ASM) (Table 1). The American educator Hamilton Holt described lecturing in 1931 as “that mysterious process by means of which the contents of the professor’s notebooks are transferred by means of the fountain pen to the pages of the student’s note-books without passing through the minds of either3.” Research suggests that our brain gets overwhelmed by the amount of content covered in traditional medical lectures, and that the information learned is only superficially understood4. This is explained by the way both working memory and cognitive interference may influence learner engagement, with studies showing that in traditional lectures the attention span wanes after 15-20 minutes and that the retention rate is estimated to be at a 5%3. Despite these deficits, all classes during M1 featured lecture as the main component of their coursework, with a median duration of 2 hours (Range: 30 minutes – 5 hours).
Table 1. Hours spent in lecture, CBL, and lab across M1
courses. Total hours for each block include ASM and Pain
hours, along with the block-specific classes.

Page 31Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021
While it’s unclear whether traditional in-person lectures improve student performance, most studies focus on compulsory education (i.e. grades 1-12) and do not reflect graduate medical education (GME) 5-7. One study looking at under-graduate education found that attending lectures only increased exam performance for first-year students, and that the only predictor of academ-ic success in later years was grade point average (GPA)8. This suggests that experienced learners, like those in GME programs, may not necessarily benefit from in-person lectures. We also observe that some periods of study appear to have more lecture hours earlier in the Block. On the other hand, less weekly lecture hours were found with simultaneous rises in hours for labs as well as CBLs (Figure 1: End of Blocks 1,2,4,5; lab spike in Block 3). These long and fre-quent lectures often include clinical correlates to the theoretical content covered. Without the space necessary to properly digest this foundational information, the spikes in lecture volume can be overwhelming9. Focusing on purely foundational material may result in shorter lectures, but those neither depend on an instructor’s expertise nor do they merit the lecture time spent learning them. If the goal is to utilize the instructor’s experience to the benefit of our education, why do our grades revolve around the theoretical education evalu-ated in USMLE-style exams rather than exercises designed by our instructors? With the pass/fail na-ture of USMLE Step 1, our lectures and examina-tions could lean towards the instructor’s clinical expertise and away from theoretical exam-focused content.
Case-Based Learning
The genesis of present-day medical ed-ucation can be traced back to the middle of the 19th century. By the 1870s, an enormous increase in medical information shocked educators and
overwhelmed physicians10. A critical consequence of this boom was the realization that knowledge is fluid and evolving rather than a fixed property. Thus, the aim of medical education had to shift away from merely absorbing facts through rote memorization towards instilling proper tech-niques of digesting medical information. In 1910, Abraham Flexner released his landmark report, where he rejected the use of lectures in GME, campaigning for an active approach that instilled a deep understanding of the scientific method in future11.At SSOM, M1 students apply their education in CBL exercises. First introduced by James Lorrain Smith in 1912, CBL is an active approach aimed at preparing students for clinical practice with authentic clinical cases12. CBLs link theory to practice and are shown to be an effective means of learning12. However, adopting a less lecture-fo-cused and more problem-solving teaching method has little potential for success without concern for how the methods are applied6. We, the au-thors, feel that CBLs are currently not the effective means of learning that they could be, and since we spend 14% of our M1 curriculum on CBLs, a greater effort should be made to capitalize on them.
Grading and Performance
Throughout this discussion, the matter of grading both within M1 as well as for the Step 1 exam has been brought forward. The objectivity of a standardized exam allowed Step 1 to become a priority in residency applications, and thus impact the structure and focus of preclinical education. The shift to a binary metric echoes the intent to focus on more clinically oriented criteria in future application rounds13. While we do not question the choice of grading entirely, we question the function of grades as they are used in our edu-cation. The internal component can be viewed as a buffer to retain our GPA when faced with seemingly more relevant National Board exams (NBMEs), legitimizing the extensive distribution of grades in online assignments and CBLs. If our grades on NBMEs correspond to future readiness to perform well on an exam that no longer neces-sitates such performance, what is their merit with-in our overall grade? If our performance on the NBME does not impact our final grade, would M1

Page 32 Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021
performance rely more heavily on the knowledge imparted during lectures? If preclinical education is no longer prioritized in the residency application, is there any point in prioritizing our academic perfor-mance during these years? If the answer to either one of these questions suggests that without grades we will not be incentivized to study, then maybe we need to reevaluate both the priorities of the SSOM preclinical education, as well as our own as future physicians.
Conclusion
In this piece, we discussed the scope of lectures and CBLs in the SSOM M1 preclinical education. The impulse to expose students at our level of education to more information in lon-ger lectures falsely assumes that they will be able to meaningfully understand and retain said the material3. We call upon our readers to consider the points raised and urge you to take a more active role in exploring alternatives to the current design. Moving forward, implementation is key. While we are encouraged to evaluate our CBLs and courses, things are not changing fast enough. If the status quo remains, students will continue struggling to balance outdated teaching methods with residency director expectations that have already changed. An increase in transparency on the structuring and causality of future curricula would benefit both the administration as well as the students.
References
1. Andolsek KM. Improving the Medical Student Performance Evaluation to Facilitate Resident Selection. Academic Medicine. 2016;91(11). doi:10.1097/ACM.0000000000001386
2. Al-Akchar M, Salih M, Fanari Z. USMLE step 1 pass/fail: the impact on international medical graduates. Avicenna Journal of Medicine. 2021;11(01). doi:10.4103/ajm.ajm_154_20
3. Cooper AZ, Richards JB. Lectures for Adult Learners: Breaking Old Habits in Graduate Medical Education. The American Journal of Medicine. 2017;130(3). doi:10.1016/j.amjmed.2016.11.009
4. Liu B. The United States Medical Licensing Examination Step 1 Is Changing—US Medical Curricula Should Too. JMIR Medical Education. 2020;6(2). doi:10.2196/20182
5. Rivkin SG, Schiman JC. Instruction time, Classroom Quality, and Academic Achievement. The Economic Journal. 2015;125(588). doi:10.1111/ecoj.12315
6. Schwerdt G, Wuppermann AC. Is traditional teaching really all that bad? A within-student between-subject approach. Economics of Education Review. 2011;30(2). doi:10.1016/j.econedurev.2010.11.005
7. van Klaveren C. Lecturing style teaching and student performance. Economics of Education Review. 2011;30(4). doi:10.1016/j.econedurev.2010.08.007
8. Nordmann E, Calder C, Bishop P, Irwin A, Comber D. Turn up, tune in, don’t drop out: the relationship between lecture attendance, use of lecture recordings, and achievement at different levels of study. Higher Education. 2019;77(6). doi:10.1007/s10734-018-0320-8
9. Maddox H, Hoole E. Performance Decrement in The Lecture. Educational Review. 1975;28:1 17-30. doi:10.1080/0013191750280102
10. Ludmerer KM. Abraham Flexner and Medical Education. Perspectives in Biology and Medicine. 2011;54(1). doi:10.1353/pbm.2011.0009
11. Flexner A. Medical Education in the United States and Canada.; 1910.
12. Thistlethwaite JE, Davies D, Ekeocha S, et al. The effectiveness of case-based learning in health professional education. A BEME systematic review: BEME Guide No. 23. Medical Teacher. 2012;34(6). doi:10.3109/0142159X.2012.680939
13. Naqvi S, Levi D, Colaco R. USMLE Step 1 changes to Pass/Fail scores: What does it really mean for IMGs? https://www.amboss.com/int/usmle/img/knowledge/step-1-pass-fail. Accessed November 7th, 2021.

Page 33Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 CA
SE REPORTShould there be a strict age cutoff for
intended parents through gestational surrogacy? A Case ReportBei Sun, Tohar Kochav Lev, Liron Barel, Tomer Singer
Background
Gestational surrogacy is defined by a process in which intended parents (IPs) arrange with a woman to carry and deliver a genetically unrelated child using assisted reproductive technology (ART). It offers a fertility alternative for individuals with un-derlying medical conditions that would increase the complication risk in potential pregnancies. Multiple failed IVF cycles or repetitive pregnancy losses, and individuals without a functional uterus, are typically at increased risk.1 As of 2016, 85% of the ART clin-ics support gestational surrogacy, as reported by the Centers for Disease Control and Prevention.2
As the prevalence of gestational surrogacy con-tinues to grow in the United States and worldwide, it is important to examine the current guidelines and their applicability toward ethical, medical, psycho-social, and legal complexities.
Within the United States, there are significant vari-ations in states’ laws on the legality of gestational surrogacy.3 While more than 20 states allow and support gestational surrogacy contracts, some states are less supportive. For example, New York and Michigan historically are least supportive of gesta-tional surrogacy, do not recognize surrogacy con-tracts, and criminally penalize compensation paid to gestational carriers (GC).4,5 Additionally, the legal landscape surrounding gestational surrogacy chang-es frequently within each state. There is a lack of both formal legal guidance and regulatory agencies that help IPs and GCs navigate the process, which inevitably leads to a significant variation in practice.
The requirements and screening process for IP’s is another controversial aspect of the GC debate. Both American Society for Reproductive Medicine (ASRM) and American College of Obstetrics and Gynecologists (ACOG) have outlined recommenda
tions for screening IPs—advocating for a thor-ough medical and psychosocial evaluation as the core of this screening process.1,6,7 However, there are no regulations enforcing these recommenda-tions, nor are there data on compliance. While most practices institute a thorough medical and psychosocial evaluation of IPs, they often imple-ment additional criteria with considerations for optimal child outcomes. These criteria, specific to the practice, are often controversial. Age eli-gibility for IPs is an example of such a criterion. While implemented with good intentions, these can potentially deprive otherwise suitable IP candidates of a lifetime opportunity to become parents. We present a case here to illustrate the problematic nature of practice-specific criteria for IPs and call for a patient-centered approach to the screening process.

Page 34 Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 C
ASE
REP
ORT
Case Presentation
A 52-year-old woman, G1P0010, diagnosed with advanced maternal age, diminished ovarian reserve and severe uterine factor infertility, has been trying to conceive with her husband for eight years. The couple has recently matched with a GC and requested an embryo transfer. They successfully completed and passed the medical and psychosocial evaluations. The request to proceed was denied due to the age cutoff for IPs of 51 implemented at the practice. In 2014, the couple underwent one cycle of autologous in vitro fertilization (IVF). Eight oocytes were retrieved, six fertilized, followed by an unsuc-cessful fresh embryo transfer. In 2018, an oocyte donation IVF cycle was performed. More than thirty oocytes were retrieved from the donor and fertilized in vitro with the husband’s sperm. Ten embryos were frozen among which some completed preim-plantation genetic screening (PGS). One elective embryo transfer was performed and was unsuccess-ful. In 2019, the patient’s last embryo transfer was performed and was again unsuccessful. The couple began searching for a GC thereafter. The process was delayed due to the COVID pandemic.
Discussion and Conclusion
Research suggests there is a lack of published data on IPs who build families through gestational surrogacy. Current IP screening process is largely derived from the ASRM and ACOG recommen-dations. Current ASRM recommendation dis-courages women over 55 years of age from using donor oocytes or embryos due to the concern for adequate psychosocial support for raising a child to adulthood. ASRM and ACOG recommendations, however, do not suggest implementing age cutoffs to screen out potential IPs. There are also very few publications on parenting issues faced by women of advanced reproductive age. In fact, the limited data highlights an advantage of greater financial and emotional stability offered by older parents.8 Furthermore, the concern that IPs aged 50 or older raising a child may lose the emotional and physi-cal capacity to care for the child before they reach adulthood, should be addressed. Lastly, arrange-ments with appointed guardians who will take care of the child in the case of parental decease should be discussed.
References
1. Family Building Through Gestational Surro-gacy | ACOG [Internet]. [cited 2021 Jun 17];Avail-able from: https://www.acog.org/clinical/clini-cal-guidance/committee-opinion/articles/2016/03/family-building-through-gestational-surrogacy
2. Department of Health U, Services Centers for Disease Control H. 2016 Assisted Reproductive Technology National Summary Report [Internet]. 2016 [cited 2021 May 7]. Available from: https://www.cdc.gov/art/reports/
3. Swanson K, Ayala NK, Barnes RB, Desai N, Miller M, Yee LM. Understanding gestational surrogacy in the United States: a primer for obste-tricians and gynecologists. Am J Obstet Gynecol 2020;222(4):330–7.
4. New York Domestic Relations - Article 8 - § 122 Public policy. :: 2014 New York Laws :: US Codes and Statutes :: US Law :: Justia [Internet]. [cited 2021 Jun 18];Available from: https://law.justia.com/codes/new-york/2014/dom/article-8/122/
5. Michigan Legislature - Section 722.851 [Internet]. [cited 2021 Jun 18];Available from: http://www.legislature.mi.gov/(S(c0fduaafwvan4uyu4aver-jkg))/mileg.aspx?page=getObject&objectName=m-cl-722-851
6. Pfeifer S, Butts S, Fossum G, Gracia C, La Barbera A, Mersereau J, et al. Recommendations for practices utilizing gestational carriers: a committee opinion. Fertil Steril 2017;107(2):e3–10.
7. Daar J, Benward J, Collins L, Davis J, Fran-cis L, Gates E, et al. Oocyte or embryo donation to women of advanced reproductive age: an Ethics Committee opinion. Fertil Steril [Internet] 2016 [cit-ed 2021 Jun 17];106(5):e3–7. Available from: https://pubmed.ncbi.nlm.nih.gov/27450186/
8. Steiner AZ, Paulson RJ. O-7. Fertil Steril [In-ternet] 2006 [cited 2021 Jun 18];85(85):S8. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0015028206002949

Page 35Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021
Can stress induced pathways regulate glycogen synthase kinase 3 beta (GSK3β) localization and thus cell growth?Noa Mecica1,2, Costin Antonescu2 1 Sackler School of Medicine, Tel Aviv University, Tel Aviv2 Ryerson University, Toronto, Canada
Abstract
Glycogen synthase kinase 3β (GSK3β) phosphorylates and regulates numerous substrates, and is involved in integral cellular processes such as cell metabolism, growth, and proliferation. Dysregulation of these cellular processes is often associated with the uncontrolled cell growth and proliferation observed in cancer, making GSK3β a potential therapeutic target. GSK3β’s numerous substrates and constitutive activation raises the question of how this enzyme acts with any control or specificity and suggests the presence of numerous
Learning Points
» GSK3β is an enzyme involved in integral cellular processes such as cell metabolism, growth, and proliferation.
» GSK3β is associated with uncon-trolled cell growth seen in cancer making it a therapeutic target.
» The p38 MAPK signaling pathway is responsible for responding to cell stress.
» p38 MAPK pathway interacts with GSK3β under stressful conditions to increase GSK3β nuclear local-ization, promote apoptosis, and thus potentially decrease uncon-trolled cell growth seen in cancer.
regulatory mechanisms in place in order to coordinate its substrate-specific activity. Studies suggest that GSK3β activity may be regulated through control of its cellular location, thus controlling GSK3β’s access to specific substrates such as oncogenes. Here, by treating retinal pigment epithelium (RPE) cells with external stress stimuli, hydrogen peroxide, and sodium arsenite, experimental results suggest that activation of cellular stress pathways in response to oxidative stress increases GSK3β nuclear localization compared to control conditions. In order to determine the stress response pathway responsible for regulating GSK3β nucleocytoplasmic localization, the p38 mitogen activated protein kinase pathway (p38 MAPK) was inhibited using compound SB 203580. Inhibition of p38 MAPK in conjunction with hydrogen peroxide and sodium arsenite stress treatments resulted in decreased nuclear localization of GSK3β. These findings suggest that nucleocytoplasmic localization of GSK3β, and thereby, control of its cellular activity can potentially be regulated through interactions between p38 MAPK and GSK3β, such that under stressful conditions GSK3β is directed to the nucleus. Nuclear localization of GSK3β may contribute to novel therapies targeting GSK3β for the treatment of cancer cell growth and survival.
ORIG
INA
L RESEARCH

Page 36 Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 O
RIG
INA
L RE
SEA
RCH
Introduction
Glycogen synthase kinase 3 (GSK3β) is a serine/threonine protein kinase that has been impli-cated in the control of numerous cellular processes such as proliferation, differentiation, metabolism, and apoptosis.1 - 4 Dysregulation of GSK3β and its associated pathways have been linked to the development of diseases such as diabetes/insulin resistance, Alzheimer’s disease, and cancer.5 GSK3β is a kinase of interest as it has the unusual character-istics of phosphorylating over 100 substrates. Also, of particular importance, GSK3β is one of the few kinases that is constitutively active in its basal state.6 This demonstrates its potentially broad and signifi-cant control of cell physiology and function, which need to be tightly regulated. GSK3β’s high substrate number raises the question of how such a kinase acts with any specificity or control, and suggests the presence of numerous regulatory mechanisms in place in order to coordinate its substrate-specific activity. Here, we explore a potential GSK3β regu-latory signaling pathway, the p38 mitogen activated protein kinase (MAPK) pathway, which is activated in response to stress to ensure cell survival and can contribute to the possibility of targeting GSK3β therapeutically.
Although GSK3β has been considered primarily a cytosolic protein, its presence is also seen in several subcellular compartments, where its concentration and activation can be regulated by various signaling pathways.7 GSK3β can be local-ized to the mitochondria and nucleus. Mitochon-drial GSK3β is often a result of apoptotic conditions such as oxidative stress and heat shock.8 Similarly, nuclear GSK3β levels rapidly increase in response to apoptotic stimuli, as well as replicative senescence in fibroblasts, cancer cells 9, 10, and loss of phosphati-dylinositol 3-kinase (PI3K)-Akt signaling in embry-onic stem cells 11. Gaining a deeper understanding of the mechanisms and pathways leading to GSK3β endomembrane localization may provide significant information about its activity and thus contribution to cell physiology and function. When present in the nucleus, GSK3β has been shown to possess apop-totic properties, in contrast to the cytosol where it has been shown to be anti- apoptotic and promote cell survival.12. Among the numerous substrates targeted by GSK3β, many are transcription factors mainly located in the nucleus, such as oncogenes c-myc and snail. Regulation of c-myc is critical, as
dysregulation of c-myc has been connected to the progression of many cancers making it one of the most potent oncogenes. 13 GSK3β acts as a c-myc regulator through phosphorylation, resulting in the consequent ubiquitination, and degradation of the transcription factor. Thus, when GSK3β is located in the nucleus it has the potential to phosphorylate and destroy more of this oncogene.14 Understanding the poorly defined mecha-nisms that regulate GSK3β nucleocytoplasmic local-ization, and what drives GSK3β activity to nuclear substrates, can potentially lead to novel therapeutic targets in disease treatment. In response to chemical and physical changes in the cell’s environment, cells alter many cellular processing, such as proliferation, metabolism and survival to maintain homeostasis.15 These environmental stressors and changes may include altered concentrations of nutrients, growth factors, cytokines, and exposure to damaging agents, which put the cell in danger. One of the main ways cells respond to stressful stimuli is through activa-tion of mitogen-activated protein kinases (MAPKS), specifically the p38 MAPK pathway, which is re-sponsible for apoptotic control. 16 Thus, gaining a deeper understanding of the mechanisms by which p38 MAPK controls cell survival can have direct im-plications on disease models of uncontrolled cellular growth such as cancer. Several studies have highlighted potential apoptotic signaling pathways, which rely on both GSK3β and p38 MAPK activity. 17 For exam-ple, a study has provided evidence to support p38 MAPK phosphorylation of GSK3β at serine 389 in the brain and thymocytes, thus regulating GSK3β’s downstream functions.18 However, to the best of our knowledge no previous research has identified how GSK3β responds to stress signaling in order to control nuclear transcription factors. Hence, further investigation into the interactions between stress response pathways such as the p38 MAPK path-way and GSK3β can provide significant insight into regulatory processes involved in cell growth under stressful conditions. We hypothesize that stressing the cell through the production of reactive oxygen species (ROS) by sodium arsenite and hydrogen peroxide will produce increased GSK3β nuclear lo-calization, thus more will be detected in the nucleus. Additionally, we hypothesize that GSK3β will re-spond to the cellular stress through the p38 MAPK pathway, thus when p38 MAPK is inhibited, GSK3β will be found in greater abundance in the cytoplasm compared to the nucleus.
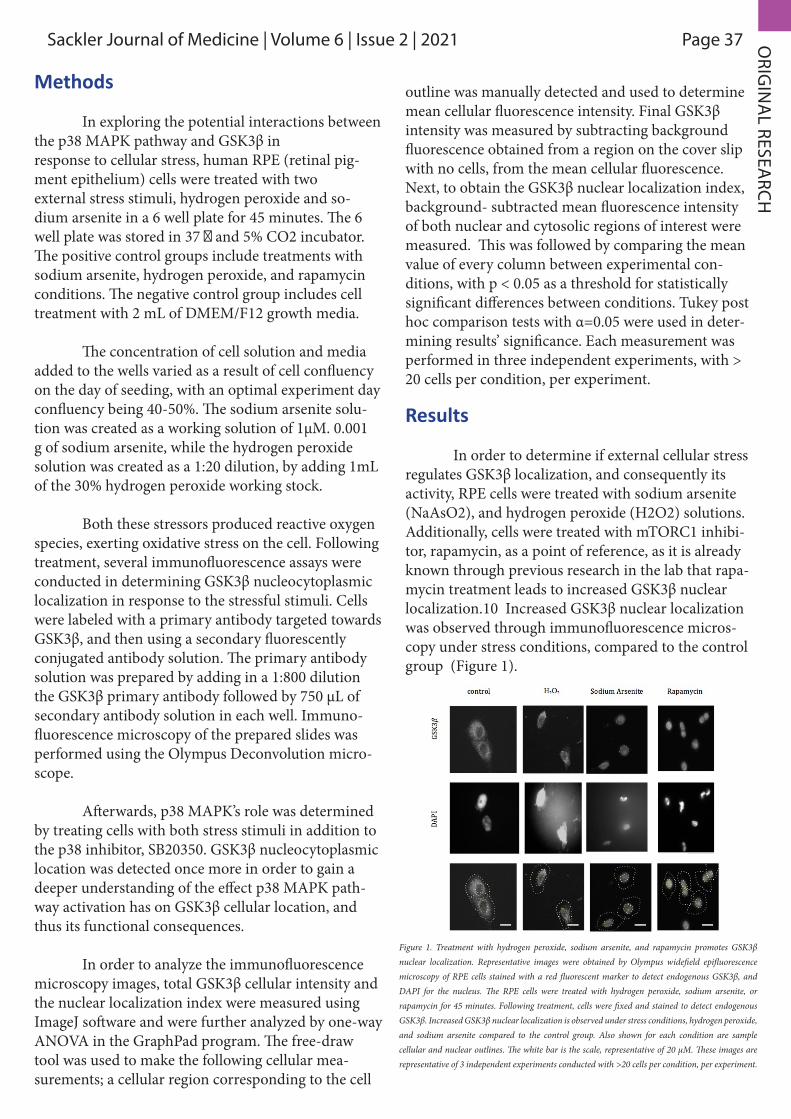
Page 37Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 ORIG
INA
L RESEARCH
Methods
In exploring the potential interactions between the p38 MAPK pathway and GSK3β inresponse to cellular stress, human RPE (retinal pig-ment epithelium) cells were treated with twoexternal stress stimuli, hydrogen peroxide and so-dium arsenite in a 6 well plate for 45 minutes. The 6 well plate was stored in 37 ‖ and 5% CO2 incubator. The positive control groups include treatments with sodium arsenite, hydrogen peroxide, and rapamycin conditions. The negative control group includes cell treatment with 2 mL of DMEM/F12 growth media.
The concentration of cell solution and media added to the wells varied as a result of cell confluency on the day of seeding, with an optimal experiment day confluency being 40-50%. The sodium arsenite solu-tion was created as a working solution of 1μM. 0.001 g of sodium arsenite, while the hydrogen peroxide solution was created as a 1:20 dilution, by adding 1mL of the 30% hydrogen peroxide working stock.
Both these stressors produced reactive oxygen species, exerting oxidative stress on the cell. Following treatment, several immunofluorescence assays were conducted in determining GSK3β nucleocytoplasmic localization in response to the stressful stimuli. Cells were labeled with a primary antibody targeted towards GSK3β, and then using a secondary fluorescently conjugated antibody solution. The primary antibody solution was prepared by adding in a 1:800 dilution the GSK3β primary antibody followed by 750 μL of secondary antibody solution in each well. Immuno-fluorescence microscopy of the prepared slides was performed using the Olympus Deconvolution micro-scope.
Afterwards, p38 MAPK’s role was determined by treating cells with both stress stimuli in addition to the p38 inhibitor, SB20350. GSK3β nucleocytoplasmic location was detected once more in order to gain a deeper understanding of the effect p38 MAPK path-way activation has on GSK3β cellular location, and thus its functional consequences.
In order to analyze the immunofluorescence microscopy images, total GSK3β cellular intensity and the nuclear localization index were measured using ImageJ software and were further analyzed by one-way ANOVA in the GraphPad program. The free-draw tool was used to make the following cellular mea-surements; a cellular region corresponding to the cell
outline was manually detected and used to determine mean cellular fluorescence intensity. Final GSK3β intensity was measured by subtracting background fluorescence obtained from a region on the cover slip with no cells, from the mean cellular fluorescence. Next, to obtain the GSK3β nuclear localization index, background- subtracted mean fluorescence intensity of both nuclear and cytosolic regions of interest were measured. This was followed by comparing the mean value of every column between experimental con-ditions, with p < 0.05 as a threshold for statistically significant differences between conditions. Tukey post hoc comparison tests with α=0.05 were used in deter-mining results’ significance. Each measurement was performed in three independent experiments, with > 20 cells per condition, per experiment.
Results
In order to determine if external cellular stress regulates GSK3β localization, and consequently its activity, RPE cells were treated with sodium arsenite (NaAsO2), and hydrogen peroxide (H2O2) solutions. Additionally, cells were treated with mTORC1 inhibi-tor, rapamycin, as a point of reference, as it is already known through previous research in the lab that rapa-mycin treatment leads to increased GSK3β nuclear localization.10 Increased GSK3β nuclear localization was observed through immunofluorescence micros-copy under stress conditions, compared to the control group (Figure 1).
Figure 1. Treatment with hydrogen peroxide, sodium arsenite, and rapamycin promotes GSK3β nuclear localization. Representative images were obtained by Olympus widefield epifluorescence microscopy of RPE cells stained with a red fluorescent marker to detect endogenous GSK3β, and DAPI for the nucleus. The RPE cells were treated with hydrogen peroxide, sodium arsenite, or rapamycin for 45 minutes. Following treatment, cells were fixed and stained to detect endogenous GSK3β. Increased GSK3β nuclear localization is observed under stress conditions, hydrogen peroxide, and sodium arsenite compared to the control group. Also shown for each condition are sample cellular and nuclear outlines. The white bar is the scale, representative of 20 μM. These images are representative of 3 independent experiments conducted with >20 cells per condition, per experiment.
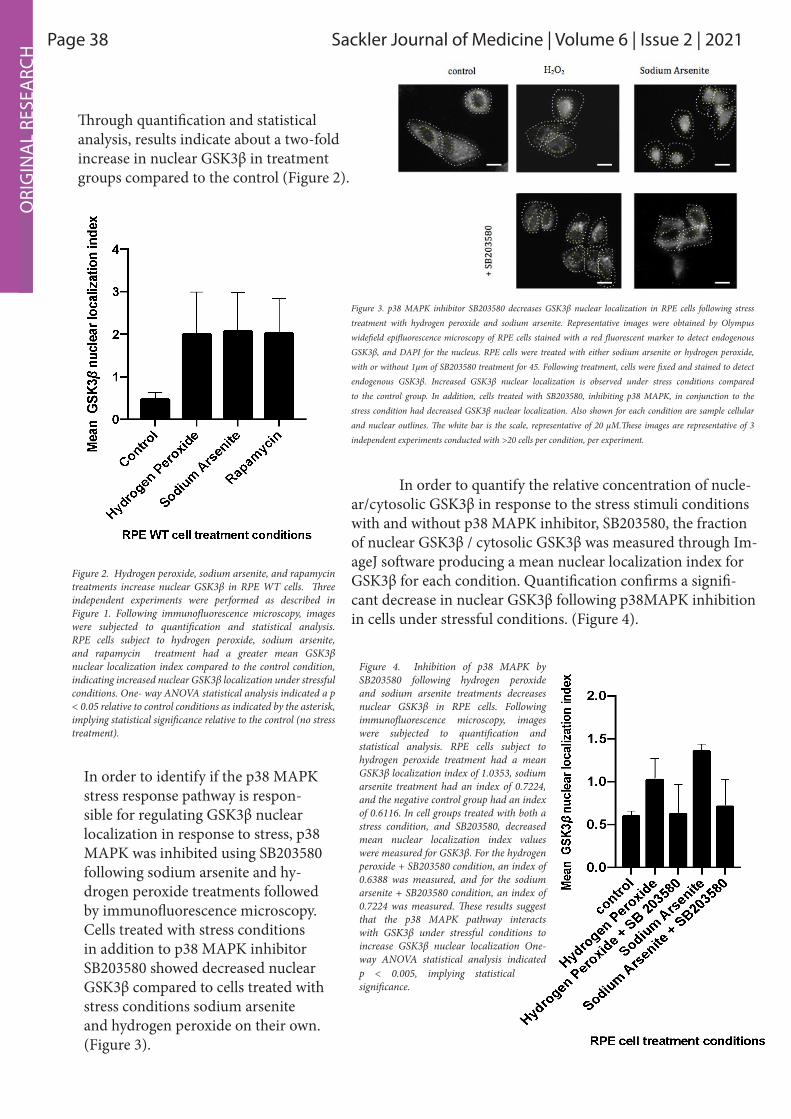
Page 38 Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 O
RIG
INA
L RE
SEA
RCH
Through quantification and statistical analysis, results indicate about a two-fold increase in nuclear GSK3β in treatment groups compared to the control (Figure 2).
In order to quantify the relative concentration of nucle-ar/cytosolic GSK3β in response to the stress stimuli conditions with and without p38 MAPK inhibitor, SB203580, the fraction of nuclear GSK3β / cytosolic GSK3β was measured through Im-ageJ software producing a mean nuclear localization index for GSK3β for each condition. Quantification confirms a signifi-cant decrease in nuclear GSK3β following p38MAPK inhibition in cells under stressful conditions. (Figure 4).
Figure 2. Hydrogen peroxide, sodium arsenite, and rapamycin treatments increase nuclear GSK3β in RPE WT cells. Three independent experiments were performed as described in Figure 1. Following immunofluorescence microscopy, images were subjected to quantification and statistical analysis. RPE cells subject to hydrogen peroxide, sodium arsenite, and rapamycin treatment had a greater mean GSK3β nuclear localization index compared to the control condition, indicating increased nuclear GSK3β localization under stressful conditions. One- way ANOVA statistical analysis indicated a p < 0.05 relative to control conditions as indicated by the asterisk, implying statistical significance relative to the control (no stress treatment).
In order to identify if the p38 MAPK stress response pathway is respon-sible for regulating GSK3β nuclear localization in response to stress, p38 MAPK was inhibited using SB203580 following sodium arsenite and hy-drogen peroxide treatments followed by immunofluorescence microscopy. Cells treated with stress conditions in addition to p38 MAPK inhibitor SB203580 showed decreased nuclear GSK3β compared to cells treated with stress conditions sodium arsenite and hydrogen peroxide on their own. (Figure 3).
Figure 3. p38 MAPK inhibitor SB203580 decreases GSK3β nuclear localization in RPE cells following stress treatment with hydrogen peroxide and sodium arsenite. Representative images were obtained by Olympus widefield epifluorescence microscopy of RPE cells stained with a red fluorescent marker to detect endogenous GSK3β, and DAPI for the nucleus. RPE cells were treated with either sodium arsenite or hydrogen peroxide, with or without 1μm of SB203580 treatment for 45. Following treatment, cells were fixed and stained to detect endogenous GSK3β. Increased GSK3β nuclear localization is observed under stress conditions compared to the control group. In addition, cells treated with SB203580, inhibiting p38 MAPK, in conjunction to the stress condition had decreased GSK3β nuclear localization. Also shown for each condition are sample cellular and nuclear outlines. The white bar is the scale, representative of 20 μM.These images are representative of 3 independent experiments conducted with >20 cells per condition, per experiment.
Figure 4. Inhibition of p38 MAPK by SB203580 following hydrogen peroxide and sodium arsenite treatments decreases nuclear GSK3β in RPE cells. Following immunofluorescence microscopy, images were subjected to quantification and statistical analysis. RPE cells subject to hydrogen peroxide treatment had a mean GSK3β localization index of 1.0353, sodium arsenite treatment had an index of 0.7224, and the negative control group had an index of 0.6116. In cell groups treated with both a stress condition, and SB203580, decreased mean nuclear localization index values were measured for GSK3β. For the hydrogen peroxide + SB203580 condition, an index of 0.6388 was measured, and for the sodium arsenite + SB203580 condition, an index of 0.7224 was measured. These results suggest that the p38 MAPK pathway interacts with GSK3β under stressful conditions to increase GSK3β nuclear localization One-way ANOVA statistical analysis indicated p < 0.005, implying statistical significance.

Page 39Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021 ORIG
INA
L RESEARCH
Discussion
Through a systematic, unbiased approach, we found that endogenous GSK3β may be regulated by stress induced pathways. When cells were treat-ed with hydrogen peroxide and sodium arsenite, a statistically significant difference was observed between nuclear GSK3β values compared to the control group. Both stress treatments lead to the production of reactive oxygen species (ROS) within the cell, leading to increased oxidative stress experi-enced by the cell. Literature has indicated that ROS can lead to both tumor growth promotion, and more commonly observed, induce apoptosis. 19 For example, chemotherapy and radiation thera-py often used in cancer treatment, rely on ROS to induce apoptosis in cancer cells. Moreover, several studies have indicated the role of ROS in extrinsic and intrinsic pathways promoting cell death.20 Our research on the regulation of GSK3β localiza-tion through stress pathway activation, may provide an additional intrinsic cellular pathway in which ROS can act and influence cell growth and prolifer-ation in a pathological setting. Specifically, an interesting follow up study would be to detect which specific nuclear transcrip-tion factors are up or down regulated as a result of the increased nuclear GSK3β in response to the stress conditions applied. By controlling GSK3β cel-lular location, one may potentially control the acti-vation or inactivation of its downstream substrates. In other words, GSK3β activity can be regulated by controlling its cellular location without directly activating or inactivating the kinase.12 Inhibition of the p38 MAPK pathway resulted in a statistically significant decrease in nuclear GSK3β compared to both the control and stress treatment conditions (Fig 4). This provides evidence to support p38 MAPK’s role in regulating GSK3β localization. As more GSK3β is present in the cytosol as a result of p38 MAPK inhibition, GSK3β does not have access to phosphorylate and regulate nuclear transcription factors in the nucle-us, which may be integral to cell growth regulation. In measuring the nuclear localization index of GSK3β, variations in values were observed between the first immunofluorescence assay measuring GSK3β in response to hydrogen peroxide and sodi-um arsenite, and the second immunofluorescence assay measuring GSK3β in response to hydrogen peroxide and sodium arsenite, as well as stress
treatments in conjunction with SB203580. A slight-ly increased mean nuclear localization index was observed in the first assay compared to the second. This variation may be attributed to both techni-cal and biological variability components. First, in conducting the treatment and immunostaining procedures a timer discrepancy may have occurred, resulting in unequal treatment times. Additionally, background noise in analyzing microscopic images may differ as a result of non-specific primary anti-body binding. Non-specific antibody binding can contribute to the detection of other proteins besides our protein of interest, GSK3β. Biological variabil-ity may have resulted as cells may have had varied glutathione concentrations. Glutathione is the cell’s natural antioxidant, acting to break down ROS, pre-venting cellular damage.21 In cells with increased glutathione concentrations, the stress conditions may not have been sufficient to induce the oxidative stress response in the cell, thus resulting in lowered nuclear GSK3β detected. In order to overcome such variability, additional technical replicates should be conducted.
What remains unknown is the mechanism by which p38 MAPK interacts with GSK3β to pro-mote nuclear localization. Two potential models of regulation may be proposed. One possibility is that p38 MAPK interacts directly with GSK3β, phos-phorylating GSK3β and consequently directing it to the nucleus. Another possibility is that p38 MAPK indirectly interacts with GSK3β by acting on the regulatory protein mTORC1(mTOR complex 1) or cytosolic proteins, which in turn interacts with GSK3β affecting its cellular localization. Attaining deeper insight into the mechanism by which the p38 MAPK pathway controls GSK3β nucleocytoplas-mic localization, and the upstream regulators that control this pathway can provide researchers with more specific therapeutic targets. By decreasing/increasing nuclear GSK3β, transcription factors associated with uncontrolled cell growth in cancer may be down regulated offering a promising ther-apeutic study. Moreover, many therapeutic cancer drugs rely on GSK3β nuclear localization as a mech-anism to decrease cell growth, such that failure to promote GSK3β nuclear signalling can lead to drug resistance. 22 Here, we propose an additional mech-anism by which this nuclear signalling can occur, combatting such drug resistance.

Page 40 Sackler Journal of Medicine | Volume 5 | Issue 2 | 2021 CO
MM
ENTA
RY/R
EVIE
W
Conclusion
Here, experimental results suggest a nov-el regulatory pathway in which the activation of stress-induced pathway, p38 MAPK, can regulate GSK3β nucleocytoplasmic localization. Treatment of RPE cells with sodium arsenite and hydrogen per-oxide led to increased GSK3β nuclear localization, thus providing GSK3β access to specific nuclear substrates, and indirectly controlling its activity. Inhibition of the p38 MAPK pathway with SB205380 led to decreased nuclear localization of GSK3β. These results indicate that the cell is responding to the stress conditions, in part through the p38 MAPK pathway, and provides evidence for a potential in-teraction between p38 MAPK and GSK3β in regu-lating GSK3β activity through localization. Future work should focus on the potential mechanism by which p38 MAPK interacts with GSK3β in response to stress conditions. Moreover, identification of the transcription factors regulated as a result of GSK3β nuclear localization can provide insight into new therapeutic targets for the control cell growth and proliferation identified in many disease models.
References
1. Beurel, E., Grieco, S. F., and Jope, R. S. Glycogen synthase kinase -3 (GSK3β): regulation, actions, and diseases. (2015) Pharmacol. Ther. 148, 114 –31
2. Doble, B. W., and Woodgett, J. R. GSK -3: tricks of the trade for a multi -tasking kinase. J. Cell Sci. (2003) 116, 1175 –86
3. Cormier, K. W., and Woodgett, J. R. Recent advances in understanding the cellular roles of GSK -3. (2017) F1000Research. 6, 167
4. Sutherland, C. What Are the bona fide GSK3β Substrates? (2011) Int. J. Alzheimers. Dis. 2011, 1 – 23
5. Jope, R. S., and Johnson, G. V. The glamour and gloom of glycogen synthase kinase -3. . (2004) Trends Biochem. Sci. 29, 95 –102
6. Beurel, E., Grieco, S. F., & Jope, R. S. Glycogen synthase kinase-3 (GSK3β): Regulation, actions, and diseases. (2015) Pharmacology & Therapeutics,148,
114-131. doi:10.1016/j.pharmthera.2014.11.016
7. Bijur GN, Jope RS. Glycogen synthase kinase-3β is highly activated in nuclei and mitochondria. Neuroreport. (2003);14:2415–2419.
8. Beurel, E., Grieco, S. F., & Jope, R. S. Glycogen synthase kinase-3 (GSK3β): Regulation, actions, and diseases. (2015). Pharmacology & Therapeutics,148, 114-131. doi:10.1016/j.pharmthera. (2014) 11.016
9. Diehl, J. A., Cheng, M., Roussel, M. F., and Sherr, C. J. Glycogen synthase kinase -3beta regulates cyclin D1 proteolysis and subcellular localization. (1998) Genes Dev. 12, 3499 –511
10. Bautista, S. J., Boras, I., Vissa, A., Mecica, N., Yip, C. M., Kim, P. K., & Antonescu, C. N. MTOR complex 1 controls the nuclear localization and function of glycogen synthase kinase 3β. (2018). Journal of Biological Chemistry,293(38), 14723-14739. doi:10.1074/jbc.ra118.002800
11. Bechard, M., and Dalton, S. Subcellular localization of glycogen synthase kinase 3beta controls embryonic stem cell self-renewal. (2009) Mol. Cell. Biol. 29, 2092 –104
12. Suzuki T, Bridges D, Nakada D, Skiniotis G, Morrison SJ, Lin JD, et al. Inhibition of AMPK Catabolic Action by GSK3β. Mol Cell. (2013) ;50:407–419.
13. Fiol, C. J., Williams, J. S., Chou, C. H., Wang, Q. M., Roach, P. J., and Andrisani, O. M. A secondary phosphorylation of CREB341 at Ser129 is required for the cAMP -mediated control of gene expression. A role for glycogen synthase kinase -3 in the control of gene expression. (1994) J. Biol. Chem. 269, 32187 –93
14. Kalkat, M., De Melo, J., Hickman, K. A., Lourenco, C., Redel, C., Resetca, D., Tamachi, A., Tu, W. B., and Penn, L. Z. MYC Deregulation in Primary Human Cancers. (2017) Genes (Basel). 8, 151
15. Franca-Koh, J.; Yeo, M.; Fraser, E.; Young, N.; Dale, T. C. J. Biol. Chem. (2002,) 277 (46), 43844-43848
ORI
GIN
AL
RESE
ARC
H

Page 41Sackler Journal of Medicine | Volume 5 | Issue 2 | 2021 COM
MEN
TARY/REVIEW
16. Zarubin, T.; Han, J. Cell Res. (2005,) 15 (1), 11-18
17. Thornton T, Pedraza-Alva G, Deng B, Wood C, Aronshtam A, Clements J, Sabio G, Davis R, Matthews D, Doble B, Rincon M. Phosphorylation by p38 MAPK as an alternative pathway for GSK3βbeta inactivation. Science. (2008;) 320:667–670
18. Ambrosino, C., & Nebreda, A. R. Cell cycle regulation by p38 MAP kinases. (2001). Biology of the Cell,93(1-2), 47-51. doi:10.1016/s0248-4900(01)01124-8
19. Valluru, L., Dasari, S., & Wudayagiri, R. Role of free radicals and antioxidants in gynecological cancers: Current status and future prospects. (2014). Oxidants and Antioxidants in Medical Science,3(1), 15. doi:10.5455/oams.201113.rv.011
20. Irani, K., Xia, Y., Zweier, J. L., Sollott, S. J., Der, C. J., Fearon, E. R., . . . Goldschmidt-Clermont, P. J. Mitogenic Signaling Mediated by Oxidants in Ras-Transformed Fibroblasts. (1997). Science,275(5306), 1649-1652. doi:10.1126/science.275.5306.1649
21. Dickinson, B. C., & Chang, C. J. Chemistry and biology of reactive oxygen species in signaling or stress responses. (2011). Nature Chemical Biology,7(8), 504-511. doi:10.1038/nchembio.607
22. He, L., Fei, D., Nagiec, M., Mutvei, A., Lamprakis, A., Kim, B. and Blenis, J., Regulation of GSK3β cellular location by FRAT modulates mTORC1-dependent cell growth and sensitivity to rapamycin. (2019) Proceedings of the National Academy of Sciences, 116(39), pp.19523-19529.
ORIG
INA
L RESEARCH

Page 42 Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021
Sackler Art of MedicineSpring 2021 Contest Winners

Page 43Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021
By Jillian Shapiro
The most logical place to start would be when I was born, but it really began well before that. Because of my father’s genetic disease, cystic fibrosis, and my mother’s poor quality ova, my twin sister and I were conceived through in vitro fertilization. We left the comfort of our mother’s womb after a brief thirty-two weeks. It was really only comfortable for me; my twin sister, not receiving the nutrients she needed, was not expected to survive. I value logic, reason, and predictability but recognize that science cannot explain everything. My biology textbook tells me that my dad is twenty years past his life expectancy. Those with cystic fibrosis are not expected to live past their mid-thirties, and yet here he is, fifty-three. Science was not able to predict my father’s future. Doctors told my parents to say goodbye to my twin sister. They suspected she would not live through the preg-nancy. Against the odds, we recently celebrated our twenty-second birthday, together. Growing up surrounded by disability and ill-ness, I learned how difficult this can be on both the patient and the family. Watching my father’s daily routine of chest physical therapy, nebulized breath-ing treatments, and fistfuls of pills was and still is exhausting. Seeing kids at school bully my blind twin sister was heartbreaking. After being engulfed in this harsh reality of disease and disability, I strive to be understanding and inclusive, to help those who feel as if they stand out blend into the sea of the ordinary. I believe that every person should feel as if they belong, and I aim to make that happen. The scientific and methodical part of me has always wanted life to be exactly like a mathematical function: for every x there is only one y, for every action there is only one possible reaction. Experi-ence has taught me that this is not true, even with our vast understanding of science and medicine. Life is not clear cut like a mathematical function; it’s not always predictable. Intellectually, I find this concept frustrating, but emotionally, I am so grateful. Be-cause of this unpredictability, I have grown up with
a loving, caring father and my twin sister as my best friend. However, throughout my life, I have had to deal with this unpredictability when it comes to the health of my family; it is scary and overwhelming to be in an unfamiliar position and to not feel in control of something you care so much about. This is something that patients and their families feel on a daily basis. A few years ago, my sister came home from one of her many surgeries. Instead of complaining about what she had been through, she excitedly told me how the anesthesiologist told her jokes as she fell asleep and that her mask smelled like chocolate chip cookies, so she dreamed of baked goods. I have observed many similar stories while interning at Boston Children’s Hospital. Over the years, I have learned it is the small interactions that can make a hospital less scary. Seeing the role that doctors, scientific re-search, and discovery have played in my family’s medical history has given me a unique perspective and solidified my desire to become a physician. I believe this perspective will be incredibly valuable in my anticipated specialty of pediatrics, where inter-personal relationships, both with the patient and with their family, are vital and unique. I plan to do this by providing high quality ethical care and using my knowledge, compassion, and kindness, just like some of the greatest doctors who helped my dad and sister along the way. Our job as physicians extends far beyond medicine; we are responsible for refuah shlema of body, mind, and spirit.
Body, Mind, and Spirit
Page 44 Sackler Journal of Medicine | Volume 6 | Issue 2 | 2021
By Hannah Sragovicz
The first time I saw my cadaver’s face, I immediately left the lab, went straight home, and binged watched The Queen’s Gambit from beginning to end in one sitting. I don’t think I blinked for seven hours. Of course, I wrote that last part for dramatic effect and it doesn’t even work because anyone reading this is probably now mentally reciting which cranial nerves are involved in blinking. I just thought this dramatic detail would be a nice touch, to paint a picture of how freaked out and overwhelmed I was that day. I spent the rest of that week daydreaming about what my dad, my sister, my nephew would look like as a midsaggital view of the larynx. How big is my spleen? How blue is my substantia nigra? I fret about acne, cellulite, a chin hair here and there…and now I fret…do I have a palmar-is longus? Honestly what even is the midbrain, and what does mine look like? I really should call my dad more because one day he will be a midsaggital view of the larynx and so will I and what’s even the point of eyeliner. Who invented pants? “Who would fardels bear, but that the dread of something after death, the undiscovered country, from whose bourn no traveler returns, puzzles the will, and makes us rather bear those ills we have than fly to others that we know not of?” Zoning out by the toaster oven as I prepare my third quesadilla of the day, I catch the reflection of a skull on the kitchen table. That’s fine! That’s okay, that’s fine. It’s a study tool, we’re learning the cranial nerves, no big deal, all good, cool…sure, totally. I honestly understand why Hamlet was having a meltdown. When did I get so melodramatic? A week later, I’m thrilled. I finally nailed down the branches of the facial nerve. I don’t even need to see them relative to each other - I know where they are based on other landmarks. “To Zanzibar, by motor car!” Behind my mask, I’m beaming. I look up from my notes and see a guy I’ve never seen before, staring at me, then at the cadaver, then back at me. Wide-eyed, stunned, clearly his first time in the lab. I recommend The Queen’s Gambit.
Alas, Poor Yorick!

Sackler Journal of Medicine
By Hannah Sragovicz
Related Documents











