ONLINE SUPPLEMENT Short-term exposure to fine particulate matter and risk of ischemic stroke Ryu Matsuo, Takehiro Michikawa, Kayo Ueda, Tetsuro Ago, Hiroshi Nitta, Takanari Kitazono, and Masahiro Kamouchi, on behalf of the Fukuoka Stroke Registry Investigators

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ONLINE SUPPLEMENT Short-term exposure to fine particulate matter and risk of ischemic stroke Ryu Matsuo, Takehiro Michikawa, Kayo Ueda, Tetsuro Ago, Hiroshi Nitta, Takanari Kitazono, and Masahiro Kamouchi, on behalf of the Fukuoka Stroke Registry Investigators

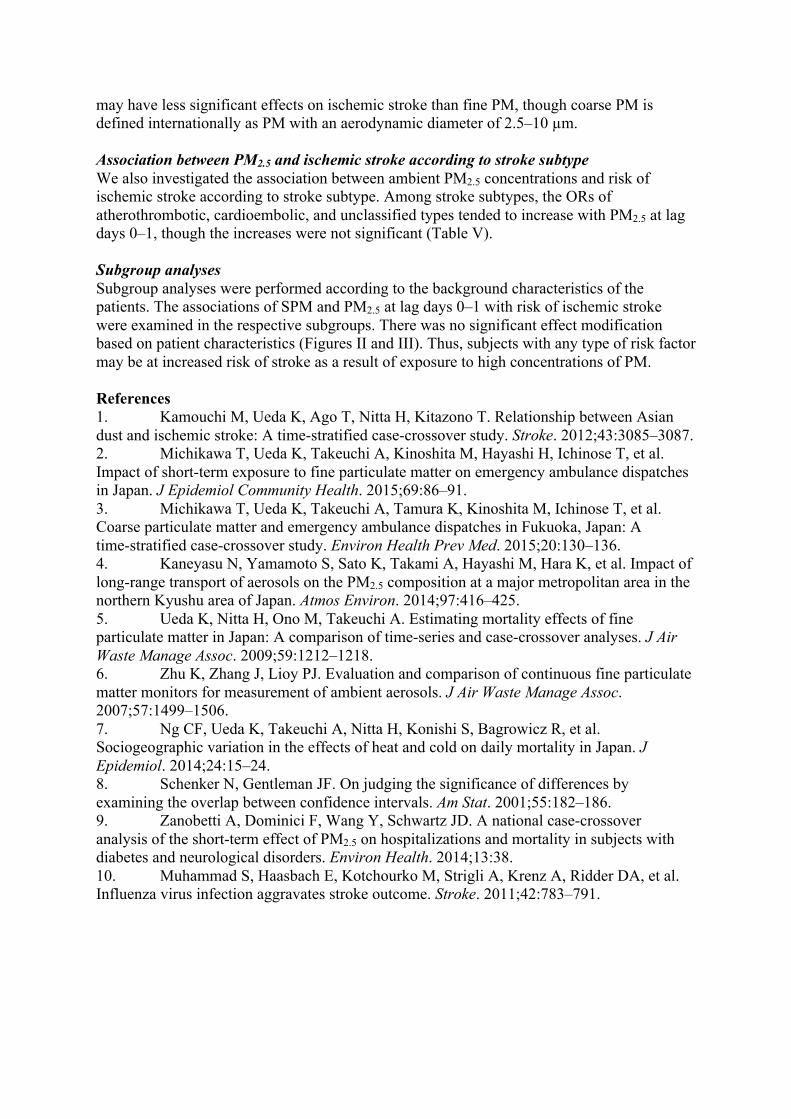
Methods Patient data We investigated the impact of ambient particulate matter (PM) prior to stroke onset on the subsequent occurrence of ischemic stroke in patients who were hospitalized in the Fukuoka Stroke Registry (FSR). The FSR is a multicenter hospital-based registry that enrolls acute stroke patients within 7 days of onset (UMIN Clinical Trial Registry 000000800). Seven hospitals in Fukuoka Prefecture (3 hospitals in Fukuoka, 1 in Koga, 2 in Kitakyushu, and 1 in Kurume), Japan, participated in the FSR. Stroke was confirmed by computed tomography or magnetic resonance imaging. The study protocol was approved by the institutional review boards of all hospitals. Ischemic stroke was classified into four subtypes: cardioembolic, atherosclerotic, lacunar, and unclassified.1 Among a total of 16,221 patients with ischemic stroke enrolled in the FSR between June 1999 and August 2014, 16,207 patients ≥20 years old were selected. The present study included ambient concentrations of PM as a variable. We therefore excluded 993 nosocomial patients and 875 patients with severely impaired activities of daily living before stroke onset (modified Rankin scale ≥4), because they may have had less opportunity to be exposed to air pollutants. Patients who were hospitalized during the period without fine PM (PM2.5) data, and patients admitted to hospital >24 hours after stroke onset were also excluded. Finally, patients with transient ischemic attack were excluded because of the ambiguity of onset time. We therefore analyzed data for the remaining 6,885 patients in this study (Figure I). Environmental data Fukuoka Prefecture is located on Kyushu island in the western part of Japan (130.24E, 33.35N). It is the closest of Japan’s main islands to the Asian continent, and is susceptible to transboundary air pollution.1-3 PM2.5 concentrations in Fukuoka are frequently elevated as a result of the inflow of long-range transported aerosols throughout the year,4 leading to a wide range of daily PM concentrations in Fukuoka.2,5 Measurements were taken at eight monitoring stations in Fukuoka, which were designed to monitor background concentrations of air pollutants. Data were averaged across the monitoring stations to calculate citywide daily mean concentrations of PM2.5, suspended particulate matter (SPM), nitrogen dioxide (NO2), and sulfur dioxide (SO2), and the citywide daily maximum 8-hour mean concentrations of photochemical oxidants (Ox, a proxy for ozone including ozone and other secondary oxidants generated by a photochemical reaction). Fukuoka was only the city in Fukuoka Prefecture measuring concentrations of PM2.5 until March 2011. Although two hospitals in Kitakyushu were located approximately 38 miles (60 km) east of Fukuoka, and one hospital in Kurume was approximately 19 miles (30 km) south of Fukuoka, we assigned the concentrations of PM2.5 in Fukuoka to all patients, given that the daily concentrations of PM2.5 in Kitakyushu were highly correlated with those in Fukuoka (Pearson’s correlation coefficient 0.92). We also assigned the concentrations of SPM, NO2, SO2, and Ox in Fukuoka to all patients based on good correlations between daily concentrations of these pollutants in Fukuoka and the other two cities. Mass concentrations of SPM were measured by β-ray absorption. PM2.5 concentrations were measured using a tapered element oscillating microbalance from April 2011 to March 2011 and by β-ray absorption from April 2011 to March 2013. The microbalance measurement was from a Japan Ministry of the Environment survey, and the other recordings were routine measurements started after the setting of an air-quality standard for PM2.5 in Japan. Concentrations of PM2.5 measured by both methods were strongly correlated with those obtained from the federal reference method.6 Under the Japan Air Quality Standards from the Japan Ministry of the Environment, SPM is defined as airborne particles with a 100% cut-off level at a 10-µm aerodynamic diameter,

which is estimated to be equivalent to PM with an aerodynamic diameter <7 µm (PM7).3 In the present study, we used the difference between the concentrations of SPM and PM2.5 as a surrogate marker of coarse PM (PM7–2.5), because PM10 (PM with an aerodynamic diameter ≤10 µm) was not monitored in Japan. Statistical analysis The average concentrations of PM with different lag times (0–1, 0–2, 0–3, 0–4, 0–5, 0–6, 2–3, or 4–6 days) were used as variables. Ambient temperature at lag 0–14 was calculated by a natural cubic spline with four degrees of freedom over 2 weeks, to account for the long delay of the effects of cold.7 Odds ratios (ORs) (95% confidence intervals) of occurrence of ischemic stroke per 10-µg/m3 increase in SPM or PM2.5 were estimated after adjusting for ambient temperature or after entering the concentrations of SPM or PM2.5 at lags of 0–1, 2–3, and 4–6 simultaneously and ambient temperature into the model. The two-pollutant model additionally adjusted for co-pollutants at lags 0–1, 2–3, and 4–6.2,3 Pearson’s correlation coefficients between air pollutants are shown in Table III. To determine if the association between PM and ischemic stroke was modified by patient characteristics, we performed stratified analyses according to the following characteristics: age (20–69 years, 70 years or older), sex (men, women), hypertension defined as systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg in the chronic stage or as current treatment with antihypertensive drugs (no, yes), diabetes mellitus defined as either the diagnostic criteria of the Japan Diabetes Society in the chronic stage or based on a medical history of diabetes (no, yes), atrial fibrillation defined based on electrocardiographic findings on admission or during hospitalization, or a previous history (no, yes), current or former smokers (no, yes), and history of ischemic stroke (no, yes). The effect modification was tested statistically using two methods. A Wald test was performed in the models with or without interaction terms for the average concentrations of PM at days 0-1 × variables of interest. Additionally, differences between point estimates in
the two subgroups and the 95% CI were also calculated as: (𝑄!-𝑄!)±1.96 𝑆𝐸!! + 𝑆𝐸!
!, where 𝑄! and 𝑄! are the estimates for the two categories, and 𝑆𝐸! and 𝑆𝐸! are their respective standard errors. The effect modification was considered important when the interval did not contain zero.8,9 We performed sensitivity analyses to determine the robustness of our primary results. First, we restricted the analyses to the cold season, when the PM2.5 concentration is primarily dominated by long-range transported air pollution rather than domestic urban air pollution.4 Second, we restricted the analyses to patients admitted to four hospitals in Fukuoka Prefecture (3 hospitals in Fukuoka and 1 hospital in Koga, which was included because of its proximity to Fukuoka) to examine the effect of distance from the monitoring stations. Third, we excluded patients who were admitted on a national holiday because of the bias in selecting controls. Fourth, we additionally adjusted for influenza epidemics, defined as weeks above the 90th percentile of the distribution during the study period7, given that influenza is a suspected trigger of stroke.10 All statistical analyses were performed using statistical software Stata14 (Stata Corporation, College Station, TX, USA) and SAS 9.4 (SAS Institute, Cary, NC, USA). Results Association between coarse PM and ischemic stroke We investigated the association between coarse PM (PM7–2.5) and the subsequent occurrence of ischemic stroke (Table IV). The ORs of ischemic stroke tended to increase with ambient coarse PM at lag days 0–1, but the result was not significant. This suggests that coarse PM
may have less significant effects on ischemic stroke than fine PM, though coarse PM is defined internationally as PM with an aerodynamic diameter of 2.5–10 µm. Association between PM2.5 and ischemic stroke according to stroke subtype We also investigated the association between ambient PM2.5 concentrations and risk of ischemic stroke according to stroke subtype. Among stroke subtypes, the ORs of atherothrombotic, cardioembolic, and unclassified types tended to increase with PM2.5 at lag days 0–1, though the increases were not significant (Table V). Subgroup analyses Subgroup analyses were performed according to the background characteristics of the patients. The associations of SPM and PM2.5 at lag days 0–1 with risk of ischemic stroke were examined in the respective subgroups. There was no significant effect modification based on patient characteristics (Figures II and III). Thus, subjects with any type of risk factor may be at increased risk of stroke as a result of exposure to high concentrations of PM. References 1. Kamouchi M, Ueda K, Ago T, Nitta H, Kitazono T. Relationship between Asian dust and ischemic stroke: A time-stratified case-crossover study. Stroke. 2012;43:3085–3087. 2. Michikawa T, Ueda K, Takeuchi A, Kinoshita M, Hayashi H, Ichinose T, et al. Impact of short-term exposure to fine particulate matter on emergency ambulance dispatches in Japan. J Epidemiol Community Health. 2015;69:86–91. 3. Michikawa T, Ueda K, Takeuchi A, Tamura K, Kinoshita M, Ichinose T, et al. Coarse particulate matter and emergency ambulance dispatches in Fukuoka, Japan: A time-stratified case-crossover study. Environ Health Prev Med. 2015;20:130–136. 4. Kaneyasu N, Yamamoto S, Sato K, Takami A, Hayashi M, Hara K, et al. Impact of long-range transport of aerosols on the PM2.5 composition at a major metropolitan area in the northern Kyushu area of Japan. Atmos Environ. 2014;97:416–425. 5. Ueda K, Nitta H, Ono M, Takeuchi A. Estimating mortality effects of fine particulate matter in Japan: A comparison of time-series and case-crossover analyses. J Air Waste Manage Assoc. 2009;59:1212–1218. 6. Zhu K, Zhang J, Lioy PJ. Evaluation and comparison of continuous fine particulate matter monitors for measurement of ambient aerosols. J Air Waste Manage Assoc. 2007;57:1499–1506. 7. Ng CF, Ueda K, Takeuchi A, Nitta H, Konishi S, Bagrowicz R, et al. Sociogeographic variation in the effects of heat and cold on daily mortality in Japan. J Epidemiol. 2014;24:15–24. 8. Schenker N, Gentleman JF. On judging the significance of differences by examining the overlap between confidence intervals. Am Stat. 2001;55:182–186. 9. Zanobetti A, Dominici F, Wang Y, Schwartz JD. A national case-crossover analysis of the short-term effect of PM2.5 on hospitalizations and mortality in subjects with diabetes and neurological disorders. Environ Health. 2014;13:38. 10. Muhammad S, Haasbach E, Kotchourko M, Strigli A, Krenz A, Ridder DA, et al. Influenza virus infection aggravates stroke outcome. Stroke. 2011;42:783–791.

Table I. Background characteristics of patients. Age, year, mean (SD) 72.2 (11.9) Women, n (%) 2711 (39.4) Risk factors, n (%) Hypertension 5298 (76.9) Diabetes 2161 (31.4) Dyslipidemia 2859 (41.5) Atrial fibrillation 1967 (28.6) Obesity 1561 (22.7) Smoking 3167 (46.0) Drinking 2397 (34.8) Previous ischemic stroke, n (%) 1414 (20.5) Ischemic heart disease, n (%) 1045 (15.2) Chronic kidney disease, n (%) 2354 (34.2) Stroke subtype, n (%) Atherothrombotic 1414 (20.5) Lacunar 2149 (31.2) Cardioembolic 1946 (28.3) Unclassified 1376 (20.0)

Table II. Daily mean levels of air pollutants and meteorological variables. Mean (SD) Min 25% 50% 75% Max Air pollutants SPM, µg/m3 (n=4383) 29.3 (16.4) 5.3 18.3 25.4 36.0 229.9 Coarse PM, µg/m3 (n=4263) 9.9 (7.3) 0.02 4.3 7.3 11.2 160.7 PM2.5, µg/m3 (n=4311) 20.5 (11.2) 2.9 12.4 17.9 25.9 94.7 NO2, ppb (n=4383) 15.2 (7.1) 1.9 9.8 13.9 19.5 51.9 Ox, ppb (n=4383) 43.7 (15.0) 4.5 33.7 42.5 53.0 122.9 SO2, ppb (n=4383) 3.5 (1.6) 0.7 2.5 3.4 4.5 15.0 Ambient temperature, °C (n=4383) 17.3 (7.9) −0.8 10.4 17.8 24.1 31.8
SPM, suspended particulate matter; PM, particulate matter; NO2, nitrogen dioxide; Ox, photochemical oxidants; SO2, sulfur dioxide; ppb, parts per billion. Data on 24-hour mean PM2.5 were available for 4311 of the 4383 study days. Concentrations of coarse PM were defined as the difference between concentrations of SPM and PM2.5. We obtained negative values for coarse PM on 48 days, and excluded those days from the analyses. Concentrations of Ox are shown as daily maximum 8-hour mean concentrations.

Table III. Pearson’s correlation coefficient between air pollutants. PM2.5 SPM Coarse PM NO2 Ox SO2 PM2.5 1.00 0.91 0.47 0.41 0.44 0.60 SPM 1.00 0.8 0.29 0.34 0.49 Coarse PM 1.00 0.02 0.09 0.19 NO2 1.00 -0.09 0.54 Ox 1.00 0.23 SO2 1.00 SPM, suspended particulate matter; PM, particulate matter; NO2, nitrogen dioxide; Ox, photochemical oxidants; SO2, sulfur dioxide. Pearson’s correlation coefficients between two pollutants are shown.

Table IV. Association between coarse particulate matter and risk of ischemic stroke. Lag 0–1 Lag 2–3 Lag 4–6 Coarse PM* 1.02 (0.97–1.07) 1.00 (0.94–1.06) 1.00 (0.94–1.06) Adjusted for NO2 1.02 (0.97-1.07) 1.00 (0.94-1.06) 0.99 (0.94-1.05) Adjusted for Ox 1.02 (0.97-1.07) 1.00 (0.95-1.06) 1.00 (0.95-1.06) Adjusted for SO2 1.01 (0.96-1.07) 1.00 (0.95-1.06) 1.00 (0.94-1.05) PM, particulate matter; NO2, nitrogen dioxide; Ox, photochemical oxidants; SO2, sulfur dioxide. *Odds ratios (95% confidence intervals) of occurrence of ischemic stroke per 10-µg/m3 increase in coarse PM were estimated by entering the concentrations of coarse PM at lags 0–1, 2–3, and 4–6 simultaneously and ambient temperature into the model. The two-pollutant model additionally adjusted for each co-pollutant at lags 0–1, 2–3, and 4–6.

Table V. Association between PM2.5 (per 10 µg/m3) and risk of each stroke subtype. Lag 0–1 Lag 2–3 Lag 4–6 Atherothrombotic (n=1 414) 1.03 (0.97–1.12) 1.01 (0.94–1.08) 0.99 (0.92–1.07) Lacunar (n=2 149) 1.01 (0.96–1.07) 0.96 (0.91–1.02) 0.96 (0.91–1.02) Cardioembolic (n=1 946) 1.03 (0.97–1.09) 0.99 (0.93–1.05) 1.04 (0.97–1.10) Unclassified (n=1 376) 1.06 (0.99–1.14) 0.94 (0.87–1.02) 1.02 (0.94–1.10) PM, particulate matter. Odds ratios (95% confidence intervals) of occurrence of ischemic stroke per 10-µg/m3 increase in PM2.5 were estimated according to stroke subtypes by entering the concentrations of PM2.5 at lags 0–1g 2–3, and 4–6 simultaneously and ambient temperature into the model.
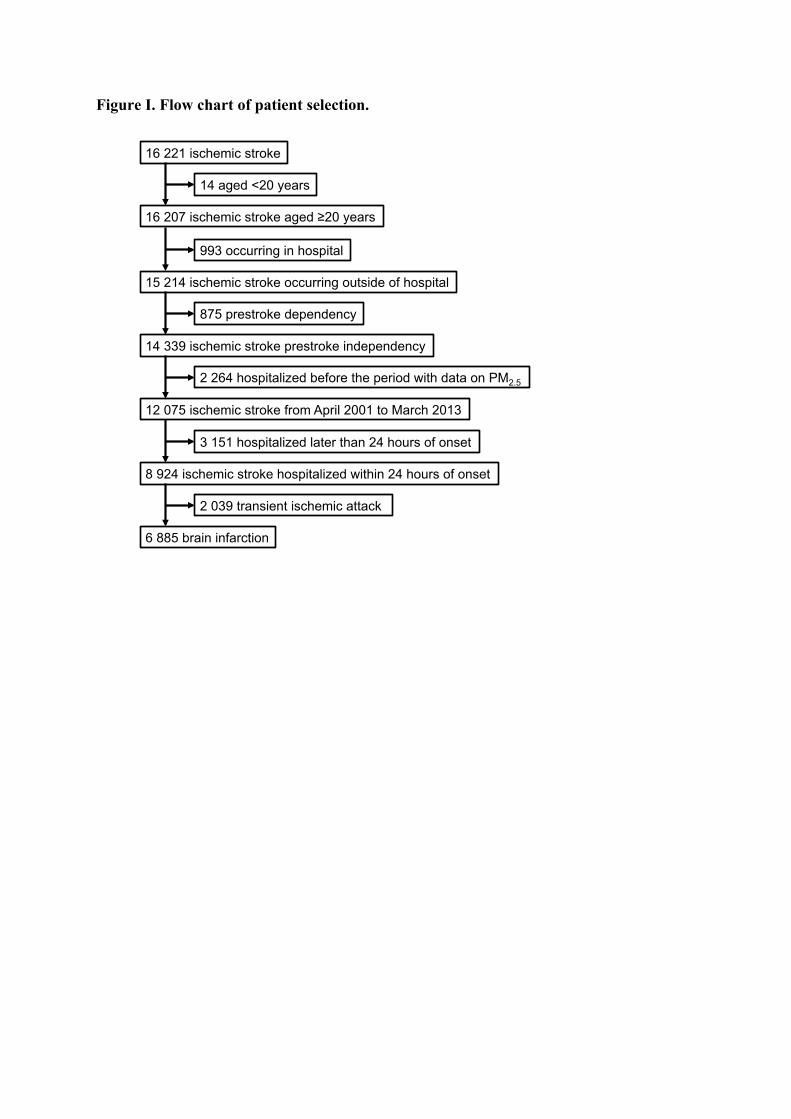
Figure I. Flow chart of patient selection.
16 221 ischemic stroke�
16 207 ischemic stroke aged ≥20 years�
14 aged <20 years�
15 214 ischemic stroke occurring outside of hospital�
993 occurring in hospital�
14 339 ischemic stroke prestroke independency�
875 prestroke dependency�
12 075 ischemic stroke from April 2001 to March 2013�
2 264 hospitalized before the period with data on PM2.5 �
8 924 ischemic stroke hospitalized within 24 hours of onset �
3 151 hospitalized later than 24 hours of onset�
6 885 brain infarction�
2 039 transient ischemic attack�
Figure II. Association between SPM (per 10 µg/m3) at lag 0–1 and risk of ischemic stroke according to patient characteristics. Multivariate-adjusted odds ratios (squares) and 95% confidence intervals (bars) per 10 µg/m3 SPM at lag 0–1 are shown according to each subgroup. The multivariate model included the concentrations of SPM at lags 0–1, 2–3, and 4–6 simultaneously and ambient temperature. P for effect modification was calculated using the interaction term.

Figure III. Association between PM2.5 (per 10 µg/m3) at lag 0–1 and risk of ischemic stroke according to patient characteristics. Multivariate-adjusted odds ratios (squares) and 95% confidence intervals (bars) per 10 µg/m3 PM2.5 at lag 0–1 are shown according to each subgroup. The multivariate model included the concentrations of PM2.5 at lags 0–1, 2–3, and 4–6 simultaneously and ambient temperature. P for effect modification was calculated using the interaction term.

Appendix The participating hospitals in the Fukuoka Stroke Registry were as follows: Kyushu University Hospital, National Hospital Organization Kyushu Medical Center, National Hospital Organization Fukuoka-Higashi Medical Center, Fukuoka Red Cross Hospital, St. Mary’s Hospital, Steel Memorial Yawata Hospital, and the Japan Labor Health and Welfare Organization Kyushu Rosai Hospital. The steering committee of the FSR included Takao Ishitsuka (Fukuoka Mirai Hospital), Setsuro Ibayashi (Seiai Rehabilitation Hospital), Kenji Kusuda (Seiai Rehabilitation Hospital), Kenichiro Fujii (Japan Seafarers Relief Association Moji Ekisaikai Hospital), Tetsuhiko Nagao (Midorino Clinic), Yasushi Okada (National Hospital Organization Kyushu Medical Center), Masahiro Yasaka (National Hospital Organization Kyushu Medical Center), Hiroaki Ooboshi (Fukuoka Dental College Medical and Dental Hospital), Takanari Kitazono (Kyushu University), Katsumi Irie (Hakujyuji Hospital), Tsuyoshi Omae (Imazu Red Cross Hospital), Kazunori Toyoda (National Cerebral and Cardiovascular Center), Hiroshi Nakane (National Hospital Organization Fukuoka-Higashi Medical Center), Masahiro Kamouchi (Kyushu University), Hiroshi Sugimori (Saga-Ken Medical Centre Koseikan), Shuji Arakawa (Steel Memorial Yawata Hospital), Kenji Fukuda (St. Mary’s Hospital), Ago Tetsuro (Kyushu University Hospital), Jiro Kitayama (Fukuoka Red Cross Hospital), Shigeru Fujimoto (Jichi Medical University), Shoji Arihiro (Japan Labor Health and Welfare Organization Kyushu Rosai Hospital), Junya Kuroda (Kyushu University Hospital), Yoshinobu Wakisaka (Kyushu University Hospital), Yoshihisa Fukushima (St. Mary’s Hospital), and Ryu Matsuo (Kyushu University).
Related Documents











